efficacy of tomosynthesis (dbt) in respect to two ... · please note: links to movies, ppt...
TRANSCRIPT

Page 1 of 22
Efficacy of tomosynthesis (DBT) in respect to two differentmodes (HR vs ST) in a clinical setting.Preliminary results.
Poster No.: C-1139
Congress: ECR 2014
Type: Educational Exhibit
Authors: M. Schulze-Hagen, N. Eshghi, J. Müller, C. Müller-Leisse;Mönchengladbach/DE
Keywords: Biopsy, Mammography, Radioprotection / Radiation dose,Oncology, Breast, Cancer
DOI: 10.1594/ecr2014/C-1139
Any information contained in this pdf file is automatically generated from digital materialsubmitted to EPOS by third parties in the form of scientific presentations. Referencesto any names, marks, products, or services of third parties or hypertext links to third-party sites or information are provided solely as a convenience to you and do not inany way constitute or imply ECR's endorsement, sponsorship or recommendation of thethird party, information, product or service. ECR is not responsible for the content ofthese pages and does not make any representations regarding the content or accuracyof material in this file.As per copyright regulations, any unauthorised use of the material or parts thereof aswell as commercial reproduction or multiple distribution by any traditional or electronicallybased reproduction/publication method ist strictly prohibited.You agree to defend, indemnify, and hold ECR harmless from and against any and allclaims, damages, costs, and expenses, including attorneys' fees, arising from or relatedto your use of these pages.Please note: Links to movies, ppt slideshows and any other multimedia files are notavailable in the pdf version of presentations.www.myESR.org

Page 2 of 22
Learning objectives
Learning objectives
Purpose: To present first impressions of digital breast tomosynthesis (DBT) in twodifferent modes: Standard Mode (ST-mode) and High Resolution Mode (HR-mode) withone of the first installed Amulet Innovality by Fujifilm.
From September 2013 to December 2013 48 breast tomosynthesis studies were acquiredin one of two ways: either ST-mode in CC-plane and HR-mode in MLO-plane or viceversa. Indications for DBT were:
1. DBT as an alternative to small focus magnification images in unclear casesin Full Field Digital Mammogrophy (FFDM),
2. DBT before surgical treatment of breast cancer in dense breast tissue (ACR3, ACR 4) and for cases with suspected multicentricity or multifocality.
Three readers (1 gynecologist, 2 radiologists) rated the images using the ACR/BI-RADSscore.
Background
Background
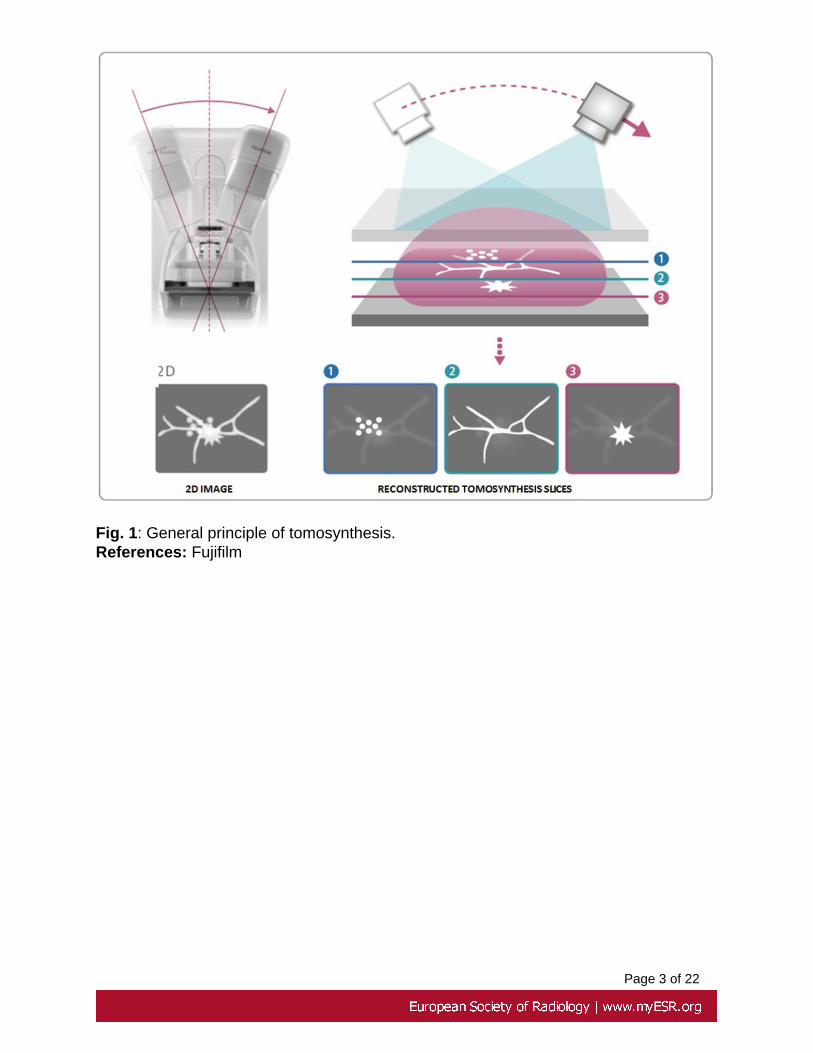
DBT is a new technology of digital mammography which obtains 3D information from alimited number of images by rotating the X-ray source within a limited angle. The breastis positioned the same way it is in a conventional mammogram. A computer algorithmreconstructs a series of image slices (interval 1mm) to depict the anatomy of the breastin 3 dimensions. (Fig.1)
Page 3 of 22
Fig. 1: General principle of tomosynthesis.References: Fujifilm
Page 4 of 22
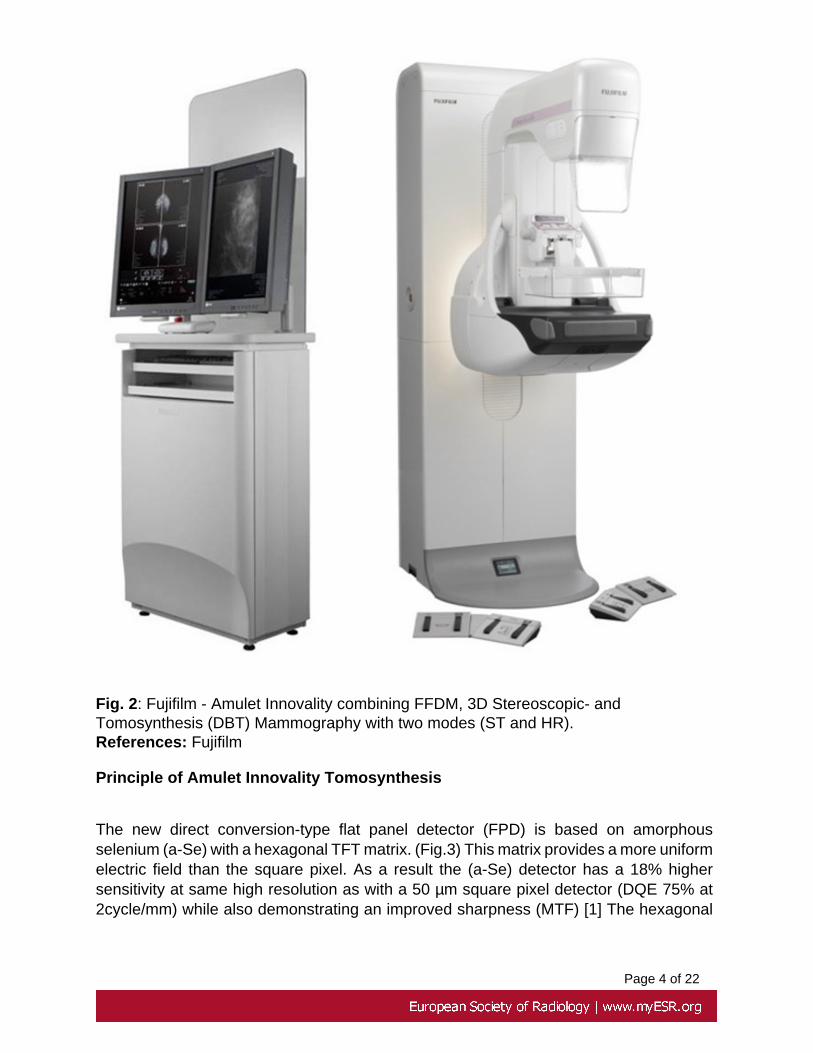
Fig. 2: Fujifilm - Amulet Innovality combining FFDM, 3D Stereoscopic- andTomosynthesis (DBT) Mammography with two modes (ST and HR).References: Fujifilm
Principle of Amulet Innovality Tomosynthesis
The new direct conversion-type flat panel detector (FPD) is based on amorphousselenium (a-Se) with a hexagonal TFT matrix. (Fig.3) This matrix provides a more uniformelectric field than the square pixel. As a result the (a-Se) detector has a 18% highersensitivity at same high resolution as with a 50 µm square pixel detector (DQE 75% at2cycle/mm) while also demonstrating an improved sharpness (MTF) [1] The hexagonal
Page 5 of 22
pixel matrix enables different image output resolutions depending on the diagnostic useand required information [2].
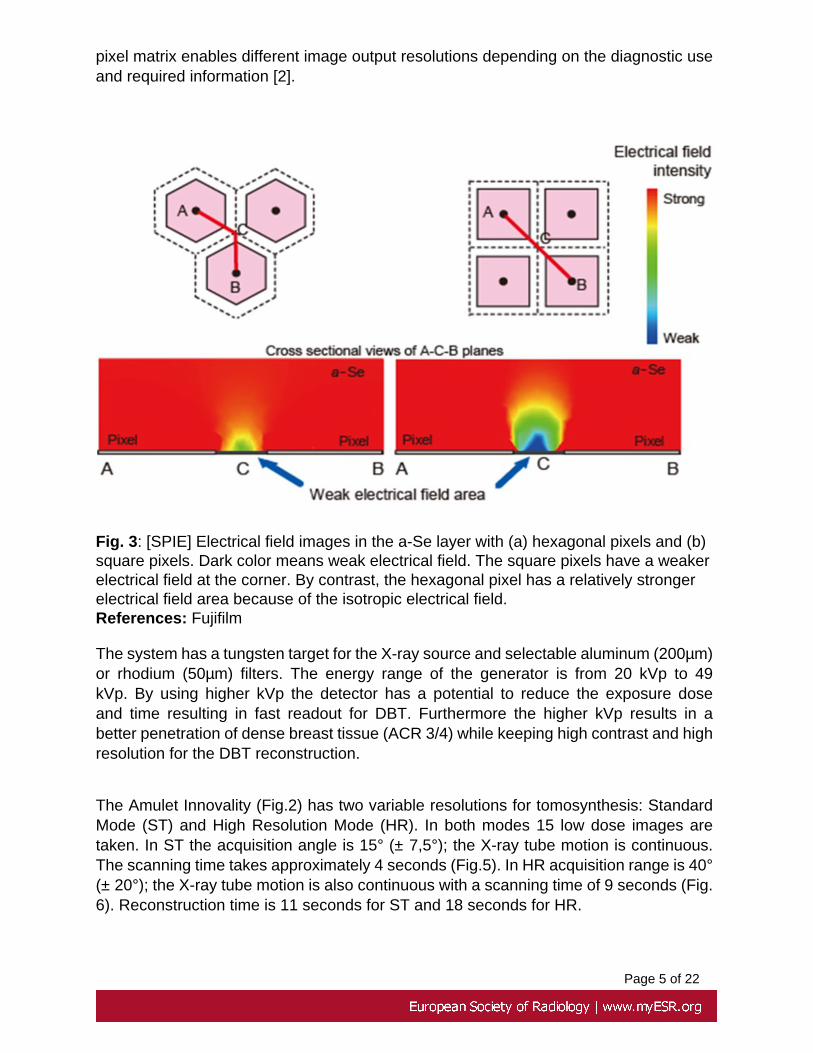
Fig. 3: [SPIE] Electrical field images in the a-Se layer with (a) hexagonal pixels and (b)square pixels. Dark color means weak electrical field. The square pixels have a weakerelectrical field at the corner. By contrast, the hexagonal pixel has a relatively strongerelectrical field area because of the isotropic electrical field.References: Fujifilm
The system has a tungsten target for the X-ray source and selectable aluminum (200µm)or rhodium (50µm) filters. The energy range of the generator is from 20 kVp to 49kVp. By using higher kVp the detector has a potential to reduce the exposure doseand time resulting in fast readout for DBT. Furthermore the higher kVp results in abetter penetration of dense breast tissue (ACR 3/4) while keeping high contrast and highresolution for the DBT reconstruction.
The Amulet Innovality (Fig.2) has two variable resolutions for tomosynthesis: StandardMode (ST) and High Resolution Mode (HR). In both modes 15 low dose images aretaken. In ST the acquisition angle is 15° (± 7,5°); the X-ray tube motion is continuous.The scanning time takes approximately 4 seconds (Fig.5). In HR acquisition range is 40°(± 20°); the X-ray tube motion is also continuous with a scanning time of 9 seconds (Fig.6). Reconstruction time is 11 seconds for ST and 18 seconds for HR.

Page 6 of 22
Together with Pixel Binning and Image Matrix a very high resolution is possible in FFDMand DBT: In FFDM 50µm, in ST 150 µm (2x2 pixel binning), and in HR 100 µm (no binning,but pixel conversion).
Radiation dose is for the normal dose mode (N-mode) 0.9 mGy for FFDM, 1.3 mGy forST mode tomosynthesis and 2.5 mGy for HR mode tomosynthesis using 40mm PMMA[3]. The low dose mode (L-mode) has a radiation dose of 0.6 mGy for FFDM, 1.0 mGy forST mode tomosynthesis and 2.0 mGy for HR mode tomosynthesis using 40 mm PMMA.In this way the ST requires only a low radiation dose for a good separation of overlappingstructures.
Fig. 4: Different pixel conversion for ST- and HR-mode digital breast tomosynthesis.References: Fujifilm

Page 7 of 22
Fig. 5: ST-Mode with low dose (L-mode 1 mGy at 40mm PMMA)and small angle (±7.5°).References: Fujifilm

Page 8 of 22
Fig. 6: HR-Mode with higher dose (L-mode 2 mGy using 40mm PMMA) and widerangle (± 20°) allows a better separation of detailed structures for in-depth assessmentof breast architecture and volumetric analysis.References: Fujifilm
Images for this section:
Fig. 1: General principle of tomosynthesis.

Page 9 of 22
Fig. 2: Fujifilm - Amulet Innovality combining FFDM, 3D Stereoscopic- andTomosynthesis (DBT) Mammography with two modes (ST and HR).

Page 10 of 22
Fig. 3: [SPIE] Electrical field images in the a-Se layer with (a) hexagonal pixels and (b)square pixels. Dark color means weak electrical field. The square pixels have a weakerelectrical field at the corner. By contrast, the hexagonal pixel has a relatively strongerelectrical field area because of the isotropic electrical field.
Fig. 4: Different pixel conversion for ST- and HR-mode digital breast tomosynthesis.

Page 11 of 22
Fig. 5: ST-Mode with low dose (L-mode 1 mGy at 40mm PMMA)and small angle (± 7.5°).
Fig. 6: HR-Mode with higher dose (L-mode 2 mGy using 40mm PMMA) and wider angle(± 20°) allows a better separation of detailed structures for in-depth assessment of breastarchitecture and volumetric analysis.

Page 12 of 22
Findings and procedure details
A specimen study at the Nagoya Medical Centre in Japan with 25 breast resectionspecimens was carried out to identify the optimum DBT images for diagnostics.
Endo et al. found that HR-mode DBT has a high-depth resolution and can providespiculations and tumors margins clearly. In ST-mode DBT depth resolution decreases,but calcification distribution and tissue structures are able to be detected in a short timewith low dose [4].
Our first clinical results rely on 48 cases of a curative setting with suspicious findings,acquired from September 2013 until December 2013. In 25 cases, Core Needle Biopsy(CNB) or Stereotactic Vacuum Needle Biopsy (SVNB) were taken (Tab. 1 and 2).
Tab. 1: (Pre-)maligne histologies
Histology N = 17
Invasive ductal carcinoma (IDC) 11
Invasive lobular carcinoma (ILC) 2
Ductal carcinoma in situ (DCIS) 2
Atypical papilloma 1
Intracystic papilloma 1
Tab. 2: Benign histologies
Histology N = 8
Fibrosis mammae 2
Lipoidnecrosis 2
Adenosis tumor 2
Infected cyst 1
Adenofibrolipoma 1
In 23 cases with a suspected lesion in FFDM, DBT revealed that these findings wereresults of overlapping structures.
Results:

Page 13 of 22
In comparison to ST-mode the HR-mode has a higher resolution in all three dimensions.This leads to better visibility of microcalcifications in HR than in ST-mode (Fig. 7).
Fig. 7: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3, BI-RADS 4b). DBT in ST and HR-mode revealed a suspicious group of microcalcificationsin the retroareolar region. Microcalcifications were more detectable in HR-mode than inST-mode. Histology of SVNB was DCIS, G2.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE
Fig. 8: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3,BI-RADS 5). Due to dense breast tissue in FFDM and suspicion of multifocality ormulticentricity DBT was performed before surgery. Architectural distortion, signs ofretraction and tumor margins displayed improved visibility in both modes of DBTcompared to FFDM; HR-mode providing even better visualisation than ST-mode.

Page 14 of 22
Microcalcifications were more detectable in HR-mode than in ST-mode. Histology ofCNB: IDC G1 + DCIS G1.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE
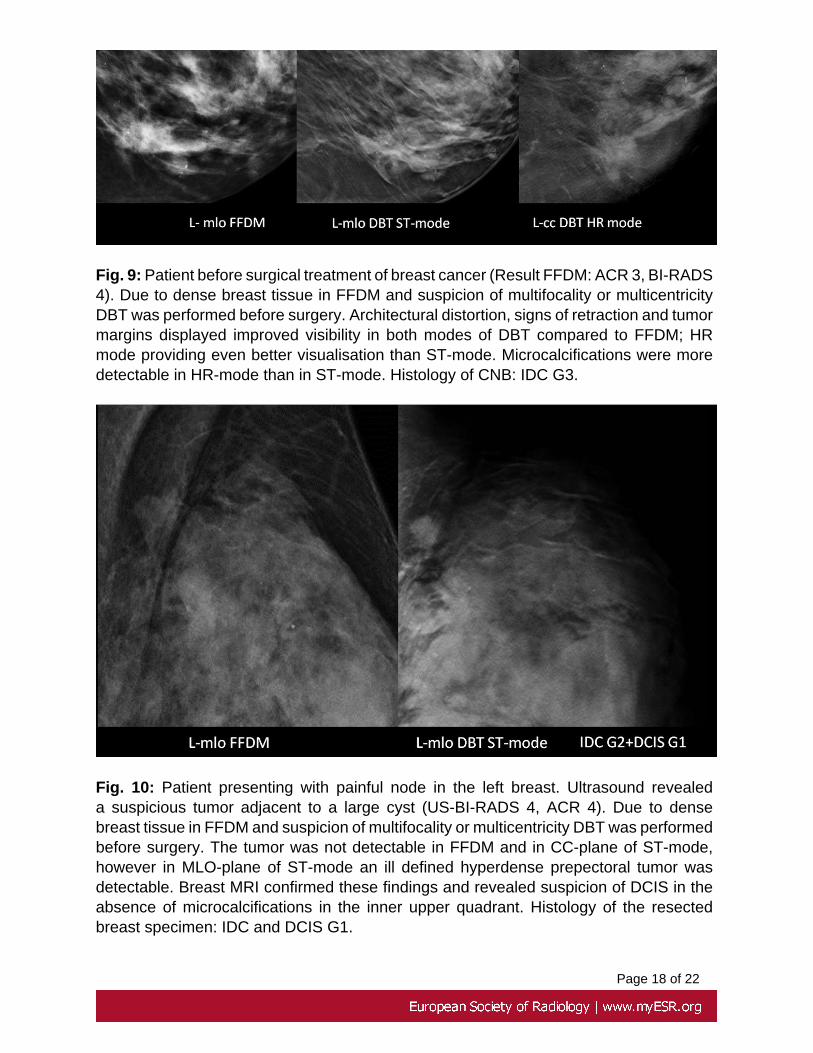
Fig. 9: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3,BI-RADS 4). Due to dense breast tissue in FFDM and suspicion of multifocality ormulticentricity DBT was performed before surgery. Architectural distortion, signs ofretraction and tumor margins displayed improved visibility in both modes of DBTcompared to FFDM; HR mode providing even better visualisation than ST-mode.Microcalcifications were more detectable in HR-mode than in ST-mode. Histology ofCNB: IDC G3.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE
Fig. 10: Patient presenting with painful node in the left breast. Ultrasound revealeda suspicious tumor adjacent to a large cyst (US-BI-RADS 4, ACR 4). Due to dense

Page 15 of 22
breast tissue in FFDM and suspicion of multifocality or multicentricity DBT wasperformed before surgery. The tumor was not detectable in FFDM and in CC-plane ofST-mode, however in MLO-plane of ST-mode an ill defined hyperdense prepectoraltumor was detectable. Breast MRI confirmed these findings and revealed suspicion ofDCIS in the absence of microcalcifications in the inner upper quadrant. Histology of theresected breast specimen: IDC and DCIS G1.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE
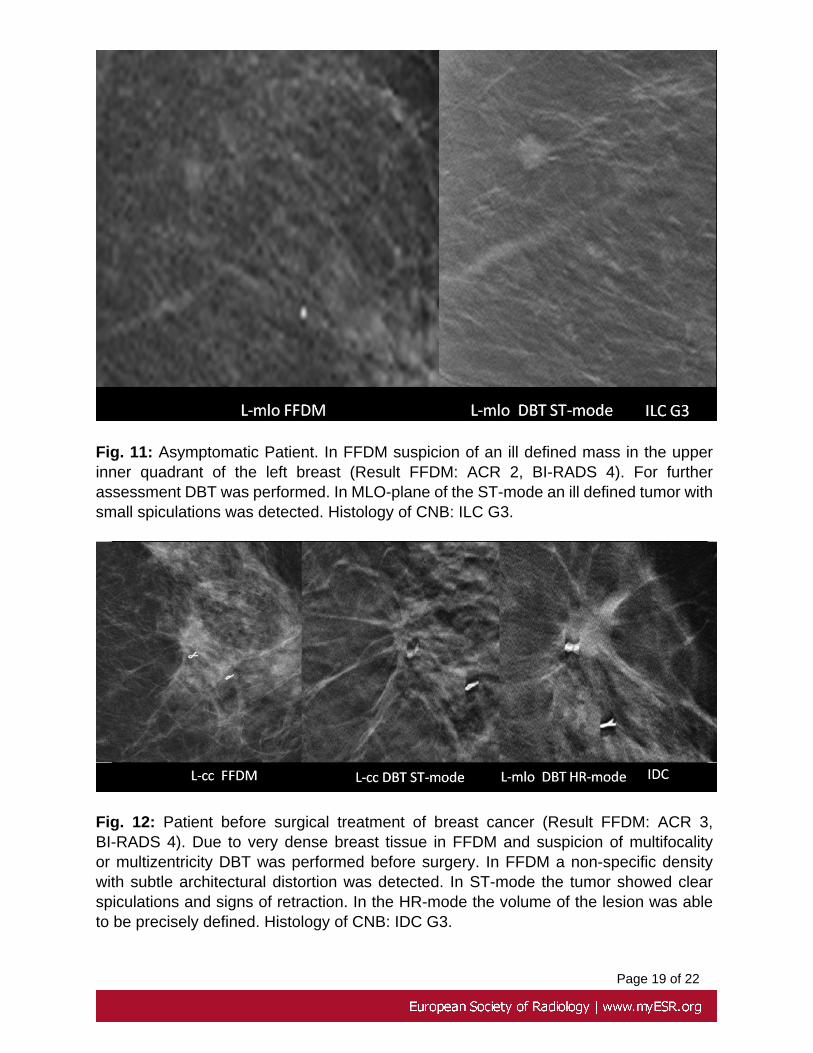
Fig. 11: Asymptomatic Patient. In FFDM suspicion of an ill defined mass in theupper inner quadrant of the left breast (Result FFDM: ACR 2, BI-RADS 4). For furtherassessment DBT was performed. In MLO-plane of the ST-mode an ill defined tumorwith small spiculations was detected. Histology of CNB: ILC G3.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE

Page 16 of 22
Fig. 12: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3, BI-RADS 4). Due to very dense breast tissue in FFDM and suspicion of multifocality ormultizentricity DBT was performed before surgery. In FFDM a non-specific densitywith subtle architectural distortion was detected. In ST-mode the tumor showed clearspiculations and signs of retraction. In the HR-mode the volume of the lesion was ableto be precisely defined. Histology of CNB: IDC G3.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE
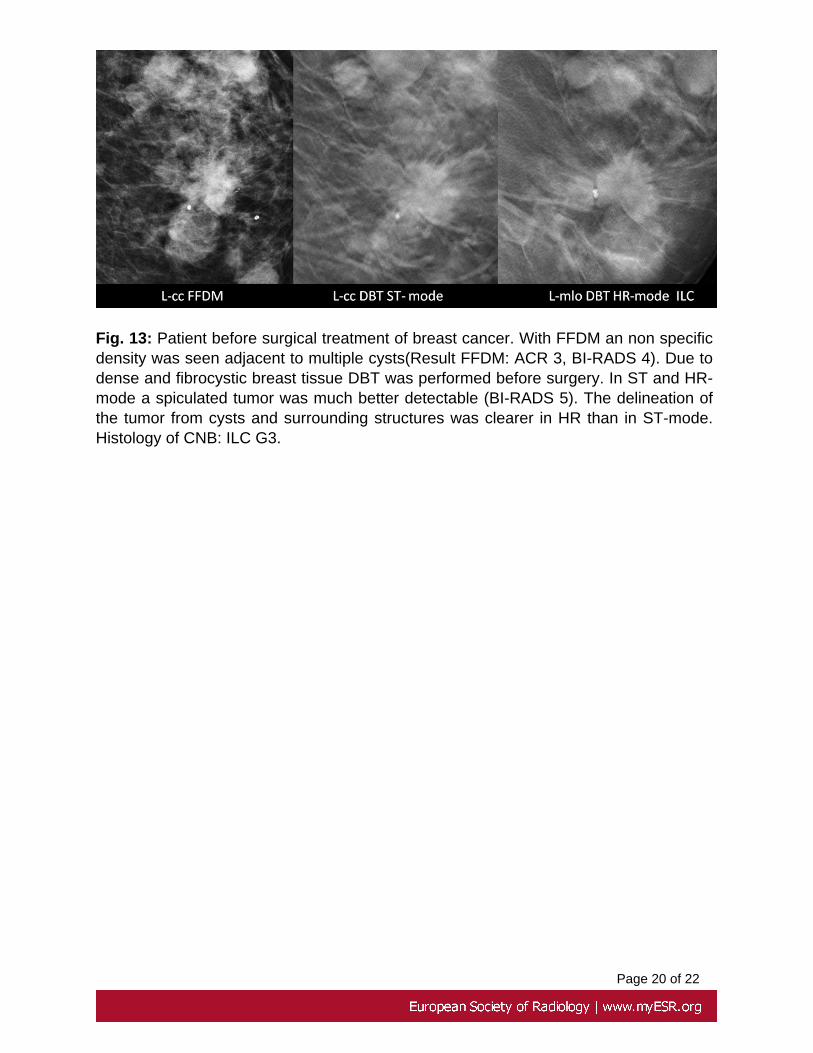
Fig. 13: Patient before surgical treatment of breast cancer. With FFDM an non specificdensity was seen adjacent to multiple cysts(Result FFDM: ACR 3, BI-RADS 4). Due todense and fibrocystic breast tissue DBT was performed before surgery. In ST and HR-mode a spiculated tumor was much better detectable (BI-RADS 5). The delineation ofthe tumor from cysts and surrounding structures was clearer in HR than in ST-mode.Histology of CNB: ILC G3.References: Radiology, Kliniken Maria Hilf - Mönchengladbach/DE

Page 17 of 22
Images for this section:
Fig. 7: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3, BI-RADS 4b). DBT in ST and HR-mode revealed a suspicious group of microcalcificationsin the retroareolar region. Microcalcifications were more detectable in HR-mode than inST-mode. Histology of SVNB was DCIS, G2.
Fig. 8: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3, BI-RADS5). Due to dense breast tissue in FFDM and suspicion of multifocality or multicentricityDBT was performed before surgery. Architectural distortion, signs of retraction and tumormargins displayed improved visibility in both modes of DBT compared to FFDM; HR-mode providing even better visualisation than ST-mode. Microcalcifications were moredetectable in HR-mode than in ST-mode. Histology of CNB: IDC G1 + DCIS G1.
Page 18 of 22
Fig. 9: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3, BI-RADS4). Due to dense breast tissue in FFDM and suspicion of multifocality or multicentricityDBT was performed before surgery. Architectural distortion, signs of retraction and tumormargins displayed improved visibility in both modes of DBT compared to FFDM; HRmode providing even better visualisation than ST-mode. Microcalcifications were moredetectable in HR-mode than in ST-mode. Histology of CNB: IDC G3.
Fig. 10: Patient presenting with painful node in the left breast. Ultrasound revealeda suspicious tumor adjacent to a large cyst (US-BI-RADS 4, ACR 4). Due to densebreast tissue in FFDM and suspicion of multifocality or multicentricity DBT was performedbefore surgery. The tumor was not detectable in FFDM and in CC-plane of ST-mode,however in MLO-plane of ST-mode an ill defined hyperdense prepectoral tumor wasdetectable. Breast MRI confirmed these findings and revealed suspicion of DCIS in theabsence of microcalcifications in the inner upper quadrant. Histology of the resectedbreast specimen: IDC and DCIS G1.
Page 19 of 22
Fig. 11: Asymptomatic Patient. In FFDM suspicion of an ill defined mass in the upperinner quadrant of the left breast (Result FFDM: ACR 2, BI-RADS 4). For furtherassessment DBT was performed. In MLO-plane of the ST-mode an ill defined tumor withsmall spiculations was detected. Histology of CNB: ILC G3.
Fig. 12: Patient before surgical treatment of breast cancer (Result FFDM: ACR 3,BI-RADS 4). Due to very dense breast tissue in FFDM and suspicion of multifocalityor multizentricity DBT was performed before surgery. In FFDM a non-specific densitywith subtle architectural distortion was detected. In ST-mode the tumor showed clearspiculations and signs of retraction. In the HR-mode the volume of the lesion was ableto be precisely defined. Histology of CNB: IDC G3.
Page 20 of 22
Fig. 13: Patient before surgical treatment of breast cancer. With FFDM an non specificdensity was seen adjacent to multiple cysts(Result FFDM: ACR 3, BI-RADS 4). Due todense and fibrocystic breast tissue DBT was performed before surgery. In ST and HR-mode a spiculated tumor was much better detectable (BI-RADS 5). The delineation ofthe tumor from cysts and surrounding structures was clearer in HR than in ST-mode.Histology of CNB: ILC G3.

Page 21 of 22
Conclusion
We report our first impressions and experiences with breast tomosynthesis (DBT) in twodifferent modes with one of the first installed Amulet Innovality by Fujifilm.
Overall, DBT seems to detect architectural distortions, signs of retraction and tumormargins much clearer than FFDM. The ST-mode offers a good potential for routineapplication as a result of good tissue separation with the use of a low dose (similarto FFDM). Due to higher resolution HR-mode DBT may be more effective in terms ofunspecific densities, unclear lesions and microcalcifications in dense breast tissue (ACR3/4), taking into account that a higher dose is needed to be applied.
Prospective clinical studies are required to confirm these first impressions. The upcomingintroduction of slice combination and synthesized 2D images of DBT may also give furtherinformation about the surrounding area, geometry and orientation in difficult cases.
Personal information
Dr. Mechthild Schulze-Hagen
Annakirchstr. 33
D-41063 Moenchengladbach
Gynecologist
Reader in German Breast Cancer Screening Program
Nagmeh Eshghi
Kliniken Maria Hilf
Sandradstr. 43
D-41061 Moenchengladbach
Radiologist
Joerg Müller
DR Product manager
Page 22 of 22
FUJIFILM Europe GmbH, Medical Systems
Heesenstr. 31
D-49549 Duesseldorf
Prof. Dr. Christoph Müller-Leisse
Head of the Department of Radiology
Kliniken Maria Hilf
Sandradstr. 43
D-41061 Moenchengladbach
Radiologist
References
1. Okada Y, Sato K, Ito T, Hosoi Y , Hayakoawa T: A newly developed a-Se mammography flat panel detector with high-sensitivity and low imageartifact , SPIE 8668-213 - (2013)
2. He X and Jia W: Hexagonal Structure for Intelligent Vision", IEEE Proc.ICICT 52-64 (2005)
3. Dance DR, Young KC, van Engen RE: Estimation of mean glandular dosefor breast tomosynthesis: factors for use with the UK, European and IAEAbreast dosimetry protocols. Physics in Medicine and Biology, 2011, 56:453-471.
4. Endo T et al.: Clinical evaluation of new mammography system withtungsten anode and image based Spectral Conversion technology, ECR2014 EPOS Nr. 3314