electrocardiographic applications of lead avr · pdf filediagnostics electrocardiographic...
TRANSCRIPT

Diagnostics
Electrocardiographic applications of lead aVR
Kelly Williamsona, Amal Mattu MDb, Claire U. Plautz MDc,d,e,Allan Binder MDc, William J. Brady MDc,d,e,*
aSchool of Medicine, University of Virginia, Charlottesville, VA, USAbDepartment of Emergency Medicine, University of Maryland, Baltimore, MD, USAcDepartment of Internal Medicine (Cardiology), University of Virginia School of Medicine, Charlottesville, VA, USAdDepartment of Emergency Medicine, School of Medicine, University of Virginia, Charlottesville, VA, USAeDepartment of Internal Medicine, School of Medicine, University of Virginia, Charlottesville, VA, USA
Received 26 May 2006; accepted 28 May 2006
Abstract Lead aVR, 1 of 12 electrocardiographic leads, is frequently ignored in clinical medicine. Infact, many clinicians refer to the 12-lead electrocardiogram (ECG) as the 11-lead ECG, noting the
commonly held belief that lead aVR rarely offers clinically useful information. In this report, we discussthe findings in lead aVR, which are potentially of value, including ST-segment elevation in the patientwith acute coronary syndrome suggestive of left main coronary artery occlusion, PR-segment elevation
in the patient with acute pericarditis, prominent R wave in the patient with significant tricyclicantidepressant poisoning, and ST-segment elevation in narrow complex tachycardia suggestive of Wolff-Parkinson-White syndrome.
D 2006 Elsevier Inc. All rights reserved.
1. Introduction
Emergency physicians (EPs) encounter a multitude ofpatients in their daily practice; the EP is required to makeurgent diagnoses with a limited amount of diagnosticinformation. The 12-lead electrocardiogram (ECG) is awidely available inexpensive bedside tool that the EP reliesupon to make rapid diagnoses such as dysrhythmias, acutemyocardial infarction (AMI), electrolyte disturbance, car-diotoxic ingestion, and conduction abnormality.
The electrical activity of the heart was first recorded byAugustus Waller in 1887, and then its development as aclinical tool was pioneered by the work ofWilliam Einthovenin the early 20th century. Electrocardiography is based upon
the principle that the depolarization and repolarization of the
myocardium generates an electrical current, which is
measurable on the surface of the body through the use of 6
precordial leads and 6 limb (both unipolar and bipolar) leads.
Characteristic findings in varied leads are associated with
different disease entities, and clinicians quickly become adept
at knowing which leads to focus on when they suspect a
certain pathophysiological process.
Although each lead relays information concerning a
specific portion of the heart, lead aVR, an augmented
unipolar limb lead placed on the lateral aspect of the right
arm, is often overlooked. Although the tracing in this lead
can be used by clinicians to obtain information from the
right upper portion of the heart, including the outflow tract
of the right ventricle and the basal portion of the septum,
many practitioners instead view lead aVR as giving
reciprocal information as to that which is derived from
0735-6757/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.ajem.2006.05.013
* Corresponding author. Department of Emergency Medicine, School
of Medicine, University of Virginia, Charlottesville, VA, USA.
E-mail address: [email protected] (W.J. Brady).
American Journal of Emergency Medicine (2006) 24, 864–874
www.elsevier.com/locate/ajem

leads aVL, II, V5, and V6, choosing therefore to use it
solely to ensure the correct placement of the other eleven
leads [1]. It is important for clinicians to use lead aVR as a
potentially important segment of the ECG in certain clinical
presentations; lead aVR should not be considered the
bforgottenQ lead. Four specific findings in lead aVR
especially worthy of discussion are ST-segment elevation
as an indicator of significant left main coronary artery
(LMCA) involvement in acute coronary syndromes, PR-
segment elevation in acute cases of pericarditis, RV wave in
tricyclic antidepressant (TCA) poisoning, and ST-segment
elevation suggestive of atrioventricular reciprocating tachy-
cardia (AVRT) in preexcitation syndromes. This review will
focus on the abnormalities in lead aVR as encountered in
these clinical situations.
2. Case presentations
2.1. Case 1
A 44-year-old man with a history of myocardial infarc-tion, hypertension, and diabetes mellitus presented to theemergency department (ED) with left shoulder pain. An ECG(Fig. 1) demonstrated sinus rhythm with ST-segment
Fig. 1 Case 1 (anterior wall STEMI with LMCA obstruction)—12-lead ECG with ST-segment elevation in leads V1 to V4 and ST-segment
depression in the inferior leads. Also note the ST-segment elevation in lead aVR, a finding that is strongly suggestive of LMCA obstructionas the cause of the anterior wall STEMI. Reprinted with permission from Mattu A, Brady WJ: ECGs for the Emergency Physician. BMJPublishing, London, 2004, pg 101.
Fig. 2 Case 2 (acute pericarditis)—12-lead ECG with ST-segment elevation in leads V1 to V6 and leads II, III, and aVF. Also note thePR-segment depression in leads II, III, and aVF as well as leads V4 to V6. A review of lead aVR reveals easily seen PR-segment elevation, afinding strongly suggestive of acute pericarditis.
Electrocardiographic applications of lead aVR 865

elevation in leads V1 to V4 with reciprocal ST-segmentdepression in the inferior leads; these findings wereconsistent with anterior wall ST-segment elevation AMI(STEMI). Also of note is the ST-segment elevation in leadaVR, a finding suggestive of LMCA obstruction. Because ofthe suspected left main lesion, the patient was transferred to anearby hospital with interventional capability. The patientwas taken to the catheterization laboratory where an LMCAocclusion with thrombus was noted. Urgent surgical consul-tation resulted in coronary artery bypass grafting (CABG).
2.2. Case 2
A 39-year-old man without medical history presented tothe ED with pain in the left side of the chest. The pain hadappeared approximately 2 days before arrival in the ED andwas worsened upon inspiration, assuming the supineposition, and with upper extremity movement; no associatedsymptoms were noted. The patient had recently experiencedan upper respiratory tract infection. The physical examina-tion was normal; no chest wall tenderness was found. A12-lead ECG (Fig. 2) revealed diffuse ST-segment elevationin leads V2 to V6, II, III, and aVF; PR-segment depression isalso seen in anterior and inferior leads. PR-segmentelevation is also seen in lead aVR. The patient’s painlessened considerably by treatment with a nonsteroidalantiinflammatory agent and morphine sulfate. The patientunderwent echocardiographic examination, which revealeda small pericardial effusion. The patient was admitted to theCardiology service for a 24-hour observation and dis-charged without incident. No etiology was discovered forthe pericarditis; an infectious etiology was suspected basedupon his recent upper respiratory tract infection symptoms.
2.3. Case 3
A 37-year-old female patient was transported to the EDby emergency medical services. The patient was last seenapproximately 4 hours before presentation; she was foundunresponsive in her bed. On arrival in the ED, the patientwas lethargic; the examination revealed an anticholinergictoxidrome. The 12-lead ECG (Fig. 3) revealed sinustachycardia with minimal QRS complex widening; a largeRV wave is also seen in lead aVR. Based on the patient’santicholinergic physical examination features and theelectrocardiographic findings, the possibility of TCAingestion was raised. The patient was orotracheally intu-bated; she received intravenous sodium bicarbonate andcharcoal via the orogastric tube. Upon further review, hermedical history was remarkable for depression complicatedby previous suicide attempts; she was managed withamitriptyline. The patient was extubated on the thirdhospital day and discharged to a psychiatric facility with adiagnosis of TCA overdose.
Fig. 3 Case 3 (TCA ingestion)—12-lead ECG with a sinus tachycardia characterized by a widened QRS complex, deep S wave in lead I,and prominent R wave in lead aVR. These findings are consistent with cardiotoxicity resulting from TCA ingestion. Reprinted with
permission from Mattu A, Brady WJ: ECGs for the Emergency Physician. BMJ Publishing, London, 2004, pg 110.
Table 1 Electrocardiographic findings of potential clinical
significance in lead aVR
LMCA obstruction
ST-segment elevation greater than 1.5 mVAcute pericarditis
PR-segment elevation
Acute TCA poisoning
Prominent RVwaveWPW-related narrow complex tachycardia
ST-segment elevation
K. Williamson et al.866
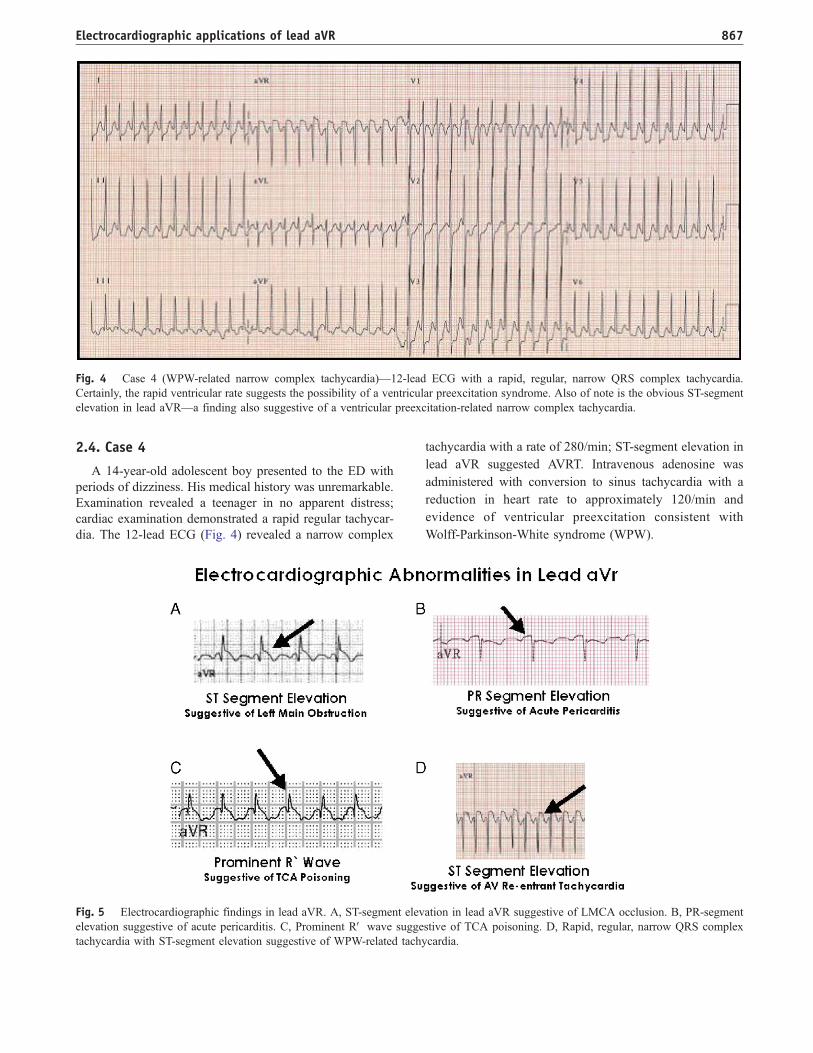
2.4. Case 4
A 14-year-old adolescent boy presented to the ED withperiods of dizziness. His medical history was unremarkable.Examination revealed a teenager in no apparent distress;cardiac examination demonstrated a rapid regular tachycar-dia. The 12-lead ECG (Fig. 4) revealed a narrow complex
tachycardia with a rate of 280/min; ST-segment elevation in
lead aVR suggested AVRT. Intravenous adenosine was
administered with conversion to sinus tachycardia with a
reduction in heart rate to approximately 120/min and
evidence of ventricular preexcitation consistent with
Wolff-Parkinson-White syndrome (WPW).
Fig. 4 Case 4 (WPW-related narrow complex tachycardia)—12-lead ECG with a rapid, regular, narrow QRS complex tachycardia.Certainly, the rapid ventricular rate suggests the possibility of a ventricular preexcitation syndrome. Also of note is the obvious ST-segmentelevation in lead aVR—a finding also suggestive of a ventricular preexcitation-related narrow complex tachycardia.
Fig. 5 Electrocardiographic findings in lead aVR. A, ST-segment elevation in lead aVR suggestive of LMCA occlusion. B, PR-segmentelevation suggestive of acute pericarditis. C, Prominent RV wave suggestive of TCA poisoning. D, Rapid, regular, narrow QRS complextachycardia with ST-segment elevation suggestive of WPW-related tachycardia.
Electrocardiographic applications of lead aVR 867
3. Discussion
Lead aVR is an electrocardiographic lead that isfrequently ignored. Many clinicians consider lead aVR as abplace holderQ in the upper tier of electrocardiographiclead tracings on the 12-lead ECG; in fact, the 11-lead ECGconcept has been proposed. In this report, we discuss thefindings in lead aVR, which are potentially of value (Fig. 5),including ST-segment elevation in the patient with acutecoronary syndrome (ACS) suggestive of LMCA occlusion(Fig. 5A), PR-segment elevation in the patient with acute
pericarditis (Fig. 5B), prominent R wave in the patient withsignificant TCA poisoning (Fig. 5C), and ST-segmentelevation in narrow complex tachycardia suggestive ofWolff-Parkinson-White syndrome (Fig. 5D; Table 1).
3.1. Acute coronary syndromes resulting from leftmain coronary obstruction
Acute myocardial infarction is diagnosed when patientsexperience 2 of the 3 following World Health Organizationcriteria: clinical history compatible with an ACS, electro-
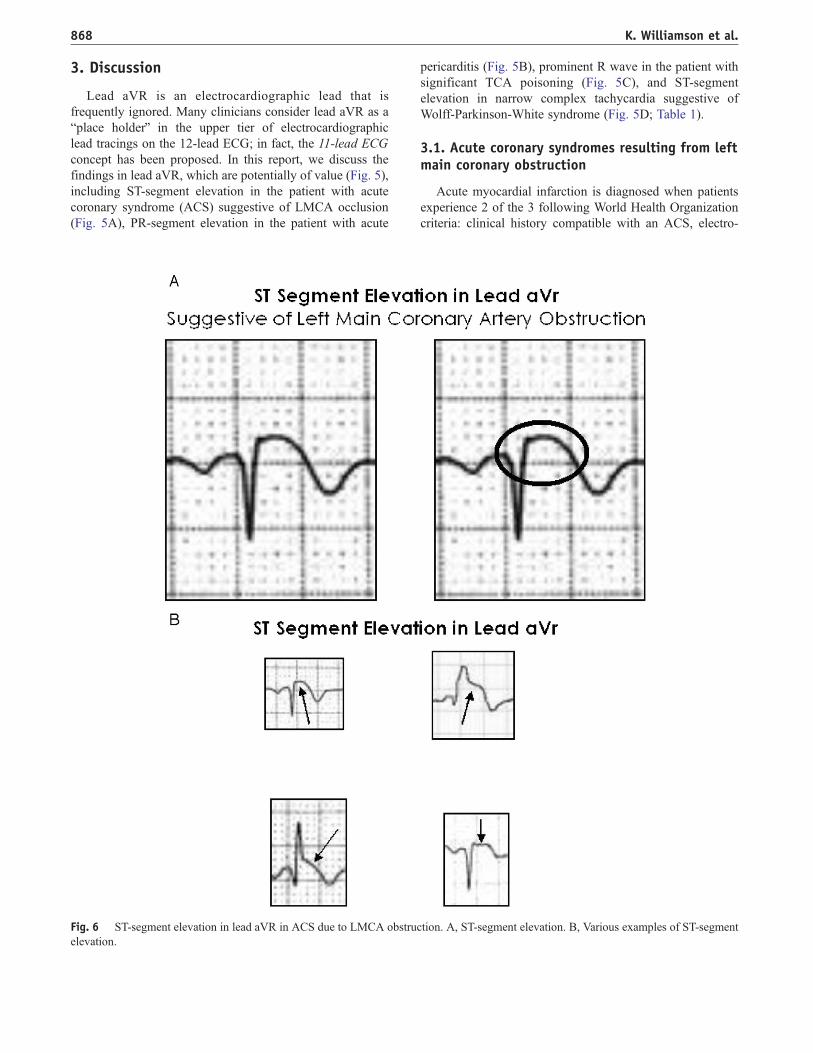
Fig. 6 ST-segment elevation in lead aVR in ACS due to LMCA obstruction. A, ST-segment elevation. B, Various examples of ST-segmentelevation.
K. Williamson et al.868

cardiographic abnormality suggestive of ACS, and positivemyocardial serum changes [2]. The rapid diagnosis of suchevents is critical to guiding early intervention andappropriate disposition in many patients with ACS.Electrocardiography is an appropriate bedside tool used inthe ED to make a rapid diagnosis of ACS, allowingphysicians to select appropriate therapy and to predictpotential cardiovascular complications. Patients withSTEMI are potential candidates for fibrinolysis or percu-taneous coronary intervention. Certain coronary arteryobstruction patterns are more appropriately managed withmechanical reperfusion therapies, such as percutaneouscoronary intervention or CABG; in particular, STEMIresulting from LMCA obstruction is associated with a veryhigh mortality rate and is most appropriately managed withstrategies other than fibrinolysis. In fact, STEMI resultingfrom an LMCA obstruction is associated with a significantmorbidity rate if managed with fibrinolysis, because thesepatients often require CABG shortly after their presentationand already have received fibrinolysis that increases theirsurgery complication rate [3].
The ability to discriminate among the various coronaryartery obstruction patterns may influence early managementdecisions; thus, the ability to identify left main STEMIpresentations is important. One such electrocardiographicpattern involves ST-segment elevation in lead aVR (Figs 1,5A, and 6)—it is theorized that this pattern of elevation isassociated with LMCA obstruction. In pursuit of this goal,Yamaji et al [4] attempted to determine the ECG features ofacute LMCA in the patient with ACS. The ECGs of86 consecutive patients who experienced ACS wereanalyzed. Sixteen patients experienced LMCA obstruction,46 patients experienced obstruction of the left anteriordescending artery, and the final 24 patients were diagnosedwith right coronary artery obstruction. In this study group,Yamaji noted the relationship between acute LMCAobstruction and ST-segment elevation greater than 0.05 mVin lead aVR. This electrocardiographic finding was presentin 88% of patients with LMCA obstruction, as opposed to43% of patients with left anterior descending obstruction,and 8% of patients with right coronary artery obstructions.From the study, the sensitivity of ST-segment elevation inlead aVR for predicting LMCA obstruction was determinedto be 81% and the specificity to be 80%.
Rostoff et al [5] continued this line of investigation in astudy that examined the relationship between ST-segmentelevation in lead aVR and significant obstruction of theLMCA. The study population consisted of 150 consecutivepatients who presented with ACS, of whom 46 were laterdetermined to have LMCA involvement, whereas the other104 patients experienced involvement of a different vessel.Upon retrospective analysis of their admitting ECG, Rost-off determined that the ST-segment elevation in lead aVRwas 2 times more common in the patient population withLMCA involvement (69.6%), as opposed to those withinvolvement of a different vessel (34.6%).
Kosuge et al [6] undertook a similar study to identify anearly, simple, and noninvasive predictor of LMCA or3-vessel disease in patients presenting with ACS. He per-formed a retrospective analysis of the ECGs of 310 patientsdiagnosed with non–ST-segment elevation ACS who laterunderwent coronary angiography. Multivariate analysis ofthe ECG findings determined ST-segment elevation greaterthan 0.5 mm in lead aVR to be the strongest predictor ofLMCA or 3-vessel disease, superior to the presence of ST-segment depression in other leads. Statistical analysis ofthis finding revealed a sensitivity of 78%, a specificity of86%, a positive predictive value of 57%, and a negativepredictive value of 95%. This reasonably high sensitivityallows the clinician to brule-inQ LMCA in the ACS patientwith lead aVR abnormality.
In addition to aiding in the diagnosis of LMCAinvolvement in patients presenting with acute coronarysyndromes, the finding of ST-segment elevation in leadaVR also has prognostic significance. In his second studyon the topic, Kosuge et al [7] examined the admissionECGs and biochemical markers of 333 patients withdiagnosed non-AMI acute coronary syndromes. AlthoughKosuge studied numerous ECG findings and a varietybiochemical markers, only ST-segment elevation greaterthan 0.5 mm in lead aVR on the admission ECG andelevated troponin T levels were determined to be inde-pendent predictors of adverse clinical events at 90 days,with an odds ratio of 13.8 and 7.9, respectively. Patientswith ST-segment elevation in lead aVR and elevatedtroponin T levels were also determined to have the highestrates of both LMCA or 3-vessel disease and 90-day ad-verse outcome (62% and 47%, respectively). This conclu-sion that ST-segment elevation in lead aVR on admissionECG was the strongest predictor of adverse outcomes at90 days in patients with non-AMI ACS, combined withits relation to LMCA or 3-vessel disease, highlights thediagnostic and prognostic significance of this electrocar-diographic finding.
Additional prognostic information is obtained from leadaVR electrocardiographic presentations, as noted by thework of Barrabes et al [8]. Barrabes examined theprognostic significance of this finding by studying theinitial ECG in 775 consecutive patients admitted with theirfirst non-AMI ACS event. Barrabes found that in-hospitalmortality increased in a stepwise fashion across increasingincrements of ST-segment elevation in lead aVR. Of thestudy population of 775 patients, only 1.3% of the 525patients without ST-segment elevation in lead aVR died,whereas 8.6% of the 116 patients with 0.05 to 0.1 mV ofelevation died, and 19.4% of the 134 patients with greaterthan 0.1 mV elevation died. The odds ratio for death withthe 2 varying degrees of ST-segment elevation was 4.2 and6.6. Upon multivariate analysis, ST-segment elevation inlead aVR was the only variable from the initial ECG thatwas strongly associated with in-hospital recurrent ischemicevents and heart failure, and was retained as an indepen-
Electrocardiographic applications of lead aVR 869

dent predictor of death. Barrabes therefore concluded thatthe poorer outcomes in these patients should influencephysicians to seek an early invasive approach in thetreatment of patients with these ominous electrocardio-graphic findings.
Thus, ST-segment elevation in lead aVR in the patientwith clinically suspected ACS suggests a strong possibilityof LMCA obstruction. This finding is important in thatsuch obstruction is associated with a markedly highermortality rate and may be more amenable to mechanical
Fig. 7 PR-segment elevation in lead aVR suggestive of acute pericarditis. A, PR-segment elevation. B, Various examples of PR-segmentelevation.
K. Williamson et al.870

reperfusion strategies rather than fibrinolysis. Furthermore,such electrocardiographic finding is associated with signif-icant risk of short-term adverse event.
3.2. Acute pericarditis
Lead aVR can also be used in the patient with suspected
acute pericarditis. Two electrocardiographic findings in this
lead are of diagnostic significance, including reciprocal ST-segment depression and PR-segment elevation. Acutepericarditis, a diffuse inflammation of the pericardial sacand superficial myocardium, has a number of underlyingcauses, including infection (primarily viral), immunologicdisorders, uremia, trauma, malignancy, cardiac ischemia,and AMI. The ECG is a useful diagnostic study in theevaluation of the patient with suspected pericarditis,because it is abnormal in 90% of cases, with the changesreflecting superficial endomyocardial inflammation. Pa-tients with acute pericarditis may manifest a range ofelectrocardiographic abnormalities, including ST-segmentelevation and depression, T-wave inversion, and PR-segment changes, to name the most common findings. Inparticular, lead aVR can demonstrate 2 particular findingsthat can suggest the diagnosis, including ST-segmentdepression and PR-segment elevation (Figs. 2, 5B, and 7).
The commonly encountered electrocardiographic abnor-malities in pericarditis are divided into 4 stages. Stage 1 isthe most characteristic of the disease process and consists ofST-segment elevation of upward concavity in almost allleads plus corresponding ST depression in a concavitypattern in lead aVR. Stage 2 involves the return of STsegments to baseline and a decrease in the T-waveamplitude. PR-segment deviations are also common in thisstage. In stage 3, the polarity of the T-wave changes withT-wave inversion was observed. Finally, stage 4 is theresolution of the abnormal electrocardiographic findings.Patients do not necessarily progress through these stages inan orderly fashion, nor does every patient have all, or evenany, of these findings. In addition, an electrocardiographicfinding of diagnostic significance that has not traditionallybeen included in the abovementioned stages is that of PR-segment elevation in lead aVR [9].
Abnormalities in lead aVR do not infrequently lead theclinician through the electrocardiographic evaluation, pro-viding clinical information establishing the correct diagno-sis. Numerous case histories illustrate this point well. Forinstance, Chew and Lim [10] discusses a case of a 25-year-old man with fever and chest pain; the 12-lead ECGrevealed diffuse concave ST-segment elevation, alongwith PR-segment depression in leads II, V5, and V6, and
Fig. 8 Prominent RV wave in lead aVR suggestive of TCA cardiotoxicity. A, Prominent RV wave. B, Various examples of prominentRV wave.
Electrocardiographic applications of lead aVR 871

PR-segment elevation in lead aVR. In another example,Sunkureddi et al [11] describes the case of a 39-year-oldman with a history of transient ischemic attack, presentingwith chest pressure. The ECG revealed ST-segmentelevation in leads I, V5, and V6, concerning for a possibleacute lateral wall myocardial infarction—yet, PR-segmentelevation in lead aVR was also noted, which stronglysuggested the correct diagnosis of acute myopericarditis.Finally, a report by Kristinsson et al [12] reviews thepresentation of a 9-year-old child with chest pain. An ECGat that time revealed PR-segment depression in lead II withreciprocal PR-segment elevation in lead aVR as the onlyabnormalities; these findings suggested the correct diagno-sis of pericarditis.
In a thorough review of the ECG in the patient suspec-ted of myopericarditis, Spodick [9] studied the ECGs of50 consecutive patients with unequivocal clinical evidenceof acute pericarditis. Although ST-segment deviations havebeen considered to be characteristic of acute pericarditis,Spodick determined that transient deviations of PR seg-ments occurred in 82% of patients, concluding that PRsegment shifts are characteristic of the syndrome. Spodicknoted that PR-segment elevation in lead aVR, likelyrepresentative of subepicardial atrial injury secondary topericardial inflammation, is ubiquitous and characteristic ofacute pericarditis, as are ST-segment deviations.
3.3. Tricyclic antidepressant ingestion
In addition to the utility of ST-segment elevation in leadaVR for diagnosing acute coronary syndromes and acutepericarditis, there are specific findings in lead aVR thatsuggest the diagnosis of TCA poisoning. The presentationof significant TCA ingestion is often nonspecific, withmental status abnormality as the primary initial finding; theECG can reveal sinus tachycardia with QRS complexabnormality, including widening and changes in theterminal portion in leads I (deep S wave) and aVR(prominent R wave; Figs. 3, 5C, and 8). Although TCAswere previously the mainstay of pharmacotherapy formajor depression, their use has now largely been replacedby that of selective serotonin reuptake inhibitors [13]. Yet,TCA poisoning remains a leading cause of morbidity andmortality involving pharmaceutical overdoses. In fact,TCAs were the second leading cause of medicationoverdose leading to death, as reported to the US poisoncenters in 1999 [14].
The ECG is an accessible, inexpensive, noninvasivebedside tool in the assessment of suspected TCA overdose,because electrocardiographic change typically precedes thedevelopment of clinically apparent neurologic and cardiactoxicity. Early electrocardiographic findings in tricyclicoverdose include sinus tachycardia, QRS complex wideninggreater than 100 milliseconds, right axis deviation of 1308to 1708, and characteristic R-wave changes in lead aVR(Figs. 3, 5C, and 8). The R wave changes in lead aVR that
are indicative of tricyclic poisoning include an increasedamplitude of the terminal R wave and an increased R waveto S wave ratio [15].
Individual case histories illustrate the use of the ECG inpatients with significant TCA ingestion, including abnor-malities in lead aVR. In one such presentation, Singh et al[15] reports a case in which electrocardiographic changeswere used as a guide to determine the severity of TCApoisoning. The report describes a 63-year-old man withaltered mental status who presented to the ED withphysical findings indicative of anticholinergic toxicity.The initial ECG revealed a widened QRS complex of140 milliseconds, a right axis deviation of 1008, and aprolonged QTc interval of 496 milliseconds. The ECGrepeated 1 hour later revealed the additional finding of aprominent R wave in lead aVR, with an R wave to S waveratio greater than 1.0. The ECG, interpreted within thispresentation, strongly suggested TCA poisoning. A secondhistory further illustrates the use of the ECG in these illpatients. McKinney and Rasmussen [14] present the casereport of a 29-year-old woman who presented comatose tothe ED 90 minutes after ingesting nortriptyline. The patientwas hypotensive on presentation with an ECG showing asinus tachycardia of 132 bpm, a QRS complex duration of124 milliseconds, a prolonged QTc interval of 586 milli-seconds, and a prominent RV wave in lead aVR. TheseECG abnormalities were resolved within a day and thepatient experienced a favorable outcome.
Liebelt et al [16] published a study in 1995 thatcompared QRS complex widening, a finding correlated tothe diagnosis of TCA poisoning, with measurements of theR wave in lead aVR. Liebelt performed this investigation todetermine which initial ECG findings most reliably identi-fied the patient with significant cardiac (ventricular arrhyth-mias) and neurologic (seizures) toxicities. The study was aprospective cohort series of 79 patients who presentedwithin 24 hours of TCA overdose; 16 patients ultimatelyexperienced seizure, whereas 5 individuals had arrhythmia.On the initial ECG, Liebelt examined the maximal QRScomplex width in a limb lead, along with the amplitude ofthe terminal R wave and the R wave to S wave ratio in leadaVR. Multiple logistic regression analysis demonstrated thatR wave amplitude greater than 3 mm in lead aVR was theonly electrocardiographic variable that could reliably beused to predict neurologic or cardiac toxicity. The R wave inlead aVR had an average measurement of 4.4 mm inpatients who experienced either seizure or arrhythmia, asopposed to an average of 1.8 mm in those patients who didnot experience these adverse events; the R wave to S waveratio was 1.4 in significantly poisoned patients comparedwith those individuals without severe adverse effect with aratio of 0.5. As a predictor of severe TCA poisoning, thesensitivity of the R wave greater than 3 mm in lead aVR was81% and that of R/S wave ratio greater than 0.7 was 75%,compared with an 82% sensitivity for QRS complex widthgreater than 100 milliseconds. The positive predictive value
K. Williamson et al.872

of the findings for significant toxicity in lead aVR was 43%and 46%, respectively, as opposed to 35% for a widenedQRS complex.
Buckley et al [17] examined the relationship betweenelectrocardiographic findings in psychotropic drug overdose
and the development of malignant arrhythmia. Buckleycompared 39 patients with TCA overdose or the antipsy-chotic thioridazine with 117 control subjects who overdosedon another substance. Buckley concluded that the frequentlyrecommended practice of using QRS complex widening
Fig. 9 Narrow QRS complex tachycardia with ST-segment elevation in lead aVR due to WPW-related tachycardia. A, ST-segmentelevation. B, Various examples of ST-segment elevation in the setting of narrow complex tachycardia.
Electrocardiographic applications of lead aVR 873

greater than 100 milliseconds as a predictor of adverseoutcomes after TCA overdose was not supported by his data.The electrocardiographic finding most strongly related to thedevelopment of an arrhythmia was, in fact, an R wave to Swave ratio greater than 0.7 in lead aVR; this electrocardio-graphic finding was found to have positive and negativepredictive values of 41% and 95%, respectively, for theprediction of significant toxicity.
3.4. Preexcitation syndrome-related narrowcomplex tachycardia
Perhaps one of the most widely accepted indications forobtaining an ECG is for the evaluation of active arrhythmia—the ECG not only provides the correct diagnosis ofdysrhythmia but also yields information regarding theetiology or substrate of the arrhythmia. One particulardysrhythmia is the narrow complex tachycardia encounteredin the WPW. The correct identification of this dysrhythmia—and its differentiation from other narrow complex tachycar-dias—certainly will impact not only the initial care of thepatient but also his/her subsequent management. In a report,Ho et al [18] reported that ST-segment elevation in lead aVR(Figs. 4, 5D, and 9) assists in the ultimate identification of themechanism of these narrow QRS complex tachycardias,including atrioventricular nodal reentrant tachycardia(AVNRT, ie, typical paroxysmal supraventricular tachycar-dia), AVRT (ie, WPW-related narrow complex tachycardia),and atrial tachycardia (AT). Ho studied 338 ECGs of patientspresenting with narrow complex tachycardia, of which 71%were AVRT, 31% were AVNRT, and 16% were AT, and thenanalyzed ST-segment changes in various leads. Logisticregression analysis revealed that ST-segment elevation inlead aVR was the only factor that reliably could be used todifferentiate among the various types of narrow complextachycardia. Atrioventricular reciprocating tachycardia(WPW-related tachycardia) was differentiated from AVNRTand ATwith a sensitivity of 71% and a specificity of 70%—ST-segment elevation in lead aVR was found to be stronglysuggestive of WPW-related narrow complex tachycardia.
4. Conclusion
Since its advent in the late 19th century, the ECG hasevolved into a clinical tool that provides valuable diagnosticinformation in a variety of settings. Althoughmany physiciansare attuned to the most characteristic electrocardiographicpatterns for common illnesses, it is important that the subtletiesof examining an ECG not be forgotten. It is especiallyimportant that lead aVR not be ignored as is common fashion,because it can provide essential diagnostic and prognosticinformation in a range of clinical presentations, as highlightedby the examples of LMCA disease, TCA poisoning, pericar-ditis, and WPW-related narrow complex tachycardia.
References
[1] Gorgels AP, Engelen DJM, Wellens HJJ. Lead aVR, a mostly ignored
but very valuable lead in clinical electrocardiography. J Am Coll
Cardiol 2001;38:1355-6.
[2] Alpert JS, Thygesen K, Antman E, et al. Myocardial infarction
redefined—a consensus document of The Joint European Society of
Cardiology/American College of Cardiology Committee for the
redefinition of myocardial infarction. J Am Coll Cardiol 2001;
36:959-69.
[3] Gaitonde RS, Sharma N, Ali-Hasan S, Miller JM, Jayachandran JV,
Kalaria VG. Prediction of significant left main coronary artery
stenosis by the 12-lead electrocardiogram in patients with rest angina
pectoris and the withholding of clopidogrel therapy. Am J Cardiol
2003;92:846 -8.
[4] Yamaji H, Iwasaki K, Kusachi S, et al. Prediction of acute left main
coronary artery obstruction by 12-lead electrocardiography. ST
segment elevation in lead aVR with less ST segment elevation in
lead V(1). J Am Coll Cardiol 2001;38:1348-54.
[5] Rostoff P, Piwowarska W, Konduracka E, Libionka A, Bobrowska-
Juszczuk M, Stopyra K, et al. Value of lead aVR in the detection of
significant left main coronary artery stenosis in acute coronary
syndrome. Kardiol Pol 2005;62:128-37.
[6] Kosuge M, Kimura K, Ishikawa T, et al. Predictors of left main or
three-vessel disease in patients who have acute coronary syn-
dromes with non–ST-segment elevation. Am J Cardiol 2005;95:
1366-9.
[7] Kosuge M, Kimura K, Ishikawa T. Combined prognostic utility of
ST segment in lead aVR and troponin T on admission in non-ST
segment elevation acute coronary syndromes. Am J Cardiol 2006;97:
334 -9.
[8] Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J.
Prognostic value of lead aVR in patients with a first non–ST-
segment elevation acute myocardial infarction. Circulation 2003;
108:814-9.
[9] Spodick DH. Diagnostic electrocardiographic sequences in acute
pericarditis. Significance of PR segment and PR vector changes.
Circulation 1973;48:575-80.
[10] Chew HC, Lim SH. Electrocardiographical case. ST elevation: is this
an infarct? Singapore Med J 2005;46:656.
[11] Sunkureddi PR, Gonzalez EB, Washington R, Salazar A, Douglass P.
A 39 year old man with sudden onset of chest pain. Cleve Clin J Med
2005;72:1050-6.
[12] Kristinsson G, Flynn P, Rapaport S, Snyder M, Kern JH. PR-segment
changes in childhood pericarditis. J Pediatr 2002;140:378.
[13] Van Mieghem C, Sabbe M, Knockaert D. The clinical value of the
ECG in noncardiac conditions. Chest 2004;125:1561 -76.
[14] McKinney PE, Rasmussen R. Reversal of severe tricyclic antidepres-
sant-induced cardiotoxicity with intravenous hypertonic saline solu-
tion. Ann Emerg Med 2003;42:20 -4.
[15] Singh N, Singh HK, Harinder K, Khan IA. Serial electrocardiographic
changes as a predictor of cardiovascular toxicity in acute tricyclic
antidepressant overdose. Am J Ther 2002;9:75-9.
[16] Liebelt EL, Francis PD, Woolf AD. ECG lead aVR versus QRS
interval in predicting seizures and arrhythmias in acute tricyclic
antidepressant toxicity. Ann Emerg Med 1995;26:195-201.
[17] Buckley NA, Chevalier S, Leditschke IA, et al. The limited utility of
electrocardiography variable used to predict arrhythmia in psychotro-
pic drug overdose. Crit Care 2003;7:101-7.
[18] Ho YL, Lin LY, Lin JL, et al. Usefulness of ST-segment ele-
vation in lead aVR during tachycardia for determining the mech-
anism of narrow QRS complex tachycardia. Am J Cardiol 2003;
92:1424-8.
K. Williamson et al.874