dr. arun agrawal md, mnams, fiap, fiams, miuat (paris), ficmch
DESCRIPTION
Approach to Floppy Infant. Dr. Arun Agrawal MD, MNAMS, FIAP, FIAMS, MIUAT (Paris), FICMCH Consultant Pediatrician & Neonatologist, Ghaziabad National Chairperson – Neurology Chapter of IAP Honorary Professor of Pediatrics ICMCH - PowerPoint PPT PresentationTRANSCRIPT

Neurology Chapter of IAP
Dr. Arun AgrawalMD, MNAMS, FIAP, FIAMS, MIUAT (Paris), FICMCH
• Consultant Pediatrician & Neonatologist, Ghaziabad• National Chairperson – Neurology Chapter of IAP • Honorary Professor of Pediatrics ICMCH • National Convener – Community Pediatrics, Chapter of IAP • National Vice President IAP 2004
Approach to
Floppy Infant

Neurology Chapter of IAP
Floppy Infant
Floppy infant refers to those children
presenting with generalized hypotonia, most
often arising out of an insult incurred during
fetal or neonatal period.
Neurology Chapter of IAP

Neurology Chapter of IAP
Posture
The floppy infant assumes a frog legged position. On ventral suspension, the baby can not maintain limb posture against gravity and assumes the position of a rag doll.

Neurology Chapter of IAP

Neurology Chapter of IAP
Movements
The muscles appear flabby. There is diminished resistance to passive movement of the limbs and the range of movement of the peripheral joints is increased.

Neurology Chapter of IAP
Scarf Sign
Put the child in a supine position and hold one of the infant’s hands. Try to put it around the neck as far as possible around the opposite shoulder. Observe how far the elbow goes across the body. In a floppy infant, the elbow easily crosses the midline.
Pull to sit:When pulled up from the supine to the sitting position, the head of the baby lags.

Neurology Chapter of IAP

Neurology Chapter of IAP
Causes of Floppy Infant Syndrome1. Central nervous system
Perinatal asphyxia, neonatal, encephalopathy, kernicterus, cerebral palsy (atonic type), intracranial hemorrhage, chromosomal anomalies including down syndrome and inborn errors of metabolism e.g., aminocidurias, mucopolysaccharidosis and cerebral lipidosis.
2. Spinal cord lesionsAnterior horn cell disease – werdnig Hoffman spinal muscular atrophy, poliomyelitis.
3. Peripheral nervousAcute polyneuropathy, familial dysautonomia, congenital sensory neuropathy.
4. Myoneural junctionNeonatal myasthenia gravis, infantile botulism, following antibiotic therapy.

Neurology Chapter of IAP
Causes of Floppy Infant Syndrome (Contd.)
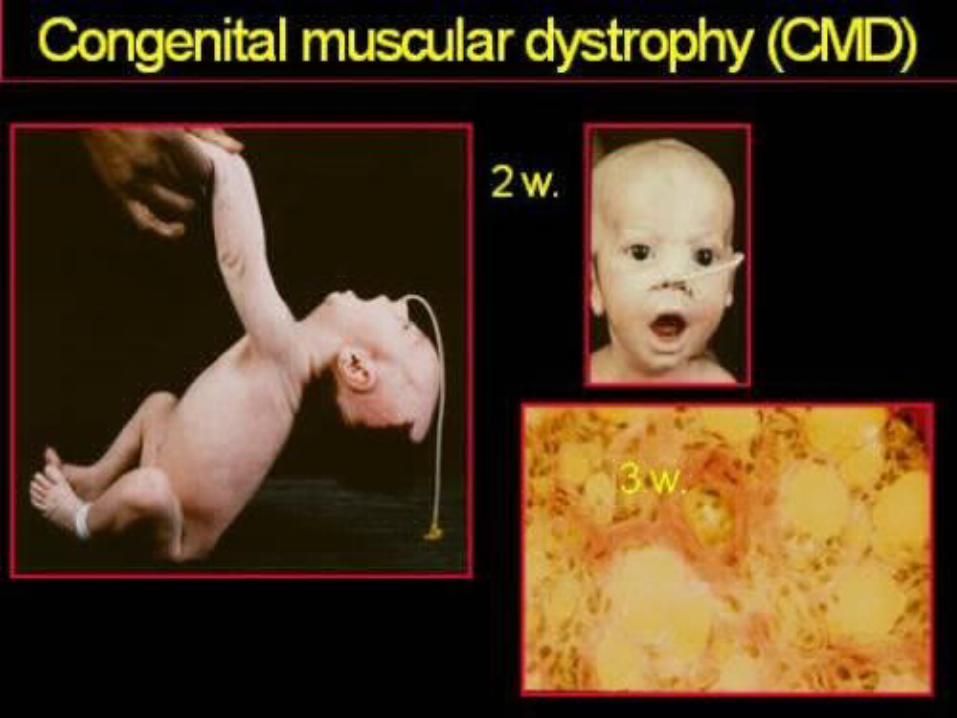
5. Muscles Muscular dystrophies, congenital myotonic dystrophies, congenital myopathies (including central core disease and nemalin myopathy), polymyositis, glycogen storage disease (pompe’s), and arthrogryposis multiplex congenital.
6. Miscellaneous Protein energy malnutrition, rickets, prader willi syndrome, malabsorption syndromes, Ehler-Danlos syndrome, cutis laxa, cretinism.

Neurology Chapter of IAP

Neurology Chapter of IAP
Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP
Differentiating Features of a Floppy Infant according to Site of Involvement
Site of involvement Extent of weakness
Proximal vs. distal weakness Face Arms Legs
Central - + + > or =
Anterior horn cell + ++++ ++++ > or =
Peripheral nerve - +++ +++ <
Neuromuscular junction
+++ +++ +++ =
Muscle Variable ++ + >

Neurology Chapter of IAP
Differentiating Features of a Floppy Infant according to Site of Involvement (Contd.)
Site of involvement Deep tendon
reflexes EMG Muscle biopsy
Central Normal or increased
Normal Normal
Anterior horn cell Absent Fasciculation / fibrillation
Denervation pattern
Peripheral nerve Decreased Fibrillation Denervation pattern
Neuromuscular junction
Normal Decremental / incremental
Normal
Muscle Decreased Short duration small amplitude potential
Characteristic

Neurology Chapter of IAP
• Signs: Perform complete physical examination • Infant with decreased muscle tone • Exam distinguishes site of disorder
– Upper motor neuron lesion – Lower motor neuron lesion
• Radiology • Head CT • Head MRI • Diagnostic Studies • Electromyogram (EMG) • Nerve Conduction Studies • Labs: Initial • Serum electrolytes • Serum Calcium • Serum Glucose
Look for
Sepsis

Neurology Chapter of IAP
• Creatine Phosphokinase (CPK) • Toxic scan• Blood Culture • Lumbar Puncture with Cerebrospinal Fluid Examination • Thyroid Function Tests • Labs: Test as indicated • Toxicology screen • Serum Ammonia and Venous pH
– Serum amino acids – Urine amino acids and organic acid
• Karyotype • TORCH Virus Screening
LooksLike
Sepsis without Sepsis

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP
Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP
Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP

Neurology Chapter of IAP
Common causes of floppy infant
Cerebral PalsyMany hypotonic children due to causes in central nervous system are mentally retarded. In atonic or hypotonic cerebral palsy, reflexes are brisk in spite of generalized flaccidity. Floppy infant due to cerebral causes is associated with lethargy, poor feeding, and lack of alertness, poor Moro’s reflex, and seizures during the neonatal period.

Neurology Chapter of IAP
Werdnig Hoffman diseaseIt is characterized by marked hypotonia, sluggish fetal movement, and fasciculation of tongue. The child is alert. Feeding behaviour and cry are poor. Deep tendon reflexes are absent. Muscle biopsy shows neurogenic type of atrophy or that the muscle spindles are atrophied in groups. Disease is inherited as an autosomal may be available. Death occurs by 2-4 years of age.

Neurology Chapter of IAP
Myasthenia gravisMmyasthenia gravis may occur in about 12 percent of the babies born to mothers with the disease. It is characterized by marked hypotonia, pooling of oral secretions, poor feeding, feeble cry and generalized muscle weakness appearing within 2-3 days after the birth. Baby is alert. Facial weakness manifests by mark-like facies, open mouth and staring look. External opthalmoplegia and ptosis are rare. Deep tendon reflexes are normal. The prognosis is substantiated by improvement in the muscle functions following intramuscular injection of edrophonium chloride 1 mg or neostigmine methyl sulfate 0.1 mg. the condition lasts for 3 to 4 weeks. The child is treated with neostigmine methyl sulphate 0.1 to 0.5 mg IM 10 minutes before each feel for 1 or 2 days followed by neostigmine bromide, 1 to 4 mg orally half an hour before each feed.

Neurology Chapter of IAP
Congenital myopathies
These are rare inherited disorders resulting in a benign congenital hypotonia, with generally good outlook for normal life span. Nemaline myopathy is the most common variant. Other disorders of this group include the central core disease, myotubular myopathy and congenital fiber type disproportion.

Neurology Chapter of IAP
OthersIn polyneuritis there is symmetrical weakness of the limbs with sensory changes. The diagnosis of Pompe’s disease is suspected when the child has macroglossia, cardiomegaly and generalized hypotonia. Babies with prader-willi syndrome are mentally retarded and obese; deep tendon reflexes are diminished. Diabetes mellitus occurs later in life. Testes may be undescended. Ehlers-danlos syndrome is characterized by hyperelasticity of the skin, hyperflexibility of joints and extreme, fragility of skin. Wound healing is delayed and there are frelly movable subcutaneous nodules. In cutis laxa, the child has loose skin hanging in baggy folds.
Neurology Chapter of IAP
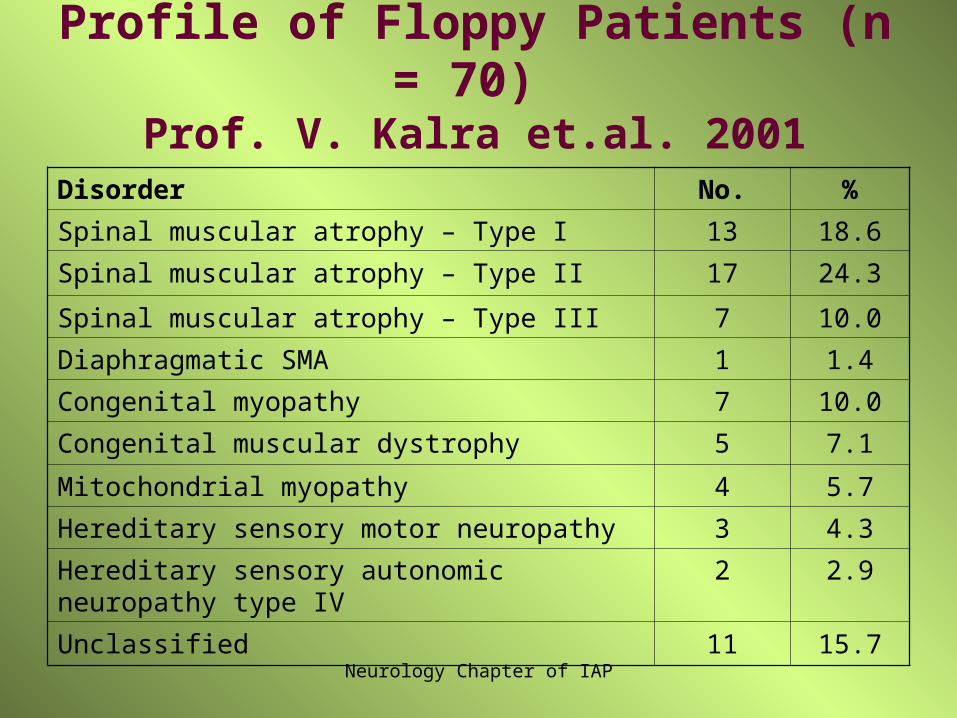
Profile of Floppy Patients (n = 70) Prof. V. Kalra et.al. 2001
Disorder No. %Spinal muscular atrophy – Type I 13 18.6Spinal muscular atrophy – Type II 17 24.3
Spinal muscular atrophy – Type III 7 10.0Diaphragmatic SMA 1 1.4Congenital myopathy 7 10.0Congenital muscular dystrophy 5 7.1
Mitochondrial myopathy 4 5.7Hereditary sensory motor neuropathy 3 4.3Hereditary sensory autonomic neuropathy type IV 2 2.9
Unclassified 11 15.7

Neurology Chapter of IAP
Key Messages of this Study
• Spinal muscular atrophy emerged as the commonest cause of floppy children followed by congenital muscle disease.
• 11% of the cases still remained unclassified despite sophisticated investigative techniques.
• EMG was a good screening modality for floppy children.
• A low gene deletion rate (50%) was observed in our phenotype
Neurology Chapter of IAP
Key Messages in Approach to a Floppy Child
• First ABC of resuscitation • Try to find out cause but again simple clinical
examination is the first thing• Any sedative drug given during labour • Investigations • Only those investigations which are necessary • Sepsis • Sepsis without sepsis• Another sophisticated investigations• Improve the quality of life probably quantity can not be
improve in most of the cases

Neurology Chapter of IAP