etude de la perfusion placentaire par irm...
TRANSCRIPT
ETUDE DE LA PERFUSION PLACENTAIRE PAR IRM DYNAMIQUE (DCE IRM) CHEZ LA RATE « L-NAME »,
MODELE DE PREECLAMPSIE ET RETARD DE CROISSANCE INTRA-UTERIN
Marie lémery Magnin, Victor Fitoussi, Nathalie Siauve, Laetitia Pidial, Daniel Balvay, Gwennhael Autret, Charles André Cuenod, Olivier Clément, Laurent J Salomon
- Laboratoire de recherche en imagerie PARCC U970 -
PLAN
Rappels Embryologie humaine et comparaison du placenta humain versus
placenta murin
Rôle du placenta, implications pathologiques
Modalités d’exploration du placenta et de sa pathologie
Modèle et technique utilisés Modèle animal utilisé : la rate « L-NAME »
Technique d’imagerie utilisée : l’IRM dynamique par injection de gadolinium sur une IRM 4,7T dédiée petit animal
Matériel et méthodes
Résultats
Discussion
Conclusion
Embryologie humaine
Similarités et différences
placentaire humain versus murin
Rappels
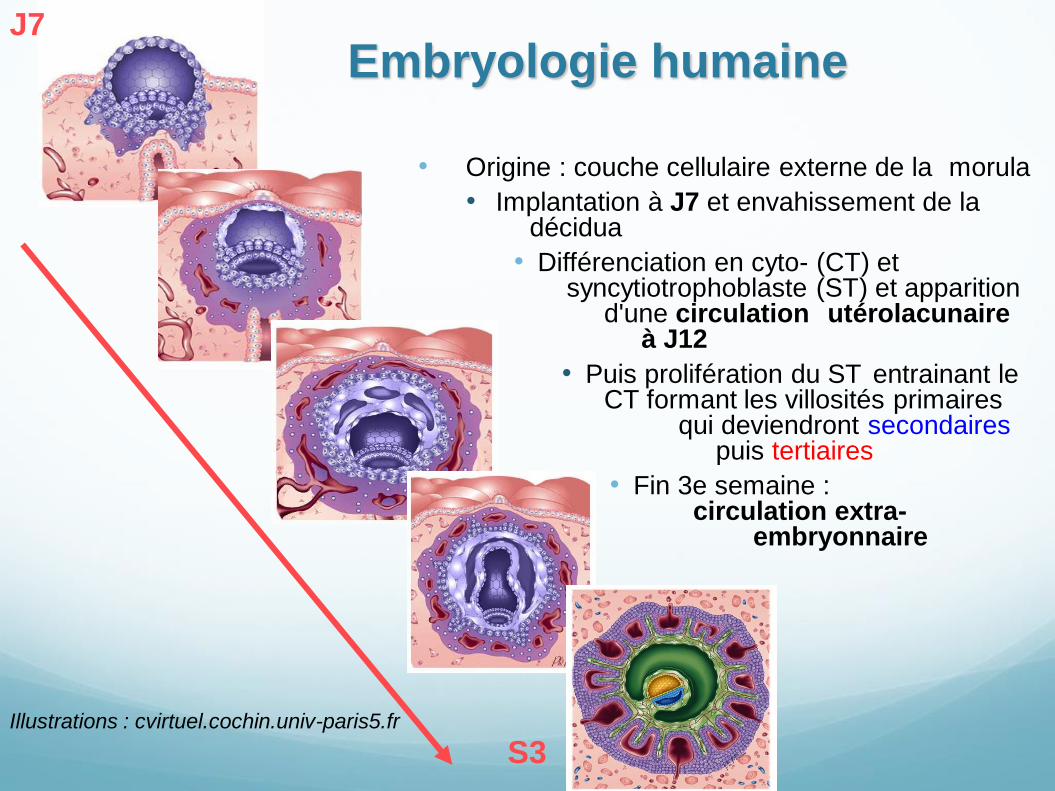
• Origine : couche cellulaire externe de la morula
• Implantation à J7 et envahissement de la décidua
• Différenciation en cyto- (CT) et syncytiotrophoblaste (ST) et apparition d'une circulation utérolacunaire à J12
• Puis prolifération du ST entrainant le CT formant les villosités primaires qui deviendront secondaires puis tertiaires
• Fin 3e semaine : circulation extra- embryonnaire
Embryologie humaine J7
S3 Illustrations : cvirtuel.cochin.univ-paris5.fr
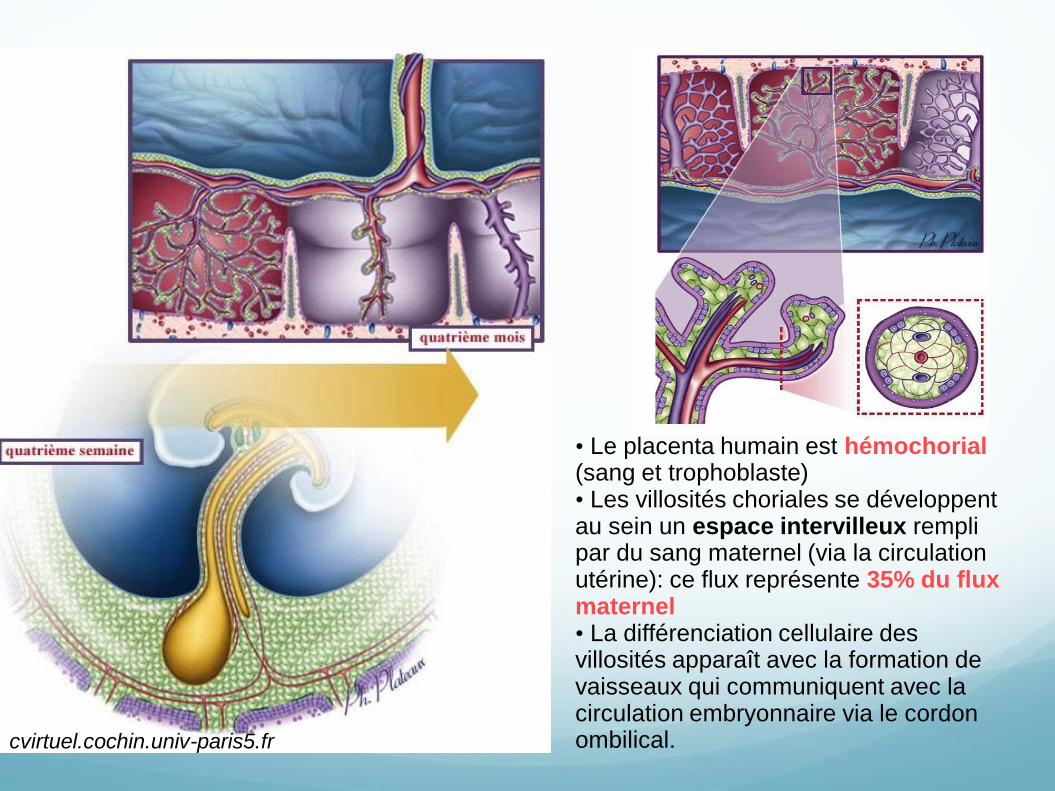
• Le placenta humain est hémochorial (sang et trophoblaste) • Les villosités choriales se développent au sein un espace intervilleux rempli par du sang maternel (via la circulation utérine): ce flux représente 35% du flux maternel • La différenciation cellulaire des villosités apparaît avec la formation de vaisseaux qui communiquent avec la circulation embryonnaire via le cordon ombilical. cvirtuel.cochin.univ-paris5.fr
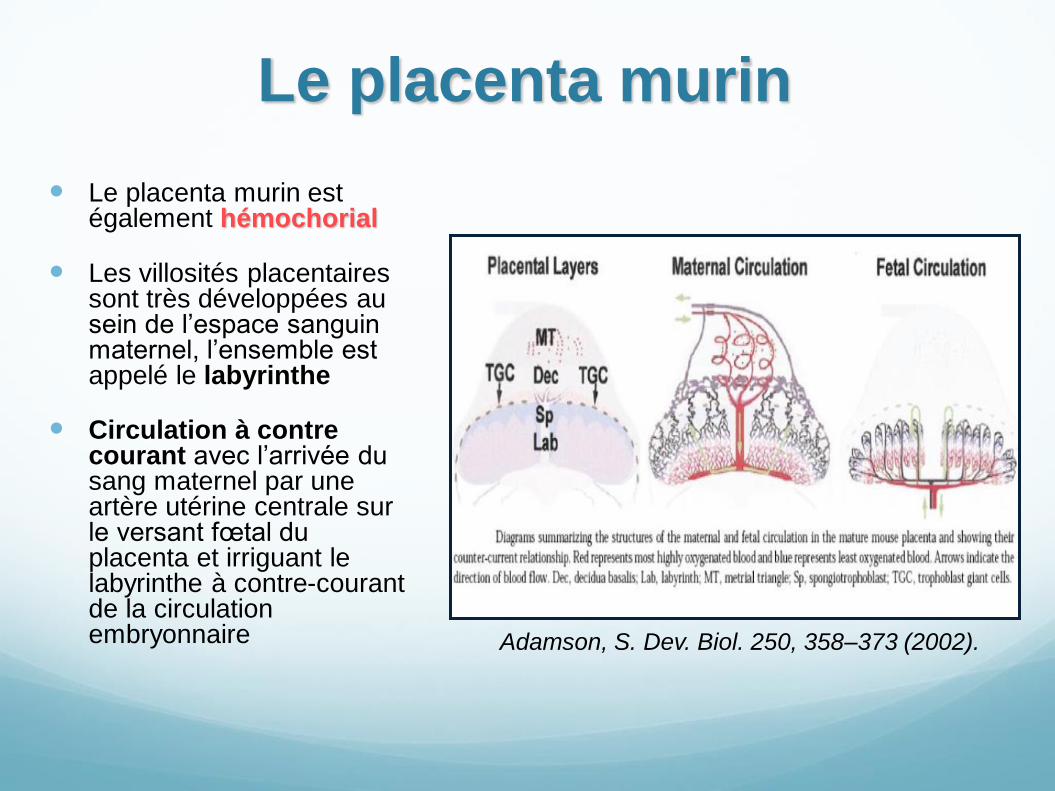
Le placenta murin
Le placenta murin est également hémochorial
Les villosités placentaires sont très développées au sein de l’espace sanguin maternel, l’ensemble est appelé le labyrinthe
Circulation à contre courant avec l’arrivée du sang maternel par une artère utérine centrale sur le versant fœtal du placenta et irriguant le labyrinthe à contre-courant de la circulation embryonnaire Adamson, S. Dev. Biol. 250, 358–373 (2002).
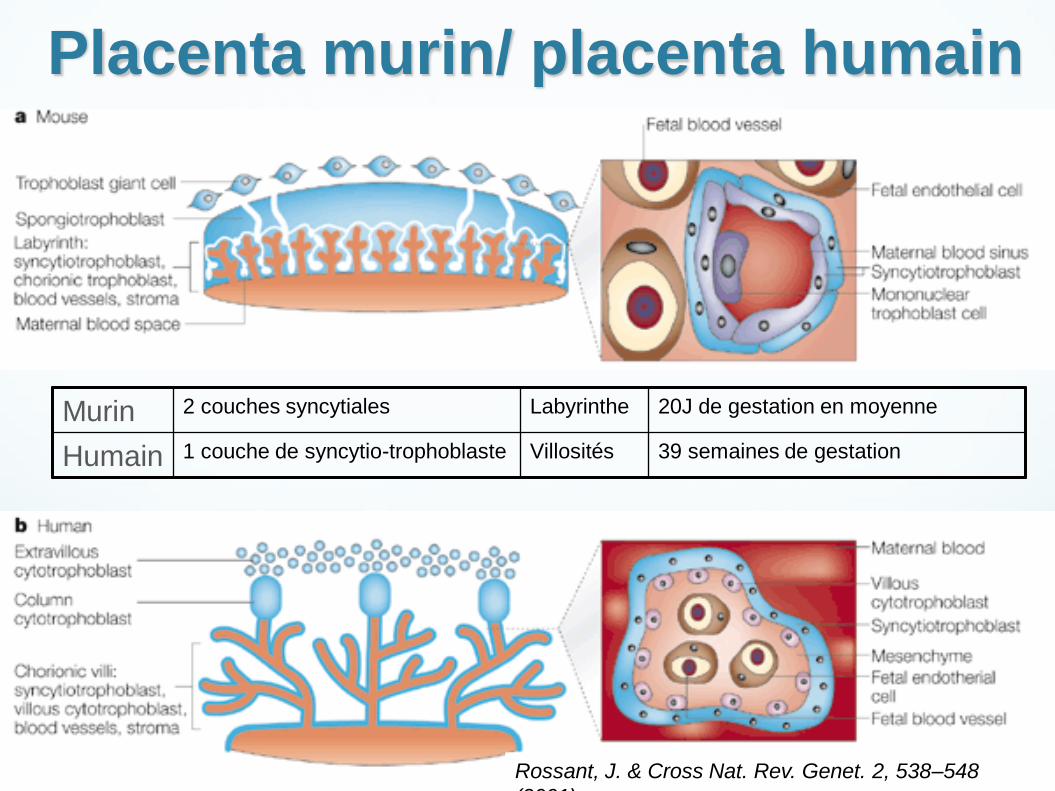
Placenta murin/ placenta humain
Rossant, J. & Cross Nat. Rev. Genet. 2, 538–548
(2001)
Murin 2 couches syncytiales Labyrinthe 20J de gestation en moyenne
Humain 1 couche de syncytio-trophoblaste Villosités 39 semaines de gestation
Rôle du placenta et implications
pathologiques
Rappels
Rôle du placenta
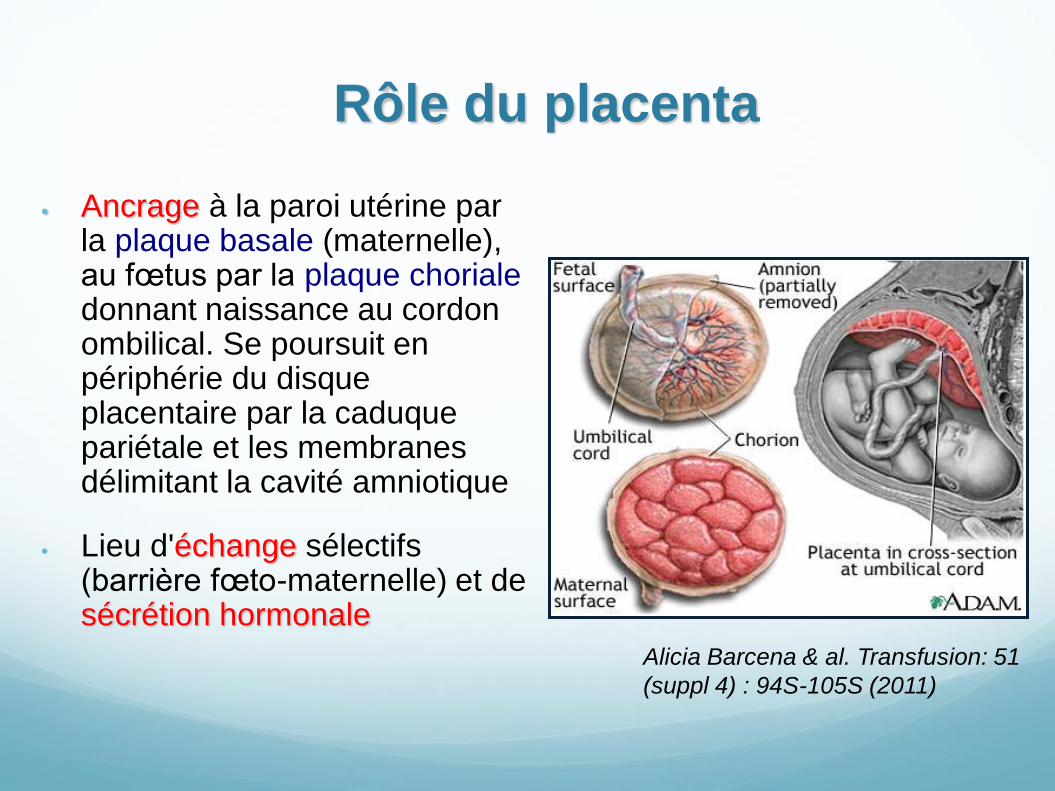
Ancrage à la paroi utérine par la plaque basale (maternelle), au fœtus par la plaque choriale donnant naissance au cordon ombilical. Se poursuit en périphérie du disque placentaire par la caduque pariétale et les membranes délimitant la cavité amniotique
Lieu d'échange sélectifs (barrière fœto-maternelle) et de sécrétion hormonale
Alicia Barcena & al. Transfusion: 51
(suppl 4) : 94S-105S (2011)
Implications pathologiques
Anomalies positionnelles
Placenta praevia,
Placenta accreta, percreta
Insuffisance placentaire :
Prééclampsie (PE),
Retard de croissance intra-utérin (RCIU) 3 à 10% des grossesses
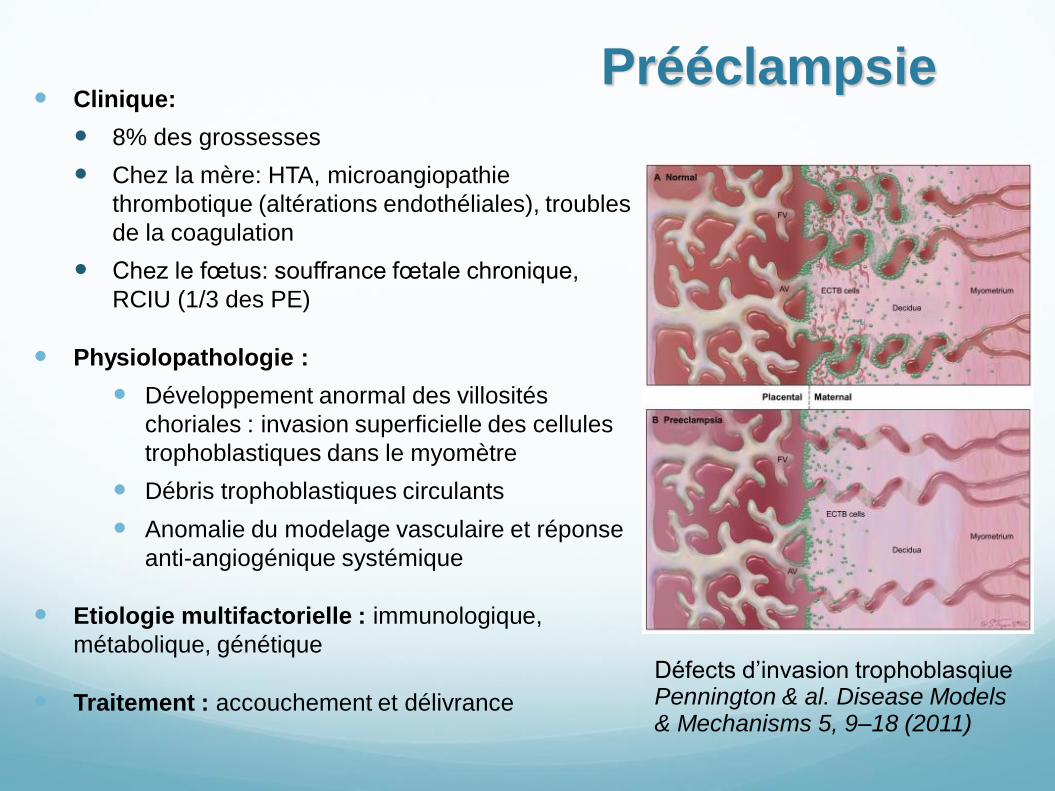
Prééclampsie Clinique:
8% des grossesses
Chez la mère: HTA, microangiopathie
thrombotique (altérations endothéliales), troubles
de la coagulation
Chez le fœtus: souffrance fœtale chronique,
RCIU (1/3 des PE)
Physiolopathologie :
Développement anormal des villosités
choriales : invasion superficielle des cellules
trophoblastiques dans le myomètre
Débris trophoblastiques circulants
Anomalie du modelage vasculaire et réponse
anti-angiogénique systémique
Etiologie multifactorielle : immunologique,
métabolique, génétique
Traitement : accouchement et délivrance
Défects d’invasion trophoblasqiue Pennington & al. Disease Models & Mechanisms 5, 9–18 (2011)
Modalités d’exploration du
placenta et de sa pathologie
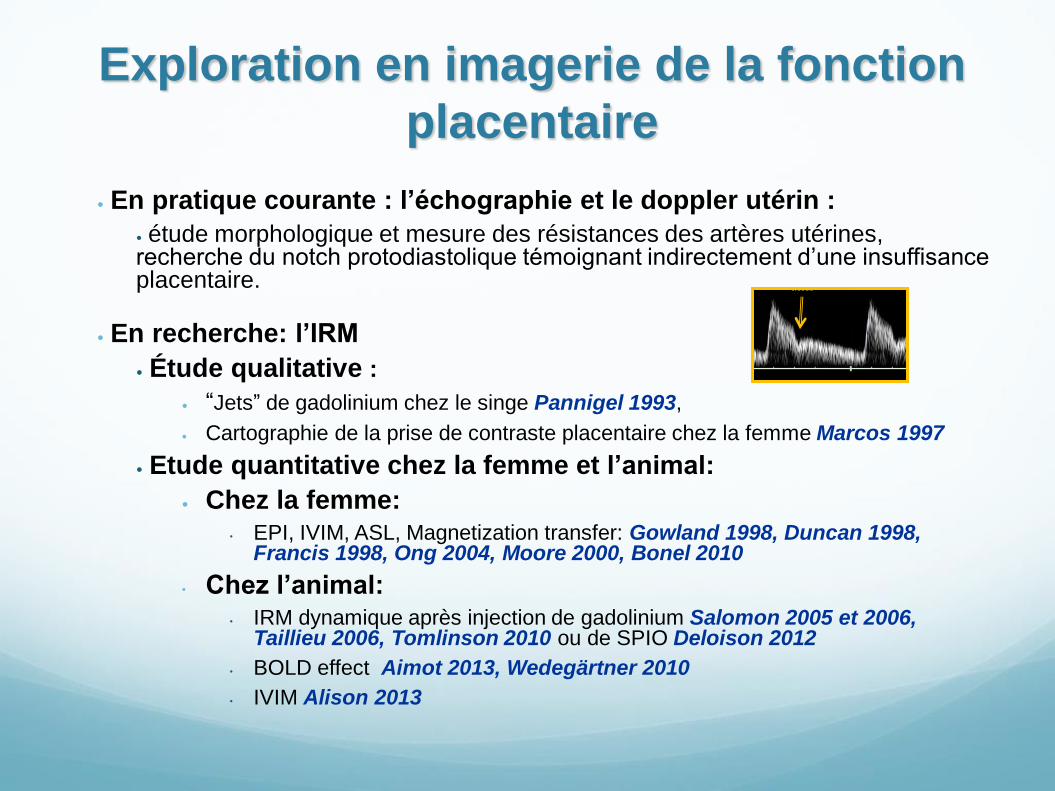
Exploration en imagerie de la fonction
placentaire
En pratique courante : l’échographie et le doppler utérin :
étude morphologique et mesure des résistances des artères utérines, recherche du notch protodiastolique témoignant indirectement d’une insuffisance placentaire.
En recherche: l’IRM
Étude qualitative :
“Jets” de gadolinium chez le singe Pannigel 1993,
Cartographie de la prise de contraste placentaire chez la femme Marcos 1997
Etude quantitative chez la femme et l’animal:
Chez la femme: • EPI, IVIM, ASL, Magnetization transfer: Gowland 1998, Duncan 1998,
Francis 1998, Ong 2004, Moore 2000, Bonel 2010
• Chez l’animal: • IRM dynamique après injection de gadolinium Salomon 2005 et 2006,
Taillieu 2006, Tomlinson 2010 ou de SPIO Deloison 2012
• BOLD effect Aimot 2013, Wedegärtner 2010
• IVIM Alison 2013
Exploration de la fonction
placentaire en recherche (IRM)
Ces études ont permis d’évaluer la perfusion
placentaire moyenne chez l’homme entre 128 et
180mL/min/100mL
Dans les études sur modèle animal de prééclampsie
et/ou retard de croissance intra-utérin, il a été démontré
une réduction d’environ 30% des taux de perfusion
placentaire en situation pathologique
Modèles animaux d’insuffisance
placentaire Modèles ischémiques (noradrénaline, modèle de Wiggleworth, etc.)
Ces modèles ont déjà été étudié en imagerie par IRM
Manipulations génétiques (eNOS knock out, transgénique p57kip2, etc.)
Modèles immunologiques (anti TNF-α, Th1-like cells, etc.)
Inductions pharmacologiques (LNAME, etc.)
Autres (hypoxie, dénutrition, hyperactivité sympatique, etc.)
Aucun modèle existant n'est le miroir exact de la prééclampsie qui est une pathologie strictement humaine La réduction de l'invasion trophoblastique caractéristique n’est en général pas retrouvée chez l'animal
MAIS
Modèle utilisé : la rate
« LNAME »
LNAME : L-Nitro Arginine Méthyl Ester
Rôle de l’oxyde nitrique (NO)
Le NO est fabriqué par la NO synthase (NOS)
Rôle :
Vasodilatateur local : régulation de la perfusion, interaction avec les autres agents
vasoactifs (VEGF et ses récepteurs VEGFR-1 (Flt-1 et Flk-1), TGF b-1, Ang-1 et 2)
effets directs sur la cellule musculaire lisse
indirects en inhibant la production d'agents vasoconstricteurs.
Rôle dans la vasculogénèse, l’angiogénèse et la maturation vasculaire:
dès le 7ème jour de développement, induit la différenciation des cellules
mésodermiques extra-embryonnaires pour former les premiers plexus capillaires
l’inhibition des NOS s’accompagnent d’une angiogénèse déficiente dans l’embryon
et le placenta avec diminution de la différenciation et de la maturation et
désorganisation vasculaire.
Chez la femme enceinte :
Augmentation des métabolites du NO dans le cordon ombilical et le placenta des
RCIU
Variation des taux de NOS dans les villosités choriales et dans les vaisseaux
ombilicaux des placentas de PE et RCIU
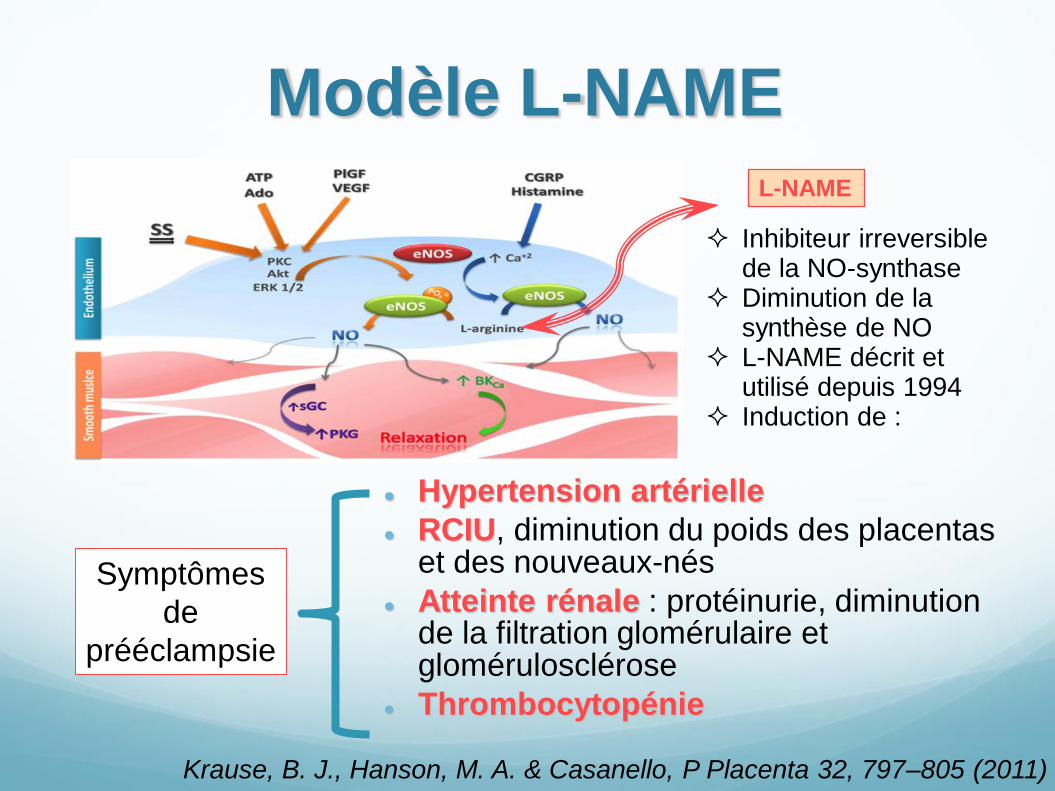
Modèle L-NAME
Hypertension artérielle
RCIU, diminution du poids des placentas et des nouveaux-nés
Atteinte rénale : protéinurie, diminution de la filtration glomérulaire et glomérulosclérose
Thrombocytopénie
L-NAME
Inhibiteur irreversible de la NO-synthase
Diminution de la synthèse de NO
L-NAME décrit et utilisé depuis 1994
Induction de :
Symptômes
de
prééclampsie
Krause, B. J., Hanson, M. A. & Casanello, P Placenta 32, 797–805 (2011)
Dynamic contrast enhanced
(DCE) IRM après injection de
gadolinium
Technique d’imagerie utilisée
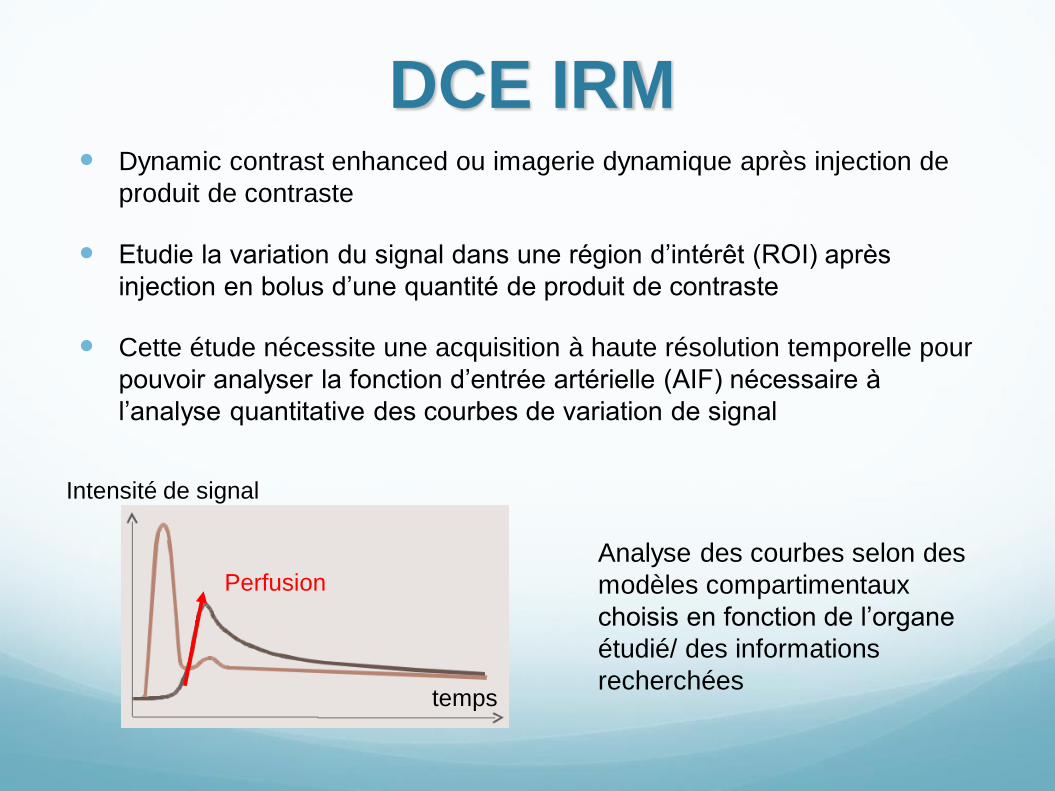
DCE IRM Dynamic contrast enhanced ou imagerie dynamique après injection de
produit de contraste
Etudie la variation du signal dans une région d’intérêt (ROI) après
injection en bolus d’une quantité de produit de contraste
Cette étude nécessite une acquisition à haute résolution temporelle pour
pouvoir analyser la fonction d’entrée artérielle (AIF) nécessaire à
l’analyse quantitative des courbes de variation de signal
temps
Intensité de signal
Perfusion
Analyse des courbes selon des
modèles compartimentaux
choisis en fonction de l’organe
étudié/ des informations
recherchées

Matériel et méthodes
Etude
Préparation du modèle
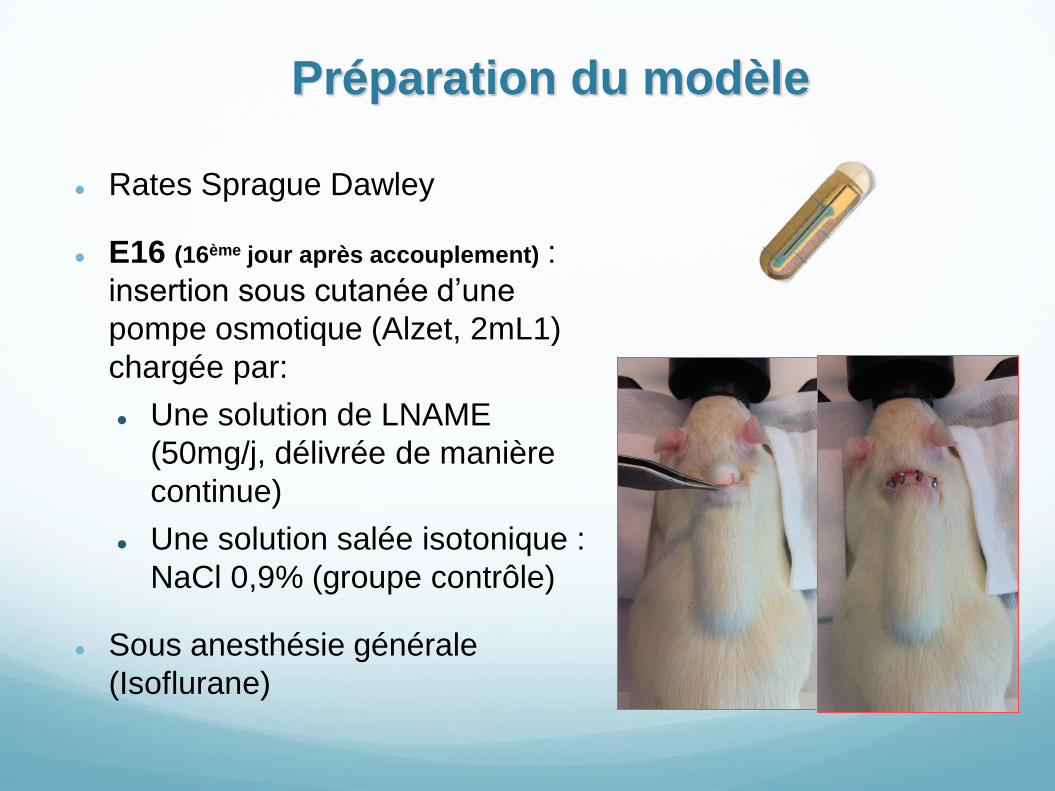
Rates Sprague Dawley
E16 (16ème jour après accouplement) :
insertion sous cutanée d’une
pompe osmotique (Alzet, 2mL1)
chargée par:
Une solution de LNAME
(50mg/j, délivrée de manière
continue)
Une solution salée isotonique :
NaCl 0,9% (groupe contrôle)
Sous anesthésie générale
(Isoflurane)
Préparation de l’IRM
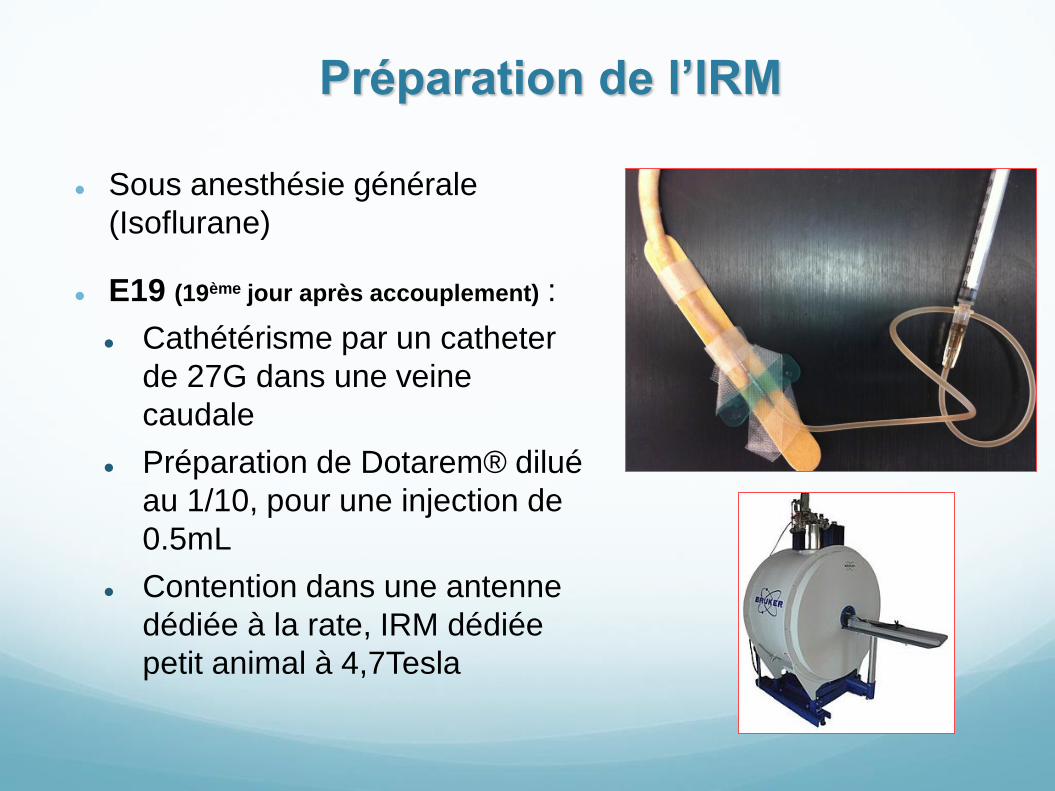
Sous anesthésie générale
(Isoflurane)
E19 (19ème jour après accouplement) :
Cathétérisme par un catheter
de 27G dans une veine
caudale
Préparation de Dotarem® dilué
au 1/10, pour une injection de
0.5mL
Contention dans une antenne
dédiée à la rate, IRM dédiée
petit animal à 4,7Tesla
Protocole d’IRM : DCE IRM
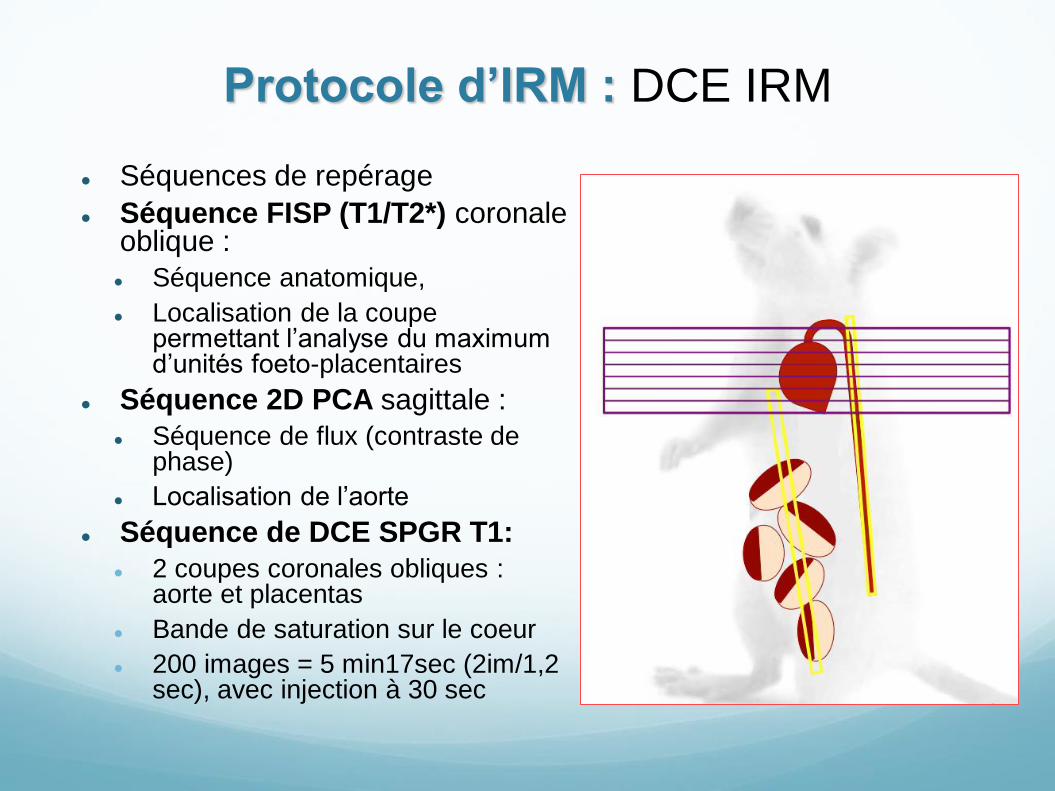
Séquences de repérage
Séquence FISP (T1/T2*) coronale oblique :
Séquence anatomique,
Localisation de la coupe permettant l’analyse du maximum d’unités foeto-placentaires
Séquence 2D PCA sagittale :
Séquence de flux (contraste de phase)
Localisation de l’aorte
Séquence de DCE SPGR T1:
2 coupes coronales obliques : aorte et placentas
Bande de saturation sur le coeur
200 images = 5 min17sec (2im/1,2 sec), avec injection à 30 sec
Césarienne et étude des unités foeto-
placentaires
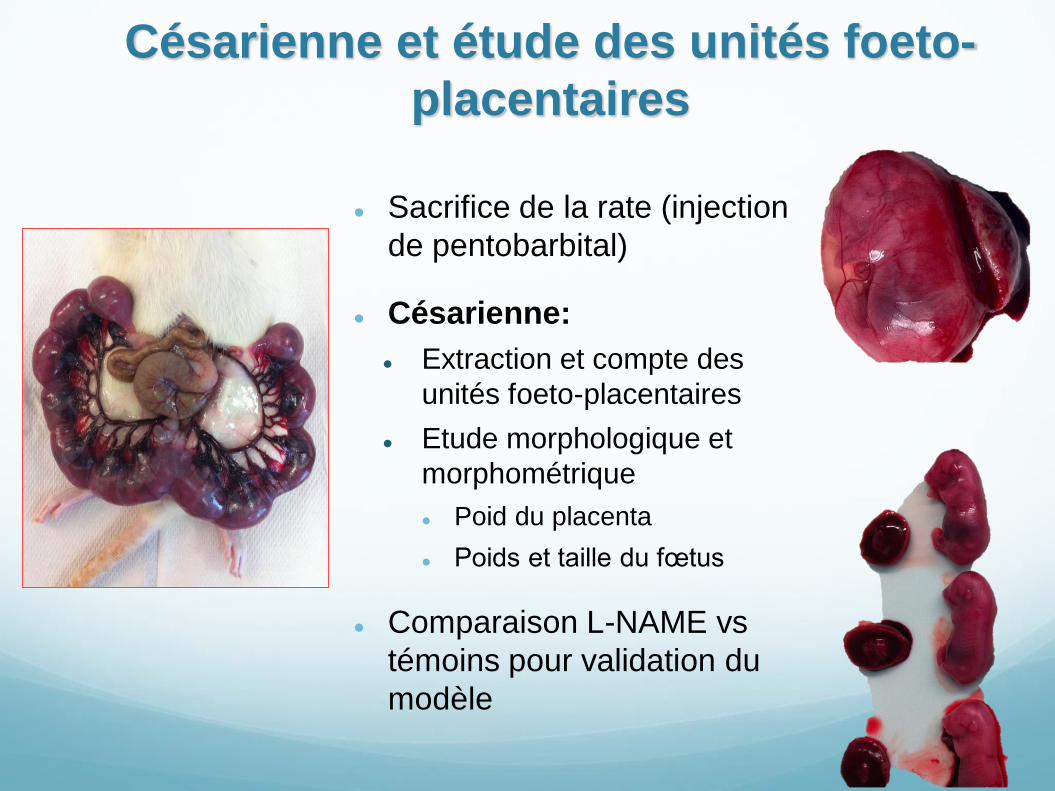
Sacrifice de la rate (injection
de pentobarbital)
Césarienne:
Extraction et compte des
unités foeto-placentaires
Etude morphologique et
morphométrique
Poid du placenta
Poids et taille du fœtus
Comparaison L-NAME vs
témoins pour validation du
modèle
Analyse des
données
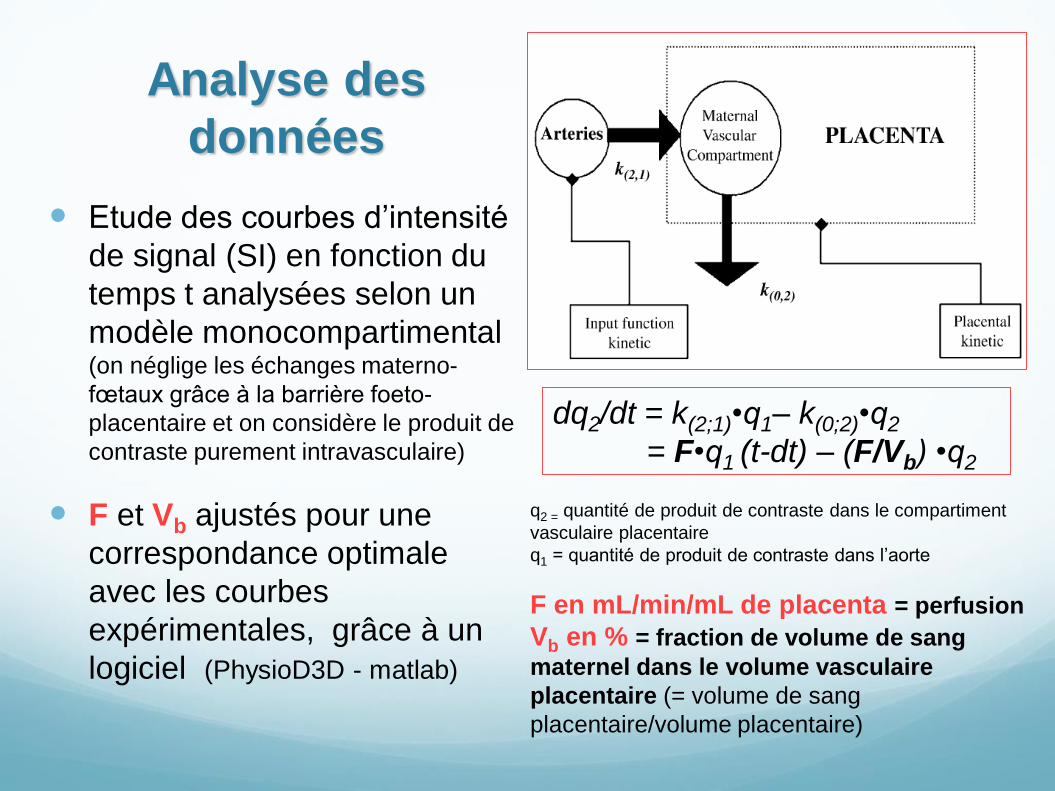
Etude des courbes d’intensité
de signal (SI) en fonction du
temps t analysées selon un
modèle monocompartimental (on néglige les échanges materno-
fœtaux grâce à la barrière foeto-
placentaire et on considère le produit de
contraste purement intravasculaire)
F et Vb ajustés pour une
correspondance optimale
avec les courbes
expérimentales, grâce à un
logiciel (PhysioD3D - matlab)
q2 = quantité de produit de contraste dans le compartiment
vasculaire placentaire
q1 = quantité de produit de contraste dans l’aorte
F en mL/min/mL de placenta = perfusion
Vb en % = fraction de volume de sang
maternel dans le volume vasculaire
placentaire (= volume de sang
placentaire/volume placentaire)
dq2/dt = k(2;1)•q1– k(0;2)•q2
= F•q1 (t-dt) – (F/Vb) •q2
Résultats
Etude
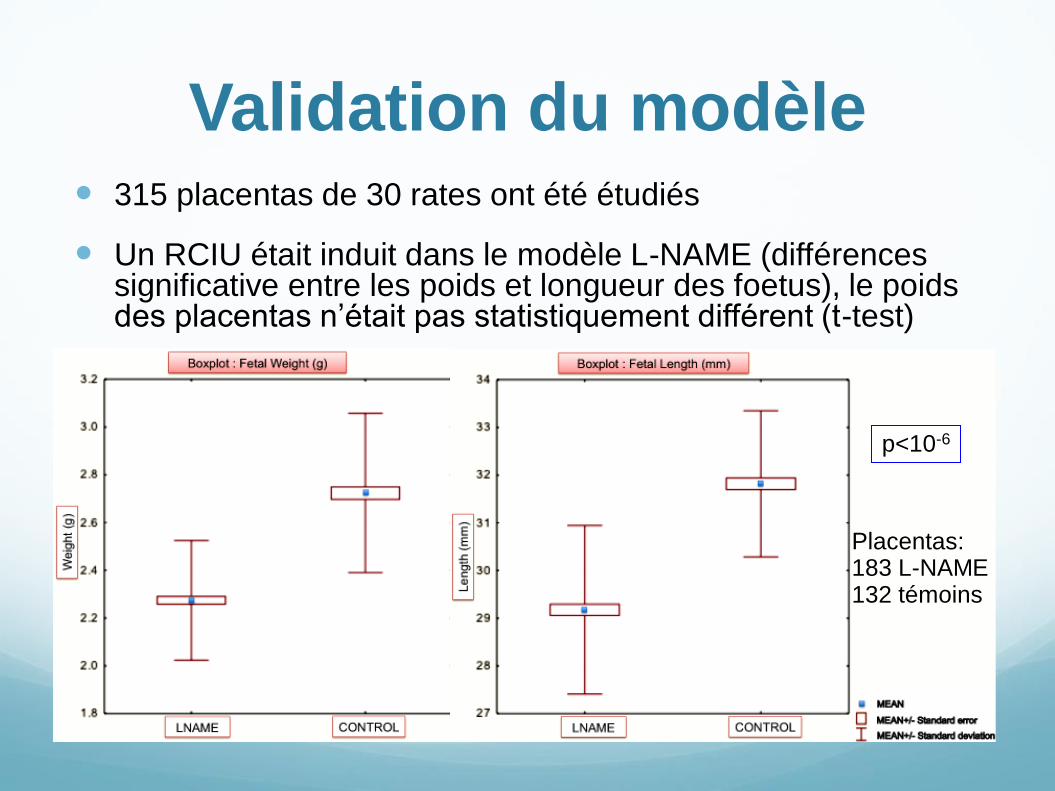
Validation du modèle 315 placentas de 30 rates ont été étudiés
Un RCIU était induit dans le modèle L-NAME (différences significative entre les poids et longueur des foetus), le poids des placentas n’était pas statistiquement différent (t-test)
p<10-6
Placentas: 183 L-NAME 132 témoins
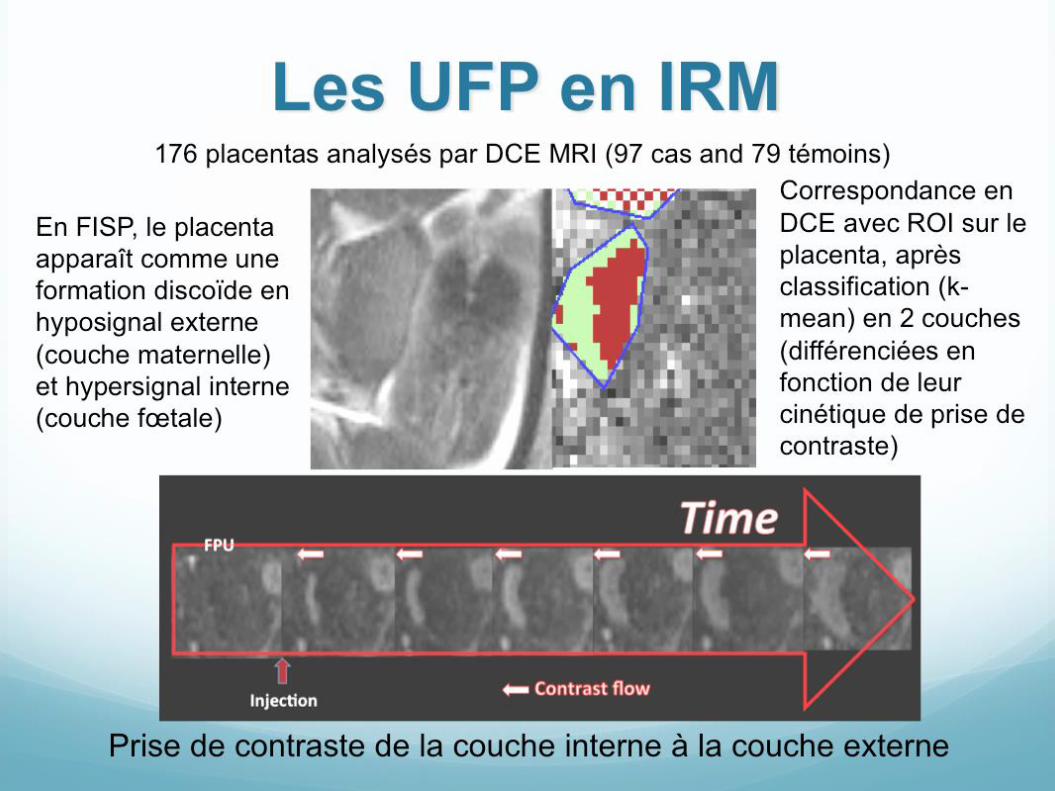
Les UFP en IRM
En FISP, le placenta
apparaît comme une
formation discoïde en
hyposignal externe
(couche maternelle)
et hypersignal interne
(couche fœtale)
Correspondance en
DCE avec ROI sur le
placenta, après
classification (k-
mean) en 2 couches
(différenciées en
fonction de leur
cinétique de prise de
contraste)
Prise de contraste de la couche interne à la couche externe
176 placentas analysés par DCE MRI (97 cas and 79 témoins)
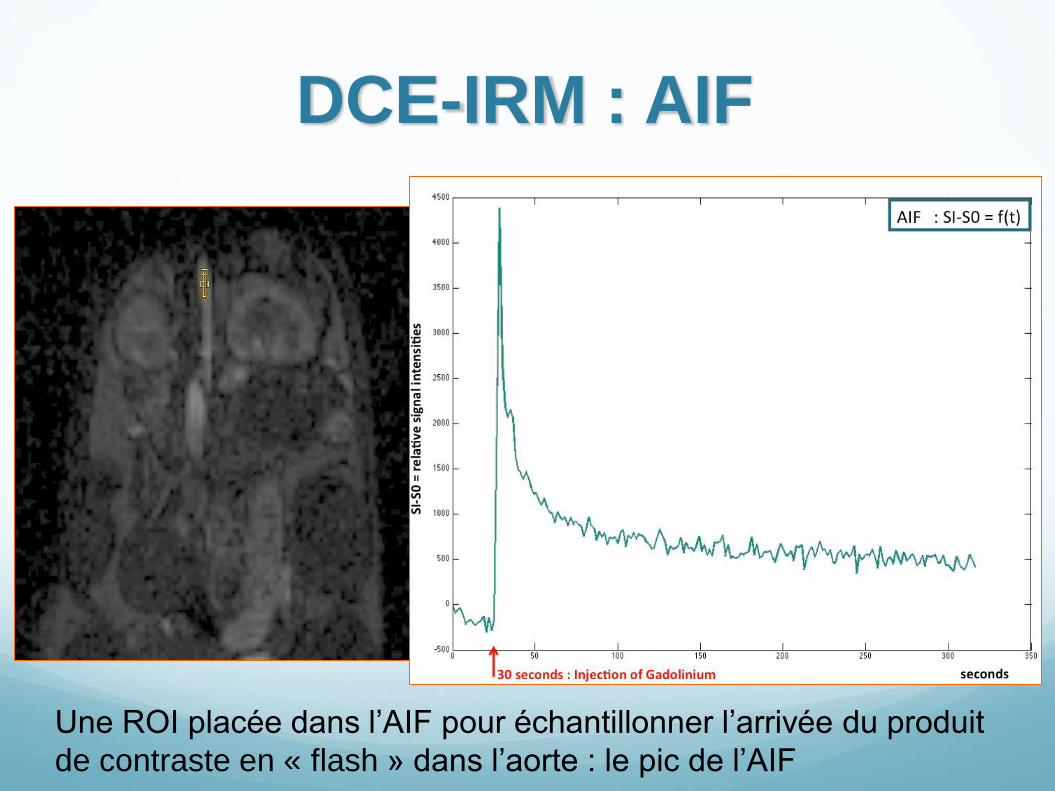
DCE-IRM : AIF
Une ROI placée dans l’AIF pour échantillonner l’arrivée du produit
de contraste en « flash » dans l’aorte : le pic de l’AIF
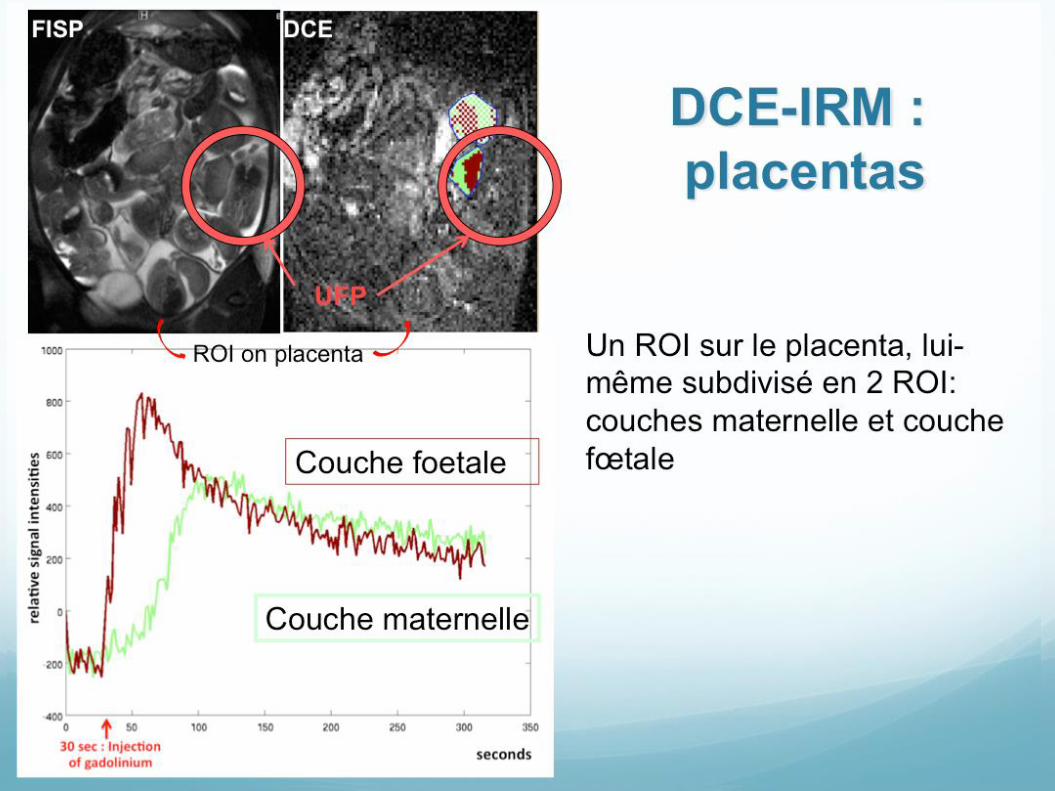
UFP
FISP DCE
Couche foetale
Couche maternelle
ROI on placenta Un ROI sur le placenta, lui-
même subdivisé en 2 ROI:
couches maternelle et couche
fœtale
DCE-IRM :
placentas
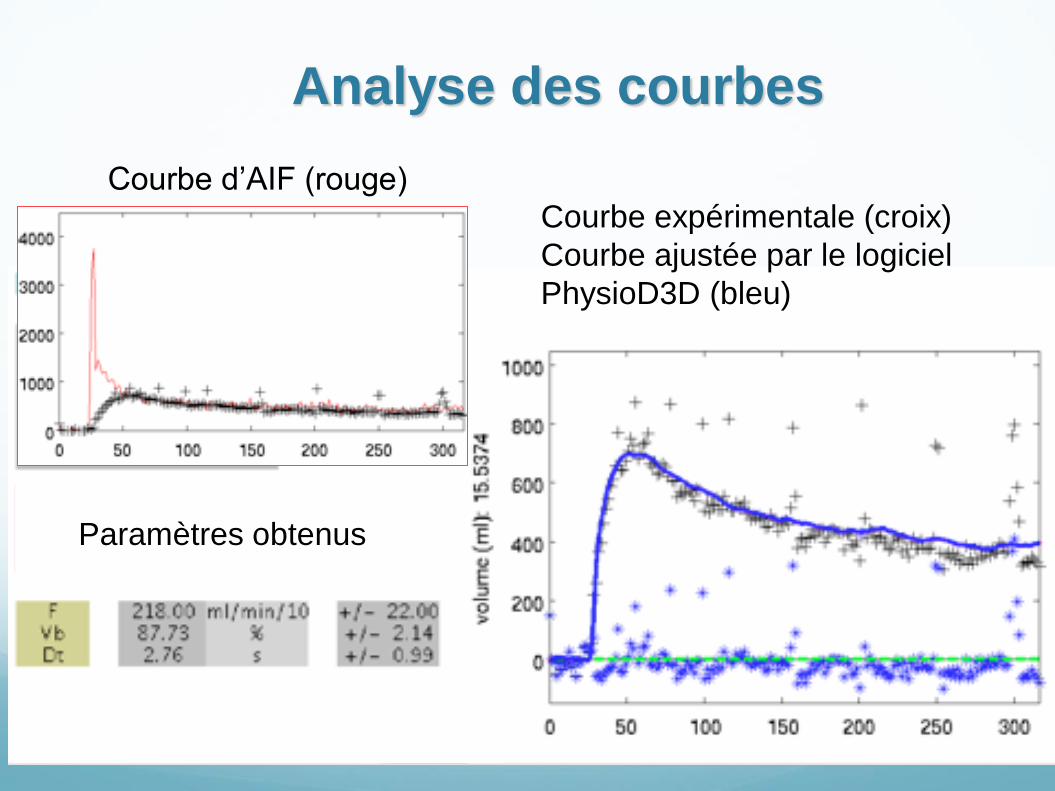
Analyse des courbes
Courbe d’AIF (rouge)
Courbe expérimentale (croix)
Courbe ajustée par le logiciel
PhysioD3D (bleu)
Paramètres obtenus
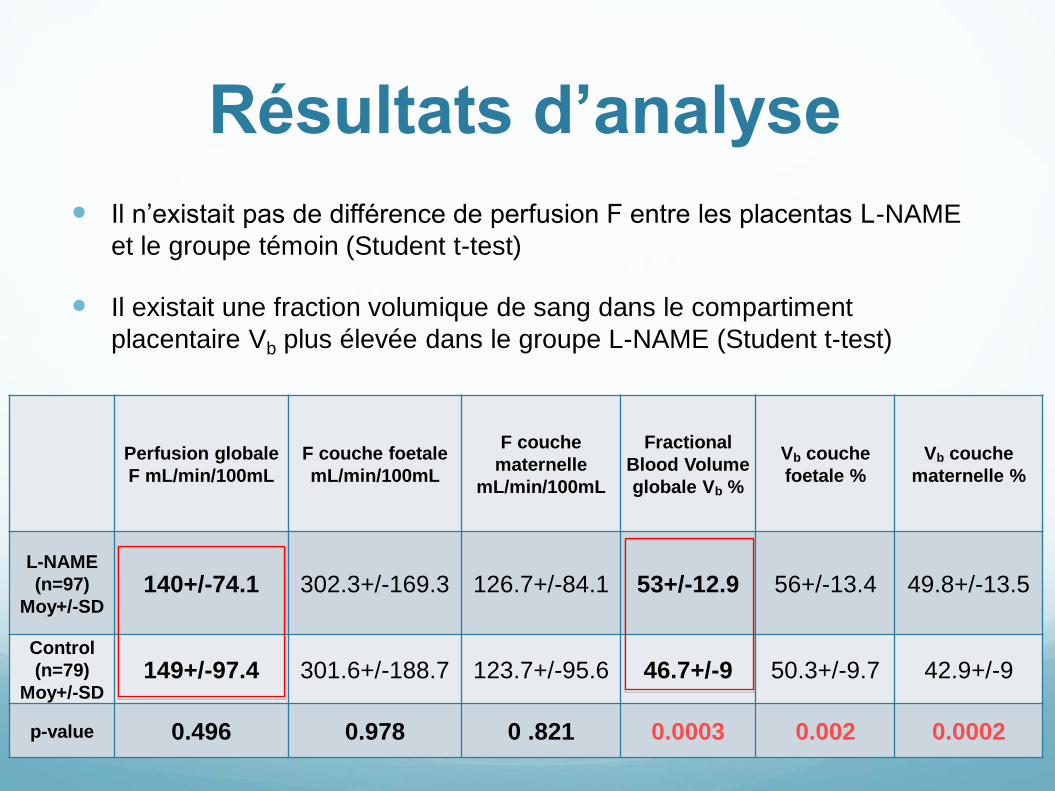
Résultats d’analyse
Il n’existait pas de différence de perfusion F entre les placentas L-NAME
et le groupe témoin (Student t-test)
Il existait une fraction volumique de sang dans le compartiment
placentaire Vb plus élevée dans le groupe L-NAME (Student t-test)
Perfusion globale
F mL/min/100mL F couche foetale
mL/min/100mL
F couche
maternelle
mL/min/100mL
Fractional
Blood Volume
globale Vb %
Vb couche
foetale % Vb couche
maternelle %
L-NAME
(n=97)
Moy+/-SD 140+/-74.1 302.3+/-169.3 126.7+/-84.1 53+/-12.9 56+/-13.4 49.8+/-13.5
Control
(n=79)
Moy+/-SD 149+/-97.4 301.6+/-188.7 123.7+/-95.6 46.7+/-9 50.3+/-9.7 42.9+/-9
p-value 0.496 0.978 0 .821 0.0003 0.002 0.0002
Discussion
Etude
Discussion
F est similaire aux valeurs de la littérature, comparable dans les deux
groupes
Les conséquences du modèle L-NAME, malgré son action vasogénique, ne
sont pas expliquées par une simple hypoperfusion placentaire
Certaines études proposent un rôle immunologique (apoptose accrue et
implication du TNF-α) de la voie du NO
Vb est plus élevé dans le groupe L-NAME
Témoignant potentiellement d’une raréfaction des villosités trophoblastiques
dans le modèle LNAME
Cette hypothèse concorde avec ce qui a déjà été décrit dans un modèle
LNAME en histologie (Tsukimori 2010)
Limites principales :
Pas de monitoring de la TA et de la protéinurie, mais le modèle L-NAME est
éprouvé et était efficace dans notre étude (RCIU)
Comparaison non faite (très difficile) entre le placenta en IRM et le placenta
ex vivo donc pas de possibilité de faire concorder les placentas de RCIU et
ceux avec un Vb élevé.
Conclusion
Etude
CONCLUSION La PE et le RCIU ne sont pas toujours la conséquence
d’une hypoperfusion placentaire
Implications multifactorielle de la voie du NO
Les symptômes de prééclampsie et le RCIU induits par le modèle L-NAME
sont d’étiologie multifactorielle et la réduction du volume villositaire
placentaire traduite par une augmentation de la fraction volumique sanguine
placentaire pourrait être à leur origine.
L’IRM fonctionnelle présente un intérêt indéniable dans la
compréhension de la dysfonction placentaire pendant la
grossesse
La faisabilité et la reproductibilité de la DCE IRM sont à l’étude chez la femme
(Placentimage, essai clinique dirigé par le Pr L. Salomon).
L’utilisation de gadolinium chez la femme enceinte reste controversée bien
qu’aucun effet indésirable n’ait été démontré à ce jour
Bibliographie Pennington, K. A., Schlitt, J. M., Jackson, D. L., Schulz, L. C. & Schust, D. J. Preeclampsia: multiple approaches for a multifactorial disease. Disease Models &
Mechanisms 5, 9–18 (2011).
Rossant, J. & Cross, J. C. Placental development: lessons from mouse mutants. Nat. Rev. Genet. 2, 538–548 (2001).
Adamson, S. L. et al. Interactions between trophoblast cells and the maternal and fetal circulation in the mouse placenta. Dev. Biol. 250, 358–373 (2002).
McCarthy, F. P., Kingdom, J. C., Kenny, L. C. & Walsh, S. K. Animal models of preeclampsia; uses and limitations. Placenta 32, 413–419 (2011).
Molnár, M., Sütö, T., Tóth, T. & Hertelendy, F. Prolonged blockade of nitric oxide synthesis in gravid rats produces sustained hypertension, proteinuria,
thrombocytopenia, and intrauterine growth retardation. Am. J. Obstet. Gynecol. 170, 1458–1466 (1994).
Krause, B. J., Hanson, M. A. & Casanello, P. Role of nitric oxide in placental vascular development and function. Placenta 32, 797–805 (2011).
Panigel, M. et al. Fast scan magnetic resonance imaging and Doppler ultrasonography of uteroplacental hemodynamics in the rhesus monkey (Macaca mulatta). J. Med.
Primatol. 22, 393–399 (1993).
Marcos, H. B., Semelka, R. C. & Worawattanakul, S. Normal placenta: gadolinium-enhanced dynamic MR imaging. Radiology 205, 493–496 (1997).
Duncan, K. R. et al. The investigation of placental relaxation and estimation of placental perfusion using echo-planar magnetic resonance imaging. Placenta 19, 539–543
(1998).
Francis, S. T. et al. Non-invasive mapping of placental perfusion. Lancet 351, 1397–1399 (1998).
Moore, R. J. et al. In vivo intravoxel incoherent motion measurements in the human placenta using echo-planar imaging at 0.5 T. Magn Reson Med 43, 295–302 (2000).
Salomon, L. J. et al. Placental Perfusion MR Imaging with Contrast Agents in a Mouse Model. Radiology 235, 73–80 (2005).
Salomon, L. J. et al. In Vivo Dynamic MRI Measurement of the Noradrenaline-induced Reduction in Placental Blood Flow in Mice. Placenta 27, 1007–1013 (2006).
Taillieu F, Salomon LJ, Siauve N, Clement O, Faye N, Balvay D, et al. Placental Perfusion and Permeability: Simultaneous Assessment with Dual-Echo Contrast-
enhanced MR Imaging in Mice. Radiology;241:737–45 (2006).
Deloison B, Siauve N, Aimot S, Balvay D, Thiam R, Cuenod C, et al. SPIO-enhanced magnetic resonance imaging study of placental perfusion in a rat model of
intrauterine growth restriction. BJOG: An International Journal of Obstetrics & Gynaecology;119:626–33 (2012).
Alison M, Quibel T, Balvay D, Autret G, Bourillon C, Chalouhi GE, et al. Measurement of placental perfusion by dynamic contrast-enhanced MRI at 4.7 T. Invest
Radiol;48:535–42 (2013).
Alison M, Chalouhi GE, Autret G, Balvay D, Thiam R, Salomon LJ, et al. Use of intravoxel incoherent motion MR imaging to assess placental perfusion in a murine
model of placental insufficiency. Invest Radiol ;48:17–23 (2013).
Tomlinson TM, Garbow JR, Anderson JR, Engelbach JA, Nelson DM, Sadovsky Y. Magnetic resonance imaging of hypoxic injury to the murine placenta. AJP:
Regulatory, Integrative and Comparative Physiology ;298:R312–R319 (2009)
Chalouhi GE, Alison M, Deloison B, Thiam R, Autret G, Balvay D, et al. Fetoplacental Oxygenation in an Intrauterine Growth Restriction Rat Model by Using Blood
Oxygen Level-Dependent MR Imaging at 4.7 T. Radiology (2013).
Aimot-Macron S, Salomon LJ, Deloison B, Thiam R, Cuenod CA, Clement O, et al. In vivo MRI assessment of placental and foetal oxygenation changes in a rat model
of growth restriction using blood oxygen level-dependent (BOLD) magnetic resonance imaging. Eur Radiol;23:1335–42 (2013).
Bonel, H. M. et al. Diffusion-weighted MR Imaging of the Placenta in Fetuses with Placental Insufficiency. Radiology 257, 810–819 (2010).
Gowland, P. . et al. In Vivo Relaxation Time Measurements in the Human Placenta Using Echo Planar Imaging at 0.5 T. Magnetic Resonance Imaging 16, 241–247
(1998).
Ong, S. Functional Magnetic Resonance Imaging (Magnetization Transfer) and Stereological Analysis of Human Placentae in Normal Pregnancy and in Pre-eclampsia
and Intrauterine Growth Restriction. Placenta 25, 408–412 (2004).
Chalouhi, G. E. et al. Dynamic contrast-enhanced magnetic resonance imaging: definitive imaging of placental function? Seminars in Fetal and Neonatal Medicine 16,
22–28 (2011).
Tsukimori, K. et al. Inhibition of nitric oxide synthetase at mid-gestation in rats is associated with increases in arterial pressure, serum tumor necrosis factor-alpha, and
placental apoptosis. Am. J. Hypertens. 21, 477–481 (2008).
1. Hertig, A. Maternal Serum sFlt1 Concentration Is an Early and Reliable Predictive Marker of Preeclampsia.
Clinical Chemistry 50, 1702–1703 (2004).
2. Pennington, K. A., Schlitt, J. M., Jackson, D. L., Schulz, L. C. & Schust, D. J. Preeclampsia: multiple
approaches for a multifactorial disease. Disease Models & Mechanisms 5, 9–18 (2011).
3. Kaufmann, P. Endovascular Trophoblast Invasion: Implications for the Pathogenesis of Intrauterine Growth
Retardation and Preeclampsia. Biology of Reproduction 69, 1–7 (2003).
4. Roberts, J. M. & Hubel, C. A. The Two Stage Model of Preeclampsia: Variations on the Theme. Placenta
30, 32–37 (2009).
5. Levine, R. J. et al. Circulating angiogenic factors and the risk of preeclampsia. N. Engl. J. Med. 350, 672–
683 (2004).
6. Odibo, A. O. et al. Placental volume and vascular flow assessed by 3D power Doppler and adverse
pregnancy outcomes. Placenta 32, 230–234 (2011).
7. Ordén, M. R., Gudmundsson, S. & Kirkinen, P. Intravascular ultrasound contrast agent: an aid in imaging
intervillous blood flow? Placenta 20, 235–240 (1999).
8. Ogawa, M. et al. Elastography for differentiation of subchorionic hematoma and placenta previa.
Ultrasound Obstet Gynecol 39, 112–114 (2012).
9. Panigel, M. et al. Fast scan magnetic resonance imaging and Doppler ultrasonography of uteroplacental
hemodynamics in the rhesus monkey (Macaca mulatta). J. Med. Primatol. 22, 393–399 (1993).
10. Marcos, H. B., Semelka, R. C. & Worawattanakul, S. Normal placenta: gadolinium-enhanced dynamic MR
imaging. Radiology 205, 493–496 (1997).
11. Duncan, K. R. et al. The investigation of placental relaxation and estimation of placental perfusion using
echo-planar magnetic resonance imaging. Placenta 19, 539–543 (1998).
12. Francis, S. T. et al. Non-invasive mapping of placental perfusion. Lancet 351, 1397–1399 (1998).
13. Moore, R. J. et al. In vivo intravoxel incoherent motion measurements in the human placenta using echo-
planar imaging at 0.5 T. Magn Reson Med 43, 295–302 (2000).
14. Salomon, L. J. et al. Placental Perfusion MR Imaging with Contrast Agents in a Mouse Model. Radiology
235, 73–80 (2005).
15. Salomon, L. J. et al. In Vivo Dynamic MRI Measurement of the Noradrenaline-induced Reduction in
Placental Blood Flow in Mice. Placenta 27, 1007–1013 (2006).
16. Taillieu, F. et al. Placental Perfusion and Permeability: Simultaneous Assessment with Dual-Echo Contrast-
enhanced MR Imaging in Mice. Radiology 241, 737–745 (2006).
17. Deloison, B. et al. SPIO-enhanced magnetic resonance imaging study of placental perfusion in a rat model
of intrauterine growth restriction. BJOG: An International Journal of Obstetrics & Gynaecology 119, 626–633
(2012).
18. WIGGLESWORTH, J. S. EXPERIMENTAL GROWTH RETARDATION IN THE FOETAL RAT. J Pathol
Bacteriol 88, 1–13 (1964).
19. Tomlinson, T. M. et al. Magnetic resonance imaging of hypoxic injury to the murine placenta. AJP:
Regulatory, Integrative and Comparative Physiology 298, R312–R319 (2009).
20. Aimot, S. et al. Evaluation of the blood oxygen level dependent (BOLD) effect in MR imaging of an intra
uterine growth restriction rat model. A new tool for placental imaging. (submitted)
21. Bonel, H. M. et al. Diffusion-weighted MR Imaging of the Placenta in Fetuses with Placental Insufficiency.
Radiology 257, 810–819 (2010).
22. Rossant, J. & Cross, J. C. Placental development: lessons from mouse mutants. Nat. Rev. Genet. 2,
538–548 (2001).
23. Adamson, S. L. et al. Interactions between trophoblast cells and the maternal and fetal circulation
in the mouse placenta. Dev. Biol. 250, 358–373 (2002).
24. McCarthy, F. P., Kingdom, J. C., Kenny, L. C. & Walsh, S. K. Animal models of preeclampsia; uses and
limitations. Placenta 32, 413–419 (2011).
25. Molnár, M., Sütö, T., Tóth, T. & Hertelendy, F. Prolonged blockade of nitric oxide synthesis in gravid rats
produces sustained hypertension, proteinuria, thrombocytopenia, and intrauterine growth retardation. Am. J.
Obstet. Gynecol. 170, 1458–1466 (1994).
26. Buhimschi, I., Yallampalli, C., Chwalisz, K. & Garfield, R. E. Pre-eclampsia-like conditions produced by
nitric oxide inhibition: effects of L-arginine, D-arginine and steroid hormones. Hum. Reprod. 10, 2723–2730
(1995).
27. Furchgott, R. F. & Zawadzki, J. V. The obligatory role of endothelial cells in the relaxation of arterial smooth
muscle by acetylcholine. Nature 288, 373–376 (1980).
28. Palmer, R. M., Ferrige, A. G. & Moncada, S. Nitric oxide release accounts for the biological activity of
endothelium-derived relaxing factor. Nature 327, 524–526 (1987).
29. Bogle, R. G., Moncada, S., Pearson, J. D. & Mann, G. E. Identification of inhibitors of nitric oxide synthase
that do not interact with the endothelial cell L-arginine transporter. Br. J. Pharmacol. 105, 768–770 (1992).
30. Inoue, Y. et al. Arginine transport in human liver. Characterization and effects of nitric oxide synthase
inhibitors. Ann. Surg. 218, 350–362; discussion 362–363 (1993).
31. Krause, B. J., Hanson, M. A. & Casanello, P. Role of nitric oxide in placental vascular development
and function. Placenta 32, 797–805 (2011).
32. Izumi, H., Yallampalli, C. & Garfield, R. E. Gestational changes in L-arginine-induced relaxation of pregnant
rat and human myometrial smooth muscle. Am. J. Obstet. Gynecol. 169, 1327–1337 (1993).
33. Yallampalli, C., Izumi, H., Byam-Smith, M. & Garfield, R. E. An L-arginine-nitric oxide-cyclic guanosine
monophosphate system exists in the uterus and inhibits contractility during pregnancy. Am. J. Obstet. Gynecol.
170, 175–185 (1994).
34. Lyall, F., Greer, I. A., Young, A. & Myatt, L. Nitric oxide concentrations are increased in the feto-placental
circulation in intrauterine growth restriction. Placenta 17, 165–168 (1996).
35. Chalouhi, G. E. et al. Dynamic contrast-enhanced magnetic resonance imaging: definitive imaging of
placental function? Seminars in Fetal and Neonatal Medicine 16, 22–28 (2011).
36. Diket, A. L. et al. Nitric oxide inhibition causes intrauterine growth retardation and hind-limb disruptions in
rats. Am. J. Obstet. Gynecol. 171, 1243–1250 (1994).
37. Fantel, A. G. et al. The teratogenicity of N(omega)-nitro-L-ariginine methyl ester (L-NAME), a nitric oxide
synthase inhibitor, in rats. Reprod. Toxicol. 11, 709–717 (1997).
38. Helmbrecht, G. D. et al. L-arginine reverses the adverse pregnancy changes induced by nitric oxide
synthase inhibition in the rat. Am. J. Obstet. Gynecol. 175, 800–805 (1996).
39. Chen, D., Wang, H., Huang, H. & Dong, M. Vascular endothelial growth factor attenuates Nomega-nitro-L-
arginine methyl ester-induced preeclampsia-like manifestations in rats. Clin. Exp. Hypertens. 30, 606–615
(2008).
40. Ma, R.-Q., Sun, M.-N. & Yang, Z. Inhibition of nitric oxide synthase lowers fatty acid oxidation in
preeclampsia-like mice at early gestational stage. Chin. Med. J. 124, 3141–3147 (2011).
41. Ramesar, S. V., Mackraj, I., Gathiram, P. & Moodley, J. Sildenafil citrate decreases sFlt-1 and sEng in
pregnant l-NAME treated Sprague-Dawley rats. Eur. J. Obstet. Gynecol. Reprod. Biol. 157, 136–140 (2011).
42. Sibai, B., Dekker, G. & Kupferminc, M. Pre-eclampsia. Lancet 365, 785–799 (2005).
43. Tsukimori, K. et al. Inhibition of nitric oxide synthetase at mid-gestation in rats is associated with increases
in arterial pressure, serum tumor necrosis factor-alpha, and placental apoptosis. Am. J. Hypertens. 21, 477–
481 (2008).
44. Gowland, P. . et al. In Vivo Relaxation Time Measurements in the Human Placenta Using Echo Planar
Imaging at 0.5 T. Magnetic Resonance Imaging 16, 241–247 (1998).
45. Ong, S. Functional Magnetic Resonance Imaging (Magnetization Transfer) and Stereological Analysis of
Human Placentae in Normal Pregnancy and in Pre-eclampsia and Intrauterine Growth Restriction. Placenta 25,
408–412 (2004).
46. Standley, C. A., Batia, L. & Yueh, G. Magnesium sulfate effectively reduces blood pressure in an animal
model of preeclampsia. Journal of Maternal-Fetal and Neonatal Medicine 19, 171–176 (2006).
47. Kaya, A. et al. The evaluation of hypoxia-inducible factor 1 in N-nitro-L-arginine methyl ester preeclampsia
model of pregnant rats. J. Investig. Med. 59, 1268–1272 (2011).
48. Weiner, C. P. & Thompson, L. P. Nitric oxide and pregnancy. Semin. Perinatol. 21, 367–380 (1997).
49. Conrad, K. P., Vill, M., McGuire, P. G., Dail, W. G. & Davis, A. K. Expression of nitric oxide synthase by
syncytiotrophoblast in human placental villi. FASEB J. 7, 1269–1276 (1993).
50. Yeh, B. M. Has the time arrived to image placental perfusion? Radiology 241, 633–634 (2006).
QUIZZ
La prééclampsie Est une pathologie liée à une insuffisance placentaire
Est une pathologie d’étiologie multifactorielle
Est de diagnostic clinique mais peut-être suspectée
grâce à l’imagerie
L’étude Doppler dans la prééclampsie permet une
analyse quantitative de la perfusion placentaire
La prééclampsie Est une pathologie liée à une insuffisance placentaire
Est une pathologie d’étiologie multifactorielle
Est de diagnostic clinique mais peut-être suspectée
grâce à l’imagerie (le doppler)
L’étude Doppler dans la prééclampsie permet une
analyse quantitative de la perfusion placentaire (critère
indirects, analyse qualitative)
Réponses justes
La DCE IRM Nécessite l’injection d’agent de contraste
Nécessite une acquisition à haute résolution temporelle
Permet l’étude de paramètres microcirculatoires
Est utilisée en pratique courante chez la femme
enceinte
La DCE IRM Nécessite l’injection d’agent de contraste (gadolinium
mais aussi SPIO)
Nécessite une acquisition à haute résolution temporelle
Permet l’étude de paramètres microcirculatoires
(notamment la perfusion, mais aussi la perméabilité)
Est utilisée en pratique courante chez la femme
enceinte (à l’étude dans un essai clinique,
Placentimage)
Réponses justes
L’étude de la perfusion
placentaire
N’est pas réalisable avec l’IRM de diffusion
N’est pas réalisable en échographie-doppler
N’est pas réalisée en pratique courante chez la femme
Est prometteuse pour la compréhension des
phénomènes de dysfonction placentaire pendant la
grossesse
L’étude de la perfusion
placentaire
N’est pas réalisable avec l’IRM de diffusion
N’est pas réalisable en échographie-doppler (étude
qualitative)
N’est pas réalisée en pratique courante chez la femme
Est prometteuse pour la compréhension des
phénomènes de dysfonction placentaire pendant la
grossesse
Réponses justes