em array - interactive meeting technology
TRANSCRIPT
Introducing ARRAY OnQiPad technology and on-site service that bring
increased engagement, more participation
and a whole new “Wow Factor” to your events.

ARRAY OnQ runs on its own private network and server, so you won’t need to worry about unreliable and expensive hotel or venue Wi-Fi service. With ARRAY OnQ there are no issues with connectivity and all data and content are secure.
The data collected using ARRAY OnQ goes into our highly powerful and user-friendly data analysis software. You can filter data sets, look at all your programming or focus on one meeting and evaluate impact. The system also creates a summary by slide of notes taken, questions asked, and slide rating.
For over 10 years, EM has provided on-site technical service at over 5,000 events ranging in size from 10 people to 1,000.
We get it.
Welcome to ARRAY OnQ.Companies are being asked to improve interaction at their live events and collect quality data points to measure impact. Educational Measures developed ARRAY for this reason and we stand apart from our competitors because:
About EM
We develop and deploy event technolgies and top-end service for a wide variety of industries.
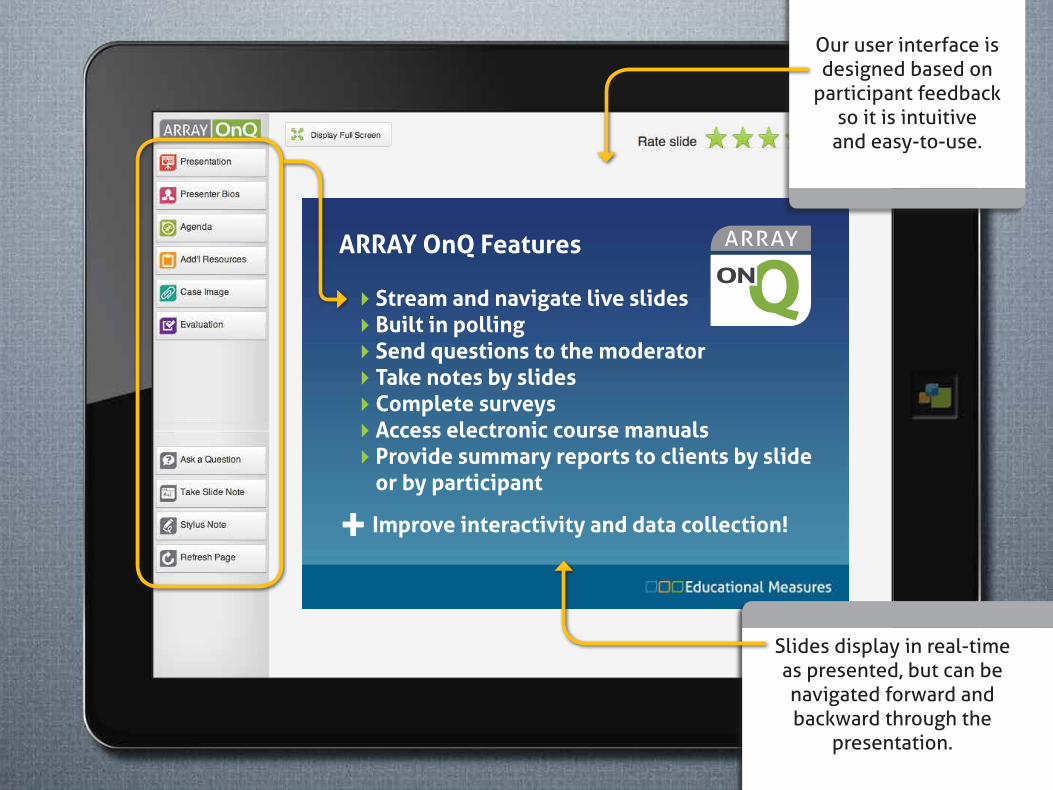
ARRAY OnQ Features
4Stream and navigate live slides4Built in polling4Send questions to the moderator4Take notes by slides4Complete surveys4Access electronic course manuals4�Provide summary reports to clients by slide
or by participant
+ Improve interactivity and data collection!
Our user interface is designed based on
participant feedback so it is intuitive
and easy-to-use.
Slides display in real-time as presented, but can be navigated forward and backward through the
presentation.
ARRAY OnQ Features
4Stream and navigate live slides4Built in polling4Send questions to the moderator4Take notes by slides4Complete surveys4Access electronic course manuals4�Provide summary reports to clients by slide
or by participant
+ Improve interactivity and data collection!
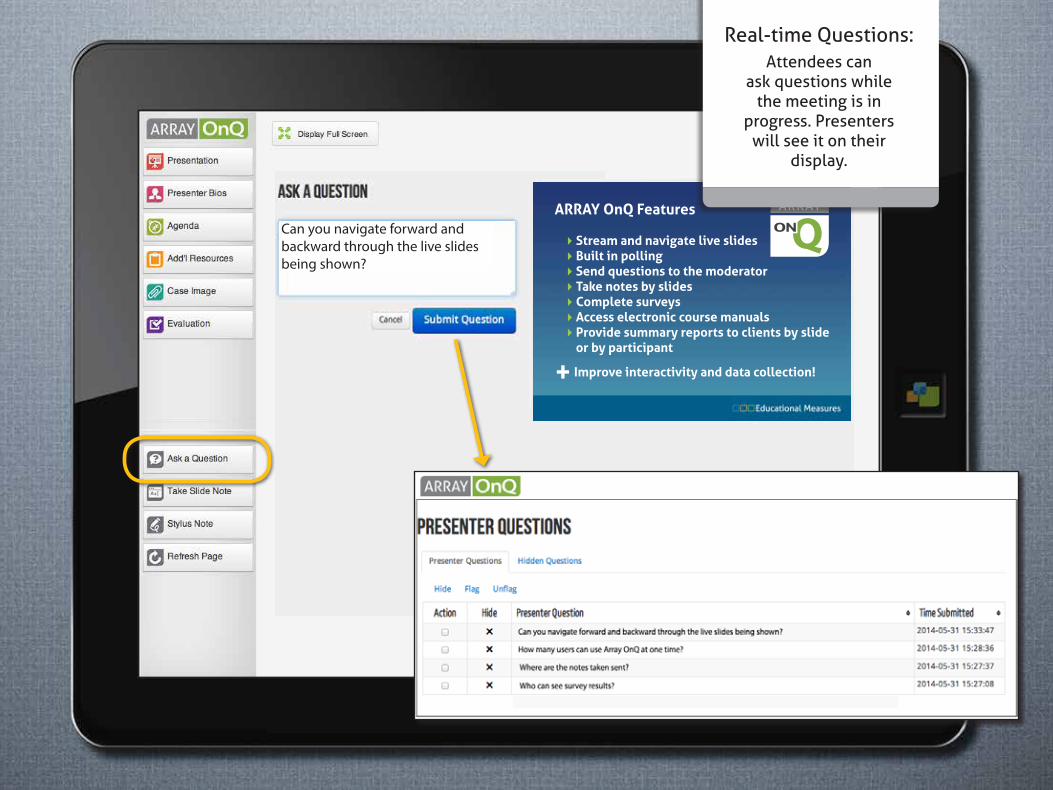
Can you navigate forward and backward through the live slides being shown?
Real-time Questions:Attendees can
ask questions whilethe meeting is in
progress. Presenterswill see it on their
display.
ARRAY OnQ Features
4Stream and navigate live slides4Built in polling4Send questions to the moderator4Take notes by slides4Complete surveys4Access electronic course manuals4�Provide summary reports to clients by slide
or by participant
+ Improve interactivity and data collection!
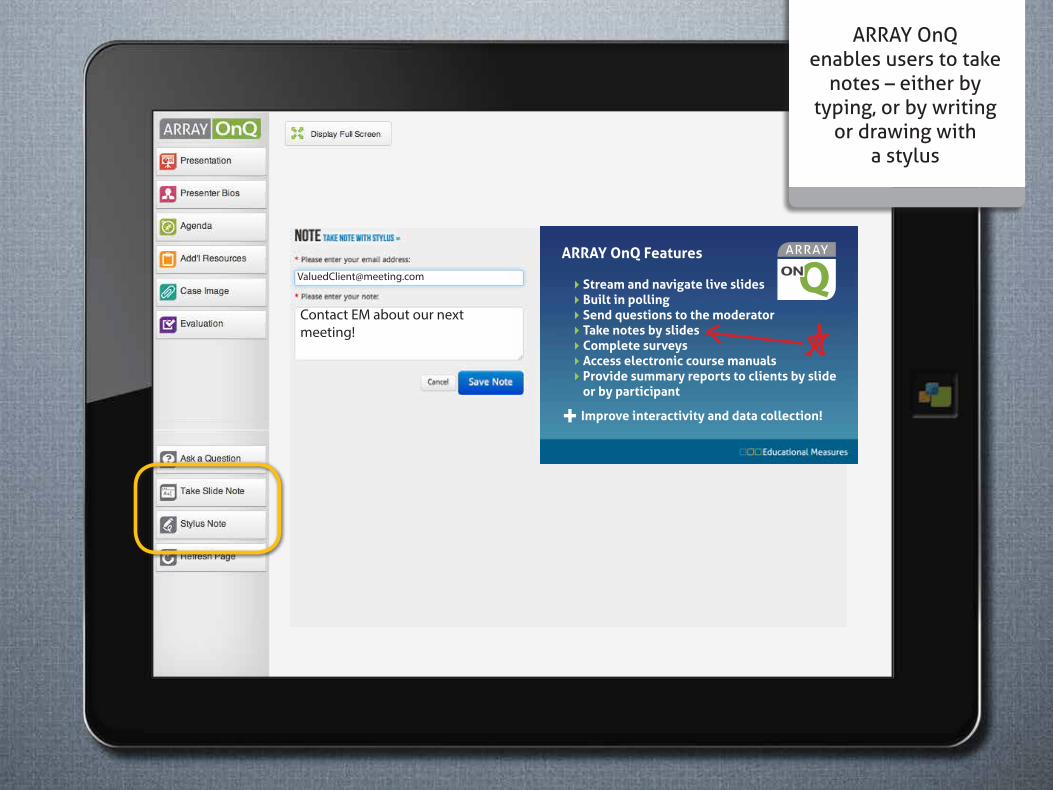
Contact EM about our next meeting!
ARRAY OnQenables users to take
notes – either bytyping, or by writing
or drawing with a stylus
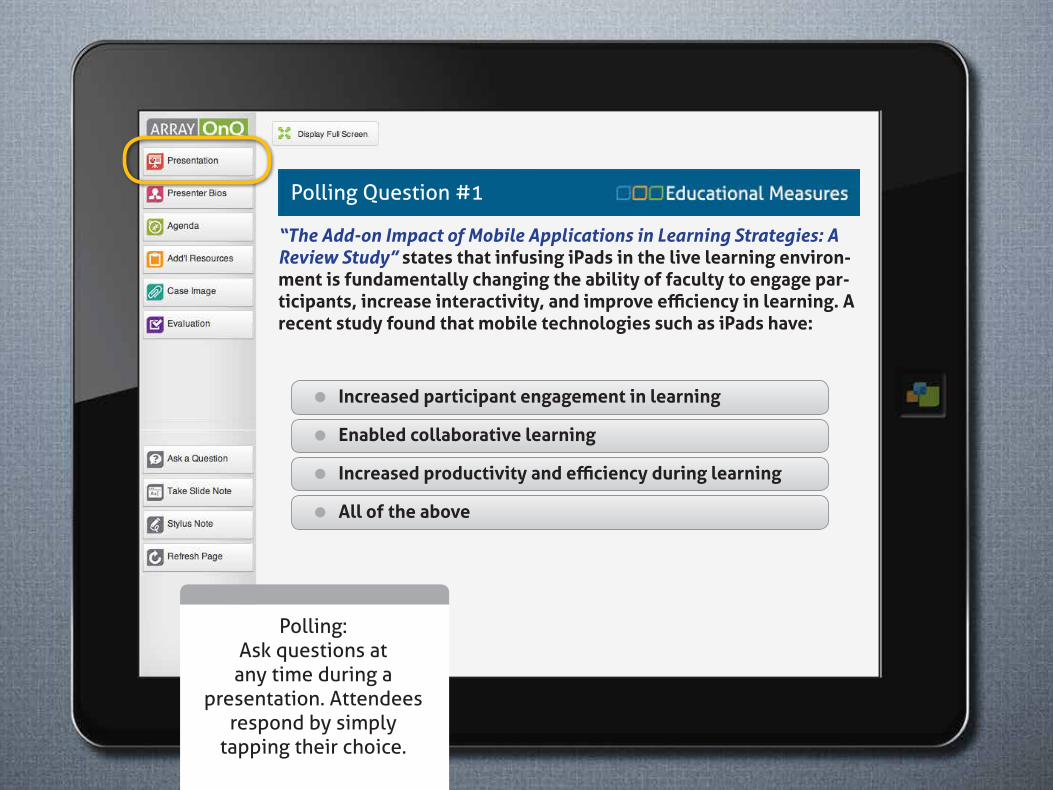
Polling:Ask questions at
any time during apresentation. Attendees
respond by simply tapping their choice.
“The Add-on Impact of Mobile Applications in Learning Strategies: A Review Study” states that infusing iPads in the live learning environ-ment is fundamentally changing the ability of faculty to engage par-ticipants, increase interactivity, and improve efficiency in learning. A recent study found that mobile technologies such as iPads have:
=�Increased participant engagement in learning
=�Enabled collaborative learning
=�Increased productivity and efficiency during learning
=�All of the above
Polling Question #1
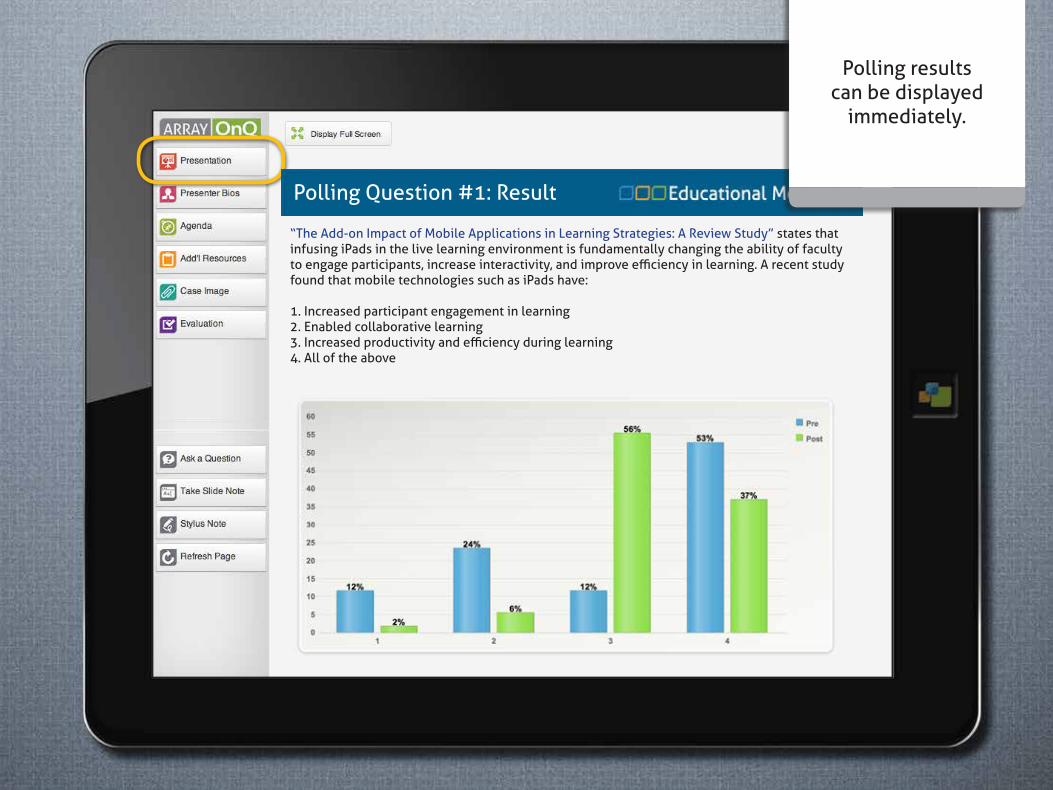
“The Add-on Impact of Mobile Applications in Learning Strategies: A Review Study” states that infusing iPads in the live learning environment is fundamentally changing the ability of faculty to engage participants, increase interactivity, and improve efficiency in learning. A recent study found that mobile technologies such as iPads have:
1. Increased participant engagement in learning2. Enabled collaborative learning3. Increased productivity and efficiency during learning4. All of the above
Polling results can be displayed
immediately.
Polling Question #1: Result
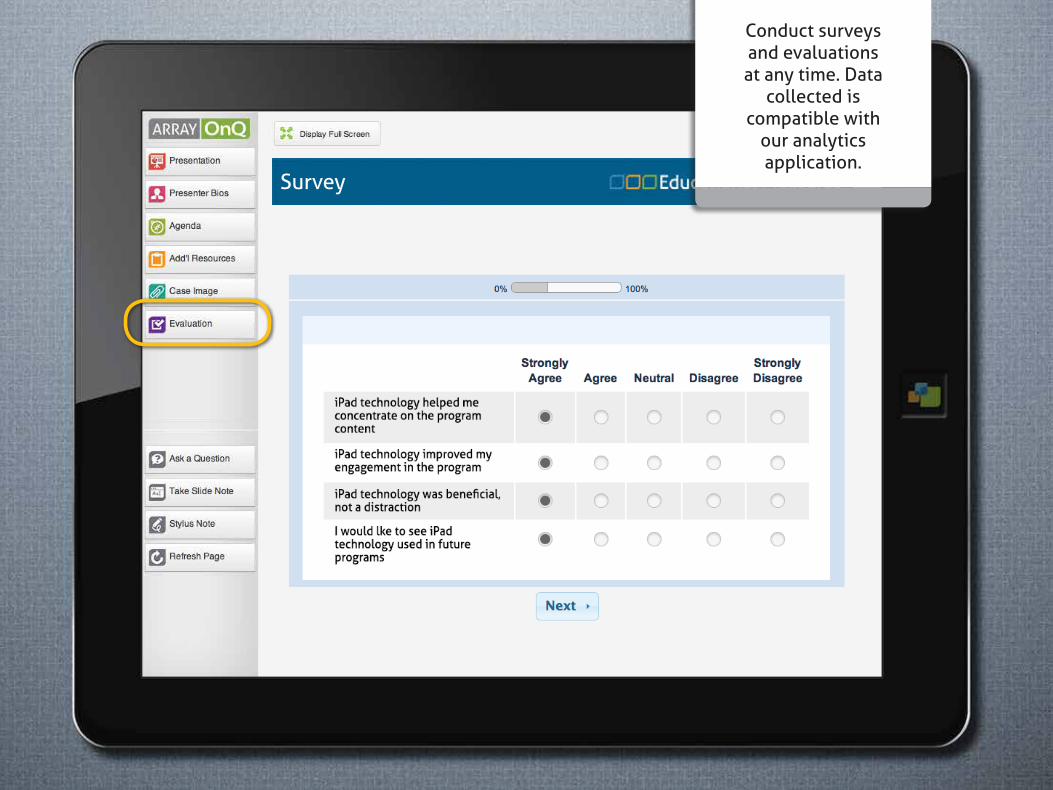
Conduct surveysand evaluationsat any time. Data
collected is compatible with
our analytics application.
Survey

Presenter Bios
Christina YiehScience DirectorTellent Labs, Inc.
Christina Yieh has been Science Director for Tellent Labs since 2011. Tellent is a world leader in microbiobial and genetic research with
over 20 years of funded experience, working closely with 11 major universities and research institutions.
Christina Yieh joined the company in 2008 and worked in a variety of positions in the US and in the UK. In 2009, she went to Paris, France as Science Development European Lead, manag-ing global research programs. She returned to New York in May 2011 as Science Director and since managed the development and launch of the division’s research paths.
Prior to joining Tellent, Yieh worked at PharMeta as a Science and lab lead. She received a Masters of Science from Columbia University, New York and a Bachelors degree in Biology from John Cabot International College in Rome, Italy.
Add allof your pertintent
meeting informationwith our flexible
tab system.

Participants canrate each slide andthe results can beviewed in the final
engagement report.
Tabs can be added and customized to
suit your needs.
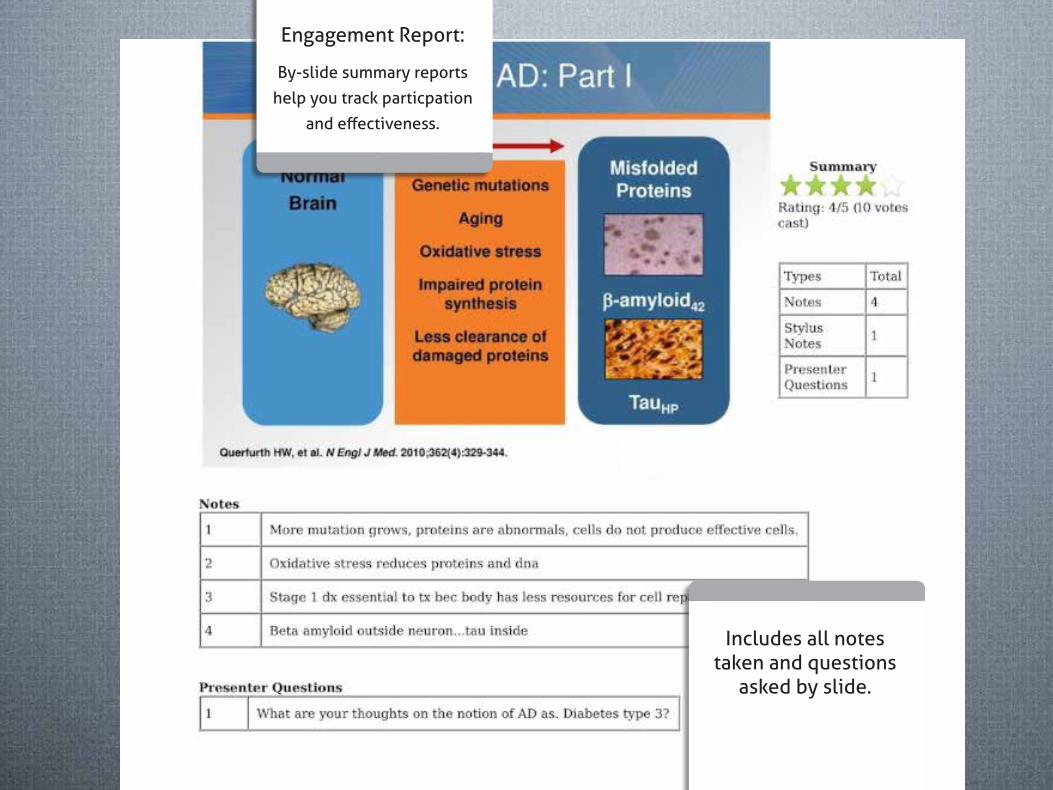
Engagement Report:
By-slide summary reports
help you track particpation
and effectiveness.
Includes all notes taken and questions
asked by slide.
Additional Reports:
ARRAY OnQ offers
you a wide range of
additional in-depth reports.
Generated by: Educational MeasuresOn: 06-‐21-‐2014
Presenter Question Report for the Activity: Review of the Presentations from the ASCO 2014 Annual MeetingPresenter Question Report for the Activity: Review of the Presentations from the ASCO 2014 Annual MeetingPresenter Question Report for the Activity: Review of the Presentations from the ASCO 2014 Annual MeetingPresenter Question Report for the Activity: Review of the Presentations from the ASCO 2014 Annual MeetingPresenter Question Report for the Activity: Review of the Presentations from the ASCO 2014 Annual Meeting
# Agenda Agenda_item Slide Deck E-‐Mail Created Question text3 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 10:47:49 So much excitement in myeloma when we will stop doing high doe chemo with transplant?4 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 10:53:53 Will a pt who has failed post transplant maintenance revlimid qualify for the anti cd38 trial?5 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:09:31 For pts with 17p del is Ibrutinib a reasonable option in the first line setting6 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:09:50 Do you consider gazyva as a first line standard of care now?7 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:11:20 Comment about ideally sib in cll8 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:11:57 Ibrutinib in myeloma?9 Agenda Morning 1130 Vij [email protected]‐06-‐21 11:12:36 How do you assess response to ibrutinib in CLL, especially in patients without lymphadenopathy? 10 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:13:12 In cll with 17p deletion will you combine ibrutinib with rituxan11 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:13:42 Heard about PTH PR. Not regular PTH causing huge hypercalcemia in CLL? I have a pt w/ stag. O CLL. Neg for cd38. 12 Agenda Morning 1130 Vij [email protected] 2014-‐06-‐21 11:20:09 Does the rituxan "clean" the circulating lymphocytes13 Agenda Morning TITLE SLIDE karl.king@ncmc-‐hospital.com2014-‐06-‐21 08:28:47 How to follow with PETi when CMS has limited a total of 3 PET per diagnosis per life time?14 Agenda Morning TITLE SLIDE [email protected] 2014-‐06-‐21 09:55:25 Is zytiga just a less toxic ketoconazole essentially?15 Agenda Morning TITLE SLIDE [email protected]‐06-‐21 09:56:23 What was the median age for trial combining taxotere and ADT.16 Agenda Morning 9:10 -‐ Carson [email protected] 2014-‐06-‐21 08:46:04 How do oncologists balance responsibility to individual patients vs responsible stewardship of healthcare costs or is that even the responsibility of the individual clinician?17 Agenda Morning 9:10 -‐ Carson [email protected] 2014-‐06-‐21 08:54:00 Comment re hospitalization of NSCLC patients: a lot get admitted for exacerbation of COPD. These patients may have had worse overall PS to begin with. Also, there was one study that showed overall there is a 3% improvement in OS all patients for each 10 further from center. That would reflect research pts. 18 Agenda Morning 9:10 -‐ Carson karl.king@ncmc-‐hospital.com2014-‐06-‐21 08:56:57 Abst. 6519: Is it possible that pts. on clinical trials are watched more closely than "real world pts." so most neutropenic fever are taken care of earlier?19 Agenda Morning 9:10 -‐ Carson [email protected] 2014-‐06-‐21 08:59:34 Could you comment on surveillance imaging on non small cell lung cancer, frequency and length of imaging, and CT vs PET??20 Agenda Morning 9:10 -‐ Carson karl.king@ncmc-‐hospital.com2014-‐06-‐21 09:00:33 Previous Asb. 8502 showed benefit for PET/CT for prediction of PRS & OS. Since CMS has limited a total PET of 3 per diagnosis per life time, any recommendation for the most effective way to follow lymphoma pts.? 21 Agenda Morning 9:10 -‐ Carson [email protected] 2014-‐06-‐21 09:03:15 How does Watson decide if those 12M pages are really valid or good studies? 22 Agenda Morning 9:10 -‐ Carson [email protected] 2014-‐06-‐21 09:04:44 Explosion of oncology meds, treatments -‐ I need Watson IBM Now, how do I sign up??23 Agenda Morning 9:10 -‐ Carson karl.king@ncmc-‐hospital.com2014-‐06-‐21 09:09:28 ASb. 6513: is it possible the 30% of stage III colon pts. Who did not receive FOLFOX x 12 due to surgical complications / bowel obstruction, those pts. Died of those complications & were not included in final analysis on. OS?24 Agenda Morning 8:30 -‐ Bartlett [email protected] 2014-‐06-‐21 07:53:17 What maintenance rituxan schedule do you recommend25 Agenda Morning 8:30 -‐ Bartlett [email protected] 2014-‐06-‐21 08:20:25 Do those FL patients with a positive PET reflect the possibility of some large cell components vs. just response to therapy? Re 850226 Agenda Morning 8:30 -‐ Bartlett [email protected]‐06-‐21 08:20:46 Does it mean that pet negative follicular lymphoma after induction does not need maintenance rituxan? 27 Agenda Morning 8:30 -‐ Bartlett [email protected] 2014-‐06-‐21 08:23:37 In pts with negative pet post tax, can you skip maintenance rituxan since OS better than PRIMA
28 Agenda Morning 9:50 -‐ Picus [email protected] 2014-‐06-‐21 09:21:30Is weekly taxotere is equally effective and better tolerated?
29 Agenda Morning 9:50 -‐ Picus [email protected] 2014-‐06-‐21 09:25:41 Will the early data on the use of taxotere in the first line setting in high volume disease change your clinical practice?30 Agenda Morning 9:50 -‐ Picus [email protected] 2014-‐06-‐21 09:48:26 Discordance between 12-‐core prostate biopsy and radical prostatectomy specimen. I have seen many radically removed prostates with a very tiny focus of cancer, localized. Why can't better technology, markers or something detect this physically isolated cancer, and prevent so many radical prostatectomies? How about microsurgery or immuno-‐chemo-‐DNA excision?
31 Agenda Afternoon 1540 Wartman karl.king@ncmc-‐hospital.com2014-‐06-‐21 15:27:29
I have a recent patient presented with diagnosis of "Sebaceous carcinoma" of the (R) facial/ mandibular area & "sebaceous adenoma" of abdominal wall area. He also has a family history strongly (+) for early colon cancer. We sent for genetic testing to rule out "Muir Torre Syndrome", but it was only remarkable for "pleomorphism".
(1) Please explain the prevalence of pleomorphism in the setting of Muir Torre syndrome;
(2) What is the clinical significance of "pleomorphism" for my patient & his family members?32 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:38:45 When we will use neuadjuvant folfox in locally advanced rectal cancer before chemo radiation?33 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:42:49 Should we be recommending multigene panels which many companies are marketing for hereditary cancers, given the ls pts carrying brca mutations?34 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:46:41 You make a case for resection of the primary tumor in CRC in the modern era. Shouldn't we do a randomized clinical trial?
35 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:47:33When to have surgery for primary in metastatic colon cancer .? Before chemo ?
36 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:49:05
Natural history of stage 4 colon cancer Surgery 7-‐8 monthsFu add 6 weeksiFL 17Folfox avast in 24-‐30 monthsHow can surgery patient will be longer?
37 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:55:20 EORTC 22921 concluded that adjuvant chemotherapy is unnecessary in patients with rectal cancer who received per operative chemo radiotherapy. Is there an explanation why the study you cited gave different results?38 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:56:17 What is maxim permissible time for starting adjuvant39 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 13:59:47 Isnt a 200 pt study underpowered to detect a difference in stage 2 colon pts for folfox, since recurrence rate is 6%40 Agenda Afternoon 2:00 -‐ Sorscher NEW [email protected] 2014-‐06-‐21 14:00:16 Stage2msi high oxali alone?41 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 11:59:14 It has been thought that immune therapy like ipilimumab is more effective when disease is present to prime the immune system, does the adjuvant data as total resection of disease make this unlikely?42 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 11:59:16 Do you think eortc 9008 should have used High dose IFN as standard arm instead of placebo against ipilimumab?43 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 12:00:43 Does Ipilimumab should replace interferon in adjuvant therapy of stage III melanoma ?44 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 12:03:28 What is the role of IL-‐2 in metastatic melanoma45 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 12:17:52 What is yours first, second, etc. line therapy for metastatic malignant melanoma? 46 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 12:22:10 Are kras and Nras mutations mutually exclusive?47 Agenda Afternoon 12:10 -‐ Linette [email protected] 2014-‐06-‐21 12:25:09 Still a role for chemo with carbo-‐taxol+Bev without braf mutation?48 Agenda Afternoon 1:20 -‐ Morgensztern NEW [email protected] 2014-‐06-‐21 12:38:47 Is Brazil going to win the World Cup?49 Agenda Afternoon 1:20 -‐ Morgensztern NEW [email protected] 2014-‐06-‐21 12:49:17 After this PCI study would you offer PCI?50 Agenda Afternoon 1:20 -‐ Morgensztern NEW karl.king@ncmc-‐hospital.com2014-‐06-‐21 12:51:26 PCI dose of 25 Gy in 10 fx. is too low . The radiobiological equivalent of only 30Gy with standard fractionation equivalent of 40Gy.51 Agenda Afternoon 1:20 -‐ Morgensztern NEW karl.king@ncmc-‐hospital.com2014-‐06-‐21 13:00:30 The CREST trial design is flawed because the radiation dose is inadequate! 30 Gy is only an adequate dose for a quick palliation. If one wants to truly evaluate the benefit for survival the radiobiological equivalent dose of at least 60 Gy using standard fractionation size of 2Gy ( as in RTOG). 60Gy/30 is radiobiologically equivalent to 45Gy/15 ( please refer to Turissi et al, International Journal of Radiation Oncology, Physics & Biology 1998).52 Agenda Afternoon 1:20 -‐ Morgensztern NEW [email protected] 2014-‐06-‐21 13:07:50 Does afatinib have activity in egfr mutant patients second line after erlotinib? How about in t790 mutants activity of afatinib?53 Agenda Afternoon 1:20 -‐ Morgensztern NEW [email protected] 2014-‐06-‐21 13:08:15 Management strategy for EGFR mutant patient progressing on Tarceva.
54 Agenda Afternoon 1:20 -‐ Morgensztern NEW [email protected] 2014-‐06-‐21 13:08:16For pts with t790m mutations, would you use the 3rd line agents in the upfront setting? If not available ,chemo or afatinib.
55 Agenda Afternoon 1:20 -‐ Morgensztern NEW karl.king@ncmc-‐hospital.com2014-‐06-‐21 13:14:40 The design of the trial is flawed. It should be to evaluate the extensive disease who has a CR after chemo radiation , not "any response". If patients have persistent disease in chest after chemo radiation , it is a "mute point" to worry about possible bone metastasis to consider PCI!56 Agenda Afternoon 1:20 -‐ Morgensztern NEW karl.king@ncmc-‐hospital.com2014-‐06-‐21 13:20:31 Dr. Morgen stern , if you want to ask a radiation oncology question, you should ask your Radiation Oncology colleagues at MIR. Radiation therapists are the technicians who operate on our linear accelerators, they are neither oncologist nor M.D.!57 Agenda Afternoon 3:00 Wang-‐Gillam karl.king@ncmc-‐hospital.com2014-‐06-‐21 14:49:48 I assume in the ARTIST trial the total dose of X rat is 4500 cGy not 45 cGy as on the side. Please correct.58 Agenda Afternoon 3:00 Wang-‐Gillam [email protected] 2014-‐06-‐21 14:55:11 What was the schedule and doses of the ruxolitinib when use Vs placebo?59 Agenda Afternoon 3:00 Wang-‐Gillam [email protected] 2014-‐06-‐21 14:56:34 What was the schedule and doses of the ruxolitinib when use Vs placebo? (Single agent)
Questions SubmittedAttendee RegistrationActivities used in this report:Activities used in this report:Activities used in this report:Activities used in this report:Review of the Presentations from the ASCO 2014 Annual MeetingReview of the Presentations from the ASCO 2014 Annual MeetingReview of the Presentations from the ASCO 2014 Annual MeetingReview of the Presentations from the ASCO 2014 Annual Meeting
Intervals used in this report:Intervals used in this report:Intervals used in this report:Intervals used in this report:PrePost
Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?Denes 1 - Which best describes your clinical practice?
Answer Pre Pre % Post Post %pure hematology (benign and malignant) 0 0 0 0mostly hematology with occasional solid tumors 5 11 0 0Mostly general solid tumor oncology with some hematology29 63 0 0General solid tumor oncology (more than 5 disease types)7 15 0 0Disease focused solid tumor oncology ( 5 disease types or less)5 11 0 0Total 46 100% 0 100%
Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?Denes 2 - Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?
Answer Pre Pre % Post Post %The number of new agents is overwhelming and I cannot keep up with the new agents11 23 0 0The number of new agents is challenging but I feel comfortable and use all of them21 45 0 0The number of new agents is challenging, so I have limited my use to a few selected agents15 32 0 0Total 47 100% 0 100%
Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?Denes 3 - How have you incorporated immune modulating agents into your practice?
Answer Pre Pre % Post Post %I feel comfortable with them and have used them in my practice31 66 0 0I feel comfortable with them but prefer not to use them in my practice4 9 0 0I do not feel comfortable with them and do not use them in my practice12 26 0 0Total 47 100% 0 100%
Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?Denes 4 - You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with extensive lung, liver , and bone metastases. Which of the following would you recommend?
Answer Pre Pre % Post Post %Single agent ipilimumab 6 13 0 0Single agent vemurafenib 9 19 0 0Combination of trametinib and dabrafenib 11 23 0 0Combination of ipilumumab and vemurafenib 3 6 0 0Refer patient to melanoma expert for management19 40 0 0Total 48 100% 0 100%
Denes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIADenes 5 - How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIA
Answer Pre Pre % Post Post %I would be comfortable in recommending a treatment plan26 54 0 0I would discuss the case with a Lymphoma expert and follow the expert’s recommendation8 17 0 0I would refer the patient to a lymphoma expert for evaluation and then treat in my office3 6 0 0I would refer the patient to a lymphoma expert for evaluation and treatment11 23 0 0Total 48 100% 0 100%
Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?Denes 6 - You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr-able positive CML. How would you manage this patient?
Answer Pre Pre % Post Post %I would be comfortable in recommending a treatment plan33 70 0 0I would discuss the case with a leukemia expert and follow the expert’s recommendation1 2 0 0I would refer the patient to a leukemia expert for evaluation and then treat in my office0 0 0 0I would refer the patient to a leukemia expert for evaluation and treatment13 28 0 0Total 47 100% 0 100%
Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?Denes 7 - A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How would you manage this patient?
Answer Pre Pre % Post Post %I would be comfortable in formulating and administering a treatment plan26 55 0 0I would discuss the case with a GU oncology expert and follow the expert’s recommendation8 17 0 0I would refer the patient to a GU oncology expert for evaluation and then treat in my office1 2 0 0I would refer the patient to a local GU oncology expert for evaluation and treatment10 21 0 0I would refer the patient to the University of Indiana for evaluation and treatment2 4 0 0Total 47 100% 0 100%
Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?Denes 8 - How often do you include a platinum analogue in first line therapy of TNBC?
Answer Pre Pre % Post Post %Usually or almost always 11 28 0 0Only in a few selected patients 14 35 0 0I usually reserve it for 2nd line and beyond 15 38 0 0Total 40 100% 0 100%
Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?Denes 9 - Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?
Answer Pre Pre % Post Post %Younger patients with a borderline resectable tumor (neoadjuvant)2 4 0 0Any patient with a borderline resectable tumor (neoadjuvant)1 2 0 0High risk patients after resection (adjuvant) 2 4 0 0Good PS patients with unresectable or metastatic disease23 51 0 0I use it in all of these settings 17 38 0 0Total 45 100% 0 100%
Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?Denes 10 - How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first line therapy?
Answer Pre Pre % Post Post %I order molecular profiling on all such patients 34 77 0 0I order molecular profiling only on never smokers 0 0 0 0I order molecular profiling only on never or light smokers1 2 0 0I order molecular profiling only on never smokers and remote light smokers4 9 0 0The likelihood of finding a treatment altering mutation is so low I don’t use it to guide first line therapy5 11 0 0Total 44 100% 0 100%
Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?Denes 11 - In patients who have failed approved therapies for advanced cancer how often have you requested genomic analysis to identify potentially “actionable” mutations?
Answer Pre Pre % Post Post %In most of such cases 12 24 0 0In about half of such cases 3 6 0 0Occasionally 15 31 0 0Never 19 39 0 0Total 49 100% 0 100%
Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?Denes 12 - How do you think your use of genomic analysis will change in the next 10 years?
Answer Pre Pre % Post Post %We will be obtaining genomic profiling on most or all cancers39 74 0 0We will be obtaining genomic profiling on half of all cancers10 19 0 0I see no change in the use of genomic profiling 2 4 0 0We’ll learn that genomic profiling will benefit very few patients and will only be rarely useful. Most of the commercial companies will be out of business2 4 0 0Total 53 100% 0 100%
Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?Bartlett 1 - What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients who are not candidates for stem cell transplant?
Answer Pre Pre % Post Post %R-‐CHOP 11 28 6 14R-‐CVP 1 3 1 2R-‐Bendamustine 18 45 25 57R-‐Bendamustine/Ara-‐C 0 0 1 2R-‐Bendamustine/Velcade 2 5 2 5E1411: R-‐Benda vs. R-‐Bendamustine/ Velcade 8 20 9 20Total 40 100% 44 100%
Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?Bartlett 2 - Do you use PET in the staging and response assessment of patients with follicular lymphoma?
Answer Pre Pre % Post Post %Yes 33 69 40 75No 15 31 13 25Total 48 100% 53 100%
Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?Carson 1 - What is the estimated annual cost of low-dose CT screening for lung cancer to Medicare if adopted?
Answer Pre Pre % Post Post %$0.5 Billion 3 6 0 0$1.1 Billion 12 24 2 3$1.9 Billion 18 36 53 90$2.5 Billion 17 34 4 7Total 50 100% 59 100%
Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?Carson 2 - What was found when the first published reports of stage III randomized controlled trials were compared to updated reports?
Answer Pre Pre % Post Post %Under estimation of outcomes and toxicity 7 15 4 7Over estimation of outcomes and toxicity 10 21 3 5Under estimation of outcomes, over estimation of toxicity7 15 0 0Over estimation of outcomes, under estimation of toxcity23 49 50 88Total 47 100% 57 100%
Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:Picus 1 - The role of cytotoxic chemotherapy in prostate cancer is best used in:
Answer Pre Pre % Post Post %1. Localized disease 0 0 0 02. Castrate Resistant Prostate Cancer 10 20 2 43. Not active in prostate cancer 0 0 1 24. Can be used for newly diagnosed metastatic disease2 4 9 205. Best used in conjunction with radiation therapy (Combined Modality Approach)3 6 2 46. 1 & 5 2 4 2 47. 2 & 4 32 65 29 64Total 49 100% 45 100%
Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:Picus 2 - Immunotherapy may have a role based on data from ASCO for:
Answer Pre Pre % Post Post %Testicular Cancer 6 12 1 2Prostate Cancer 12 24 3 6Bladder Cancer 6 12 30 56Kidney cancer 27 53 20 37Total 51 100% 54 100%
Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:Picus 3 - Hormone therapy in prostate cancer can be used with:
Answer Pre Pre % Post Post %1. Localized disease 1 2 2 52. Castrate Resistant Prostate Cancer 2 5 1 23. Not active in prostate cancer 1 2 1 24. Can be used for newly diagnosed metastatic disease8 19 4 105. Best used in conjunction with radiation therapy (Combined Modality Approach)1 2 2 56. 1 & 5 15 36 11 277. 2 & 4 14 33 20 49Total 42 100% 41 100%
Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.Picus 4 - When using immunotherapy and in particular inhibtiors of the PD-1 signaling pathway, staining for PD-1 or PD-L1 expression is predictive of response.
Answer Pre Pre % Post Post %True 30 58 15 26False 22 42 42 74Total 52 100% 57 100%
Vij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitorVij 1 - Panobinostat is a selective HDAC-6 inhibitor
Answer Pre Pre % Post Post %True 39 80 28 56False 10 20 22 44Total 49 100% 50 100%
Vij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab isVij 2 - Blinatumomab is
Answer Pre Pre % Post Post %A bispecific T-‐cell engaging (BiTE) antibody 17 36 50 89A dual affinity retargeting (DART) antibody 14 30 4 7A glyco-‐engineered antibody 7 15 1 2A conjugated antibody 9 19 1 2Total 47 100% 56 100%
Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.Sorscher 1 - Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-year RFS.
Answer Pre Pre % Post Post %True 38 73 6 12False 14 27 43 88Total 52 100% 49 100%
Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?Sorscher 2 - Which adjuvant chemotherapy is superior in 3-year DFS?
Answer Pre Pre % Post Post %FOLFOX 20 38 2 4CAPEOX 1 2 0 01 and 2 provide the same 3-‐year DFS 31 60 49 96Total 52 100% 51 100%
Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?Sorscher 3 - Which neoadjuvant therapy is superior for 5-year DFS for rectal cancer?
Answer Pre Pre % Post Post %RT/5FU 9 17 0 0RT/Capecitabine 8 15 4 9Equally effective in 5-‐year DFS 35 67 41 91Total 52 100% 45 100%
Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?Sorscher 4 - How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or the first part of 2014?
Answer Pre Pre % Post Post %5 5 10 0 09 11 23 0 012 16 33 0 019 16 33 33 100
Total 48 100% 33 100%
Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?Sorscher 5 - As an oncologist, which better describes your philosophy?
Answer Pre Pre % Post Post %Empiricist 6 13 19 45Rationalist 25 52 10 24Neither 17 35 13 31Total 48 100% 42 100%
Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.Wartman 1 - True or false: the major obstacle to the clinical implantation of next-generation comprehensive sequencing tests remains the cost of data generation.
Answer Pre Pre % Post Post %True 20 69 2 17False 9 31 10 83Total 29 100% 12 100%
Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.Wartman 2 - True or false: the percentage of patients found to have variants of unknown significance (VUS) currently outnumbers the number of patients found to have known pathogenic or likely pathogenic variants identified in gene panel testing for inherited cancer disorders.
Answer Pre Pre % Post Post %True 18 72 9 75False 7 28 3 25Total 25 100% 12 100%
0
20
40
60
80
True False
44
56
20
80Panobinostat is a selective HDAC-‐6 inhibitor
%
Pre %Post %
0
22.5
45
67.5
90
A bispecific T-‐cell engaging (BiTE) antibody A glyco-‐engineered antibody
227
89
1915
3036
Blinatumomab is
%
Pre %Post %
0
17.5
35
52.5
70
pure hematology (benign and malignant) General solid tumor oncology (more than 5 disease types)
00000
1115
63
11
0
Which best describes your clinical practice?
%
Pre %Post %
0
12.5
25
37.5
50
The number of new agents is overwhelming and I cannot keep up with the new agents
000
32
45
23
Which best reflects your feelings about the rapid expansion of “targeted” therapies in oncology?
%
Pre %Post %
0
17.5
35
52.5
70
I feel comfortable with them and have used them in my practice I do not feel comfortable with them and do not use them in my practice
000
26
9
66
How have you incorporated immune modulating agents into your practice?
%
Pre %Post %
0
10
20
30
40
Single agent ipilimumab Combination of trametinib and dabrafenib Refer patient to melanoma expert for management
00000
40
6
23
19
13
You are referred a 55 year old man with newly diagnosed V600E mutated metastatic melanoma with exten
%
Pre %Post %
0
15
30
45
60
I would be comfortable in recommending a treatment plan I would refer the patient to a lymphoma expert for evaluation and treatment
0000
23
6
17
54
How would you manage a patient with newly diagnosed Hodgkin Lymphoma stage IIIA
%
Pre %Post %
0
17.5
35
52.5
70
I would be comfortable in recommending a treatment plan I would refer the patient to a leukemia expert for evaluation and treatment
0000
28
02
70You are referred a patient for evaluatin of splenomegaly and make the diagnosis of chronic phase bcr
%
Pre %Post %
0
15
30
45
60
I would be comfortable in formulating and administering a treatment plan I would refer the patient to the University of Indiana for evaluation and treatment
000004
21
2
17
55
A 22 year old college student with a stage II mixed germ cell tumor is referred for evaluation. How
%
Pre %Post %
0
10
20
30
40
Usually or almost always Only in a few selected patients I usually reserve it for 2nd line and beyond
000
3835
28
How often do you include a platinum analogue in first line therapy of TNBC?
%
Pre %Post %
0
15
30
45
60
Younger patients with a borderline resectable tumor (neoadjuvant) Good PS patients with unresectable or metastatic disease
00000
38
51
424
Which patients with pancreatic cancer do you most commonly treat with FOLFIRINOX?
%
Pre %Post %
0
22.5
45
67.5
90
True False
88
12
27
73
Initiating adjuvant chemotherapy for colon cancer before 8 weeks improves 5-‐year RFS.
%
Pre %Post %
0
25
50
75
100
FOLFOX CAPEOX 1 and 2 provide the same 3-‐year DFS
96
04
60
2
38
Which adjuvant chemotherapy is superior in 3-‐year DFS?
%
Pre %Post %
0
25
50
75
100
RT/5FU RT/Capecitabine Equally effective in 5-‐year DFS
91
90
67
1517
Which neoadjuvant therapy is superior for 5-‐year DFS for rectal cancer?
%
Pre %Post %
0
25
50
75
100
5 9 12 19
100
000
3333
23
10
How many drugs for solid tumor malignancies were approved or given an expanded indication in 2013 or
%
Pre %Post %
0
15
30
45
60
Empiricist Rationalist Neither
31
24
45
35
52
13
As an oncologist, which better describes your philosophy?
%
Pre %Post %
0
22.5
45
67.5
90
True False
83
17
31
69
True or false: the major obstacle to the clinical implantation of next-‐generation comprehensive sequ
%
Pre %Post %
0
20
40
60
80
True False
25
75
28
72
True or false: the percentage of patients found to have variants of unknown significance (VUS) curre
%
Pre %Post %
0
15
30
45
60
R-‐CHOP R-‐Bendamustine R-‐Bendamustine/Velcade
20
52
57
2
14
20
5
0
45
3
28
What induction regimen do you prefer for patients with newly diagnosed mantle cell lymphoma patients
%
Pre %Post %
0
20
40
60
80
Yes No
25
75
31
69
Do you use PET in the staging and response assessment of patients with follicular lymphoma?
%
Pre %Post %
0
22.5
45
67.5
90
$0.5 Billion $1.1 Billion $1.9 Billion $2.5 Billion
7
90
30
3436
24
6
What is the estimated annual cost of low-‐dose CT screening for lung cancer to Medicare if adopted?
%
Pre %Post %
0
22.5
45
67.5
90
Under estimation of outcomes and toxicity Under estimation of outcomes, over estimation of toxicity
88
057
49
1521
15
What was found when the first published reports of stage III randomized controlled trials were compa
%
Pre %Post %
0
17.5
35
52.5
70
1. Localized disease 4. Can be used for newly diagnosed metastatic disease 7. 2 & 4
64
44
20
240
65
4640
20
0
The role of cytotoxic chemotherapy in prostate cancer is best used in:
%
Pre %Post %
0
15
30
45
60
Testicular Cancer Prostate Cancer Bladder Cancer Kidney cancer
37
56
62
53
12
24
12
Immunotherapy may have a role based on data from ASCO for:
%
Pre %Post %
0
12.5
25
37.5
50
1. Localized disease 4. Can be used for newly diagnosed metastatic disease 7. 2 & 4
49
27
5
10
225
3336
2
19
25
2
Hormone therapy in prostate cancer can be used with:
%
Pre %Post %
0
20
40
60
80
True False
74
26
42
58
When using immunotherapy and in particular inhibtiors of the PD-‐1 signaling pathway, staining for PD
%
Pre %Post %
0
20
40
60
80
I order molecular profiling on all such patients I order molecular profiling only on never smokers and remote light smokers
00000
119
20
77
How do you use molecular testing in patients with advanced non squamous NSCLC presenting for first l
%
Pre %Post %
0
10
20
30
40
In most of such cases In about half of such cases Occasionally Never
0000
39
31
6
24
In patients who have failed approved therapies for advanced cancer how often have you requested geno
%
Pre %Post %
0
20
40
60
80
We will be obtaining genomic profiling on most or all cancers I see no change in the use of genomic profiling
000044
19
74
How do you think your use of genomic analysis will change in the next 10 years?
%
Pre %Post %
Polling Results

Additional Features &
ServicesReduce Costs
Data Compatibility EM Customer Service
Bundled Services
EM offers a complete rangeof event services including full service A/V. Ask about
how you can save bybundling services.
ARRAY OnQ helpsyou beat high printing costs by making materials available in
digital form, and giving you the flexibility to make last minute
changes to content.
Make the most of your collected data
by importing into our ARRAY Analytics tool.
Our highly skilledon-site service team
is always there toensure your event
is perfect.
A / V , A R S , A n d M o R e
ARRAY Analytics
educationalmeasures.com
Would you like to see more? If you would like to arrange a demo, or drop in on a live event to see ARRAY OnQ in action, let us know – We’d love to work with you!