evidence, platforms and priorities vani sethi, ph.d. child development and nutrition section unicef...
TRANSCRIPT

Evidence, Platforms and Priorities
Vani Sethi, Ph.D.Child Development and Nutrition Section
UNICEF India
Turning-around India’s Persistent Child Undernutrition Story
Improving Women’s Nutrition during preconception, during pregnancy
and lactation
What
Evidenceexists to advocate women’s nutrition?

EV
IDE
NC
E F
OR
W
OM
EN
NU
TR
ITIO
N
GU
IDE
LIN
ES

Lancet series on maternal child
nutrition(June, 2013)
EV
IDE
NC
E F
OR
W
OM
EN
NU
TR
ITIO
N

EvidenceKey take-aways

20
29
47
58 56 54 56
0-5 mo 6-11 mo 12-17 mo 18-23 mo 24-35 mo 36-47 mo 48-59 mo
India: 60% children 18-23 months are stunted
NFHS 3 mo = months

730 days270 days
Low Birth Weight
imaginary line
50% growth failure accrued by 24 months, occurs in womb
Proportion of children stunted as per NFHS-3 (%)
Peak foetal weight velocity occurs at around 30 wks
Peak foetal length velocity occurs at around 20 wks
Foetal stunting evident by 8 wks
P&PE Suppl. 2013, UNICEF 2013, Gillespie 1997
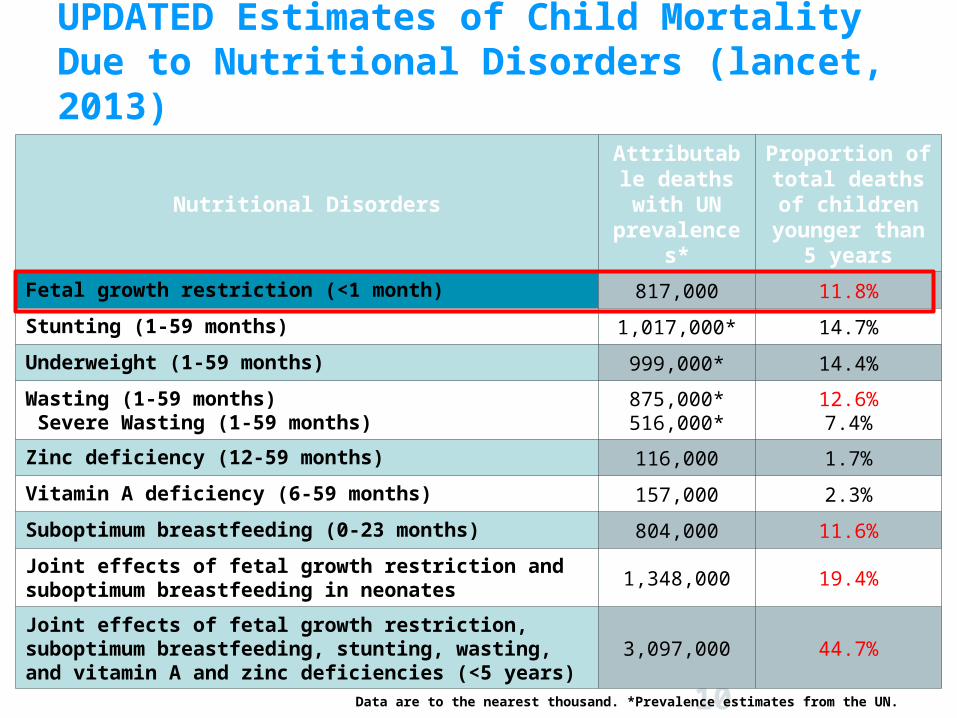
UPDATED Estimates of Child Mortality Due to Nutritional Disorders (lancet, 2013)
10
Nutritional Disorders
Attributable deaths with
UN prevalences*
Proportion of total deaths of
children younger than 5
years
Fetal growth restriction (<1 month) 817,000 11.8%
Stunting (1-59 months) 1,017,000* 14.7%
Underweight (1-59 months) 999,000* 14.4%
Wasting (1-59 months) Severe Wasting (1-59 months)
875,000*516,000*
12.6%7.4%
Zinc deficiency (12-59 months) 116,000 1.7%
Vitamin A deficiency (6-59 months) 157,000 2.3%
Suboptimum breastfeeding (0-23 months) 804,000 11.6%
Joint effects of fetal growth restriction and suboptimum breastfeeding in neonates
1,348,000 19.4%
Joint effects of fetal growth restriction, suboptimum breastfeeding, stunting, wasting, and vitamin A and zinc deficiencies (<5 years)
3,097,000 44.7%
Data are to the nearest thousand. *Prevalence estimates from the UN.
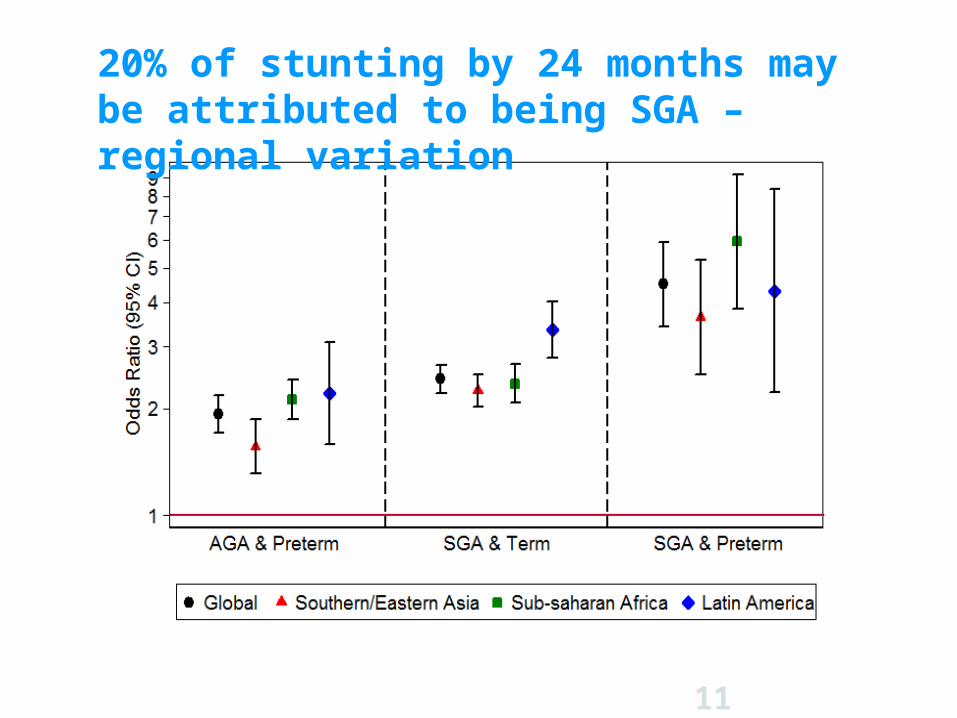
20% of stunting by 24 months may be attributed to being SGA – regional variation
11

LBW in India is largely driven by fetal growth restriction (Piwoz et al, 2013)
12
Total live births in India = 27.2M
N= 0.9M (3%)
N= 0.8M (3%)
N= 1.8M (7%)
N= 6.9M (25%)
N= 5.8M (21%)
N= 11.0M (40%)
% of total live births
Low Birth Weight (LBW) 28%
Small for Gestational Age (SGA)
47%
SGA, not LBW 25%
SGA, LBW 21%
Preterm (PT) 13%
PT & LBW 6%
PT, LBW & SGA 3%
PT, LBW & AGA 3%
Breakdown of live births in India
Source: CHERG, unpublished data
Diet in 1st trimester positively/negatively influence birth weight/length
Weight gain from 1st to 2nd trimester predicts infant length at birth
P&PE Suppl. 2013, Kramer et al, 1998, Gillespie, 1997
To improve foetal outcomes – Ideally intervene before pregnancy and no later than 1st trimester
Three major predictors of IUGR: Short maternal stature (maternal stunting) Low pre-pregnancy weight Poor weight gain during pregnancyOther: Non-nutrition factors (40 percent of pie)
Pre-pregnancy weight (+) weight gain during pregnancy have independent and additive effects on IUGR
Maternal micronutrient deficiencies (Iron, Vitamin A, Zinc, Iodine and Folate deficiency) negatively influence birth outcomes
IUGR: Intrauterine growth retardation
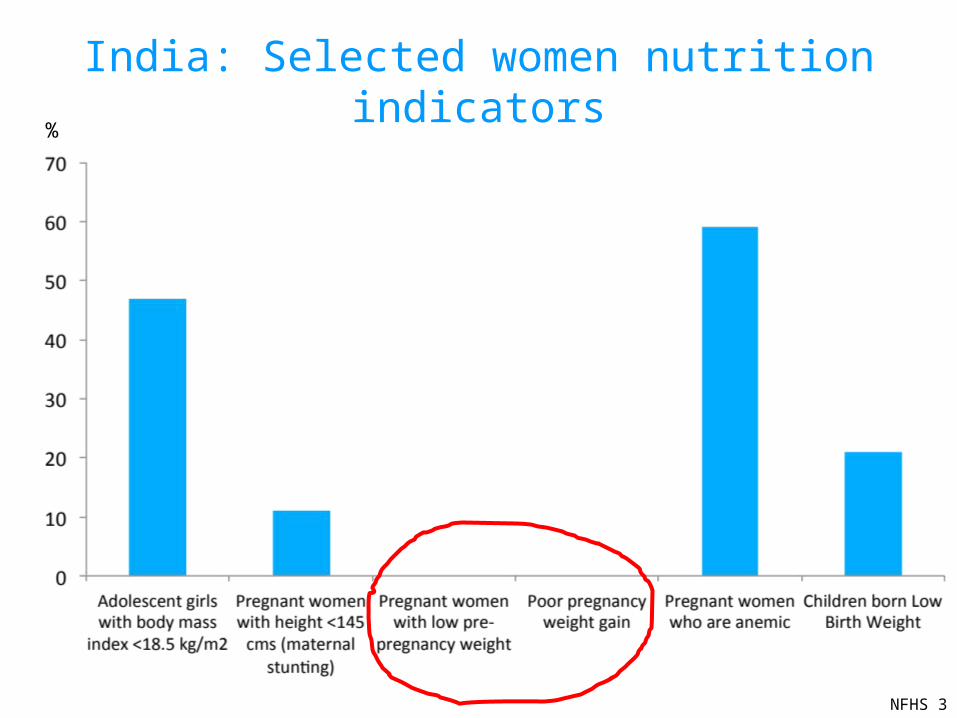
India: Selected women nutrition indicators
NFHS 3
%

Conceptual framework REACH
REACH: Conceptual framework to reduce stunting includes foetal growth faltering
High rates of stunting among under-fives
Foetal growth faltering Postnatal growth faltering
• Intrauterine growth retardation
• Premature childbirth
• Poor food and nutrient Intake• High rates of infections
• Poor maternal nutrition and care before and during pregnancy
• Poor access/utilization of health care services
• Household food insecurity• Poor infant feeding and care• Poor access/utilization of health
care services
Poor socioeconomic status and social norms
REACH: Renewed Effort Against Child Hunger and undernutrition
Directcauses
Underlyingcauses
Basiccauses

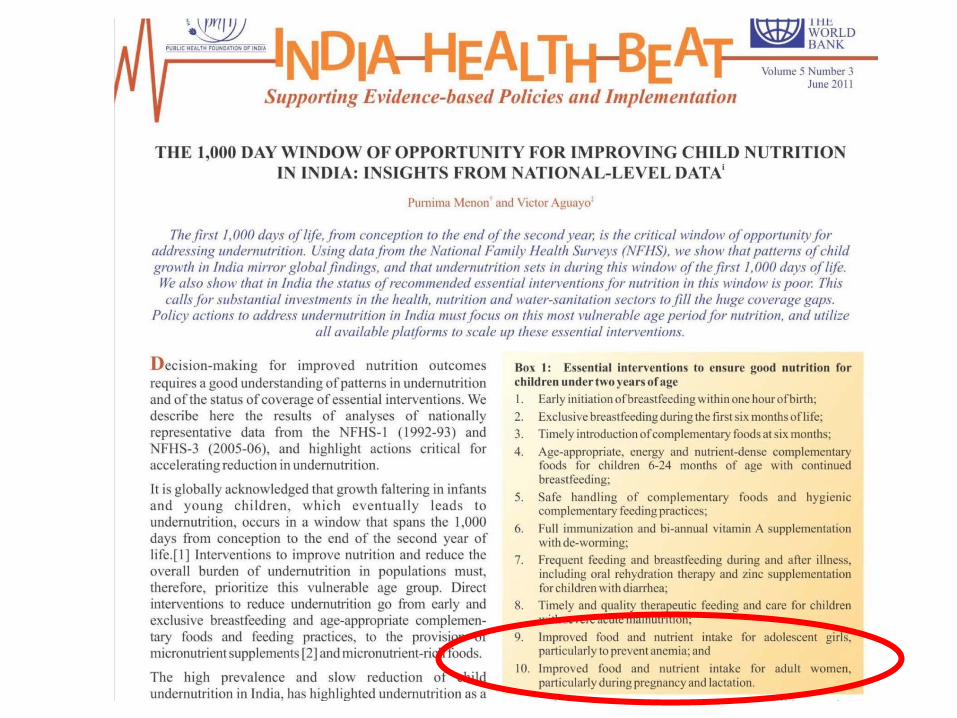
Improving women’s nutrition Improves her own
productively and health
Reduces maternal mortality risk
And What about the women herself …

focus on 4*54 Issues*5 Interventions
Evidence

4 Issues
2. Maternal thinness
Increase caloric intake Reduce energy expenditure Reduce caloric depletion (e.g., infections)
Increase birth weight Enhance infant growth Improve adolescent
growth
1. Maternal stunting
3. Micronutrient deficiencies and anemia
4. Female discrimination

Food consumed is adequate in quantity and nutrient quality1
i. Improve household access to generalized ration (through public distribution system)
ii. Improve access/use of ICDS micro-nutrient fortified supplementary food (to bridge calorie, protein, micronutrient gap)
iii. Devise community-based food security systems (as coping mechanisms)
iv. Access to knowledge to improve local diet, production and HH behaviours (work with influencers/families) Use of locally available nutrient dense micro-nutrient rich food Gender-sensitive intra-household food distribution Averting food related cultural beliefs and taboos
i. Iron and folic acid supplementation and deworming
ii. Universal use of iodized salt
iii. Malaria prevention and treatment, in malaria endemic zones
iv. Access to knowledge to stop using tobacco
v. pre- and peri conceptual folic acid
vi. Maternal calcium supplementation
vii. Maternal vitamin A supplement within 8 weeks after delivery
Prevent micronutrient deficiencies and anemia 2
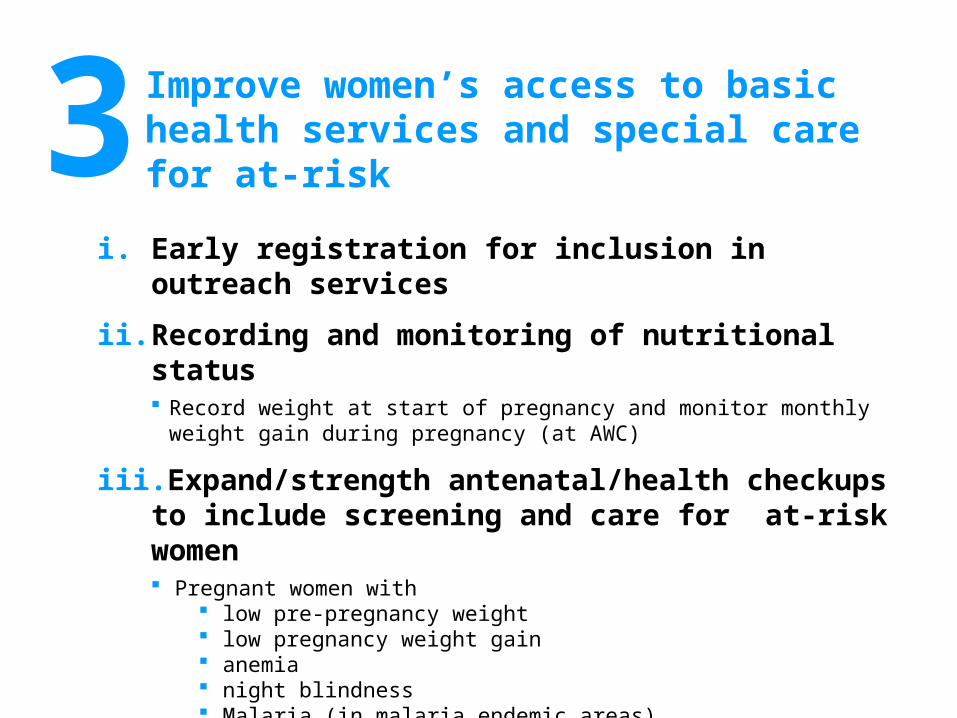
i. Early registration for inclusion in outreach services
ii. Recording and monitoring of nutritional status Record weight at start of pregnancy and monitor monthly weight gain during
pregnancy (at AWC)
iii. Expand/strength antenatal/health checkups to include screening and care for at-risk women Pregnant women with
low pre-pregnancy weight low pregnancy weight gain anemia night blindness Malaria (in malaria endemic areas)
iv. Universalize skilled facility-based delivery
Improve women’s access to basic health services and special care for at-risk3

i. Sanitation and hygiene education (including menstrual hygiene)
ii. Access to safe drinking water and improved sanitation facilities
Improve hygiene and sanitation practices and access to safe drinking water4

i. Ensuring marriage at/after legal age of 18 through awareness and incentivizing/compulsating secondary education for girls
ii. Family planning advice, incentives and options in pre-pregnancy (donot miss newly wed)
iii. Promoting community support system for women, their skill development and income earning potential
Preventing pregnancies – too early, too many and too soon5
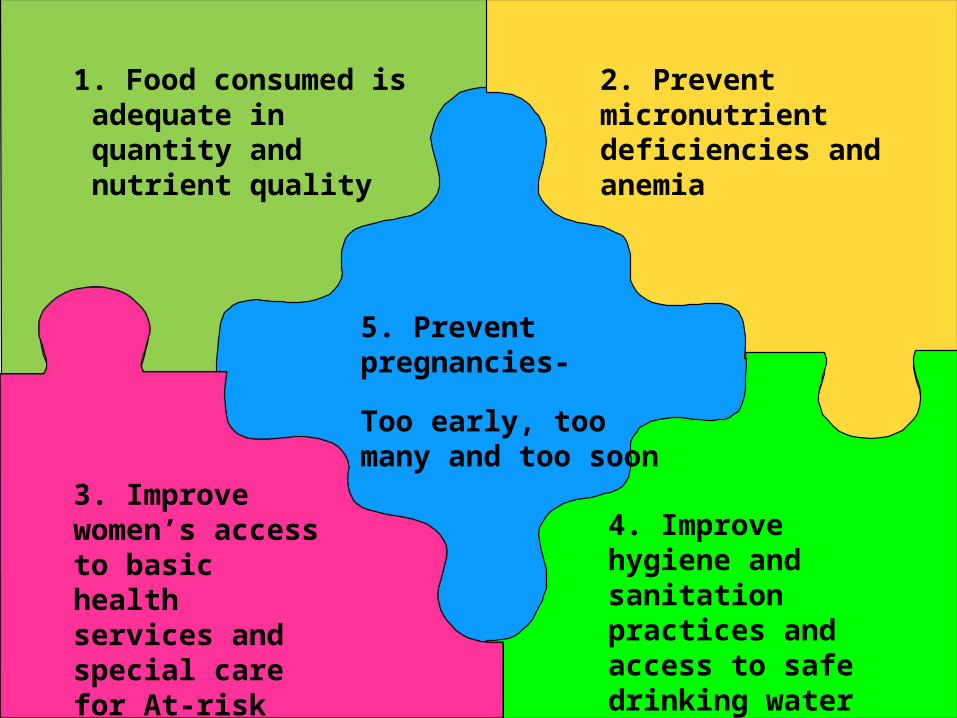
2. Prevent micronutrient deficiencies and anemia
1. Food consumed is adequate in quantity and nutrient quality
3. Improve women’s access to basic health services and special care for At-risk
4. Improve hygiene and sanitation practices and access to safe drinking water
5. Prevent pregnancies-
Too early, too many and too soon
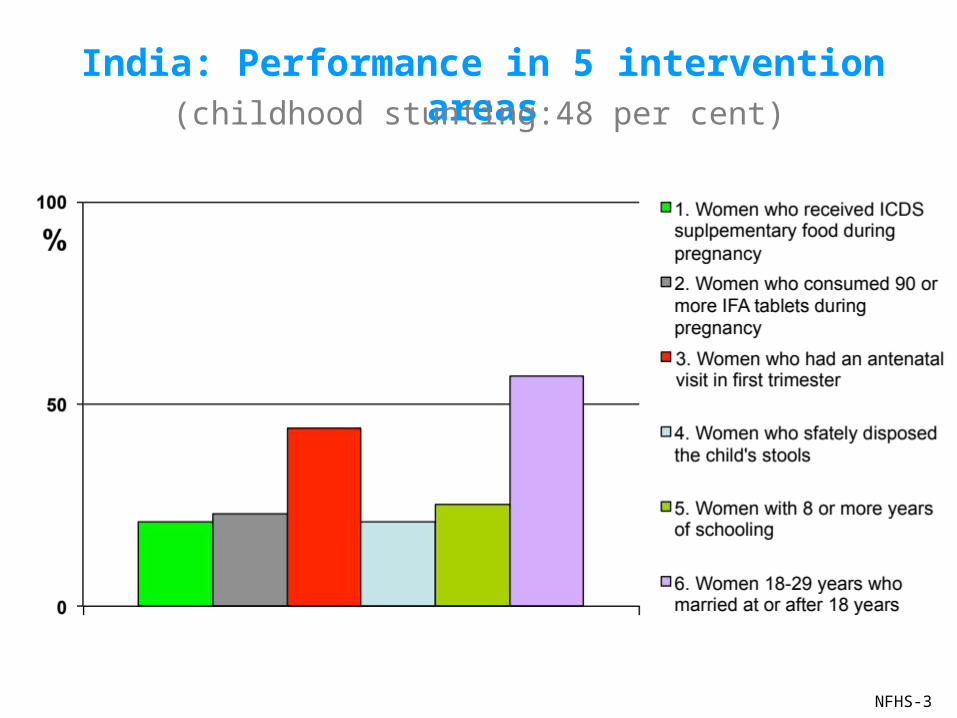
India: Performance in 5 intervention areas
NFHS-3
(childhood stunting:48 per cent)
NFHS-3
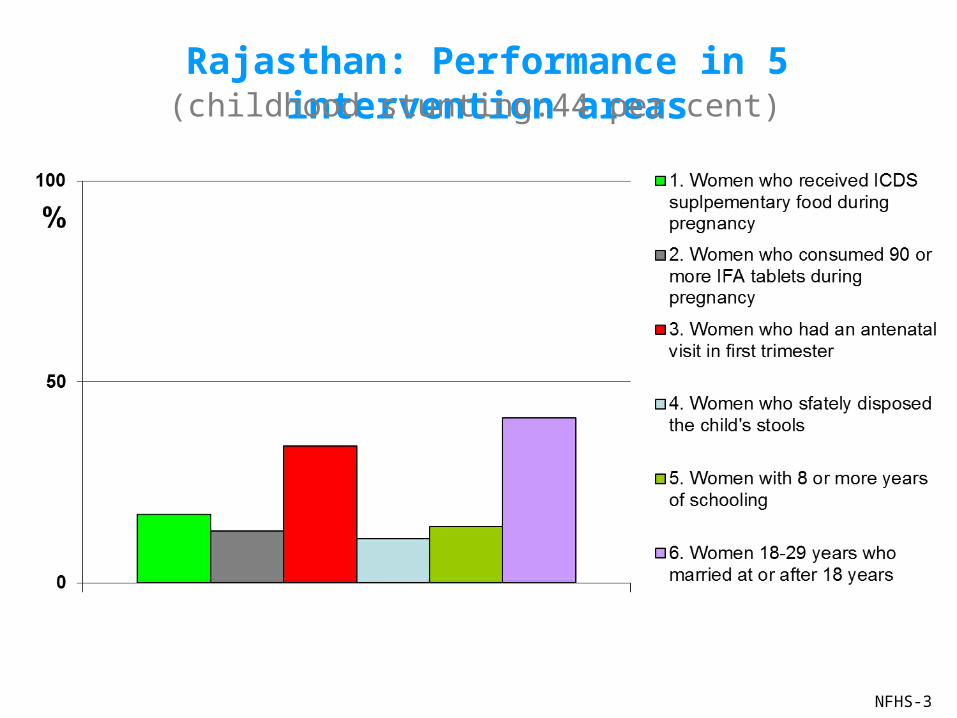
Rajasthan: Performance in 5 intervention areas(childhood stunting:44 per cent)

NFHS-3
Kerala: Performance in 5 intervention areas(childhood stunting:24 per cent)
Platforms to tap/strengthen to deliver 5 essential
interventions for girls and women

Intervention Platforms
1Improve quantity and nutrient quality of food consumed
• MWCD (ICDS)• Food and Civil Supplies (PDS)• MRD (livelihood missions)
2Prevent micronutrient deficiencies
• MWCD (ICDS)• MHFW (NRHM, Tribal-RCH)
3Improve access to basic health services
• MHFW (NRHM, MH-Tribal-RCH)• M/DWS (SWB)
4Improve hygiene and sanitation practices and access to safe drinking water
5Prevent pregnancies- too early, too many and too soon
• MHFW (Family planning)• MWCD (cash transfer)• MHRD (secondary education)• MRD (Aajeevika)
Research Questions
1. Can participation in women’s groups improve pre-pregnancy weight and weight gain in pregnancy?
2. What is the effectiveness of a package of interventions in improving nutrition status of adolescent girls?
3. What is the effectiveness of a package of interventions in improving nutrition status of pre-conceptually?
4. What is the effectiveness of a package of interventions in improving nutrition status of pregnant women?
Road map for improving coverage and quality of 5 ENI-W
1. Evidence-building : •Quantitative indicators on coverage of 5 ENI-W (report cards)•Platforms and strategies to deliver the 5 ENI-W interventions •Qualitative information gathering on barriers and opportunities to improve 5 ENI-W
2. Stakeholder consultations to arrive at recommendations•With practitioners for vetting information and gathering experiential evidence•Presenting recommendations to related government officials under the chairmanship of highest authority
3. Development of Action plan
4. Working with related department to implement the action plan