People with Parkinson’s Need You to Be Aware in Care Joan Gardner RN BSN Nurse Clinician, Clinic Supervisor Struthers Parkinson’s Center Minneapolis, MN
A National Parkinson Foundation Center of Excellence
Parkinson’s Disease Care in the Assisted Living Care Setting
▶ The launch of the National Parkinson Foundation (NPF) Aware in Care Program has helped raise awareness of the unique care needs of the hospitalized patient with Parkinson’s disease (PD) – Lack of understanding regarding
medication management in PD – Lack of understanding of contraindicated
medications for those with PD ▶ Information learned from the hospital
Aware in Care program can be transferred to care gaps in the Assisted Living care setting
The Aware in Care toolkit ▶ Helps patients and families advocate for themselves
– Understand the risks associated with hospital stays – Be prepared in case you have to go to the hospital—whether
planned or unplanned – Develop strategies to get better care in the hospital
▶ Draws attention to the high rate of complications when PD pills are not given on time
• 3 out of 4 people with Parkinson’s disease do not receive medications on time in the hospital
• 61% of patients who did not get their medications on time had serious complications from it

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
Parkinson's Disease in the Assisted Living Setting
▶ Nursing staff and direct care staff may not have much experience with PD residents
▶ Staffing shortages and/or staffing cuts - little time to invest in education
▶ If education occurs, usually is focused on the nursing staff, not on direct care staff
▶ Any knowledge taught is lost with frequent staff turnover
Importance of Care Staff to be Aware in Care
▶ Incidence of PD is expected to double by 2030 – Increasing longevity of Americans with better
management of chronic conditions of middle-age such as diabetes, hypertension, high cholesterol, etc.
▶ Many with Parkinson’s will need to leave their home due to need of hands-on care as PD symptoms progress

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

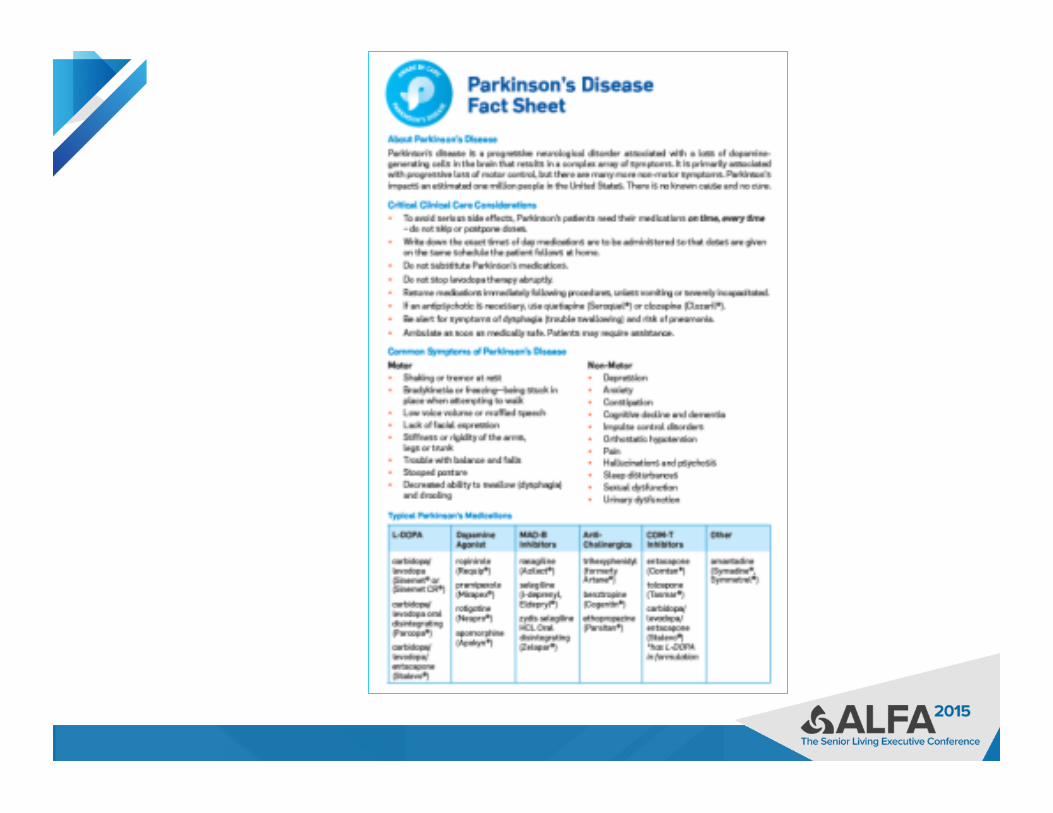
▶ Parkinson’s disease (PD) is a chronic progressive neurological disorder caused by loss of dopamine producing cells in the brain – Gradual onset, not everyone has all the features
▶ Multiple causes/precipitants – Rarely genetic, rarely clearly environmental
▶ Predictable course, within reason ▶ Rate of progression and symptoms variable
from person to person ▶ No cure (yet), but symptoms are treatable
What is Parkinson’s disease?
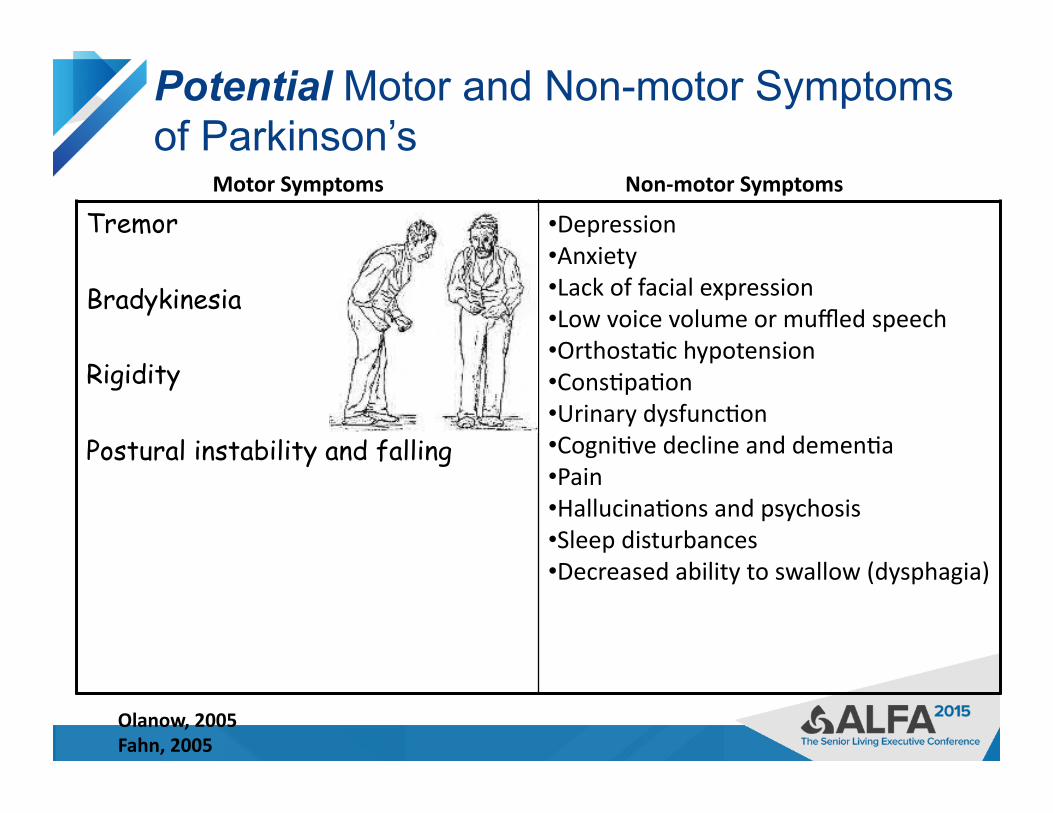
Potential Motor and Non-motor Symptoms of Parkinson’s
Tremor
Bradykinesia
Rigidity
Postural instability and falling
• Depression • Anxiety • Lack of facial expression • Low voice volume or muffled speech • Orthosta<c hypotension • Cons<pa<on • Urinary dysfunc<on • Cogni<ve decline and demen<a • Pain • Hallucina<ons and psychosis • Sleep disturbances • Decreased ability to swallow (dysphagia)
Motor Symptoms Non-‐motor Symptoms
Olanow, 2005 Fahn, 2005
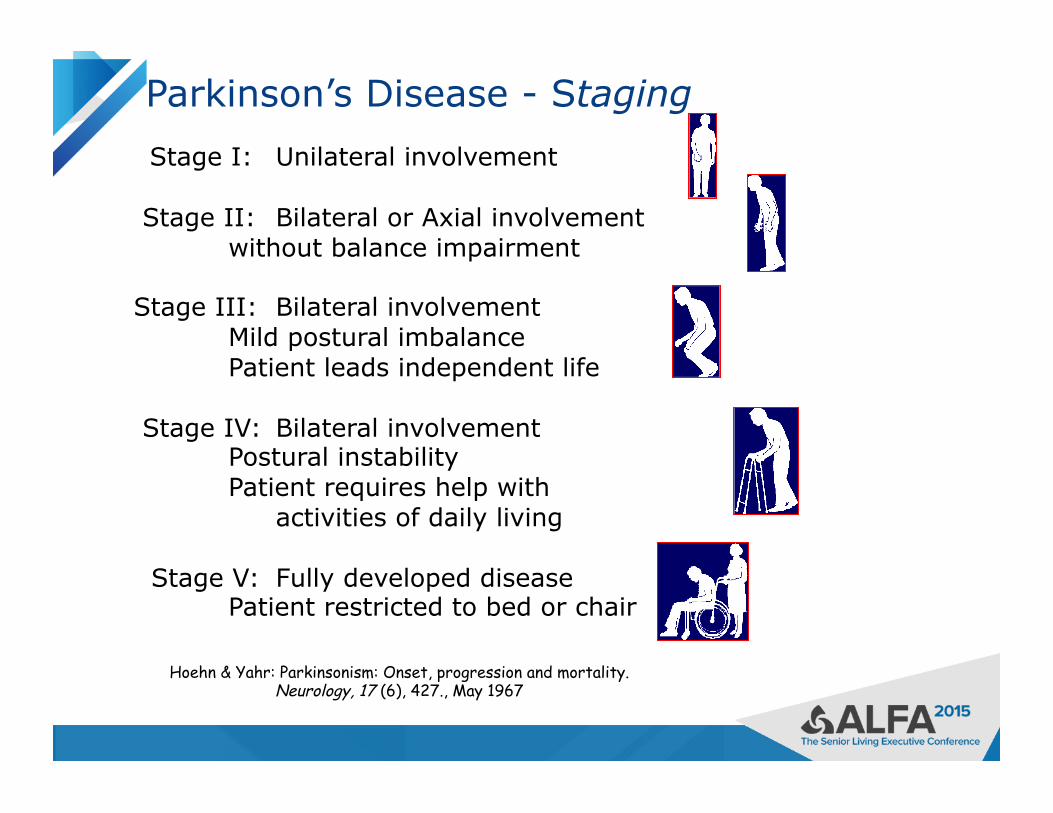
Hoehn & Yahr: Parkinsonism: Onset, progression and mortality. Neurology, 17 (6), 427., May 1967
Parkinson’s Disease - Staging
Stage I: Unilateral involvement
Stage II: Bilateral or Axial involvement without balance impairment
Stage III: Bilateral involvement Mild postural imbalance Patient leads independent life
Stage IV: Bilateral involvement Postural instability Patient requires help with activities of daily living
Stage V: Fully developed disease Patient restricted to bed or chair

Treatment Options
▶ Medication
▶ Surgery
▶ Rehabilitation therapies
▶ Complementary therapies
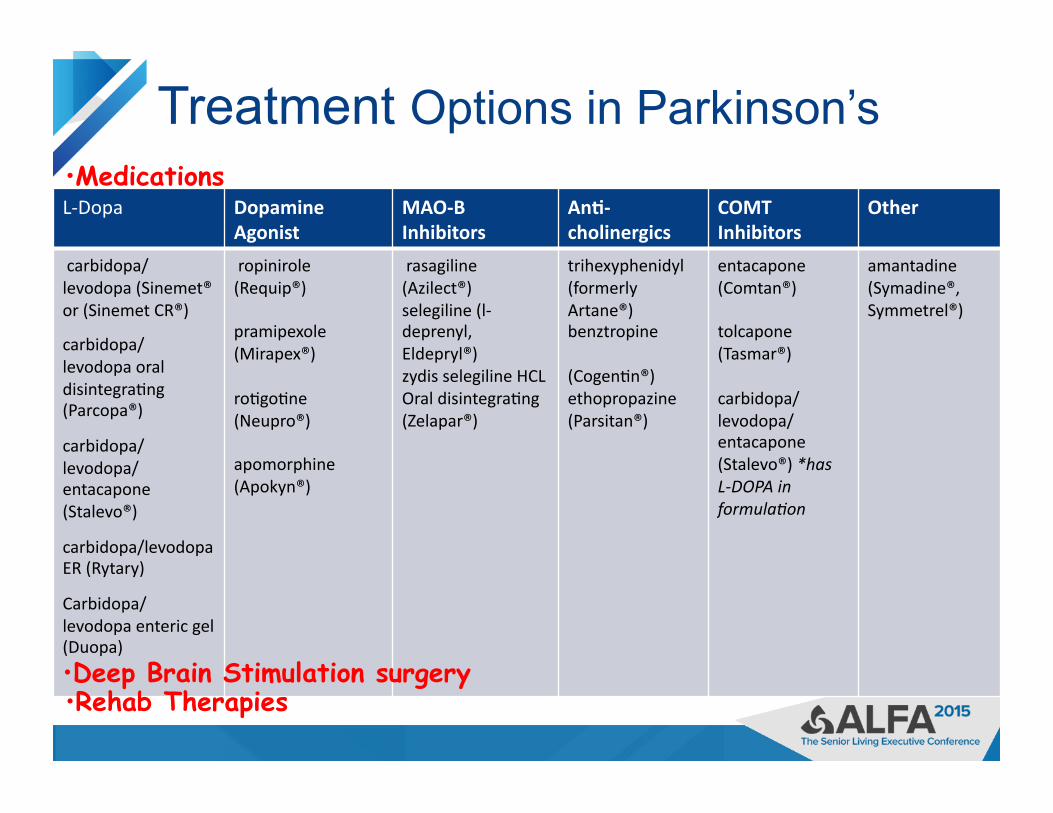
Treatment Options in Parkinson’s
▶
L-‐Dopa Dopamine Agonist
MAO-‐B Inhibitors
An@-‐cholinergics
COMT Inhibitors
Other
carbidopa/ levodopa (Sinemet® or (Sinemet CR®)
carbidopa/ levodopa oral disintegra<ng (Parcopa®)
carbidopa/ levodopa/ entacapone (Stalevo®)
carbidopa/levodopa ER (Rytary)
Carbidopa/levodopa enteric gel (Duopa)
ropinirole (Requip®)
pramipexole (Mirapex®)
ro<go<ne (Neupro®)
apomorphine (Apokyn®)
rasagiline (Azilect®) selegiline (l-‐deprenyl, Eldepryl®) zydis selegiline HCL Oral disintegra<ng (Zelapar®)
trihexyphenidyl (formerly Artane®) benztropine
(Cogen<n®) ethopropazine (Parsitan®)
entacapone (Comtan®)
tolcapone (Tasmar®)
carbidopa/ levodopa/ entacapone (Stalevo®) *has L-‐DOPA in formula4on
amantadine (Symadine®, Symmetrel®)
• Deep Brain Stimulation surgery
• Medications
• Rehab Therapies
Medication Management of Parkinson’s Disease
Goal of medication treatment is to:
• Increase dopamine levels in the brain
• Improve symptoms of Parkinson’s
• Minimize medication side effects
Carbidopa/Levodopa
▶ By mid-late stage PD, almost all with PD are taking some form of carbidopa/levodopa
▶ Levodopa converts to dopamine in the brain ▶ Carbidopa is a buffer for nausea ▶ Available in
– immediate release formulation – immediate release orally disintegrating tablet – controlled or long acting formulation – New capsule of IR and CR “beads” in a 1:4 ratio – New levodopa gel delivered through an intestinal
infusion pump
Protein and Levodopa
▶ Potential for interference of dietary protein with absorption of levodopa – Would notice a decrease or lack of levodopa
effectiveness when taken too close to a protein meal
▶ A major issue for some
▶ For best effectiveness, take levodopa – 30-60 minutes before you eat – 2 hours after
Difficult to achieve with frequent levodopa dosing

Medication Management in Parkinson’s:
▶ Each medication is scheduled when it is expected to provide the best control of symptoms – Medication schedules vary from person to person – May be simple of complex based on symptoms and stage
of disease ▶ As Parkinson’s symptoms progress, and medication
effectiveness changes, medications need to be adjusted over time.
▶ Medications need to be taken frequently through the day and sometimes at night
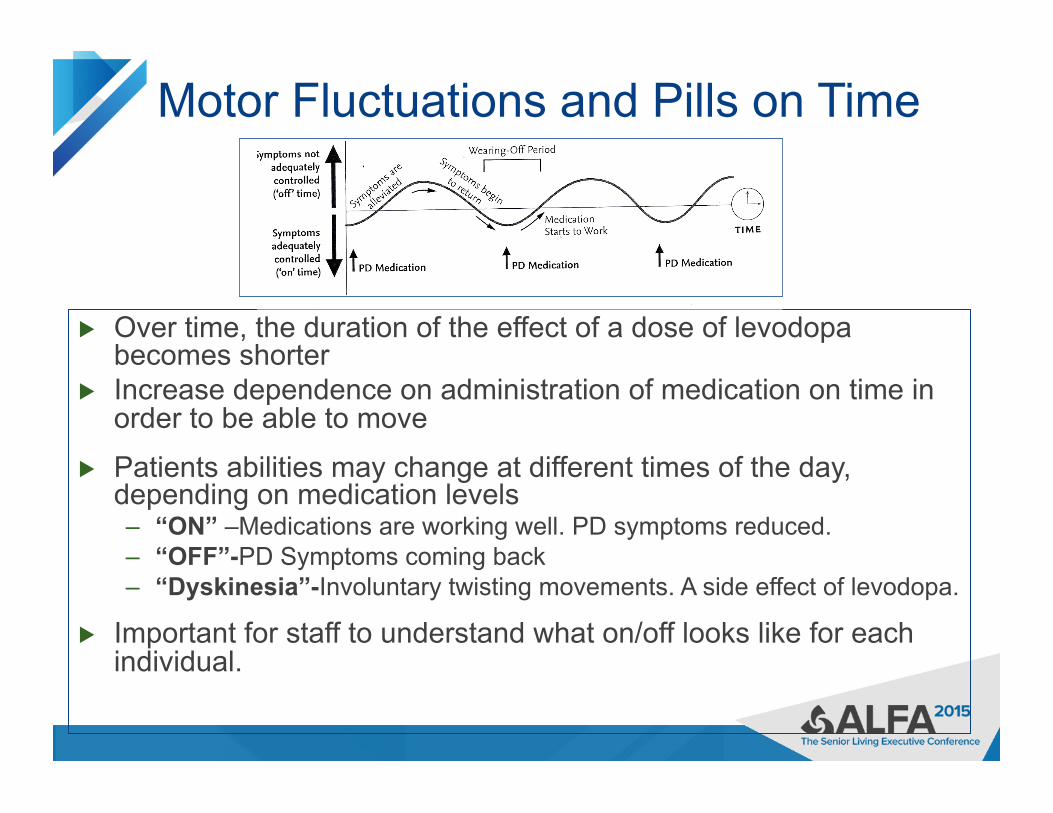
Motor Fluctuations and Pills on Time
▶ Over time, the duration of the effect of a dose of levodopa becomes shorter
▶ Increase dependence on administration of medication on time in order to be able to move
▶ Patients abilities may change at different times of the day, depending on medication levels – “ON” –Medications are working well. PD symptoms reduced. – “OFF”-PD Symptoms coming back – “Dyskinesia”-Involuntary twisting movements. A side effect of levodopa.
▶ Important for staff to understand what on/off looks like for each individual.
Care Considerations
▶ If PD patients are “OFF”. . . – At risk for falls because of impaired mobility – Trouble with fine motor skills, such as eating, toileting – Slowness in movement and thinking – Delayed response to questions – Need more assistance from staff
▶ If PD patients are “ON”. . . – Less rigidity, tremor, slowness – Better mobility – Improved thinking and response to questions

Often misconstrued as stubborn, manipulative, or attention-seeking behavior
Fluctuations On Off
Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

Medication Management in Parkinson’s: The importance of pills on time
– Important for optimal functioning. Pills taken according to a schedule to help stay ahead of symptoms
– If medications are taken late, PD symptoms may be more difficult to control
• For some, 15 minutes late may cause symptoms to increase • May have an entire “bad” or “off” day if medications are late
– May lead to social isolation as they are afraid of being “off” in public
Pills on Time Everytime
▶ Nurses have a window for administering medications as a compromise for busy nursing staff who care for multiple patients
▶ As a result, PD residents will receive their medications at seemingly random times
▶ Standard policy for “on time” administration of pills 1 hour before or after prescribed time does not work well for individuals with PD.
▶ Need intentional process for keeping pills on time ▶ Need awareness and plan for pill doses if resident is
away from their room

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

Contraindicated Medications for PD Medical Purpose Safe Medica@ons Medica@ons to Avoid
An@psycho@cs que<apine (Seroquel®), clozapine (Clozaril®). These drugs minimally affect Parkinson symptoms.
avoid all other typical and atypical an<-‐psycho<cs, such as haloperidol (Haldol®)
Pain Medica@on most are safe to use, but narco<c medica<ons may cause confusion/ psychosis and cons<pa<on
if pa<ent is taking MAOB inhibitor such as selegiline or rasagiline (Azilect®), avoid meperidine (Demerol®)
Nausea/ GI Drugs domperidone (Mo<lium®), trimethobenzamide (Tigan®), ondansetron (Zofran®), dolasetron (Anzemet®), granisetron (Kytril®)
prochlormethazine (Compazine®), metoclopramide (Reglan®), promethazine (Phenergan®), droperidol (Inapsine®), as they can worsen Parkinson symptoms
Surgery for Parkinson’s: Deep Brain Stimulation (DBS)
▶ Not an initial therapy, but may be an option when medications do not adequately control the symptoms
▶ Reduces tremor, slowness, rigidity, dystonia, and dyskinesia on the opposite side of the body
▶ Does not help with balance, falls, memory, or non-motor symptoms
▶ Not a cure ▶ Does not stop disease progression ▶ Well-tolerated and can be done on both
sides of the brain
▶ Physical Stressors
▶ a cold or flu ▶ illness ▶ infection ▶ surgery ▶ injury
▶ Emotional Stressors
▶ anxiety ▶ worry ▶ feeling rushed ▶ feeling angry or
upset
Stress has a negative impact on all symptoms of Parkinson’s disease

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
▶ Levodopa – almost all patients respond ▶ Converts to dopamine in the brain
– Immediate release carbidopa-levodopa • 10/100, 25/100, 25/250
– Controlled (extended) release carbidopa-levodopa • 25/100, 50/200
– Oral dissolving • Parcopa 10/100, 25/100, 25/250
– With entacapone • Stalevo 50, 75, 100, 125, 150, 200
– Extended release capsules (combination levodopa formulation “beads”)
• Rytary 23.75/95, 36.25/145, 48.75/195, 61.25/245 – Enteral gel suspension delivered through PEG-J tube
• Duopa – 2000 mg cartridges
Levodopa – most effective treatment – cannot substitute one formulation for another

Care Transitions into the care setting
At intake, it is Important to ask the patient/family the schedule and dosing interval (time between doses) for PD medications
• For dosing intervals, typical bid, tid, qid medication schedules are not typical for a person with Parkinson's • When entering medications into the electronic or paper record, specify PD med times to help ensure accurate schedules
• With the patient/family, verify exact dosages and formulations (immediate release, controlled release, etc).
• Double check with medication bottles if possible
• Communicate this schedule to those who will be caring for the patient • Patient may need a dose of PD meds before meds are received from the pharmacy
• is there a way to accommodate this?

Care Transitions from the hospital • Check the discharge summary or ask the pa<ent/family about medica<on changes made in the hospital.
• If medica<ons or schedules were changed during hospitaliza<on a follow-‐up with the Neurologist is recommended
Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
Care considerations Observing for PD Med Side Effects
• Balance medication effects and side effects
• Dose-limiting side effects: • Nausea • Dyskinesia • Hallucinations • Orthostatic hypotension

Considerations for Care
▶ Take into consideration the time the last dose of levodopa was taken when considering cares, therapies and procedures. Allow for medications to “kick in”.
▶ If medications have to be crushed and administered through a tube, give them at least one hour prior to meals
▶ Dissolvable form of levodopa may be useful in some patients with swallowing difficulties
▶ Narcotics, muscle relaxants, bladder, sleep and pain medications can increase the risk of confusion, hallucinations or delirium
Other Potential Care Concerns – to be addressed in adapting your residence for PD
▶ Assisting mobility – Addressing the environment for falls reduction
▶ Understanding mood changes ▶ Cognitive changes ▶ Coping with sleep changes ▶ Pain control ▶ Other
– Constipation – Bladder changes – Skin changes