exercise interventions for successful aging miriam c. morey va and duke medical centers durham, nc
TRANSCRIPT

Exercise Interventions For Successful Aging
Miriam C. Morey
VA and Duke Medical Centers
Durham, NC

Objectives
• General overview of PA guidelines
• Overview of VA/ Duke PA programs
• Thoughts about implementation

National Physical Activity GuidelinesACSM, AHA
• Recommendations:
Aerobic• ≥ 30 min or 3 bouts of ≥10 min/day • ≥ 5 days/week• moderate intensity = 5-6 on a 10-point scale in addition to
routine ADL’s• Or, 20 minutes of vigorous activity 3 days / week
Strength• 8-10 exercises (major muscle groups), 10-15 repetitions• ≥2 nonconsecutive days/week • moderate to high intensity = 5-8 on a 10-point scale
Circulation:2007;116

Guidelines
• Recommendations:
Flexibility• ≥ 10 min ≥2 days/week • flexibility to maintain/improve range of motion (i.e. stretching
of major muscle/tendon groups, yoga)
Balance• Balance exercises for those at risk for falls (i.e. Tai Chi,
individualized balanced exercises)

Guidelines
• Recommendations:
Plan• create a single physical activity (PA) plan that integrates
preventive and therapeutic treatment of chronic conditions
Benefit• Exceed the minimum recommended amount to accrue
greater benefits

Exercise Interventions For Successful Aging
• If you do it, it will work

Exercise Interventions For Successful Aging
• If you do it, it will work
The devil is in the details

2005 National Average: Recommended Physical
Activity 65+ Strength
Training (2001)
Recommended 40% 10%
Insufficient 35%
Inactive 25%

From CDC website

Exercise program for older veterans
Clinical research program with focus on the older adult Provider training
in physical activity for older adults
Exercise rotation for medical students and fellows in geriatric training program
Pepper CenterAging Center/ Duke Medical Center
GEROFITDurham VA Medical Center

Gerofit Program• Facility-based exercise and health promotion program
established in 1986 as a GRECC clinical demonstration project.
• Developed in response to Veterans Health Care Amendment of 1983 mandating implementation of preventive medicine in VA’s. Fitness programming identified as a targeted area of need.
• Individually tailored to meet needs of older veterans with chronic conditions and physical impairments, many as a result of military service.

Veterans ages 65 and over have access to facility-based supervised exercise program (treadmills, stationary bicycles, stair machine, weight training machines, floor exercises, tai chi, water aerobics)
-Over 1200 patients referred -Average daily census + 60 patients
Referred by primary care providers and other health care specialists
Special consultative services available as needed
Telephone counseling offered to: -Patients who live too far to attend the facility-
based program - Patients under age 65

Key published clinical outcomes• Veterans participating in Gerofit report significant improvements in
exercise capacity, cardiovascular risk factors and psychological well-being. JAGS (37):1989; J Appl Ger (10):1991.
• Examination of impact of burden of disease (no disease vs. 1
disease vs. 2 diseases) on exercise parameters and 5-year trajectories of performance. JAGS (44):1996.
• Older veterans with chronic diseases experience a long-term beneficial mortality effect from participation in facility-based program. JAGS (50):2002.
• Older veterans enrolling in Gerofit have significantly poorer physical performance than national normative data. And, veterans participating in Gerofit for 6 months or more have physical performance on par or higher than reported national norms. JRRD (41):2004.
Transition to Funded Research
• Aerobic vs. Axial/Aerobic Training: Improvement in Function (PI: Morey, 1992-1995) (facility to home-based) Duke Pepper Center
• Phoning for Function: Promoting Health After Cancer (PI: Demark, 1997-2003) (home-based) Duke Pepper Center
• Improving Fitness and Function in Elders (LIFE 1) (PI: Morey, 2001-2004) (home-based): VA Rehabilitation Research Service
• Learning to Improve Fitness and Function in Elders (LIFE 2) (PI: Morey, 2004-2008) (home-based): VA Rehabilitation Research
• RENEW: Reach Out to Enhance Wellness in Older Survivors (PI Demark 2004-2008) (home-based) National Cancer Institute

Aerobic vs. Axial/Aerobic Training: Improvement in Function (facility to home-based)
Randomized clinical trial Randomized clinical trial •Three months of supervised exerciseThree months of supervised exercise• Followed by six months of home-based exerciseFollowed by six months of home-based exercise
with telephone follow-upwith telephone follow-up
Intervention (3 days per week)Intervention (3 days per week)• Axial/Aerobic group Axial/Aerobic group 20 minutes axial mobility exercises20 minutes axial mobility exercises 20 minutes aerobic exercise20 minutes aerobic exercise• Aerobic groupAerobic group 40 minutes aerobic exercise40 minutes aerobic exercise

Change in Aerobic Capacity
Findings:
Significant overall improvement,
both groups, p=0.0001
0-3 mos.
group*time interaction, p=0.0014
(dose response)
0-9 mos: p=0.0717
17.5
18
18.5
19
19.5
20
20.5
0 3 9
Axial/Aerobic
Aerobic
MonthsMonths
VVOO22 PPeeaakk ml/kg/minml/kg/min
Morey et al., J Geron Med Sci 1999 54A M335-M342.
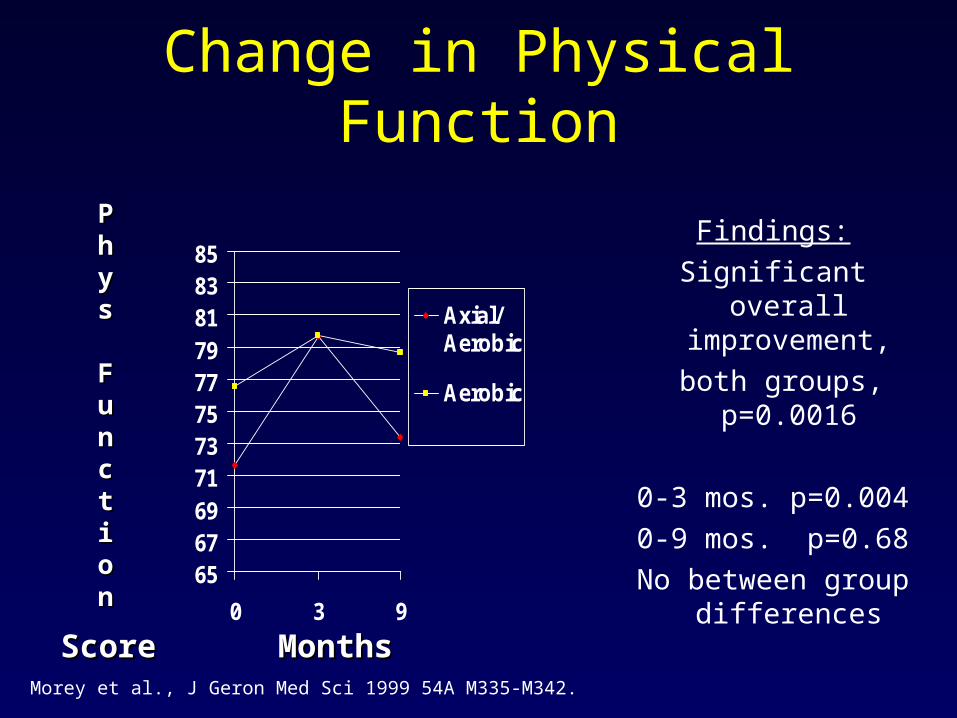
Change in Physical Function
Findings:
Significant overall improvement,
both groups, p=0.0016
0-3 mos. p=0.004
0-9 mos. p=0.68
No between group differences
6567697173757779818385
0 3 9
Axial/Aerobic
Aerobic
MonthsMonths
PPhhyyss
FFuunnccttiioonn
ScoreScoreMorey et al., J Geron Med Sci 1999 54A M335-M342.

Secondary Improvements
• Health Related Quality of Life, p= 0.0009
• Total Number of Symptoms Reported, p=0.0001
• Effect of Symptoms on Functional Limitations, p=0.0001
Morey et al., J Geron Med Sci 1999 54A M335-M342.

What did we learn and where do we go from here?
• Facility-based have more robust outcomes; but most people choose home-based exercise
• How can we successfully apply these approaches to home-based intervention?
• How can we enhance adherence in the home-based setting?

Predictors of adherence
• Number of diseases • Body mass index • Physical function • Pain• **Weekend
adherence
0
10
20
30
40
50
60
70
80
90
1 3 5 7 9 11 13 15 17 19 21 23 25
Perc
ent A
dher
ent
AdherentsNon adherents
Weeks
Morey, et al. J Aging Phys Act 2003, 11,351-368

Functional Outcomes by Level of Adherence: SF-36 Physical Function
50556065707580859095100
0 3 9
AdherentNon-Adh
Findings:Change in physical function
scores between 3 and 9 months differed by level of adherence. (Chi sq. = 5.67, 1 df, p= 0.017)
Adherents maintained gains
Non adherents declined to baseline functional score.
MonthMonthss
FFuunnccttiioonn
Project LIFE 1 And 2
• Use state of the art counseling methods to enhance adherence
• Desire to include primary care providers as part of counseling team
• Needed to involve more functionally limited elders
Project Life 1
• Six-month feasibility trial
• Primary care providers endorsed PA one-time in clinic
• Health counselor gave baseline PA counseling to everyone prior to randomization
• High intensity group had 3 months bi-weekly PA counseling and 3 months monthly PA counseling

Project LIFE 1
• One-time counseling had short-term benefit that was not sustained
• Patients valued primary care provider involvement
• More frequent telephone contact was needed
0
5
10
15
20
25
Baselin
e
3 m
onth
6 m
onth
Physic
al A
ctivity F
requency
HighIntensity
AttentionControl
UsualCare
Morey, et al. J Aging Phys Act 2006 14 324-343

Project LIFE 2
• 12-month multi component PA trial comparing counseling to usual care– One-time in person– Provider endorsement– Sustained telephone counseling– Sustained provider endorsement by automated
telephone messaging– Mailed quarterly progress report
• Goal: 30 min 5 days/week aerobic
15 min strength training 3 days/wk

Project LIFE 2
• Counseling must be sustained
• It takes one year to get close to recommended PA guidelines
• Provider involvement is highly acceptable
• These changes are accompanied by very modest improvements in physical function
Minutes of self reported exercise per week
0
50
100
150
0 3 6 12
Months
Rep
orte
d m
inut
es p
er
wee
k
Counsel
UC

New approaches to enhance PA adherence
• SMART Design

From Physical Activity to Physical Function
• Data from 2 clinical trials (Life 1 and Phoning for Function)
• Both 6 months w telephone PA counseling
• Examined impact of 150 minutes PA
Pooled data from several studies
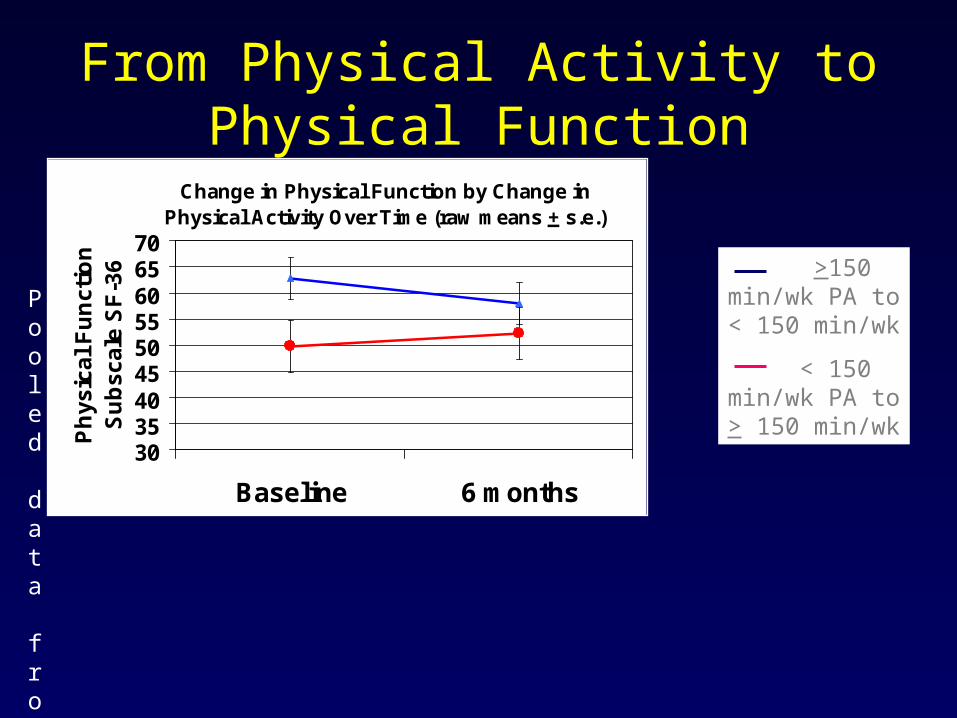
From Physical Activity to Physical Function
Change in Physical Function by Change in Physical Activity Over Time (raw means + s.e.)
303540455055606570
Baseline 6 months
Ph
ysic
al F
un
ctio
n
Su
bsc
ale
SF
-36
Pooled data from several studies
>150 min/wk PA to < 150 min/wk
< 150 min/wk PA to > 150 min/wk

Physical Activity to Physical Function
• Benefits are more easily achieved among adults of higher physical function
• Exercise modality is not crucial – any exercise is better than being sedentary
• Among more impaired adults and those with multiple morbidities results are more tenuous. New health events occur frequently.
Partnering with Specialists to Enhance PA in Special Populations• Innovative use of advances in
Telemedicine
• Health Buddy for monitoring PA adherence in stroke patients (Chumbler and Hoenig, Co-PI’s)

Provider Education
• All VA primary care providers trained in PA counseling using PACE methods and materials
• Gerofit rotation offered to all geriatric fellows; observe nurse-based physical activity counseling and follow new patient for 6-8 weeks
• Modified rotation offered to medical students (fourth year, geriatric intern rotation, and others). Establish link between exercise prescription and physical function

Partnering with Specialists to Enhance PA in Special Populations• Telemedicine for Intensive Care Rehab
(Ely and Hoenig, Co-Pi’s)

Conclusions
• Physical activity interventions of diverse content can be implemented across multiple settings
• Integration of clinical, research and educational programs have expanded the successful implementation of PA programs at our medical centers