factor vii inhibitor
TRANSCRIPT

Factor VII Inhibitor
EARL CAMPBELL, M.D.*
SALAHATI’IN SANAL. M.D.
JOAN MAlTSON. M.D.
LEO WALKER, M.D.. SUZANNE ESTRY, MS.
LOUISE MUELLER, MS.
MANFRED SCHWARZ. MS. SUE HAMPTON, B.S.
East Lansing, Michigan
From the Departments of Medicine and Pathol- ogy, College of Human Medicine, Michigan State University, East Lansing, Michigan: and St. Lawrence Hospital, East Lansing, Michigan. Requests for reprints should be addressed to Dr. Earl Campbell. Manuscript accepted August 23, 1979.
* Present address: Department of Medicine, Medical College of Ohio, C.S. 10006. Toledo. Ohio 43699.
Factor VII inhibitor activity was identified in a 66 year old man with probable bronchogerdc carcinoma. Initial studies indicated a normal partial tbromboplastin time (PTlJ and a prothrombin time (ITJ prolongation which increased with incubation. PT correction failed to occur with 50 per cent normal plasma in vitro and 2 U of fresh frozen plasma in vivo, indicating inhibitor activity. Specific factor assay levels fell within normal limits except for a factor VII level of 30 per cent. Subquent evaluation with andglobulin studies sug- gested an inhibitor of immunoglobulin G [IgG] origin.
The occurrence of inhibitors to coagulaiion factors is infrequent and best understood in those with factor VIII hemophilia in whom the in- cidence ranges between 8 and 14 per cent, presumably related to fre- quent transfusion of exogenous factor VIII. Coagulation factor inhib- itors tend to occur as secondary features of collagen diseases, dys- proteinemias, amyloidosis, blood product transfusions and, less fre- quently, as apparent idiopathic events. A clinically significant factor VII inhibitor has not been documented prior to this time in the English language literature [1,2).
CASE REPORT
A 66 year old white man was admitted for evaluation following roentgeno- graphic evidence of an abnormal mass in the upper lobe of the right lung. Contributory history included a’beater than %pacWyear smoking habit, a five year history of chronic bronchitis, an absence of prior tuberculosis or fungal disorder, a 15 pound weight loss during two months prior to hospitalization, a recent loss of appetite and ankle edema. No history of bone, joint or con- nective tissue disorders was elicited.
At admission the patient was noted to be well developed, without significant emaciation, and in no acute distress. Vital signs, aside from a respiratory rate of Wmin, showed no abnormalities. Pertinent physical features included bilaterally prominent neck veins at 45 degrees, symmetrical diaphragmatic excursion with diffuse diminutibn of breath sounds and no localizing physical sounds. Heart tones were distant without a palpable point of maximal impulse. Minima1 clubbing was evident in the absence of other joint deformities. Ankles and feet showed bilateral pitting edema. No petechiae or purpurae were noted. Ecchymoses at venipuncture sites were evident.
Hemogram showed a hemoglobin level of Il.5 g/100. a hematocrit value of 35 per cent, a leukocyte count of i’,6tWmm3 with 66 per cent granulocytes, 20 per cent lymphocytes, 10 per cent monocytes and 2 per cent eodnophils, and a platelet count of 353,@Wmms. Chest roentgenogram showed a mass in the upper lobe of the right lung which, upon tomography, was suggestive of a pri-
962 June 1980 The American Journal of Medicine Volume 68
FACTOR VII INHIBITOR-CAMPBELL ET AL.
mary neoplasm. Bronchoscopy did not reveal any discrete lesion. Sputum cytology demonstrated a clump of cells with nondiagnostic dysplastic features. Bone and brain scans dis- closed no abnormalities. A liver scan revealed features con- sistent with possible metastatic disease. In view of the pro- longed prothrombin times, further surgical studies were not made. Presently, the patient has frank hepatic and brain me- tastases.
Protein electrophoresis was unremarkable with the excep- tion of a diffuse increase in alpha globulin of 2.1 g/dl; anti- nuclear antibody [ANA] was positive at 1:320 with a nucleolar pattern; two lupus erythematosus preparations were positive and a rheumatoid arthritis test gave negative results.
Partial thromboplastin time was 28 seconds (control 32 seconds): prothrombin time 20 seconds (control 12.2 seconds);
bleeding time 7.5 minutes. Repeat prothrombin time, per- formed 1 hour after 2 U of fresh frozen plasma were injected, was 20 seconds; prothrombin time, using 50 per cent normal plasma and 50 per cent patent plasma, was 17 seconds; factor VII level was 30 per cent and Stypven time was not deter- mined.
METHODS
The nature of the immunoglobulin in the factor VII inhibitory activity was investigated by incubating the patient’s plasma with antibodies to human immunoglobulin G [IgG], immu- noglobulin A (IgA) and immunoglobulin M (IgM) (Miles Laboratories, Elkhart, Indiana] at a final concentration of 200 pg/ml for 60 minutes at 37’C. Following incubation, plasma samples were divided into two aliquots, one of which was as- sayed immediately for factor VII inhibitory activity. The re- maining aliquot from each sample incubated further at 4OC overnight, centrifuged at 4,500 G for 20 minutes at 4OC and the supernatants were then tested for factor VII inhibitory activity [3]. Inhibitory activity was measured by mixing equal volumes of patient plasma and normal plasma, then determining a one-stage prothrombin time [4]. The assay was performed both immediately after the addition of patient plasma to control plasma (0 time) and following 5 minutes incubation at 37OC. Five minute incubation was selected on the basis of a time- course inhibition study which indicated a plateau of inhibition effect at 5 minutes. In a separate procedure, to determine the general effect of large molecule protein upon determinations, albumin (Sigma bovine) was substituted for globulin. All studies were performed in triplicate and the results were then averaged.
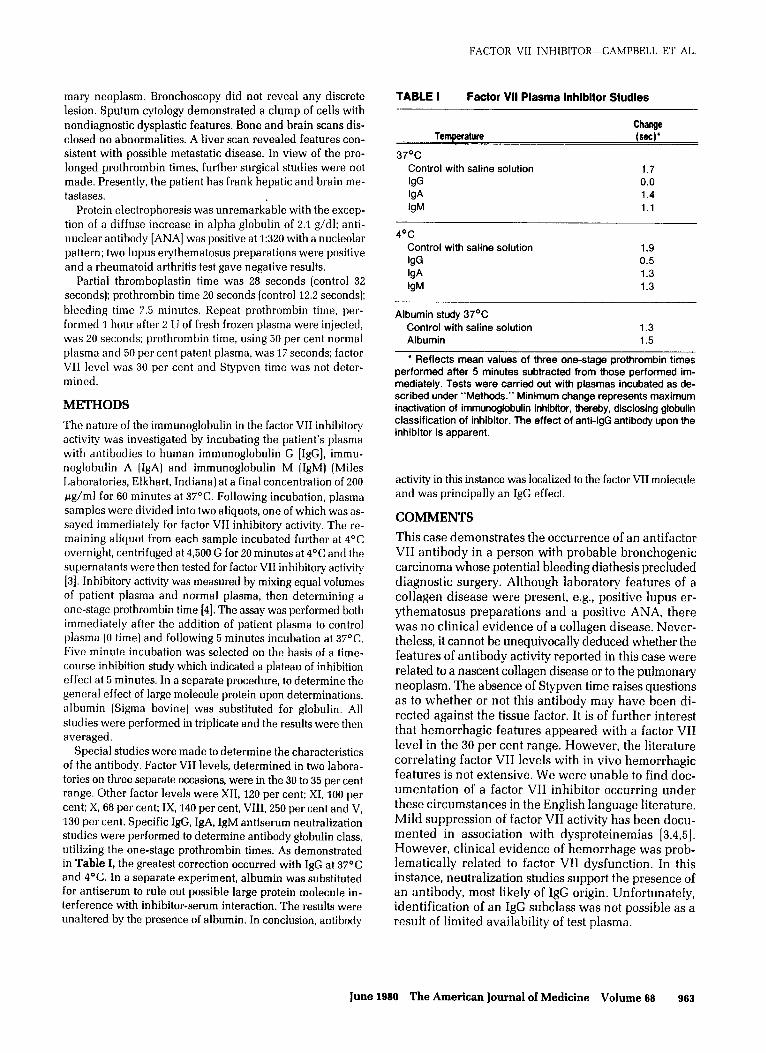
Special studies were made to determine the characteristics of the antibody. Factor VII levels, determined in two labora- tories on three separate occasions, were in the 30 to 35 per cent range. Other factor levels were XII, 120 per cent: XI, 100 per cent; X, 68 per cent; IX, 140 per cent, VIII, 250 per cent and V. 130 per cent. Specific IgG. IgA, IgM antiserum neutralization studies were performed to determine antibody globulin class, utilizing the one-stage prothrombin times. As demonstrated in Table I, the greatest correction occurred with IgG at 37OC and 4’C. In a separate experiment, albumin was substituted for antiserum to rule out possible large protein molecule in- terference with inhibitor-serum interaction. The results were
unaltered by the presence of albumin. In conclusion, antibody
TABLE I Factor VII Plasma lnhlbltor Studies
Temperature
37OC
Control with saline solution
lgG lgA IgM
Change (set)’
1.7 0.0 1.4 1.1
4V Control with saline solution
lgG lgA lgM
1.9 0.5 1.3 1.3
Albumin study 37% Control with saline solution 1.3 Albumin 1.5
l Reflects mean values of three one-stage prothrombin times performed after 5 minutes subtracted from those performed im- mediately. Tests were carried out with plasmas incubated as de- scribed under “Methods.” Minimum change represents maximum inactivation of immunoglobulin inhibitor, thereby, disclosing globulin classification of inhibitor. The effect of anti-IgG antibody upon the inhibitor is apparent.
activity in this instance was localized to the factor VII molecule and was principally an IgG effect.
COMMENTS
This case demonstrates the occurrence of an antifactor VII antibody in a person with probable bronchogenic
carcinoma whose potential bleeding diathesis precluded diagnostic surgery. Although laboratory features of a collagen disease were present, e.g., positive lupus er- ythematosus preparations and a positive ANA, there was no clinical evidence of a collagen disease. Never- theless, it cannot be unequivocally deduced whether the features of antibody activity reported in this case were related to a nascent collagen disease or to the pulmonary neoplasm. The absence of Stypven time raises questions as to whether or not this antibody may have been di- rected against the tissue factor. It is of further interest that hemorrhagic features appeared with a factor VII level in the 30 per cent range. However, the literature correlating factor VII levels with in vivo hemorrhagic features is not extensive. We were unable to find doc- umentation of a factor VII inhibitor occurring under these circumstances in the English language literature. Mild suppression of factor VII activity has been docu- mented in association with dysproteinemias [3,4,5]. However, clinical evidence of hemorrhage was prob- lematically related to factor VII dysfunction. In this instance, neutralization studies support the presence of an antibody, most likely of IgG origin. Unfortunately, identification of an IgG subclass was not possible as a result of limited availability of test plasma.
June 1980 The American Journal of Medicine Volume 88 963

FACTOR VII INHIBITOR-CAMPBELL ET AL.
REFERENCES
1. Feinstein DI, Rapaport SI: Acquired inhibitors of blood coagulation. Prog Hemost Thromb 1972; 1: 75-95.
2. Shapiro SS, Hultin M: Acquired inhibitors to the blood coag- ulation factors. Semin Thromb Hemostas 1975; 1: 336- 365.
3. Penner J: Blood coa !Y
lation laboratory manual. Ann Arbor: University of Mic tgan, 1976; 17: 36.
4. Ibid.
5. Nilehn JE, Nilsson IM: Coagulation studies in different zrlQ;f myeioma. Acta Med Stand 1966; 445 [suppl]:
6. Bjerrum dJ, Weeke B: Two M components(a GK and a ML] in different ceils of the same patient. Stand J Haemtoll966; 5: 215-234.
7. Perkins HA, MacKenzie MR. Fundenberg HH: Hemostatic defects in dysproteinemias. Blood 1977: 35: 690-706.
884 June 1880 The American Journal of MedIche Volume 88