focused on autoimmune and in˜ammatory diseases biopharma... · focused on autoimmune and...
TRANSCRIPT

Biopharmaceuticals
Focused on Autoimmune and In�ammatory Diseases

2
BiopharmaceuticalsDisclaimer
The views presented in this document are for discussion purposes only. Innovate Biopharmaceuticals, Inc. (“Innovate” or the “Company”) is not advocating any of the courses of action presented in it, which are being presented solely to illustrate a range of available options. This analysis is presented on the understanding that, apart from showing this document to those of your officers, employees or advisers who are engaged in reviewing it on your behalf, its contents will not be reproduced, redistributed or passed on, directly or indirectly, by you to any other person or published, in whole or in part, for any purpose without our written permission.This document does not constitute or form part of any offer for purchase, sale or subscription of, or solicitation or invitation of any offer to buy, sell or to subscribe for, any securities nor may it or any part of it be relied on in connection with any contract or commitment whatsoever. If you do not have professional experience in matters relating to investments you should not act or rely on it, and you should return this document. The distribution of this document in other jurisdictions may be restricted by law, and persons into whose possession this document comes should inform themselves about, and observe, any such restrictions. By accepting this document you agree to be bound by the terms of this notice.
This document has been prepared from information which is believed at the date of this document to be reliable. Phrases like "expects," "believes," "anticipates" and similar phrases do not constitute warranties or guarantees of any kind, expressed or implied. The information in this document is subject to change without notice. We undertake no responsibility or obligation to provide you with any additional information or to update the document or to correct any inaccuracies in it that may become apparent.The information in this document must not be used as the basis for any prescribing decisions and may not represent the approved label in all territories. Our affiliate and subsidiary companies retain the right to request the return of this document at any time. The Company’s affiliate and subsidiary companies expressly disclaim any and all liability for representations or warranties, expressed or implied, contained in, or for omissions from, this document or any written or oral communication concerning it or its subject matter transmitted or made available to any person.

3
Biopharmaceuticals
Autoimmune - Inflammation
Celiac DiseaseLarazotide
INN-202
Phase 3Ulcerative Colitis INN-108
Phase 2
First drug to market
Statistically significant Phase 2b
Highly predictive Phase 3
Platform for autoimmune diseases
Potential superiority to mesalamine
Orphan Drug Designation Grantedfor pediatric UC
Liquid oral formulation
Avoid steroids / delay anti-TNFs

4
Biopharmaceuticals
Autoimmune disease with genetic components
All patients with HLA DQ2 or DQ8 haplotype
Triggered by Gluten -> Gliadin fragments -> activate cytotoxic T Cells
Intestinal barrier weakness due to in�ammation: “Intestinal-In�ammatory Loop”
Gluten Free Foods contain up to20 ppm of gluten
Gluten found in toothpaste, mouthwash, beer, cosmetics / lipstick / gloss / balms, OTC meds/ vitamins / supplements
What is Celiac Disease?

5
BiopharmaceuticalsNo Approved Drug for Celiac Disease (Unmet Need)
Million of Patients
8M
6M6.1M
6.6M7.1M
7.6M
4M
2M
2003 2008 2013 2018
Consulted
Prevalence
3 million patients (US)3.5 million patients (EU)15 million (ROW)
Gluten Free Diet is the only therapy
Patients symptomatic on a Gluten Free Diet (GFD) su�er from :
Patient Population
abdominal pain diarrheabloating
gasabdominal cramps
loose stool
headache fatigue
nausea

6
Biopharmaceuticals
Enteropathy-associated T-cell lymphoma
Abdominal Pain Dermatitis herpetiformis
“Brain Fog” / Ataxia Neuropathy Headaches
Anemia Osteoporosis Infertility
Single environmental trigger
Many diverse consequences
Debilitating GI and non-GI symptoms
Dramatic decrease in Quality of Life (QoL)
>60% of pts su�er abdominal symptoms >1 / wk
Celiac Disease Manifestation

Paracellular Transport
Lumen
7
Biopharmaceuticals
Blood Vessels
Lumen
Lumen
Villi
Blood Vessels Lamina propia
Tight Junctions
Intestine
Intestinal Permeability: Gateway to Autoimmune Disorders

8
Biopharmaceuticals
Anti-Tissue Transglutaminase-2(tTG-2)
Deaminated peptides
Stro
nger
Bind
ing
T-cell Receptor
HLADQ2 or
DQ8
APC B-CellT-Cell PlasmaCell
Anti-tTG2 antibodies
secreted into bloodstream
Wheat Gluten Gliadin Peptides
Gliadin Peptides
Nucleus
Tight Junction
Z0-1
Proteases in Brush Border
Lamina Propria
Lumen
In�ammatory CytokineRelease
IntestinalPermeability: Gateway to Autoimmune Disorders

9
Biopharmaceuticals
Intestinal Permeability and Tight Junction Regulation
Chronic Kidney Disease
Environmental Enteric Dysfunction
Necrotizing Enterocolitis
Nonalcoholic Steatohepatitis
Crohn’s Disease
Irritable Bowel Syndrome
LARAZOTIDE
(NASH)
Ulcerative Colitis(colonic delivery)
(IBS)
(CKD)
(NEC)
(EED)
Proven in animal model

Courtesy of Elena Verdu, MD, PhD, McMaster University
Paracellular Transport
Lumen
10
Biopharmaceuticals
Phase 3
Gluten + Larazotide
Celiac DiseaseLarazotide / INN-202
• >800 Patients exposed• No systemic exposure• Safety comparable to placebo• Fast Track Designation Granted
H2N
NH2
HN
HN
HN
HN
HN
HN
N
O
O
O
OH
O
OO
O
O
O
Gly-Gly-Val-Leu-Val-Gln-Pro-Gly-OH
8 amino acidsProprietary formulation for small bowel delivery
Transgenic mouse model of CeliacLamina Propria

11
BiopharmaceuticalsPhase 2b / Phase 3: “Real-Life” Clinical Trial Design
1-1-2-3 0 2 3 4 5 6 7 8 9 10 11 12 13Weeks
Visit 1Visit 2
Randomization Visit 3
Visit 4Visit 5
End of Trial Visit
Visit 6
End of Treatment
Screening & Placebo Run-in Period
Placebo TID (12 weeks)
Larazotide TID (12 weeks)
Trial design for Phase 2b (Study ‘012) and Phase 3

12
BiopharmaceuticalsClinically Meaningful Phase 2b Trial (‘012) Results
31%
10% 9% 8% 14%
41%
Target 1550 mg TID
Target 2550 mg TID
Study 1100 mg
Study 2100 mg
Trial 1290 mcg
Trial 2290 mcg
Amitiza 04318 mcg BID
Amitiza 04328 mcg BID14.3%
14.3%Treatment
E�ect
28.6%Drug E�ect
Larazotide
Placebo E�ect
41%
32%
25%
17%
7%
12.1%
5.1%
6% 6%
13.8%
7.8%
13.8%
7.8%
9.7%
12.7%
3%
30%
16%
INN-202
Source: Gastroenterology 2015;148:1311–1319; p. 1315 and FDA Drug Labels
MITT population, n=340Mean on-treatment score (abdominal pain, abdominal cramping, bloating, and gas); p-values derived from CMH testCeD PRO = Celiac Disease Patient Reported Outcome. Primary Endpoint validated for Phase 3.
p = 0.022
CeD PRO - P2b Trial (‘012)
28.6%
14.3%
14.3%
Placebo0%
10%
20%
30%
0.5 mg TID
Treatment E�ect
Source: Gastroenterology 2015;148:1311–1319; p. 1315
Trial powered to 80%

13
BiopharmaceuticalsLarazotide: Development Timeline
GMP Drug Product
EU Partnership
Open Label Extension Safety Study
Phase 3 Trials: 450 pts each
NDA Filing
Phase 3 Trials: 450 pts each
Autoimmune DiseaseEnd of P2 Meeting
IBS-D
Approval & Launch
2017 2018 2019 2020
14
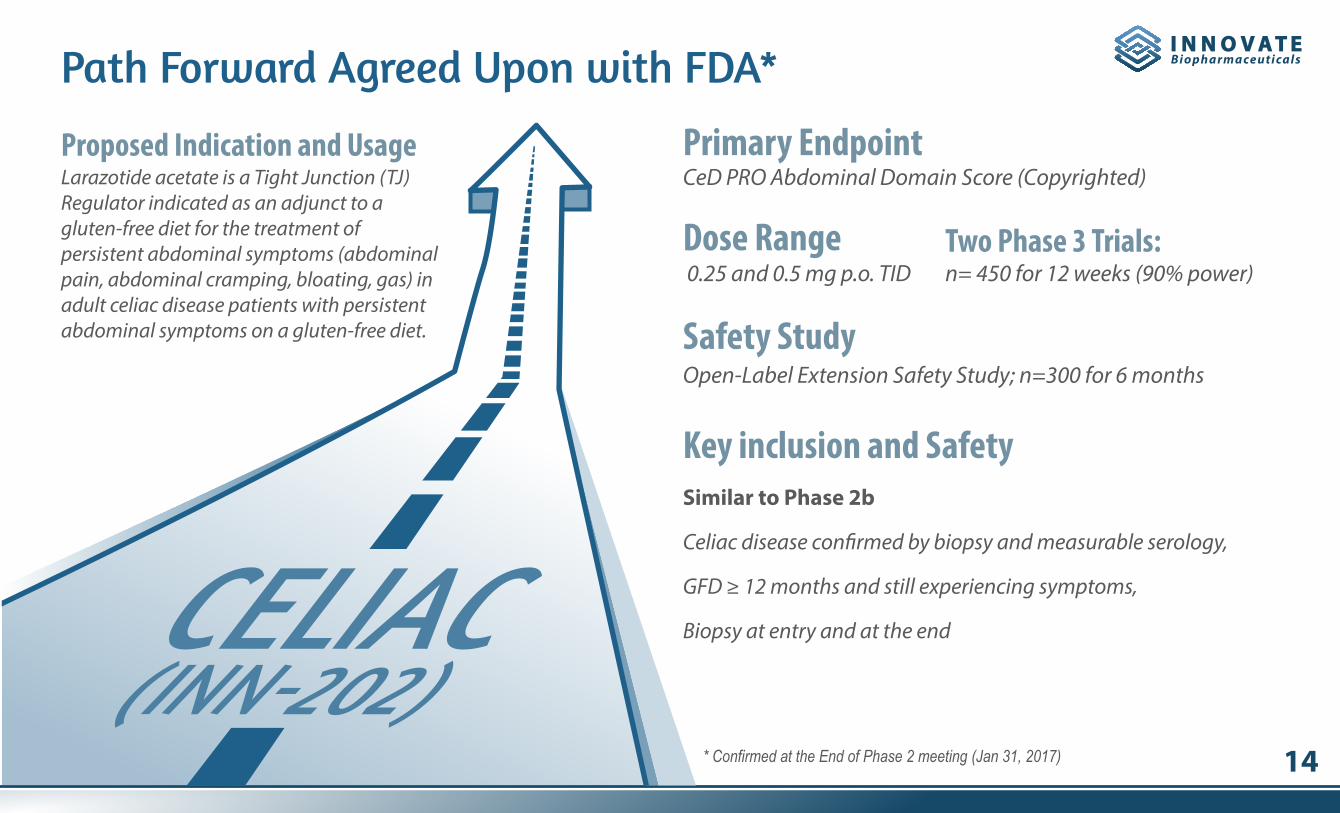
BiopharmaceuticalsPath Forward Agreed Upon with FDA*
Larazotide acetate is a Tight Junction (TJ) Regulator indicated as an adjunct to a gluten-free diet for the treatment of persistent abdominal symptoms (abdominal pain, abdominal cramping, bloating, gas) in adult celiac disease patients with persistent abdominal symptoms on a gluten-free diet.
CeD PRO Abdominal Domain Score (Copyrighted)Proposed Indication and Usage Primary Endpoint
n= 450 for 12 weeks (90% power)Two Phase 3 Trials:
Open-Label Extension Safety Study; n=300 for 6 monthsSafety Study
Similar to Phase 2b
Celiac disease con�rmed by biopsy and measurable serology,
GFD ≥ 12 months and still experiencing symptoms,
Biopsy at entry and at the end
Key inclusion and Safety
0.25 and 0.5 mg p.o. TIDDose Range
* Confirmed at the End of Phase 2 meeting (Jan 31, 2017)

15
BiopharmaceuticalsScientific Advisors: Larazotide (INN-202)
Professor of Medicine, Division of Gastroenterology and Hepatology Mayo Clinic, Rochester, Minnesota
Professor of Medicine, Harvard Medical School, Chief of the Herrman L. Blumgart Internal Medicine Firm, Dir. of Gastroenterology Training and Medical Director of the Celiac Center at BIDMC
Ciaran Kelly, M.D.
Former Chair and Professor of Pediatrics at the University of Tampere and Tampere University Hospital in Finland. Dr. Maki was Secretary-General of the European Society of Pediatric Gastroenterol-ogy, Hepatology and Nutrition (ESPGHAN) from 1997-2000
Markku Mäki, M.D.Professor of Clinical Medicine at the College of Physicians and Surgeons, Columbia University. Director of The Celiac Disease Center at Columbia University
Peter H. Green, M.D.
Joseph A. Murray, M.D.William Rorer Professor of Medicine, Chief of the Division of Gastroenterology and Hepatology at Thomas Je�erson University Hospital, Director, Celiac Center
Anthony Jay DiMarino, M.D.

16
Biopharmaceuticals
Ulcerative ColitisINN-108
Phase 2Our Second Program

17
BiopharmaceuticalsAzo-Bond Creates Stable Pro-Drug w/ Directed Delivery to Colon
Only disassociates in the colon Mesalamine
AZO BOND
5-ASA (mesalamine)4-APAA (Actarit)Inhibits in�ammatory Arachidonicacid metabolic pathways
Sulfasalazine (predecessor of 5-ASA)was initially approved for RA in 1950s
Inhibits pro-in�ammatory cytokines: TNF-α and IL-1
Approved in Japan in 1994 for RA
Decades of safety data
Mesalamine(TRx)
(mesalamine) 1.2gdelayed release tablets
(mesalamine)delayed-release tablets
Pentasamesalamine
(mesalamine, USP)
apriso(mesalamine) 0.375g
EXTENDED RELEASE CAPSULES
Mesalamine Reformulations �+$2Bn in US Sales
Orphan Drug Designation Granted for Pediatric UC

18
Biopharmaceuticals
Surgery
COSTS ($) COSTS ($)
Surgery
Generics
BiologicsAnti-TNFs
BiologicsAnti-TNFs
Most patients are mild to moderate.Branded 5-ASAs go generic *
Payors will put pressure on biologic pricing in spite of biosimilars.
Source: Adapted from Danese S, Siegel CA, Peyrin‐Biroulet L. integrating budesonide‐MMX into treatment algorithms for mild‐to‐moderate ulcerative colitis. Alimentary pharmacology & therapeutics. 2014 May 1;39(10):1095-103.
*The �rst generic launch of a branded mesalamine was by Zydus Cadila on July 19, 2017 of Shire’s Lialda
Generic MesalaminesBranded
Branded ASAsBranded Mesalamines
AZA/6-MP
Mild to Moderate UC
MethotrexateAZA/6-MP
Methotrexate
SteroidsBudesonide-MMX
SteroidsBudesonide-MMX
INN-108 Opportunity

19
Biopharmaceuticals
Sulfasalizine
INN-108
INN-108 Showed Significant Benefit in Animal StudiesToxin A induced Colitis Model in Rats
1 mg/kg
Normal
Toxin A
10 mg/kg 100 mg/kg
1 mg/kg 10 mg/kg 100 mg/kg
Sulfasalazine is a prodrug composed of mesalamine (5-aminosalicylic acid (5-ASA)) linked via an azo-bond to sulfapyridine (a side chain without any therapeutic e�ect).

20
BiopharmaceuticalsINN-108: Development Timeline
GMP ManufacturingEx US Partnerships
Phase 2 Trial
Adult orphanPhase 2b/3 Trial
Phase 2 meeting
2017 2018 2019
21
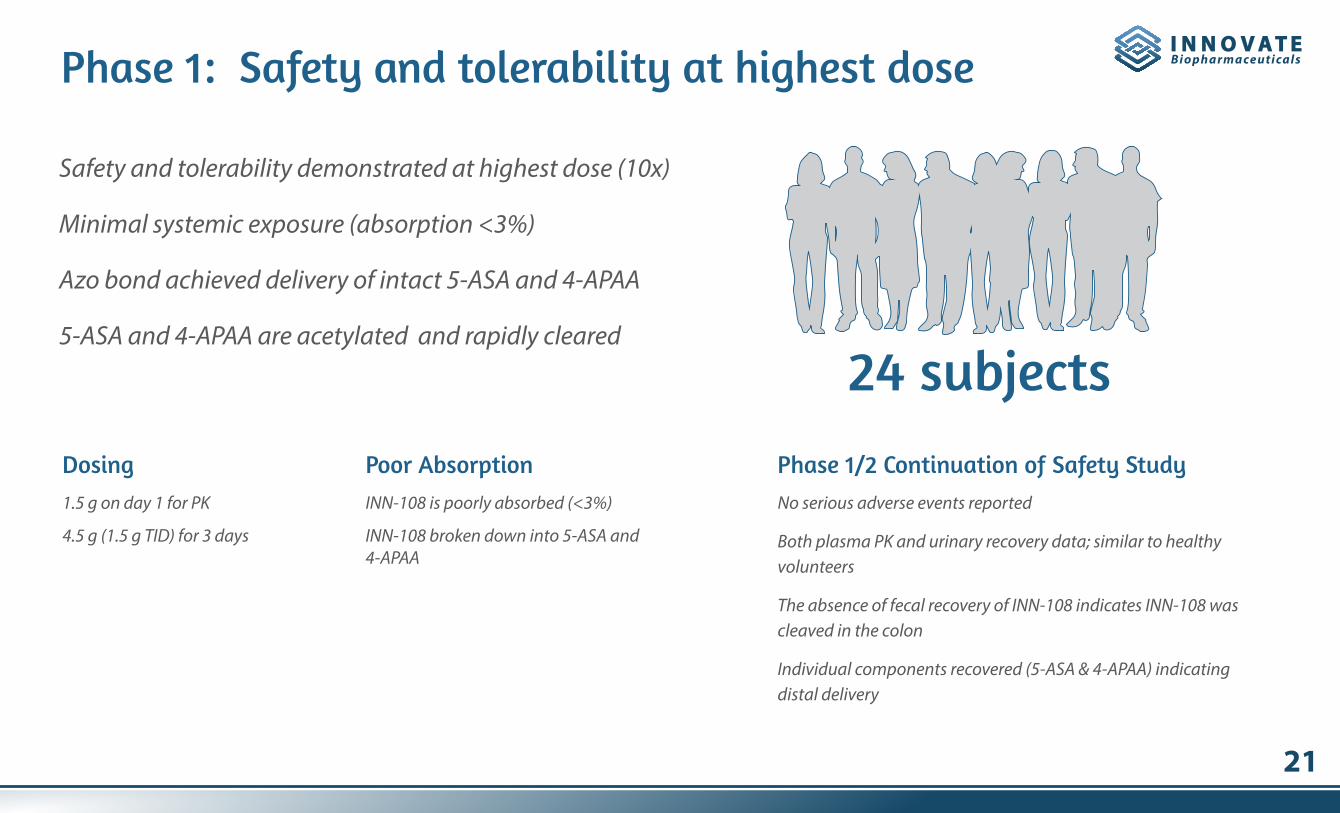
BiopharmaceuticalsPhase 1: Safety and tolerability at highest dose
Dosing Poor Absorption Phase 1/2 Continuation of Safety Study
24 subjects
Safety and tolerability demonstrated at highest dose (10x)
Minimal systemic exposure (absorption <3%)
Azo bond achieved delivery of intact 5-ASA and 4-APAA
5-ASA and 4-APAA are acetylated and rapidly cleared
1.5 g on day 1 for PK
4.5 g (1.5 g TID) for 3 days
INN-108 is poorly absorbed (<3%)
INN-108 broken down into 5-ASA and 4-APAA
No serious adverse events reported
Both plasma PK and urinary recovery data; similar to healthy volunteers
The absence of fecal recovery of INN-108 indicates INN-108 was cleaved in the colon
Individual components recovered (5-ASA & 4-APAA) indicating distal delivery
22
BiopharmaceuticalsScientific Advisory Board: INN-108
William Sandborn, M.D. Roger Liddle, M.D.
Brian Feagan, M.D. Aida Habtezion, M.D., M.Sc.
Assoc. Prof. of Medicine, Div. of Gastroenterology and Hepatology; Vice Chair for Basic and Translational Research. Dr. Lipkin is a board certi�ed Medical Geneticist with a focus on genetic testing for gastrointestinal diseases
Dr. Liddle is currently Professor of Medicine at Duke University Medical Center and former Chief of Division of Gastroenterology. Worked with early development of INN-108
Head of Department of Gastroenterology at UC San Diego. World-recognized thought leader in IBD
Dr. Habtezion is currently an Assistant Professor in the Division of Gastroenterology & Hepatology, and Immunology Program at Stanford University. She is a member of NIH study section and Stanford In�ammatory Bowel Disease Program
Dr. Feagan is a specialist in Internal Medicine, with training in clinical epidemiology and gastroenterology. CEO of Robards Clinical Trial Research Group. World-recognized thought leader in IBD
Steven Lipkin, M.D., PhD

23
BiopharmaceuticalsLeadership Board of Directors
Chief Executive O�cerChris Prior, PhD
Founded and sold Biorexis to P�zer (2001-08)
Sold Principia to Human Genome Sciences (1999-2000)
PhaseBio (2009-2014)
Sano�-Aventis, Biogen
PhD: Columbia University
Post-Doc: Rockefeller Univ.
Reliance Life Sciences
Millipore
Dade Behring
Goodwin
Washing State Univ.
Univ. of Mumbai
Alba Therapeutics
Onyx Pharmaceuticals
Proteolix , VP Operations
Praecis Pharmaceuticals,
VP, Alkermes
Amgen Subsidiary
Jay P. MadanGary Musso, PhDPresident & Corp DevelopmentCMC
CMO, AstraZeneca/ZS Pharma,
Head Clinical Dev., Novo Nordisk
Advisor/CMO, Genvec, Nabi Pharma, Alba Therapeutics
Henrik Rasmussen, MD, PhDChief Medical O�cer Director
Lorin Johnson, PhD
Sandeep “Steve” Laumas, MDDirector
Rose CraneDirector
Bearing Circle Capital
North Sound Capital
Goldman Sachs
Yale School of Medicine
Dana-Farber Cancer Institute
Albany Medical College
Cornell University
Founder, Salix Pharmaceuticals
Salix sold to Valeant (2015) for $16 B
Chief Scientist at California Biotechnology (Scios)
Stanford University School of Medicine and UCSF
Member, Board of Directors: Teva Pharmaceutical (Israel)Zealand Pharma (Denmark)
Group Chair, J&J
Head Primary Care, Bristol-Myer Squibb
Epocrates (Former CEO) and Mela Biosciences

24
Biopharmaceuticals
S I G N I F I C A N T A P P E T I T E F O R N E W P R O D U C T S
Nestle Health & Sciences Publicly announced that they want to be the
largest player in GI by 2020
IBD Blockbuster: Entyvio
Former world-class GI franchise with PPI Drugs
$25 Bn
$1 Bn
$3 Bn
$16 Bn
$3 Bn
$7 Bn
$3 Bn$5 Bn
World-class GI franchise with Remicade

25
Biopharmaceuticals
Focused on Autoimmune and In�ammatory Diseases
8480 Honeycutt Road, Suite 200 | Raleigh NC 27615 | Tel: (919) 275-1933 | [email protected] | www.innovatebiopharma.com

26
Biopharmaceuticals
Appendix

27
Biopharmaceuticals
Tall Villi Flattened Villi Lymphocyte In�ltration
Shallow Crypts
“Crypt Hyperplasia”
* Rubio-Tapia A, Rahim MW, See JA, Lahr BD, Wu TT, Murray JA. Mucosal recovery and mortality in adults with celiac disease after treatment with a gluten-free diet. The American journal of gastroenterology. 2010 Jun 1;105(6):1412-20.
Long Crypts
Celiac Disease patients have �attened villi
Celiac Disease �attened villi, areas of IELs in�ltrate and crypt hyperplasia
After starting on a Gluten Free Diet (GFD) it takes several years to recover the normal villi architecture
Even after 5 years on a GFD, up to 1/3 of patients continue to show histology characteristic of Celiac Disease *
Histological improvement is a variable and long-term measure of recovery
Urgent need for symptoms relief
Endoscopy
Healthy Celiac Disease
Normal Celiac Disease
Histology

28
BiopharmaceuticalsPrimary Endpoint Confirmed For Phase 3 Trials
* Confirmed at the End of Phase 2 meeting (Jan 31, 2017)** CeD PRO is copyrighted for 99 years and is the only validated Celiac Disease endpoint
A patient with at least a 50% reduction from baseline in weekly mean CeD PRO** Abdominal Domain score in at least 6 out of 12 weeks
Agreed Upon Primary Endpoint *
Comprised of the 4 abdominal symptoms: abdominal pain,
abdominal cramping, bloating, and gas
Calculated by adding the 4 individual abdominal
symptom scores and dividing them by 4
Is the weekly average of the 7 daily diary scores for each
patient
Has a range of “0” to “10” with higher scores, indicating
greater symptom severity

29
Biopharmaceuticals
2 mg
1 mg
0.5 mg
15 mins 30 mins
Dos
e Act
ivit
y
Time 0.5 mg 1 mg 2 mg Dose
Higher a�nity AP selectively saturates local binding sites
AP: Active (Intact) PeptideIP: Inactive (Degraded) Peptide
IP acts as an inhibitor by displacing AP at a threshold concentration ~1mg. Excess AP IP
Threshold [IP]
[IP] acts as inhibitor and displaces IP
Graph of vs. Dose
[AP][IP]
[AP][IP]
Graph of vs. Activity[AP][IP]
= 1 [AP][IP]
= 0.5 [AP][IP]
= 0.25
Potential PK Model for Larazotide’s Mechanism of Action