dr kerstin wyssusek - royal brisbane hospital - implementing a waste segregation & recycling...
TRANSCRIPT
Implementing a Waste Segregation
and Recycling Initiative
8th Operating Theatre Management Conference
Dr Kerstin Wyssusek
Background
• Operating rooms produce up to 30% of the total daily
hospital waste [1]
• Around 80% of clinical hospital waste could be disposed of
as general waste [2]
• Of the general OT waste approximately 70% is potentially
recyclable [3-7]
• No waste segregation or recycling existent in central OT
complex at tertiary hospital
• 7 to 1 cost difference between clinical waste and general
waste disposal
Aim
• To introduce waste segregation and recycling to the
Operating Theatre complex at a tertiary hospital
• reduce the amount of clinical waste
• reduce cost for disposing of waste
• reduce the carbon footprint
Assessment of motivation to
separate waste
negative
• No chance to start this
• Not interested
• That’s not how we do it
• We will get a fine
• We will be reprimanded
• It doesn’t work here
positive
• That’s what we do at home
• It’s good for the
environment
• We shouldn’t be paying so
much
• It is done in other hospitals
• We need a leader
Methods
1. Establishing baseline by measuring over a 4-week period the amount of waste produced by OTs.
2. Basic waste segregation by collecting clinical waste and general waste in separate containers as per hospital waste management guidelines and measuring it over a 4-week period [9].
3. Refined waste segregation by collecting recyclable cardboard, Kimguard® and hard, clean plastics in separate containers and measuring it over a 4-week period.
4. Categorised determination of waste weight and corresponding disposal costs.
From 21 operating theatres at central OT complex of 780 bed tertiary hospital with 22,000 surgeries/year.
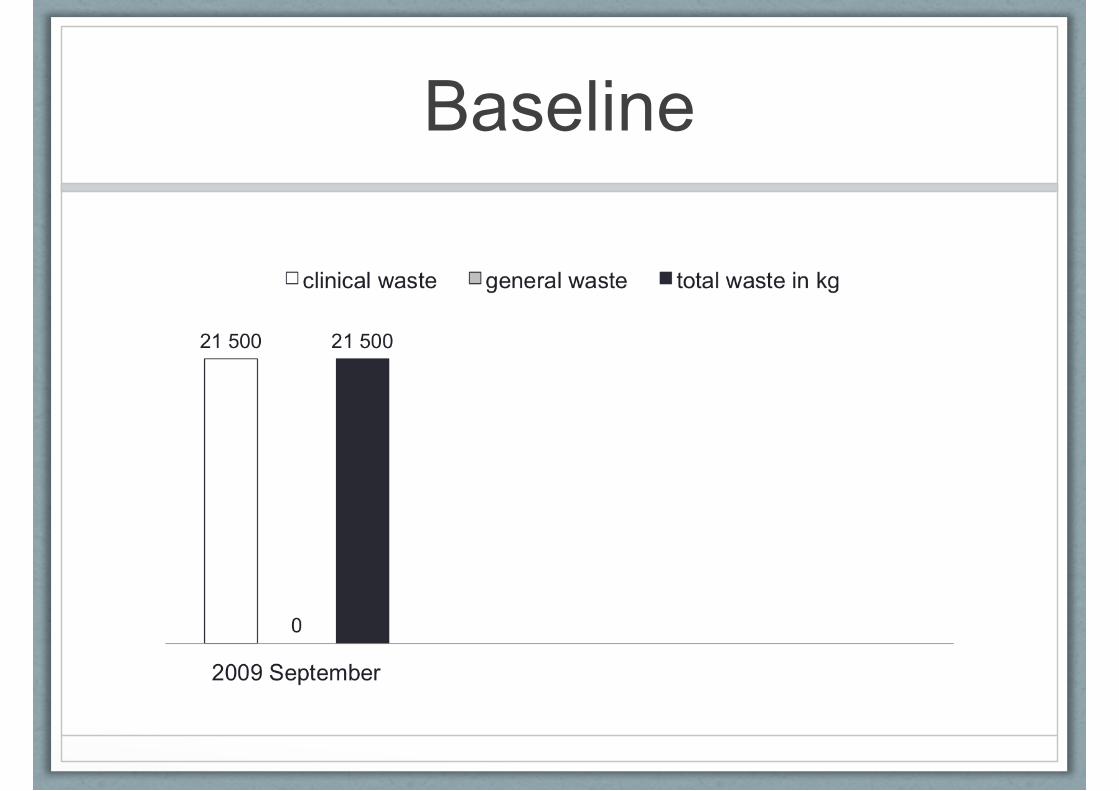
Baseline
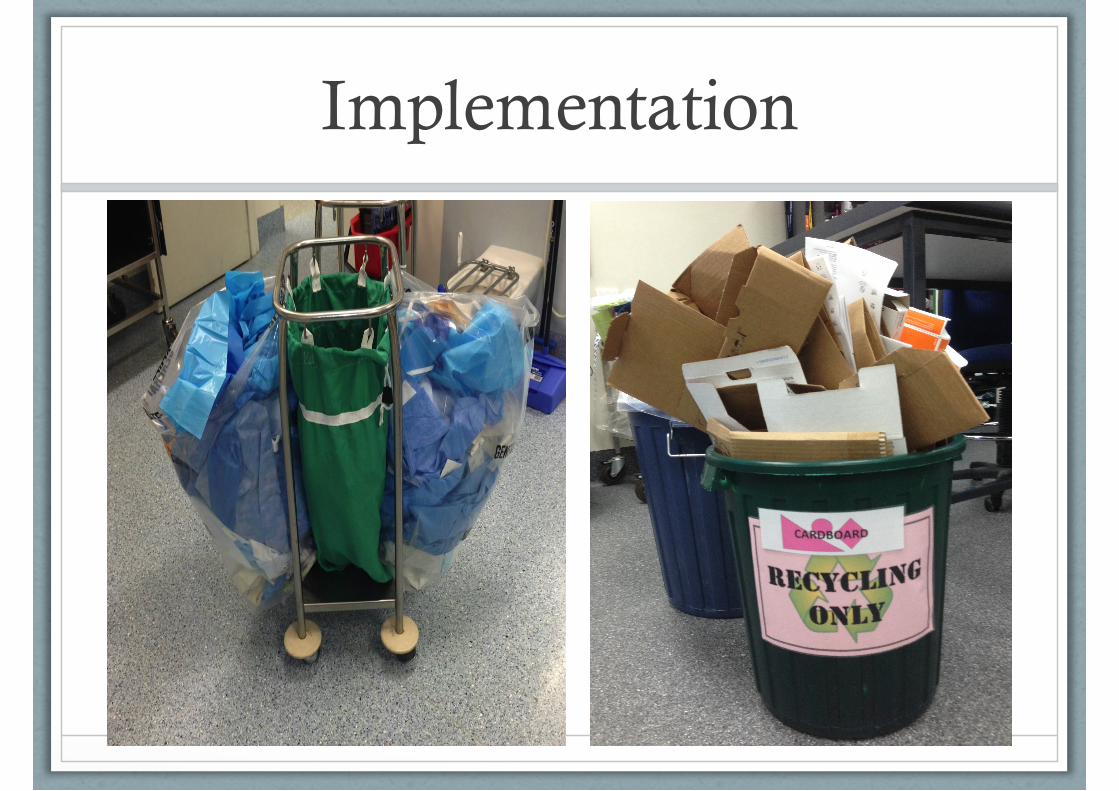
Implementation
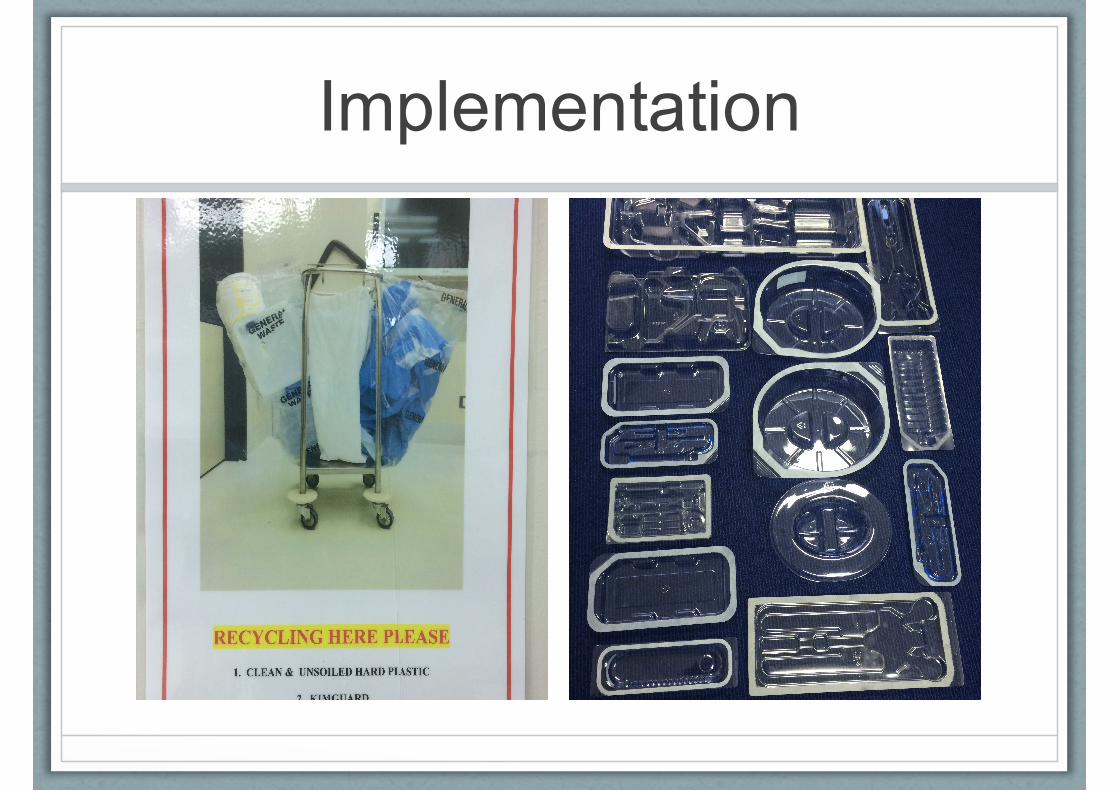
Implementation
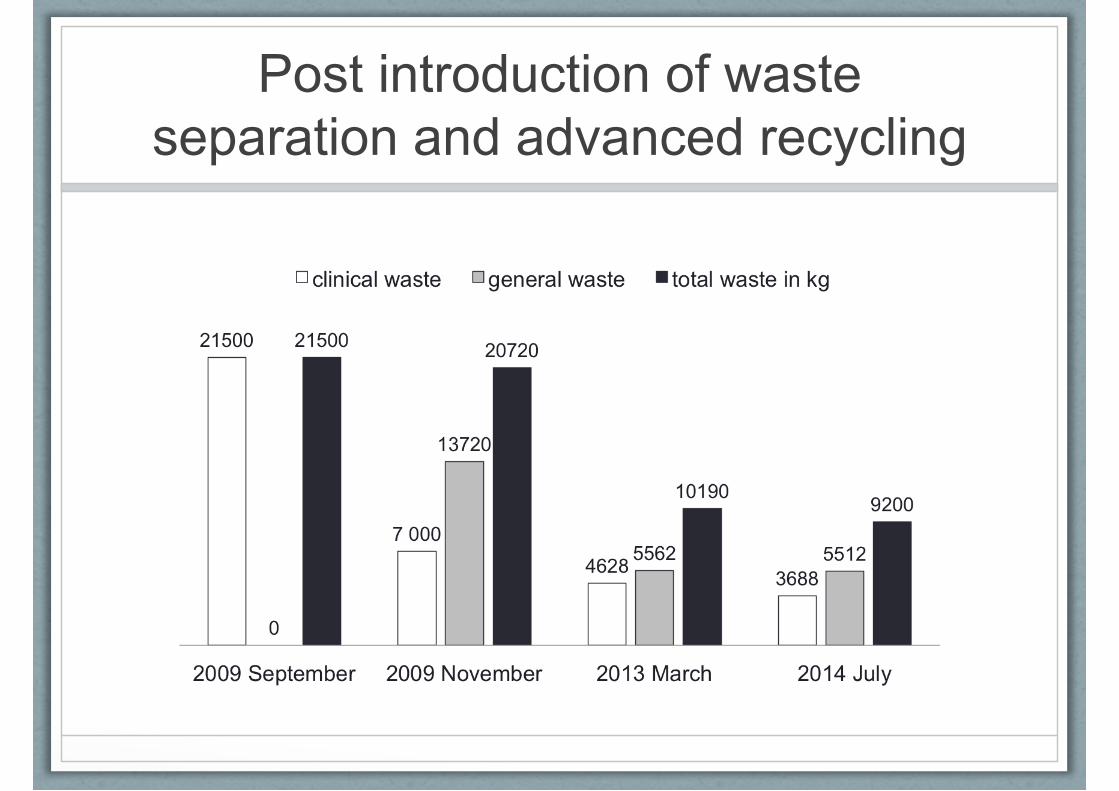
Post introduction of waste
separation and advanced recycling
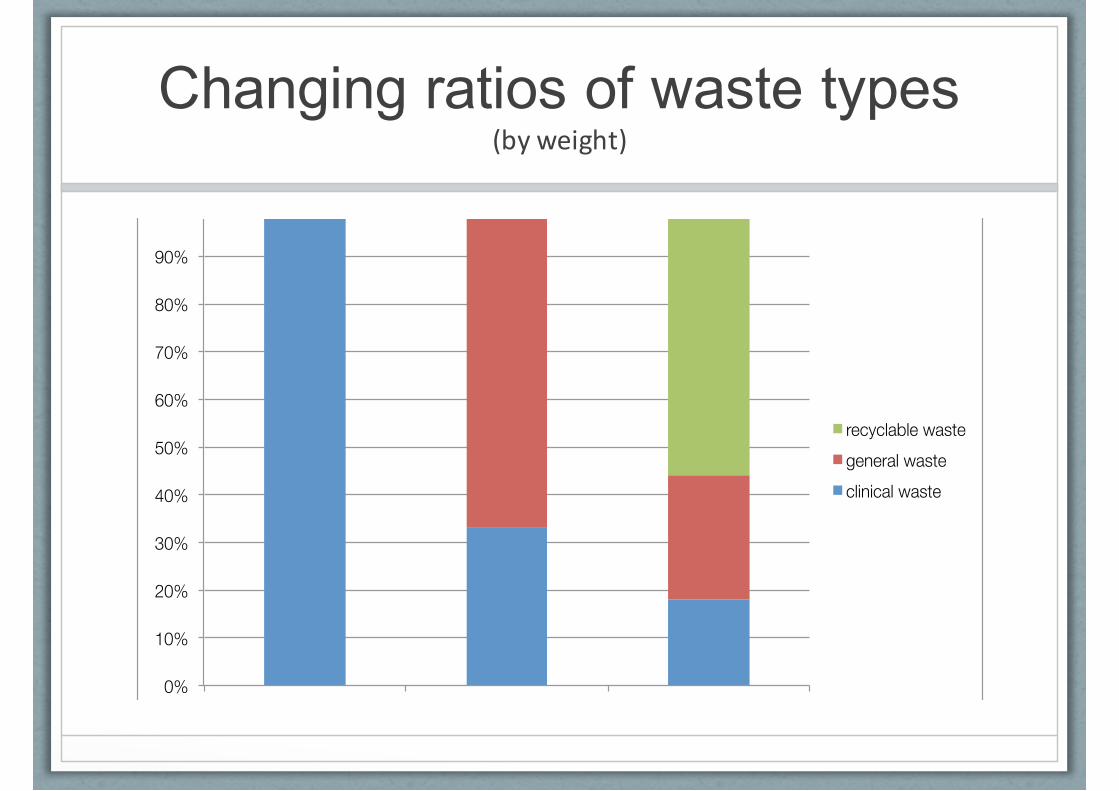
Changing ratios of waste types (byweight)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
baseline segregation segregation and recycling
recyclable waste general waste clinical waste

Changing cost structure for OT
waste disposal
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
baseline segregation segregation and recycling
general waste clinical waste
Implementation
• Success
• Very enthusiastic and passionate theatre staff
• Self driven, dedicated
• Support by hospital waste management
• Stakeholders are supportive
• Determination never to give up
• Challenges
• Increased work load for porter, nurses and medical staff
• Storage capacity
• Auditing system
• Waste tracking system
• Waste collection contractor
Perspective
• Recycling
• copper, stainless steel, single use medical devices, PVC
• Fluid Management System
• medical fluids
• Improve existing strategies
• maximise waste segregation
• maximise recycling activities
• Improve collaboration
• ‘Waste Action Group’
• Improve education
• Input from Waste Management and Waste Champions
Conclusion
• Clinical practice
• Medical waste is directly related to clinical practice, it
represents use/misuse of resources that could otherwise
be spent on patient care [10]
• Local impact
• The proposed recycling program needs to be one
component of a portfolio of hospital-wide green initiatives
• HHS/QLD Health impact
• Well designed waste management programs and the
execution of them help benchmarking services and
facilities

most importantly
• Motivated
• Empowered
• Engage
• Improved morale
• Developed positive attitude and
confidence for change
• Created trust and consistency
• Champions ‘Waste Action
Group’
References
1. Waste Management in Scottish hospitals 2001. Prepared by Audit Scotland. http://www.audit-scotland.gov.uk/
2. Francis M, Metoyer L, Kaye A. Exclusion of noninfectious medical waste from contaminated waste stream. Infection Control and Hospital Epidemiology 1997; 18: 656–658
3. Tieszen M, Gruenberg J. A quantitative, qualitative, and critical assessment of surgical waste. Surgeons venture through the trash can. JAMA 1992; 267: 2765–2768
4. McGain F, Story D, Hendel S. An Audit of intensive care unit recyclable waste. Anaesthesia 2009; 64: 1299–1302
5. D. Brouwer. Survey of Operating Theatre Recycling Practices in Victorian Public Hospitals. http://www.asa.org.au/
6. McGain F, Hendel SA, Story DA. An audit of potentially recyclable waste from anaesthetic practice. Anaesthesia and Intensive Care 2009; 37: 820–823
7. McGain F, Clark M, Williams T, Wardlaw T. Recycling plastics from the operating suite. Anaesthesia and Intensive Care 2008; 36:3–4
8. Jones D, Mitchell A. Lean thinking for the NHS. The NHS Confederation
9. PAH Waste Management Operational Handling Guidelines, Clinical and related Waste Management plan 2012–2018; 6.8: Recyclable Waste
10. Yong PL, Saunders RS, Olsen LA. The Health Care Imperative. Lowering Costs and Improving Outcomes. 2010; National Academies Press