final report - 6 august 2008 - who.int hpsr iprq_makere... · 2.3.1 literature search and review...
TRANSCRIPT
Final Report – 6 August 2008
Priority Research Questions Study Makerere Institute of Social Research 1
IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING; HUMAN RESOURCES FOR HEALTH
AND THE ROLE OF NON-STATE SECTOR
Prepared by
Delius Asiimwe
Senior Research Fellow, MISR
Supported by
Alliance for Health Policy and Systems Research
Reproduced with permission

Final Report – 6 August 2008
Priority Research Questions Study Makerere Institute of Social Research 2

Final Report – 6 August 2008
Priority Research Questions Study Makerere Institute of Social Research 3
TABLE OF CONTENTS
ACKNOWLEDGEMENTS ....................................................................................................................................... 5
EXECUTIVE SUMMARY ........................................................................................................................................ 6
Background ....................................................................................................................................................... 6
Study Description and Methods ..................................................................................................................... 6
Findings ............................................................................................................................................................. 7
Policy Concerns – Health Financing .......................................................................................................... 7
Policy concerns – Human Resource for Health........................................................................................ 7
Policy Concerns – Non-state Sector .......................................................................................................... 7
Priority Research Questions ....................................................................................................................... 7
ABBREVIATIONS .................................................................................................................................................. 9
1.0 STUDY CONTEXT ................................................................................................................................... 11
1.1 Objectives of the Study ................................................................................................................... 12
2.0 METHODOLOGY ..................................................................................................................................... 12
2.1 Scope.................................................................................................................................................. 12
2.2 Selection of organizations and respondents................................................................................. 12
2.3 Methods of Data Collection ............................................................................................................. 12
2.3.1 Literature Search and Review .................................................................................................... 12
2.3.2 Pre-visits ........................................................................................................................................ 13
2.3.3 In-depth interviews with Key Informants................................................................................. 13
2.4 Data Analysis..................................................................................................................................... 14
3.0 LITERATURE REVIEW ........................................................................................................................... 14
3.1 Introduction....................................................................................................................................... 14
3.1.1 Health Care Financing ................................................................................................................. 15
3.1.2 Human Resource for Health ....................................................................................................... 16
3.1.3 Non-State Sector .......................................................................................................................... 17
4.0 FINDINGS FROM KEY INFORMANT INTERVIEWS ............................................................................ 19
4.1 Policy Concerns - Health financing ................................................................................................ 19

Final Report – 6 August 2008
Priority Research Questions Study Makerere Institute of Social Research 4
4.1.1 Budgeting and Resource allocation for the health sector ..................................................... 19
4.1.2 Public financing of the private sector........................................................................................ 19
4.1.3 Alternative source of financing................................................................................................... 20
4.2 Research Priority Questions - Health Financing........................................................................... 22
4.3 Policy Concerns – Human Resource for Health............................................................................ 23
4.3.1 Numbers, deployment and attrition .......................................................................................... 23
4.3.2 Record Keeping and Data Management ................................................................................... 23
4.3.3 Human Resource for Health Training........................................................................................ 24
4.3.4 Management of Human Resource for Health........................................................................... 24
4.4 Research Priorities Areas – Human Resource for Health ........................................................... 25
4.5 Policy Concerns – Non-State Sector .............................................................................................. 26
4.6 Research Priorities Areas – Non-State Sector .............................................................................. 26
5.0 DISCUSSION ........................................................................................................................................... 27
5.1 Uganda’s Health Policy Environment ............................................................................................. 27
5.2 Health Financing ............................................................................................................................... 27
5.3 Human Resource for Health............................................................................................................ 28
5.4 Non-State Sector .............................................................................................................................. 28
5.5 Strength of the study Methodology ............................................................................................... 29
5.6 Short Comings of the Study Methodology .................................................................................... 29
6.0 REFERENCES .......................................................................................................................................... 30
Annexes:........................................................................................................................................................... 31
1: List of Key Informants .............................................................................................................................. 31
2: Key Informant Tools ................................................................................................................................. 31

Priority Research Questions Study Makerere Institute of Social Research
5
5
ACKNOWLEDGEMENTS This report was prepared by Makerere Institute of social Research, Makerere University as part of the collaborative study with Faculty of Arts and Social Sciences, University of Dar es Salaam Tanzania.
The author would like to thank Alliance for Health Policy and Systems Research, WHO, Geneva for supporting this study. He also wishes to extend his gratitude to Sara Bennett, Manager and Michael Kent Ranson, Consultant both of Alliance HPSR for their input that shaped the outcome of this study.
I am also grateful for the thoughtful guidance of the Dr. Francis Runumi, Commissioner Health Service Planning and Dr. Basaaza, Senior Planner, Ministry of Health, Kampala during the preparatory stages of the study.
On behalf of Makerere Institute of Social Research, I would especially like to thank the informants that participated in the study – policy makers and program staff from the various government ministries, leaders of NGOs providing health care and providers’ associations as well as private providers who freely gave in their time to answer questions and provided reflections on policy concerns and priority research questions. Special tribute goes to the leadership of the health consumer and users organization in championing the communities’ voices in health care and hope that these findings will contribute to improving the health and quality care of the people of Uganda and the region.

Priority Research Questions Study Makerere Institute of Social Research
6
6
EXECUTIVE SUMMARY
Background Uganda is among the twenty poorest countries in the world with a per capita GDP of about $300 with about 31 percent of Ugandans still living below the poverty line as of 2006. Its economy is predominantly agricultural where the majority of the population is dependant on subsistence farming and light agro-based industries.
The government’s significant investment in the social sector since the 1980s has increased the health sector funding to 13% of the total national budget (7.6% of the GDP as of 2004) from 7% in 1995. Consistent with the decentralized system of governance much of health care functions and responsibilities were devolved to a three tier local governments- the district; municipality and Sub-county/Town council. The central government retained the mandates of making national policies, setting standards and supervision. In order to improve access to basic services, the delivery of health care is through a layered system of health units, ranging from national referral hospitals, regional referral hospitals, district hospitals, health sub-districts to lower level health centre IIIs and IIs at sub-county and parish levels.
Despite these achievements, the Health sector still has glaring gaps in quality and reliability of services. Infant mortality stands at 75/1000, maternal mortality ratio is 435/100,000, 38 percent of children less than five years are stunted and only 44 percent of eligible children complete the full immunization cycle. There is shortage of manpower, physical infrastructure and inadequate financing among others to cater for the soaring patient numbers and changing needs in health care in Uganda.
Study Description and Methods This study is intended to identify priority research questions in Health Financing, Human Resource for Health and Non-State Sector in the Low and Middle income countries in the Eastern Africa Region. Following socio-economic reforms of the countries in the region beginning the late 1980s, much has been done to support their health sectors. However, the planning, financing and delivery of health care in most countries remain poor. The main purpose of the study therefore, is to ensure that in the next 5-10 years, generation of information for policy and decision making in three thematic areas is mainly guided by policy concerns of key stakeholders in health care.
The objectives are: (i) identifying and ranking policy concerns at national and regional levels as perceived by policy makers and Civil Society in the three thematic areas and; (ii) Identifying and ranking the emerging national and regional research priority questions in the three thematic areas in Uganda and Tanzania.
The study was carried out in the public and private sector covering key ministries, Non-Governmental Organisations (NGOs), private health facilities, Bi/multi-lateral organizations, public and private provider associations as well as research and consumers’ organizations. A total of 35 strategically placed policy makers, managers and staff from selected organizations/ agencies/ministries/associations were interviewed.
Data from key informants was collected using qualitative methods of In-depth interview. A set of tools with each tailored to the roles and responsibilities of the selected informants were used as guides during the interview.
Secondly, a comprehensive literature search of official documents and grey literature in libraries; information centers and on the internet was carried out. The search yielded hard and soft copies of national health policies, strategic plans, partnership policies survey reports and program documents among others. The key and related literature has been reviewed for purposes of writing this report. All the literature that has been identified and collected has been capture in a database to be further developed and packaged by Alliance for Health Policy and Systems Research for wider dissemination.

Priority Research Questions Study Makerere Institute of Social Research
7
7
Findings
Policy Concerns – Health Financing
The National Health Policy priorities in Uganda focus at ensuring access to the Minimum Health Care Package. However available data shows that delivery of the Minimum Health Care Package shows a big resource gap between the requirements of HSSP II and resources available under the current Medium Term Expenditure Framework (MTEF).1
The informants major concern was that the costing of HSSP II like that of HSSP I remain largely facility based and applies to only government and Faith Based-NGO facilities excluding private for profit providers, employers’ clinics and the complementary and traditional medicine sub-sector. These together underpin the lack of systematic mechanisms needed to ensure adequate financing of the national health care delivery in Uganda.
Policy concerns – Human Resource for Health
The major human resource problems in Uganda’s health sector were reported as mal-allocation of human resources; shortage of trained staff in the health sector and; attrition of qualified staff from private not-for-profit to public facilities and private for-profit practice. In addition, poor remuneration of health workers and over dependence on untrained personnel in the primary health care facilities, pose major challenges to effective implementation of health programmes in Uganda.
The absence of adequate information as an input to Human Resource for Health development and management raise a key policy concern among policy makers. The current information on of HRH is disjointed, difficult to access and not standardized to provide basis for determining the required numbers, categories, quality of training and the impact of dual employment as well as attrition of health workers particularly from the PNFPs to the public health sector and other organisations.
Policy Concerns – Non-state Sector
The Non-State Sector role in health services delivery was widely acknowledged by most informants. However much of its contribution to the national health care delivery in not well known except for the facility based PNFPs whose contribution is about 40% of the national health care delivery. In support to PNFPs, government willingness to spend and the condition that user fees be kept minimal overrides the basis of what is required to delivery the PNFP services. The inelastic funding from the public sector tend to force PNFPs to increase user fees rendering their services in accessible to the very poor that are unable to pay higher fees.
On the other hand, though the PFP and Traditional medicine sub-sectors are recognized as partners in the health care delivery, they are never provided for in the national health sector strategic planning creating a gap in planning for services already being expended in the national health system.
Priority Research Questions
Health Financing
The holistic costing to ascertain a unit cost and the health burden of a country in relation to per capita GDP of Ugandans was ranked the first priority research question.
1 MTEF is the overall mechanism by which resources are expected from government including donor budget support allocated to and within sectors. It sets sector and local government spending ceilings within a three year rolling framework and also links planning and development in budgeting based on the amount of resources available.
Priority Research Questions Study Makerere Institute of Social Research
8
8
The second was to generated evidence on resources use, application and the cost-effectiveness of financing the burden of disease in a resource constrained environment.
The third priority research question in health financing was the cost benefit analysis of the National Social Health Insurance Scheme with regard to information on equity, management and financial analysis for decision making.
Human Resource for Health
The first priority research question was to assess the human resource for health in national health care system to help develop a harmonized management system and a consolidated human resource development plan. The second is the review of the training curricula in light of the new diseases, changing clients’ health care seeking patterns, new policies and the occupational issues of health workers. The third was the assessment of human resources development and deployment synergies between the public and private sectors. The data generated would address the challenges of building synergies for effective utilization of human resource between public and private sectors.
Non-State Sector
The first priority research question is the development of Health Management Information System (HMIS) to capture information from the private sector (PNFP, PFP and Traditional and Complimentary Medicine) to be reflected in the national official documents for planning and policy making purposes. The second was to assess the weak/absence of relationships/synergies in the health sector to help provide strategies to information the partnership among the different sub-sectors in health care delivery. The third was the mapping private sector with regard to categories, range and pricing of services, kind of patients handled by the private health providers, costs and treatment procedure as well as information made available to patients. The fourth was a national survey of consumers’ views and value for money audit of health providers to assess the clients’ satisfaction with health service delivery.
Conclusion
The health financing, human resources for health and Non-State Sector hurdles seem to stem from the governance and financing regimes. The governance and policy environment for Uganda’s health sector that is made up of various actors (public, private and donors) requires harmonization of basic rules, standards as well as information and management systems. The financing regimes need a system to plan and utilize resources effectively in order to realize cost effective interventions. Priority setting should be based on information on the overall health sector to help assess cost effectiveness use of human and financial resources.

Priority Research Questions Study Makerere Institute of Social Research
9
9
ABBREVIATIONS
ACT Artemesinin-based Combination Therapy
AIDS Acquired Immune Deficiency Syndrome
ARV Antiretroviral
CEO Chief Executive Officer
ENHR Essential National Health Research
FB-PNFP Faith Based Private Not For Profit
FY Financial Year
GAVI Global Alliance for Vaccine Immunization
GDP Growth Domestic Product
HIV Human Immunodeficiency Virus
HMIS Health Information Management Systems
HRH Human Resource for Health
HRHP Human Resource for Health Policy
HSSP I Health Sector Strategic Plan (2000/01-2004/05
HSSP II Health Sector Strategic Plan (2005/06 -2009/2010
HW Health Worker
MDGs Millennium Development Goals
MISR Makerere Institute of Social Research
MoES Ministry of Education and Sports
MoFPED Ministry of Finance Planning and Economic Development
MoH Ministry of Health
MTEF Mid-Term Expenditure Framework
NFB-PNFP Non-Faith Based Private Not For Profit
NGO Non-Governmental Organisation
OPD Out Patients Department
PEAP Poverty Eradication Action Plan
PFP Private For Profit
PHC Primary Health Care

Priority Research Questions Study Makerere Institute of Social Research
10
10
PPPH Public Private Partnership for Health
SAPs Structural Adjustment Programmes
STI Sexual Transmitted diseases
SWAP Sector Wide Approach
TCM Traditional and Complementary Medicine
UAHPC Uganda Allied Health Professionals Council
UBOS Uganda Bureau of Statistics
UDHS Uganda Demographic Health Survey
UMDPC Uganda Medical and Dental Practitioners Council
UNEB Uganda National Examination Board
UNHS Uganda National Household Survey
UNHRO Uganda National Health Research Organisation
UNMC Uganda Nurses and Midwives Council
UNMHCP Uganda National Minimum Health Care Package
UPC Uganda Pharmacists Council
UPE Universal Primary Education
US$ United States Dollars
USE Universal Secondary Education
WHO World Health Organisation
Priority Research Questions Study Makerere Institute of Social Research
11
11
1.0 STUDY CONTEXT Uganda is a Sub-Saharan country with a population of 24.7 million people. Close to 90 percent of these live in rural areas, and engage in peasant subsistence agriculture (UBOS, 2002). The country remains among the twenty poorest countries with a per capita GDP of about $300 (UNHS, 2006). As a strategy to confront poverty, the government launched a series of poverty eradication Programmes being implemented through the Poverty Eradication Action Plan (PEAP) first drafted in 1997 to provide an overarching framework to guide public action to eradicate poverty. As a result there has been a reduction in the proportion of Ugandans living in absolute poverty from 56 percent in 1992 to 35 percent in 2000 and currently estimated at 31 percent (PEAP 2004/5-2007/8).
The government has since late 1980s continued to invest significantly in the improvement of social and economic infrastructure, such as road and communication networks, education, and health services with the goal of improving access to basic services, especially for the poor. Health sector funding has also increased to 13 percent of the total national budget, up from 7 percent in 1995 (MoFPED, 2005) or 7.6 percent of the GDP (2004) (WHO, 2007)2
In order to enhance access, health services have been decentralized to communities through a layered system of health units, ranging from national referral hospitals, regional referral hospitals, district hospitals, health sub-districts to lower level health centre IIIs and IIs at sub-county and parish levels respectively. This arrangement is consistent with the devolving of functions and responsibilities including health to decentralized three tier local governments - the district; municipality and Sub-county/Town council. The central government retained the mandate of making national policies, setting standards and supervision of the services (The Local Government Act, 1997).
Despite the achievements, the country continues to host a big mass of people engulfed by poverty and disease. The Infant mortality stands at 75/1000, maternal mortality ratio is 435/100,000, 38 percent of children less than five years are stunted and only 44 percent of eligible children complete the full immunization cycle. HIV prevalence is at 7 percent with high percentage recorded among women in the reproductive age (15-49 years) (UDHS 2006).
In response the government developed several policies, strategies and programmes to help improve health status and life of its people. In particular, the National Health Strategic Plan 2005/06 -2009/10 (HSSP II) as a consolidation and extension of the Health Sector Strategic Plan I (HSSP I) (2000/01-2004/05 has an overriding priority of contributing to the Poverty Eradication Action Plan (PEAP) and the Millennium Development Goals (MDGs). The plan emphasizes the role of communities and households targeting the poor, orphans, children, women, the elderly, refugees and internally displaced persons among others so as to foster a sense of individual ownership of health services.
However, a number of challenges continue to override the overall objective of the National Health Policy of reducing mortality, morbidity and fertility, and the disparities therein. Key among them are the health financing costs required to achieve the policy objectives agreed upon by government of Uganda and its development partners. The human resource for health that pose a number of problems such as mal-allocation; shortage and attrition of qualified staff within and outside various health care delivery points. The fragile relationships between the public and private sector3 that undermining one of the National Health Policy objective of making the private sector a major partner for successful scaling up and improvement of health care delivery.
2 Figures are for 2005 from World Health Organisation Statistics, 2007. 3 The Private Sector in health includes: Private Not for Profit Health Providers (PNFP), Private Health Practitioners and, Traditional and Complementary Medicine Practitioners (TCMP). The PNFP includes Facility Based (FB-PNFP) and are mainly faith-based for example Uganda Catholic Medical Bureau and; Non-facility based (NFB-PNFP) such as NGOs both local and international.
Priority Research Questions Study Makerere Institute of Social Research
12
12
1.1 Objectives of the Study The main purpose of the study is to ensure that in the next 5-10 years, research agendas in the Low and Middle income countries are driven by policy concerns of the time other than the researchers’ interests and funding sources. The strategy is to identifying research priority questions in the areas of Health Financing; Human Resources for Health and the Role of the Non-State Sector arising out of policy concerns/challenges among policy makers and other key stakeholders as well as from the processed and Grey literature in Uganda, and Tanzania.
The objectives are:
i) Identifying and ranking policy concerns at national and regional levels as perceived by policy makers and Civil Society in the three thematic areas and;
ii) Identifying and ranking the emerging national and regional research priority questions in the three thematic areas in Uganda and Tanzania.
2.0 METHODOLOGY
2.1 Scope This study is an attempt to provide an insight into the existing and/or desired relationship between policy development and information generated through research in the health sector. The task is viewed as systematically examining the policy making cycle to help capture the policy concerns and issues that give birth to priority research questions for national policy agenda setting. These may be influenced by Global issues and local concerns such as the Millennium Development Goals (MDGs); combating HIV/AIDS; Human resources and professionalism for health; poverty and ill-health; immunization; health financing options and public/private health care mix and delivery.
In each country the study covered government ministries, Non-Governmental Organisations (NGOs), Bi/multi-lateral organizations, research organizations, private health facilities and consumer organizations.
2.2 Selection of organizations and respondents The selection of the organizations/agencies/ministries was guided by their roles in the national health system and health care delivery. The number of respondents from each organization/agency/ministry was based on its role, coverage of health programmes and activities in health care delivery system. Consequently the Ministry of Health had the highest number of respondents due to its central role in health care policy and management in the country but also because of the departmentalized nature of the activities and programmes in the three thematic areas of the study. A total of 35 strategically placed policy makers, managers and staff in the selected organizations/agencies/associations in Uganda were visited to conduct key informant interviews (see Annex: 1).
2.3 Methods of Data Collection
2.3.1 Literature Search and Review
A search strategy for literature to review and develop a data base was three pronged. First was a search on the internet that enabled the team access to the readily available public and other documents based on potential sources of critical information. The internet search also helped to inform the design of search strategy plan and provided benchmark for literature review.
Secondly, literature search was conducted in key libraries and resource centres of organizations, ministries, universities and research institutions. The target was to collect hard and soft copies of programme documents as well as survey and evaluation reports on the subject matter.

Priority Research Questions Study Makerere Institute of Social Research
13
13
Thirdly, in consideration of the practice of poor record keeping prevalent in most middle and low income countries, personal contact with key stakeholders in organizations/agencies/ministries was used to access literature (official or grey) before and during the course of the interviews with the key informants. This part of literature search mainly yielded hard copies of official documents, survey reports and publications.
The documents (hard and soft copies) and grey literature in the three thematic areas were reviewed in the light of the study objectives. All the details of documents and literature identified were captured by region, author, year, type of document (e.g Policy, Strategic Plan etc); thematic area of the study and country onto which the information mainly focused for the purposes of creating a completed and edited data base, whose soft copies will be available for wider dissemination.
2.3.2 Pre-visits
In June, 2007 two pre-visits were made to the Ministry of Health, Kampala. The purpose was to seek guidance and equip the team with information on policies and priority setting in Uganda’s health care system. In the first visit, the team discussed with the Commissioner, Health Services - Planning while in the second one the discussion was held with Senior Planner/Health Economist in charge financing together with a few Health Economists of the health financing section of the ministry. The pre-visits generated valuable information on the potential areas of investigation and key informants in the three thematic areas of the study. The information was also used in the planning of the data collection exercise and the revision of the zero draft study tools.
2.3.3 In-depth interviews with Key Informants
In-depth interviews were conducted with national level public policy makers and heads of selected sections in three Ministries of Health, Finance, Planning and Economic Development and Local Government. The heads of Special Health Programs such as HV/AIDS, Immunization and Clinical Services in the Ministry of Health were also interviewed. In the private sector interviews were held with heads of Private Health Facilities (Pharmacies, Hospitals and Clinics), heads of NGOs involved in delivery and supporting of Health care as well as members of various health workers’ Associations. Others were program heads of Bilateral and Multi-lateral Organizations, head(s) of public and private Research Organizations/Agencies that engage in health related research and health user and consumer organization.
The tools for various categories of key informants were designed to elicit information on policy processes, current and future policy concerns and the research questions that could address the raised concerns. Others focused on the research agendas, programme activities and support in relation to health policy concerns in the three thematic areas of the study (see Annex: 2).
Interviews with policy makers helped to provide insight into the policy environment within which health services are delivered. The existing and perceived policy concerns, challenges to implementation and partnerships as well as research questions to inform policy were also raised.
Interviews with Heads of selected sections and Heads of Special Health Programs yielded data on experiences of delivering health services with a key focus on both their program and policy in the study thematic areas. In addition, the impact of current policies on quality and quantity of services and challenges and recommendations of managing services were also explored.
Similarly, interviews with Heads of Private Health Facilities and Faith-Based health NGOs as well as health workers associations generated data on realities of delivering health services within in the national health system. The working experiences, financing mechanisms, partnerships with public sector and impact of current health policies in the delivery of health care were explored and a number of research priority questions identified.
The interviews with Bilateral and Multi-lateral organizations focused on their key activities and concerns regarding national health policy and system. In the research organizations the relationships
Priority Research Questions Study Makerere Institute of Social Research
14
14
between the organizations’ research agendas in relation to national health sector activities and priorities were explored. In both cases, the interviews were used to assess their perspectives and identify key research priority questions for future health policy making and programming.
2.4 Data Analysis Content Analysis was used to analyze the generated qualitative data on the basis of emerging themes and sub-themes in line with the study objectives. Descriptive summaries and use of quotes was utilized. This analysis was useful in identifying the major issues for each of the thematic areas with regard to policy concerns and priority research questions. It also facilitated comparisons and contrasts of views of informants from different organizations.
The data collected through document reviews was used to assess historical, current and emerging policy concerns in the three thematic areas. The same set of data was used to draw up generalization on the regional level on the emerging health policy concerns and priority research questions in the three thematic areas. The soft copies from the internet, libraries and offices have been systematically captured and listed while a detailed list of hard copies has been developed for the purposes of creating a data base of the generated literature.
Finally, the analysis of the data enabled triangulation of data from key informant interview and literature review on two specific issues of emerging policy concerns and priority research questions pertaining in the country.
3.0 LITERATURE REVIEW
3.1 Introduction The Uganda’s National Health Policy, 1999 (for a period 1999-2009) focuses on health services that are demonstrably cost-effective and have the largest impact on reducing mortality and morbidity. Consequently the major contributors to the burden of disease at all levels that include malaria, STI/HIV/AIDS tuberculosis, diarrheal diseases, acute lower tract infections and maternal conditions attributable to high fertility and poorly spaced births, vaccine preventable childhood illnesses, malnutrition, injuries, and physical and mental disability were not given highest priority. The overall objective of the National Health Policy, 1999, was to reduce mortality, morbidity and fertility, and the disparities therein with efforts focused at ensuring access to the minimum health care package4. The policy further provides objectives and guidelines specific to health care financing, human resource for health, and private health sector in general. The exception in the National Health Policy was stating the objective of Complementary and Traditional Medicine Practitioners but not providing specific guidelines.
The actions lined up to achieve the overall objective of the National Health Policy with regard to the three thematic areas are clearly stipulated in the health policy as:
• Provision of additional resources for Primary Health Care (PHC) in the form of conditional and equalization grants or similar mechanisms with increased funding specifically on immunization as a component of public health (HSSP 2000/01 – 2004/05.
• Clarifying the relationship between the key stakeholders, notably health related line ministries, the Health Service Commission, the Local Governments, Donors, Private Practitioners, NGOs, and Traditional Practitioners within the decentralized system.
4 The minimum health care package comprises interventions that address the major cause of burden of disease. This is taken to be a cardinal reference in determining allocation of public funds and other essential inputs in the health sector. The minimum health care package involves control of communicable diseases (malaria), STI/HIV/AIDS, and Tuberculosis); integrated management of childhood illness; Sexual and reproductive health and rights; and other public health interventions.

Priority Research Questions Study Makerere Institute of Social Research
15
15
• Implementing the organization and management reform of the Ministry of Health in line with its new roles and responsibilities.
In 1990, when the country embraced the concept of Essential National Health Research (ENHR), efforts were made to set a health research agenda in Uganda. To achieve this objective, policy makers, researchers and civil society were to be called upon to participate at various stages in the evolution and development of research. The activities that included wider consultations and workshop to draw-up a health research plan were carried out in second half of 1990s.
Available literature shows a Health Research and Development brochures (1999) listing research priority areas for the period 1997-20015 and updated for the period 2005-20106. The research priorities were reportedly identified in consultation with district health officers at their regional meeting, a few representatives of research institutions and senior officers of the Ministry of Health. In this case the district officials verbally gave their research priorities mainly based on their experience. Moreover, the proposed research priorities (2005-210) are over 75 sub-topics under 9 topics such as maternal child health and nutrition; HIV/AIDS; Malaria; Drug use studies and; non-communicable diseases rather than priority research questions.
Among the steps taken to support the implementation of health research was the formation of an indigenous organization called Uganda National Health Research Organisation (UNHRO)7 intended to develop, coordinate, promote and strengthen health research which is essential for the health and development of the people of Uganda. However, UNHRO is not yet not legally established, is limited in consultations, does not have data base due to lack of funding and have no information on the kinds and nature of much of health research that has been done in the country.
3.1.1 Health Care Financing
Uganda like Kenya and Tanzania has had a tradition of using government treasury resources to finance health care. For example, Uganda and Tanzania health care financing was mainly run by the government funds to ensure that citizens accessed all health care services free of charge. The non-profit sector participation in health services delivery was with a heavy level of government subsidy to ensure affordability (Ashington Ngigi and Daniel Macharia, May 2006). Though, health care financing is increasingly being done by both the government and the private sector, the government through the Ministries in charge of health is still the major financier and provider of health care services in the three countries.
The three countries have also had a gamble on alternative financing options. In Uganda for example the fee for service (sometimes referred to as cost-sharing) has been introduced, abolished or re-introduced (formally and informally) and health insurance is planned. The common factor being the governments’ inability to provide unlimited free care because of budgetary allocations that are insufficient to meet rising health costs (Asiimwe D., Mwesigye F., McPake B., and Streefland P., 1997; HSSP II, 2005/06-2009/2010).
Uganda’s Health Sector Strategic Plan (HSSP I) 2000/01 – 2004/05 provides indicative cost analysis for the HSSP I of a total cost of US$ 954 million for the five year period of the plan. The annual total costs are US$ 159 million in year one; US$ 179 million in year two; US$207 million in year three; US$ 209 million in year four; and US$ 201 million in year five. A number of challenges remained, key among these being under funding with current level of public funding of about US$8 per capita falling
5 Uganda National Health Research organization (UNHRO), 1997-2001, (Brochure 1999), UNHRO, Entebbe 6 A brochure of Uganda National Health Research organization (UNHRO) Research Priorities 2005-210, UNHRO, Entebbe 7 UNHRO is health research organization owned by government with Research institutions of government not directly supervised by UNHRO and Private practitioners/ private researchers as affiliates (see also UNHRO, Bill 2006)

Priority Research Questions Study Makerere Institute of Social Research
16
16
far below the estimated requirements (US$ 28 per capita). In effect only 30% of HSSP I was funded excluding the activities and financing of private for profit providers, employers’ clinics and the traditional sector. The percentage of the government of Uganda budget that is allocated to the health sector declined from 10.8% in FY 2004/05 to 8.9% in 2005/06 against the target of 11.1%. The percentage of the government expenditure on health as a percentage of total government expenditure also declined from 9.75% in FY 2004/05 to 8.3% in FY 2005/06 (MoH, October 2006).
In development of HSSP II, when the inputs for the delivery of the Minimum Health Package were identified, quantified and costed, there was a big resource gap between the requirements of HSSP II and the resource available in the current MTEF. The medium term costing scenario that scales down the inputs to be more inline with the MTEF was therefore proposed. In the light of this, emphasis of HSSP II is to concentrate effort and resources on a limited set of evidence–based, cost-effective intervention under each of the elements of the Uganda National Minimum Health Care Package (UNMHCP) (HSSP 2005/06 – 2009/10).
Like in HSSP I, costing methodology8 of HSSP II remains largely facility based except for the estimated costs at central level. Furthermore the costing applies to only government and Faith Based-NGO facilities and like HSSP I, HSSPII does not cover the private profit providers, employers’ clinics and the complementary and traditional medicine sector. As pointed out in the Draft Policy on Public Private Partnership, 2006, limited national awareness of the potential contribution of the private sector to national health care delivery and apparent absence of a national policy on partnership and financing in Uganda are major impediments to inadequate support to the Complementary and Traditional Medicine and Private Health providers.
Upon a review of the existing documents one can deduce critical issues around financing health services in the country. These include:
• The public/ Private Mix in health care financing • Costing delivery of health services • Alternative Health financing mechanisms including health insurance • Accessibility, equity and affordability of non-state sector health services especially the poor
and vulnerable groups • Sustainability in financing health care in public and private domains
3.1.2 Human Resource for Health
The National Health Policy (1999) and Draft National Policy on Public Private Partnership in Health, 2006, point out three major human resource problems in Uganda’s health sector. These are: (a) mal-allocation of human resources with 54% of the health workers concentrated in hospitals; (b) shortage of trained health workers in the health sector and; (c) attrition of qualified staff from private not- for- profit practitioners to public facilities and private practice. These together with poor remuneration of health workers pose major challenges to effective implementation of health programmes in Uganda.
In response, the Ministry of health attempted to address the major constraints of inadequate numbers and inappropriate distribution of trained health personnel. The HSSP I aimed to attain at least 75% of the minimum staffing norms at each level of the district health system. This was revised to 52% of all the approved posts to be filled by appropriate trained staff. The recruitment of health workers during HSSP I raised the proportion of approved posts filled with trained health workers from 33% to 68%. However, in HSSP II it is noted that though the numbers of qualified health workers improved, it is still constrained by unequal distribution and inappropriate skills-mix with nursing assistants constituting the bulk of the health workers at all levels of health care.
8 This costing methodology is detailed on pages 81 – 85 of the HSSP I and Page 76 of HSSP II
Priority Research Questions Study Makerere Institute of Social Research
17
17
In a related effort, the Human Resource for Health Policy (HRHP), 2006 was developed with the main rationale of providing a framework and guidance for effective and efficient implementation of the National Health Policy. The HRHP policy goal is to develop and maintain a health workforce that is appropriately sized, structured, skilled, well balanced, distributed, resourced, committed and performing efficiently and effectively in order to provide all Ugandans with equal access to a minimum health care package, sufficient to meet Uganda’s health development targets within affordable resources.
The objectives of the Human Resource for Health Policy are to ensure that:
• planning for human resource for health is rational and financing is adequate, education and training of HRH is relevant to the health needs and health personnel requirements of Uganda,
• management of HRH is improved at all levels;
• standards and rights of health professionals and clients are upheld;
• information and research on HRH are strengthened;
• partnership among public, private not for profit and private stakeholders in HRH is promoted;
• benefits of globalization are reaped and its ill-effects mitigated; the institutional framework for HRH functions is strengthened.
The strategy is to attain the right HRH numbers and skills mix to populate the health sector taking into account recurrent budget constraints. The plan target is that the total health workforce in the public and private sectors will increase by 66% from a current level of 59,000 to 98,000 for the period 2005-2020 compared with a population growth rate of 60% giving a slightly improved health worker to population ratio (MoH, June 2007).
The human resources needs, development and deployment raise a number of issues (MoH, June 2007; Uganda AIDS Commission, April 2007; MoH, April 2006; HSSPII 2005/06 – 2009/2010; The World Bank, 2003)
The philosophical tenets informing the Human resource policy making process
. Employment/labor laws, statutory environment and their relationships to effective health care services delivery . Rules and regulations concerning human resources in the health sector including
remuneration structures, motivation, retention and development . Health workers preferences between Urban and rural areas; and public and private health
sector . Capacity building standardization of skills training for effective health services delivery . Professional organizations and their role in ethical practice maintenance. . Commercialization vs professionalization in the growing private health sector . Human resources budgeting for health services provision . Market competitiveness for health related human resources and job security
3.1.3 Non-State Sector
For a long period since independence, the health services financing and provision in Uganda remained largely the province of the government with substantial government subsidies to the non-profit organizations in the three countries. It is in the post Structural Adjustment Programmes that these countries formally invited the non-state profit oriented and non-profit making organizations to

Priority Research Questions Study Makerere Institute of Social Research
18
18
participate in the financing and provision of health care services9. For example in Uganda non-state sector role in financing and provision of services were formally recognized as late as 1998. (Kiyonga C.W.B., (1997; MoH, 1998).
The National Health Policy (1999) recognizes existence of insufficient collaboration between the public and the ‘private sector’10 and Traditional Health providers. The major objective is to make the private sector a major partner in Uganda’s national health development by encouraging and supporting its participation in all aspects of the national health programmes.
The draft National Policy on Public Private Partnership in Health (PPPH), 2006, provides a general framework for effective partnership between the Ministry of Health and the Private Not-for Profit; Private Health Practitioners, Traditional and Complementary Medicine Practitioners as key actors that form the private health sector. The purpose for the framework is to institutionalize and guide the implementation of the partnership between government and the private health providers.
It also encourages registration of providers with their respective councils such as; the Uganda Medical and Dental Practitioners Council (UMDPC), the Uganda Nurses and Midwives Council (UNMC), the Uganda Pharmacists Council (UPC), and the Uganda Allied Health Professionals Council (UAHPC). The policy further provides policy makers and other stakeholders with guidelines of identifying and addressing partnership concerns when taking policy decisions.
A number of issues to be observed with regards to the role of the non-state sector arise out of the fact that it is now a major player in health services financing and delivery and these may include, inter alia:
. Size and coverage of the private sector in the health care system including referral
. Type of services rendered by the private health sector
. Regulatory framework, supervision and quality assurance for private health care provision
. Investment and consumer choices in terms of meeting standards of quality, safety, quantity, utilization and value for money with increased private sector participation
. Incentives or disincentive and state-based mechanisms to ensure increased role of the non-
state sector with an assurance of equity of social and geographical dimension of access or distribution of services
. Training of professionals such as physicians, nurses and technicians for the private sector
. Intra and extra mural participation by publicly employed professionals (parallel working) in the non-state sector and its impact on health care delivery.
9 Peter Berman and Ravindra Rannan-Eliya, October 1993, Factors affecting the development of private health care in developing countries: Review of Concepts and Literature and Preliminary Field Design, Health Financing and Sustainability Project, Montgomery, USA. 10 The Private Sector in health includes: Private Not for Profit Health Providers (PNFP), Private Health Practitioners and, Traditional and Complementary Medicine Practitioners (TCMP). The PNFP includes Facility Based (FB-PNFP) and are religious based for example Uganda Catholic Medical Bureau and; Non-facility based (NFB-PNFP) such as NGOs both local and international.

Priority Research Questions Study Makerere Institute of Social Research
19
19
4.0 FINDINGS FROM KEY INFORMANT INTERVIEWS
4.1 Policy Concerns - Health financing
4.1.1 Budgeting and Resource allocation for the health sector
The budgeting process for the health sector seemed very clear to majority senior policy makers. As reported by one of the informants from Ministry of Finance, the Medium Term Expenditure Framework (MTEF) is the overall mechanism by which resources are expected from government, including donor budget support and allocated sectors. The MTEF sets sector and local government spending ceilings within a three year rolling framework. The sectoral ministries through Sector Wider Approach (SWAP) then decide on spending within available resources in the context of their strategic plans such as HSSP II of the Ministry of Health. This is expected to link planning and development in budgeting based on the amount of resources available.
The majority of policy makers particularly in planning department and financing section of the Ministry of Health reported that though the budgetary resource allocation to the health sector had increased over the period of HSSP I from 7.6% of the government budget in 2000/01 to 10.3% in 2003/04, the sector is still grossly under funded. As clearly expressed by one informant, in reality the money got from all the three sources (government, donors and user fees) can just be US$ 18-20 per person per year but only US$ 9 per person per year is available in the budget of the Ministry of Health. Again this is considered far less compared to Uganda’s unit cost estimated at US$ 30 per person per year and the World Health Organisation (WHO) minimum requirement of US$ 30-40 per year per year excluding bed nets, ARVs, ACT and some vaccines for children. A senior policy maker in charge of Ministry of Health planning alluded;
In 2002/2004 the health sector budget was about 220 billion shillings and rose to 242 billion shillings in 2007/2008 instead of the expected - over 430 billion. …. In real terms the budget being used is just for 8 million people to provide health services to the population of about 27 million people. (Senior Policy Maker, Planning, MoH)
The under funding of the health sector raises a number of policy concerns reflecting the continuing colonial legacy. The major source of funding for the health sector remains the tax base system supported by donor funds with limited health insurance and user fees. Though user fees were retained in private wings in public referral hospitals and Private Not-For-Profit (PNFPs) facilities after they were abolished in 2001, they do not cover a full cost recovery component at any point of service delivery. On the other hand health insurance remains limited to a few corporate bodies and companies that make specific arrangements for their staff with private health providers. A senior public officer hinted on the implications of inadequate national resource envelope:
Ministry of Finance Planning and Economic Development does not envisage massive resources coming into the national budget, Therefore review of current funding priorities may be needed to encourage reallocation of resources or look for efficiency savings within the sectors (Principal Officer, MoFPED, Kampala)
4.1.2 Public financing of the private sector
The PNFPs contribution to health service delivery in Uganda was reported to be of close to 40% by most policy makers and leaders of PNFPs. For example 37% OPD services and; 35% of delivery of mothers is by PNFPs. Despite this sizeable contribution, government financial support to PNFPs is very low. Currently government contributes only 22% with 38% covered by user fees and 40% from

Priority Research Questions Study Makerere Institute of Social Research
20
20
donations. Yet PNFPs are by law bound to provide Primary Health Care service (PHC) such as immunization of children and mothers that is at 29% coverage. In addition, public policy makers acknowledge that hardly any support was being extended to non-facility based PNFPs until the global initiatives that are pushing for more focus in that direction using GAVI and the Global funds.
The misconception by government that PNFPs get a lot of external funding from international organizations should be corrected. The external grants are not even regular in the way they come. (Head/Programme Officer, Faith Based NGO Medical Bureau, Kampala)
The PNFPs further reported experiencing problems related to inelastic funding from the public sector. Key among these is the exodus of health workers from PNFPs to government sector, which is providing better pay and employment motivation such as various allowances, shorter working hours and career development opportunities. The PNFPs are said to have responded by increasing user fees to raise funds to sustain their services. They have also resorted to using part time doctors, employing clinical officers and nursing assistants instead of highly trained nurses. This tends to breed overload of staff resulting into general poor quality of services provided because fewer staff can not give patients enough time. These combined are reported to discouraged many people who are not able to pay more from seeking health services as well as low trust in the quality services and performing capacity of health facilities.
Few patients tend to seek services due to the low trust they develop. The quality of health care is down below average. So as a way of survival PNFPs tried to increase user fees to sustain qualified health workers (Head/Programme Officer, Faith Based NGO Medical Bureau, Kampala)
Generally small facilities do not attract any good funding but rely on user fees. The impact of user fees has been the reduction of clients seeking services in faith based facilities (Head, Faith Based NGO Medical Bureau, Kampala)
4.1.3 Alternative source of financing
The proposed National Health Insurance Scheme is considered one of the key alternative sources of financing the sector. The policy makers reported that the scheme which is derived from the National Health Policy of 1999, expects everybody to pay for health services. The piloting of the scheme expected to start with the formally employed in both public and the private sector plans government contribution of 50%, employer 10% and the beneficiary 40% to raise 2.5% of the health budget in about five years. The informants from the public sector raised a number of concerns related to the scheme. The first was the concern on the financial implications on employers business as they contribute to the scheme. Second was how to get everybody (unemployed and informal sector) into the scheme and make it affordable to most people. Others are the mechanisms of collection and disbursement of funds and; lack of credible institutions to run the scheme given Uganda’s past experience with poor management of provident funds.
Employers are skeptical about financial implication of the scheme on their businesses. The requirement that employers contribute to the scheme is what is causing the controversies. The national health insurance policy is very sensitive because it touches on the private money. (Senior Policy Maker, Planning, MoH , Kampala)
The informants in the public and private sector further expressed doubt on the implementation of the national social insurance scheme when it eventually becomes law. The non-governmental key partners in health care delivery such as PNFPs and PFPs are reluctant to enter the national health scheme because the government has not studied and determined costs and mechanisms of taking up contractual arrangements. The costing of services remains very complex with apparent lack of
Priority Research Questions Study Makerere Institute of Social Research
21
21
adequate data that can be immediately and effectively utilized by the scheme. The implementation of the scheme is not in the foreseeable future with the MoH envisaged to concentrate on setting up institutions and management systems of the scheme during the period of HSSP II.
Private –not- for- profit health care providers are reluctant to enter the national social health insurance scheme because it has not been studied to determine cost of contracting arrangements and mechanisms of taking up contractual arrangements. There is no information or financial analysis to guide decision making (Head, Faith Based NGO Medical Bureau, Kampala)
I have not seen the costing of health service delivery in Uganda. … Yet we are now going for the National Social Health Insurance Scheme. Since government does not have any costing strategy, either the service provider or client is going to be cheated (CEO, Faith Based NGO Medical Bureau, Kampala)
The unit cost of delivering services should be established so that the decision remains on the individual. We cannot cost health services in isolation of traditional and PFP providers who are currently not brought on board (Senior Planner, MoH, Kampala)
The informants from the private sector envisage that the scheme might negatively impact on the rural poor who are the majority of Uganda’s population. They assert that leaving out majority rural population can negatively affect health indicators because of high dependence syndrome in a country like Uganda. In addition this may create high expectations in a situation where there is no adequate financing for its implementation. It is also suspect to introducing inequity at service delivery points because those insured and those not insured may have different fees thus denying the latter access to health services. The second policy concern on health financing relate to funds that are never captured in the national budgets rendering it very difficult to plan and predict its impact on health care delivery. This happens because some partners continue to put aside resources to directly fund projects in districts and for others that prefer to fund specific activities of their interest even after the Sector Wide Approach (SWAP) developed in 2002 to pool all the funds to cover agreed activities and avoid duplication of services in a few areas among development partners. The policy makers in the ministry of health acknowledge the challenges of weak systems and poor transparency in the management of funds that force some donors to pull out of the SWAP arrangement at anytime.
The dominant role of donor support to the health budgets is distorting funding of the health sector components. This is because donor initiatives are project based and thus distort the funding of the health sector.(Head, Faith-Based NGO Medical Bureau, Kampala)
The challenge of donor funding is that it is driven by their interests. Secondly the process of fund acquisition is stringent, so the funds come late and delays activities. Donor funding does not cater for human resource component. (Medical Coordinator, HIV/AIDS Service NGO, Kampala)

Priority Research Questions Study Makerere Institute of Social Research
22
22
4.2 Research Priority Questions - Health Financing The holistic costing of the health strategy rather than costing of health service delivery based on available resources was identified as the first priority question. The assessment should provide answers regarding the health burden of a country, the cost in relation to per capita GDP of the Ugandans and the health standards to be adopted in the delivery of health care. The informants particularly from the MoH and MoFPED were emphatic on determining of a unit cost of delivery of services rather than the Minimum Health Package to guide assessment the staffing levels and stocking of health facilities with drugs and equipment. The informant from the MoFPED argued that while, they may know that the health sector needs additional human resources and funding for drugs, they lack critical information for determining the numbers of health workers and amount and categories/kinds of drugs needed. A senior planner in the MoH, noted that the total cost of health care delivery is important in directing priorities towards certain areas. Another informant from a multi-lateral organization asserted that costing of health services should be based on a system that can help guide in gauging services delivered and setting realistic interventions.
The need to track cost effectiveness of resources allocated to the Ministry of Health was ranked the second priority research area in the health sector. The shared reason, invariably stated by key policy makers in the MoH and MoFPED as well as informants in NGO and Multilateral organizations was the need to assess the value for money that is currently allocated to the health sector. Needles to say an informant from MoFPED, reported that Uganda as a low income country which does not envisage massive financial resources coming into the national budget. In such a case the optimum as well as evidence-based prioritization in the use of the limited resources becomes an obvious option. The majority of the informants agreed that this research area calls for examination of the priority activities to which resources are spent and identification of factors responsible for non-improvement of health indicators in Uganda over a period of time. This research was seen to be helpful in generating evidence to support review of the current funding, programs, reallocation of resources and priority setting.
There is need to track cost effectiveness of resources allocated to the Ministry of Health to find out whether resources are spent on priority activities. … Ideally, we need research to track movement of resources allocated and how they have improved the health indicators (Principal Officer, MoFPED, Kampala)
The cost-benefit analysis of the health sector to support the proposed health insurance scheme in analyzing the situation was proposed as the third priority research area. Among the issues are mechanisms of collection of money and disbursement, accrediting institutions to provide health services and inclusion, equity and affordability issues in the scheme.
Costing of health interventions should be based on a system; because it’s a system which can guide in gauging how services can be delivered and helps in the process of setting realistic interventions. Planning should as well be based on a comprehensive required system or intervention rather than planning being driven by isolated significant problems like HIV/AIDS and Malaria. ( Health Specialist, Multi-lateral Organization , Kampala)

Priority Research Questions Study Makerere Institute of Social Research
23
23
The National Social Insurance Scheme, now a bill before the cabinet was viewed by policy makers as an alternative source of financing the health sector. Almost all the informants in the public and private sectors were skeptical regarding the implementation of the scheme. They foresee problems related to access and equity in service delivery, discrimination in costs of services, absence managerial arrangements and skills among others. There were calls for the information to address issues of policy, implementation, financing and management of the scheme across the board.
4.3 Policy Concerns – Human Resource for Health
4.3.1 Numbers, deployment and attrition
According to the public policy makers, the numbers, deployment and skills mix of health workers in health facilities present a puzzle regarding developing and managing human resource for health in Uganda. The presence of health workers in the public health units is said to be skewed towards urban areas with the majority in big hospitals despite efforts of by government to ensure equitable distribution during deployment. The problem of staff deployment was closely related to that of retaining of staff hired by the public sector. The informants from the Human Resource Department of MoH, reported that most health workers do not want to work in ‘hard to reach areas’ where they are deployed. They also leave the public to private sector or the health sector all together due to low salaries, workload and poor incentives. The attrition of health workers extends to the private sector. This was reported to have started in 2003/2004 when government selectively increased the salaries and conducted a massive recruitment exercise to fill the 6000 positions of health workers in the in public service. The private health workers mainly in the PNFPs were attracted to the public sector since PNFPs were already paying lower salaries. There was considerable concern among PNFPs that the human resources in their units may further be depleted due to government ear-marked salary increment in year 2008 and the dishonoring of PNFPs’ proposal to government requesting for an increase in subsidies to raise health workers salaries.
In 2003/2004, Uganda Protestant Medical Bureau lost over 2000 health workers, 71% of these were clinical officer. About 40% of those that left PNFPs went to government. (CEO, Faith Based NGO Medical Bureau, Kampala)
Salaries in the public sector are higher than in the private not for profit sub-sector, so our problem is to find a way of retaining staff because these providers serve the most rural areas not served by government (Senior Policy Maker, Human Resource Dept., MoH, Kampala).
The ministries of health and public services acknowledge the apparent lack of proper mechanisms for tracking staff deployment including those on normal transfers and those that go outside the country for various reasons such as studies. The regulation and code of conduct of health workers is also said to be very poor that even when there are numbers and skills mix, the poor work ethics override them.
4.3.2 Record Keeping and Data Management The poor record keeping in the public sector was reported as one of the serious problems. Though the HRH information exists, it is found to be disjointed, difficult to access and not standardized sometimes creating contradictions in sets of data such as the pay roll and the general register of health workers. For example the MoFPED urged that they may know that the health sector needs

Priority Research Questions Study Makerere Institute of Social Research
24
24
additional human resources but lack aggregated information for decision making on the numbers and categories of staff needed.
Only one person based in the ministry of health manages data with a lot of secrecy. 0ne time we were in a planning workshop and we wanted information from MoH but we couldn’t get it because the person managing the data was sick and admitted at Mulago national referral hospital. The computer had to be taken to him in hospital and he was so protective in not wanting others to see the password (Senior Policy Maker, Human Resource Dept., Ministry of Public Service, Kampala)
The policy makers reported that currently there is no information on different categories, specializations and health staff ratios such as nurses and doctors at health centers, regional and district hospitals. There are also no standards required to develop a skills mix formula to be applied to provide proportionately required numbers for the various health facilities.
There is need to study the existing human resource status to establish numbers skills mix and related strategies for human resources development (Advisor, Human Resource Dept., MoH, Kampala)
4.3.3 Human Resource for Health Training
The quality of training health workers is another major concern expressed by most informants. In Uganda all medical training schools were hurriedly transferred to Ministry of Education and Sports (MoES) from that of Health without streamlining the management of the institutions and relationship between the two ministries. The controversy was reported to be wide spread to include ownership, management and conflict of roles between the two ministries. For example, while the Nurses and Midwives Council is mandated by law to set examination for medical students, UNEB under the MoES is also mandated to set examinations for the same medical students such that some nurses who didn’t do examinations set by the Medical Council in the previous years had not been registered by time of interview. The conflict was reported to have considerable devastating impact on human resource training. Three informants from human resource department of the ministry of health and one from the ministry of public service reported that the problems range from losing focus on human resource development aspect, lack/inadequacy of teaching materials like gloves to low quality of training of health workers.
The shifting of medical schools to MOE has revealed the poor coordination between MoES and MOH … Both MoES and the Nurses and Midwives Council have exercised their mandates and given nurses contradicting examinations. ( CEO, Faith Based NGO Medical Bureau, Kampala)
4.3.4 Management of Human Resource for Health
Another key concern identified by the informants in public and private sector is the management of the current human resource for health. In Uganda’s decentralized system of governance, Health service delivery is decentralized to local governments. The informants in the public sector reported that every district recruits and keeps their staff which the MoH is not mandated to supervise and transfer. Moreover the districts health staff are not answerable to human resource Development department, of the MoH which makes districts independent in their health workforce operations. Even in situations where some district health services have been poorly managed, MoH reported that it was unable to intervene and discipline the decentralized staff or easily apply sanctions such as refusing to fund those districts. For example some districts have recruited District Medical Officers of low caliber since much of the recruitment in local government is characterized with nepotism.

Priority Research Questions Study Makerere Institute of Social Research
25
25
In addition, some staff seconded to PNFPs could go for further studies without MoH’s consent, while some became difficult to manage by their bosses in PNFPs claiming allegiance to MoH, which in essence doesn’t have any control over them. This forced the Ministry of Public Service to abolish the seconding of health workers to Private Not-for-Profit (PNFP) facilities. A related concern was that of dual employment of public health workers reported to greatly affect the performance of the public sector. The dual employment of public health workers has implications on quality and management of health care delivery such as indiscipline, time loss and poor work ethics. The tendency is for the health workers valuing job security and addresses from the pubic sector that make them even more recognized in their private practice.
The President of the Republic Uganda directed us up to come up with a figure to pay staff and stop dual employment but it is still a difficult thing to do due to lack of data on the cost efficiency of the health sector ( Senior Policy Maker, Human Resource Dept., Ministry of Public Service, Kampala)
4.4 Research Priorities Areas – Human Resource for Health The absence of a harmonized human resource management system and a consolidated human resource development data creates a need for a Human Resource for Health systems study. The first priority research area was an assessment of the current recruitment, deployment and management systems of health workers in the public health sector. The study is intended to review the current system to identify the strength and weaknesses and develop a monitoring and evaluation system for existing HRH. The policy makers in charge of human resource in Ministries of health and public service expressed the need for information on the number of staff and their categories in public and private health sectors, their qualifications and distribution in the service as the second research area. For example the lack of this kind of data continue to make it difficult to calculate and process pensions of retiring staff, determine the number of staff recruited at certain time, assess the workload and future human resource needs. The research question was the study on the number, categories and length of service of public and private health workers. In this study an assessment of the skills mix was also considered important to help in developing a skills mix formula/strategy that can proportionately provide required numbers for various health facilities. The third research question was to review the training curricula to address the health sector needs in light of the new diseases, changing health care seeking patterns, new policies and the occupational issues of health workers. The increasing workload for health workers and the emerging issues such as task shifting where doctors should be able to shade off some tasks to nurses require re-examination of the training curricula. The challenges of building synergies for human resources between the sectors to address problems of dual employment, staff specializations and training discussed earlier presented a fourth research area. The research question is the need to examine the relationship with regard to human resources deployment and development between the two sectors and the impact on performance of the public and private health sectors.

Priority Research Questions Study Makerere Institute of Social Research
26
26
4.5 Policy Concerns – Non-State Sector The public and private sector have had a lot of informal collaboration dating back in 1960s. However, public and private informants reported that the partnership between government and the PNFP sub-sector was still weak. The government stills gives PNFPs little money amidst considerable contribution. In addition both government and PNFPs have different focus and objectives in health care delivery.
The general situation is that there are weak partnerships between government and the PNFP sub-sector and lacking in the PFP and Traditional sub-sectors.(Senior Policy Maker, Public Private Partnership, MoH, Kampala)
The reports from private providers indicated that there was hardly any meaningful relationship between the government, PFP and Traditional sub-sectors. They complained of being unrecognized by government with the traditional sub-sector being considered informal and not legally recognized. However, the private sector pay taxes, employ health workers and make services readily available to communities apart from being required to provide immunization and ARV services free of charge.
Private for-Profit (PFP) providers are taken as people out there just making money yet PFPs are providing highly required and specialized services such as heart surgery (Chief Executive Officer, Private Hospital, Kampala)
This hospital is actually spending about Uganda Shillings 1.5 million monthly to pay for the delivery of free public services (Medical Director, Private Hospital, Kampala)
4.6 Research Priorities Areas – Non-State Sector
The first priority research question is to develop a comprehensive Health Management Information System (HMIS) to generate information from the private sector (PNFP, PFP and Traditional and Complimentary Medicine). The data generated should be reflected in the national official documents for planning and policy making purposes.
The second important research question is to provide an account for the weak/absence of relationships/synergies in the health sector. The information is intended to provide strategies to improve and establish desired collaboration among the different sub-sectors in health care delivery. The third should be a national mapping of the private health facilities and providers, categorize them. The study should also generate data on pricing of services, kind of patients handled by the private sector, costs and treatment procedure as well as information made available to patients by providers. The fourth would be a national survey on consumer satisfaction. The survey would help bring out consumers’ views regarding improving service delivery and establish the value for money audit from the health consumers.

Priority Research Questions Study Makerere Institute of Social Research
27
27
5.0 DISCUSSION
5.1 Uganda’s Health Policy Environment The health sector policy development process is considered to be interactive involving key stakeholders addressing particular areas. These initiate policy ideas that are brought to the attention of the ministry of health or the ministry itself can initiate policy development process. In each case a concept policy paper has to be developed by MoH in collaboration with representative of stakeholders. When agreed upon and endorsed by the Minister responsible it then becomes a policy guidelines paper. It is a committee working closely with implementers that develops a draft policy. Finally when a policy is enacted it becomes a living document and can be reviewed to address some emerging issues. This tends to imply that the policy development is harmonious and all inclusive exercise where policy ideas of most key players in the national health system are usually considered and acted upon. However, the study results show that that some critical players such as PFPs and traditional medicine have always been merely recognized but not streamlined in the health policy making process. The abundance of policy concerns among public policy makers, private providers, and representative of public providers and users/consumers of health care point to limited consultations in the health policy environment. The financing mechanisms applied by MoFPED, proposed National health insurance scheme, lack of data on most aspects of human resource for health and weak/absence of relationship between public and much of the private sector are a few examples that show limited involvement of key stakeholders in health policy making.
5.2 Health Financing The costing and allocation financial resources for health emphasize minimum health care package to ensure universal access to health services by all people. The health resource allocation criteria do not only greatly vary across providers but is based on few factors. For example in the public sector the allocation of resources to district health services are based on factors such as population size in the district; levels of poverty using the human poverty index provided by Ministry of Finance Planning and Economic Development; level of development of the district in terms of road network, access to electricity and health infrastructure. For the PNFPs that access public funding consideration has been given to facility based units on the basis of number of beds and level of the unit. For the other key players such as the PFPs and Traditional medicine has not any known basis upon which they access or may access public financing.
The practice of costing and allocation of public financial resources appeared to be driven by limited resources of the health sector. This means that priority setting and adequate health care delivery is likely to remain a formidable challenge even with the available resources.
The holistic costing of health care delivery that was identified and ranked number one of the priority research question thus become critical in generating information to help setting priorities in a resource constrained country like Uganda.

Priority Research Questions Study Makerere Institute of Social Research
28
28
5.3 Human Resource for Health The Human Resource for Health Policy (HRHP), 2006 and the strategic plan 2005-2020 have clearly identified the major problems but not the factors responsible for the key problems with regard to Human Resource for Health. Anecdotal evidence indicates that these problems are a result of a combination of factors the main ones being poor remuneration, conditions of services as well as lack of harmonized human resource development and management system in the national health system. With current information on HRH disjointed, difficult to access and not standardized, majority of health workers have been known to take advantage and engage in dual employment to earn additional income11 default on deployment or migrate in search of better conditions of service. Attaining the desired goals and standards of the Human Resource for Health Policy may need major overhaul of government human resource management systems, revised conditions of service and clearly developed human resource deployment arrangements between the public and private heath sectors. These actions will require information on most attributes as well as the development and management systems of human resource in the health sector.
5.4 Non-State Sector The Non-State sector is large and widespread. By comparison to the public sector, private health facilities are relatively abundant and much closer to the majority of the population and present to users a wide variety of types and levels of services.12
The role and contribution of the Non-State sector in health care delivery is as varied as the players. For example, the role of faith based PNFPs provide health care as a social services to the public targeting the vulnerable people. The PNFPs health services extend to the very remote areas where government services are not existent. Available data shows that PNFPs cover 36% of fixed facilities offer 7800 beds compared to 9500 beds of the government. In that respect, the public and private sectors are considered ‘natural’ partners in health care delivery. The non-state sector is recognized as a key stakeholder in HSSPI and II as well as in the proposed National Social Health Insurance Scheme. However, weak partnerships between the government and the PNFP sub-sector. The most significant factors fostering current partnership between government and PNFP is basically that NGOs have structures that government finds easier to deal with; as opposed to the private for profit (PFP) and traditional sub sectors. On the other hand, any partnership hardly exists between government, the Private for profit and Traditional sub-sectors. The PFP were considered by policy makers to be much disorganized during policy development meetings even in instances where they have an association while traditional Spiritualists’ shied away from policy development process because they could not meet the modern religious spiritualists. The funding methodology or unit costing to private sector continue to based on the capacity of the health facilities in terms of the number of beds and level of the health unit. Consequently the support has been limited to facility based PNFPs leaving out the majority of private sector providers. Even then government total funding has since 2004 remained stagnant despite the increase in the number of PNFPs sharing the fund. The contributions of PFPs and Traditional Medicine providers are not reflected in any national documents and no systematic support has been extended to them from the public sector. Consequently, the generation of comprehensive data on numbers, categorize and
11 Asiimwe D., Mwesigye F., McPake B., and Streefland P., (1997), Informal Health Markets and formal Health Financing Policy in Uganda, Final Report, Makerere institute of Social Research, Kampala.
See also: Jitta J. and van der Hiejden, T., (1993) , Economic Survival Strategies of Health workers in Uganda, Study Report, Child Health Development Centre, Makerere University, Kampala
12 Delius Asiimwe (1999), The Current Private Health Care delivery System in Uganda, Makerere Institute of social Research , Kampala

Priority Research Questions Study Makerere Institute of Social Research
29
29
range of services and their costs and contribution remain critical in development of harmonized health system. The proposed National Social Health Insurance Scheme is derived from the National Health Policy of 1999, out of the need for a financing strategy and system to generate own funding to supplement government resources. In a situation where the employer together with the beneficiary contributes 50%, a number of controversies and challenges arise to make national health insurance policy a very sensitive issue. Its piloting is proposed to start with the formally employed in both public and the private sector making it accessible and affordable to just a few people. The mechanisms of collection; disbursement of funds and accrediting of institutions to provide health services are not current feasible in a situation where the Uganda government is ridden with corruption and bad experiences of management of provident funds. These and other challenges make employers and beneficiaries skeptical about financial and management implications of the scheme requiring that the government revisits the proposed bill of the scheme.
5.5 Strength of the study Methodology The focus on policy makers as informants, the majority in the health sector enabled using interview schedules with relatively similar questions to deal with issues related to the study objectives. This made the analysis easy when it came to drawing similarities and differences in the data from various respondents. The interview with such knowledgeable respondents also permitted exploring in detail a wide range of issues as well as sharing of experiences on the three thematic areas under study.
The other strength was the factor that the study utilized a wide range of literature from official document, surveys, reports and publications that were collected from the varied sources such as internet, libraries and offices of key policy makers. This method was helpful in collecting documented data that formed a basis for follow‐up questions and supplemented the data from key informants.
These two together presented a comprehensive assessment of the priority research questions from the available key sources of information in the country.
5.6 Short Comings of the Study Methodology The selection of the key informant interviews was subjective in that the knowledge and experience on issues under study was linked to the position held by the individual in the targeted organization. In a few cases where individuals were not conversant with much of the subject matter and never suggested alternative source, less valuable information was obtained.
The focus on policy makers as informants meant generating information mainly on questions and issues affecting their planning and implementation processes. This left out much of the information on concerns and questions of most health providers and users of the health services in the country.
The study assumed a coherent and vibrant non‐state sector. However, Uganda’s non –state health sector is highly fragmented and efforts to interview a cross‐section of informants did not yield much valuable data. The lack of knowledge regarding government plans and policies and the non‐state sector exclusion from mainstream development processes as well as poor record keeping in both sectors limited the information being sought.

Priority Research Questions Study Makerere Institute of Social Research
30
30
6.0 REFERENCES 1. Ashington Ngigi and Daniel Macharia , Health Sector Policy Overview Paper, May 2006, IT Power East Africa
(http://www.enable.nu/publication/D_1_7_Kenya_Policy_Overview.pdf) (accessed 30/07/07)
2. Asiimwe D., Mwesigye F., McPake B., and Streefland P., (1997), Informal Health Markets and formal Health Financing Policy in Uganda, Final Report, Makerere institute of Social Research, Kampala.
3. Draft National Policy on Public Private Partnership in Health Care, (PPPH) 2006.
4. http://www.who.int/countries/uga/en/ (accessed 29/01/08)
5. Kiyonga C.W.B (1997), Minister of Health, Health Policy Statement 1997/98, Ministry of Health, Entebbe
6. Magnus Lindelow, Ritva Reinneka and Jakob Svensson (2003), Health care on the Frontlines: Survey Evidence on public and private providers in Uganda, African Region Human Development Working Paper Series, The World Bank, Washington D.C
7. Ministry of Finance, Planning and Economic Development: Budget Speech, Financial Year 2005/2006, June 2005, Kampala.
8. Ministry of Health (October 2006), Annual Health Sector Performance Report, Financial Year 2005/2006, Kampala
9. Ministry of Health, Draft Health Policy, 1998, Entebbe
10. Ministry of Health, Human Resources for Health Policy, April 2006, Kampala
11. The Health Sector Strategic Plan (HSSP) 2000/01 – 2004/05
12. The Health Sector Strategic Plan (HSSP) 2005/06 – 2009/2010
13. The Republic of Uganda, The Local Government Act, 1997
14. The Republic of Uganda , Poverty Eradication Action Plan 2004/5 – 2007/8, Ministry of Finance, Planning and Economic Development, Kampala, December, 2004
15. The Republic of Uganda, National Health Policy, September 1999, MoH, Kampala
16. Uganda AIDS Commission, (April 2007); Accelerating HIV Prevention: The Road Map towards Universal Access to HIV Prevention in Uganda, Uganda HIV/AIDS Partnership Committee, Kampala
17. Uganda Bureau of Statistics and ORC/Macro, August 2007, Uganda Demographic and Health Survey 2006, Entebbe: Bureau of Statistics, and Calverton, Maryland: ORC/Macro.
18. Uganda Bureau of Statistics and ORC/Macro: 2002 Uganda Population and Housing Census, 2002, Entebbe
19. Uganda Bureau of Statistics, Uganda National Household Survey, 2006

Priority Research Questions Study Makerere Institute of Social Research
31
31
Annexes:
1: List of Key Informants
2: Key Informant Tools

Priority Research Questions Study Makerere Institute of Social Research
32
32
LIST OF KEY INFORMANTS
NAME TITLE ORGANISATION/INSTITUTE
MINISTRY 1. Dr. Naomi Kyobutungi Assistant Commissioner, Health Services (Human
Resource Department) Ministry of Health
2. Mr. Moses Arinaitwe Assistant Commissioner, Human Resource Development Ministry of Health
3. Dr. J.H. Kyabaggu Technical Advisor, Human Resource Department Ministry of Health
4. Dr. Eddie Mukooyo and Mr. Amos Nzabarita Assistant Commissioner, Health Services (In‐charge of Resource Centre) and Principal Bio‐Statistician
Ministry of Health
5. Dr. Robert Basaaza Senior Planner / Health Economist Ministry of Health
6. Dr. Grace Mulindwa Head, Health Financing Section Ministry of Health
7. Dr. Francis Runumi Commissioner, Planning Ministry of Health
8. Dr. Nathan Kenya‐Mugisha representing Director General, Health Services
Director, Clinical Services and Community Medicine Ministry of Health
9. Ms. Jane Mwesiga Assistant Commissioner, Human Resource Development Ministry of Public Service
10. Mrs. Elizabeth Imagara representing Commissioner, Planning
Principal Policy Analyst Ministry of Local Government
11. Mr. Laban Mbulamuko Principal Economist, Budget and Evaluation Department Ministry of Finance Planning Economic Development (MoFPED) – Medium Term Expenditure Framework Email: [email protected]
SPECIAL HEALTH PROGRAMS
12. Dr. Jacinto Amandua Commissioner, Clinical Services Ministry of Health
13. Dr. Elizabeth Madraa Program Manager AIDS Control Program, Ministry of Health
14. Dr. Nelson Musooba Assistant Commissioner, Public Private Partnership Ministry of Health
15. Mr. Elly Mugumya Executive Director Family Planning Association of Uganda (FPAU) Email: [email protected]
16. Prof. John Rwomushana Director, Policy and Research Uganda AIDS Commission

Priority Research Questions Study Makerere Institute of Social Research
33
33
NAME TITLE ORGANISATION/INSTITUTE
17. Dr. Possy Mugyenyi representing Program
Manager, EPI
Deputy Manager, Expanded Program on Immunization Uganda National Expanded Program on Immunization
BI/MULTILATERAL ORGANISATIONS 18. Dr. Peter Okwero Health Specialist World Bank 19. Mr. Dan Ahimbisibwe Programme Officer, HIV/AIDS USAID 20. Dr. Juliet Nabyonga and Dr. William Mbabazi National Professional Officers, Health Economics /
Surveillance World Health Organisation (WHO) Email: [email protected] ; [email protected]
RESEARCH INSTITUTES & ORGANISATIONS 21. Dr. Simon Peter Rutabajuuka Executive Director Centre for Basic Research, Uganda
Email: srutabajuka@cbr‐ug.org 22. Dr. Grace Nambatya Executive Director Traditional & Complementary Medicine Laboratory,
Uganda 23. Prof. Ralph Owor Director Uganda Health Research Organisation (UNHRO)
PRIVATE FOR PROFIT HOSPITAL 24. Dr. Ian Clarke Chief Executive Officer International Hospital Kampala (IHK)
Email: [email protected] PRIVATE CLINIC 25. Dr. Henry Kasozi Medical Director KADIC Hospital
Email: [email protected] PHARMACEUTICAL OUTLET 26. Mr. Crescent Muhumuza Pharmacist Friecca Pharmacy NON GOVERNMENTAL ORGANISATIONS (NGOs) 27. Dr. James Tamale Secretary The Pharmaceutical Society of Uganda
28. Ms. Mary Namusisi Branch Programmes Coordinator Uganda Private Midwives Association 29. Dr. Geoffrey Mulindwa and Vanessa
Tremamunno representing Executive Director Medical Service Coordinator and Public Relations and Advocacy Manager
AIDS Information Centre (AIC) Email: [email protected] ; [email protected]
30. Dr. Jennifer Kavuma General Secretary Uganda Medical Association (U.M.A) 31. Ms. Robinah K. Kaitiritimba National Coordinator Uganda National Health Users/Consumers’
Organisation 32. Dr. Christine Nabiryo Lwanga representing
Executive Director Director, Projects and Planning The AIDS Support Organisation (TASO)
Email: [email protected] FAITH BASED ‐ PRIVATE HEALTH FACILITIES

Priority Research Questions Study Makerere Institute of Social Research
34
34
NAME TITLE ORGANISATION/INSTITUTE
33. Dr. Ahmed Kiswezi Executive Secretary Uganda Muslim Medical Bureau 34. Dr. Lorna B. Muhirwe Executive Director Uganda Protestant Medical Bureau
Email: [email protected] 35. Bro. Daniele Giusti Executive Secretary Uganda Catholic Medical Bureau
Email: [email protected]

Priority Research Questions Study Makerere Institute of Social Research
35
35
Annex 4: KEY INFORMANT TOOLS
INTERVIEW SCHEDULE WITH TOP OFFICIALS IN THE MINISTRY OF HEALTH

Priority Research Questions Study Makerere Institute of Social Research
36
36
Director General Health Services Assistant Commissioner Health Services (Human Resources
Department) Assistant Commissioner Health Services (In-charge Human Resource Centre)
Commissioner Planning, MoH Commissioner Planning, Local Government Resident Consultant, Human Resource Department Head, Health Financing Section Principle Personnel Officer
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key policy maker to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End

Priority Research Questions Study Makerere Institute of Social Research
37
37
The concern of the researcher/interviewer is to set up a knowledge productive environment to stimulate open but managed discussion to find out:
1. Briefly give an overview of key policy aspects of:
• Health Financing • Human resources for Health • Non-State sector participation in health care delivery
2. What are the policy challenges that face the health sector in the next 5-10 years in the areas of:
a) Health services financing (current sources, alternative sources, financing arrangements, resource allocation) b) Human resources for Health (planning, recruitment, performance, Professionalism and ethics, regulations and incentives,
deployment turn over and immigration) c) Role of the non state sector/ Private sector (coverage, Range of services, patterns of care, quality and regulation, costs and
client choices, public private mix)
3. What are current and future national health policy concerns in:
a) Health financing? b) Human resources for health? c) Non-state sector participation in health care delivery?
4. How are the policy concerns identified with reference to:
a) Health services financing; b) Human resources for Health; c) Role of Non-State sector in health care delivery
5. What are the priority research questions that could address such policy concerns?
a) Health sector financing b) Human resources for health
c) Non-State sector in health care delivery
6. Why is each of those considered to be a priority Research Question in health sector? (Health services financing; Human resources for Health; Role of Non-state sector)
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
38
38
INTERVIEW SCHEDULE WITH PROGRAMME HEADS OF BI/MULTILATERAL ORGANISATIONS
WHO, Programme Managers; HIV/AIDS; Immunization
World Bank: Officer in-charge of Health matters
USAID: Officer of Health and HIV/AIDS
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key development partner to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End
Priority Research Questions Study Makerere Institute of Social Research
39
39
The concern of the researcher/interviewer is to set up a knowledge productive environment to stimulate open but managed discussion to find out:
1. What are the key national health policy areas supported by the agency/organization and WHY?
2. Kindly comment on:
a. Health financing? b. Human resources for health? c. Non-state sector participation in health care delivery?
3. What are current and future national health policy concerns identified by your organization in:
a. Health financing? b. Human resources for health? c. Non-state sector participation in health care delivery?
4. Why is each of those considered to be a national health policy concerns in the health sector? (Health services financing; Human resources for Health; Role of Non-state sector)
5. What are the Priority Research Questions to address such policy concerns with respect to:
a. Health financing? b. Human resources for health? c. Non-state sector participation in Health care delivery?
6. Why is each of those considered to be a priority Research Question in the health sector?
(Health services financing; Human resources for Health; Role of Non-state sector)
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
40
40
INTERVIEW SCHEDULE WITH HEADS OF SECTIONS
Head- Health Financing Head- Human Resource Head- Non-State Sector
Head – Medium Expenditure Fund (Ministry of Finance) Local Government –Officer in Charge of Finance Head - Information Services and Data Bank
Assistant Commissioner, Disease Surveillance at MOH;
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key stakeholder to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End
The concern of the researcher/interviewer is to conduct In‐depth interview with respondents. The specific respondent such as Head Health Financing will only address the general Questions and those specific to his/her thematic area
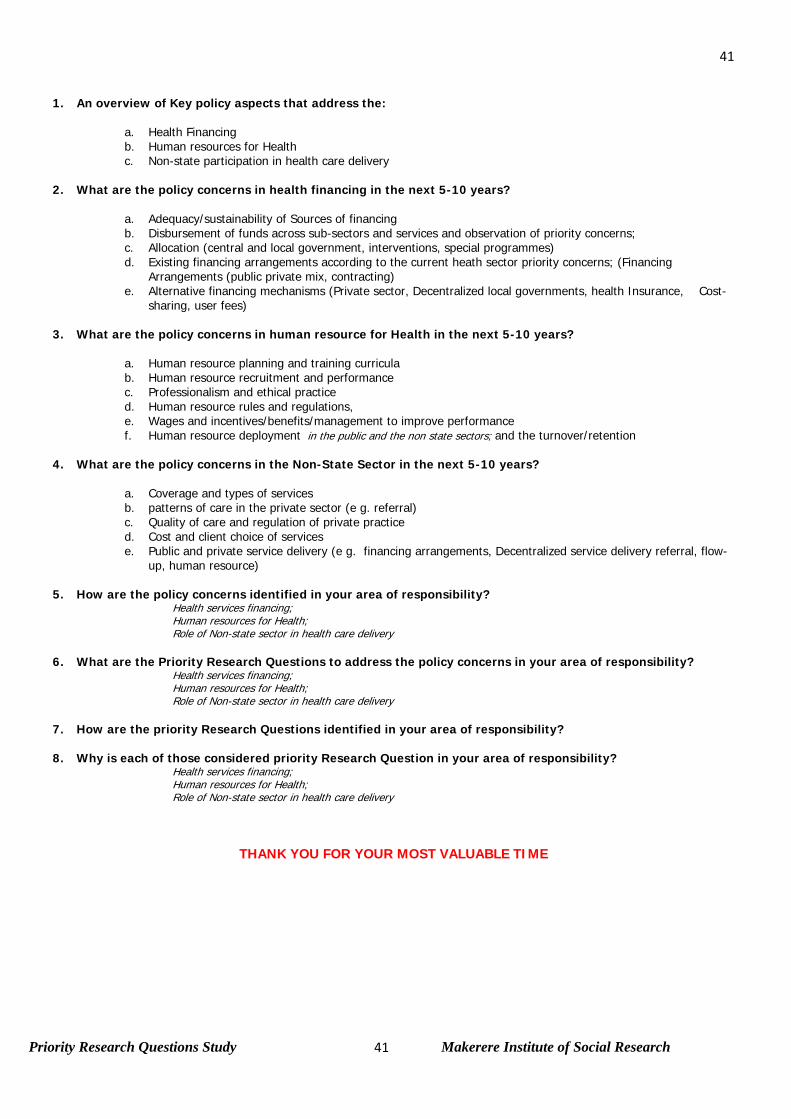
Priority Research Questions Study Makerere Institute of Social Research
41
41
1. An overview of Key policy aspects that address the:
a. Health Financing b. Human resources for Health c. Non-state participation in health care delivery
2. What are the policy concerns in health financing in the next 5-10 years?
a. Adequacy/sustainability of Sources of financing b. Disbursement of funds across sub-sectors and services and observation of priority concerns; c. Allocation (central and local government, interventions, special programmes) d. Existing financing arrangements according to the current heath sector priority concerns; (Financing
Arrangements (public private mix, contracting) e. Alternative financing mechanisms (Private sector, Decentralized local governments, health Insurance, Cost-
sharing, user fees)
3. What are the policy concerns in human resource for Health in the next 5-10 years?
a. Human resource planning and training curricula b. Human resource recruitment and performance c. Professionalism and ethical practice d. Human resource rules and regulations, e. Wages and incentives/benefits/management to improve performance f. Human resource deployment in the public and the non state sectors; and the turnover/retention
4. What are the policy concerns in the Non-State Sector in the next 5-10 years?
a. Coverage and types of services b. patterns of care in the private sector (e g. referral) c. Quality of care and regulation of private practice d. Cost and client choice of services e. Public and private service delivery (e g. financing arrangements, Decentralized service delivery referral, flow-
up, human resource)
5. How are the policy concerns identified in your area of responsibility? Health services financing; Human resources for Health; Role of Non-state sector in health care delivery
6. What are the Priority Research Questions to address the policy concerns in your area of responsibility?
Health services financing; Human resources for Health; Role of Non-state sector in health care delivery
7. How are the priority Research Questions identified in your area of responsibility? 8. Why is each of those considered priority Research Question in your area of responsibility?
Health services financing; Human resources for Health; Role of Non-state sector in health care delivery
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
42
42
INTERVIEW SCHEDULE WITH HEADS OF SPECIAL HEALTH PROGRAM
Director General, Uganda AIDS Commission Commissioner, Clinical Services (MoH)
Assistant Commissioner, Reproductive Health (MoH)
Programme Manager, Uganda National expanded programme on Immunization
Programme Manager, AIDS Control Program (MOH)
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key stakeholder to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End

Priority Research Questions Study Makerere Institute of Social Research
43
43
The concern of researcher/interviewer is to conduct In‐depth interview with respondents. The respondent such as the Director General, Uganda AIDS Commission should address the Questions with specific reference to his/her programme.
1. An overview of how your program is reflected in the national policy priorities. 2. What is the current and future financing system for the programme with regard to:
a. Sources of financing b. Financing arrangements (contracting relationships) c. Provider autonomy, d. Public private mix
3. What are current and future human resource capital concerns with reference to:
a. Availability of required Human resource b. Professionalism capacity for effective performance c. Human resource regulations, d. Wages and incentives/benefits e. Human resource deployment
4. What do you consider to be the current and future role of Non-State Sector in:
a. Level of involvement in the health sector and types of services to be delivered b. Product/services mix c. Regulation of private practice for quality d. Influence on the cost of services or price determination e. Influence on client health seeking behavior in private services
5. What are the current and future policy concerns in the implementation of your programme with reference to:
a. Health services financing b. Human resources for Health c. Role of Non-state sector in health care delivery
6. Why is each of those considered to be a policy concern for your programme? 7. What do you consider to be priority Research Questions to address the raised policy concerns in:
a. Health services financing? b. Human resources for Health? c. Role of Non-state sector in health care delivery?
8. Why is each of those considered to be priority Research Questions for your programme?
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
44
44
INTERVIEW SCHEDULE WITH HEADS OF PRIVATE HEALTH FACILITIES
Head, Uganda Protestant Medical Bureau Head, Uganda Catholic Medical Bureau CEO/Managers, Private for Profit hospital
Managers, Pharmaceutical outlets Managers, Private Clinics
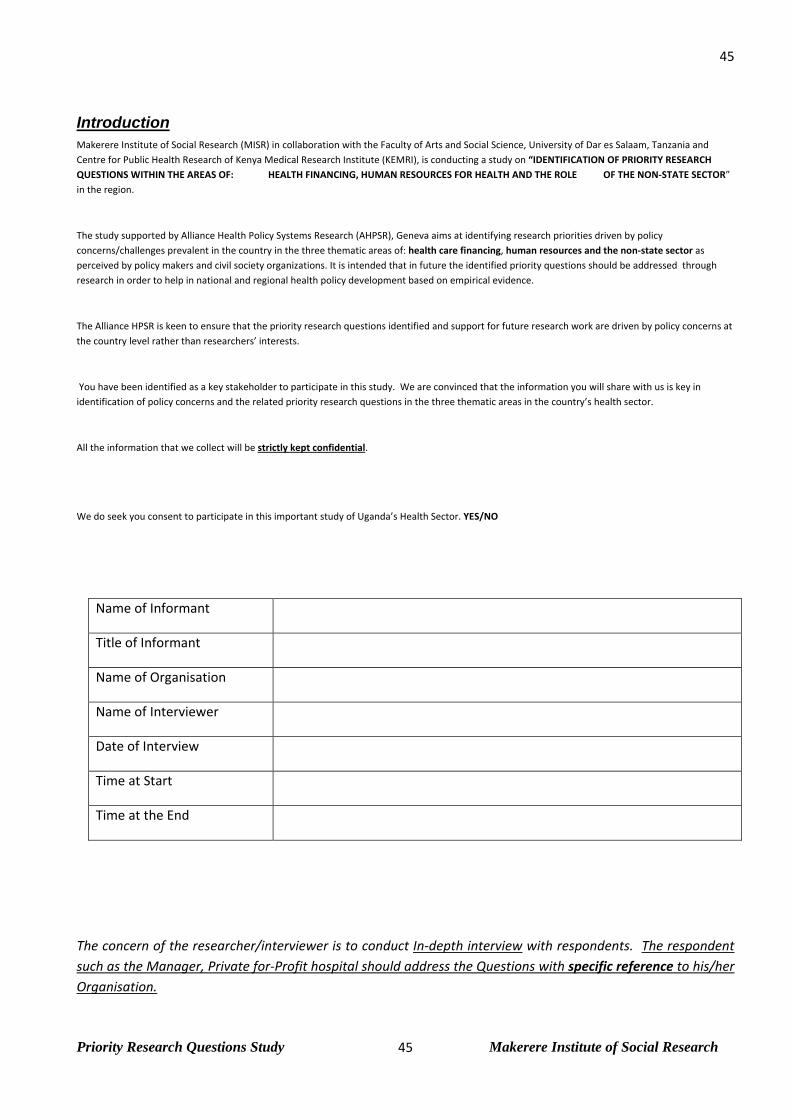
Priority Research Questions Study Makerere Institute of Social Research
45
45
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key stakeholder to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End
The concern of the researcher/interviewer is to conduct In‐depth interview with respondents. The respondent such as the Manager, Private for‐Profit hospital should address the Questions with specific reference to his/her Organisation.

Priority Research Questions Study Makerere Institute of Social Research
46
46
1. An overview of the Bureau/Hospital/Clinic/Pharmacy identification with the country’s health sector?
2. The key business/organization activities inline with national health policy? Explain the relationship (s) in terms of:
a. Health Financing b. Human Resource for Health c. Non-state sector participation in health care delivery
3. What is your role as Non-State Sector business/organization in health care delivery? a. Coverage and types of services b. Investment c. Patterns of care in the private sector (e g. referral) d. Product/services mix e. Quality of care and regulation of private practice f. Regulation of private practice for quality g. Influence on the cost of services or price determination h. Influence on client health seeking behavior in private services i. Cost and client choice of services j. Public and private service delivery (e g. financing arrangements, Decentralized service delivery
referral, flow-up,)
4. What are the health policy concerns identified by business/organization for the next 5-10 years in the areas of :
a. Health financing in the country? b. Human resources for health? c. Non-state sector participation in Health care?
5. Why is each of those considered to be a health policy concerns? (Health services financing; Human resources for Health; Role of Non-state sector)
6. What are the Priority Research Questions to address the raised policy concerns?
7. Why is each of those considered to be a priority Research Question? (Health services financing; Human resources for Health; Role of Non-state sector)
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
47
47
INTERVIEW SCHEDULE WITH HEADS NON-GOVERNMENTAL ORGANISATIONS
Director, The AIDS Support Organisation (TASO), Uganda AIDS Information Centre (AIC), Uganda President, Uganda Medical Association (UMA)
President, Uganda Pharmaceuticals Association Director, Uganda Private Midwives Association Head, Uganda Consumers’ Organization
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key stakeholder to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End
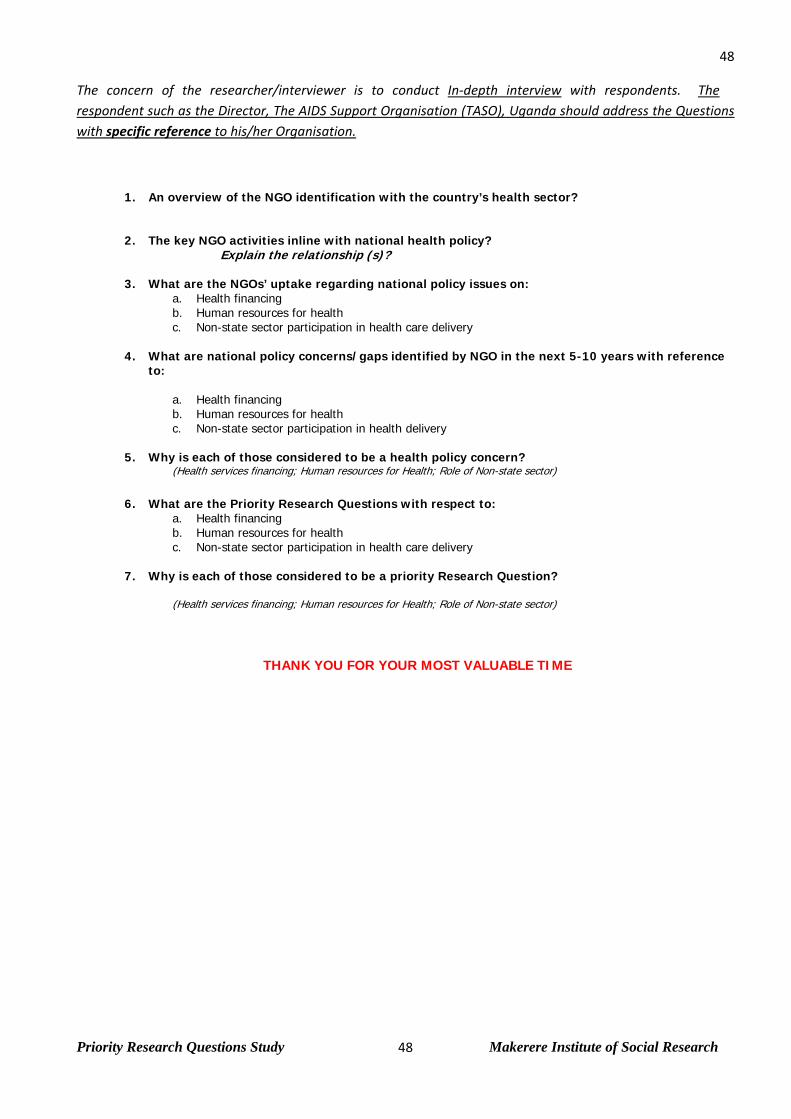
Priority Research Questions Study Makerere Institute of Social Research
48
48
The concern of the researcher/interviewer is to conduct In‐depth interview with respondents. The respondent such as the Director, The AIDS Support Organisation (TASO), Uganda should address the Questions with specific reference to his/her Organisation.
1. An overview of the NGO identification with the country’s health sector?
2. The key NGO activities inline with national health policy? Explain the relationship (s)?
3. What are the NGOs’ uptake regarding national policy issues on:
a. Health financing b. Human resources for health c. Non-state sector participation in health care delivery
4. What are national policy concerns/gaps identified by NGO in the next 5-10 years with reference to:
a. Health financing b. Human resources for health c. Non-state sector participation in health delivery
5. Why is each of those considered to be a health policy concern? (Health services financing; Human resources for Health; Role of Non-state sector)
6. What are the Priority Research Questions with respect to:
a. Health financing b. Human resources for health c. Non-state sector participation in health care delivery
7. Why is each of those considered to be a priority Research Question?
(Health services financing; Human resources for Health; Role of Non-state sector)
THANK YOU FOR YOUR MOST VALUABLE TIME

Priority Research Questions Study Makerere Institute of Social Research
49
49
INTERVIEW SCHEDULE WITH RESEARCH INSTITUTES AND ORGANISATIONS
Africa Medical Research Foundation (Regional) Uganda Health Research Organization (UNHRO) Centre for Basic Research, Uganda Traditional and Complementary Medicine Laboratory, Uganda
Introduction Makerere Institute of Social Research (MISR) in collaboration with the Faculty of Arts and Social Science, University of Dar es Salaam, Tanzania and Centre for Public Health Research of Kenya Medical Research Institute (KEMRI), is conducting a study on “IDENTIFICATION OF PRIORITY RESEARCH QUESTIONS WITHIN THE AREAS OF: HEALTH FINANCING, HUMAN RESOURCES FOR HEALTH AND THE ROLE OF THE NON‐STATE SECTOR” in the region.
The study supported by Alliance Health Policy Systems Research (AHPSR), Geneva aims at identifying research priorities driven by policy concerns/challenges prevalent in the country in the three thematic areas of: health care financing, human resources and the non‐state sector as perceived by policy makers and civil society organizations. It is intended that in future the identified priority questions should be addressed through research in order to help in national and regional health policy development based on empirical evidence.
The Alliance HPSR is keen to ensure that the priority research questions identified and support for future research work are driven by policy concerns at the country level rather than researchers’ interests.
You have been identified as a key stakeholder to participate in this study. We are convinced that the information you will share with us is key in identification of policy concerns and the related priority research questions in the three thematic areas in the country’s health sector.
All the information that we collect will be strictly kept confidential.
We do seek you consent to participate in this important study of Uganda’s Health Sector. YES/NO
Name of Informant
Title of Informant
Name of Organisation
Name of Interviewer
Date of Interview
Time at Start
Time at the End

Priority Research Questions Study Makerere Institute of Social Research
50
50
The concern of the researcher/interviewer is to conduct In‐depth interview with respondents. The respondent such as Director, Uganda Virus Research Institute should address the Questions with specific reference to his/her Institute/Organisation.
1. An overview of the Institute/organization’s research agenda?
2. The key Institute/organization’s research activities with focus on national health sector?
3. What is the Institute/organization’s research priorities and uptake with reference to:
a. Health financing b. Human resources for health c. Non-state sector participation in health care delivery
4. What knowledge gaps have been identified by your Institute/organization in the country’s health sector with reference to:
a. Health financing b. Human resources for health c. Non-state sector participation in health care delivery
5. How are the knowledge gaps identified in your institution/organization?
Health services financing; Human resources for Health; Role of Non-state sector in health care delivery
6. What are considered Priority Research Questions by the Institute/organization in the next 5-10 years in:
a. Health financing in the country b. Human resources for Health c. Non-state sector participation in health care delivery
6. Why is each of those considered to be a priority Research Question? (Health services financing; Human resources for Health; Role of Non-state sector)
THANK YOU FOR YOUR MOST VALUABLE TIME