experiences and metrics for calculating return on investment€¦ · for calculating return on...
TRANSCRIPT
Experiences and Metrics for Calculating Return on Investment
September 20, 2013

©2013 HIMSS 2
Experiences and Metrics for Calculating Return on Investment
Contributors
• Ángel Blanco RubioOrganizationandProcessesDirector.Idcsalud.
• Miguel CabrerHIMSS(HealthcareInformationandManagementSystemsSociety)-EuropeGoverningCouncil.
• Julio Díaz OjedaDeputyDirectorofInformationSystemsandTechnologies.HospitalRegionalUniversitarioCarlosHaya(CarlosHayaUniversityRegionalHospital).
• Vicent Moncho MasDirectorofInformationSystems.HospitalMarinaSaluddeDénia(MarinaSaluddeDéniaHospital).
• Manuel Pérez VallinaSeniorAdvisor.HIMSSEurope.
• Carlos Piqueras PicónHealthDirector.Intel.
• Jesús Redrado RedradoDirectorofInformationSystems.ClínicaUniversidaddeNavarra(UniversityHospitalofNavarra).
• Guillermo Vázquez FernándezDeputyDirectorofInformationSystems.ComplexoHospitalarioUniversitarioACoruña(ACoruñaUniversityHospitalComplex).
• David Vidal FernándezDirectorofInformationSystems.HospitalClínicBarcelona(HospitalClinicBarcelona).
Mediapartner
©2013 HIMSS 3
Contents
Introduction 4
Purpose of the document 5
Automation of administrative processes and work in real time 6
Management of requests: Referrals 9
Digital imaging 13
Hospital medication process 15
Management of complex treatments in the day hospital 18
Nursing care management 21
Improves surgical planning 24
Clinical decision support systems 27
Non face-to-face services 30
©2013 HIMSS 4
IntroductionCost,value,return,inshort,measurement.Itisimpossibletoconsidercarryingoutanybusiness-relatedactivityorserviceproperlyiftheseconceptsarenotonthedecision-makingagenda.Beingabletomeasurethevaluegenerated,toplantheenvironmentinwhichthemultipliereffectofaninvestment’svaluewillbeofthegreatestbenefittousers,andtoachievethemaximumreturnoninvestmentwithinitseconomicdimension,hasbeentheobjectiveofhealthmanagersanddecision-makersforyears.
Thereisaneedtoassesstheimpactoftheeconomicsituationonhealthcare.Theenvironmentofstableorgrowingdemandcontainsfactorsthatputpressureonexpensereduction.Thesefactorsmakeitnecessarytogobeyondtheobviousandtosearchfortheperfectsolutiontoincreaseefficiency,withinnovativeproposalsandbravemanagementdecisions.
Inaddition,inhealthcaresystems,costreduction,improvementofprocessesandinnovationortheimplementationofinformationandcommunicationtechnologies(ICT)areamuchhigherprioritythanmaintaininganequilibriuminthebalancesheetorreorganization.Fordecades,healthcareeconomists,healthcareITpersonnel,planners,andclinicalandnursingdirectorshavemadestridesintheestablishmentoftheconceptof“healthcareoutcomes”,inwhichimprovementineconomicindicatorsisalsototheadvantageofpatients,throughamorepersonalizedcare,avoidingunnecessaryactions,orimprovedinformationinthehandsofprofessionalsandthepatientsthemselves.
Withoutadoubtoneofthemostprevalentideasinthisenvironmentisthatthemassivedeploymentofinformationandcommunicationtechnologiesinthehealthcarefieldleadstocostsavings,improvespatientsafetyandintegratescarelevels.Eventhoughitispracticallyadogma,theideaitselfisnotenough:themanagersanddecision-makersneedtomeasureit,andtheallocationofresourcesisnowmoreofastrategictaskthanever.
ThisiswhyROI(ReturnOnInvestment)initsmoreorthodoxeconomicdimension,orwhenitisassociatedwithimprovementsinsatisfactionandpatientprocedures,isaconstantinallinformaloracademicdiscussionsabouthowtomaintainthequalitystandardsforwhichSpanishhealthcareisgloballyrenowned.
TheattentiontocostsandthecalculationoftheseisaregularaccompanimentofICTinvestmentsinhealthcare
institutions.However,themonitoring,measuringandverificationofthesuitabilityoftheseprojectsovertime,onceintroduced,isnotcommonpractice.
AtHIMSSEurope,incollaborationwithIntel,wehaveformedagroupofCIOs(ChiefInformationOfficers)tocarryoutanexercisethatcangivevaluetotheICTs(InformationandCommunicationTechnologies),whicharecurrentlysetupinhealthorganizations,aswellasimplementationplansthroughoutthecontinent.
WhattoolsdoesaCIOhaveinordertoprioritizetheirinvestmentprojects?HowdoyouconvincemanagementthattheICTpathleadstocostreductioninhealthorganizations?HowdoyoumeasureincreasesinpatientsafetyasprovidedbyacomprehensiveandintegratedElectronicMedicalRecord?ArethereobjectivereasonsforgivingpreferencetoICTinvestmentsoverhospitalequipment?Theseandotherquestionsariseintheday-to-dayofhealthorganizationsasanelementofdiscussion,prioritizationanddisputeaboutresourceallocation.
ROI = (Gain from investment - Cost of investment)
Cost of investment
©2013 HIMSS 5
Purpose of the documentTherefore,itisnecessarytomeasurewiththeutmostrigor,keepinginmindthedifficultyofquantifyingsomeoftheresults,andthatitmaynotalwaysbepossibletoestablishaone-to-onerelationshipbetweenanactionanditsresult,especiallyinverycomplexorganizationalecosystemssuchashospitals.
Suchcomplexitymeansthatthedeploymentoftechnologyalonewillnotbeabletoimproveprocessesorresults.Inaddition,theresultsobtainedhaveamulti-factorialorigin.Theyrequirepeople,processesandsystemsanditisnotalwayspossibletodeterminethespecificweightofeach.
Anobjectiveorbusinessneedtocovercostsavings,healthcarequalityandsafetyimprovements,andprocessefficiencyimprovements,etc.,willrequirepeopleandprocessestobedefinedandorganized,aswellastheInformationSystems(ICT),inorderforthemtojointlyrespondtothisobjectiveorneed,providingaddedvaluetotheorganization.
Themarketproposestechnologicalsolutionsfor99%oftheproblemsbutitisimportanttorememberthatpeopleandprocessesarethekeyfactorintheseprojects:thetechnologyismerelyameans.
Thepurposeofthedocumentis,therefore,topresentinterestingcases,whichhavebeensummarizedbuthaveanappropriatelevelofunderstanding,withoutsacrificingthecomplexityoftheideas,orthestringencyoftheconclusions.ThesecasesshouldgeneratewithintheICThealthcarecommunityaninterestinmeasuringandadvancingresultsinprojectplanning.
Therefore,itisnecessarytomeasurewiththeutmostrigor,keepinginmindthedifficultyofquantifyingsomeoftheresults,andthatitmaynotalwaysbepossibletoestablishaone-to-onerelationshipbetweenanactionanditsresult,especiallyinverycomplexorganizationalecosystemssuchashospitals.
Suchcomplexitymeansthatthedeploymentoftechnologyalonewillnotbeabletoimproveprocessesorresults.Inaddition,theresultsobtainedhaveamulti-factorialorigin.Theyrequirepeople,processesandsystemsanditisnotalwayspossibletodeterminethespecificweightofeach.
Anobjectiveorbusinessneedtocovercostsavings,healthcarequalityandsafetyimprovements,andprocessefficiencyimprovements,etc.,willrequirepeopleandprocessestobedefinedandorganized,aswellastheInformationSystems(ICT),inorderforthemtojointlyrespondtothisobjectiveorneed,providingaddedvaluetotheorganization.
Themarketproposestechnologicalsolutionsfor99%oftheproblemsbutitisimportanttorememberthatpeopleandprocessesarethekeyfactorintheseprojects:thetechnologyismerelyameans.
Thepurposeofthedocumentis,therefore,topresentinterestingcases,whichhavebeensummarizedbuthaveanappropriatelevelofunderstanding,withoutsacrificingthecomplexityoftheideas,orthestringencyoftheconclusions.ThesecasesshouldgeneratewithintheICThealthcarecommunityaninterestinmeasuringandadvancingresultsinprojectplanning.
©2013 HIMSS 6
Automation of administrative processes and work in real timeMosthospitalshavealreadycomputerizedthebasicadministrativeprocesses,suchaspatientadmission,centralizedappointments,dischargeorregistrationofthemedicalepisodewiththerelevantcodification.Thishasmadeitpossibletoimprovecertainprocessesandstudythecenter’sactivity.
Inthissection,wedealwithsituationsthatincludereal-timemanagementcriteria,andtheautomationandeliminationofadministrativetasks.Thisinvolvesnotonlytheclinicalpracticebutalsothemanagementofandrelationshipwiththepatient.
• Arrangingappointmentsforfuturetestswhennecessary,withthepatientpresent.
• Avoidinglinesandadministrativedelayshelpsthepatienttohaveabetterperceptionofthehealthcaretheyreceive.
Aspartofthehealthcareprocess,whencreatingtheattendancenoteordischargereportthepatientisautomaticallygiven,viaacomputeralgorithm,thedayandtimeofthetests.Itispossibletochangethedetailsatthetimeifnecessaryortosimplyleavethemastheyare,andthesecanbeprintedonthedocument.Ifthepatientdecidestochangethemforanyreason,theycandosoatalaterdatebyanyavailablemeans,eitherinperson,byphoneifthereisacallcenter,byInternetoratspecificserviceterminals.
Ifsubsequentappointmentsareprocessedatthepatient’shomewewillgainanumberofbenefits,notonlyofaneconomicnature,whichhavebeenseenanddemonstratedintheIDC(IberiadeDiagnósticoyCirugía)healthcenters:
• Savingofadministrativestaffforappointment-makingorinformationtasks,beingabletoappointthesestafftomoreproductivetaskswithinthehealthorganization.Theexperiencegainedis1administrativeassistantforevery32,000appointments(assumingthatthereare150appointmentsperpersonperday).
• Improvementinpatientsatisfaction:theyonlyhavetogototheirhealthcenterorhospitaltoreceivehealthcare,ratherthanhavingtogothroughtheadministrativeproceedings.
• Itreinforcestheclinicalact.Aninstructionsuchas“check-upin3months”isaclinicalprocedure,but“check-uponSeptember16at11:00”givesfarmoreimportanceandaccuracy,withouttheneedforanadditionaladministrativeprocedureascarriedoutbyathirdpartywhohastothenrepeattheidentificationtasks,understandwhatneedstobedone,forwhenandthesignificancethereof.
CalculationofROIattheHospitalSurdeAlcorcón(SurdeAlcorcónHospital)
• TotalICTinvestmentproject €17,000
• Administrativehoursavoided 1,232
• Approximatecostavoided €19,000
• Annualcorporatemaintenance € 3,000
ROI = 112%
Contacting the patient when test results arrive
Thepresenceofthepatientisnotnecessaryinallhealthcareprocesses.
Methodology
Definingaresultsmanagementsystemmeansthatcertain“routine”taskscanbecarriedoutwithouttheneedforthepatienttobepresent:
• On-lineresults.Thepatientcanseetheirresultswithouthavingtotraveltotheclinic.
©2013 HIMSS 7
• Incaseswherenecessary,healthcarestaffcangetincontactwiththepatientwhenresultsarriveinordertodecideiftheface-to-faceconsultationneedstogoahead,ifthereisaneedtobringitforwardorpostponeit,maintainorchangethetreatment,explainthediagnosisorsubsequentsteps.
• Asamoreadvancedmechanism,remoteconsultationscanbecarriedoutwithaspecialist:referralsinthecenteritself,fromresidences,primarycarecenters,correctionalinstitutions,etc.
Results
• Adecreaseinunnecessaryface-to-faceconsultations:Thistranslatesintothereductionofwaitinglistsandgreaterpatientsatisfactionbypreventingunnecessarytraveltothehealthcenterorhospital.
• Advancedresultsreview.Whentheseoccurandnotwhenthepatientcomesforacheck-up.
Opensupchannelsofnonface-to-facecommunicationwithpatients:Appointments,administrativeproceedings,clinicalinformation.
Givesthepatientthenecessarytoolssothattheycancarryoutcertainadministrativeproceduresthemselvesandalsobemoreinvolvedinmanagingtheirownhealth.
Thesetoolscanincludemakingon-lineappointments,healtharchiving,sendingappointmentremindersviaSMSoremail.
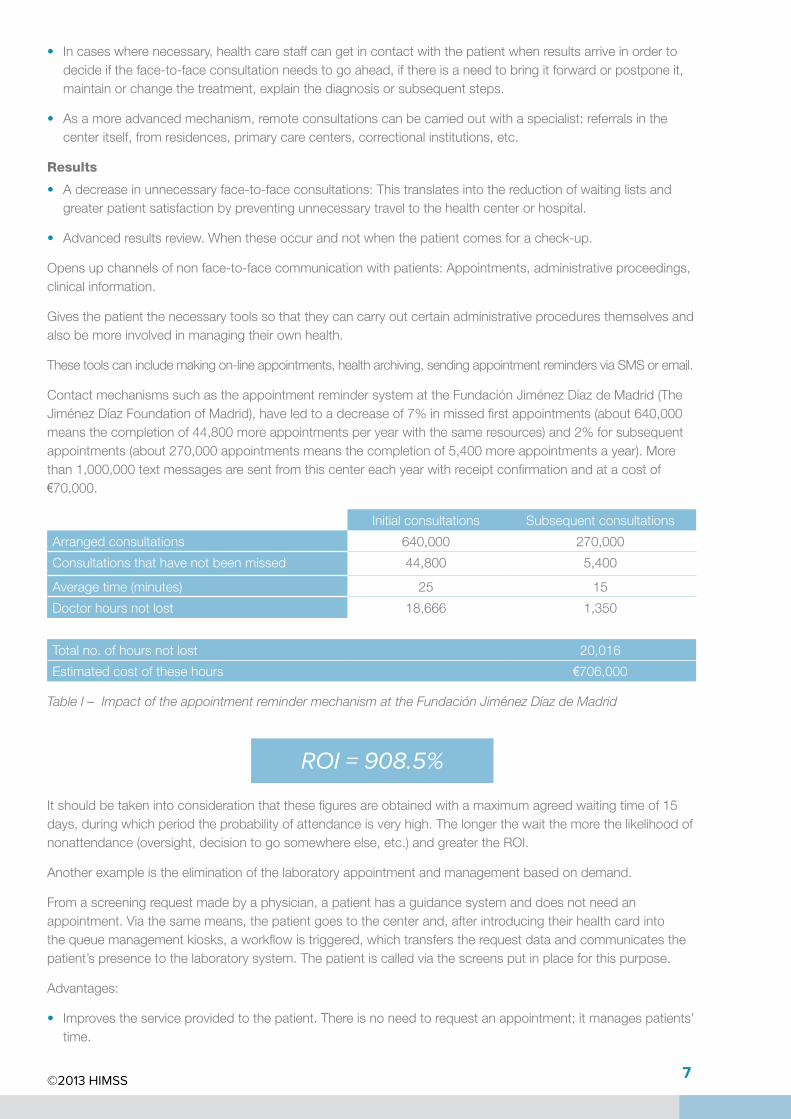
ContactmechanismssuchastheappointmentremindersystemattheFundaciónJiménezDíazdeMadrid(TheJiménezDíazFoundationofMadrid),haveledtoadecreaseof7%inmissedfirstappointments(about640,000meansthecompletionof44,800moreappointmentsperyearwiththesameresources)and2%forsubsequentappointments(about270,000appointmentsmeansthecompletionof5,400moreappointmentsayear).Morethan1,000,000textmessagesaresentfromthiscentereachyearwithreceiptconfirmationandatacostof€70,000.
Initialconsultations Subsequentconsultations
Arrangedconsultations 640,000 270,000
Consultationsthathavenotbeenmissed 44,800 5,400
Averagetime(minutes) 25 15
Doctorhoursnotlost 18,666 1,350
Totalno.ofhoursnotlost 20,016
Estimatedcostofthesehours €706,000
Table I – Impact of the appointment reminder mechanism at the Fundación Jiménez Díaz de Madrid
ROI = 908.5%
Itshouldbetakenintoconsiderationthatthesefiguresareobtainedwithamaximumagreedwaitingtimeof15days,duringwhichperiodtheprobabilityofattendanceisveryhigh.Thelongerthewaitthemorethelikelihoodofnonattendance(oversight,decisiontogosomewhereelse,etc.)andgreatertheROI.
Anotherexampleistheeliminationofthelaboratoryappointmentandmanagementbasedondemand.
Fromascreeningrequestmadebyaphysician,apatienthasaguidancesystemanddoesnotneedanappointment.Viathesamemeans,thepatientgoestothecenterand,afterintroducingtheirhealthcardintothequeuemanagementkiosks,aworkflowistriggered,whichtransferstherequestdataandcommunicatesthepatient’spresencetothelaboratorysystem.Thepatientiscalledviathescreensputinplaceforthispurpose.
Advantages:
• Improvestheserviceprovidedtothepatient.Thereisnoneedtorequestanappointment;itmanagespatients’time.
©2013 HIMSS 8
• Lesswaitinginline.Thepatientdoesnothavetogetinline;theyarecalledinstead.
ROIcalculationattheFundaciónJiménezDíaz:
• ICTinvestmentindevelopmentandconfiguration €19,000
• ICTinvestmentHW,PCs,printers,labels,kiosksandmonitors €19,400
• Annualplatformmaintenance €5,000
• Hoursavoidedofhavingadministrativeassistantsatreception:3,600h(3administrativeassistantsonweekdaysfrom7to12).
• Approximatecostavoided €57,500
• Waitingtime:previouslynotmeasurable.Currently,15minutesmaximumondayswithapeakactivityof500samples.
ROI = 150%
Eliminate manual systems using informed consent biometric signatures
Theinformedconsentprocessisadoctor-patientprocedurewhichproducesadocumentthatservesasproofofthesameandwhichincludesbothsignatures.Thisdocumentrequiresamanualsignature,collection,archivingandsearchsystemtobemaintainedifnecessary.
Itsautomationisbasedonaperson’shandwrittensignatureascarriedoutonatouchscreencapturedevice,althoughitisnecessarytoreviewthelegalsettingineachcase.
Thecapturedevicerecordsparameterssuchasthespeedandpressuremadeduringthesigningandgeneratesacalligraphicpatternofthesignaturebasedontheseparameters.
Itrequirestheintroductionofdevicesforsigninginallareaswhereapatient’sorphysician’ssignaturemightberequired.
Results
• Economicbenefits:
� IntheHospitalReyJuanCarlosdeMóstoles(ReyJuanCarlosdeMóstolesHospital),aninvestmentof150devicesmeansaninvestmentrecoverytimeoffewerthan8months,assumingadailycollectionof500signatures.Maintainingamanualsystemwouldrequirebetween2-3people/yearforcollecting,archivingorscanning,indexing,retrieval,etc.
� Furthermore,itsavesonthecostswhichthephysicalspaceandpaperworkofamanualconsentfilewouldmean.
• Itprovidesincreasedsecuritytothemanagementsystemandsafe-keepingoftheconsentmaterial.
• Professionalsatisfaction:thepatient’sconsentcanbetraced.
InitialHardwareandSoftwareInvestment €31,750
Annualadministrativesavings €60,000
Table II – Biometric signature project at the Hospital Rey Juan Carlos de Móstoles
ROI = 89%

©2013 HIMSS 9
Management of requests: ReferralsIncludedinthehealthcareproceduresthatformpartofthedailypracticeofhealthcarepersonnelarefoundrequestsfordiagnosistests,consultationswithotherspecialistclinics,treatment,etc.Thesearecomplexprocessesthatcombineclinicalandadministrativetasks,theimplementationofanelectronicsystemtoreplacethepaper-basedprocessesandwhich,amongotherthings,monitorsthefollowingresults:
Request management objectives
Quality of care
Economic
Savings of time
Increase in patient safety
Recording of compound requests
Reduction in response times
Prevents unnecessary tests
Prevents duplicate tests
Methodology
Tomeasuretheprofitabilityofthistypeofproject,itisproposedtocomparetheestimateofthepaperrequestsmanagementprocesswiththeelectronicprocess.Forexample,intheradiologytestsrequestprocesswecancalculatethetimeusedbyeachparticipantinanenvironmentthatusespaperandinanelectronicenvironmentfromthetimethedoctormakestherequestuntilthetestiscarriedout.
Results
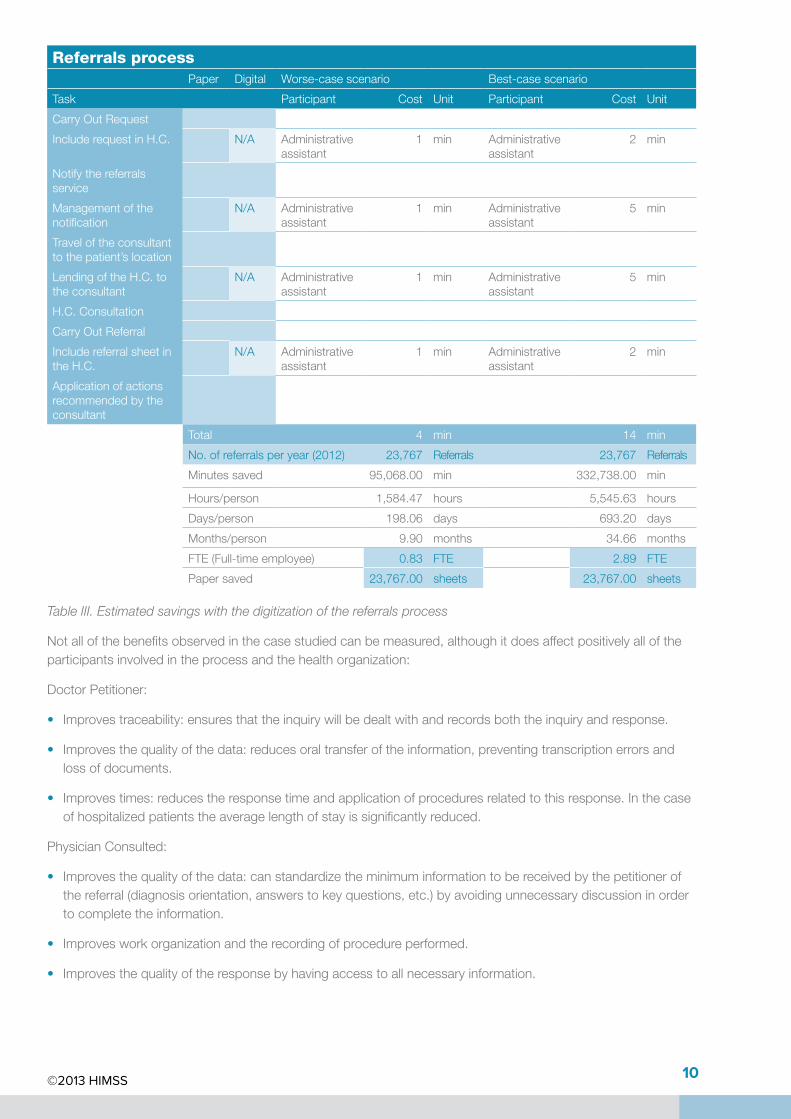
TheHospitalMarinaSaluddeDéniacarefullystudiedthecaseoftherequestforreferraltootherspecialists.Itsresultsinclude,intableIII,anobvioussavingoftime,whichcontributesmoreeffectivelytotheprocess.
©2013 HIMSS 10
Referrals processPaper Digital Worse-casescenario Best-casescenario
Task Participant Cost Unit Participant Cost Unit
CarryOutRequest
IncluderequestinH.C. N/A Administrativeassistant
1 min Administrativeassistant
2 min
Notifythereferralsservice
Managementofthenotification
N/A Administrativeassistant
1 min Administrativeassistant
5 min
Traveloftheconsultanttothepatient’slocation
LendingoftheH.C.totheconsultant
N/A Administrativeassistant
1 min Administrativeassistant
5 min
H.C.Consultation
CarryOutReferral
IncludereferralsheetintheH.C.
N/A Administrativeassistant
1 min Administrativeassistant
2 min
Applicationofactionsrecommendedbytheconsultant
Total 4 min 14 min
No.ofreferralsperyear(2012) 23,767 Referrals 23,767 Referrals
Minutessaved 95,068.00 min 332,738.00 min
Hours/person 1,584.47 hours 5,545.63 hours
Days/person 198.06 days 693.20 days
Months/person 9.90 months 34.66 months
FTE(Full-timeemployee) 0.83 FTE 2.89 FTE
Papersaved 23,767.00 sheets 23,767.00 sheets
Table III. Estimated savings with the digitization of the referrals process
Notallofthebenefitsobservedinthecasestudiedcanbemeasured,althoughitdoesaffectpositivelyalloftheparticipantsinvolvedintheprocessandthehealthorganization:
DoctorPetitioner:
• Improvestraceability:ensuresthattheinquirywillbedealtwithandrecordsboththeinquiryandresponse.
• Improvesthequalityofthedata:reducesoraltransferoftheinformation,preventingtranscriptionerrorsandlossofdocuments.
• Improvestimes:reducestheresponsetimeandapplicationofproceduresrelatedtothisresponse.Inthecaseofhospitalizedpatientstheaveragelengthofstayissignificantlyreduced.
PhysicianConsulted:
• Improvesthequalityofthedata:canstandardizetheminimuminformationtobereceivedbythepetitionerofthereferral(diagnosisorientation,answerstokeyquestions,etc.)byavoidingunnecessarydiscussioninordertocompletetheinformation.
• Improvesworkorganizationandtherecordingofprocedureperformed.
• Improvesthequalityoftheresponsebyhavingaccesstoallnecessaryinformation.
©2013 HIMSS 11
Patient:
• Improvesthequalityofcare.
• Reinforcespatientsafetybydecreasingthechancesofmislaidormissinginformation.
• Improvesresponsetimes.
Organization:
• Byimprovingthequalityandstructureofthedataobtained:
� Opportunitytotracetheprocess.
� Usingtheinformationformeasuringpurposesandcontinuousimprovement.
• Thestructuredinformationservesasasupportinclinicalsessionsandtraining.
• Itpreventsthephysicalrelocationofthepatient’smedicalhistory.
• Promotescollaborationandteamwork.Thedoctorpetitionerhascompleteinformationabouttherequestanditstimesandtheconsultantphysicianhasdetailsofwhentherequestwasmade.
ThefollowingtablesreflecttheaverageresponsetimesattheComplexoHospitalarioUniversitariodeACoruñaandattheHospitalMarinaSaluddeDénia,obtaininganaverageresponsetimewhichimpliesthatvirtuallyallofthereferralsareansweredinthesametimeslotorthesubsequentone.
Thelackoftraceabilityintheoldpaper-basedprocesspreventsusfromcomparingtheseresultswiththetimespriortotheimplementationoftheICTforreferralsmanagement.However,wecanstillsaythattheprocessissubstantiallyimproved.
Service Averageresponsetime
Endocrinology 14:23:00
Table IV – Average response times of Endocrinology referrals at theComplexo Hospitalario Universitario de A Coruña
©2013 HIMSS 12
Service Averageresponsetime
AllergyUnit 3:23:30
AnesthesiaandRecovery 5:18:17
Cardiology 10:05:02
Dermatology 41:46:08
DigestiveMedicine 30:31:30
Ear,NoseandThroat 3:37:18
EmergencyPhysician 0:09:00
Endocrinology 3:26:53
GeneralandGastrointestinalSurgery 11:57:29
GynecologyandObstetrics 23:45:29
HealthCareNetwork 0:40:00
HeartSurgery 17:16:30
Hematology 11:27:43
HomeHospitalCareUnit 5:40:09
InternalMedicine 28:25:41
MaxillofacialSurgeon 38:53:15
Nephrology 1:28:45
Neurology 16:53:44
Neurosurgery 15:17:00
OccupationalHealth 10:51:00
Oncology 5:56:00
Ophthalmology 5:33:58
OrthopedicSurgeryandTrauma 2:21:18
Pediatrics 9:07:20
Pharmacy 48:12:07
PlasticSurgery 18:18:40
Psychiatry 21:42:57
Pulmonology 14:39:57
Rehabilitation 21:36:20
ResidentAnesthetist 8:48:30
ResidentCardiology 3:11:20
Rheumatology 5:15:45
SocialWorker 12:45:49
ThoracicSurgery 12:47:00
Urology 19:10:38
Total 12:23:57
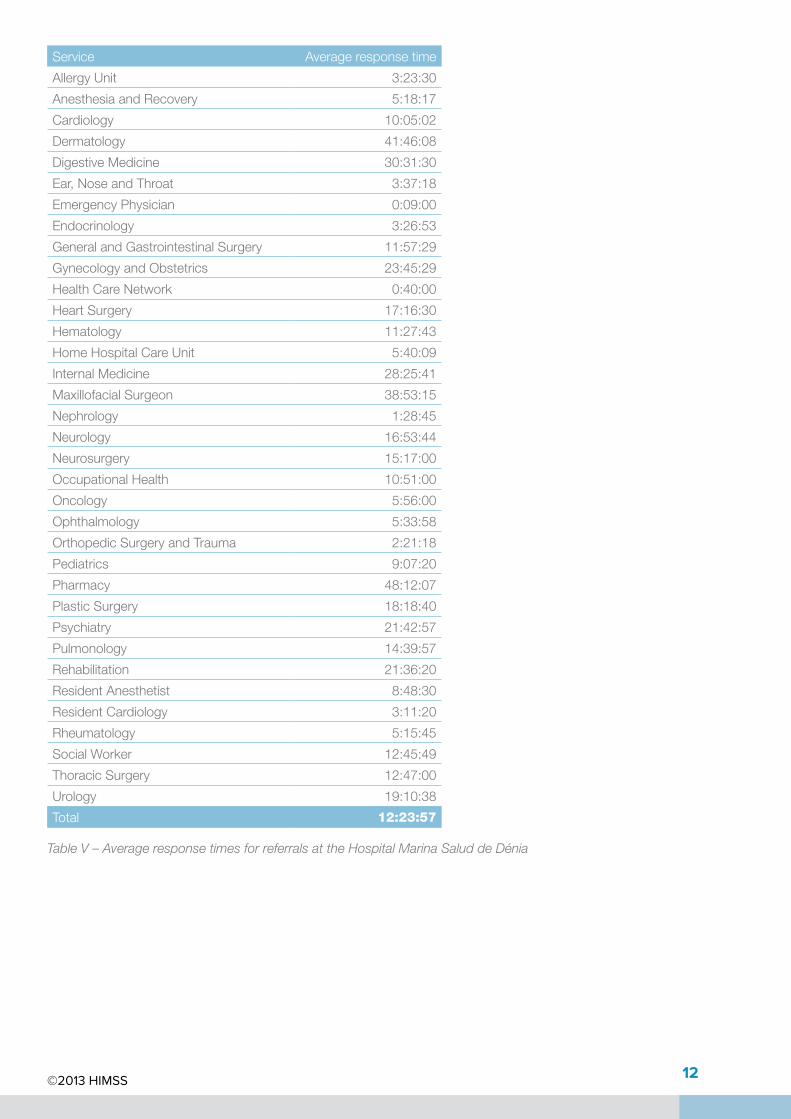
Table V – Average response times for referrals at the Hospital Marina Salud de Dénia
©2013 HIMSS 13
Digital imagingTraditionally,theservicesofradiologyandnuclearmedicinehavebeenthemaindrivingforcebehindmedicalimagingsystemsinhealthorganizations,buttherearemanyotherservicesanddevicesthatalsoproduceimaging.Therefore,itisimportanttoclarifythatwhenwerefertodigitalmedicalimagingwearenotjusttalkingaboutradiologicalimaging.
Methodology
Whenanorganizationconsidersimplementingadigitalimagingsystem,itshouldtakethefollowingfactorsintoaccount:
• Requirementsofthemedicalservicesinvolved.
• Worksystem:
� Imageanalysis.
� Informedprocess.
• Technologicalaspectsforintegratingwiththerestoftheorganization’ssystems.
• Economicfactor:
� Investment.
� Expenditure,includingrecurringspendingforsystemmaintenance.
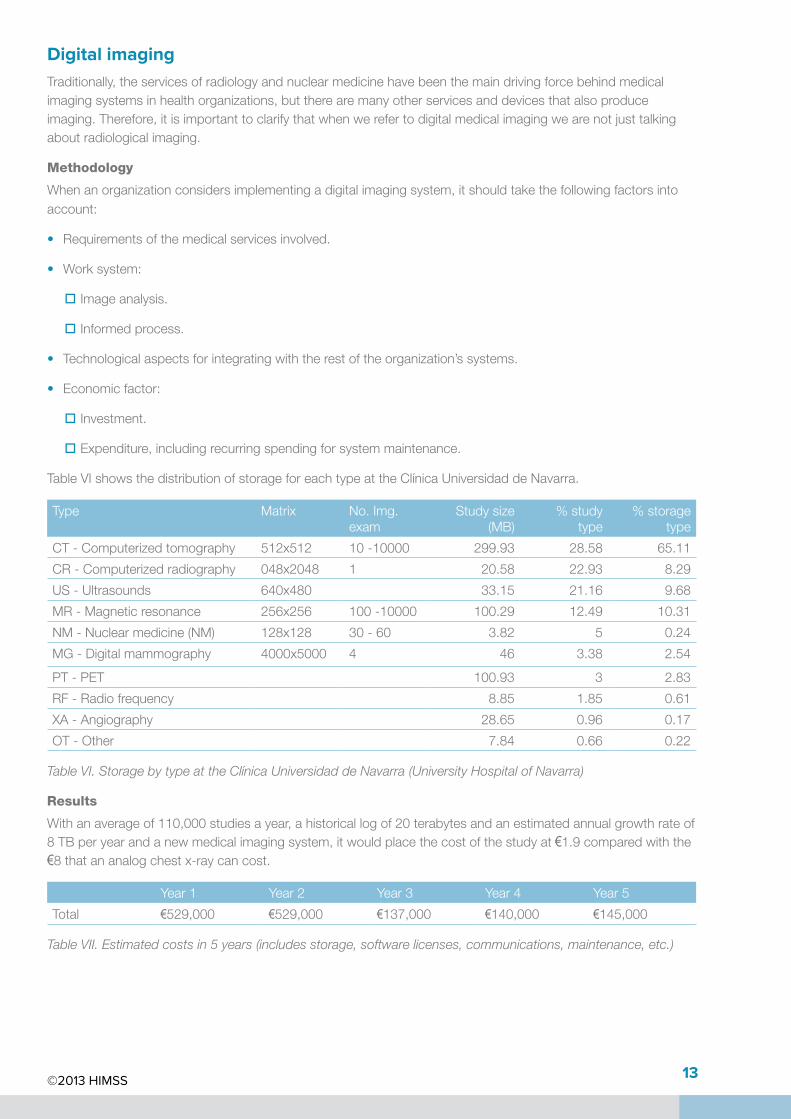
TableVIshowsthedistributionofstorageforeachtypeattheClínicaUniversidaddeNavarra.
Type Matrix No.Img.exam
Studysize(MB)
%studytype
%storagetype
CT-Computerizedtomography 512x512 10-10000 299.93 28.58 65.11
CR-Computerizedradiography 048x2048 1 20.58 22.93 8.29
US-Ultrasounds 640x480 33.15 21.16 9.68
MR-Magneticresonance 256x256 100-10000 100.29 12.49 10.31
NM-Nuclearmedicine(NM) 128x128 30-60 3.82 5 0.24
MG-Digitalmammography 4000x5000 4 46 3.38 2.54
PT-PET 100.93 3 2.83
RF-Radiofrequency 8.85 1.85 0.61
XA-Angiography 28.65 0.96 0.17
OT-Other 7.84 0.66 0.22
Table VI. Storage by type at the Clínica Universidad de Navarra (University Hospital of Navarra)
Results
Withanaverageof110,000studiesayear,ahistoricallogof20terabytesandanestimatedannualgrowthrateof8TBperyearandanewmedicalimagingsystem,itwouldplacethecostofthestudyat €1.9comparedwiththe€8thatananalogchestx-raycancost.
Year1 Year2 Year3 Year4 Year5
Total €529,000 €529,000 €137,000 €140,000 €145,000
Table VII. Estimated costs in 5 years (includes storage, software licenses, communications, maintenance, etc.)
©2013 HIMSS 14
Otherbenefits:
• Thearchitectureandplatformofdigitalimagingallowyoutostoreanyothermultimediainformationthatcomesfrommedicaldevicesinstandardformat(DICOM).
• Improvessatisfactionofhealthcareprofessionals.
• Improvesreportpreparationtimes,particularlyrelevantforcriticalservices,suchas,forexample,theEmergencyDepartment.
• Facilitatesuniversalaccesstoanytypeofmedicalimaging.
• Facilitatesimplementationofsecondmedicalopinionsystemsandsharingofthepatient’scasereport.
• Improvesthesecurityofinformationwhenestablishingaccesscontrolsthroughauser/password.
• Itcanhelptoimprovethebillingcyclebyreducingthereportingtimes.
• Reducespatienttravel(forexample,betweenprimaryandspecializedcare).
• Improveswaitinglistmanagement,allowingthespecialisttoscreenpatientswhohavetobechecked.
©2013 HIMSS 15
Hospital medication processThehospitalmedicationprocess,fromanexclusivelyclinicalstandpoint,isclearlyoneofthemostcriticalareasoftheentirehospitalcaresystem,duetotheimportantimplicationsforqualityofcareandthepotentiallysignificantimpactonclinicalpatientsafety,whichinextremesituations,canposearisktothelifeofthesesameindividuals.
Fromapurelyfinancialpointofview,thisisanenvironmentinwhichhigh-volumeconsumptionandeconomiccostaremanaged,essentiallymedication,masterformularies,parenteralnutrition,etc.
Ourproposalrelatesexclusivelytotheautomationofthemedicationprocess,whichisshownschematicallybelow:
1 – Hospital medication process workflow
Themedicationprocessworkflowhasafewtypicalandstringentrequirementsintermsofdataandinteractionsamongprofessionals,toensureappropriatecommunicationbetweenthem,andeffectivedataexchangeinorderforthemtocorrectlymonitortasks.
AnICTimplementationprojectinthehospitalmedicationprocessshouldincludethefollowingobjectives:
Hospital medication process
Economic
Quality of care
Organizational
Saving on consumption
Time optimization
Prevention of legal costs
More collaborative work
Systems/schedule management
Continuity of care
Ability to use the information
Reduction of adverse events
Increase in the use of appropriate therapies
©2013 HIMSS 16
Results
Wewillalsolookattheproject’sresultindicatorsfromthreekeyreturnareas:
EconomicReturn:
• Totalconsumptionofmedicationinhospital.
• Totalconsumptionofmedicationinhospitalperpatient.
• %Return/Decreaseinmedicationduetoexpiration(Costofreturns/Totalcostofmedication,bothin€/yearor€/month).
• %Adjustmenttomedicationindication“highcost”or“critical”(No.ofprescriptionsadjustedtoindication/Totalno.ofprescriptionsofmedication,inayearormonth).
• %Returnofmedicationfromfactorytopharmacy(No.ofprescriptionsreturnedtopharmacy/Totalno.ofprescriptions,inayearormonth).
• Averagepharmaceuticalwrite-uptime(min/day).
• Averagepharmaceuticalvalidationtime(min/day).
• Averagetimefor“administrative”nursingtasks(min/day).
• Averagetimeforpharmacytechnicianpreparationanddispensing(min/day).
Clinicalreturns(qualityofcareandclinicalsafety):
• %Adverseprescriptionevents(No.ofadverseprescriptionevents/Totalno.ofprescriptions,inayearormonth,totalorbymedication).
• %Prescriptionsbasedonprotocol(No.ofprescriptionsbasedonprotocol/Totalno.ofprescriptions,inayearormonth,totalorbymedication).
• %Adverseadministrationevents(No.ofadverseadministrationevents/Totalno.ofprescriptions,inayearormonth,totalorbymedication).
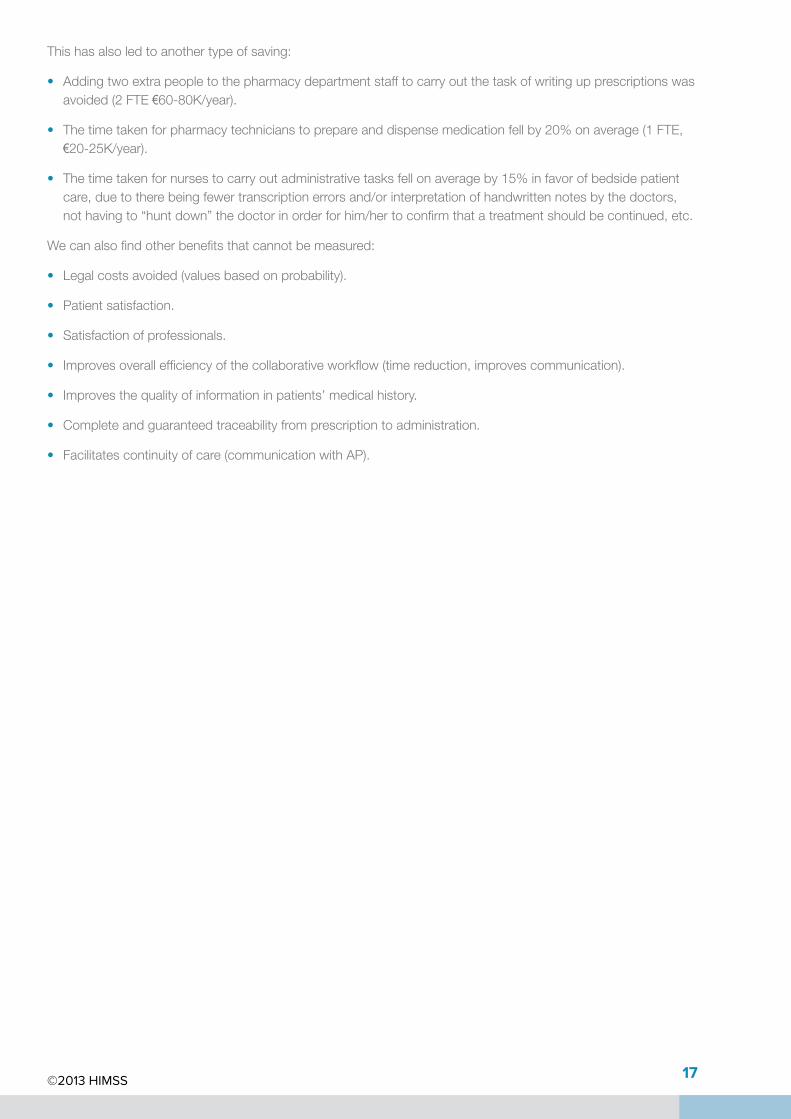
TheHospitalClinicdeBarcelonaisinvolvedinimplementingthehospitalmedicationprocedure,havingobtainedthefollowingresultssofar:
Before After Savings
Totalconsumptionofmedicationinhospital
€ /dayofstay €73 €62 15.7%
€ /patientdischarge €418 €347 16.99%
Totalconsumptionofanti‐infectivemedicationinhospital
€ /dayofstay €21 €16 28.57%
€ /patientdischarge €118 €97 17.80%
Genericprescriptionmedicationfordischargedpatients
%prescription 45% 57% 26.67%(increase)
Medicationstockmanagement
Daysinstock 27 19 29.63%
Table VIII – Savings achieved at the Hospital Clinic de Barcelona
©2013 HIMSS 17
Thishasalsoledtoanothertypeofsaving:
• Addingtwoextrapeopletothepharmacydepartmentstafftocarryoutthetaskofwritingupprescriptionswasavoided(2FTE€60-80K/year).
• Thetimetakenforpharmacytechnicianstoprepareanddispensemedicationfellby20%onaverage(1FTE,€20-25K/year).
• Thetimetakenfornursestocarryoutadministrativetasksfellonaverageby15%infavorofbedsidepatientcare,duetotherebeingfewertranscriptionerrorsand/orinterpretationofhandwrittennotesbythedoctors,nothavingto“huntdown”thedoctorinorderforhim/hertoconfirmthatatreatmentshouldbecontinued,etc.
Wecanalsofindotherbenefitsthatcannotbemeasured:
• Legalcostsavoided(valuesbasedonprobability).
• Patientsatisfaction.
• Satisfactionofprofessionals.
• Improvesoverallefficiencyofthecollaborativeworkflow(timereduction,improvescommunication).
• Improvesthequalityofinformationinpatients’medicalhistory.
• Completeandguaranteedtraceabilityfromprescriptiontoadministration.
• Facilitatescontinuityofcare(communicationwithAP).

©2013 HIMSS 18
Management of complex treatments in the day hospitalAllthemedicationsincludedinthecomplextreatmentscategoryhaveparticularcharacteristicsintermsoftheprescription,preparationand/oradministrationprocess,suchas,forexample:
• Forseriouspathologies:neurological,cardiovascular,musculoskeletalandchronicdiseasesorcancer,etc.
• Theycontainactivesubstancesthathavebeenrecentlyauthorized(withinthelast5years),sotheyareapriorityforthereportingofsuspectedadversereactions(RD1344/2007,orotherlawsdependingonthecountry).
• Next-generationmedication(geneticengineering).
• Hightreatmentcost.
• Orphandrugs.
• Medicationforrarediseases.
Therefore,takingintoaccountthecharacteristicsofthemedication,thoseofthepatientsandthenormaloperationofthedayhospital,aninformationandalertsystemisneeded,whichallowseffective,efficientandsafeautomationofstorage,queriesandmodificationsofallthedataassociatedwithtraceabilityofthepatientandthemedication.Thesearenecessarytocarryoutthemedicalcareprocessforthepatientwiththeutmostsafety,othinthedayhospitalandinthehealthorganization’spharmacyservice.
2 – Complex medication workflow procedure in the day hospital
Methodology
Toimplementanautomatedtraceabilitysystemforthecomplextreatmentprocess,wirelesslocalizationtechnologiescanbeused.Theinvestmentforthisneedstoberecoupedasdetailedinsubsequentsectionsoftheanalysis.
TheComplexoHospitalarioUniversitariodeACoruñainstalledanRFID+WIFIsystemforthemanagementofadayhospitalwithavolumeof1,000patients/yearwhoreceive6,380doses.Thefirst-yearexpenditureinconsumablesis€44,759.48,whichaddedtothecostsforhardwareandsoftwareinfrastructuregivesusatotalamount,includingthecostofthefirstyear,of€99,959.48.InformationindetailcanbeseenintablesIXandX
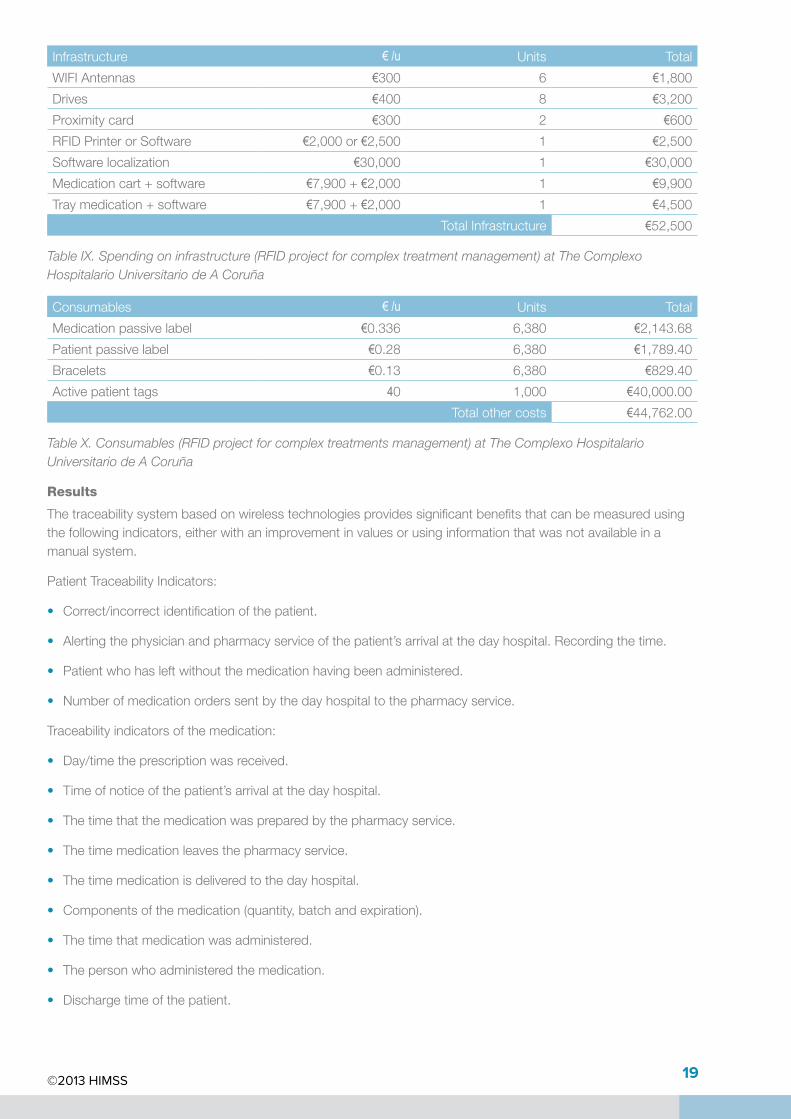
©2013 HIMSS 19
Infrastructure € /u Units Total
WIFIAntennas €300 6 €1,800
Drives €400 8 €3,200
Proximitycard €300 2 €600
RFIDPrinterorSoftware €2,000or€2,500 1 €2,500
Softwarelocalization €30,000 1 €30,000
Medicationcart+software €7,900+€2,000 1 €9,900
Traymedication+software €7,900+€2,000 1 €4,500
TotalInfrastructure €52,500
Table IX. Spending on infrastructure (RFID project for complex treatment management) at The Complexo Hospitalario Universitario de A Coruña
Consumables € /u Units Total
Medicationpassivelabel €0.336 6,380 €2,143.68
Patientpassivelabel €0.28 6,380 €1,789.40
Bracelets €0.13 6,380 €829.40
Activepatienttags 40 1,000 €40,000.00
Totalothercosts €44,762.00
Table X. Consumables (RFID project for complex treatments management) at The Complexo Hospitalario Universitario de A Coruña
Results
Thetraceabilitysystembasedonwirelesstechnologiesprovidessignificantbenefitsthatcanbemeasuredusingthefollowingindicators,eitherwithanimprovementinvaluesorusinginformationthatwasnotavailableinamanualsystem.
PatientTraceabilityIndicators:
• Correct/incorrectidentificationofthepatient.
• Alertingthephysicianandpharmacyserviceofthepatient’sarrivalatthedayhospital.Recordingthetime.
• Patientwhohasleftwithoutthemedicationhavingbeenadministered.
• Numberofmedicationorderssentbythedayhospitaltothepharmacyservice.
Traceabilityindicatorsofthemedication:
• Day/timetheprescriptionwasreceived.
• Timeofnoticeofthepatient’sarrivalatthedayhospital.
• Thetimethatthemedicationwaspreparedbythepharmacyservice.
• Thetimemedicationleavesthepharmacyservice.
• Thetimemedicationisdeliveredtothedayhospital.
• Componentsofthemedication(quantity,batchandexpiration).
• Thetimethatmedicationwasadministered.
• Thepersonwhoadministeredthemedication.
• Dischargetimeofthepatient.
©2013 HIMSS 20
CostIndicators:
• Patientwhohasleftwithoutthemedicationhavingbeenadministered.
• Medicationthatexpiresbeforebeingadministeredtothepatient.
• Costoftheunusedmedication:doselostornotused.
• Amountofmedicationreturnedbythedayhospital.
SafetyIndicators:
• Misidentificationofthepatient.
• Patientwhohasleftwithoutthemedicationhavingbeenadministered.
• Medicationthatexpiresbeforebeingadministeredtothepatient.
• Conditionsfortheprescriptionanduseofthemedication.
• Adverse/secondarypharmacologicaleffects:allergy,interaction,intoxication.
• Numberofadverseeventsprevented.
• Batchofthemedication.
• Expirationdate.
In2012thetotalcostofmedicationadministeredintheHospitaldeDíadelComplexoHospitalarioUniversitariodeACoruña,cameto€9,724,179.17.Althoughthereisnodefinitivedataatthetimeofwritingthisdocument,itisestimatedthattheimplementationofthesystemwillmeanasavingof15%(€1,458,626.88)ofthemedicationadministeredinthedayhospital.
ROI = 1,399%
Otherbenefitsobtained:
• Adeclineinadditionaldosepreparation.
• Animprovementinstockmanagement.
• Anincreaseinservicequalitythroughthedecreaseinorders.
• Significantimprovementsinthequalityandefficiencyofpatientcareandservicethroughautomationofprocessesand,therefore,adecreaseinthenumberofhumanerrorsasaresultofthedevelopmentoftheseprocesses.
• Contributestosustainabilityduetoincreasedefficiencyoftheprocesses,reducingthenumberofunuseddoses.
• Anincreaseinstaffsatisfactionthroughtheimplementationofimprovementactionsthroughouttheprocessprescription-validation-preparation/dosage-dispensing-administeringofmedicationtopatientsinthedayhospital.
• Anincreaseinpatientsafetyduringtheprescription-preparation-dispensingandadministeringprocess.And,therefore,areductionintheoccurrenceofadverseevents:
� Animprovementinthetraceabilityofthemedicinesadministered(batchandexpirationdate).
� Animprovementinpatientidentification,medicationandpatient/prescribedmedicationmatching.
� Availabilityinrealtimeandinauniqueinformationlabelrelevanttothepatient’ssafety:thepatient’sclinicaldata,composition,timeofpreparation,pharmacistresponsible,deliverytime,whoitwaspreparedby,stability,specialconditionsofuse,previousmedication,infusionrate,etc.
©2013 HIMSS 21
Nursing care managementThenursingcaremanagementprocess,fromanexclusivelyclinicalstandpoint,isclearlyoneoftheareasinthehospitalcareprocesswiththeheaviestworkloadsandvolumesofdocumentation.Thishasimportantimplicationsforthequalityofcareandwell-beingofpatientsduringtheirstayinhospital,aswellasfortheirclinicalsafety.
Fromafinancialpointofview,intermsofhumanresources,thisisthelargestareaofexpenditureforahospital,anditsplanningandcontrolareextremelycomplicated,duetothehighvolumeandthenecessityofmanagingteamsin24x7x365shifts.
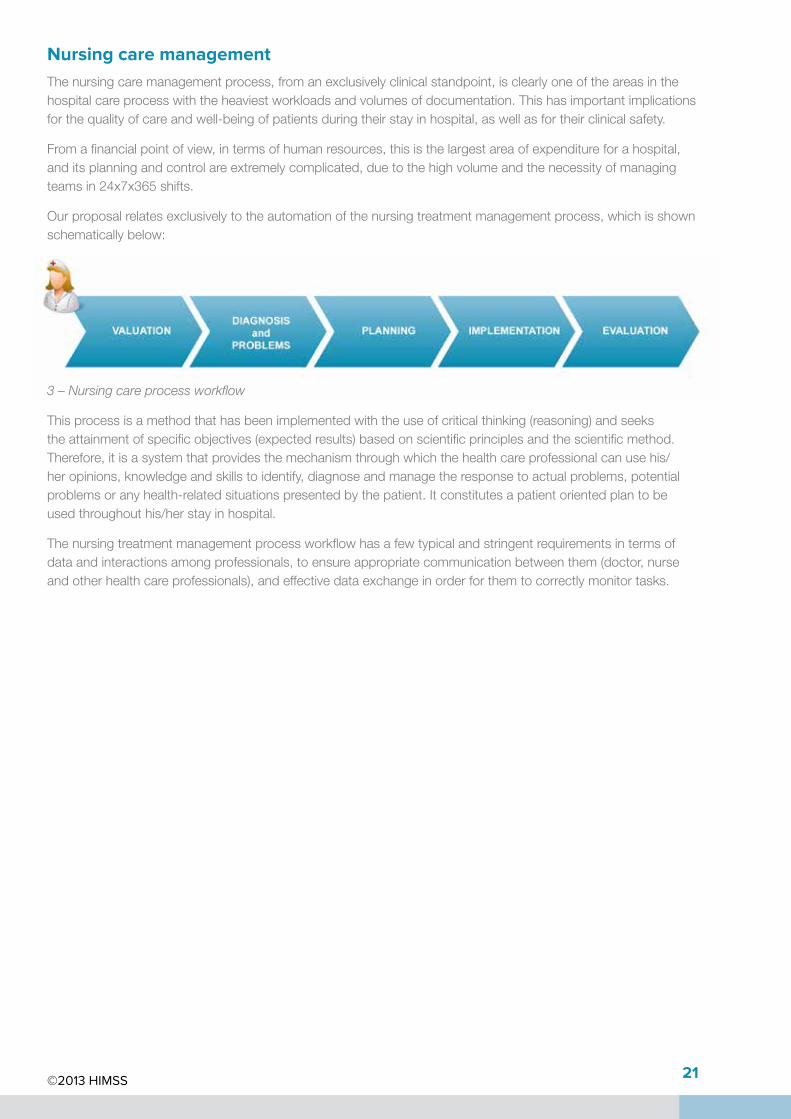
Ourproposalrelatesexclusivelytotheautomationofthenursingtreatmentmanagementprocess,whichisshownschematicallybelow:
3 – Nursing care process workflow
Thisprocessisamethodthathasbeenimplementedwiththeuseofcriticalthinking(reasoning)andseekstheattainmentofspecificobjectives(expectedresults)basedonscientificprinciplesandthescientificmethod.Therefore,itisasystemthatprovidesthemechanismthroughwhichthehealthcareprofessionalcanusehis/heropinions,knowledgeandskillstoidentify,diagnoseandmanagetheresponsetoactualproblems,potentialproblemsoranyhealth-relatedsituationspresentedbythepatient.Itconstitutesapatient‐orientedplantobeusedthroughouthis/herstayinhospital.
Thenursingtreatmentmanagementprocessworkflowhasafewtypicalandstringentrequirementsintermsofdataandinteractionsamongprofessionals,toensureappropriatecommunicationbetweenthem(doctor,nurseandotherhealthcareprofessionals),andeffectivedataexchangeinorderforthemtocorrectlymonitortasks.
©2013 HIMSS 22
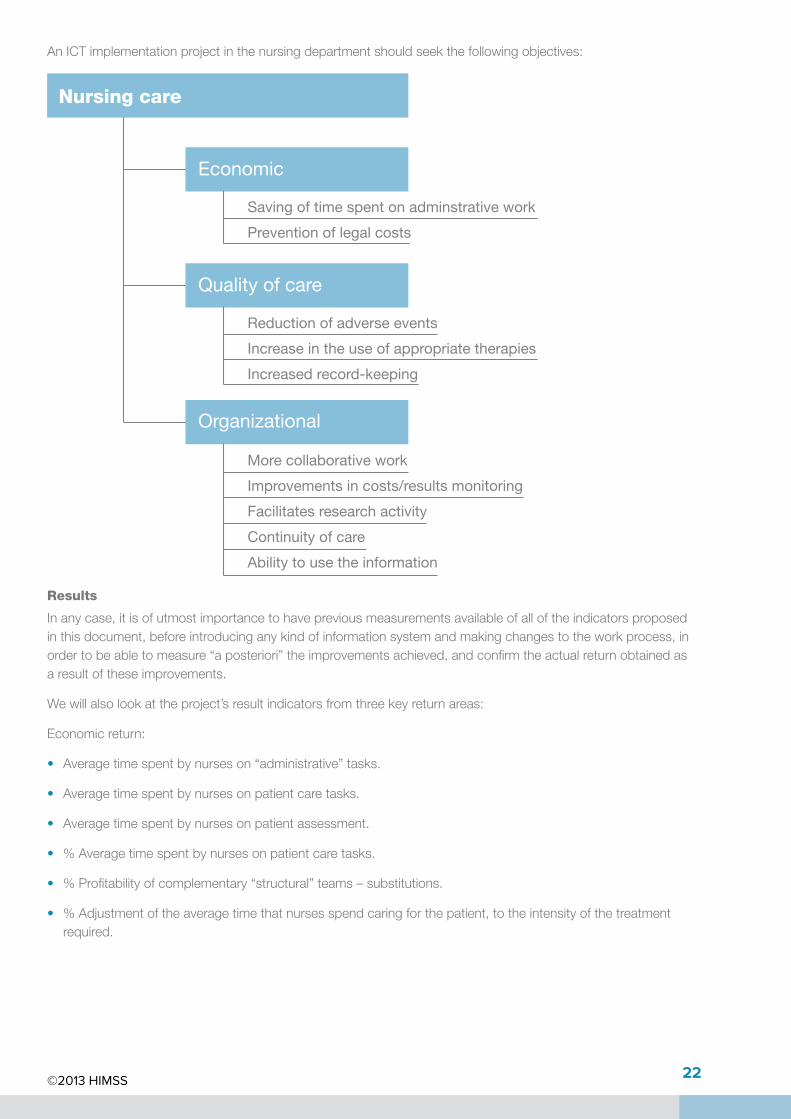
Nursing care
Economic
Quality of care
Organizational
Saving of time spent on adminstrative work
Prevention of legal costs
More collaborative work
Improvements in costs/results monitoring
Facilitates research activity
Continuity of care
Ability to use the information
Reduction of adverse events
Increase in the use of appropriate therapies
Increased record-keeping
AnICTimplementationprojectinthenursingdepartmentshouldseekthefollowingobjectives:
Results
Inanycase,itisofutmostimportancetohavepreviousmeasurementsavailableofalloftheindicatorsproposedinthisdocument,beforeintroducinganykindofinformationsystemandmakingchangestotheworkprocess,inordertobeabletomeasure“aposteriori”theimprovementsachieved,andconfirmtheactualreturnobtainedasaresultoftheseimprovements.
Wewillalsolookattheproject’sresultindicatorsfromthreekeyreturnareas:
Economicreturn:
• Averagetimespentbynurseson“administrative”tasks.
• Averagetimespentbynursesonpatientcaretasks.
• Averagetimespentbynursesonpatientassessment.
• %Averagetimespentbynursesonpatientcaretasks.
• %Profitabilityofcomplementary“structural”teams–substitutions.
• %Adjustmentoftheaveragetimethatnursesspendcaringforthepatient,totheintensityofthetreatmentrequired.
©2013 HIMSS 23
Clinicalreturns(qualityofcareandclinicalsafety):
• %Careplansbasedonprotocol.
• Indicators.
• %Adverseeventsofcareplans.
Non-quantifiableresults:
• Legalcostsavoided(valuecouldbecalculatedbasedonprobability).
• Patientsatisfaction.
• Satisfactionofprofessionals.
• Quantificationofthecostofcare(€,allowssubsequentmanagementandcostoptimization).
• Improvestheoverallefficiencyofthecollaborativeworkflow(reducedtimes,improvedcommunication).
• Improvescommunicationbetweenprofessionals(writtenrecord,relevance,acumen).
• Improvesthequalityofinformationinpatients’medicalhistory.
• Facilitates“continuity”ofcare(communicationwithAP).
• Facilitatesresearchactivities(forcontinuousimprovement).
©2013 HIMSS 24
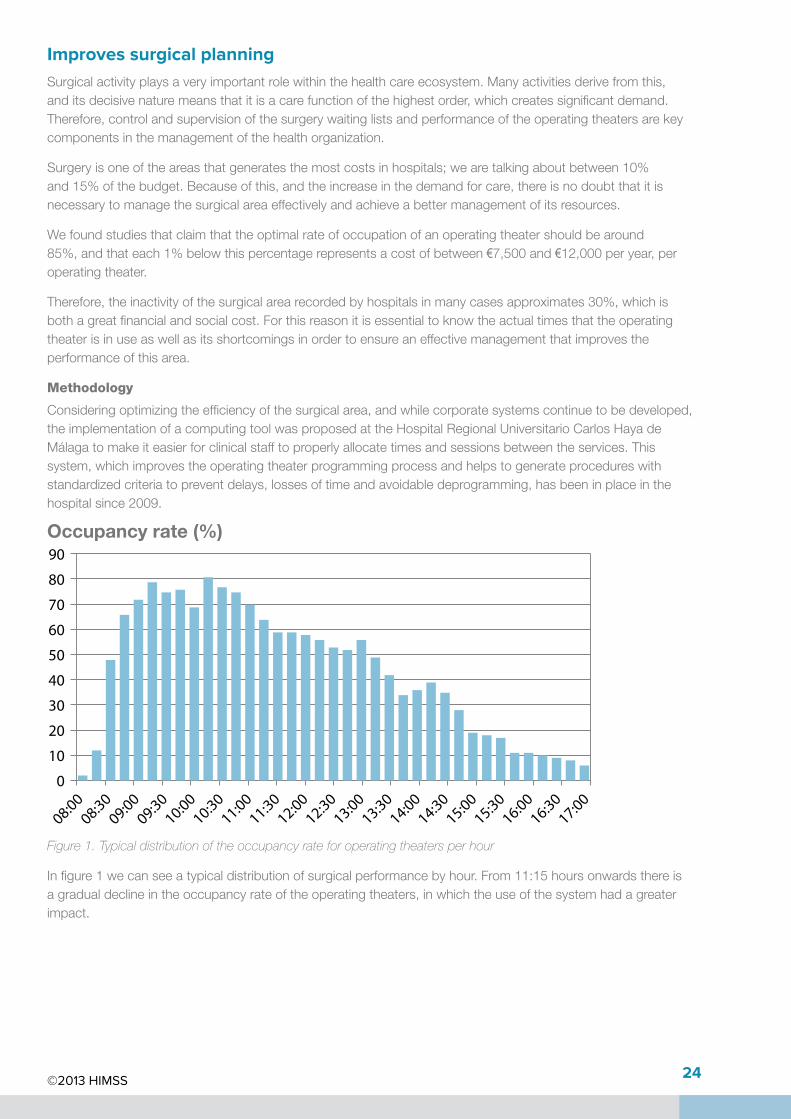
Improves surgical planningSurgicalactivityplaysaveryimportantrolewithinthehealthcareecosystem.Manyactivitiesderivefromthis,anditsdecisivenaturemeansthatitisacarefunctionofthehighestorder,whichcreatessignificantdemand.Therefore,controlandsupervisionofthesurgerywaitinglistsandperformanceoftheoperatingtheatersarekeycomponentsinthemanagementofthehealthorganization.
Surgeryisoneoftheareasthatgeneratesthemostcostsinhospitals;wearetalkingaboutbetween10%and15%ofthebudget.Becauseofthis,andtheincreaseinthedemandforcare,thereisnodoubtthatitisnecessarytomanagethesurgicalareaeffectivelyandachieveabettermanagementofitsresources.
Wefoundstudiesthatclaimthattheoptimalrateofoccupationofanoperatingtheatershouldbearound85%,andthateach1%belowthispercentagerepresentsacostofbetween€7,500and€12,000peryear,peroperatingtheater.
Therefore,theinactivityofthesurgicalarearecordedbyhospitalsinmanycasesapproximates30%,whichisbothagreatfinancialandsocialcost.Forthisreasonitisessentialtoknowtheactualtimesthattheoperatingtheaterisinuseaswellasitsshortcomingsinordertoensureaneffectivemanagementthatimprovestheperformanceofthisarea.
Methodology
Consideringoptimizingtheefficiencyofthesurgicalarea,andwhilecorporatesystemscontinuetobedeveloped,theimplementationofacomputingtoolwasproposedattheHospitalRegionalUniversitarioCarlosHayadeMálagatomakeiteasierforclinicalstafftoproperlyallocatetimesandsessionsbetweentheservices.Thissystem,whichimprovestheoperatingtheaterprogrammingprocessandhelpstogenerateprocedureswithstandardizedcriteriatopreventdelays,lossesoftimeandavoidabledeprogramming,hasbeeninplaceinthehospitalsince2009.
Occupancy rate (%)90
80
70
60
50
40
30
20
10
0
08:0008:30
09:0009:30
10:0010:30
11:0011:30
12:0012:30
13:0013:30
14:0014:30
15:0015:30
16:0016:30
17:00
76%
74%
72%
70%
68%
66%
64%
62%
60%
Jan ’0
9
Apr ’09
Jul ’0
9
Sep ’09
Jan ’1
0
Apr ’10
Jul ’1
0
Sep ’10
Jan ’1
1
Apr ’11
Jul ’1
1
Sep ’11
Jan ’1
2
Apr ’12
Jul ’1
2
Sep ’12
Figure 1. Typical distribution of the occupancy rate for operating theaters per hour
Infigure1wecanseeatypicaldistributionofsurgicalperformancebyhour.From11:15hoursonwardsthereisagradualdeclineintheoccupancyrateoftheoperatingtheaters,inwhichtheuseofthesystemhadagreaterimpact.
©2013 HIMSS 25
Results
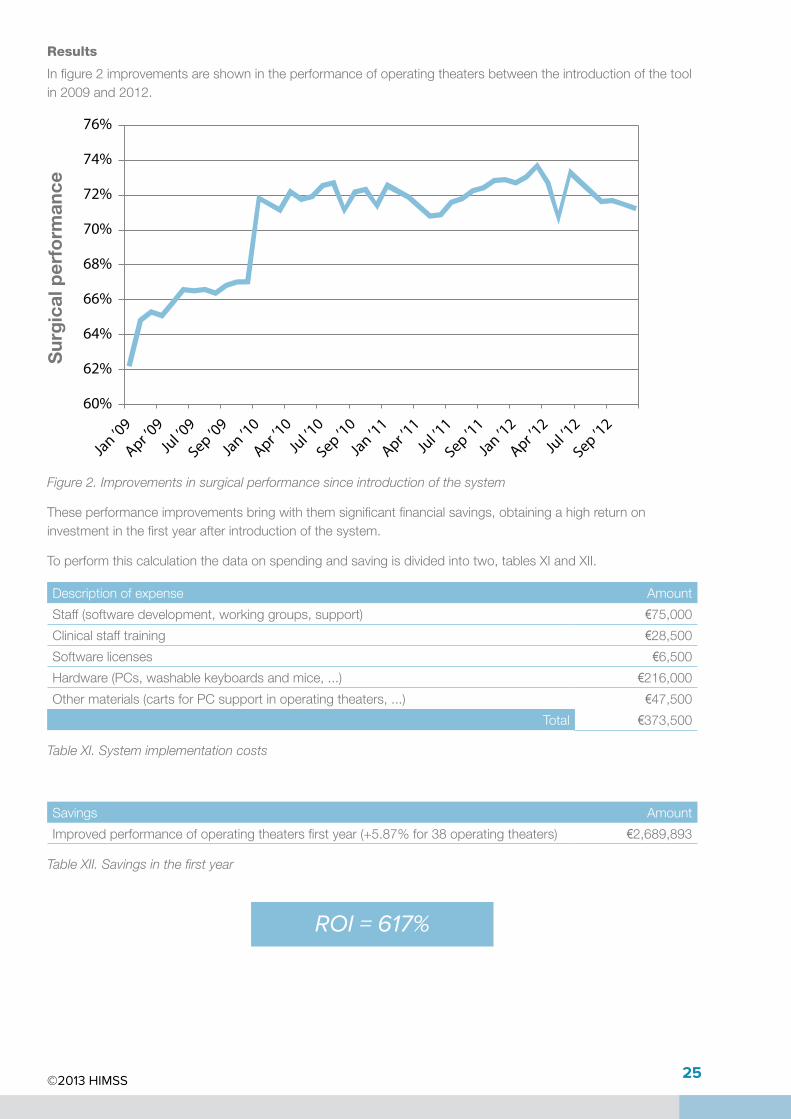
Infigure2improvementsareshownintheperformanceofoperatingtheatersbetweentheintroductionofthetoolin2009and2012.
90
80
70
60
50
40
30
20
10
0
08:0008:30
09:0009:30
10:0010:30
11:0011:30
12:0012:30
13:0013:30
14:0014:30
15:0015:30
16:0016:30
17:00
76%
74%
72%
70%
68%
66%
64%
62%
60%
Jan ’0
9
Apr ’09
Jul ’0
9
Sep ’09
Jan ’1
0
Apr ’10
Jul ’1
0
Sep ’10
Jan ’1
1
Apr ’11
Jul ’1
1
Sep ’11
Jan ’1
2
Apr ’12
Jul ’1
2
Sep ’12
Sur
gic
al p
erfo
rman
ce
Figure 2. Improvements in surgical performance since introduction of the system
Theseperformanceimprovementsbringwiththemsignificantfinancialsavings,obtainingahighreturnoninvestmentinthefirstyearafterintroductionofthesystem.
Toperformthiscalculationthedataonspendingandsavingisdividedintotwo,tablesXIandXII.
Descriptionofexpense Amount
Staff(softwaredevelopment,workinggroups,support) €75,000
Clinicalstafftraining €28,500
Softwarelicenses €6,500
Hardware(PCs,washablekeyboardsandmice,...) €216,000
Othermaterials(cartsforPCsupportinoperatingtheaters,...) €47,500
Total €373,500
Table XI. System implementation costs
Savings Amount
Improvedperformanceofoperatingtheatersfirstyear(+5.87%for38operatingtheaters) €2,689,893
Table XII. Savings in the first year
ROI = 617%

©2013 HIMSS 26
Thenumbersspeakforthemselves:theROIobtainedduringthefirstyearofimplementationattheHospitalRegionalUniversitarioCarlosHayaisveryhigh;however,otherbenefitsthatmaynotbeaseasytoquantifyshouldalsobenoted:
• Reductionofwaitinglists:
� Improveshealthcaresystemuseraccessibility.
� Improvespatientsatisfaction.
• Improvespatientsafety.
• Higherqualityofdata:
� Improvesqualityandcontinuityofcare.
� Hasapositiveimpactonthemanagementofthehealthorganization.
Finally,itisimportanttohighlightinparticularthewayinwhichtheWorldHealthOrganization’ssurgicalchecklisthasbeencomputerized,convertingitintoausefultoolwhichisveryeasytomanageinsidetheoperatingtheaters.ThedesignedsolutionhasbeenintegratedwiththeHospitalInformationSystem(HIS)toreceivepatientandproceduredatafromthis,andtosendtheresultsofthechecklisttotheElectronicMedicalRecord.Suchcomputerizationalsopreventstherequireditemsfrombeingaffectedasaresultofsometypeoferrororsimplyduetoanoversight,anditispossibletohaveanautomaticrecordofwhotheconfirmationwascarriedoutbyandwhen.
Theliteratureconsultedonsimilarimplementationsshowsomespectacularresults.Inparticular,thecenterswheretheresultsarecomparedbeforeestablishingthesurgicalchecklistandafteritsintroduction,confirmtheusefulnessofthesurgicalchecklistsasthenumberofcomplicationsfromsurgeryfellfrom27.3%to16.7%,andthemortalityratedeclinedfrom1.5%to0.8%.Theyalsoshowthatinthemajorityofcases,theresponsibilityusuallylieswiththeentireteam(surgeon,nurseandanesthetist),andthat,hadtherebeenachecklist,themajorityoftheseerrorswouldnothaveoccurred.
©2013 HIMSS 27
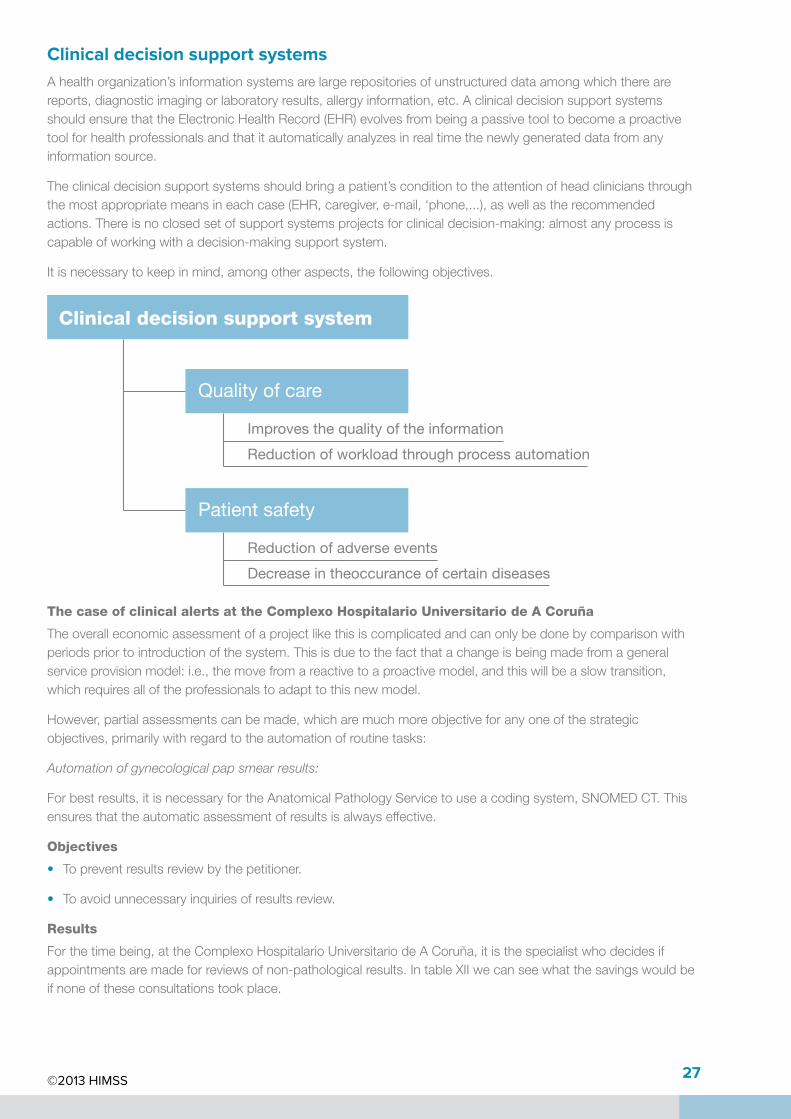
Clinical decision support systemsAhealthorganization’sinformationsystemsarelargerepositoriesofunstructureddataamongwhichtherearereports,diagnosticimagingorlaboratoryresults,allergyinformation,etc.AclinicaldecisionsupportsystemsshouldensurethattheElectronicHealthRecord(EHR)evolvesfrombeingapassivetooltobecomeaproactivetoolforhealthprofessionalsandthatitautomaticallyanalyzesinrealtimethenewlygenerateddatafromanyinformationsource.
Theclinicaldecisionsupportsystemsshouldbringapatient’sconditiontotheattentionofheadcliniciansthroughthemostappropriatemeansineachcase(EHR,caregiver,e-mail,‘phone,...),aswellastherecommendedactions.Thereisnoclosedsetofsupportsystemsprojectsforclinicaldecision-making:almostanyprocessiscapableofworkingwithadecision-makingsupportsystem.
Itisnecessarytokeepinmind,amongotheraspects,thefollowingobjectives.
Clinical decision support system
Quality of care
Patient safety
Improves the quality of the information
Reduction of workload through process automation
Reduction of adverse events
Decrease in theoccurance of certain diseases
The case of clinical alerts at the Complexo Hospitalario Universitario de A Coruña
Theoveralleconomicassessmentofaprojectlikethisiscomplicatedandcanonlybedonebycomparisonwithperiodspriortointroductionofthesystem.Thisisduetothefactthatachangeisbeingmadefromageneralserviceprovisionmodel:i.e.,themovefromareactivetoaproactivemodel,andthiswillbeaslowtransition,whichrequiresalloftheprofessionalstoadapttothisnewmodel.
However,partialassessmentscanbemade,whicharemuchmoreobjectiveforanyoneofthestrategicobjectives,primarilywithregardtotheautomationofroutinetasks:
Automation of gynecological pap smear results:
Forbestresults,itisnecessaryfortheAnatomicalPathologyServicetouseacodingsystem,SNOMEDCT.Thisensuresthattheautomaticassessmentofresultsisalwayseffective.
Objectives
• Topreventresultsreviewbythepetitioner.
• Toavoidunnecessaryinquiriesofresultsreview.
Results
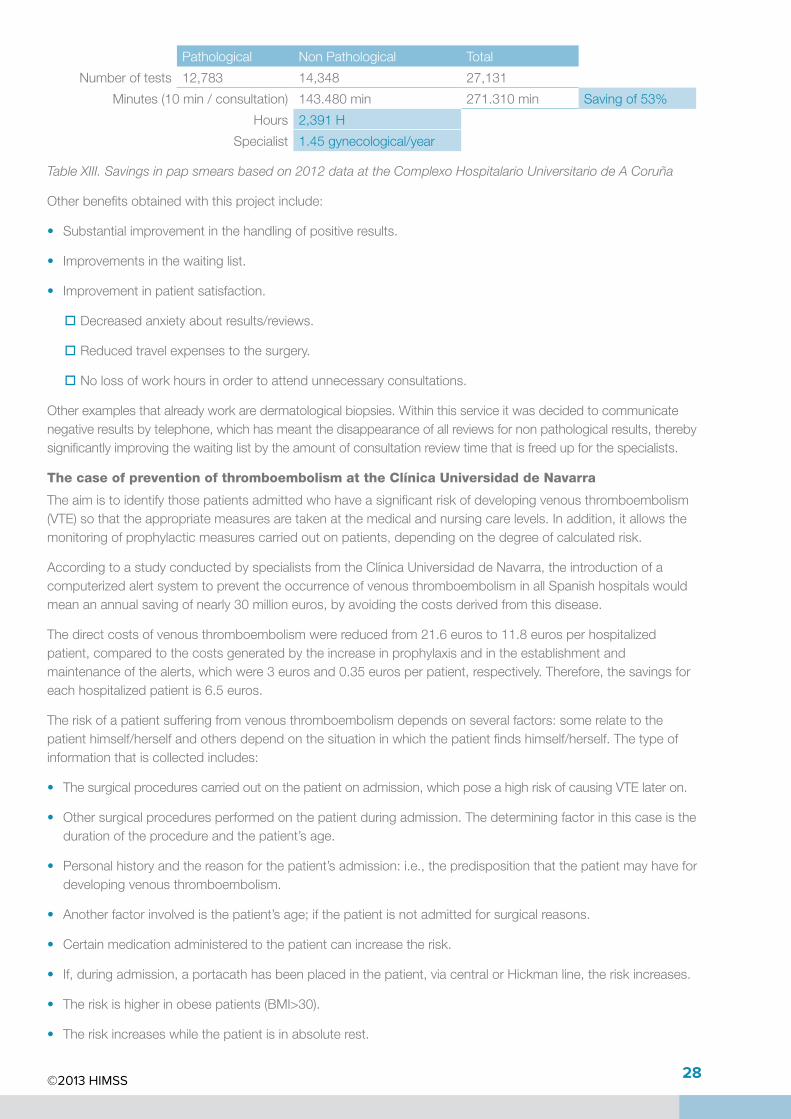
Forthetimebeing,attheComplexoHospitalarioUniversitariodeACoruña,itisthespecialistwhodecidesifappointmentsaremadeforreviewsofnon-pathologicalresults.IntableXIIwecanseewhatthesavingswouldbeifnoneoftheseconsultationstookplace.
©2013 HIMSS 28
Pathological NonPathological Total
Numberoftests 12,783 14,348 27,131
Minutes(10min/consultation) 143.480min 271.310min Savingof53%
Hours 2,391H
Specialist 1.45gynecological/year
Table XIII. Savings in pap smears based on 2012 data at the Complexo Hospitalario Universitario de A Coruña
Otherbenefitsobtainedwiththisprojectinclude:
• Substantialimprovementinthehandlingofpositiveresults.
• Improvementsinthewaitinglist.
• Improvementinpatientsatisfaction.
� Decreasedanxietyaboutresults/reviews.
� Reducedtravelexpensestothesurgery.
� Nolossofworkhoursinordertoattendunnecessaryconsultations.
Otherexamplesthatalreadyworkaredermatologicalbiopsies.Withinthisserviceitwasdecidedtocommunicatenegativeresultsbytelephone,whichhasmeantthedisappearanceofallreviewsfornon‐pathologicalresults,therebysignificantlyimprovingthewaitinglistbytheamountofconsultationreviewtimethatisfreedupforthespecialists.
The case of prevention of thromboembolism at the Clínica Universidad de Navarra
Theaimistoidentifythosepatientsadmittedwhohaveasignificantriskofdevelopingvenousthromboembolism(VTE)sothattheappropriatemeasuresaretakenatthemedicalandnursingcarelevels.Inaddition,itallowsthemonitoringofprophylacticmeasurescarriedoutonpatients,dependingonthedegreeofcalculatedrisk.
AccordingtoastudyconductedbyspecialistsfromtheClínicaUniversidaddeNavarra,theintroductionofacomputerizedalertsystemtopreventtheoccurrenceofvenousthromboembolisminallSpanishhospitalswouldmeananannualsavingofnearly30millioneuros,byavoidingthecostsderivedfromthisdisease.
Thedirectcostsofvenousthromboembolismwerereducedfrom21.6eurosto11.8eurosperhospitalizedpatient,comparedtothecostsgeneratedbytheincreaseinprophylaxisandintheestablishmentandmaintenanceofthealerts,whichwere3eurosand0.35eurosperpatient,respectively.Therefore,thesavingsforeachhospitalizedpatientis6.5euros.
Theriskofapatientsufferingfromvenousthromboembolismdependsonseveralfactors:somerelatetothepatienthimself/herselfandothersdependonthesituationinwhichthepatientfindshimself/herself.Thetypeofinformationthatiscollectedincludes:
• Thesurgicalprocedurescarriedoutonthepatientonadmission,whichposeahighriskofcausingVTElateron.
• Othersurgicalproceduresperformedonthepatientduringadmission.Thedeterminingfactorinthiscaseisthedurationoftheprocedureandthepatient’sage.
• Personalhistoryandthereasonforthepatient’sadmission:i.e.,thepredispositionthatthepatientmayhavefordevelopingvenousthromboembolism.
• Anotherfactorinvolvedisthepatient’sage;ifthepatientisnotadmittedforsurgicalreasons.
• Certainmedicationadministeredtothepatientcanincreasetherisk.
• If,duringadmission,aportacathhasbeenplacedinthepatient,viacentralorHickmanline,theriskincreases.
• Theriskishigherinobesepatients(BMI>30).
• Theriskincreaseswhilethepatientisinabsoluterest.
©2013 HIMSS 29
Alloftheabovefactorsareinvolvedinthecalculationoftheriskofsufferingfromathromboembolism.Allofthisdataiscollectedfromthevariousinformationsystemmodules:nursingcare,doctor’sorders,nursingrecordofvitalsignsandprocedurescarriedout.
The case of the Sepsis clinical pathway at the Hospital Marina Salud de Dénia
FourteenSpanishscientificcompaniessignedtheDeclarationofMajorcainNovember2012topromotethecreationofCodeSepsis,bothatthelocallevelaswellasattheinstitutionallevelsupportedbynationalhealthauthoritiesandthedifferentAutonomousCommunities.Theaimof“CodeSepsis”istheearlydetectionofpatientswithsevereSepsis(inthedifferentlevelsofcare),thestructuredapplicationofthesetofrecommendedmeasuresinordertodiagnose,monitorandtreatthesepatients,andthedefinitionofafewcareindicatorsforassessingcompliancewiththerecommendationsandtheresultsoftheapplicationofthecodeatthelocalandnationallevel.
TheoptimizationofSepsismanagementisassociatedwithareductioninhealthcarecosts,whicharecurrentlyquantifiedataround€17,000percase.
Methodology
TheSepsisprotocolisbasedonthefollowingkeypoints:
1. TheSepsisRule:“Acontinuousandongoingradarorguard”ofthedatastoredinthepatient’sEHR,whichwillalertuswhenapatientmeetsthepredefinedSepsiscriteria,andwhosefunctionistheearlydetectionofSepsis.
2. Aclinicalpathwayof“SevereSepsisandSepticShock,first6hours,”whichconstitutesaremindersystemthatdisplaysadiagnosticandtherapeuticroadmap,activatingtheSepsisteamandcollectinginastandardizedmannerthediagnosticandtherapeuticmeasurestobecarriedoutinthefirst6hours,associatedwithdecreasedmortality,andrangingfromtheparameterstobemonitored,relevantparametersforthemicrobiologicaldiagnosisandsourcecontrol,theoptimalempiricalantibiotictreatmentforeachclinicalsituationandhemodynamicresuscitation.Allofthis,assupportforthephysician,withoutlimitingthemodificationsthattheymaywanttomakeaccordingtotheirbestjudgment.
Objectives
• ToreducethenumberofcasesofSepsisperyearineachofthe3stages(septicshock,SepsisandsevereSepsis).
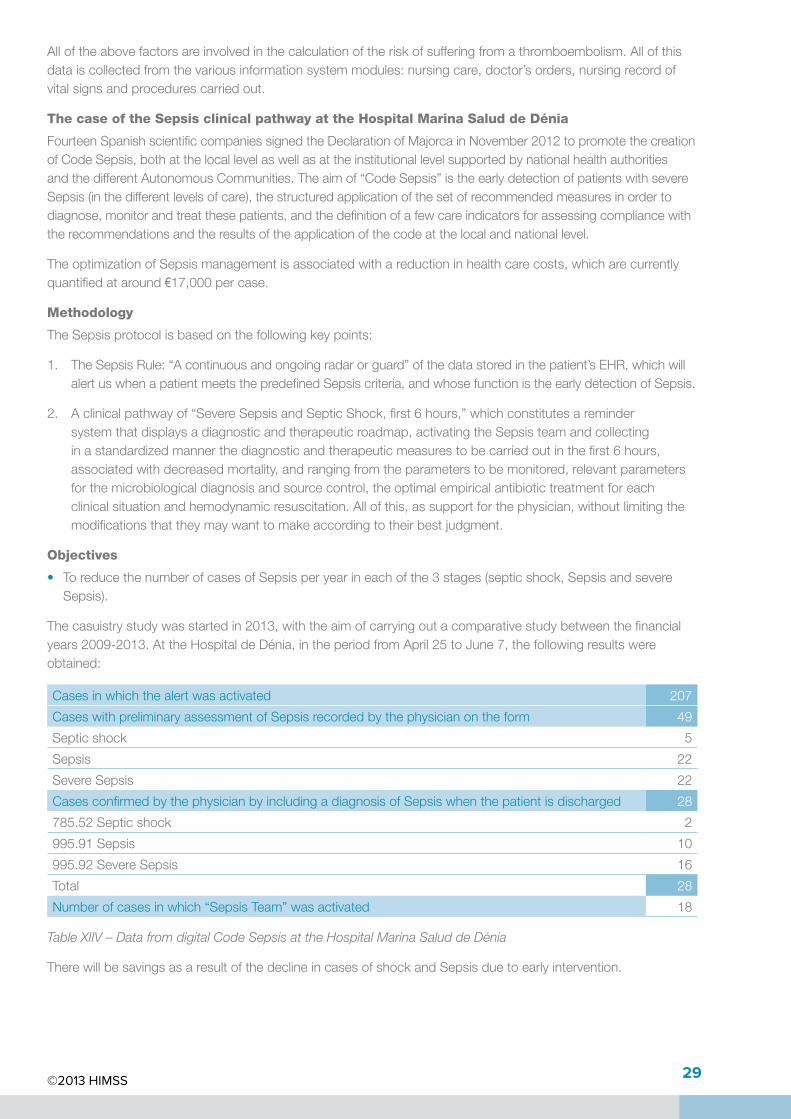
Thecasuistrystudywasstartedin2013,withtheaimofcarryingoutacomparativestudybetweenthefinancialyears2009-2013.AttheHospitaldeDénia,intheperiodfromApril25toJune7,thefollowingresultswereobtained:
Casesinwhichthealertwasactivated 207
CaseswithpreliminaryassessmentofSepsisrecordedbythephysicianontheform 49
Septicshock 5
Sepsis 22
SevereSepsis 22
CasesconfirmedbythephysicianbyincludingadiagnosisofSepsiswhenthepatientisdischarged 28
785.52Septicshock 2
995.91Sepsis 10
995.92SevereSepsis 16
Total 28
Numberofcasesinwhich“SepsisTeam”wasactivated 18
Table XIIV – Data from digital Code Sepsis at the Hospital Marina Salud de Dénia
TherewillbesavingsasaresultofthedeclineincasesofshockandSepsisduetoearlyintervention.
©2013 HIMSS 30
Non face-to-face servicesWhenwetalkaboutnonface-to-faceserviceswerefertothoseserviceswhichduetoICThelpimprovecareservicesortheclinicalcoordinationbetweenprofessionalsand/orpatientssuchastelemedicine,telecareorcollaborativeworkplatforms.TheseprojectsaremadepossibleasaresultofICTandenablethetransformationofclinicalprocesses,systemrestructuringandtheconnectionofprofessionalsandhospitalswithotherhealthcentersinremotelocations.
Asynchronous Telemedicine
Foryearsasynchronousandsynchronoustelemedicinehasbeenusedfordifferentprocessesandspecialties.Inseveralspecialtiesithasbeenconfirmedthatasynchronoustelemedicineprojectsproducethefollowingresults:
• Eliminationofunnecessarytravelofthepatienttothehospital.
• Reductioninthediagnosistimeincasesoflowandmediumcomplexity.
• Sharingofknowledgebetweenspecialistsandfamilyphysicians.
• Providestheopportunitytoworkwithexpertsfromoutsidetheorganization.
• Acceptanceonalargescaleofthetechnologicalsolutionbyphysiciansandspecialists.
• Reductioninwaitingliststoseeamedicalspecialist.
• Preventsduplicationofdiagnostictests.
However,ithasalwayscostalottosetupthetelemedicineprocessasamoreacceptedsystemwithinthehealthorganization.Whilethetechnologyisreadyandvalidated,itinvolvesachangeintheprocessandinthecoordinationofcarethataffectsdifferentclinicalunitsbothinsideandoutsidethehospital.However,technologyadvancesanditallowsyoutotakeanotherstepforward,notonlybyfacilitatingtheexchangeofimagesbutalsobyprocessingtheseimages.
Forexample,thedevelopmentofasoftwaresystemfortheautomaticscreeningofdiabeticretinopathyimagesenablesearlydetectionofthediseaseinthediabeticpopulation.Automaticprocessingisshowntobeareliablemeansofobtainingafirstleveldiagnosiswithoutrequiringspecialistintervention.
DiabetesisthesecondcauseofblindnessinSpainandtheprimarycauseoftotallossofvisionintheworkingagepopulation.Itisestimatedthatbetween15%and30%ofpeoplewithdiabetessufferfromdiabeticretinopathy.Thebestprotectionagainsttheprogressionofthisdisease,inadditiontocontrollingdiabetes,istheearlydetectionoftheretinopathythroughperiodicchecksinwhichFundusphotographyiscarriedoutinbotheyesofchronicpatients.
Afterthetakingofimages,eachFundusphotographshouldbecheckedanaverageoftwotimesbyqualifiedspecialists,throughaslowprocess,whichistediousandexpensive,withtheaimofissuinganaccuratediagnosis.
Todaytherearenonface-to-facecapture,transmissionandimaginganalysissystems.
TheimagesobtainedbytheFundusphotographsaresentsecurelytoacentralizedrepository(thecloud),fromwhereanautomaticscreeningalgorithm(alsointhecloud)evaluatesanddetectsthepresenceorabsenceofretinallesions.Ophthalmologistscanconsultthescreeningresultsdirectly,beingabletofilterthosepatientswithlesionsforasubsequentexaminationandtheissuingofanewdiagnosis.
Trialswiththefollowingresultshavebeencarriedout:
• 15,000patientsexaminedinoneyear.
• 20%diagnosedwithdiabeticretinopathy.
• 95%sensitivityandspecificityof70%.
• Theworkloadofdoctorswasreducedby45%anditallowsthespecialisttofocusonthepatients’pathologies.
©2013 HIMSS 31
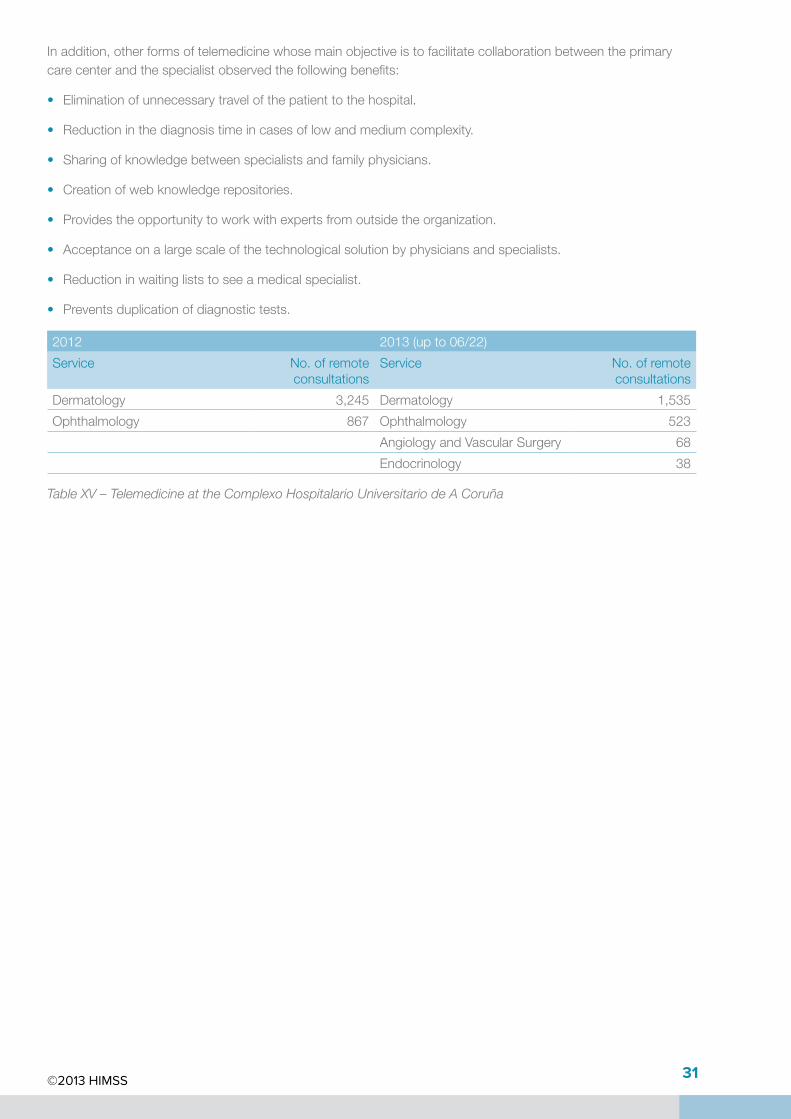
Inaddition,otherformsoftelemedicinewhosemainobjectiveistofacilitatecollaborationbetweentheprimarycarecenterandthespecialistobservedthefollowingbenefits:
• Eliminationofunnecessarytravelofthepatienttothehospital.
• Reductioninthediagnosistimeincasesoflowandmediumcomplexity.
• Sharingofknowledgebetweenspecialistsandfamilyphysicians.
• Creationofwebknowledgerepositories.
• Providestheopportunitytoworkwithexpertsfromoutsidetheorganization.
• Acceptanceonalargescaleofthetechnologicalsolutionbyphysiciansandspecialists.
• Reductioninwaitingliststoseeamedicalspecialist.
• Preventsduplicationofdiagnostictests.
2012 2013(upto06/22)
Service No.ofremoteconsultations
Service No.ofremoteconsultations
Dermatology 3,245 Dermatology 1,535
Ophthalmology 867 Ophthalmology 523
AngiologyandVascularSurgery 68
Endocrinology 38
Table XV – Telemedicine at the Complexo Hospitalario Universitario de A Coruña
©2013 HIMSS 32
Health 2.0: Collaborative environments
Socialnetworks,collaborativetoolsandweb2.0haveledtoarevolutionintheformationofnewvirtualcommunitiesthatcommunicate,shareandcollaborateonaglobalanduniversalbasis.Theysharephotos,personalcomments,messagesandprofessionalinformation.Anyonecanhaveanonlineprofileonanyofthereferencedsites(LinkedIn,Facebook,Twitter,etc.).
Inhealthcare,theuseofthistypeoftoolcreatesnewandinterestingscenarioswherethesharingandcollaborationofknowledgecanhelpfostertheobtainingofafasterandmoreaccuratediagnosisaswellastoconnectpatientswithpatients,doctorswithdoctorsanddoctorswithpatients.
TherearemanyinitiativesfortheuseofspecificorstandardtoolsforHealth2.0projects.Manyaredangerous,oldordisruptive.Someareconsolidatingandallowthetraditionalformsofclinicalcollaborationtobechanged.Werefertoprojectsthatenablecollaborationbetweenclinicalprofessionalsforthediscussionandsharingofclinicalcaseswheretherisktoprivacyisminimal(anonymousclinicalcase)andtheresultingcareisimprovedthankstothecollaborativecare.Projectsthatprovideasecondmedicalopinionbyspecialistslocatedremotely;collaborationwithlessdevelopedcountries(Spain-Africa);knowledgesharingformedicaltraining;accesstospecialistsinanypartoftheworldorvirtualtumorcommittees.
Itallowsyoutoorganizevirtualtumorcommitteeswithprofessionalsfromdifferenthospitals.
Theworkflowisbasedonthecreationandsharingofclinicalcasesthatarepresentedattumorcommitteemeetings.Thiscaseissharedprivatelyamongagroupofprofessionalstoencouragethemultidisciplinaryapproach.Itgeneratesadiscussionthroughcommentsontheclinicalcaseinordertomakedecisionsaboutthetreatment,diagnosisormonitoringofthesame.
Afterthesurveywasconductedontherelevantusers,itwasconcluded:
Thatthethreebasicreasonsforacceptingandusingaprofessionalcollaborativeplatformare:
• Rapiddecision-making,predictionofdecisionsandpreparationofcases.
• Inclusionofalltheclinicalelementsnecessaryfordiagnosis(casesummary,images,documents,reports).
• Whenthebindingdecision,madeinthetumorcommittee,isrecorded,thatitsimplementationispromotedinpractice.
• Thepossibilityofdevelopingnonface-to-facecommittees,helpindecision-makingandencouragingparticipationbetweenhospitals.
Benefitsobserved:
• Facilitateshomogeneityintheinformationforpresentationofclinicalcases.
• Compactstherelevantinformationonclinicalcases,whichcentersthedecision-makingprocessfirmlywithintheTumorsCommittee.
• Predictsanddocumentstheopinionsofdifferentspecialties/specialistsinvolvedintheTumorCommittee.
• Standardizescommunicationbetweenhospitalsthatreferclinicalcases.
• RecordsthecasestreatedintheTumorCommitteesasanimportantsourceofteachingandresearchmaterial.
• Improvesthequalityofhealthcaregiventothepatient:multidisciplinaryapproach.
• User(clinical)assessmentisverypositive.
• Preventsrepetitionofcomplementarytestsinpatientscomingfromotherservicesorhospitals.
• Helpstoreducewaitingtimes.Additionalguidanceonearlytreatmentbysharingthesameinformationfromapatientinrealtime.
©2013 HIMSS 33
• Facilitatestheselectionofpatientsforinclusioninclinicaltrials(costsavingsforthehospital).
• Enhancesandpromotescollaborationwithintheindustry:powerfultoolwithwhichtopromoteclinicalresearchinthehospital.
• Improvessystemmanagement.FacilitatestheTumorCommittee’sselfmanagement.
• Supportsthedisseminationofpublications.
• StandardizationofclinicalpracticeinnewproceduressuchasIORT(intraoperativeradiationtherapy).
• Teaching:Repositoryofmedicalknowledgethatisusedinthetrainingofmedicalstudentsandresidents.
SomecentersarerethinkingtheworkingsofthecommitteesbothinsidethehospitalandattheAutonomousCommunitylevel.Thereorganizingofhealthcareservicescanevenbecontemplatedthroughaconcentrationofspecializedkeyservices(oncology,dermatology,ophthalmology).
©2013 HIMSS 34
References
[1]. MacarioA.Areyouroperatingrooms‘efficient’?ORManager.2007;23:16-8.
[2]. [NúñezC.Computerizationofthesurgicalblock,thekeytohealthinthetwenty-firstcentury.TodoHospital.2008;248:432-3.
[3]. Antares.IntegratedmanagementprojectoftheSurgicalBlock.AntaresConsulting;2008.
[4]. LingardL,RegehrG,OrserB,ReznikR,BakerG,DoranDetal.Evaluationofapreoperativechecklistandteambriefingamongsurgeons,nurses,andanaesthesiologiststoreducefailuresincommunication.ArchSurg.2008;143:12-18.
[5]. DíazJ,CanoJ,JiménezAandAlonsoA.Software-assistedimprovementofsurgicalmanagementatCarlosHayaRegionalUniversityHospitalinMalaga,Spain.In:FinalProgramandBookofAbstracts:4thInternationalJointConferenceonBiomedicalEngineeringSystemsandTechnologies.Rome,Italy;2011.p.155-6.
[6]. BotchkarevA,AndruP.AReturnonInvestmentasametricforevaluatinginformationsystems:taxonomyandapplication.InterdisciplinaryJournalofInformation,KnowledgeandManagement.2011;6:245-69.
[7]. ldenSolovy,BarryChaikenM.D.–2003–“ROIunderscrutiny:theradicalredefinitionofacoreconcept”–FrontiersofHealthservicesmanagement19(3)http://www.docsnetwork.com/articles/BPC03130.pdf
[8]. DouglasGoldstein,PeterGroen–18/7/2006–“ValuemeasurementandreturnoninvestmentforEHRs”–VirtualMedicalworlds.http://www.hoise.com/vmw/06/articles/vmw/LV-VM-08-06-19.html
[9]. BobHerman–3/10/2012–“6wayshospitalscananalyzetechnology’sreturnoninvestment”–Becker’sHospitalreviewhttp://www.beckershospitalreview.com/healthcare-information-technology/6-ways-hospitals-can-analyze-technologys-return-on-investment.html
[10]. HIMSS–4/3/2013–“2013HIMSSiHITReport”http://himss.files.cms-plus.com/newsletters/ClinicalInformatics/HIMSS%202013%20iHIT%20Study.pdf
[11]. P.J.Murray,M.Cabrer,M.Hansen,C.Paton,P.L.Elkin,W.S.ErdleyTowardsAddressingtheOpportunitiesandChallengesofWeb2.0forHealthandInformaticsIMIAYearbookofMedicalInformatics200831:44-51.
[12]. ORManager.WHOsurgicalsafetychecklistlinkedtofewerdeaths,complications.ORManager.2009;25:7-8.
[13]. VriesE,PrinsH,CrollaR,OuterA,AndelG,HeldenSetal.EffectofaComprehensiveSurgicalSafetySystemonPatientOutcomes.NEnglJMed.2010;363:1928-37.
[14]. LecumberriR,PanizoE,Gomez-GuiuA,etal.Economicimpactofanelectronicalertsystemtopreventvenousthromboembolisminhospitalisedpatients.JThrombHaemost2011;9:1108-15
©2013 HIMSS 35
