dr carlo tascini direttore prima divisione malattie ... · dr carlo tascini direttore prima...
TRANSCRIPT

Dr Carlo Tascini
Direttore Prima Divisione Malattie
Infettive
Ospedale Cotugno
Napoli

Il sottoscritto Carlo Tasciniai sensi dell’art. 3.3 sul Conflitto di Interessi, pag. 17 del Reg. Applicativo dell’Accordo Stato-Regione del 5 novembre 2009,
dichiara
che negli ultimi due anni ha avuto rapporti diretti di finanziamento con i seguenti soggetti portatori di interessi commerciali in campo sanitario:
- Astra- Merck- Pfizer- Astellas- Angelini- Gilead- Novartis.
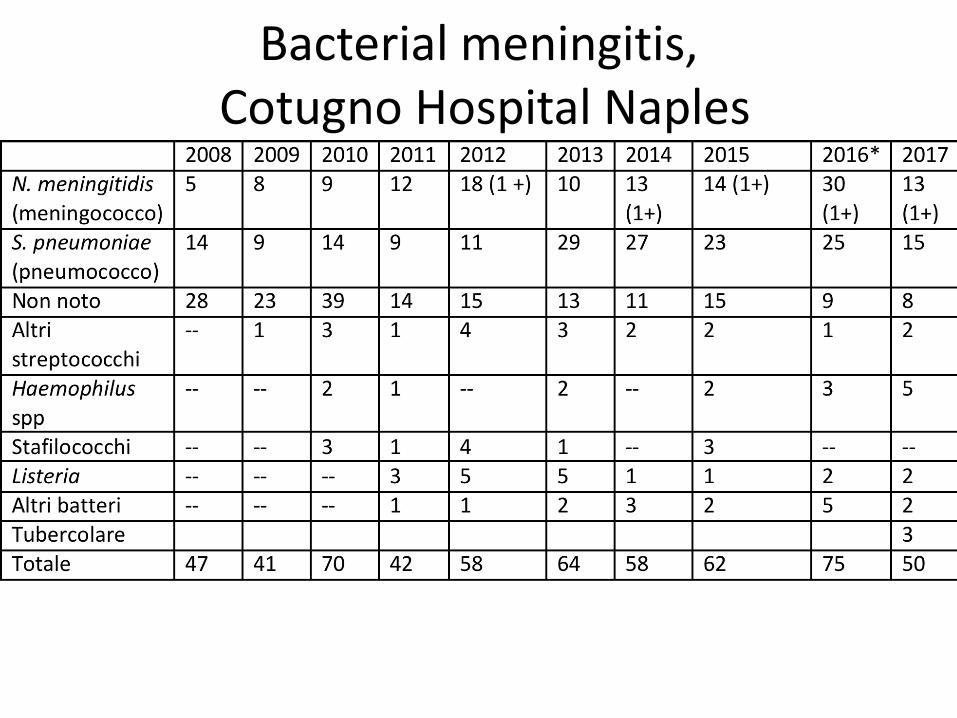
Bacterial meningitis,Cotugno Hospital Naples

Meningococcal Invasive DiseaseCotugno Hospital Naples, Italy

Cortesia prof. Menichetti

Necrosi delle dita da CID
Emergenza medica





Segno Sensibilità Specificità VPP VPN
Rigidità nucale
31% 71% 41% 61%
Kernig 11% 95% 50% 60%
Brudzinski 9% 95% 60% 62%
Brouwer MC: lancet 2012

Adjunctivedexamethasonein adultswithmeningococcal meningitis
Sebastiaan G.B.
Heckenberg, MD*
MatthijsC. Brouwer,
MD, PhD*
Arievan der Ende, PhD
Diederik van deBeek,
MD, PhD
ABSTRACT
Objectives: We evaluated the implementat ion and ef fect iveness of adjunct ive dexamethasone in
adults with meningococcal meningit is.
Methods: We compared 2 Dutch prospect ive nat ionwide cohort studies on community-acquired me-
ningococcal meningit is. A total of 258 pat ients with CSF culture-proven meningit is were enrolled
between 1998 and 2002, before rout ine dexamethasone therapy was introduced, and 100 pat ients
from March 2006 to January 2011, after guidelines recommended dexamethasone.
Results: Dexamethasone was administered in 43 of 258 (17% ) pat ients in the 1998–2002 co-
hort and in 86 of 96 (90% ) pat ients in the 2006–2011 cohort (p 0 .001 ), and was started with
or before the f irst dose of ant ibiot ics in 12 of 258 (5% ) and 85 of 96 (89% ) pat ients (p 0 .001 ).
Rates of unfavorable outcome were similar between cohorts (12 of 100 [12% ] vs 30 of 258
[12% ]; p 0 .67 ), also af ter correct ion for meningococcal serogroup. The rates of hearing loss (3
of 9 6 [3 % ] vs 1 9 of 2 3 7 [8 % ]; p 0 .1 0 ) and death (4 of 1 0 0 [4 % ] vs 1 9 of 2 5 8 [7 % ];
p 0 .24 ) were lower in the 2006–2011 cohort , but this did not reach signif icance. The rate of
arthrit is was lower in pat ients t reated with dexamethasone (32 of 258 [12% ] vs 5 of 96 [5% ], p
0 .046 ). Dexamethasone was not associated with adverse events.
Conclusions: Adjunct ive dexamethasone is widely prescribed for pat ients with meningococcal
meningit is and is not associated with harm. The rate of arthrit is has decreased af ter the imple-
mentat ion of dexamethasone.
Classification of evidence: This study provides Class III evidence that adjuvant dexamethasone in
adults with meningococcal meningit is does not increase negat ive outcomes such as deafness,
death, or negat ive Glasgow Outcome Scale measures. Neurology® 2012 ;79 :1563–1569
GLOSSARY
cc clonal complex; GOS Glasgow Outcome Scale; MLST mult ilocus sequence typing; NRLBM Netherlands Refer-
ence Laboratory for Bacterial Meningit is.
Bacterial meningitis remainsan important cause of morbidity and mortality worldwide, even
though effective antibiotic therapy is available and vaccination strategies have been imple-
mented.1–3 The most common causesare Streptococcuspneumoniaeand Neisseria meningitidis,
accountingfor 85%of casesin adults.1–3Fatality ratesin patientswithmeningitiscaused bythesemicro-
organismsaresignificant, with ratesof 26%and 10%, respectively,1,4,5 andof survivingpatients, 30%to
50%haveneurologicdeficitsincludinghearingloss6andcognitivedeficits.7,8
Several adjunctive therapies have been evaluated in bacterial meningitis.9,10 Randomized
clinical trialshaveevaluated theefficacy of adjunctivecorticosteroid therapy.11,12 A largeEuro-
pean randomized controlled trial in adults showed a beneficial effect of dexamethasone in
*Theseauthorscontributed equally to thiswork.
From theDepartments of Neurology (S.G.B.H., M.C.B., D.v.d.B.), Medical Microbiology (A.v.d.E.), Center of Infection and Immunity Amsterdam
(CINIMA), and TheNetherlands Reference Laboratory for Bacterial Meningitis Academic Medical Center (A.v.d.E.), University of Amsterdam,
Amsterdam; and Department of Neurology (S.G.B.H.), Kennemer Gasthuis, Haarlem, theNetherlands.
Coinvestigators are listed on theNeurology®Web siteat www.neurology.org.
Study funding: Supported by theNetherlands Organization for Health Research and Development (ZonMw NWO-Veni grant 2006 [916.76.023] and
ZonMw NWO-Vidi grant 2010 [917.11.358], both to D.v.d.B.), theAcademic Medical Center (AMC Fellowship 2008 to D.v.d.B.), and European
Research Council (ERC Starting Grant [281156] to D.v.d.B.).
Go to Neurology.org for full disclosures. Disclosures deemed relevant by theauthors, if any, areprovided at theend of thisarticle.
Editorial, page 1528
Supplemental data atwww.neurology.org
Supplemental Data
CME
Correspondence & reprint
requests to Dr. van deBeek:
Copyright © 2 0 1 2 by AAN Enterprises, Inc. 1 5 6 3


IGAM yes IGAM no
35 76

Primo caso meningococco
• Ragazzo di 18 anni, V anno liceo scientifico
• Febbre dolori articolari
• Non rigidità nucale, mai meningite
• Petecchie cutanee in repentino aumento
• UTI
• Steroide, meropenem, linezolid
• Pentaglobin
• Ceftriaxone

Ore 7 Ore 13

Ag su urine

Secondo caso
• 24 anni studente di Fisica
• In coma al pronto soccorso da almeno 4
ore : TAC, neurologo attesa esami
• Ceftriaxone, desametasone, pentaglobin
• UTI


N. meningitidis gruppo Y
• Paziente di 13 anni arriva in coma all’Ospedale Cotugno: rigidità nucale e febbre
• Nessuna petecchia
• Ricovero in UTI: si programma PL
• Arriva anche il fratello di 11 anni: febbre, nessun segno neurologico
• EO: negativo, torace, addome, cuore, non rigidità nucale: non si tolgono le calze

Sepsi meningococcica senza meningite: non trattata 80% mortalità

N. meningitidis gruppo Y
• Dopo due ore, il paziente rientra con numerose petecchie
• Sia lui che il fratello hanno N. meningitidisgruppo Y , lui isolato solo da sangue, il fratello solo da liquor



Vero caso?
• Dopo due giorni dal secondo caso di Pisa
• Arriva al PS paziente di 21 anni con febbre
e cefalea
• Il medico del pronto soccorso chiede se il
paziente riesce a piegare la testa, si nota
che il paziente ha rigidità nucale, non
petecchie
• Il medico chiede se è confuso
• Dopo poco tempo confusione mentale

Vero caso?
• Consulenza infettivologica: paziente rigido confuso, febbrile: sospetta meningite batterica
• Chiesta TAC cranio: non lesioni occupanti spazio
• Richiesta consulenza rianimatoria: si decide di iniziare desametasone e ceftriaxone, ma di stare attenti che potrebbe andare in coma per il rilascio citochinico.

Vero caso?
• Inizia ceftriaxone dopo desametasone. Il
paziente va in coma: glasgow 4 intubato
• PL: liquor limpido: 1 cellula, antigeni
negativi
• Il paziente viene portato in UTI, non ha
nemmeno i riflessi al dolore: isteria?
• Estubato, senza problemi,
• Trasferito in medicina: faringite
streptococcica

Vero caso?
• Crisi catatonica di conversione: può
arrivare al coma
• Nel sub-conscio mimava tutti i sintomi che
venivano descritti dagli operatori del PS

Faringite
• Infermiere della Chirurgia generale
• Musicista in gruppi rock
• Faringite da alcuni giorni: tampone
effettuato alle malattie Infettive ed inviato
dalla chirurgia: risposta N. meningitidis
gruppo C.
• Il paziente viaggia in treno lungo la linea
tirrenica
• Panico in ospedale e sul treno

Faringite da N. meningitidis

Terapia empirica e mirata

TAC prima della puntura lombare
• Una delle cause più frequenti del ritardo della terapia steroidea ed antibiotica

Motivi per effettuare la TAC prima della PL
• Papilledema
• Segni neurologici focali
• Riduzione moderato o grave dello stato di coscienza (tolto dalle LG svedesi)
• Immuno-depressione
• Nuovo esordio di crisi epilettiche (tolte dalle LG svedesi)







Cortisone

Adjunctivedexamethasonein adultswithmeningococcal meningitis
Sebastiaan G.B.
Heckenberg, MD*
MatthijsC. Brouwer,
MD, PhD*
Arievan der Ende, PhD
Diederik van deBeek,
MD, PhD
ABSTRACT
Objectives: We evaluated the implementat ion and ef fect iveness of adjunct ive dexamethasone in
adults with meningococcal meningit is.
Methods: We compared 2 Dutch prospect ive nat ionwide cohort studies on community-acquired me-
ningococcal meningit is. A total of 258 pat ients with CSF culture-proven meningit is were enrolled
between 1998 and 2002, before rout ine dexamethasone therapy was introduced, and 100 pat ients
from March 2006 to January 2011, after guidelines recommended dexamethasone.
Results: Dexamethasone was administered in 43 of 258 (17% ) pat ients in the 1998–2002 co-
hort and in 86 of 96 (90% ) pat ients in the 2006–2011 cohort (p 0 .001 ), and was started with
or before the f irst dose of ant ibiot ics in 12 of 258 (5% ) and 85 of 96 (89% ) pat ients (p 0 .001 ).
Rates of unfavorable outcome were similar between cohorts (12 of 100 [12% ] vs 30 of 258
[12% ]; p 0 .67 ), also af ter correct ion for meningococcal serogroup. The rates of hearing loss (3
of 9 6 [3 % ] vs 1 9 of 2 3 7 [8 % ]; p 0 .1 0 ) and death (4 of 1 0 0 [4 % ] vs 1 9 of 2 5 8 [7 % ];
p 0 .24 ) were lower in the 2006–2011 cohort , but this did not reach signif icance. The rate of
arthrit is was lower in pat ients t reated with dexamethasone (32 of 258 [12% ] vs 5 of 96 [5% ], p
0 .046 ). Dexamethasone was not associated with adverse events.
Conclusions: Adjunct ive dexamethasone is widely prescribed for pat ients with meningococcal
meningit is and is not associated with harm. The rate of arthrit is has decreased af ter the imple-
mentat ion of dexamethasone.
Classification of evidence: This study provides Class III evidence that adjuvant dexamethasone in
adults with meningococcal meningit is does not increase negat ive outcomes such as deafness,
death, or negat ive Glasgow Outcome Scale measures. Neurology® 2012 ;79 :1563–1569
GLOSSARY
cc clonal complex; GOS Glasgow Outcome Scale; MLST mult ilocus sequence typing; NRLBM Netherlands Refer-
ence Laboratory for Bacterial Meningit is.
Bacterial meningitis remainsan important cause of morbidity and mortality worldwide, even
though effective antibiotic therapy is available and vaccination strategies have been imple-
mented.1–3 The most common causesare Streptococcuspneumoniaeand Neisseria meningitidis,
accountingfor 85%of casesin adults.1–3Fatality ratesin patientswithmeningitiscaused bythesemicro-
organismsaresignificant, with ratesof 26%and 10%, respectively,1,4,5 andof survivingpatients, 30%to
50%haveneurologicdeficitsincludinghearingloss6andcognitivedeficits.7,8
Several adjunctive therapies have been evaluated in bacterial meningitis.9,10 Randomized
clinical trialshaveevaluated theefficacy of adjunctivecorticosteroid therapy.11,12 A largeEuro-
pean randomized controlled trial in adults showed a beneficial effect of dexamethasone in
*Theseauthorscontributed equally to thiswork.
From theDepartments of Neurology (S.G.B.H., M.C.B., D.v.d.B.), Medical Microbiology (A.v.d.E.), Center of Infection and Immunity Amsterdam
(CINIMA), and TheNetherlands Reference Laboratory for Bacterial Meningitis Academic Medical Center (A.v.d.E.), University of Amsterdam,
Amsterdam; and Department of Neurology (S.G.B.H.), Kennemer Gasthuis, Haarlem, theNetherlands.
Coinvestigators are listed on theNeurology®Web siteat www.neurology.org.
Study funding: Supported by theNetherlands Organization for Health Research and Development (ZonMw NWO-Veni grant 2006 [916.76.023] and
ZonMw NWO-Vidi grant 2010 [917.11.358], both to D.v.d.B.), theAcademic Medical Center (AMC Fellowship 2008 to D.v.d.B.), and European
Research Council (ERC Starting Grant [281156] to D.v.d.B.).
Go to Neurology.org for full disclosures. Disclosures deemed relevant by theauthors, if any, areprovided at theend of thisarticle.
Editorial, page 1528
Supplemental data atwww.neurology.org
Supplemental Data
CME
Correspondence & reprint
requests to Dr. van deBeek:
Copyright © 2 0 1 2 by AAN Enterprises, Inc. 1 5 6 3



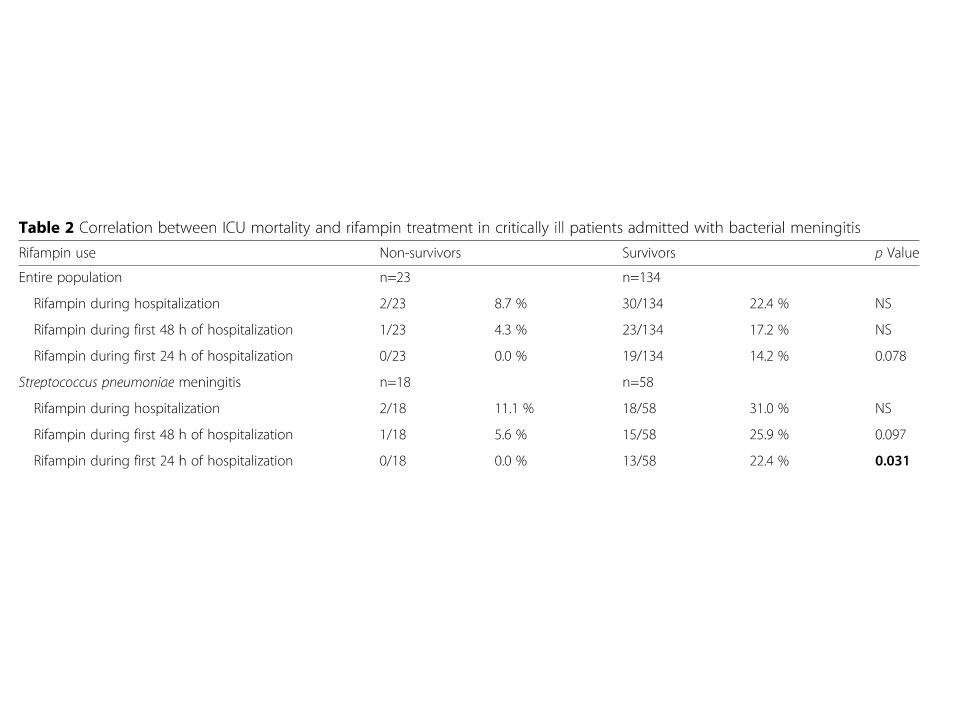
Rifampicina

PAI-1 activation by LPS

LPS attiva PAI-1


Immunity
• SBA: protective≥ 1:4
• Meningococcal vescicles and blebs are full
of antigens that might be able to reduce the
bactericidal activity of serum (false target)

Membrana esterna




Glicerolo


• Terapia colistina 2 mg/Kg + IGAM 5ml/Kg ogni 12 ore, (0,25mg/Kg/die), per 2 gg
• Sopravvivenza 8/11 (72%) contro 6/21 (28%) controli storici


Intensive Care Med
LETTER
Dear Editor,
Despite timely and appropriate treatment, invasive
meningococcal disease (IMD) may be associated with
high mortality and permanent sequelae [1, 2]. Severe
meningococcal infections are able to impair the innate
immune defence for effective phagocytosis of bacte-
ria [3]. IgM adjuvant therapy seems to be a promising
strategy for the control of severe N. meningitidis infec-
tions because they neutralize bacterial endotoxins and
exotoxins and enhance opsonisation and phagocytosis
of evading pathogens [4]. e only available polyclonal
preparation enriched with IgM immunoglobulins is
Pentaglobin® (Biotest-AG, Dreieich, Germany), which
contains 76% IgG, 12% IgA and 12% IgM, and showed
in vitro killing of gram-negative bacilli through enhance-
ment of phagocytosis [5].
In order to evaluate the role of IgM-enriched immu-
noglobulins (Ig-GAM) as adjuvant treatment in reduc-
ing death and permanent sequelae we retrospectively
reviewed 111 cases of documented IMD that occurred in
Italy, in the Tuscany region (53 cases) and the Naples area
(58 cases), from October 2013 to December 2016. Mate-
rials and methods are described in Supplementary Elec-
tronic Material. All patients were treated with adequate
antibiotic and supportive therapy and either with (35
patients) or without (76 patients) Ig-GAM. More patients
cared for without Ig-GAM were in the Tuscany region,
had increased age, meningitis alone and serogroup C N.
meningitidis (see Supplementary Table 1).
Death was documented in 3% of patients receiving Ig-
GAM (1/35) and in 16% (12/76) of those not treated with
Ig-GAM adjuvant therapy. Severe complications causing
permanent sequelae were registered in 6% of patients
receiving Ig-GAM (2/35 had amputation of the extremi-
ties) and in 12% (11/76) of those not receiving Ig-GAM
(5/11 amputation of the extremities and 6/11 hearing
loss). Overall, death or permanent sequelae were docu-
mented in 9% of patients cared for with Ig-GAM (3/35)
and in 30% of those treated without (23/76), a statistically
significant difference (p = 0.023). No episode of AKI, sec-
ondary to Ig-GAM therapy were reported.
Kaplan–Meier analysis of aggregated censored events
(deaths and permanent sequelae) showed a statistically
significant difference favouring patients treated with Ig-
GAM (p = 0.006) (Fig. 1).
e causal effect of Ig-GAM on death and permanent
sequelae, assessed with the propensity score “doubly
robust” approach, appeared to be protective and signifi-
cant (OR = 0.832 95% CI OR = 0.726–0953; p = 0.009)
(see Supplementary Tables 2–5). e use of steroid ther-
apy was similar in treated and control patients (Supple-
mentary Table 1), and, per multivariate analysis, was not
a predictor for death or permanent sequelae (Supplemen-
tary Table 2).
With the multivariate penalized logistic regres-
sion model, the risk factors were purpura fulminans
Author's personal copy

IGAM yes IGAM no
35 76


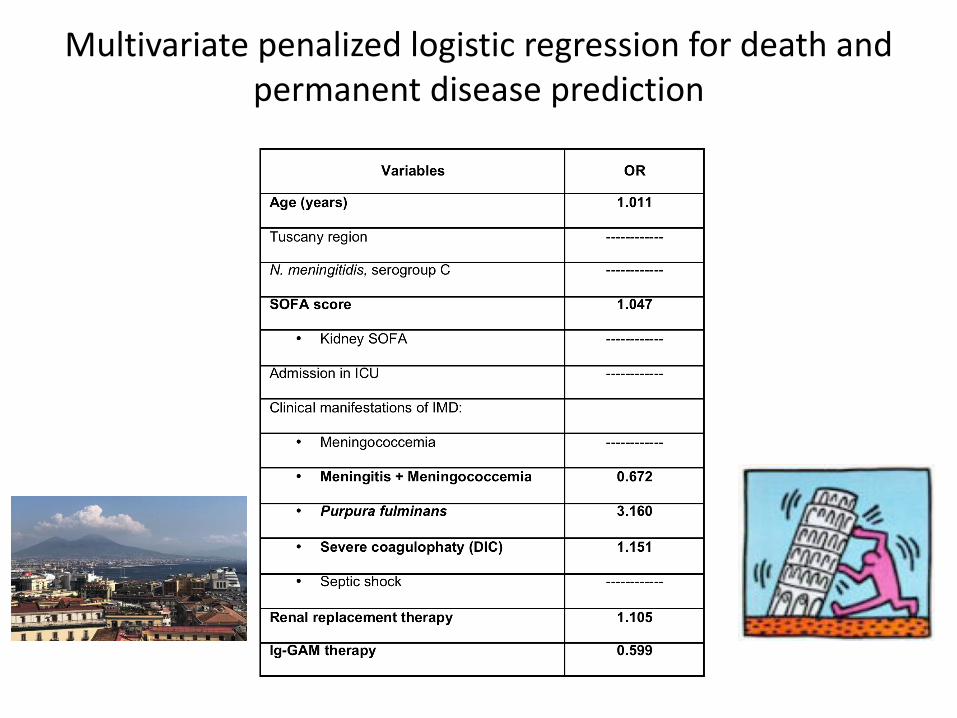
Multivariate penalized logistic regression for death and permanent disease prediction

progetto
MENINGITALYMeningiti batteriche e malattie invasive ad esse correlate:
caratteristiche epidemiologiche, cliniche ed approcci
terapeutici
Studio osservazionale, prospettico, multicentrico
Raccolta di dati clinici, epidemiologici, microbiologici e terapeutici mediante scheda
informatizzata (Google Moduli) di casi di meningite batterica (non tubercolare) e malattie
invasive ad esse correlate
Obiettivo: creazione di un registro nazionale prospettico
Centri partecipanti al momento: 1) Prima Divisione, Malattie Infettive ad indirizzo
neurologico, Osp. Cotugno, AORN dei Colli, Napoli; 2) Clinica delle Malattie Infettive, AOU
di Perugia; 3) Clinica delle Malattie Infettive, AO di Terni
Carlo [email protected]
Prima Divisione, Osp. Cotugno, AORN dei Colli
Carlo [email protected]
Prima Divisione, Osp. Cotugno, AORN dei Colli; Sez. Malattie Infettive, Dip. Medicina,
Università di Perugia

Conclusioni
• La diagnosi clinica di IMD può essere molto sfumata: al minimo sospetto procedere con la PL (TAC?)
• La porpora fulminante deve essere riconosciuta: emocolture (test molecolare su sangue, campione per ISS)
• Desametasone
• Rifampicina
• Ceftriaxone
• IGAM
• Aderite a meningitaly
