fluids and electrolytes - school of medicine and electrolytes understand replacement strategies for...
TRANSCRIPT

S a m L a i , M D J u l y 2 016 “A d a p te d ” f ro m B in d u S wa ro o p , M D W i l l i a m G r a h a m , M D
FLUIDS AND ELECTROLYTES

Understand replacement strategies for common electrolytes Potassium Magnesium Phosphorus Calcium
Know the common clinical manifestations of electrolyte
disturbances
Know the common causes of electrolyte disturbances
F/E: OBJECTIVES

Mr. Frodo, a 60 y/o male from New Zealand with no significant medical history, presents to the UCI ER for increased fatigue and lethargy. He is noted to have dry mucous membranes and, although he denies any medication usage, in his knapsack is a prescription for Lasix. His K is found to be 3.0. The intern on call, Dr. Acula, stops his Lasix and decides to replace his potassium. 1. What are other manifestations of hypokalemia?
2. What are the most common causes of hypokalemia?
3. How do you replace potassium?
F/E: OVERVIEW

1. Clinical manifestations of hypokalemia? Cardiac AV block, PAC, PVC, Vtach/Vfib
MSK Ascending weakness Rhabdomyolysis (vasoconstriction during exercise)
GI Nausea/vomiting
F/E: HYPOKALEMIA

2. What are the most common causes of hypokalemia?
GI/GU losses Diuretic usage Diarrhea
F/E: HYPOKALEMIA

3. How do you treat hypokalemia?
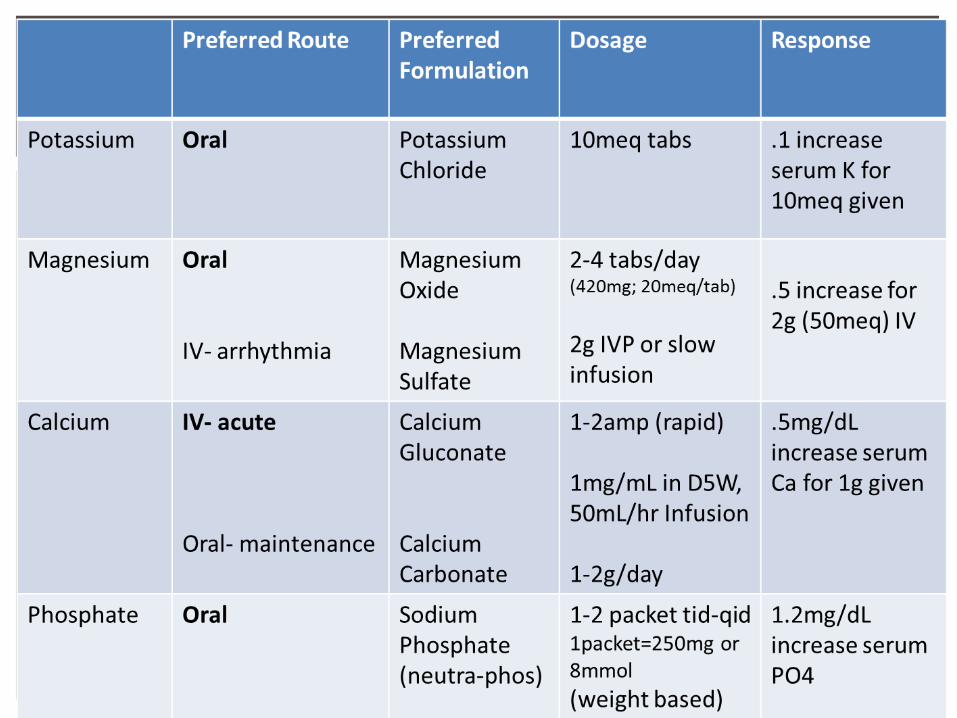
Oral: Potassium Chloride (most common formulation) Usually patients are also hypochloremic and alkalotic Can be liquid or pill form
Potassium Phosphate (if concomitant hypophosatemia)
IV Potassium Chloride Can be painful if infusion through a peripheral vein
F/E: HYPOKALEMIA
0.1 increase in serum K for each 10 meq given
(Goal K – Serum K)
Serum Creatinine

Mr. Frodo, a 60 y/o male from New Zealand with no significant medical history, presents to the UCI ER for increased fatigue and lethargy. He is noted to have dry mucous membranes and, although he denies any medication usage, in his knapsack is a prescription for Lasix. His K is found to be 3.0. The intern on call, Dr. Acula, stops his Lasix and decides to replace his potassium.
How would you treat his potassium deficit?
F/E: CONTINUED
Dr. Acula checks on Mr. Frodo after 4 hours and, while checking his blood pressure, he notices that Mr. Frodo’s hand starts to curl and twist. He starts to mumble… “I won’t make it Sam…. Sam…..”. Repeat BMP shows K of 2.8. 1. What are the common manifestations of hypomagnesemia?
2. What are some common causes of hypomagnesemia?
3. How do you replace magnesium?
F/E: CONTINUED

1. What are the common manifestations of hypomagnesemia?
Neuromuscular Tetany (Trousseau’s and Chvostek’s sign) Seizures Delirium
Cardiovascular Widening QRS Torsades
Electrolytes Hypokalemia Luminal transporters on the collecting ducts are inhibited by magnesium Low magnesium allows high intracellular potassium to efflux in to the
urine
F/E: HYPOMAGNESEMIA

2. What are the most common causes of hypomagnesemia?
GI/GU losses Chronic diarrhea Chronic diuretic usage
F/E: HYPOMAGNESEMIA

3. How do you replace magnesium?
Oral (Each has 60-80 mg of elemental magnesium) Take 3 tabs/day for mild, 6 tabs/day for moderate Magnesium Chloride Mag-Tab SR
IV If Mg < 1 mg/dL 8 grams over 12 hours If Mg 1 - 1.5 mg/dL 4 grams over 6 hours If Mg 1.5 – 2 mg/dL 2 grams over 2 hours
F/E: HYPOMAGNESEMIA
0.5 increase for 2g given

Dr. Acula checks on Mr. Frodo after 4 hours and, while checking his blood pressure, he notices that Mr. Frodo’s hand starts to curl and twist. He starts to mumble… “I won’t make it Sam…. Sam…..”. Repeat BMP shows K of 2.8.
Mg shown to be 1.4
How would you treat his hypomagnesemia?
F/E: CONTINUED
After his brief blood break, Dr. Acula walks by Mr. Frodo’s telemetry and notices a prolonged QT interval. While checking on Mr. Frodo, he notices some mild muscle twitching. Mr. Frodo asks him “Where have you taken it? It’s MINE!” His repeat BMP shows normal K and Mg, but calcium of 7.0. 1. What are the common manifestations of hypocalcemia?
2. What are some common causes of hypocalcemia?
3. How do you replace hypocalcemia?
F/E: CONTINUED

1. What are the common manifestations of hypocalcemia? Neuropsychiatric Tetany, Seizures Hallucinations and frank psychosis
Cardiovascular Hypotension Heart Failure Prolonged QT Arrhythmia
F/E: HYPOCALCEMIA

2. What are some common causes of hypocalcemia? Electrolytes Hyperphosphatemia Hypomagnesemia Inhibits PTH secretion in response to hypocalcemia
Vitamin D resistance/deficiency
Primary PTH disorders Surgery Autoimmune
F/E: HYPOCALCEMIA

3. How do you replace hypocalcemia? Oral (~ 1000-1200 mg elemental calcium/day) Calcium Carbonate Calcium Citrate
IV (symptomatic or < 7.5 mg/dL) Calcium Gluconate (1-2g over 20 minutes) Calcium Chloride (can cause tissue necrosis) Must treat with slow infusion afterwards
F/E: HYPOCALCEMIA
0.5 increase for 1 g given
After infusing Mr. Frodo with calcium, Dr. Acula goes to his coffin-l ike sleep-room. Nurse Weasley pages him a few minutes later, just as he’s about to fall asleep. “Hey doctor, Mr. Frodo in room 9 ¾ can’t breathe, just FYI” Labs show Phosphorus of 1 mg/dL 1. What are the common manifestations of hypophosphatemia?
2. What are some common causes of hypophosphatemia?
3. How do you replace hypophosphatemia?
F/E: CONTINUED

1. What are the common manifestations of hypophosphatemia? Lungs Respiratory failure from diaphragm weakness
MSK Rhabdomyolysis Dysphagia
Neuro Paresthesia or confusion
F/E: HYPOPHOSPHATEMIA

2. What are some common causes of hypophosphatemia? Refeeding syndrome
Malabsorption Vitamin D deficiency Chronic diarrhea
Increased urinary excretion Primary/Secondary Hyperparathyroidism
F/E: HYPOPHOSPHATEMIA

3. How do you replace hypophosphatemia? Oral Sodium-Phos (tab/powder, each one = 250 mg or 8 mmol)
IV Sodium Phosphate IV If Phos > 1.3 mg/dL 0.2 mmol/kg over 6 hours If Phos < 1.3 mg/dL 0.4 mmol/kg over 12 hours
F/E: HYPOPHOSPHATEMIA

Mr. Frodo returns to UC Irvine and is found to have abnormal CXR and CT Chest concerning for malignancy. He is NPO after midnight for possible bronch and biopsy. He weighs 85 kg. As Mr. Frodo is a bounce-back admission, Dr. Acula places him on D5 ½ NS @ 75 mL/hr Is that the right rate?
FLUIDS: OVERVIEW
Understand the basics of fluid distribution
Understand daily fluid and electrolyte requirements
Differentiate between dif ferent fluid preparations
Maintenance versus Repletion
Know the basic distribution of a fluid bolus
FLUIDS: OBJECTIVES

FLUIDS: BASICS
Total Body Water
Intracellular Fluids (2/3 of TBW)
Extracellular Fluids (1/3 of TBW)
Interstitial Fluid (2/3 of ECF)
Intravascular Fluid (1/3 of ECF)

Total Body Water Weight (kg) x 0.6 (Male) or 0.5 (female) Example: 70 kg male TBW = 70 kg x 0.6 = 42 Liters
FLUIDS: TOTAL BODY WATER

FLUIDS: BASICS
Total Body Water 42 L
Intracellular Fluids 28 L
Extracellular Fluids 14 L
Interstitial Fluid 11 L
Intravascular Fluid 3 L
70 kg male
1/4

Understand the basics of fluid distribution
Understand daily fluid and electrolyte requirements
Differentiate between dif ferent fluid preparations
Maintenance versus Repletion
Know the basic distribution of a fluid bolus
FLUIDS: OBJECTIVES

MINIMAL Daily Water output: Urine: 500 mL Skin: 500 mL Respiratory: 400 mL Stool: 200 mL
MINIMAL Daily Water input Ingested: 500 mL Water Content, Food: 800 mL Water Oxidation: 300 mL
FLUID: DAILY
OUTPUT = 1600 mL
INPUT = 1600 mL
Average adult 35 mL/kg/day Fever?
GI Loss?

Understand the basics of fluid distribution
Understand daily fluid and electrolyte requirements
Differentiate between dif ferent fluid preparations
Maintenance versus Repletion
Know the basic distribution of a fluid bolus
FLUIDS: OBJECTIVES

FLUIDS: TYPES
Na (mEq/L)
K (mEq/L)
K (mEq/L)
HCO3 (mEq/L)
Dextrose (gm/L)
Osmolality (mOsm/L)
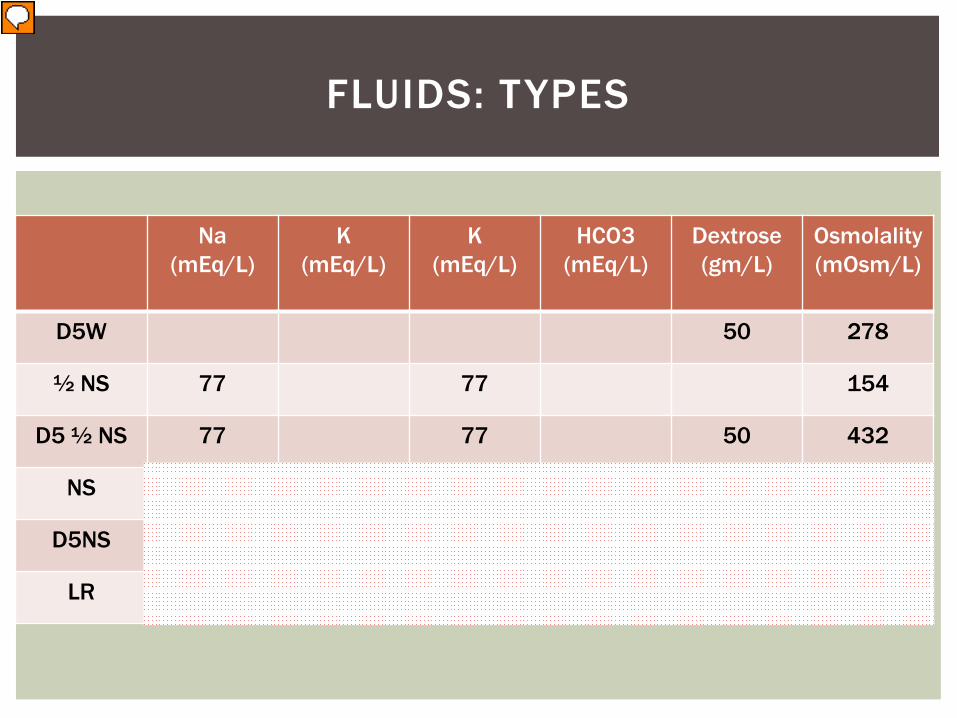
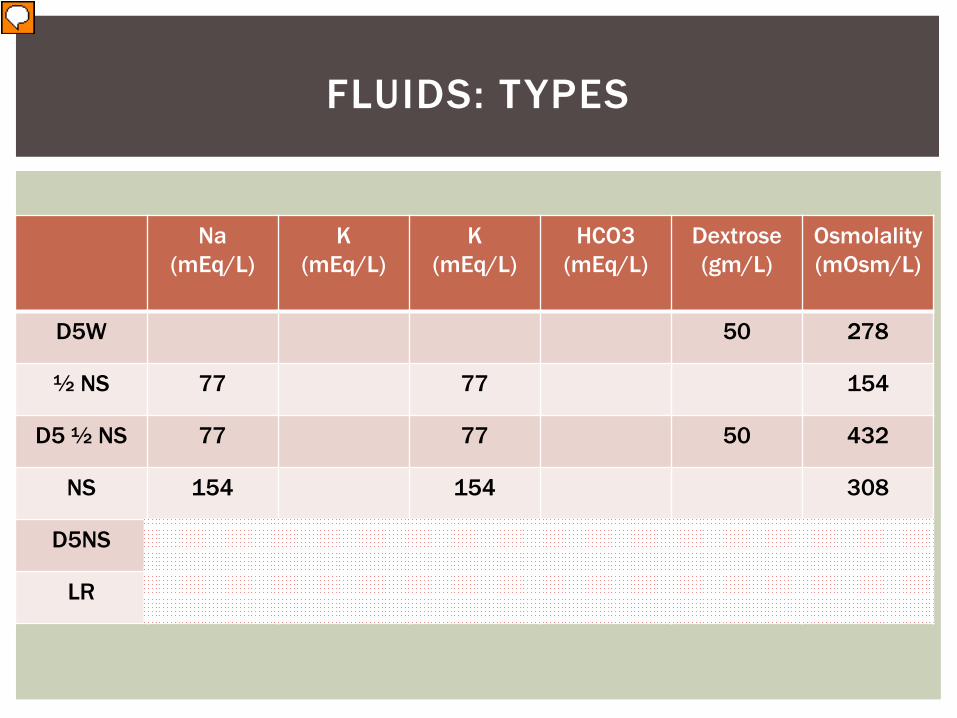
D5W 50 278
½ NS 77 77 154
D5 ½ NS 77 77 50 432
NS 154 154 308
D5NS 154 154 50 586
LR 130 4 109 28 50 272

FLUIDS: TYPES
Na (mEq/L)
K (mEq/L)
K (mEq/L)
HCO3 (mEq/L)
Dextrose (gm/L)
Osmolality (mOsm/L)
D5W 50 278
½ NS 77 77 154
D5 ½ NS 77 77 50 432
NS 154 154 308
D5NS 154 154 50 586
LR 130 4 109 28 50 272

FLUIDS: TYPES
Na (mEq/L)
K (mEq/L)
K (mEq/L)
HCO3 (mEq/L)
Dextrose (gm/L)
Osmolality (mOsm/L)
D5W 50 278
½ NS 77 77 154
D5 ½ NS 77 77 50 432
NS 154 154 308
D5NS 154 154 50 586
LR 130 4 109 28 50 272
FLUIDS: TYPES
Na (mEq/L)
K (mEq/L)
K (mEq/L)
HCO3 (mEq/L)
Dextrose (gm/L)
Osmolality (mOsm/L)
D5W 50 278
½ NS 77 77 154
D5 ½ NS 77 77 50 432
NS 154 154 308
D5NS 154 154 50 586
LR 130 4 109 28 50 272
FLUIDS: TYPES
Na (mEq/L)
K (mEq/L)
K (mEq/L)
HCO3 (mEq/L)
Dextrose (gm/L)
Osmolality (mOsm/L)
D5W 50 278
½ NS 77 77 154
D5 ½ NS 77 77 50 432
NS 154 154 308
D5NS 154 154 50 586
LR 130 4 109 28 50 272
Understand the basics of fluid distribution
Understand daily fluid and electrolyte requirements
Differentiate between dif ferent fluid preparations
Maintenance fluid calculation
Know the basic distribution of a fluid bolus
FLUIDS: OBJECTIVES

What is the goal of maintenance fluid? Replace ongoing losses of water/electrolytes under normal
conditions Such as when patient is not eating and afebrile
FLUIDS: MAINTENANCE

3 ways you can calculate rate Use hard math 35 mL/kg/day x weight (kg)
Use easier math: “4-2-1 rule” 4 mL/kg/hr for first 10 kg 2 mL/kg/hr for next 10 kg 1 mL/kg/hr for remaining weight
Use easiest math! Weight (kg) + 40
FLUIDS: MAINTENANCE

Mr. Frodo returns to UC Irvine and is found to have abnormal CXR and CT Chest concerning for malignancy. He is NPO after midnight for possible bronch and biopsy. He weighs 85 kg. As Mr. Frodo is a bounce-back admission, Dr. Acula places him on D5 ½ NS @ 75 mL/hr Is that the right rate?
FLUIDS: MAINTENANCE

Is that the right rate? Weight (kg) + 40 85 kg + 40 125 mL/hr
FLUIDS: MAINTENANCE
After his biopsy by Dr. Dumbledore, the patient spikes a temperature to 103 F, HR 110 and BP 80/60. Dr. Acula decides to initiate fluid resuscitation with 2L of ½ NS. Is this the right fluid solution?
FLUIDS: MAINTENANCE

Understand the basics of fluid distribution
Understand daily fluid and electrolyte requirements
Differentiate between dif ferent fluid preparations
Maintenance versus resuscitation
Know the basic distribution of a fluid bolus
FLUIDS: OBJECTIVES
CONCEPTS
Free water is essentially distributed across all compartments
Sodium is essentially confined in the extracellular space
Remember the 2/3 and 1/3, then ¾ and ¼ rule for fluids
FLUIDS: CONCEPTS

FLUIDS: WHERE’S THE BOLUS GOING?
1000 mL D5W distributed into Total Body Water
Interstitial
255cc
Intra-vascular
85cc (8.5%)!!
FLUIDS: WHERE’S THE BOLUS GOING?
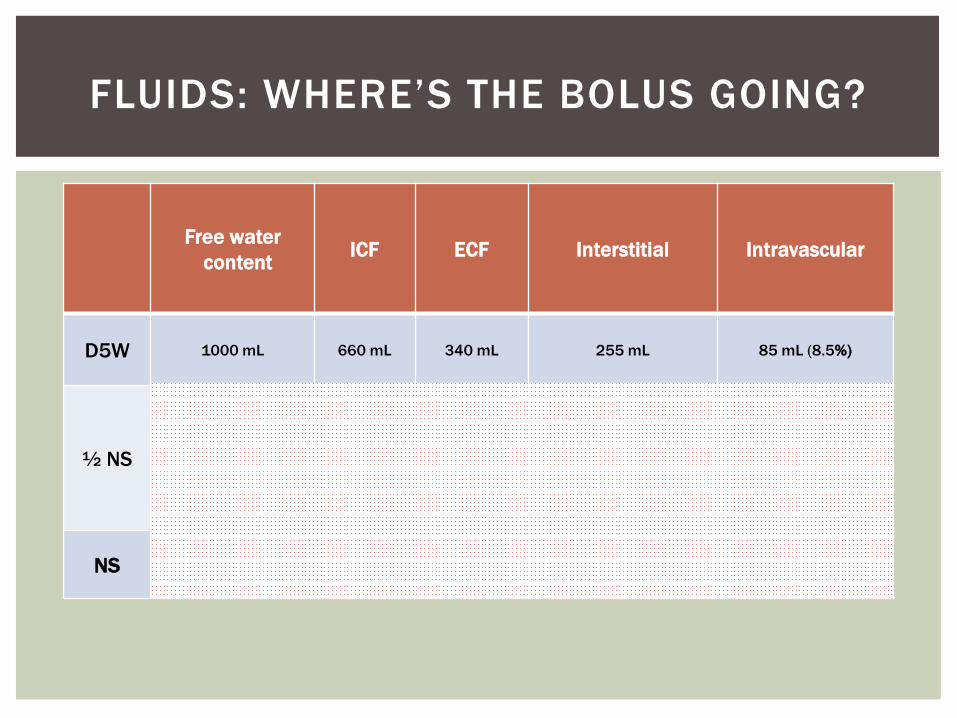
Free water content ICF ECF Interstitial Intravascular
D5W 1000 mL 660 mL 340 mL 255 mL 85 mL (8.5%)
½ NS 500 mL 500 mL 670 mL 500 mL 170 mL (17%)
NS 0 0 1000 mL 750 mL 250 mL (25%)
FLUIDS: WHERE’S THE BOLUS GOING?
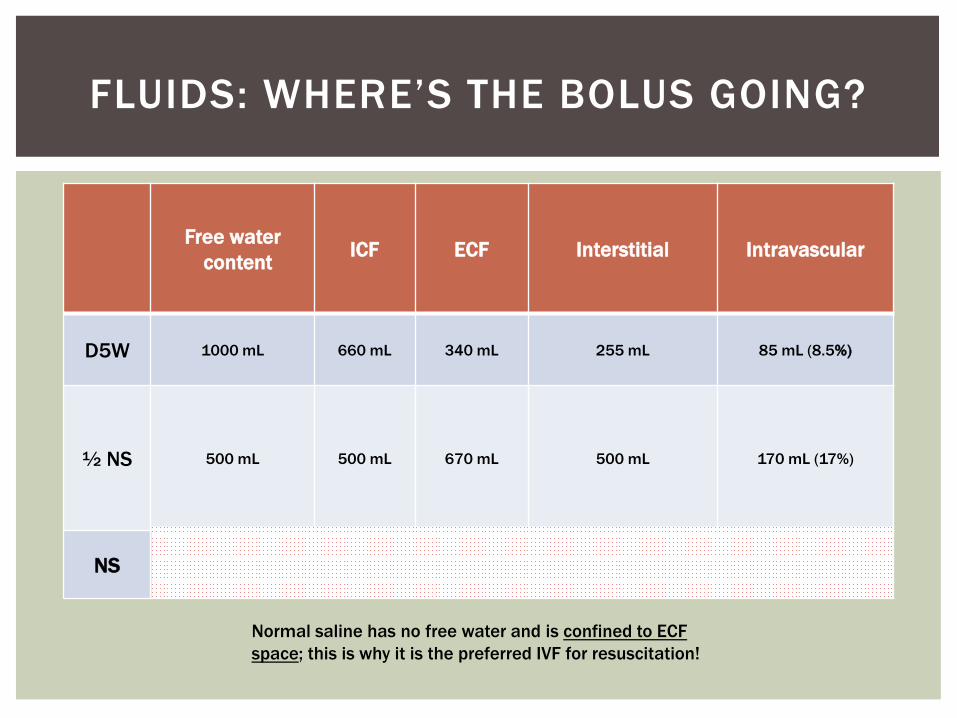
Free water content ICF ECF Interstitial Intravascular
D5W 1000 mL 660 mL 340 mL 255 mL 85 mL (8.5%)
½ NS 500 mL 500 mL 670 mL 500 mL 170 mL (17%)
NS 0 0 1000 mL 750 mL 250 mL (25%)
Normal saline has no free water and is confined to ECF space; this is why it is the preferred IVF for resuscitation!
Mr. Frodo goes home to New Zealand. Dr. Acula follows up with him in a few days and tells him the good news! The mass was just a metal ring and the doctors threw it away.
FLUIDS: THE END

It also turns out the hospital has had multiple units of blood missing from the blood bank.
Dr. Acula
FLUIDS: THE END
Dracula

Assess DAILY the need for fluids
Choose fluids based on weight
Remember the 1/3 and 2/3 rule!
Recognize the concentration of solutes in each fluid
FLUIDS: SUMMARY