future dimensions - clinical nutrition management dpg winter... · 2015-02-12 · dpg was selected...
TRANSCRIPT
Inside this issue:
CPE (1) Article:
Malnutrition in
Acute Care:
Diagnosis, Docu-
mentation and
Reimbursement
Impact
3-10
Key Information
Related to
Long-Term Care
and F 325
11-15
CNM DPG
Updates 16-17
Featured
Member 18-19
CNM Executive
Committee 20
Greetings Colleagues!
This year seems to be flying by –
hopefully, most of you are seeing
signs of Spring approaching along
with a feeling of renewal. These
are exciting times to be a nutri-
tion leader as we make significant
contributions to the changing
landscape of healthcare. You are
making a difference each and
every day in how our profession is
perceived and the impact we can
have on the quality of individual
lives as well as healthcare eco-
nomics.
We are making great strides in
accomplishing the objectives set
forth in our strategic plan. Some
of the recent and notable suc-
cesses include the establishment
of our first Quality and Process
Improvement Project Award and
poster submissions for display at
the annual symposium. Kudos to
Sherri Jones and Cindy Hamilton
for their efforts to bring this to
fruition!
Special recognition should also
go to our Research Committee lead by Susan DeHoog and Bar-
bara Isaacs-Jordan for their tire-
less efforts to complete the first
phase of our staffing and produc-
tivity study. They not only pre-
sented the results at FNCE but
will pursue a pilot project to de-
termine how we can apply these
findings towards the develop-
ment of a user friendly tool. We
can all be proud that our CNM
DPG was selected by the Acad-
emy to assist in developing this
much sought after tool for man-
agers, directors and hospital ad-
ministrators.
You also may have noticed en-
hancements to our website and
social media utilization with addi-
tional tools, resources and search
capabilities – thanks to Barb
Pyper and Janel Welch for staying
on top of this.
Also, as I am sure you know, reg-
istration for our Annual Sympo-
sium is open and the agenda is
PACKED with excellent and
timely topics and extraordinary speakers. This is our very first
Future Dimensions
In Clinical Nutrition Practice
A Message From the Chair Winter, 2015
Volume 34, No 1
Kathy Allen, MA, RD, CSO
Chair, CNM DPG
2014-2015
Like us on Facebook! https://www.facebook.c
om/ClinicalNutritionMan
agementDpg
Complete the member survey and
you could win a $25 gift card!
https://www.surveymonkey.com/s/CNM2015svy.

2
Future Dimensions in Clinical Nutrition Practice Winter 2015
symposium in the northwest. Please be sure to
check out the location and program and share it
with your colleagues.
Last but not least --- PLEASE complete the mem-
ber survey. Your input is extremely valuable to
us. Our main objective as your leadership team is
to serve you, our members, to the best of our
abilities. We cannot do this without your input.
This year, you will have the to opportunity to cast
your vote for a potential DPG name change. https://www.surveymonkey.com/s/CNM2015svy
Warmest Regards,
Kathy
3
Future Dimensions in Clinical Nutrition Practice Winter 2015
Malnutrition in Acute Care: Diagnosis,
Documentation and Reimbursement Impact By Alicia Taub, MS, MBA, RDN, CNSC and Holly Guzman, RDN, CSP, CNSC
Protein Calorie Malnutrition (PCM), a condition
present on admission or that develops during
hospitalization, is associated with many adverse
outcomes. Increased risk of infection,1,2
delayed
wound healing,3,4
and extended hospitaliza-
tions5,6
are all known outcomes associated with
malnutrition. Early identification and treatment
of malnutrition can attenuate these outcomes7
and, as the expert in the nutritional care of pa-
tients, it is incumbent upon the Registered Dieti-
tian Nutritionist (RDN) to identify, document and
treat malnutrition within the RDN’s scope of
practice.
The RDN’s comprehensive nutrition assessment
includes the collection of data needed to deter-
mine the patient’s nutritional status. Whether a
patient is found to be adequately nourished or
malnourished, this determination is necessary to
lay the foundation for the plan of care. Based on
the signs and symptoms collected in the nutrition
assessment, the appropriate nutrition diagnosis
is identified and documented using the Interna-
tional Dietetics and Nutrition Terminology
(IDNT).8 In the case of malnutrition, the criteria
established by The Academy of Nutrition and
Dietetics (Academy) and the American Society
for Parenteral and Enteral Nutrition (ASPEN),9
along with clinical judgment, assist the RDN in
selecting the nutrition diagnosis for malnutrition
consistent with the signs and symptoms.
Although the RDN is the expert in nutrition, it is
still the responsibility of the physician to make
the medical diagnosis of malnutrition, as only the
medical diagnoses are coded by documentation
specialists. The physician’s diagnosis is the medi-
cal diagnosis of malnutrition and the RDN’s diag-
nosis is the nutritional diagnosis of malnutrition.
As a member of the healthcare team, the RDN
should share his or her nutritional diagnosis of
malnutrition and plan of care with the physician
so these findings and interventions are consid-
ered when medical diagnoses are made.
The medical diagnosis of malnutrition by the
physician can impact reimbursement. In some
cases, the diagnosis of malnutrition can alter the
final Diagnosis Related Group (DRG) which, de-
pending on the insurer, can increase reimburse-
ment.10
Also, the diagnosis of malnutrition,
along with all other diagnoses, has the ability to
impact Case Mix Index (CMI), a measure of the
severity of illness of the patient population.
The purpose of this article is to:
1. Describe the steps implemented by the clini-
cal nutrition team at St. John Hospital and
Medical Center (SJHMC) in Detroit, MI, in di-
agnosing and documenting malnutrition util-
izing the most current guidelines and tools;
2. Share the impact of RDN malnutrition diag-
nosis on physician medical diagnosis of mal-
nutrition; and
3. Review the revenue impact of the medical
malnutrition diagnosis both in terms of:
a. Revenue realized due to inclusion of
medical malnutrition diagnosis; and
b. Revenue not realized due to omission of
medical malnutrition diagnosis.
RDN Diagnosis of Malnutrition
In the spring of 2013, RDNs at SJHMC were
trained in the Nutrition Focused Physical Assess-
ment (NFPA) portion of the nutrition assessment.
This process began with viewing the following
webinars:
• Nutrition-Focused Physical Examination: En-
hancing Your Clinical Toolbox by W. James
Brewer, DCN, RD, CNSD and Sara Perdue, MS,
RD, CSG, LD. February 28, 2013.
• Applying Academy/ASPEN Guidelines to Iden-
tify and Document Adult Malnutrition: A
Change in Practice by Cynthia Hamilton, MS,
RD, LD and Robert DeChicco, MS, RD, LD,
CNSC. March 21, 2013.

4
Future Dimensions in Clinical Nutrition Practice
These videos set the foundation for understand-
ing the steps in completing the NFPA and the im-
portance of incorporating these criteria in the
diagnosis of malnutrition. The next step was
hands-on physical assessment training by our
senior nutrition support dietitian who was
trained in NFPA (Nancy Park, MS, RD, CNSC). Our
physician nutrition champion also served as a
mentor in this training (Dr. Thomas E. Knuth, MD,
MPH, FACS, CNSC). The training process involved
direct hands-on demonstration for evaluating
muscle mass, fat mass and edema. RDNs were
required to observe the physical assessment
process a few times and demonstrate compe-
tency via return demonstration.
Our RDN Nutrition Assessment Form was modi-
fied to include an area under “Clinical Findings”
to document the results from the NFPA. A mal-
nutrition pocket guide was developed as a handy
reference tool for the RDN to use when complet-
ing nutrition assessments. This tool included: 1)
markers of inflammation to determine the con-
text of malnutrition, 2) physical markers describ-
ing degrees of depletion for muscle and fat mass
and for levels of edema, and 3) criteria for diag-
nosing malnutrition and degree of severity. The
tool also included examples for writing Problem-
Etiology-Signs/Symptoms (PES) statements incor-
porating the type and degree of malnutrition.
RDNs recorded on their work logs the name and
financial identification number (FIN) of all pa-
tients seen on a daily basis. These logs were
modified to allow the RDN to include the nutri-
tional diagnosis of malnutrition (moderate or se-
vere) if the patient met the criteria. Following
each fiscal quarter, all dietitian logs were re-
viewed and each patient with a nutritional diag-
nosis of malnutrition was placed on a master list.
This list was then used to evaluate the reim-
bursement impact, both realized (optimization
achieved due to the inclusion of medical diagno-
sis of malnutrition) and not realized (optimization
missed due to exclusion of medical diagnosis of malnutrition) on cases with RDN intervention.
Documentation of Malnutrition using IDNT
Documentation of malnutrition, moderate or se-
vere, and in which context (social / environ-
mental or illness related – acute or chronic), was
designed using the IDNT PES format. For patients
with Severe Malnutrition, IDNT problem Malnu-
trition (Nutrition Intake - NI – 5.2) was used. For
patients with Moderate Malnutrition, IDNT prob-
lem Inadequate Protein-Energy Intake (NI – 5.3)
was used. Different nutrition diagnoses were
used because the signs and symptoms listed for
each of these nutrition problems corresponded
more closely to the criteria for the malnutrition
diagnosis.9 In creating the PES statement, the
RDN included all signs and symptoms gathered in the nutrition assessment that supported the di-
agnosis of malnutrition. An example of docu-
mentation of the nutrition diagnosis of severe
malnutrition follows:
Malnutrition (NI-5.2) (May have Severe Pro-
tein-Calorie Malnutrition in the context of
chronic illness) related to increased energy
expenditure second to chronic catabolic ill-
ness and altered GI function as evidenced by
underweight status indicated by BMI = 18.4,
severe weight loss of 12% x 3-4 Months ( -
8.2 kg x 3-4 months), poor PO intake <50-
75% of estimated needs x 3-4 months, poor
appetite, chronic colitis, abdominal pain, di-
arrhea, colon CA on chemotherapy, severe
subcutaneous fat and severe muscle wasting
identified as evidenced by very apparent de-
pression between ribs, prominent acromion
process and bilateral depression muscle on
thighs with prominent bones around knees
per RDN physical assessment
Understanding Reimbursement for Hospitals11,12
Medicare, the primary insurer of hospitalized pa-
tients, pays providers via Medicare’s Inpatient
Prospective Payment System (IPPS), which util-
izes the Medicare Severity Diagnosis Related
Groups (MS-DRG) for reimbursement. Medicaid
also uses the same reimbursement system, as do
many other third party payers. Therefore, it is
important to understand how MS-DRGs are de-
signed with the International Classification of Dis-
Winter 2015
5
eases, Ninth Revision, Clinical Modification (ICD-
9-CM) codes in order to understand how a diag-
nosis of malnutrition can impact reimbursement.
ICD-9-CM Codes
ICD-9-CM is based on the World Health Organiza-
tion's Ninth Revision, International Classification
of Diseases (ICD-9). ICD-9-CM is the official sys-
tem of assigning codes to diagnoses and proce-
dures associated with hospital utilization in the
United States. ICD-9-CM codes are divided into
three groups based on severity of illness:
• Major Complication/Co-Morbidity (MCC),
reflecting the highest level of severity and
requiring the highest level of resource use;
• Complication/Co-Morbidity (CC), next
level of severity and less resource use;
and
• Non-CC, not expected to significantly af-
fect severity of illness and resource use.
MS-DRG Codes
Each MS-DRG is denoted by a number and each
inpatient hospital discharge is assigned one MS-
DRG. Assignment of the DRG is based on princi-
ple diagnosis and additional diagnoses, principle
and additional procedures, gender and discharge
status.
MS-DRGs are grouped together based on princi-
pal diagnosis and then subdivided into one, two
or three groups based on secondary diagnosis,
although most are divided into three groups.
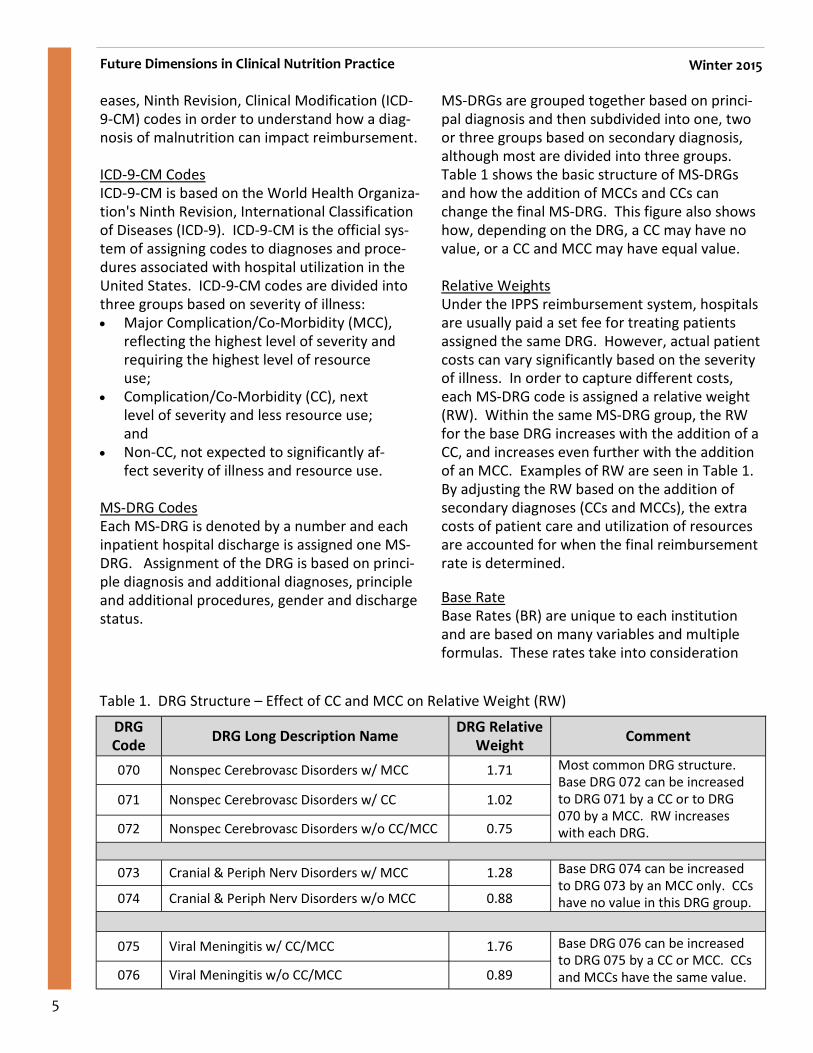
Table 1 shows the basic structure of MS-DRGs
and how the addition of MCCs and CCs can
change the final MS-DRG. This figure also shows
how, depending on the DRG, a CC may have no
value, or a CC and MCC may have equal value.
Relative Weights
Under the IPPS reimbursement system, hospitals
are usually paid a set fee for treating patients
assigned the same DRG. However, actual patient
costs can vary significantly based on the severity of illness. In order to capture different costs,
each MS-DRG code is assigned a relative weight
(RW). Within the same MS-DRG group, the RW
for the base DRG increases with the addition of a
CC, and increases even further with the addition
of an MCC. Examples of RW are seen in Table 1.
By adjusting the RW based on the addition of
secondary diagnoses (CCs and MCCs), the extra
costs of patient care and utilization of resources
are accounted for when the final reimbursement
rate is determined.
Base Rate
Base Rates (BR) are unique to each institution
and are based on many variables and multiple
formulas. These rates take into consideration
Future Dimensions in Clinical Nutrition Practice Winter 2015
DRG
Code DRG Long Description Name
DRG Relative
Weight Comment
070 Nonspec Cerebrovasc Disorders w/ MCC 1.71 Most common DRG structure.
Base DRG 072 can be increased
to DRG 071 by a CC or to DRG
070 by a MCC. RW increases
with each DRG.
071 Nonspec Cerebrovasc Disorders w/ CC 1.02
072 Nonspec Cerebrovasc Disorders w/o CC/MCC 0.75
073 Cranial & Periph Nerv Disorders w/ MCC 1.28 Base DRG 074 can be increased
to DRG 073 by an MCC only. CCs
have no value in this DRG group. 074 Cranial & Periph Nerv Disorders w/o MCC 0.88
075 Viral Meningitis w/ CC/MCC 1.76 Base DRG 076 can be increased
to DRG 075 by a CC or MCC. CCs
and MCCs have the same value. 076 Viral Meningitis w/o CC/MCC 0.89
Table 1. DRG Structure – Effect of CC and MCC on Relative Weight (RW)
6
operating and capital expenses and are adjusted
for geographic region, local market labor costs,
indigent care, use of technologies, resident train-
ing and medical education programs. In essence,
the BR is the reimbursement a hospital would
receive for treating the average patient. The BR
for each insurer differs; Medicare’s BR is differ-
ent from Medicaid’s BR which is different from
other insurers’ BRs.
MS-DRG Reimbursement
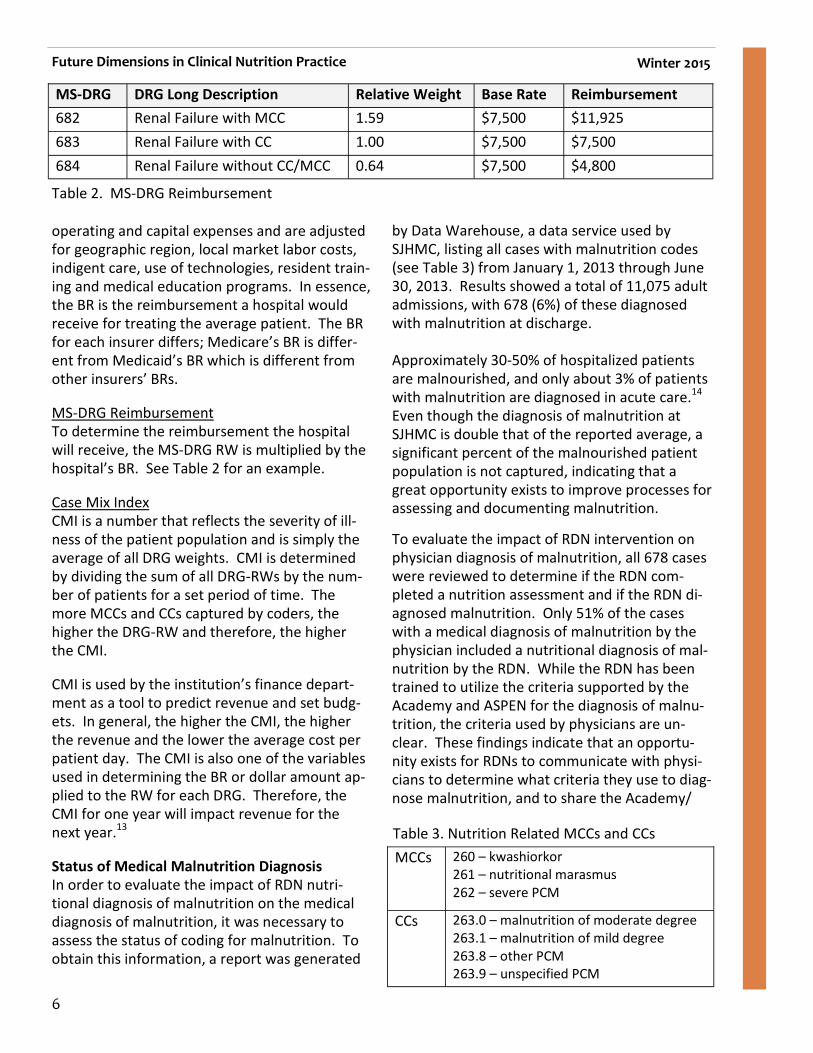
To determine the reimbursement the hospital
will receive, the MS-DRG RW is multiplied by the
hospital’s BR. See Table 2 for an example.
Case Mix Index
CMI is a number that reflects the severity of ill-
ness of the patient population and is simply the
average of all DRG weights. CMI is determined
by dividing the sum of all DRG-RWs by the num-
ber of patients for a set period of time. The
more MCCs and CCs captured by coders, the
higher the DRG-RW and therefore, the higher
the CMI.
CMI is used by the institution’s finance depart-
ment as a tool to predict revenue and set budg-
ets. In general, the higher the CMI, the higher
the revenue and the lower the average cost per
patient day. The CMI is also one of the variables
used in determining the BR or dollar amount ap-
plied to the RW for each DRG. Therefore, the
CMI for one year will impact revenue for the
next year.13
Status of Medical Malnutrition Diagnosis
In order to evaluate the impact of RDN nutri-
tional diagnosis of malnutrition on the medical
diagnosis of malnutrition, it was necessary to
assess the status of coding for malnutrition. To
obtain this information, a report was generated
by Data Warehouse, a data service used by
SJHMC, listing all cases with malnutrition codes
(see Table 3) from January 1, 2013 through June
30, 2013. Results showed a total of 11,075 adult
admissions, with 678 (6%) of these diagnosed
with malnutrition at discharge.
Approximately 30-50% of hospitalized patients
are malnourished, and only about 3% of patients
with malnutrition are diagnosed in acute care.14
Even though the diagnosis of malnutrition at
SJHMC is double that of the reported average, a
significant percent of the malnourished patient
population is not captured, indicating that a
great opportunity exists to improve processes for assessing and documenting malnutrition.
To evaluate the impact of RDN intervention on
physician diagnosis of malnutrition, all 678 cases
were reviewed to determine if the RDN com-
pleted a nutrition assessment and if the RDN di-
agnosed malnutrition. Only 51% of the cases
with a medical diagnosis of malnutrition by the
physician included a nutritional diagnosis of mal-
nutrition by the RDN. While the RDN has been trained to utilize the criteria supported by the
Academy and ASPEN for the diagnosis of malnu-
trition, the criteria used by physicians are un-
clear. These findings indicate that an opportu-
nity exists for RDNs to communicate with physi-
cians to determine what criteria they use to diag-
nose malnutrition, and to share the Academy/
Future Dimensions in Clinical Nutrition Practice Winter 2015
MS-DRG DRG Long Description Relative Weight Base Rate Reimbursement
682 Renal Failure with MCC 1.59 $7,500 $11,925
683 Renal Failure with CC 1.00 $7,500 $7,500
684 Renal Failure without CC/MCC 0.64 $7,500 $4,800
Table 2. MS-DRG Reimbursement
MCCs 260 – kwashiorkor
261 – nutritional marasmus
262 – severe PCM
CCs 263.0 – malnutrition of moderate degree
263.1 – malnutrition of mild degree
263.8 – other PCM
263.9 – unspecified PCM
Table 3. Nutrition Related MCCs and CCs
7
ASPEN criteria to improve consistency in the di-
agnosis and documentation of malnutrition.
The 678 cases with a malnutrition diagnosis were
evaluated to determine if the final DRG was opti-
mized (changed to a higher weighted DRG in the
same group) by malnutrition coding and, in the
cases that were optimized, if the RDN’s nutrition assessment included the nutritional diagnosis of
malnutrition.
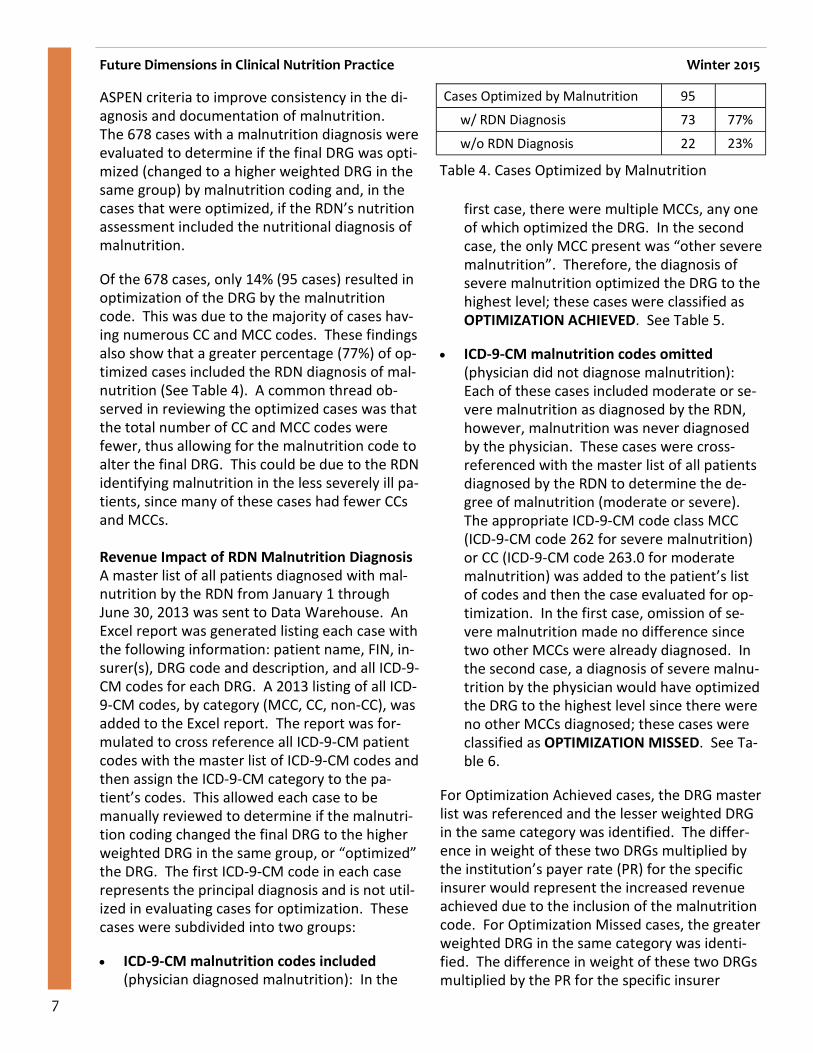
Of the 678 cases, only 14% (95 cases) resulted in
optimization of the DRG by the malnutrition
code. This was due to the majority of cases hav-
ing numerous CC and MCC codes. These findings
also show that a greater percentage (77%) of op-
timized cases included the RDN diagnosis of mal-
nutrition (See Table 4). A common thread ob-
served in reviewing the optimized cases was that
the total number of CC and MCC codes were
fewer, thus allowing for the malnutrition code to
alter the final DRG. This could be due to the RDN
identifying malnutrition in the less severely ill pa-
tients, since many of these cases had fewer CCs
and MCCs.
Revenue Impact of RDN Malnutrition Diagnosis
A master list of all patients diagnosed with mal-nutrition by the RDN from January 1 through
June 30, 2013 was sent to Data Warehouse. An
Excel report was generated listing each case with
the following information: patient name, FIN, in-
surer(s), DRG code and description, and all ICD-9-
CM codes for each DRG. A 2013 listing of all ICD-
9-CM codes, by category (MCC, CC, non-CC), was
added to the Excel report. The report was for-
mulated to cross reference all ICD-9-CM patient
codes with the master list of ICD-9-CM codes and
then assign the ICD-9-CM category to the pa-
tient’s codes. This allowed each case to be
manually reviewed to determine if the malnutri-
tion coding changed the final DRG to the higher
weighted DRG in the same group, or “optimized”
the DRG. The first ICD-9-CM code in each case
represents the principal diagnosis and is not util-
ized in evaluating cases for optimization. These
cases were subdivided into two groups:
• ICD-9-CM malnutrition codes included (physician diagnosed malnutrition): In the
first case, there were multiple MCCs, any one
of which optimized the DRG. In the second
case, the only MCC present was “other severe
malnutrition”. Therefore, the diagnosis of
severe malnutrition optimized the DRG to the
highest level; these cases were classified as
OPTIMIZATION ACHIEVED. See Table 5.
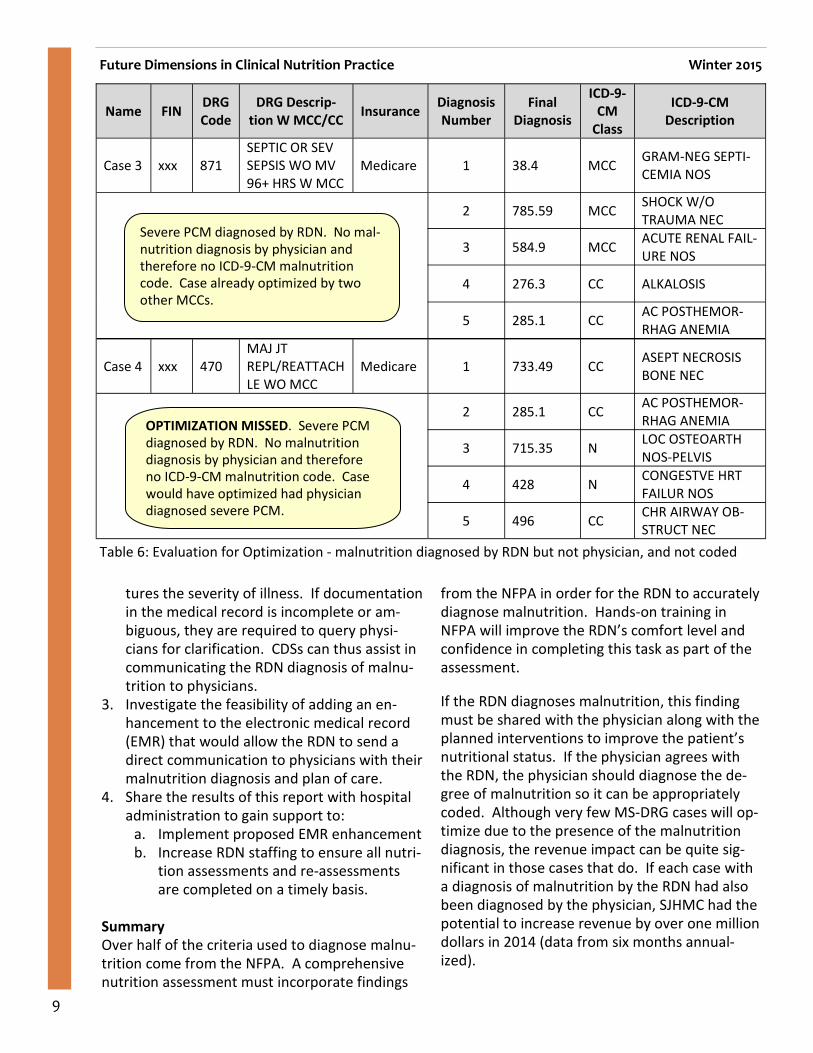
• ICD-9-CM malnutrition codes omitted
(physician did not diagnose malnutrition):
Each of these cases included moderate or se-
vere malnutrition as diagnosed by the RDN,
however, malnutrition was never diagnosed
by the physician. These cases were cross-
referenced with the master list of all patients
diagnosed by the RDN to determine the de-
gree of malnutrition (moderate or severe).
The appropriate ICD-9-CM code class MCC
(ICD-9-CM code 262 for severe malnutrition)
or CC (ICD-9-CM code 263.0 for moderate
malnutrition) was added to the patient’s list
of codes and then the case evaluated for op-
timization. In the first case, omission of se-
vere malnutrition made no difference since
two other MCCs were already diagnosed. In
the second case, a diagnosis of severe malnu-
trition by the physician would have optimized the DRG to the highest level since there were
no other MCCs diagnosed; these cases were
classified as OPTIMIZATION MISSED. See Ta-
ble 6.
For Optimization Achieved cases, the DRG master
list was referenced and the lesser weighted DRG
in the same category was identified. The differ-
ence in weight of these two DRGs multiplied by
the institution’s payer rate (PR) for the specific
insurer would represent the increased revenue
achieved due to the inclusion of the malnutrition
code. For Optimization Missed cases, the greater
weighted DRG in the same category was identi-
fied. The difference in weight of these two DRGs
multiplied by the PR for the specific insurer
Future Dimensions in Clinical Nutrition Practice Winter 2015
Cases Optimized by Malnutrition 95
w/ RDN Diagnosis 73 77%
w/o RDN Diagnosis 22 23%
Table 4. Cases Optimized by Malnutrition

8
Future Dimensions in Clinical Nutrition Practice Winter 2015
would represent the revenue missed due to the
exclusion of the malnutrition code.
Financial analysis of revenue can be determined
by multiplying changes in DRG weights by the PR.
However, cases were not limited to Medicare
and Medicaid patients but included all patients
regardless of insurer. Many commercial insurers
also utilize the MS-DRG reimbursement system
but these third party payers frequently have ex-
ceptions in their contracts that may cap reim-
bursement based on certain criteria. Therefore,
revenue data based on Optimization Achieved
and Optimization Missed cases were determined
by financial analysts on a case-by-case basis al-
lowing for insurer contracts and caveats within the MS-DRG system to be included. The reim-
bursement impact, both Achieved and Missed,
for RDN cases for the 1st
and 2nd
quarters of 2013
are summarized in Tables 7 and 8 (page 10).
Of the 985 cases diagnosed with malnutrition by
the RDN, only 275 were coded, or 28%. Of these,
44 cases optimized the DRG, yielding increased
reimbursement of $296,464 (annualized:
$592,928). Of the 710 cases not coded, 120
cases would have optimized if malnutrition had
been diagnosed by the physician, yielding in-
creased reimbursement of $539,659 (annualized:
$1,079,319). Overall, RDN intervention in malnu-
trition diagnosis and documentation represented
an increase in annualized reimbursement of up to
$1,672,247, of which only 35% was realized.
Plans for Improvement
1. Ensure the diagnosis of malnutrition is consis-
tent between the RDN and physician by edu-
cating physicians on the criteria established by the Academy/ASPEN.
2. Ensure Clinical Documentation Specialists
(CDS) are familiar with Academy/ASPEN crite-
ria for malnutrition diagnosis and RDN docu-
mentation in the medical record. CDSs are
employed by hospitals to review the medical
record and ensure that documentation cap-
Name FIN DRG
Code
DRG Descrip-
tion W MCC/CC Insurance
Diagnosis
Number
Final
Diagnosis
ICD-
9-CM
Class
ICD-9-CM
Description
Case 1 xxx 871
SEPTIC OR SEV
SEPSIS WO MV
96+ HRS W MCC
Medicare 1 38.9 MCC SEPTICEMIA NOS
2 486 MCC PNEUMONIA,
ORGANISM NOS
3 262.00 MCC OTH SEVERE
MALNUTRITION
4 707.23 MCC PRESSURE ULCER
STAGE III
5 204.1 CC CHR LYMPH LEUK
NO REMISS
Case 2 xxx 329
MAJ SML & LG
BOWEL PX W
MCC
Medicare 1 560 CC INTUSSUSCEP-
TION
2 262.00 MCC OTH SEVERE
MALNUTRITION
3 518 CC PULMONARY
COLLAPSE
4 511.9 CC PLEURAL EFFU-
SION NOS
5 V85.22 N BD MS INDX
26.0-26.9 ADL
Table 5: Evaluation for Optimization - malnutrition diagnosed by RDN and physician, and coded
ICD-9-CM 262.0 - Severe PCM is one
of many MCC codes. DRG can be opti-
mized by any MCC.
OPTIMIZATION ACHIEVED. ICD-9-CM
262.0 - Severe PCM is the ONLY MCC
and is responsible for optimization of
DRG.
9
Future Dimensions in Clinical Nutrition Practice Winter 2015
tures the severity of illness. If documentation
in the medical record is incomplete or am-
biguous, they are required to query physi-
cians for clarification. CDSs can thus assist in
communicating the RDN diagnosis of malnu-
trition to physicians.
3. Investigate the feasibility of adding an en-
hancement to the electronic medical record
(EMR) that would allow the RDN to send a
direct communication to physicians with their
malnutrition diagnosis and plan of care.
4. Share the results of this report with hospital
administration to gain support to:
a. Implement proposed EMR enhancement
b. Increase RDN staffing to ensure all nutri-tion assessments and re-assessments
are completed on a timely basis.
Summary
Over half of the criteria used to diagnose malnu-
trition come from the NFPA. A comprehensive
nutrition assessment must incorporate findings
from the NFPA in order for the RDN to accurately
diagnose malnutrition. Hands-on training in
NFPA will improve the RDN’s comfort level and
confidence in completing this task as part of the
assessment.
If the RDN diagnoses malnutrition, this finding
must be shared with the physician along with the
planned interventions to improve the patient’s
nutritional status. If the physician agrees with
the RDN, the physician should diagnose the de-
gree of malnutrition so it can be appropriately
coded. Although very few MS-DRG cases will op-
timize due to the presence of the malnutrition
diagnosis, the revenue impact can be quite sig-
nificant in those cases that do. If each case with
a diagnosis of malnutrition by the RDN had also
been diagnosed by the physician, SJHMC had the
potential to increase revenue by over one million
dollars in 2014 (data from six months annual-
ized).
Name FIN DRG
Code
DRG Descrip-
tion W MCC/CC Insurance
Diagnosis
Number
Final
Diagnosis
ICD-9-
CM
Class
ICD-9-CM
Description
Case 3 xxx 871
SEPTIC OR SEV
SEPSIS WO MV
96+ HRS W MCC
Medicare 1 38.4 MCC GRAM-NEG SEPTI-
CEMIA NOS
2 785.59 MCC SHOCK W/O
TRAUMA NEC
3 584.9 MCC ACUTE RENAL FAIL-
URE NOS
4 276.3 CC ALKALOSIS
5 285.1 CC AC POSTHEMOR-
RHAG ANEMIA
Case 4 xxx 470
MAJ JT
REPL/REATTACH
LE WO MCC
Medicare 1 733.49 CC ASEPT NECROSIS
BONE NEC
2 285.1 CC AC POSTHEMOR-
RHAG ANEMIA
3 715.35 N LOC OSTEOARTH
NOS-PELVIS
4 428 N CONGESTVE HRT
FAILUR NOS
5 496 CC CHR AIRWAY OB-
STRUCT NEC
Table 6: Evaluation for Optimization - malnutrition diagnosed by RDN but not physician, and not coded
Severe PCM diagnosed by RDN. No mal-
nutrition diagnosis by physician and
therefore no ICD-9-CM malnutrition
code. Case already optimized by two
other MCCs.
OPTIMIZATION MISSED. Severe PCM
diagnosed by RDN. No malnutrition
diagnosis by physician and therefore
no ICD-9-CM malnutrition code. Case
would have optimized had physician
diagnosed severe PCM.

10
Future Dimensions in Clinical Nutrition Practice Winter 2015
Cases Jan - Mar Apr - Jun
Submitted by RDNs 477 508
Coded *
ICD-9-CM Code 262 70 98
ICD-9-CM Code 263.9 52 55
Total 122 153
Optimized by Malnutrition 19 25
Revenue $128,780 $167,683
RDNs are the experts in nutrition and have the
tools to assess patients and diagnose malnutri-
tion. Communicating their findings and interven-
tions with physicians can improve patient out-
comes and the medical diagnosis of malnutrition.
Coders can then apply the appropriate ICD-9-CM
codes for malnutrition. Documenting all cases of
malnutrition can significantly increase revenue as
was demonstrated in the review of medical re-
port for wound-healing patients. Am J Surg.
2004;188(1A Suppl):52-56.
5. Braunschweig C, Gomez S, Sheean PM. Impact
of declines in nutritional status on outcomes in
adult patients hospitalized for more than 7
days. J Am Diet Assoc. 2000; 100(11):1316-
1322.
6. Neumayer LA, Smout RJ, Horn HG, Horn SD.
Early and sufficient feeding reduces length of
stay and charges in surgical patients. J Surg Res.
2001;95(1):73-77.
7. Somanchi M, Tao X, Mullin GE. The facilitated
early enteral and dietary management effec-
tiveness trial in hospitalized patients with mal-
nutrition. J Parenter Enteral Nutr. 2011;35
(2):209-216.
8. Academy of Nutrition and Dietetics. Interna-
tional Dietetics and Nutrition Terminology
(IDNT) Reference Manual. Standardized Lan-
guage for the Nutrition Care Process. Fourth
Edition. 2012.
9. White JV, Geunter P, Jensen G, et al. Consensus
statement of the Academy of Nutrition and Die-
tetics / American Society for Parenteral and
Enteral Nutrition: characteristics recommended
for the identification and documentation of
adult malnutrition (undernutrition). J Parenter
Enteral Nutr. 2012;36(3):275-283.
10. Giannopoulos GA, Merriman LR, Rumsey A,
Zwiebel DS. Malnutrition coding 101: financial
impact and more. Nutr Clin Pract. 2013;28
(6):698-709.
11. Centers for Disease Control. http://
www.cdc.gov/nchs/icd/icd9cm.htm. Retrieved
1/1/2015.
12. Advance Healthcare Network. http://health-
information.advanceweb.com/Web-Extras/CCS-
Prep/An-Inpatient-Prospective-Payment-
System-Refresher-MS-DRGs-2.aspx Retrieved
1/1/2015.
13. Sturgeon J. Stew on This: Case Mix Basics. For
The Record. 2007;10(11):6.
http://www.fortherecordmag.com
14. Corkins ME, Guenter P, DiMaria-Ghalili RA, et
al. A.S.P.E.N. Data Brief 2014: Use of enteral
and parenteral nutrition in hospitalized patients
with a diagnosis of malnutrition: United States,
2010. Nutr Clin Pract. 2014;29(5):698-700.
Alicia Taub is the Clinical Nutrition Manager and
Holly Guzman a Neonatal and Nutrition Support
Table 7. OPTIMIZATION ACHIEVED – malnutri-
tion diagnosis documented by RDN, and coded *
Coders did not use ICD-9-CM codes: 263, 263.1 or 263.8
Cases Jan - Mar Apr - Jun
Submitted by RDNs 477 508
Not Coded 355 355
Optimization Missed 56 64
Revenue missed $219,927 $319,732
Table 8. OPTIMIZATION MISSED – malnutrition
diagnosis documented by RDN, but not coded
cord coding and financial data at SJHMC.
References
1. DiMaria-Ghalili RA. Changes in nutritional
status and postoperative outcomes in elderly
CABG patients. Biol Res Nurs. 2004;4(2):73-84.
2. Hoffer LJ. Clinical nutrition: 1. Protein-energy
malnutrition in the inpatient. Can Med Assoc J.
2001;165(10):1345-49.
3. Baldwin C, Parson TJ. Dietary advice and nutri-
tional supplements in the management of ill-
ness-related malnutrition: a systematic review.
Clin Nutr. 2004;23(6):1267-1279.
4. Mechanick JI. Practical aspects of nutrition sup-
11
Future Dimensions in Clinical Nutrition Practice Winter 2015
Key Information Related to
Long-Term Care and F 325 By Krista Clark, MBA, RD, LD
In long-term care (LTC), Registered Dietitian Nu-
tritionists (RDNs) are keenly aware of F 325,
which relates to nutrition. F 325 is the CMS
guideline for surveyors that states:
Based on a resident’s comprehensive assess-
ment, the facility must ensure that a resident--
§483.25(i)(1) Maintains acceptable parame-
ters of nutritional status, such as body weight
and protein levels, unless the resident’s clini-
cal condition demonstrates that this is not
possible; and
§483.25(i)(2) Receives a therapeutic diet
when there is a nutritional problem1
We know that impaired nutritional status is NOT
a normal part of aging and may be associated
with an increased risk of mortality, impaired
wound healing, a decline in function, fluid and
electrolyte imbalance/dehydration, and un-
planned weight change. Since intake is not the
only factor that affects nutritional status, nutri-
tion-related interventions only sometimes im-
prove markers of nutritional status such as body
weight and laboratory results. While they can
often be stabilized or improved, nutritional defi-
cits and imbalances may take time to improve or
they may not be fully correctable in some indi-
viduals. Therefore, to optimize a resident’s nu-
tritional status, we must use a systematic ap-
proach:
• Identify and assess BOTH the resident’s
nutritional status and risk factors for nutri-
tional compromise
• Evaluate and analyze the assessment in-
formation, which must include subjective
information from the resident or family
• Develop and consistently implement perti-
nent approaches
• Monitor the effectiveness of interventions
and revise them as necessary
Nutrition Assessment
Assessment is a systematic process of obtaining,
verifying, and interpreting data in order to make
decisions about the nature and cause of nutrition
-related problems. It provides information that
helps to define meaningful interventions to ad-
dress any nutrition-related problems. It should
include observation, gathering, and considera-
tion of information relevant to each resident’s
eating and nutritional status to clarify nutritional
issues, needs, and goals in the context of the
resident’s overall condition. It is key to identify
usual body weight, a history of reduced appetite
or progressive weight loss or gain prior to admis-
sion, medical conditions such as a stroke, and
events such as recent surgery which may have
affected a resident’s nutritional status and risks.2
In LTC, physical and functional assessment of a
resident should include a description of his or
her overall appearance such as robust, thin,
obese, or cachectic and other findings including
level of consciousness, responsiveness, affect,
oral health and dentition, ability to use the hands
and arms, and the condition of the hair, nails,
and skin that may affect or reflect nutritional
status.3
Further information on nutritional physi-
cal and functional assessment can be found else-
where.
Height should be actually measured by the resi-
dent standing or estimated via arm span or knee
height, as often reported heights or height docu-
mented from acute facilities are inaccurate.
Weight must also be measured upon admission
or readmission to establish a baseline weight,
weekly for the first four weeks after admission,
and at least monthly thereafter to help identify
and document trends such as insidious weight
loss. Weighing may also be pertinent if there is a
significant change in condition, food intake has

12
Future Dimensions in Clinical Nutrition Practice Winter 2015
declined and persisted (e.g. for more than a
week), or there is evidence of altered nutritional
status or fluid and electrolyte imbalance. In
some cases, weight monitoring is not indicated,
such as when the individual is terminally ill and
requests only comfort care.4
Both nutrient and fluid needs
should be estimated and
compared to intake to deter-
mine if intake is adequate to
meet those needs. Usually
meal intakes are documented
as a percentage such as 25%,
50%, 75%, or 100%. Dieti-
tians may become concerned
if meal intake is 50% or less
but those residents with lower calorie needs may
actually be meeting their nutritional require-
ments. Thus, meal intake should be compared to
estimated nutrient needs and the nutrient con-
tent of meals.3
When estimating needs and evaluating intake,
the RDN must consider underlying illnesses or
problems. The inability to consume meals pro-
vided may be the result of the form or consis-
tency of food or fluid, cognitive or functional de-
cline, arthritis-related impaired movement, neu-
ropathic pain, or insufficient assistance. Food or
fluid provision may be inadequate at meals or
through tube feedings. Environmental factors
may affect intake or appetite such as the comfort
and level of disruption in the dining environment.
Adverse consequences related to medications
should be considered. The resident may require
increased calories due to wandering, pacing, or
rocking. Digestion and absorption may be im-
paired due to gastrointestinal disorders or gastric
surgery. Nutrient and fluid loss may occur from
prolonged diarrhea or vomiting. Further, hyper-
metabolic states such as pressure ulcers, other
wounds, advanced COPD, pneumonia and other
infections, cancer, hyperthyroidism, and fever
increase demands for calories, protein, and
fluid.2
In analysis, assessment information is used to
determine a resident’s nutritional status AND to
develop an individualized plan of care. Conclu-
sions may include, but are not limited to, a target
desirable body weight range that is based on the
individual’s overall condition, goals, prognosis,
and usual body weight; approxi-
mate nutrient and fluid needs;
whether and to what extent
weight stabilization or improve-
ment can be anticipated;
whether altered weight or nutri-
tional status could be related to
an underlying medical condition;
unplanned or undesirable weight
change and significance of that
change; identification of a clini-
cally pertinent basis for a conclusion that a resi-
dent could not attain or maintain acceptable pa-
rameters of nutritional status; and specification
of the nutritional concern(s). A clear statement
of the nature of nutritional concerns provides the
basis for resident-specific interventions. The fol-
lowing are examples:
• Poor food and fluid intake – The resident is
consuming less than 50% of calorie and
protein needs, and has increased nutri-
tional needs due to constant pacing. The
resident has also lost significant weight of
5% over the last month and is taking medi-
cations that may affect appetite.
• Specific clinical conditions – The resident
has an infection with a fever and is in a
hypermetabolic state associated with in-
creased demand for energy, protein, and
fluid. The resident also has a neuromuscu-
lar disorder and impaired cognition affect-
ing attention and the ability to feed self.
Resident Rights
The Care Plan MUST consider resident choice.
The RDN, with the interdisciplinary team, can
help the resident exercise their rights effectively
by discussing with the resident (or the resident’s
representative), the resident’s condition, treat-
ment options and related risks and benefits, ex-
“The Care Plan MUST con-
sider resident choice. The
RDN, with the interdiscipli-
nary team, can help the
resident exercise their
rights effectively...”

13
pected outcomes, personal preferences, and any
potential consequences of accepting or refusing
treatment. If the resident or representative de-
clines specific interventions, the facility must ad-
dress the resident’s concerns and offer relevant
alternatives. Many risk factors and some causes
of weight loss can be addressed, at least par-
tially, BUT others may not be modifiable – cer-
tain interventions may not be indicated or appro-
priate, based on individual goals and prognosis.
In regards to a therapeutic or mechanically al-
tered diet, dietary restrictions may help in select
situations. The use must be justified however, as
restrictions may also impair adequate nutrition
and lead to further decline in nutritional status,
especially in already malnourished or at-risk indi-
viduals. Diet liberalization can enhance the qual-
ity of life and nutritional status in older adults in
LTC. A resident or their representative may de-
cide to decline medically relevant dietary restric-
tions. If so, benefits vs. risks must be identified,
communicated, and documented, AND the resi-
dent and RDN with the interdisciplinary team
should collaborate to identify possible alterna-
tives.
Nutrition Monitoring
Monitoring is necessary for all residents whether
nutritionally stable or nutritionally compromised
or at risk for compromise, although more inten-
sive monitoring is indicated for residents with
impaired or at-risk nutritional status. In LTC,
monitoring should include a review of resident-
specific factors identified as part of the compre-
hensive resident assessment and any follow-up
assessments. Observing for and recognizing the
emergence of new risk factors such as acute
medical illness, pressure ulcers, or fever is im-
perative. The continued relevance of any current
nutritional interventions such as therapeutic di-
ets, tube feedings, or nutritional supplements
must be reviewed and the rationale for continu-
ing or stopping interventions must be docu-
mented.
The CMS Survey in LTC
CMS surveyors use a very detailed investigative
protocol when assessing compliance with F 325.
Their objectives are to determine if the facility
has practices in place to maintain acceptable pa-
rameters of nutritional status based on the com-
prehensive assessment. They evaluate whether
failure to maintain acceptable parameters of nu-
tritional status was avoidable or unavoidable.
They determine if the resident has received a
therapeutic diet if indicated. Finally, they deter-
mine if the facility identified and addressed risk
factors for, and causes of, impaired nutritional
status, or documented why they could not or
should not do so for a resident at nutritional risk.
Residents are observed during the initial tour
and throughout the survey process. Two meals
are observed with attention to serving sizes,
preferences, nutritional supplements, adaptive
equipment, feeding assistance, and prescribed
therapeutic diets to determine if interventions in
the care plan are implemented. The resident,
family, and/or resident’s representative is inter-
viewed to determine if the staff are responsive
to the resident’s eating ability and support
needs, food and dining preferences, whether the
resident is offered choices and substitutions at
meal times, and if treatment options, related
risks and benefits, expected outcomes, possible
consequences, and alternatives or other inter-
ventions were discussed and offered.
Interdisciplinary team members on all shifts, in-
cluding the RDN, are interviewed to determine
how food and fluid intake, oral eating ability, and
weight – and any changes to these parameters –
are monitored and reported and how nutrition
interventions are provided. If documented inter-
ventions or care provided appear to be inconsis-
tent with current standards of practice, physi-
cians and other healthcare providers are inter-
viewed to collect information about the resi-
dent’s nutritional risks and needs, including the
rationale for chosen interventions, how current
interventions are evaluated for effectiveness,
how interventions are managed, how the inter-
disciplinary team decided to maintain or change
interventions, and the rationale for not interven-
ing to address identified needs.5
Future Dimensions in Clinical Nutrition Practice Winter 2015
14
Future Dimensions in Clinical Nutrition Practice Winter 2015
Additionally, the medical record documentation
is reviewed thoroughly to ensure each resident
has been evaluated for nutritional status, those
who are at nutritional risk are clearly identified,
whether interventions have been developed and
implemented in a timely fashion, whether the
residents were monitored for progress, the effec-
tiveness of interventions, and especially if a resi-
dent’s decline or failure to improve from a nutri-
tional standpoint was avoidable or unavoidable.
Specifically, dietitians must document all of the
following, when applicable:
• Desirable body weight range
• Weight loss or gain and whether it was
significant
• Significant change in a resident’s intake
and reasons for the change, if known
• Appropriate interventions implemented
• If dietary restrictions are indicated
• If the resident was encouraged to make
food and care choices
• Chewing and/or swallowing problems and
how these are addressed
• Type of assistance needed to eat or drink
• Identified medication interactions
• Review of abnormal lab results and how
these were addressed nutritionally, if ap-
propriate
• If the resident’s current nutritional status
is met or improving towards established
goals
Finally, the care plan is reviewed to determine if
it is based on the assessment. It must have
measurable objectives and appropriate time
frames for goals to be met. Specific interventions
must be outlined for each problem identified to
try to maintain or improve parameters of nutri-
tional status. Further, it must take into consid-
eration the resident’s overall personal goals,
choices, preferences, prognosis, conditions, as-
sessed risks, and needs.1
Ultimately, the facility is in compliance with F
325, Nutrition, if staff have:
• Assessed the residents’ nutritional status
and identified factors that put the resi-
dent at risk of not maintaining acceptable
parameters of nutritional status
• Analyzed all available information to iden-
tify the medical conditions, causes, and
problems related to the residents’ condi-
tion and needs
• Provided a therapeutic diet when indi-
cated or provided justification for not pro-
viding a therapeutic diet
• Clearly defined and implemented inter-
ventions to maintain or improve nutri-
tional status that are consistent with the
residents’ assessed needs, choices, goals,
and recognized standards of practice
• Provided clinical justification for why in-
terventions were not implemented
• Monitored and evaluated the residents’
response to interventions and revised ap-
proaches as needed, or justified continua-
tion of current approaches1
Conclusion
LTC is a very complex field. Unlike acute care,
residents typically stay in the facility for the re-
mainder of their lives. Therefore, nutritional care
is a long-term and ongoing process. Residents
must be reassessed constantly and care plans
and interventions revised based on the progres-
sion or decline of their nutritional status. Dieti-
tians are key in improving and stabilizing the resi-
dents’ quality of life.
References
1. Department of Health and Human Services/
CMS. Nursing Homes - Issuance of Revised
Nutrition and Sanitary Conditions (Tags F325
and F371) as Part of Appendix PP, State Op-
erations Manual, and Training Materials. Bal-
timore, MD. June 20, 2008.
2. Morley JE, Thomas DR, Kamel HK. Nutritional
deficiencies in long-term care. Council for Nu-
tritional Clinical Strategies in Long-Term Care.
February 2004. www.LTCnutrition.org.
3. Bowman JJ, Keller HH. Assessing nutritional
risk of long-term care residents. Can J Diet
Pract Res. 2005;66(3):155-161.

15
Future Dimensions in Clinical Nutrition Practice Winter 2015
Managing Editor:
Jennifer Doley, MBA, RD,
CNSC, FAND
520-872-6109
Lead Features Editor:
Lisa Trombley, MA, RD, CNSC
310-903-2900
Features Editors:
Leigh-Anne Wooten, MS, RD, LDN
704-355-6660
Amanda Nederostek, MS, RD, CD
(801) 662-5303
Interested in contributing an article to the newsletter? Topics of interest in-
clude leadership, management, inno-
vations in clinical practice, research
and outcomes, nutrition legislation
and public policy, reimbursement and
coding, informatics, healthcare re-
form, and many others. If interested,
please contact an editor.
4. Richardson B. Long term care nutrition and
the CMS 2007 Action Plan. Association of Nu-
trition and Food Service Professionals. Die-
tary Manager. May 2007. Pp 17-21.
5. Handy L. Deficiency free in nutrition status:
using new interpretive guidance and protocol
for F325. Association of Nutrition and Food
Service Professionals. Dietary Manager. Sep-
tember 2008. Pp 10-15.
Krista Clark is a member of the Academy Infor-
matics committee focusing on long term
care. She has also provided nutrition services in
long term care for 12 years. She can be reached
Visit us at the CNM DPG website—cnmdpg.org. Available resources include:
• Searchable member directory
• Resource library
• The DPG’s guiding principles and strategic plan
• The Standards of Professional Performance for Dietitians in Clinical Nutrition Management
• Newsletter archives
• CNM annual report to members
• Eblast archives
• Information on the Informatics and Quality and Process Improvement (QPI) subunits
• Sign up for the CNM electronic mailing list (EML)
• Sign up for the QPI EML—in the members only section, click on the Subunits tab, then QPI
• Update your CNM profile—click on Edit Your Profile in the Member Info section
For additional information, contact us at: [email protected]
One free CPEU available to CNM DPG members!
1. Read the article titled “Malnutrition in Acute Care: Diagnosis, Documentation and Reimburse-
ment Impact” by Alicia Taub and Holly Guzman.
2. Log on to the CNM DPG website at cnmdpg.org
3. Go to the member’s only section and click on the link for the CPE Exam
4. Take the exam; your CPE certificate will be emailed to you within one week
This article has been approved for 1 CPE, Level 3; Learning Needs Codes 3005, 7080, 7170. The
test will remain available for three years after the publication date of this edition of Future
Dimensions in Clinical Nutrition Practice (February 9th
, 2015).
16
Future Dimensions in Clinical Nutrition Practice Winter 2015
Quality and Process Improvement
Sub-Unit Update By Sherri Jones, MS, MBA, RDN, LDN, FAND
QPI Project Contest Update:
Several communications went out about the new Quality/Process Improvement Project Award Program. Appli-
cations for the contest were accepted through January 16, 2015. This was an extension from the original De-
cember 29, 2014 deadline, as it was difficult for CNM members to meet the December deadline with the hustle
and bustle of the holiday season. I am thrilled to report that we received a total of 17 project submissions.
That is fantastic for the kickoff year of the contest. I want to thank those CNM members who submitted and
those who encouraged others to submit. A variety of projects were received covering both clinical and food
service topics, for example: Malnutrition Identification, In Room Dining, Volume Based Tube Feedings, and Pa-
tient Feeding Programs to name a few.
The next step is for the 17 projects to be judged by a 5 member panel from the CNM Executive Committee. The
projects will be ranked into the “top ten” and a 1st
place winner will be identified. The 1st
place winner will be
announced on stage at the 2015 CNM Symposium and will receive free symposium registration (a $360 value).
In addition, the top ten projects will be showcased as poster presentations at the symposium for additional
CEUs. This will provide the opportunity to learn from the quality improvement initiatives others have accom-
plished. We also plan to publish the top ten projects in the CNM newsletter as well as on the QPI Sub-Unit
website. Look for the winners to be announced…
QPI Sub-Unit Session @ Annual CNM Symposium – April 2015:
The QPI Sub-Unit is gearing up for our session at the CNM Symposium this year in Seattle, WA. We will high-
light our sub-unit updates, and most excitedly, announce the 1st
place winner for our QPI Project Contest. We
will then turn the remainder of the session over to our guest speaker, Sharon McCauley, Director Quality Man-
agement for the Academy of Nutrition and Dietetics. Sharon will review what has been happening in Quality at
the Academy and resources available to Academy members. We are looking forward to what Sharon has to
share. CNMs will surely be enlightened.
Special QPI Sub-Unit Electronic Mailing List (EML):
Reminder…don’t forget about our special EML. We have more than 100 subscribers. The purpose of this QPI
EML is to pose questions and share resources related to quality and process improvement. If you are not cur-
rently subscribed to the QPI EML and wish to do so, go through the QPI Sub-Unit webpage or enter the follow-
ing URL directly: http://www.cnmdpg.org/members/page/qpi-sub-unit-member-info.
And as always, if you have any questions or suggestions for the new Quality and Process Improvement Sub-
Unit feel free to contact the sub-unit Chair and/or Vice-Chair. The sub-unit is a member benefit, and thus, we
want to be sure to meet your needs and expectations. Continue to visit the QPI Sub-Unit section of the web-
site for updates.
QPI Sub-Unit Chair: Sherri Jones, MS, MBA, RDN, LDN, FAND [email protected]
QPI Sub-Unit Vice-Chair: Cindy Hamilton, MS, RD, LD [email protected]
CNM DPG Announcements
17
Future Dimensions in Clinical Nutrition Practice Winter 2015
Research Committee Report By Susan DeHoog, RD
Phase 1 of the staffing and productivity study was completed last summer. Results were presented at
a session at FNCE in Atlanta, and will be presented again at the CNM Symposium in Seattle. A poster
reviewing the outcomes of the study is also being displayed at Nutrition Week in February . A journal
article has been submitted to the Journal of the Academy of Nutrition and Dietetics; publication is
expected in the next couple of months.
Financial support from the CDR is being considered for Phase 2, in which studies will assess the corre-
lation, if any, between RDN time and patient outcomes in order to develop and validate a gold stan-
dard staffing model. We expect to hear soon if we will receive a grant for this phase.
Informatics Sub-Unit Report By Janel Welch, MS, RD, LD
The Informatics Sub Committee has been working to roll out the 2015 CNM Member Survey. The sur-
vey will run February 20 until April 5. If you complete the survey, your name will be entered into a
drawing for a $25.00 gift card. The CNM Executive Committee would like to get your feedback re-
garding the idea of changing our DPG name. Yes, this is a big decision, however we want our name to
welcome members in all areas of leadership and management, not just clinical nutrition manage-
ment. The survey will provide the option of keeping our original name so if you are opposed to a
change that will be accounted for. We are hoping for a great response rate so we encourage you to
please take the time to respond: https://www.surveymonkey.com/s/CNM2015svy.
The Informatics Sub-Unit also encourages you to visit the CNM website and check out the resources
available for members. If you are interested in sharing materials with other members, please post
them on the member EML, as we continuously monitor for tools that all members would benefit
from. Another feature of the website is the member profile directory. This gives you the ability to
find other CNM members who have similar interests or are using the same electronic medical record
as you are. This gives members another opportunity to network with peers.
Advertisements in Future Dimensions
CNM accepts advertising for publication in Future Dimensions in Clinical Nutrition Management. All ads are
subject to approval by the Review Committee and must meet established guidelines. All ads must be camera
ready and received by the Editor by copy deadlines. Fees must accompany the ad at the time of submission.
CNM members receive a 20% discount. Send all inquiries to the Managing Editor, Future Dimensions in Clinical
Nutrition Management. Publication of an advertisement in Future Dimensions in Clinical Nutrition Manage-
ment should not be construed as endorsement of the advertiser or the product by the CNM DPG or the Acad-
emy of Nutrition and Dietetics.
Future Dimensions In Clinical Nutrition Management Viewpoints and statements in these materials do not necessarily reflect policies and/or official positions of the
Clinical Nutrition Management Dietetic Practice Group or the Academy of Nutrition and Dietetics. © 2014
Clinical Nutrition Management Dietetic Practice Group of the Academy of Nutrition and Dietetics. All rights re-
served.

18
Future Dimensions in Clinical Nutrition Practice
Briefly describe your
current job and rele-
vant past positions.
I am the Clinical Nutri-
tion Operations Man-
ager for UnityPoint
Health in Des Moines,
Iowa. Our depart-
ment services 4 Unity-
Point hospitals on 3
campuses, serving
neonates to cente-
narians. We have 24
inpatient dietitians, three outpatient dietitians,
three consultant dietitians, eight diet technicians, one supervisor and a room service call center
that processes about 40,000-50,000 meal re-
quests and patient orders each month.
My job is focused on CBORD database mainte-
nance, patient menu development and imple-
mentation (in concert with Aramark), policies and
procedures, and auditing records for clinical and
non-clinical performance measures. I am also
charged with the management of our outpatient
counseling and consulting staff. We are also
working on plans to staff about 30 UnityPoint
outpatient clinics in central Iowa with RDs.
Prior to this position, I was an inpatient clinical
dietitian at UnityPoint Health for 15 years, spe-
cializing in cardiac and critical care. I was a late-
comer to dietetics, passing the exam at the age of
38. I have been many things in this life; a profes-
sional athlete and a college coach, a foods re-
searcher, a concert promoter, a medical records
officer for a charity hospital overseas, and an en-
trepreneur in agribusiness.
What do you love most about your job?
I love the team with whom I work, and I really
enjoy the camaraderie of the other Clinical Nutri-
tion Managers for the UnityPoint Health affiliates
from Sioux City, Iowa to Madison, Wisconsin. I
do love the idea that I am a coach and a guide by
the side. I enjoy the change of tasks from week
to week. I still enjoy patient contact via inten-
tional rounding and bilingual education.
What is the most challenging part of your job?
We have a very experienced staff; almost ½ of
the clinical staff have been with us for more than
20 years. That is a double-edged sword; on one
hand we have a wealth of expertise and on the
other, there is on occasion incredible inertia
against positive change. My CNM counterpart
and I have found some deeply entrenched be-
havior that is challenging to coach and difficult to
finesse, given our relatively recent arrival. We are working on it.
I also struggle with the devil that lives in the de-
tails. The diet management system and the elec-
tronic health records that we use are a marvel,
but the incredible detail work that they require
pulls my attention away from other pressing
matters more than I would like.
Healthcare is not an agile enterprise. We are a
large hospital group with a large food service
contract organization, and I have had to re-think
my horizons about change since starting this job.
In my old business, we could re-tool and start a
new venture inside of two weeks. That doesn’t
happen here, and I have to consider that.
What advice do you have for RDs new to man-
agement, or for those interested in becoming
managers?
Go into business. Get an MBA. Better yet, do
both. Do something other than just clinical work
if you want to be a great manager. I don’t want
to discount clinical dietetics experience, but I do
so precious little with it now since I left the floors
just 15 months ago. The skills that carry the day
for me now are what I learned from starting my
own business and what I learned being an ath-
letic coach.
Featured Member: Brian J. Smith, RDN, LD
Winter 2015

19
Future Dimensions in Clinical Nutrition Practice Winter 2015
Describe what you think the ideal role of the RD
should be 30 years from now. What do you
think we need to do as a profession to get to
that point?
There will be many roles for dietitians in 30 years.
I think we need to make the tent a little bigger for
dietitians who are not inclined to take care of a
hospital floor for a living. There is so much op-
portunity and so very few people who are able to
capitalize on those opportunities. The trick is to
be very good at matchmaking skill sets to what
the job requires. I hope to be one of those
matchmakers as we proceed into the future.
The fact remains that in 10-15 years, we will be staring down a significant shortfall of qualified
people relative to the jobs available. I would go
after those who are not traditionally thought of
for our profession. As a male, I find it almost
laughable that I am in a minority of about 3% in
this profession. We have some work to do.
Finally, we still need to advocate for credentialing
and reimbursement for our work. It is very diffi-
cult for us to justify our value to the organization
when we provide so very little in the way of reve-
nue. Money still talks.
If you couldn’t be a dietitian anymore, what pro-
fession would you choose?
I would probably either go back into education or
into consulting. I loved a teaching gig that I had
at the Iowa Culinary Institute, which I had to quit
when my wife passed away. When my children
are out of the house, I might consider going back
into post-secondary teaching. The consulting idea
also intrigues me. I did project work overseas and I would like to do that again possibly when my
daughters are launched into their adult lives.
20
Chair
Kathryn Allen, MA, RD, CSO
Chair-Elect
Caroline Steele, MS, RD, CSP, IBCLC
Immediate Past Chair
Young Hee Kim, MS, RD, LDN, CNSC
Secretary
Jennifer Wilson, MS, RD, LDN
Treasurer
Janet Barcroft, RD, LDN
Newsletter Managing Editor
Jennifer Doley, MBA, RD, CNSC, FAND
Features Editors
Lisa E. Trombley, MA, RD, CNSC
Leigh-Anne Wooten, MS, RD, LDN
Amanda Nederostek, MS, RD, CD
Nominating Committee Chair
Lisa Cherry, MS, RD, CNSC
Chair Elect
Wendy Phillips, MS, RD, CNSC, CLE
Committee Members
Tamara Smith, RD, LD
Kelly Danis, RD, LDN
CNM DPG Delegate to the HOD
Mary Jane Rogalski, MBA, RD, LDN
Nutrition Informatics Chair
Janel Welch, MS, RD, LD
Nutrition Informatics Vice-Chair
Ann Childers, MS, RDN, MHA, LD
Committee Members
Krista Clark, MBA, RD, LD
CNM EML Administrator
Deb Hutsler, MS, RD, LD
Assistant Administrator
Laurie Szekely
Public Policy Chair
Julie Haase, MS, RD, CD
Member Services Chair
Kerry Scott, RDN, CD
Committee Members
Alexandra Lautenschlaeger,
RD, LD, LDN
Alexandra.Lautenschlaeger@
rutherfordregional.com
Renee S. Winter-Bertsch,
Marsha Kenner, MS, RD, LDN
Lynn Becker, RD, LD
Professional Development Chair
Kelly Danis, RD, LDN
Committee Members
Beverly J.D. Hernandez,
PhD, RD, LDN
Winter 2015 Future Dimensions in Clinical Nutrition Practice
Clinical Nutrition Management Dietetic Practice Group
2014—2015 Executive Committee
Cathy Montgomery, RD, LD
Melissa Payne, MS, RD, LDN [email protected]
Research Co-Chairs
Susan DeHoog, RD
Barbara Isaacs Jordan, MS, RD,
CDN
Research DPBRN Liaison
Jessie Pavlinac, MS, RD, CSR, LD
Committee Members
Debby Kasper, RD, LDN, SNS
Barbara Lusk, RD, LDN
Quality and Process
Improvement Chair
Sherri L. Jones,
MS, MBA, RD, LDN, FAND
Quality and Process
Improvement Vice-Chair
Cynthia Hamilton, MS, RD, LD
Fundraising Chair
Sharron Lent, RD, LD
Immediate Past Chair
Monica Milonovich, MS, RD, LD
Academy of Nutrition and
Dietetics Manager, DPG / MIG
Relations
Mya Wilson, MPH, MBA