epuration hépatique par le système marsph 7,49 + 0,04 7,49 + 0,03 0,749 urée 15,7 + 4,7 15,4 +...
TRANSCRIPT

Epuration Hépatiquepar
le Système MARS
Pr Faouzi SALIBA
Centre Hépato-Biliaire
Hôpital Paul Brousse - Villejuif
Epuration hépatique MARSIndications
Hépatite Fulminante ou subfulminante
Décompensation aigue chez le cirrhotique
Ictère cholestatique sévère
Encéphalopathie/Coma Hépatique
Syndrome hépato-rénal
Autres Indications :
Insuffisance hépatique sévère après chirurgie hépatique
Non fonctionnement primaire du greffon (PNF après TH)
Prurit réfractaire au cours des maladies chroniques cholestatiques
Intoxications médicamenteuses

Conséquences des hépatectomiessur foie sain (Donneur familial)
Hépatectomie droite sans clampage vasculaireet sans transfusion sanguine

E.T., femme de 41 ans
0
20
40
60
80
100
120
-1 1 3 5 7 9 11 13 15
TP Facteur II
0
50
100
150
200
250
-1 1 3 5 7 9 11 13 15
Bilirubine Gamma-GT
0
50
100
150
200
250
-1 1 3 5 7 9 11 13 15
GOT GPT
10
20
30
40
50
60
-1 1 3 5 7 9 11 13 15
Albumine
Foie droit : 960 cc Foie gauche : 400 cc (29%) Poids Greffon: 660 g (69%)Estimation foie gauche: 270 g , Hospitalisation: 12 J dont Réanimation: 4 J
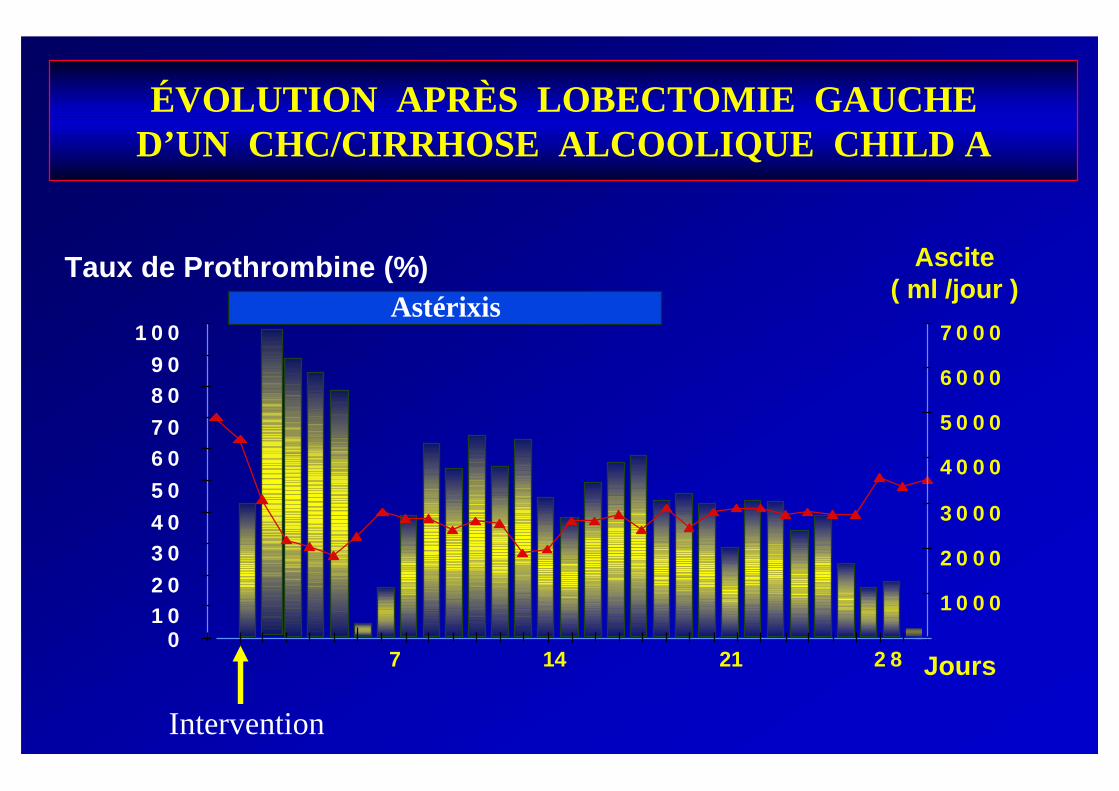
ÉVOLUTION APRÈS LOBECTOMIE GAUCHED’UN CHC/CIRRHOSE ALCOOLIQUE CHILD A
01 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
7 14 21 2 8
1 0 0 0
2 0 0 0
3 0 0 0
4 0 0 0
5 0 0 0
6 0 0 0
7 0 0 0
Jours
Taux de Prothrombine (%) Ascite( ml /jour )
Astérixis
Intervention

• PGE1 (Prostaglandines) en perfusion continue*– Voie intraveineuse
– voie intra-artérielle hépatique
• Hémodiafiltration continue
• Epuration Hépatique MARS
• Foie Bioartificiel
• Transplantation hépatique (donneur familial, foie domino)
Insuffisance Hépatique après Hépatectomie
TRAITEMENTS SPÉCIFIQUES
*Sato T et al. Hepatogastroenterology 2000Sato T et al. Dig Surg 2000
Hanazaki K et al. Hepatogastroenterology 2000NaKai T et al. J Gastroenterology 1998

Foie BioartificielExpérience du CHB (Hôpital Paul Brousse)
Bioréacteur composé de
microfibres creuses
Présence d’Hépatocytes séparés
par une membrane semi-
perméable à travers laquelle
passe le plasma (Demetriou)

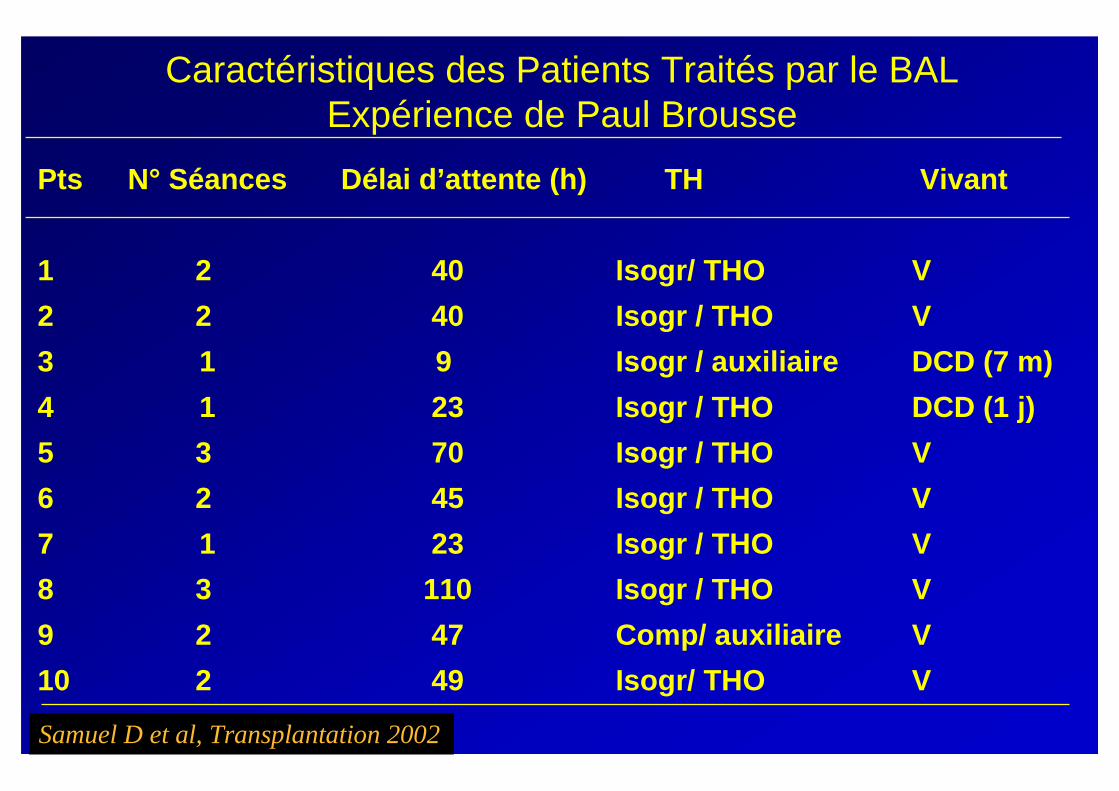
Caractéristiques des Patients Traités par le BALExpérience de Paul Brousse
Pts
1
2
3
4
5
6
7
8
9
10
Sexe/ Age
F / 27
M / 44
M / 14
F / 24
F / 25
M /17
F / 37
F / 47
F / 38
M / 37
Etiologie
Wilson
Indéterminée
Indéterminée
Indéterminée
Pyrazinamide
Indéterminée
Indéterminée
Virale A
Indéterminée
Virale B
Coma
Début BAL
Gr 2
Gr 2
Gr 2
Gr 3
Gr 1
Gr 2
Gr 1
Gr 1
Gr 3
Gr 2
Ventilation
Mécanique
+
+
-
+
-
-
-
-
-
-
Fact V
%
16
15
15
15
4
14
15
16
18
12
Samuel D et al, Transplantation 2002
Pts
1
2
3
4
5
6
7
8
9
10
N° Séances
2
2
1
1
3
2
1
3
2
2
Délai d’attente (h)
40
40
9
23
70
45
23
110
47
49
TH
Isogr/ THO
Isogr / THO
Isogr / auxiliaire
Isogr / THO
Isogr / THO
Isogr / THO
Isogr / THO
Isogr / THO
Comp/ auxiliaire
Isogr/ THO
Vivant
V
V
DCD (7 m)
DCD (1 j)
V
V
V
V
V
V
Caractéristiques des Patients Traités par le BALExpérience de Paul Brousse
Samuel D et al, Transplantation 2002
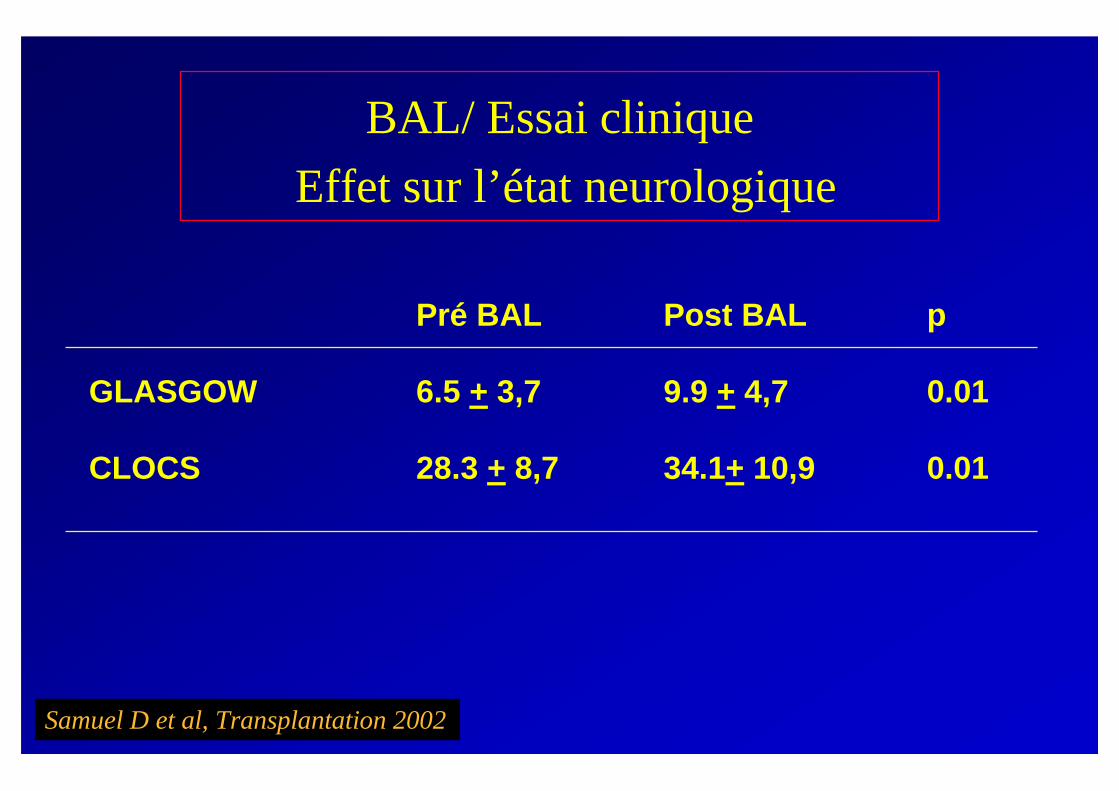
BAL/ Essai clinique
Effet sur l’état neurologique
GLASGOW
CLOCS
Pré BAL
6.5 + 3,7
28.3 + 8,7
Post BAL
9.9 + 4,7
34.1+ 10,9
p
0.01
0.01
Samuel D et al, Transplantation 2002

BAL/ Essai cliniqueEffet sur les paramètres Métaboliques
Pre BAL Post BAL p
Héma tocri te 33 + 6,9 28,3 + 5,45 0,01
GB 13,4 + 7,6 16 + 8,7 0,15
Pla quettes 194,7 + 48,5 140,9 + 42,9 0,006
Bilirubine 486,6 + 163 347 + 125 0,0005
ALAT 573 + 4420 388 + 261 0,0067
Protéinestotales
53,8 + 8 41,5 + 5 < 0,0001
Facteur V 17,4 + 6,6 11,6 + 5,6 0,022
Lactates 3,6 + 2,55 2,8 + 1,28 0,31
Ammoniémie 114 + 64 96 + 45 0,26
PH 7,49 + 0,04 7,49 + 0,03 0,749
Urée 15,7 + 4,7 15,4 + 4,6 0,724
Créatinine 88,4 + 68,4 80,1 + 51 0,217
Samuel D et al, Transplantation 2002

Epuration Hépatique MARS
Dialyse hépatique utilisant lepouvoir de fixation del’albumine

Insuffisance hépatiqueSubstances pathogènes
Bilirubine, acides biliaires
Ammoniémie
Benzodiazepines endogènes
Acides gras à chaines courte et moyenne
Tryptophan (AAA / AAR )
Faux neurotransmetteurs (phényl éthylamine)
NO
Phenols, mercaptans
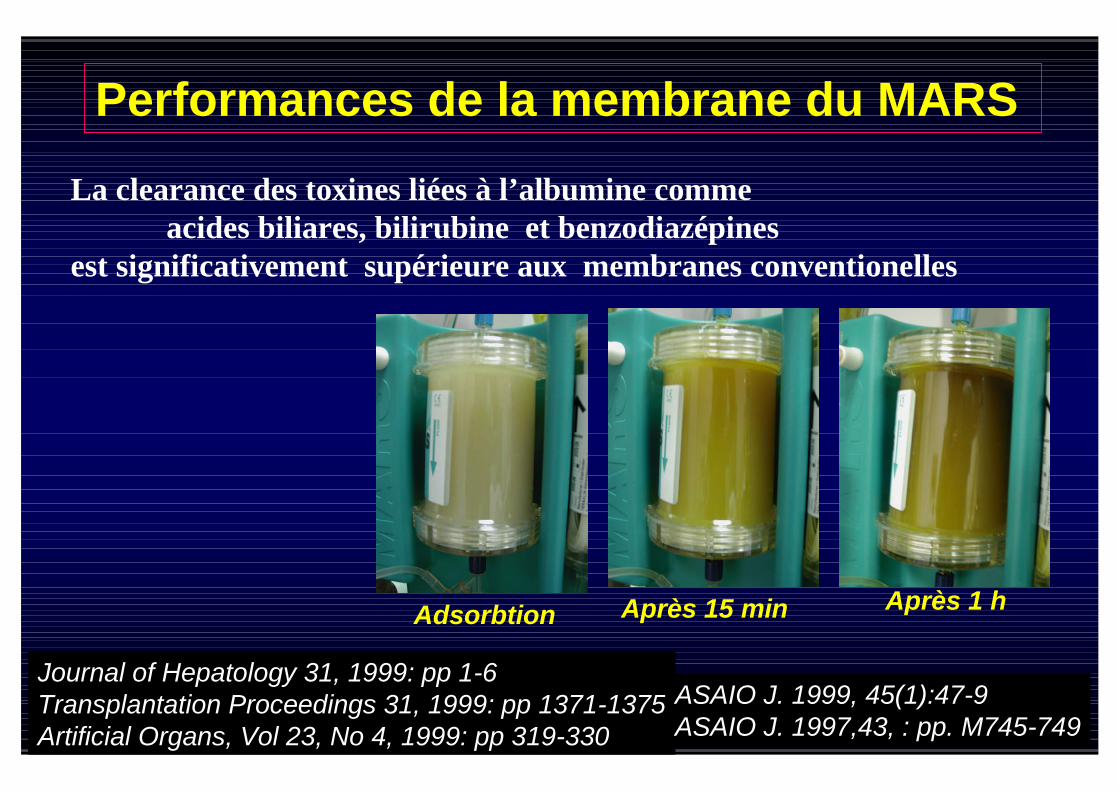
Adsorbtion Après 15 min Après 1 h
Performances de la membrane du MARS
La clearance des toxines liées à l’albumine commeacides biliares, bilirubine et benzodiazépines
est significativement supérieure aux membranes conventionelles
Journal of Hepatology 31, 1999: pp 1-6Transplantation Proceedings 31, 1999: pp 1371-1375Artificial Organs, Vol 23, No 4, 1999: pp 319-330
ASAIO J. 1999, 45(1):47-9ASAIO J. 1997,43, : pp. M745-749

0
50
100
150
200
µm
ol
/h
Acides Biliaires Acides gras libres
MARS
HF n = 8 : 2 + 3
n = 8 : 160 + 40
n = 12 : 10 + 2
n = 12 : 15 0 + 120
MARS
HF
MARS® vs. Hémodiafiltration
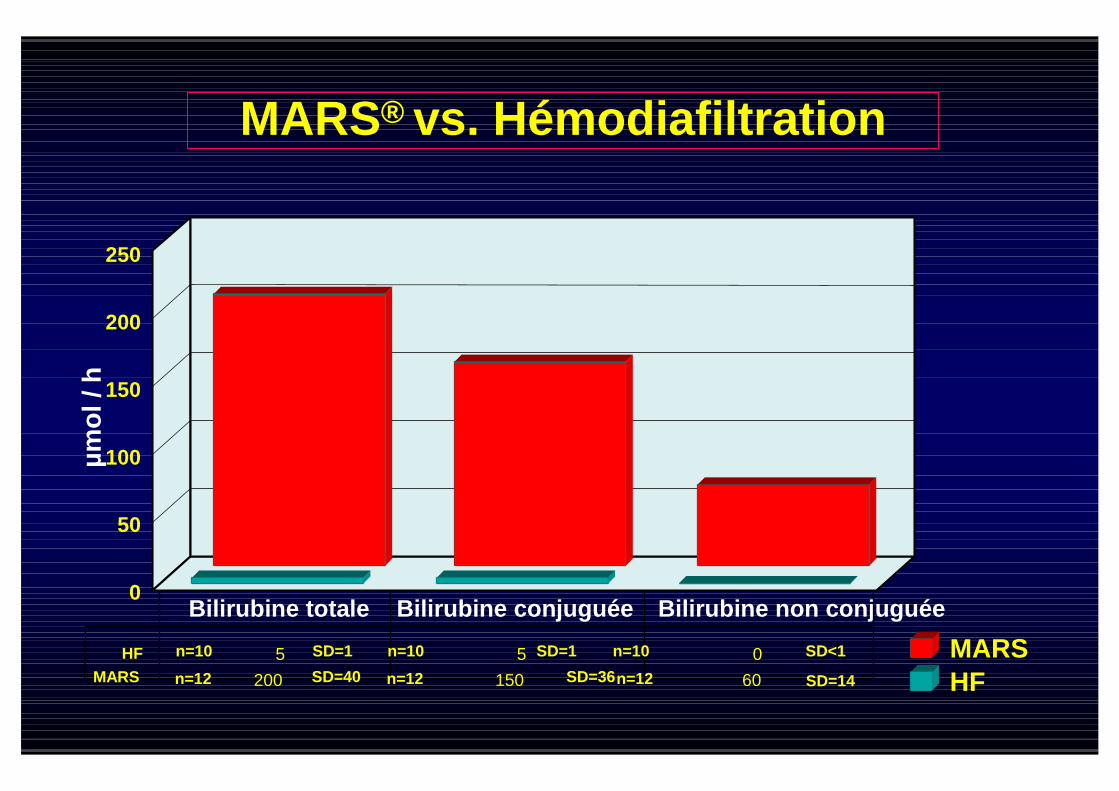
Bilirubine totale Bilirubine conjuguée Bilirubine non conjuguée
5 5 0
200 150 60SD=40 SD=36 SD=14
SD=1 SD=1 SD<1n=10 n=10 n=10
n=12 n=12 n=12
HF
MARS
0
50
100
150
200
µm
ol/h
250
MARS
HF
MARS® vs. Hémodiafiltration

Change of Fisher-Index
HDF MARS®
Ch
an
ge
of
init
ial
Blo
od
level
(%)
-60
100
80
60
40
20
0
-20
-40
Increase
Decrease
p = 0,05
Fischer-Index:BCAA - Branched-chain Amino AcidsAAA - Aromatic Amino Acids
MARS® vs. Hémodiafiltration
Ratio : BCAA/AAA
Ratio of BCAA/AAA

3 études pilotes dans 3 Centres :
Copenhagen, Rostock, Tel Aviv.
42 Patients
Liver Transplantation, Vol 6, No 5 (Sept.), 2000: pp 603-613Hepatology, Vol 32, No 4, Pt2, 2000: pp 401A; 612AArtificial Organs, Vol 23, No 4, 1999: pp 319-330
MARS et Hépatopathie chronique avec Cholestase
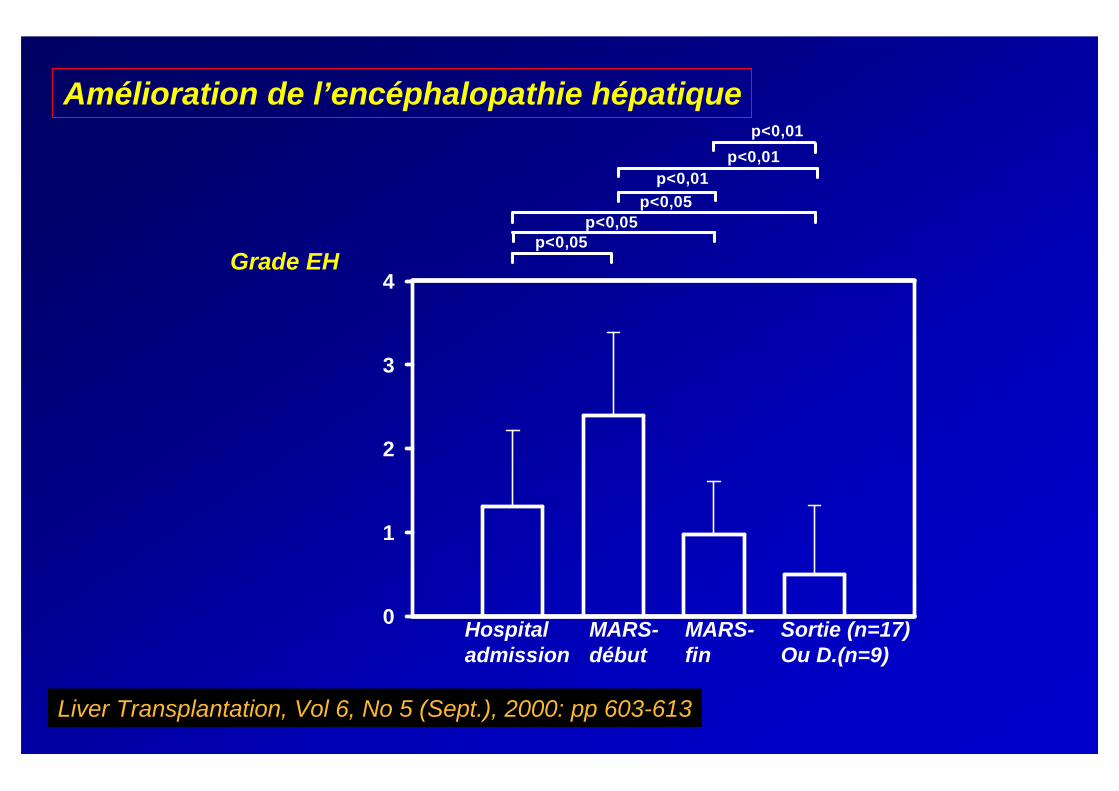
0
1
2
3
4
p<0,05p<0,05
p<0,05
p<0,01
p<0,01
p<0,01
Amélioration de l’encéphalopathie hépatique
Liver Transplantation, Vol 6, No 5 (Sept.), 2000: pp 603-613
Hospitaladmission
MARS-début
MARS-fin
Sortie (n=17)Ou D.(n=9)
Grade EH

Amélioration du score de Child-Pugh
Score Child-Pugh
Hospitaladmission
MARS-start
MARS-end
Discharge (n=17)or d.(n=9)
CT
P-S
co
re
5
6
7
8
9
10
11
12
13
14
15
p<0,05p<0,05
p<0,01
p<0,01
p<0,01
p<0,05
Liver Transplantation, Vol 6, No 5 (Sept.), 2000: pp 603-613
Hospitaladmission
MARS-début
MARS-fin
Sortie (n=17)Ou D.(n=9)
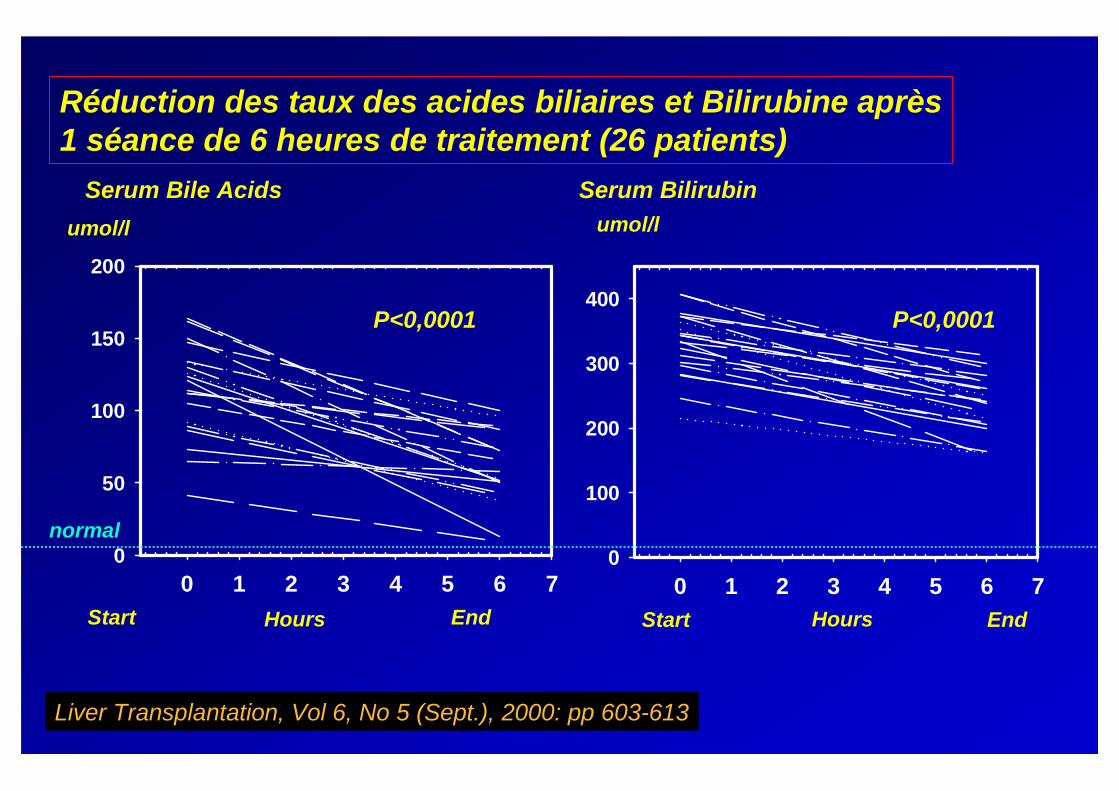
Réduction des taux des acides biliaires et Bilirubine après1 séance de 6 heures de traitement (26 patients)
Liver Transplantation, Vol 6, No 5 (Sept.), 2000: pp 603-613
Serum Bilirubin
Start EndHours
umol/l
0 1 2 3 4 5 6 7
0
100
200
300
400
Serum Bile Acids
Start
0 1 2 3 4 5 6 7
0
50
100
150
200
End
umol/l
Hours
P<0,0001 P<0,0001
normal

Recov2III20UGI
Bleeding
ACM618
Recov2II/III19SepsisAmyo + FMFF297
Recov3III17UTIACF376
Recov1IV28UnknownACM605
D (1day)2II/III27SBPPCF674
OLT (recov)2II/III18UGI
Bleeding
CF243
D (60 days)8III/IV21BAC+CM452
D (30 days)5III/IV30SBP
+UGI
Bleeding
AC + CM561
OutcomeNoMARS
EncepApIIEventPrimary
Liver
disease
SexAgePts
Phase I Trial: Liver failure and cholestasis
Sorkine P., 2000, Tel Aviv, Israel

Effect of MARS on Metabolic and Renal Function
Parameters Pre-MARS Post-MARS p
Ammonia (mg/dL) 279.90 ±67.48 65.25 ± 6.40 <0.005
Lactate (mmol/L) 6.53 ± 1.21 2.81 ± 0.72 <0.02
Albumin (g/dL) 3.92 ± 0.45 4.02 ± 0.94 ns
BUN (mg/dL) 29.34 ± 3.21 10.21 ± 1.34 <0.03
Creatinine (mg/dL) 2.36 ± 0.18 1.23 ± 0.67 <0.04
Glucose (mg/dl) 145.62 ± 10.56 134.26 ±9.56 ns
Sorkine P., 2000, Tel Aviv, Israel

Effect of MARS on Liver Function Tests
ns121.3 ± 12.3128.4 ± 9.7AP U/l
ns518 ± 23836.7 ± 448.9ALT U/l
ns584.4 ± 305.9938 ± 305.9AST U/l
< 0.043.46 ± 1.58.2 ± 2.4Ind Bilirubin(mg/dl)
< 0.038.6 ± 1.716.9 ± 3.6Direct Bilirubin(mg/dl)
<0.0312.1 ± 2.525.15 ± 6Total Bilirubin(mg/dl)
pPost- MarsPre-MarsParameter
Sorkine P., 2000, Tel Aviv, Israel

MAP (mmHg)
Before During After
50
60
70
80
90
100
110
Sorkine P., 2000, Tel Aviv, Israel
before during after

Systemic Vascular Resistance Index (dyn s/cm5/m
2)
Before After500
600
700
800
900
1000
1100
1200
Schmidt et al, 2000. Rigshospitalet, Copenhagen, Denmark.

ICP (mmHg)
Before During After
6
8
10
12
14
16
18
20
22
24
Sorkine P., 2000, Tel Aviv, Israel

Cerebral Blood Flow (cm/sec)
Before After0
20
40
60
80
100
120
Schmidt et al, 2000. Rigshospitalet, Copenhagen, Denmark.

MAP and urine volume in patients with type I HRS
0
20
40
60
80
100
120
MAP Urine volume
MA
P(m
mH
g)
0
200
400
600
800
1000
1200
uri
ne
vo
lum
e(m
l/d
ay)
MARS pre treatment MARS post treatment HDF pre treatment HDF post treatment
p < 0,05
Liver Transpl 2000 May;6(3):277-86
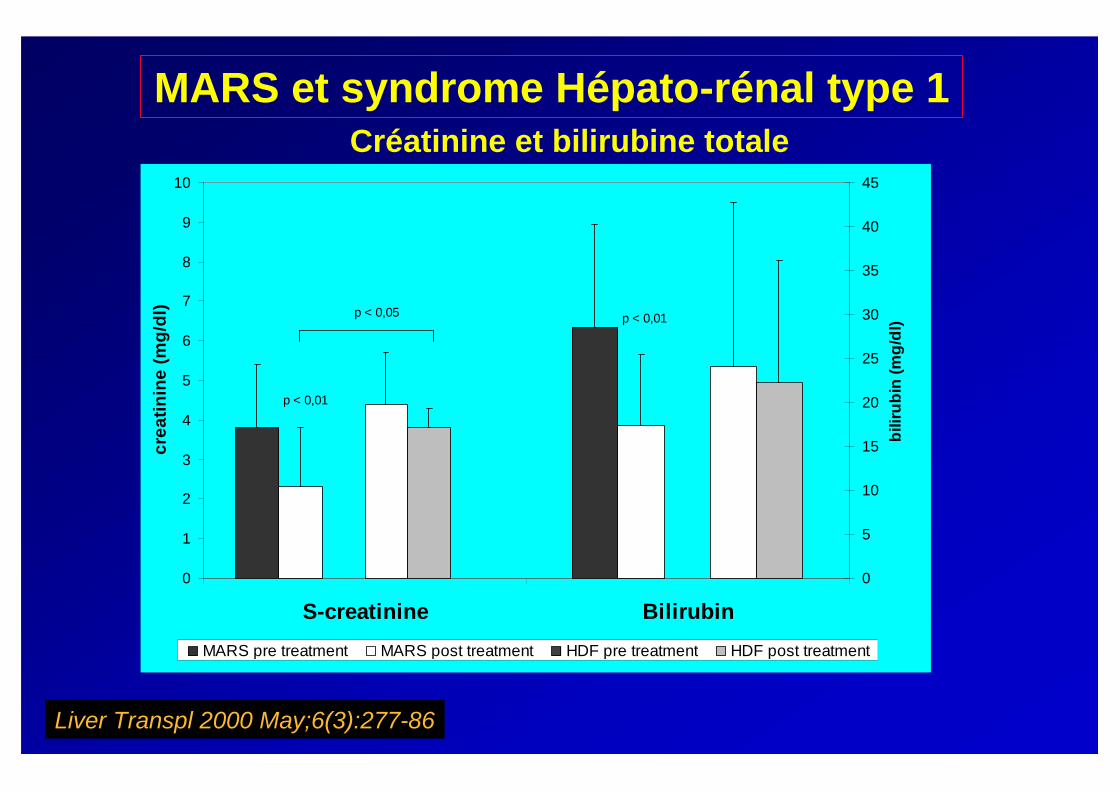
MARS et syndrome Hépato-rénal type 1Etude prospective, Randomisée, Contrôlée
Cirrhose 13 pts: 8 HDF+MARS, 5 traités par HDF seul
0
1
2
3
4
5
6
7
8
9
10
S-creatinine Bilirubin
cre
ati
nin
e(m
g/d
l)
0
5
10
15
20
25
30
35
40
45
bilir
ub
in(m
g/d
l)
MARS pre treatment MARS post treatment HDF pre treatment HDF post treatment
p < 0,01
p < 0,05 p < 0,01
Créatinine et bilirubine totale
Liver Transpl 2000 May;6(3):277-86
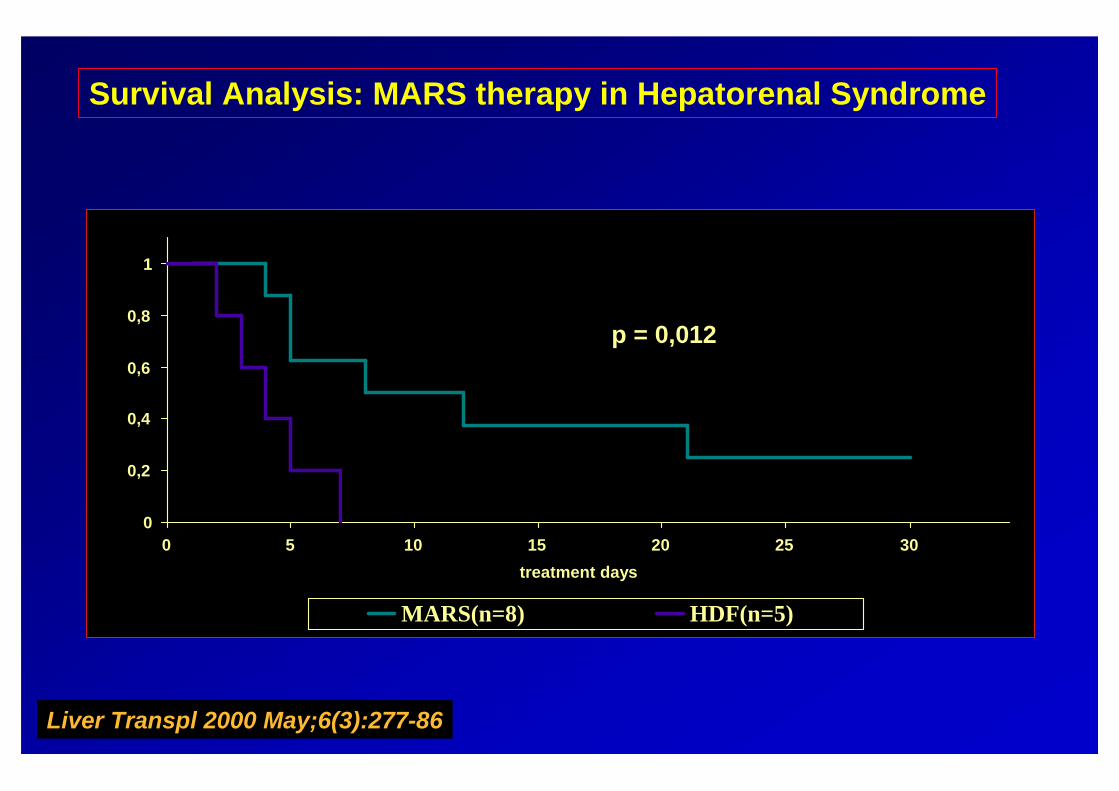
MARS et syndrome Hépato-rénal type 1
0
0,2
0,4
0,6
0,8
1
0 5 10 15 20 25 30
treatment days
MARS(n=8) HDF(n=5)
p = 0,012
Survival Analysis: MARS therapy in Hepatorenal Syndrome
Liver Transpl 2000 May;6(3):277-86

MARSHypothetical impact on HRS
plasmatic NO
effective arterial volume
peripheral vasodilatation
renal perfusion/function
hepatocellular hepatic overload
intrahepatic pressure
cell edema
renal perfusion/function
normalization of circulation
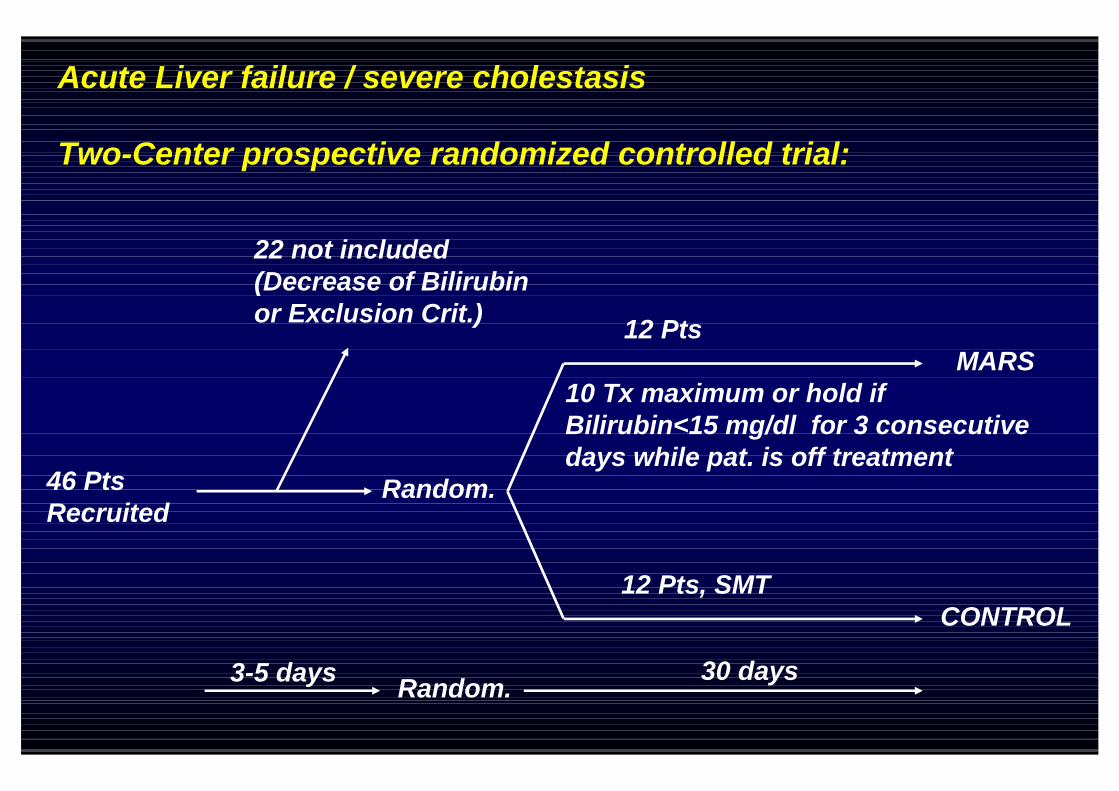
Acute Liver failure / severe cholestasis
Two-Center prospective randomized controlled trial:
46 PtsRecruited
22 not included(Decrease of Bilirubinor Exclusion Crit.)
Random.
12 Pts
10 Tx maximum or hold ifBilirubin<15 mg/dl for 3 consecutivedays while pat. is off treatment
12 Pts, SMT
MARS
CONTROL
Random.3-5 days 30 days
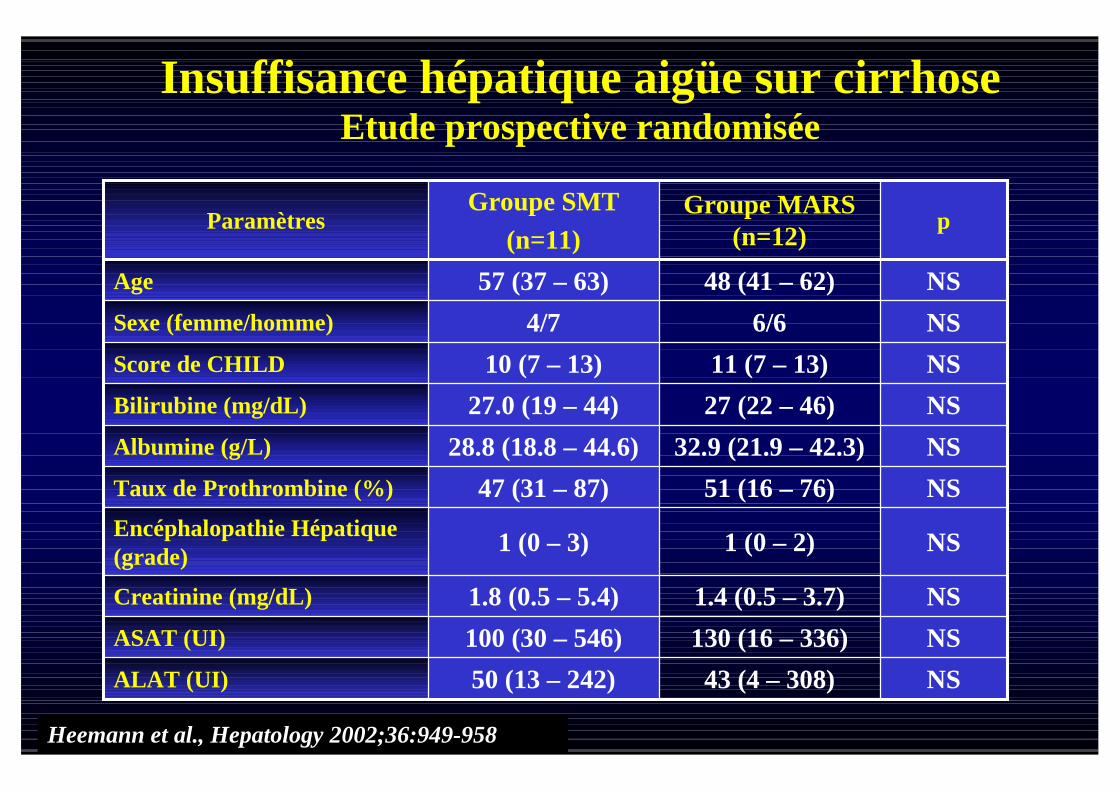
NS1 (0 – 2)1 (0 – 3)Encéphalopathie Hépatique(grade)
NS1.4 (0.5 – 3.7)1.8 (0.5 – 5.4)Creatinine (mg/dL)
NS130 (16 – 336)100 (30 – 546)ASAT (UI)
NS43 (4 – 308)50 (13 – 242)ALAT (UI)
NS51 (16 – 76)47 (31 – 87)Taux de Prothrombine (%)
NS32.9 (21.9 – 42.3)28.8 (18.8 – 44.6)Albumine (g/L)
NS27 (22 – 46)27.0 (19 – 44)Bilirubine (mg/dL)
NS11 (7 – 13)10 (7 – 13)Score de CHILD
NS6/64/7Sexe (femme/homme)
NS48 (41 – 62)57 (37 – 63)Age
pGroupe MARS
(n=12)
Groupe SMT
(n=11)Paramètres
Heemann et al., Hepatology 2002;36:949-958
Insuffisance hépatique aigüe sur cirrhoseEtude prospective randomisée

M a in V is it N u m b e r
Hep
ati
cE
ncep
halo
path
yG
rad
e
0
1
2
3
4
S ta n d a rd M e d ic a l T h e ra p y
M A R S p lu s S ta n d a rd M e d ic a l T h e ra p y
p = 0 ,0 2 6 *p = 0 ,0 2 *
(B a s e lin e )
1 2 3 4 5
n .s .
p = 0 ,0 3 *p = 0 ,0 3 2 *
p = 0 ,0 2 2 *
p = 0 ,0 0 8 * p = 0 ,0 2 *p = 0 ,0 0 9 *
Impact on Hepatic EncephalopathyMARS

Impact on Child Turquotte Pugh(CTP-Score)
MARS
Main Visit Number
Ch
ild
Tu
rqu
ott
eP
ug
hS
co
re
6
8
10
12
14
Standard Medical Therapy
MARS plus Standard Medical Therapy
p=0,005 *
(Baseline)
1 2 3 4 5
p=0,057
p=0,02 *p=0,034 *
n.s.

M ain Visit N um ber
Bilir
ub
in/m
g/d
l
0
10
20
30
40
50
60
Standard M edical Therapy
M ARS plus Standard M edical Therapy
p<0,001 **
(Baseline)
1 2 3 4 5
p=0,021 *
p=0,04 *
n.s.
Impact on Serum BilirubinMARS
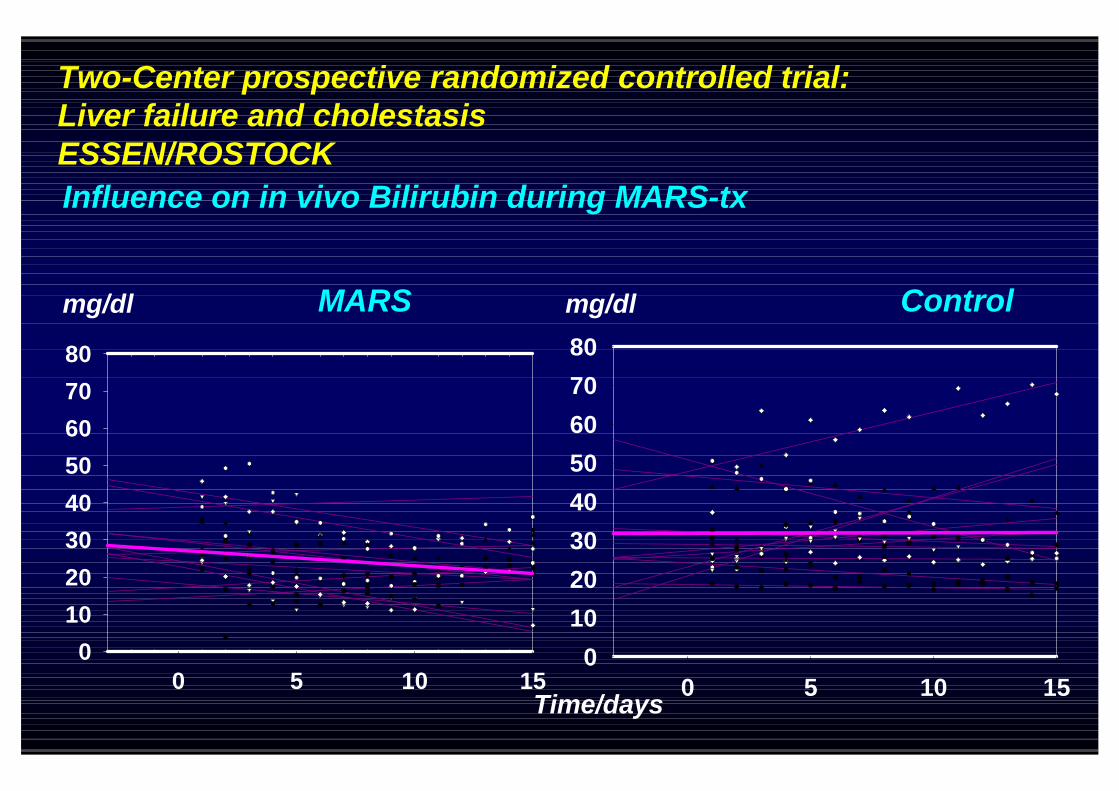
Two-Center prospective randomized controlled trial:Liver failure and cholestasisESSEN/ROSTOCK
Influence on in vivo Bilirubin during MARS-tx
MARS Control
0 5 10 150
10
20
30
40
50
60
70
80
0 5 10 150
10
20
30
40
50
60
70
80
mg/dl mg/dl
Time/days

M ain V is it N um ber
MA
Pch
an
ge
fro
mb
aselin
e/m
mH
g
De
cre
ase
Incre
ase
-40
-30
-20
-10
0
10
20
30
S tandard M edical Therapy
M AR S plus S tandard M edica l Therapy
85,5+14
77 ,6+11
B aseline
p=0,04 *p=0,06
(B aseline)
1 2 3 4 5
n .s. p=0,011 * p=0,013 *
p=0,021 *
Impact on Mean Arterial Pressure(MAP) Change from Baseline
MARS

M ain Visit Num ber
Cre
ati
nin
ch
an
ge
fro
mb
as
eli
ne
/m
g/d
l
De
cre
ase
Incre
ase
-2
-1
0
1
2
3
4
Standard M edical Therapy
M AR S plus Standard M edical Therapy
1,96+1,3
1,43+0,8
p=0,021 *
B aseline
p=0,055p=0,05 *
(Baseline)
1 2 3 4 5
n.s.
Impact on CreatinineChange from Baseline
MARS

Pression Aortique moyenne
Heemann et al., Hepatology 2002;36:949-958
MARS
0
1
2
3
4
0 10 20 30jours
SMT
SMT + MARSG
rad
een
cép
ha
lop
ath
ie
p < 0.01
Encéphalopathie hépatique
- 20%
- 10%
Baseline
+ 10%
+ 20%
10 20 30jours
MA
Pch
an
gem
ent
/b
ase
lin
ein
e% MARS
SMT
SMT + MARS
P < 0.05
Insuffisance hépatique aigüe sur cirrhoseParamtètres hémodynamique et neurologiques

0
0,2
0,4
0,6
0,8
1
0 10 20 30
Su
rvie
Cu
mu
lée
jours
SMT
SMT + MARS
P < 0.05
Survie 30 jours(Kaplan-Meier-plot)
Heemann et al., Hepatology 2002;36:949-958
Insuffisance hépatique aigüe sur cirrhoseEtude prospective randomisée

NS01Hémaorragie rupture VO
NS43Coagulopathie
NS01Apparition d‘ascite
< 0.05410Troubles électrolytiques
< 0.0517SHR
NS32Hypotension sévère
< 0.0503Aggravation encéphalopathie
< 0.0516Décès hôpital
pMARS(n=12)
SMT(n = 11)
Heemann et al., Hepatology 2002;36:949-958
Insuffisance hépatique aigüe sur cirrhoseComplications liées au stade terminal de la cirrhose
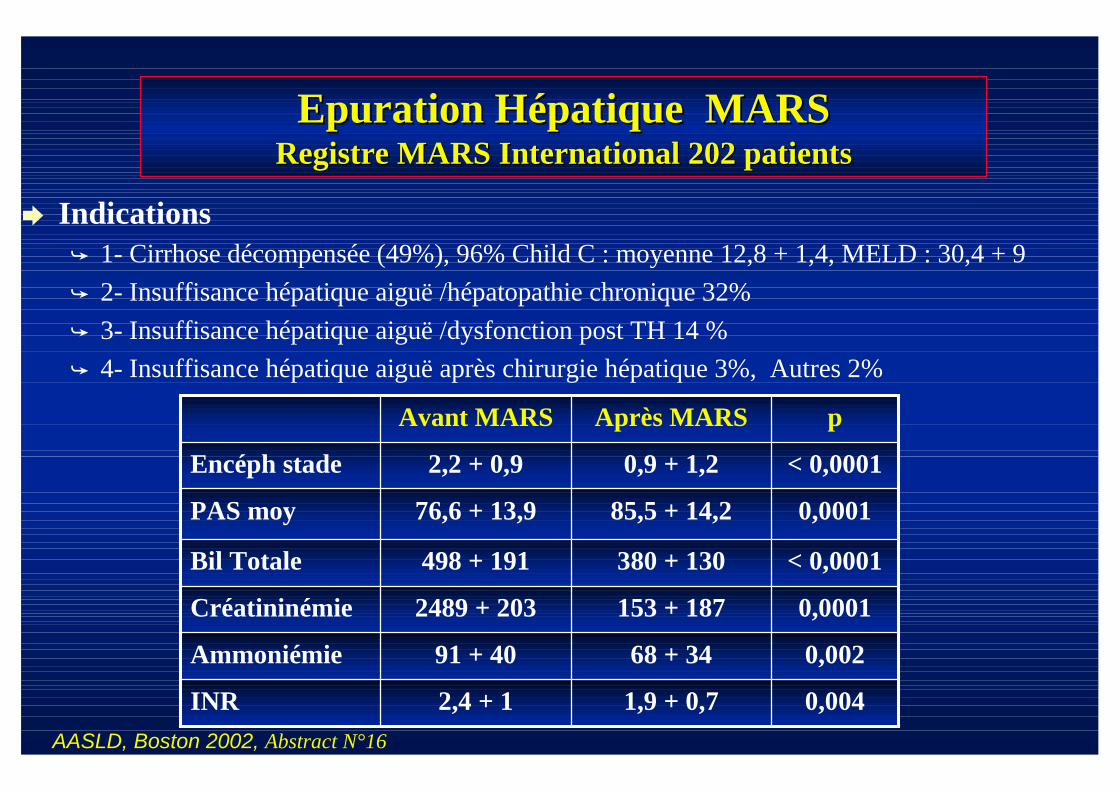
Epuration Hépatique MARSEpuration Hépatique MARSRegistre MARS International 202 patientsRegistre MARS International 202 patients
AASLD, Boston 2002, Abstract N°16
Indications 1- Cirrhose décompensée (49%), 96% Child C : moyenne 12,8 + 1,4, MELD : 30,4 + 9
2- Insuffisance hépatique aiguë /hépatopathie chronique 32%
3- Insuffisance hépatique aiguë /dysfonction post TH 14 %
4- Insuffisance hépatique aiguë après chirurgie hépatique 3%, Autres 2%
0,0041,9 + 0,72,4 + 1INR
0,00268 + 3491 + 40Ammoniémie
0,0001153 + 1872489 + 203Créatininémie
< 0,0001380 + 130498 + 191Bil Totale
0,000185,5 + 14,276,6 + 13,9PAS moy
< 0,00010,9 + 1,22,2 + 0,9Encéph stade
pAprès MARSAvant MARS

Epuration Hépatique MARSEpuration Hépatique MARSRegistre MARS International 202 patientsRegistre MARS International 202 patients
Cirrhose décompensée (49%), 96% Child C , MELD : 30,4 + 9Child 10 100% ,Child 12 71 %Child 14 55%Child 15 0%
Insuffisance hépatique aiguë /hépatopathie chronique
Survie hospitalière 61%
17 (27%) TH15/17 ( 88%) vivants
Insuffisance hépatique aiguë /dysfonction post TH
Survie après TH 56% 15 pts sans reTH
AASLD, Boston 2002, Abstract N°16
Survie Patient

Epuration Hépatique MARSEpuration Hépatique MARSExpérience du Centre HépatoExpérience du Centre Hépato--BiliaireBiliaire
2002 - 2003
13 patients : Age 43ans (10-66 ans)
Cirrhose : 3 patients
Hep Fulminante, PNF : 9 patients
MOF : 1 patient
Nbre de séances : 2,5 (1-8 séances)
Glasgow avant /après Mars : 5,8 + 2 / 7,7 + 4
Vivants 9/13 pts (70%)
TH : 8/13 (61%) Cirrhose : 2/3
HF : 6/9
MOF : 1/1

Le système MARS a prouvé son efficacité dans l‘épuration de nombreuxsubstances toxiques au cours de l‘insuffisance hépatique aigue
hydrosoluble : ammoniac, lactate, creatinine , urea
liposolubles : bilirubine, acides biliaires, acides aminésaromatiques, triglycérides à chaînes courtes etmoyennes, etc.
Dans l‘amélioration de la survie de ces patients
CONCLUSION