people with parkinson's need you to be aware in care
DESCRIPTION
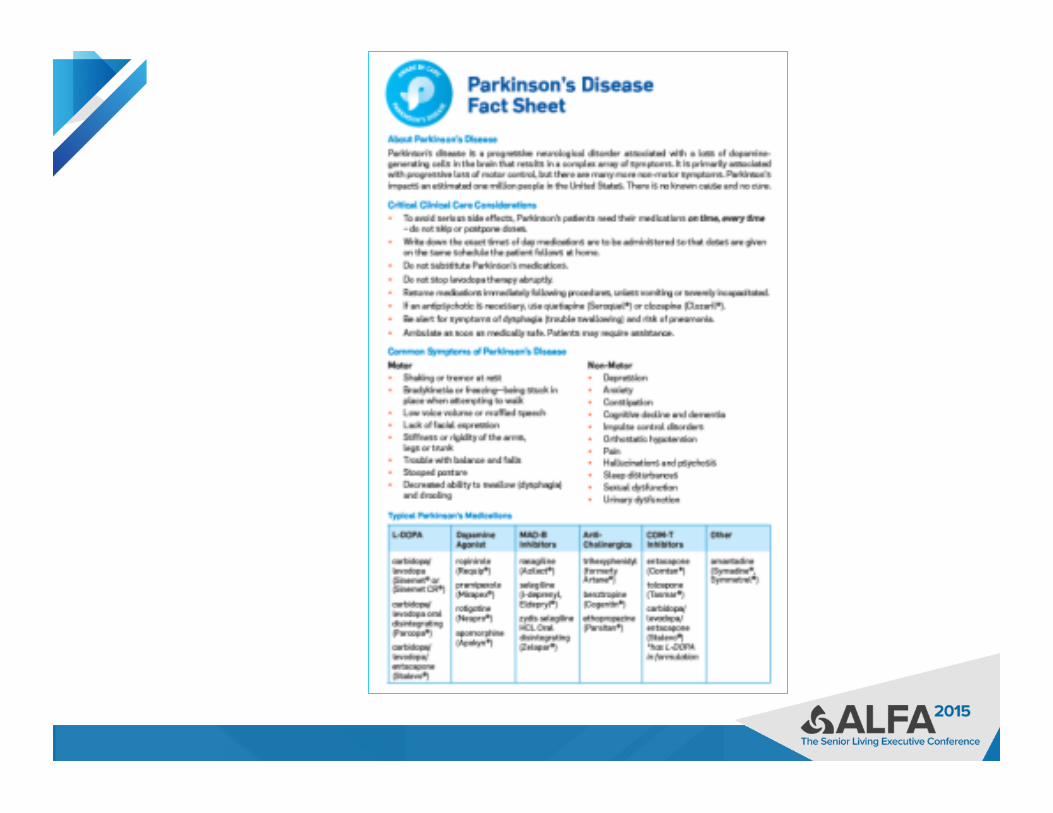
National Parkinson Foundation-funded research has shown that transition into a new care setting poses unique challenges for people living with Parkinson’s disease (PD), particularly when it comes to getting pills on time. The standard rule of “one hour before and after” does not work in PD; the worsening of symptoms can happen quickly, leading to frustrating and sometimes painful “off time.” Learn what your staff needs to know regarding medication management in Parkinson’s to avoid complications in care. Joan Gardner, RN, BSN, Clinic Supervisor, Struthers Parkinson's CenterTRANSCRIPT

People with Parkinson’s Need You to Be Aware in Care Joan Gardner RN BSN Nurse Clinician, Clinic Supervisor Struthers Parkinson’s Center Minneapolis, MN
A National Parkinson Foundation Center of Excellence
Parkinson’s Disease Care in the Assisted Living Care Setting
▶ The launch of the National Parkinson Foundation (NPF) Aware in Care Program has helped raise awareness of the unique care needs of the hospitalized patient with Parkinson’s disease (PD) – Lack of understanding regarding
medication management in PD – Lack of understanding of contraindicated
medications for those with PD ▶ Information learned from the hospital
Aware in Care program can be transferred to care gaps in the Assisted Living care setting
The Aware in Care toolkit ▶ Helps patients and families advocate for themselves
– Understand the risks associated with hospital stays – Be prepared in case you have to go to the hospital—whether
planned or unplanned – Develop strategies to get better care in the hospital
▶ Draws attention to the high rate of complications when PD pills are not given on time
• 3 out of 4 people with Parkinson’s disease do not receive medications on time in the hospital
• 61% of patients who did not get their medications on time had serious complications from it

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
Parkinson's Disease in the Assisted Living Setting
▶ Nursing staff and direct care staff may not have much experience with PD residents
▶ Staffing shortages and/or staffing cuts - little time to invest in education
▶ If education occurs, usually is focused on the nursing staff, not on direct care staff
▶ Any knowledge taught is lost with frequent staff turnover
Importance of Care Staff to be Aware in Care
▶ Incidence of PD is expected to double by 2030 – Increasing longevity of Americans with better
management of chronic conditions of middle-age such as diabetes, hypertension, high cholesterol, etc.
▶ Many with Parkinson’s will need to leave their home due to need of hands-on care as PD symptoms progress

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

▶ Parkinson’s disease (PD) is a chronic progressive neurological disorder caused by loss of dopamine producing cells in the brain – Gradual onset, not everyone has all the features
▶ Multiple causes/precipitants – Rarely genetic, rarely clearly environmental
▶ Predictable course, within reason ▶ Rate of progression and symptoms variable
from person to person ▶ No cure (yet), but symptoms are treatable
What is Parkinson’s disease?
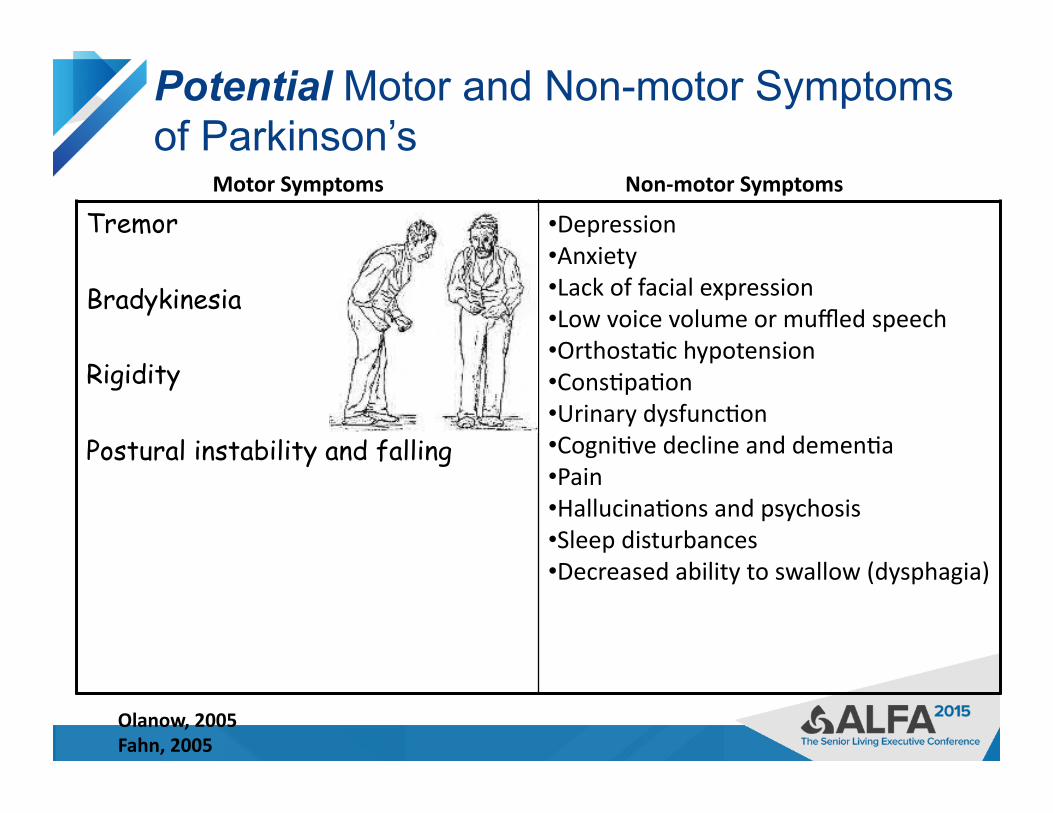
Potential Motor and Non-motor Symptoms of Parkinson’s
Tremor
Bradykinesia
Rigidity
Postural instability and falling
• Depression • Anxiety • Lack of facial expression • Low voice volume or muffled speech • Orthosta<c hypotension • Cons<pa<on • Urinary dysfunc<on • Cogni<ve decline and demen<a • Pain • Hallucina<ons and psychosis • Sleep disturbances • Decreased ability to swallow (dysphagia)
Motor Symptoms Non-‐motor Symptoms
Olanow, 2005 Fahn, 2005
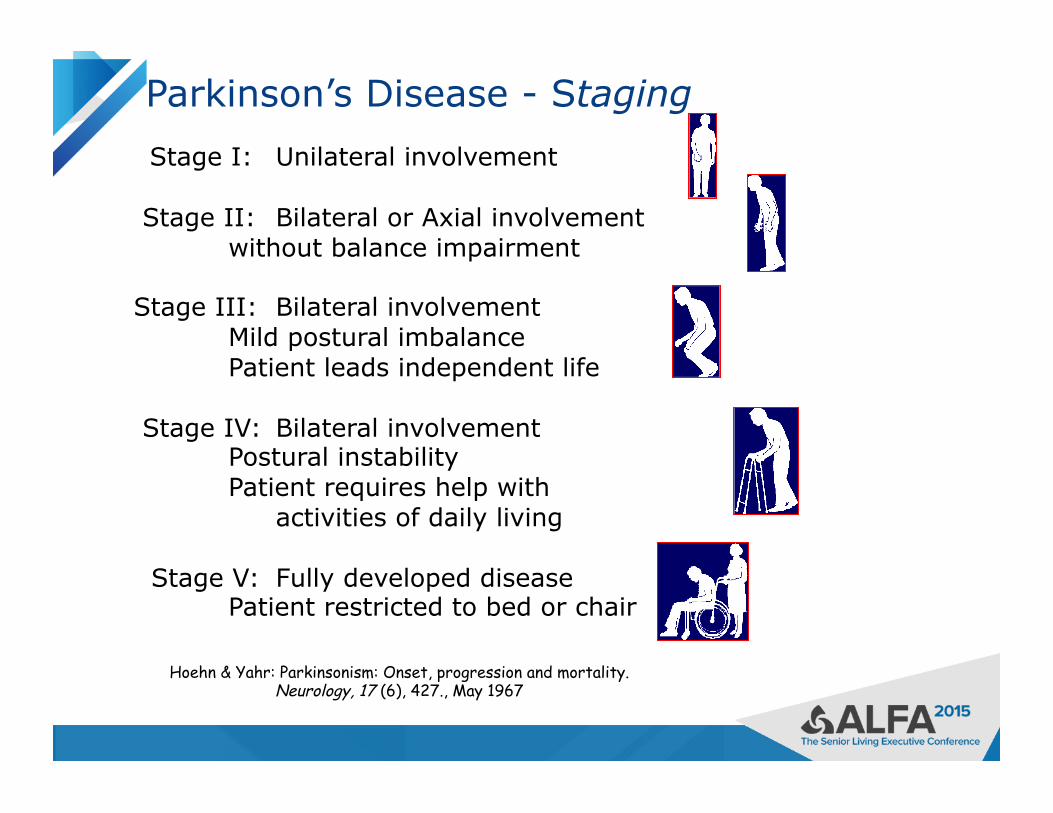
Hoehn & Yahr: Parkinsonism: Onset, progression and mortality. Neurology, 17 (6), 427., May 1967
Parkinson’s Disease - Staging
Stage I: Unilateral involvement
Stage II: Bilateral or Axial involvement without balance impairment
Stage III: Bilateral involvement Mild postural imbalance Patient leads independent life
Stage IV: Bilateral involvement Postural instability Patient requires help with activities of daily living
Stage V: Fully developed disease Patient restricted to bed or chair

Treatment Options
▶ Medication
▶ Surgery
▶ Rehabilitation therapies
▶ Complementary therapies
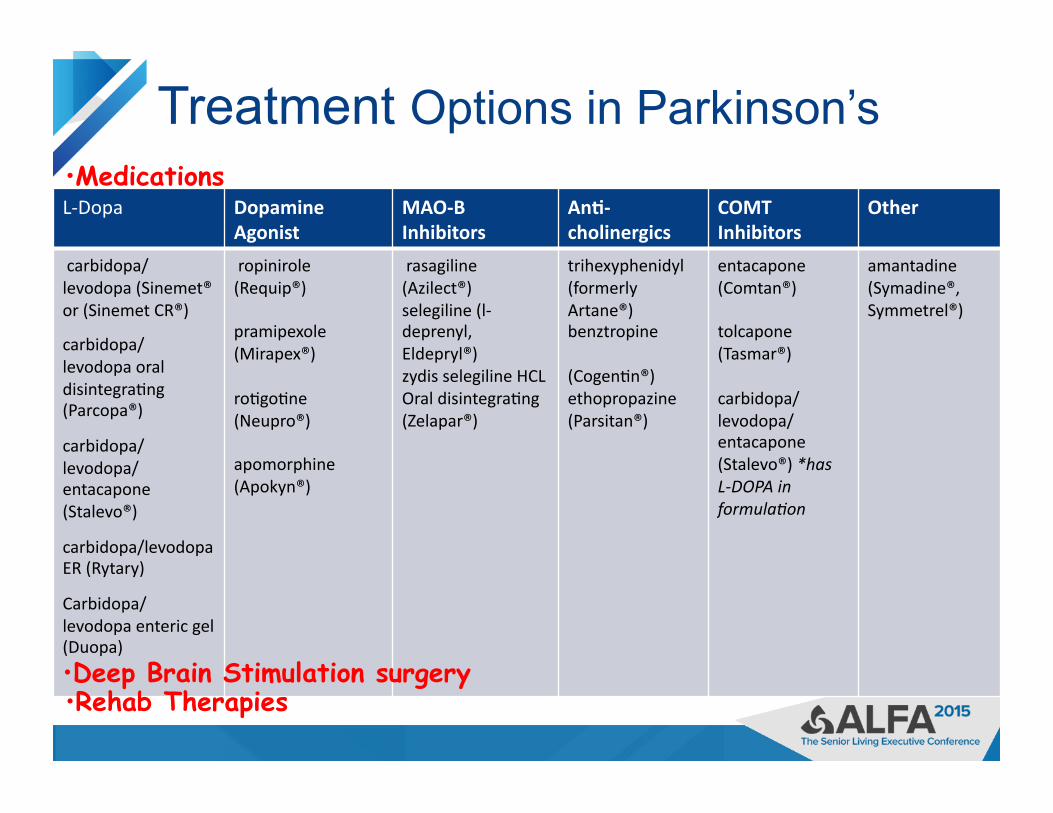
Treatment Options in Parkinson’s
▶
L-‐Dopa Dopamine Agonist
MAO-‐B Inhibitors
An@-‐cholinergics
COMT Inhibitors
Other
carbidopa/ levodopa (Sinemet® or (Sinemet CR®)
carbidopa/ levodopa oral disintegra<ng (Parcopa®)
carbidopa/ levodopa/ entacapone (Stalevo®)
carbidopa/levodopa ER (Rytary)
Carbidopa/levodopa enteric gel (Duopa)
ropinirole (Requip®)
pramipexole (Mirapex®)
ro<go<ne (Neupro®)
apomorphine (Apokyn®)
rasagiline (Azilect®) selegiline (l-‐deprenyl, Eldepryl®) zydis selegiline HCL Oral disintegra<ng (Zelapar®)
trihexyphenidyl (formerly Artane®) benztropine
(Cogen<n®) ethopropazine (Parsitan®)
entacapone (Comtan®)
tolcapone (Tasmar®)
carbidopa/ levodopa/ entacapone (Stalevo®) *has L-‐DOPA in formula4on
amantadine (Symadine®, Symmetrel®)
• Deep Brain Stimulation surgery
• Medications
• Rehab Therapies
Medication Management of Parkinson’s Disease
Goal of medication treatment is to:
• Increase dopamine levels in the brain
• Improve symptoms of Parkinson’s
• Minimize medication side effects
Carbidopa/Levodopa
▶ By mid-late stage PD, almost all with PD are taking some form of carbidopa/levodopa
▶ Levodopa converts to dopamine in the brain ▶ Carbidopa is a buffer for nausea ▶ Available in
– immediate release formulation – immediate release orally disintegrating tablet – controlled or long acting formulation – New capsule of IR and CR “beads” in a 1:4 ratio – New levodopa gel delivered through an intestinal
infusion pump
Protein and Levodopa
▶ Potential for interference of dietary protein with absorption of levodopa – Would notice a decrease or lack of levodopa
effectiveness when taken too close to a protein meal
▶ A major issue for some
▶ For best effectiveness, take levodopa – 30-60 minutes before you eat – 2 hours after
Difficult to achieve with frequent levodopa dosing

Medication Management in Parkinson’s:
▶ Each medication is scheduled when it is expected to provide the best control of symptoms – Medication schedules vary from person to person – May be simple of complex based on symptoms and stage
of disease ▶ As Parkinson’s symptoms progress, and medication
effectiveness changes, medications need to be adjusted over time.
▶ Medications need to be taken frequently through the day and sometimes at night
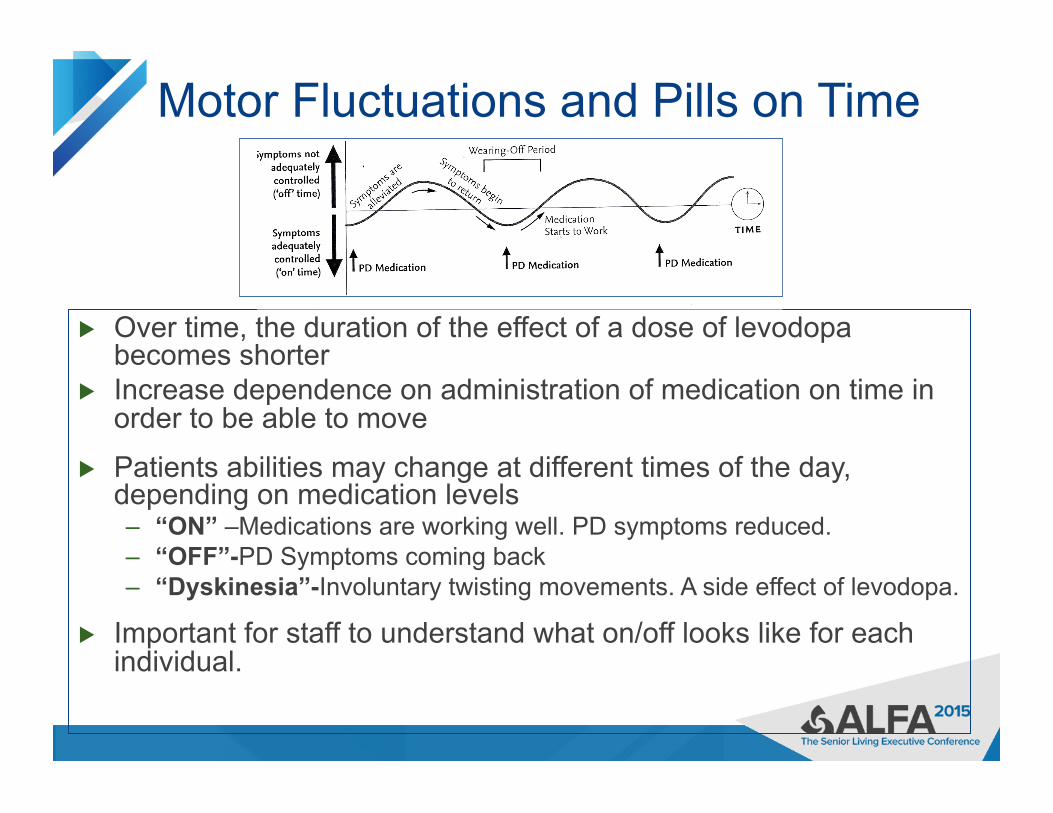
Motor Fluctuations and Pills on Time
▶ Over time, the duration of the effect of a dose of levodopa becomes shorter
▶ Increase dependence on administration of medication on time in order to be able to move
▶ Patients abilities may change at different times of the day, depending on medication levels – “ON” –Medications are working well. PD symptoms reduced. – “OFF”-PD Symptoms coming back – “Dyskinesia”-Involuntary twisting movements. A side effect of levodopa.
▶ Important for staff to understand what on/off looks like for each individual.
Care Considerations
▶ If PD patients are “OFF”. . . – At risk for falls because of impaired mobility – Trouble with fine motor skills, such as eating, toileting – Slowness in movement and thinking – Delayed response to questions – Need more assistance from staff
▶ If PD patients are “ON”. . . – Less rigidity, tremor, slowness – Better mobility – Improved thinking and response to questions

Often misconstrued as stubborn, manipulative, or attention-seeking behavior
Fluctuations On Off
Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

Medication Management in Parkinson’s: The importance of pills on time
– Important for optimal functioning. Pills taken according to a schedule to help stay ahead of symptoms
– If medications are taken late, PD symptoms may be more difficult to control
• For some, 15 minutes late may cause symptoms to increase • May have an entire “bad” or “off” day if medications are late
– May lead to social isolation as they are afraid of being “off” in public
Pills on Time Everytime
▶ Nurses have a window for administering medications as a compromise for busy nursing staff who care for multiple patients
▶ As a result, PD residents will receive their medications at seemingly random times
▶ Standard policy for “on time” administration of pills 1 hour before or after prescribed time does not work well for individuals with PD.
▶ Need intentional process for keeping pills on time ▶ Need awareness and plan for pill doses if resident is
away from their room

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms

Contraindicated Medications for PD Medical Purpose Safe Medica@ons Medica@ons to Avoid
An@psycho@cs que<apine (Seroquel®), clozapine (Clozaril®). These drugs minimally affect Parkinson symptoms.
avoid all other typical and atypical an<-‐psycho<cs, such as haloperidol (Haldol®)
Pain Medica@on most are safe to use, but narco<c medica<ons may cause confusion/ psychosis and cons<pa<on
if pa<ent is taking MAOB inhibitor such as selegiline or rasagiline (Azilect®), avoid meperidine (Demerol®)
Nausea/ GI Drugs domperidone (Mo<lium®), trimethobenzamide (Tigan®), ondansetron (Zofran®), dolasetron (Anzemet®), granisetron (Kytril®)
prochlormethazine (Compazine®), metoclopramide (Reglan®), promethazine (Phenergan®), droperidol (Inapsine®), as they can worsen Parkinson symptoms
Surgery for Parkinson’s: Deep Brain Stimulation (DBS)
▶ Not an initial therapy, but may be an option when medications do not adequately control the symptoms
▶ Reduces tremor, slowness, rigidity, dystonia, and dyskinesia on the opposite side of the body
▶ Does not help with balance, falls, memory, or non-motor symptoms
▶ Not a cure ▶ Does not stop disease progression ▶ Well-tolerated and can be done on both
sides of the brain
▶ Physical Stressors
▶ a cold or flu ▶ illness ▶ infection ▶ surgery ▶ injury
▶ Emotional Stressors
▶ anxiety ▶ worry ▶ feeling rushed ▶ feeling angry or
upset
Stress has a negative impact on all symptoms of Parkinson’s disease

Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
▶ Levodopa – almost all patients respond ▶ Converts to dopamine in the brain
– Immediate release carbidopa-levodopa • 10/100, 25/100, 25/250
– Controlled (extended) release carbidopa-levodopa • 25/100, 50/200
– Oral dissolving • Parcopa 10/100, 25/100, 25/250
– With entacapone • Stalevo 50, 75, 100, 125, 150, 200
– Extended release capsules (combination levodopa formulation “beads”)
• Rytary 23.75/95, 36.25/145, 48.75/195, 61.25/245 – Enteral gel suspension delivered through PEG-J tube
• Duopa – 2000 mg cartridges
Levodopa – most effective treatment – cannot substitute one formulation for another

Care Transitions into the care setting
At intake, it is Important to ask the patient/family the schedule and dosing interval (time between doses) for PD medications
• For dosing intervals, typical bid, tid, qid medication schedules are not typical for a person with Parkinson's • When entering medications into the electronic or paper record, specify PD med times to help ensure accurate schedules
• With the patient/family, verify exact dosages and formulations (immediate release, controlled release, etc).
• Double check with medication bottles if possible
• Communicate this schedule to those who will be caring for the patient • Patient may need a dose of PD meds before meds are received from the pharmacy
• is there a way to accommodate this?

Care Transitions from the hospital • Check the discharge summary or ask the pa<ent/family about medica<on changes made in the hospital.
• If medica<ons or schedules were changed during hospitaliza<on a follow-‐up with the Neurologist is recommended
Primary Problems of PD Care Management
▶ Lack of understanding of Parkinson’s disease – symptoms, treatment, etc.
▶ Lack of awareness about the critical importance of Parkinson’s medication timing
▶ Lack of awareness that many common medications for pain, nausea, depression, and psychosis are unsafe for people with Parkinson’s
▶ Hospital pharmacies that do not stock the full array of PD medications
▶ Lack of awareness that poorly-managed PD might result in mental confusion and other serious symptoms
Care considerations Observing for PD Med Side Effects
• Balance medication effects and side effects
• Dose-limiting side effects: • Nausea • Dyskinesia • Hallucinations • Orthostatic hypotension

Considerations for Care
▶ Take into consideration the time the last dose of levodopa was taken when considering cares, therapies and procedures. Allow for medications to “kick in”.
▶ If medications have to be crushed and administered through a tube, give them at least one hour prior to meals
▶ Dissolvable form of levodopa may be useful in some patients with swallowing difficulties
▶ Narcotics, muscle relaxants, bladder, sleep and pain medications can increase the risk of confusion, hallucinations or delirium
Other Potential Care Concerns – to be addressed in adapting your residence for PD
▶ Assisting mobility – Addressing the environment for falls reduction
▶ Understanding mood changes ▶ Cognitive changes ▶ Coping with sleep changes ▶ Pain control ▶ Other
– Constipation – Bladder changes – Skin changes