effect of a spacer on pulmonary aerosol deposition from a jet
TRANSCRIPT

Thorax 1995;50:50-53
Effect of a spacer on pulmonary aerosoldeposition from a jet nebuliser duringmechanical ventilation
C J Harvey, M J O'Doherty, C J Page, S H L Thomas, T 0 Nunan, D F Treacher
AbstractBackground - Several factors have beenidentified which improve nebulised aero-sol delivery in vitro. One of these is theaddition ofa spacer to the ventilator circuitwhich improves aerosol delivery from a jetnebuliser to a model lung by ap-proximately 30%. The current study wasdesigned to demonstrate whether similarimprovements could be demonstrated invivo.Methods - Ten patients (seven men) werestudied during mechanical ventilation(Siemens Servo 900C) after open heartsurgery. Aerosol was delivered using a Sie-mens Servo 945 nebuliser system (highsetting) driving a System 22 Acorn jet ne-buliser (Medic-Aid) containing 3 ml tech-netium-99m labeliled human serumalbumin (9Tc-HSA (50 tg); activity in thefirst nebulisation, 90 MBq; in the secondnebulisation, 185 MBq). Central and peri-pheral lung aerosol deposition and thetime to complete deposition were meas-ured using a gamma camera and com-pared when the nebuliser was connectedto the inspiratory limb using a simple T-piece or a 600 ml spacer.Results - The addition of the spacer in-creased total lung deposition (mean (SD)percentage initial nebuliser activity) from2-2 (0-7)% to 3 (0.8)%. There was nodifference in the time required to completenebulisation (18-2 min v 18-3 min re-spectively for T-piece and spacer) or inthe retention of activity in the nebuliser(46-2% v 47-1% respectively).Conclusions -The combination ofa spacerwith a jet nebuliser increased lung de-position by 36% in mechanically ventilatedpatients and is a simple way of increasingdrug deposition or reducing the amountof an expensive drug required for ne-bulisation.(Thorax 1995;50:50-53)
Keywords: ventilator, aerosol, nebuliser.
The administration of nebulised drug aerosolsto mechanically ventilated patients is increasingin intensive therapy units. Several studies haveshown in vivo pulmonary aerosol deposition tobe poor, in the range 1-2-2-9%.1-3 In vitromethods investigating pulmonary deposition,using ventilator circuits and artificial lungs,have shown a number of ways in which aerosoldelivery may be improved during mechanical
ventilation"6 including changing the type ofnebuliser or ventilator settings or increasing thevolume of fill of the nebuliser.The addition of a chamber to conserve aero-
sol formed by jet nebulisers during the ex-piratory phase of respiration for subsequentdelivery during inspiration has been shown al-most to double aerosol deposition in spon-taneously breathing subjects.7 In vitro studieshave shown that the addition of a similar cham-ber or spacer also improves delivery of aerosolfrom a jet nebuliser to a lung model by atleast 25% during mechanical ventilation.56 Thiseffect has not been shown in vivo. This studywas therefore designed to determine whetherthe addition of a spacer to a jet nebuliserimproves pulmonary deposition in mech-anically ventilated patients.
MethodsPATIENT SELECTIONTen patients (seven men, eight ex-smokers andtwo never smokers) were studied during mech-anical ventilation after open heart surgery. Thestudy was approved by the ethics committeeof West Lambeth Health District. Informedconsent was obtained from all patients prior toelective open heart surgery. Measurements offorced expiratory volume in one second (FEVy),forced vital capacity (FVC), and peak ex-piratory flow rate (PEFR)) were made pre-operatively (table 1). Patients with pre-existingrespiratory symptoms or disease were excludedas the aim of the study was to document aerosoldeposition in patients with normal lungs. Stud-ies were only performed on patients who re-quired mechanical ventilation on clinicalgrounds and were commenced within a fewhours of the operative procedure.
STUDY DESIGNAll patients were studied during mechanicalventilation via an endotracheal tube (Siemens
Table 1 Morphometric data, lung function, andventilator settings in 10 ventilated patients
Mean Range
Preoperative assessment:Age (years) 65-1 55-74FEV, (1) 2-1 1-3-3-8FVC (1) 26 16-4-8PEFR (1/min) 444 327-657
Mechanical ventilation settings:Respiratory rate (breaths/ 15 14-16
min)Minute volume (1/min) 9-6 7-7-11-0Inspiratory time (%) 26 25-33Pause time (%) 11 10-20
Intensive TherapyUnitC J HarveyD F Treacher
Department ofNuclear MedicineM J O'DohertyC J PageT 0 Nunan
St Thomas' Hospital,UMDS, LondonSEI 7EH, UK
Wolfson Departmentof ClinicalPharmacology,University ofNewcastle,Newcastle upon TyneNEI 7RU, UKS H L Thomas
Reprint requests to:Dr M J O'Doherty.Received 27 May 1994Returned to authors1 September 1994Revised version received23 September 1994Accepted for publication26 September 1994
50
Effect of a spacer on pulmonary aerosol deposition from a jet nebuliser during mechanical ventilation
Y piece
Catheter moun
In
Heated water Insertion of spacer or
bath T-piece and nebuliser
Figure I The circuit used to ventilate patients with a Siemens 900C ventilator andsite of the nebuliser, T-piece or spacer.
RT
RT LT RT
w-ith T-piece with spacer
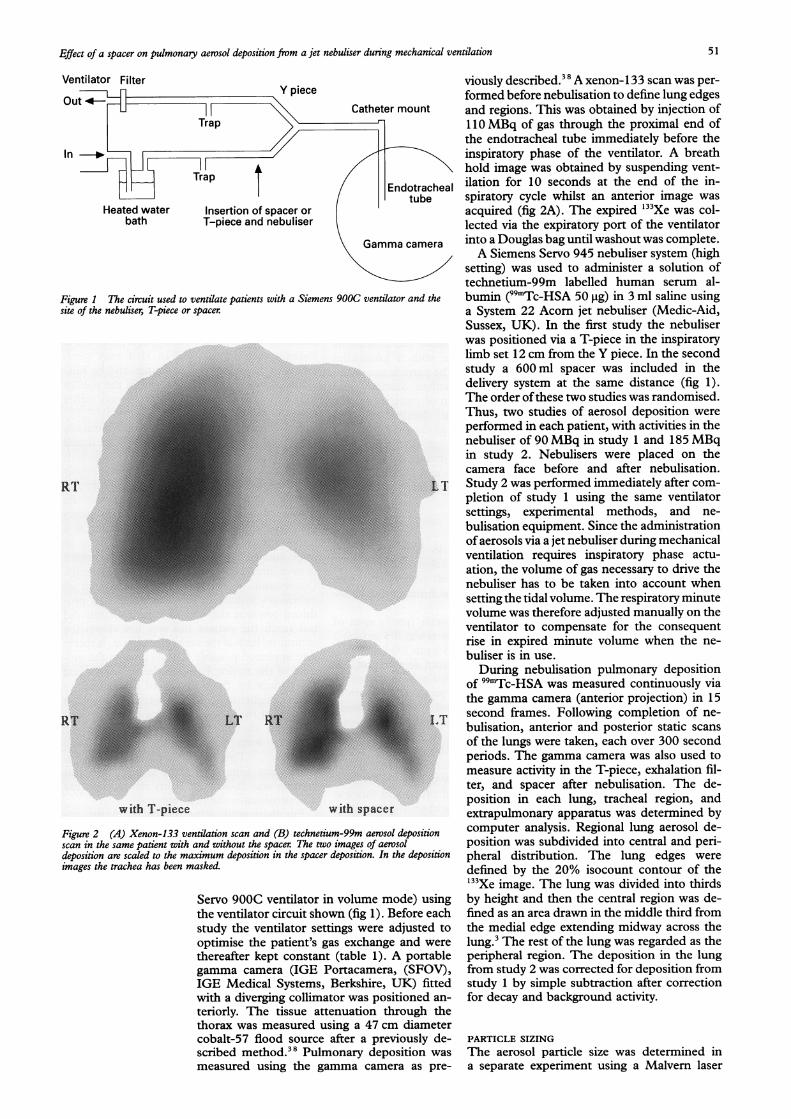
Figure 2 (A) Xenon-133 ventilation scan and (B) technetium-99m aerosol depositscan in the same patient with and without the spacer. The two images of aerosoldeposition are scaled to the maximum deposition in the spacer deposition. In the depoimages the trachea has been masked.
Servo 900C ventilator in volume mode) uthe ventilator circuit shown (fig 1). Beforestudy the ventilator settings were adjusteoptimise the patient's gas exchange and i
thereafter kept constant (table 1). A portgamma camera (IGE Portacamera, (SF4IGE Medical Systems, Berkshire, UK) fwith a diverging collimator was positionecteriorly. The tissue attenuation throughthorax was measured using a 47 cm dian
cobalt-57 flood source after a previouslyscribed method.'8 Pulmonary depositionmeasured using the gamma camera as
viously described.38 A xenon- 133 scan was per-
formed before nebulisation to define lung edgesIt and regions. This was obtained by injection of
110 MBq of gas through the proximal end ofthe endotracheal tube immediately before theinspiratory phase of the ventilator. A breathhold image was obtained by suspending vent-
cheal ilation for 10 seconds at the end of the in-e spiratory cycle whilst an anterior image was
acquired (fig 2A). The expired '33Xe was col-lected via the expiratory port of the ventilator
era into a Douglas bag until washout was complete.A Siemens Servo 945 nebuliser system (high
setting) was used to administer a solution oftechnetium-99m labelled human serum al-
the bumin (99mTc-HSA 50 ,tg) in 3 ml saline usinga System 22 Acorn jet nebuliser (Medic-Aid,Sussex, UK). In the first study the nebuliserwas positioned via a T-piece in the inspiratorylimb set 12 cm from the Y piece. In the secondstudy a 600 ml spacer was included in thedelivery system at the same distance (fig 1).The order ofthese two studies was randomised.Thus, two studies of aerosol deposition were
performed in each patient, with activities in thenebuliser of 90 MBq in study 1 and 185 MBqin study 2. Nebulisers were placed on thecamera face before and after nebulisation.
LT Study 2 was performed immediately after com-pletion of study 1 using the same ventilatorsettings, experimental methods, and ne-
bulisation equipment. Since the administrationof aerosols via a jet nebuliser during mechanicalventilation requires inspiratory phase actu-ation, the volume of gas necessary to drive thenebuliser has to be taken into account whensetting the tidal volume. The respiratory minutevolume was therefore adjusted manually on theventilator to compensate for the consequentrise in expired minute volume when the ne-
buliser is in use.
During nebulisation pulmonary depositionof 99mTc-HSA was measured continuously viathe gamma camera (anterior projection) in 15
LT second frames. Following completion of ne-
bulisation, anterior and posterior static scans
of the lungs were taken, each over 300 secondperiods. The gamma camera was also used tomeasure activity in the T-piece, exhalation fil-ter, and spacer after nebulisation. The de-position in each lung, tracheal region, andextrapulmonary apparatus was determined by
ion computer analysis. Regional lung aerosol de-position was subdivided into central and peri-
sition pheral distribution. The lung edges were
defined by the 20% isocount contour of the133Xe image. The lung was divided into thirds
ising by height and then the central region was de-each fined as an area drawn in the middle third from:d to the medial edge extending midway across thewere lung.3 The rest of the lung was regarded as thetable peripheral region. The deposition in the lungOV), from study 2 was corrected for deposition fromitted study 1 by simple subtraction after correctionI an- for decay and background activity.the
aeterr de- PARTICLE SIZINGwas The aerosol particle size was determined inpre- a separate experiment using a Malvern laser
Ventilator Filter
Out Hh
51

Harvey, O'Doherty, Page, Thomas, Nunan, Treacher
Table 2 Mean (SD) aerosol deposition in 10 ventilatedpatients with and without a spacer
T-piece Spacer
Pulmonary deposition:Both lungs 2-19 (0-73) 2-99 (078)*Peripheral 2-00 (0-69) 2-54 (0 70)*Central 0 19 (0 1) 0 45 (0 2)*Right lung 1-47 (0-58) 2-04 (0-66)*Left lung 0-71 (0-25) 0 95 (0 28)*
Extrapulmonary deposition:Tracheal endotracheal tube 1-14 (0-49) 1-48 (0 93)Exhalation filter 18-10 (2 48) 15-45 (1-5)T-piece or spacer 1 09 (0-39) 5-65 (15)Nebuliser retention 46-20 (7-3) 47-10 (7 9)
Time to completion of 18-2 (5) 18-3 (4-5)nebulisation (min)* p<0 02, two tailed paired t test.
mastersizer. The aerosol was measured at thetip of the endotracheal tube; the conditionswere otherwise the same with a humidifieroperating in the circuit. The particle sizes wererecorded as the mass median diameter andthe span. The distribution of particles from anebuliser have a gaussian distribution. Thespan is therefore defined as the ratio obtainedby subtracting the 10th centile particle sizediameter from the larger diameter of the 90thcentile particle dimension and dividing by thesize of the 50th centile particle.
ResultsPatient details are given in table 1. All hadundergone either cardiac valve replacement or
coronary artery bypass graft surgery and wereintubated with an 8 mm or 9 mm cuffed endo-tracheal tube.The mass median diameter (gm) ± span of
the aerosol without the spacer was 3 5 gim + 0 2and with the spacer was 3 5 um+±0 1.The pattern of radioaerosol distribution, ex-
pressed as percentage initial nebuliser activity,is given in table 2. As previously reported,aerosol deposition varied widely betweenpatients. In the left lung ventilation and aerosoldeposition were reduced in all patients; thescan of one patient is shown in fig 2 andclearly illustrates this. The addition of a spacerincreased total pulmonary deposition by 36%(p<0.02, paired two tailed t test) and this wasassociated with a reduction in aerosol loss downthe expiratory limb of the circuit. Ap-proximately 30% ofthe initial nebuliser activityis unaccounted for and is presumed to be de-posited in the ventilator circuit. It was notpossible to measure this because of technicaldifficulties in scanning long lengths of tubing,traps, and a heated water bath.
DiscussionImproving the efficiency of aerosol deliveryby nebulisers is worthwhile because this mayincrease their clinical value and reduce theexpense of drugs administered using this route.There are a number offactors that affect aerosoldelivery from a nebuliser during mechanicalventilation which have been identified invitro.' Delivery may be increased by optim-
ising the nebuliser position, changing the gasflow to the nebuliser, increasing the inspiratoryfraction, reducing the respiratory rate or minutevolume, increasing nebuliser fill, or reducinghumidity.4 These in vitro measurements in-dicate possible ways of increasing delivery topatients but they cannot allow for the specificsof airway geometry and humidity, lung disease,or mucus secretion. Neither can they predictthe site of deposition within the bronchial tree.Thus, in vivo studies are needed to quantifythe amount deposited in the trachea, majorairways, and "peripheral" lung. In vitro aerosoldelivery will be greater than the in vivo lungdeposition since the filter used in the modelventilator circuit captures all delivered aerosolparticles and cannot quantify the propositionthat would be exhaled or deposited in themajor airways and the endotracheal tube. Otherindirect techniques used in vivo may over-estimate the delivery to the lungs and be mis-leading since the deposition within the patientmay be in the trachea or major airways ratherthan the peripheral lung.8
Nebulised aerosol deposition in mechanicallyventilated patients has previously been foundto be between 1P2% and 2-9%,'-' which isnot as efficient as deposition in spontaneouslybreathing subjects even though the nebuliser isusually only activated during lung inflation. Asaerosol therapy may be of value in manypatients requiring mechanical ventilation, it isimportant to establish why deposition is sopoor and to design nebuliser systems whichdeliver therapeutic aerosols more efficiently.Observation of inspiratory phase activated jetnebulisers indicated that some aerosol pro-duced towards the end of lung inflation didnot reach the patient but was lost down theexpiratory limb ofthe ventilator circuit. It there-fore appeared possible that increasing the vol-ume of the tubing between the nebuliser andthe patient by the addition of a reservoir orspacer might conserve this wasted aerosol fordelivery at the subsequent lung inflation. Thishas been shown in spontaneously breathingsubjects with aerosol and metered doseinhalers.79"-" This effect was confirmed in vitroby studies using a 600 ml spacer5 and thisvolume was chosen for study in vivo becauseit approximates the tidal volume.For these studies the System 22 Acorn ne-
buliser and Siemens 945 nebuliser activatingsystem were chosen because they are commonlyused on intensive care units and produce suit-ably sized particles, small enough to passthrough the ventilator circuit and endotrachealtubing to reach the patient. The experimentalprotocol, involving two separate but sequentialexperiments in the same patient, was chosenbecause it is convenient and allows a pairedcomparison. Its validity and reproducibilityhave been reported previously.'The results confirmed that total pulmonary
deposition is consistent with values found inprevious studies as is the percentage depositedin the endotracheal tube/trachea and retainedin the nebuliser.3 Pulmonary deposition andventilation were reduced in the left lung. Thiswas most probably due to the opening of the
52

Effect of a spacer on pulmonary aerosol deposition from a jet nebuliser during mechanical ventilation
pleura on the left side during the operativeprocedure. This would result in the greaterdegree ofcollapse ofthe left lung with the lowerlobe expansion being most affected post-operatively. The results also showed that theimprovement in aerosol delivery with a spacerobtained in vitro could be produced in vivo,and that aerosol delivery was significantly in-creased to all regions of the lung. This is animportant observation as it illustrates the valueof in vitro studies using lung models for pre-dicting the effects of nebuliser or ventilatorcircuit modifications on aerosol delivery in vivo.The increase was associated with a reductionin aerosol entering the expiratory limb of thecircuit and this is consistent with the way thespacer works. The observed improvement ismodest and is unlikely to be of great clinicalimportance when used alone. However, whenused in combination with other modifications- for example, increased volume of fluid inthe nebuliser - it may make a useful con-tribution to an overall improvement in aerosoldeposition. It was to be expected that the im-provement in delivery with an aerosol reservoirwould not be as great during volume cycledventilation as in spontaneously breathing sub-jects, as in the former the nebuliser is in-spiratory phase activated and a largerproportion of the aerosol is produced duringlung inflation. Larger improvements would bepredicted if the nebuliser was driven through-out the respiratory cycle, as happens with pres-sure cycled ventilation. It may also be that
600 ml is not the optimum spacer volume andfurther studies in this area would be useful.The authors thank the nursing staff and technicians of MeadWard, St Thomas' Hospital, especially Valerie Arnold, for theircooperation and technical assistance. We are particularly gratefulto Mr C Young, Mr G Venn, Dr C Apps, Dr T Hunt, and DrR Linton for allowing them to study their patients.
1 Fuller HD, Dolovich MB, Posmituck G, Wong Pack W,Newhouse MT. Pressurised aerosol versus jet aerosol de-livery to mechanically ventilated patients. Comparison ofdose to the lungs. Am Rev Respir Dis 1990;141:440-4.
2 MacIntyre NR, Silver RM, Miller CW, Schuler F, ColemanRE. Aerosol delivery in intubated mechanically ventilatedpatients. Crit Care Med 1985;13:81-4.
3 Thomas SHL, O'Doherty MJ, Fidler HM, Page CJ,Treacher DF, Nunan TO. Pulmonary deposition of anebulised aerosol during mechanical ventilation. Thorax1993;48: 154-9.
4 O'Riordan TG, Greco MJ, Perry RJ, Smaldone GC. Ne-bulizer function during mechanical ventilation. Am RevRespir Dis 1992;145:1117-22.
5 O'Doherty MJ, Thomas SHL, Page CJ, Treacher DF,Nunan TO. Delivery of a nebulised aerosol to a lungmodel during mechanical ventilation: effect of ventilatorsettings and nebuliser type, position and volume of fill.Am Rev Respir Dis 1992;146:383-8.
6 Thomas SHL, O'Doherty MJ, Page CJ, Treacher DF,Nunan TO. Delivery of ultrasonic nebulised aerosols toa lung model during mechanical ventilation. Am Rev RespirDis 1993;148:872-7.
7 Thomas SHL, Langford JA, George RDG, Geddes DM.Improving the efficiency of drug administration with jetnebulisers. Lancet 1988;i:126.
8 O'Riordan TG, Palmer LB, Smaldone GC. Aerosol de-position in mechanically ventilated patients: optimisingnebuliser delivery. Am J Respir Crit Care Med 1994;149:214-9.
9 Newman SP, Moren F, Pavia D, Little F, Clarke SW.Deposition of pressurised suspension aerosols inhaledthrough extension devices. Am Rev Respir Dis 1981;124:317-20.
10 Newman SP, Millar AB, Lennard-Jones TR, Moren F,Clarke SW. Improvement ofpressurised aerosol depositionwith Nebuhaler spacer device. Thorax 1984;39:935-41.
11 Vidgren MT, Paronen TPi, Karkkainen A, Karjalainen P.Effect of extension devices on drug deposition from in-halation aerosols. Int -Pharm 1987;39:107-12.
53