general therapeutic principles of oncology jamilah alsaidan msc
TRANSCRIPT

General Therapeutic Principles of oncology
Jamilah Alsaidan Msc
Outline
• Describe etiology , risk factors of cancer• Cancer statistics in Saudi Arabia • Highlight diagnosis and screening of cancer • Define cancer staging system • Describe relative roles of available treatments• ( Chemotherapy, radiation, surgery) • Classify chemotherapeutic drugs and distinguish mechanisms and adverse
effects • Identify certain medications ( and their rational for common malignancies)

INTRODUCTION
• Cancer is synonymous with the terms: • Neoplasm • Malignancy • Oncologic disease • Cancer is not a single disease, rather, it is a group of diseases
characterized by uncontrolled growth and spread of abnormal cells.
GENERAL THERAPEUTIC PRINCIPLES OF ONCOLOGY
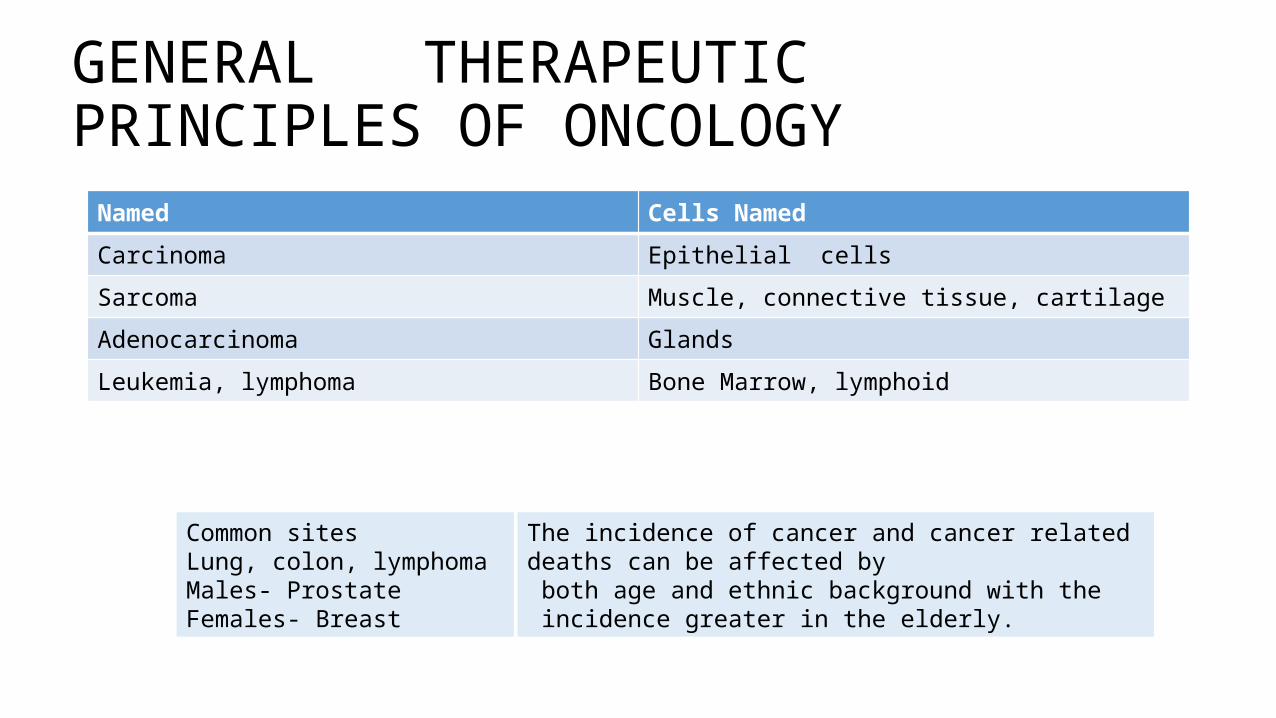
Named Cells Named
Carcinoma Epithelial cells
Sarcoma Muscle, connective tissue, cartilage
Adenocarcinoma Glands
Leukemia, lymphoma Bone Marrow, lymphoid
Common sitesLung, colon, lymphoma Males- Prostate Females- Breast
The incidence of cancer and cancer related deaths can be affected by both age and ethnic background with the incidence greater in the elderly.

Cancer statistics in Saudi Arabia
• Between January 01 and December 31, 2007, the total number of cancer incident cases reported to the SCR was 12,309. • Overall cancer was slightly more among women than men. Cancers
affected 5,982 (48.6%) males and 6,321 (51.4%) females.
Cancer Incidence and Survival Report, Saudi Arabia ( Accessed Online 2011)

GENERAL THERAPEUTIC PRINCIPLES OF ONCOLOGY • These abnormal cells :• Are often described as poorly differentiated or immature • cannot interact with other cells • cannot carry out the physiologic functions of their normal healthy
mature counterparts • Have the ability to invade adjacent normal tissues and break away
from the primary tumor (metastasize) and travel through the blood or lymph to establish a new tumor ( or metastases) at a new site.
GENERAL THERAPEUTIC PRINCIPLES OF ONCOLOGY • A neoplasm is benign when it grows in an unregulated fashion
without tissue invasion.• A neoplasm is malignant when it grows in unregulated fashion with
tissue invasion.

Etiology • Etiology Cancers arise from the transformation of a single normal cell.
A certain initial “event” causes damage or mutation to the cell’s DNA.
Etiology
Genetics Exposure to genetics

Basic Principles of Oncology Pharmacotherapy • Cancer at the molecular level: Two gene classes, oncogenes and
tumor suppressor genes may play a major role in the origin of cancer.• Oncogenes ( Turn on Cancer) • Tumor Suppressor Genes ( Turn off Cancer) • Genetic alterations including chromosomal translocations, deletions,
insertions, and point mutations of their normal counterparts- dysfunction- possible cancer.

Basic Principles of Oncology Pharmacotherapy • In normal cells Proto-oncogenes code for proteins that stimulate cell
division. Oncogenes arise from genetic alterations to Proto- oncogenes. • These oncogenes cause overgrowth of stimulatory proteins that lead
to excessive proliferation or growth and ultimately a malignant transformation. • Tumor suppressor genes encode for proteins that control inappropriate
cell division or growth. If these genes are lost, mutated or inactivated there will be elimination of the normal inhibition of cell division. • Tumor suppressor genes and proto- oncogenes together provide the
stimulatory and the inhibitory signal that determine whether a cell will enter the life cycle to divide and grow.
Basic Principles of Oncology Pharmacotherapy • These abnormal cells :• Are often described as poorly differentiated or immature • cannot interact with other cells • cannot carry out the physiologic functions of their normal healthy
mature counterparts • Have the ability to invade adjacent normal tissues and break away
from the primary tumor (metastasize) and travel through the blood or lymph to establish a new tumor ( or metastases) at a new site.

Basic Principles of Oncology Pharmacotherapy• Another characteristic of cancer cells that differs from normal cells is
that they often lack the normal cell-to- cell adhesion molecules called cadherins, and the cell to extracellular matrix molecules called integrins. • This allows the cancerous cells to break away from the primary tumor
mass, move through the body and form metastatic sites.

Basic Principles of Oncology Pharmacotherapy• Another characteristic of cancer cells that differs from normal cells is
that they often lack the normal cell-to- cell adhesion molecules called cadherins, and the cell to extracellular matrix molecules called integrins. • This allows the cancerous cells to break away from the primary tumor
mass, move through the body and form metastatic sites.
Basic Principles of Oncology Pharmacotherapy• Events that may induce alterations on the genetic level include
occupational, lifestyle, and environmental factors, some medications and of course hereditary factors.• Another term used could be risk factors or carcinogens. Some are
modifiable, that is a person can control their presence while others such as hereditary predisposition are not modifiable

Basic Principles of Oncology Pharmacotherapy Carcinogens associated with an increased risk of cancer
• Environmental:• Ionizing radiation ( radon gas
emitted from soil containing uranium deposits) • Ultraviolet radiation
Occupational • Asbestos • Chromium, Nickel, Vinyl
chloride, Benzene
• Associated Cancer• Leukemia, breast, lung, thyroid. • Skin melanoma • Lung, mesothelioma • Lung, liver

Basic Principles of Oncology Pharmacotherapy Carcinogens associated with an increased risk of cancer • Lifestyle • Alcohol • Dietary Factors • Tobacco
• Medical Drugs • Diethylstilbosterol
• Alkylating agents • Estrogens • Cyclophosphamide
• Associated Cancers• Esophagus, liver, stomach, oropharynx, larynx • Colon, Breast, Gall bladder• Lung, oropharynx, pharynx, larynx, esophagus, gall
bladder
• Breast, testes, ovary, and in offspring vaginal • Leukemia, bladder • Endometrial • Bladder

Basic Principles of Oncology PharmacotherapyScreening
• Because cancers are most curable with surgery or radiation before they have metastasized, early detection and treatment have obvious potential benefits • Early detection not possible for some cancers cause they don’t produce
signs or symptoms until they have become large or have metastasized • Lack of effective screening methods for some cancers • Inaccessibility of some anatomic sites • For some cancers effective screening methods do exist • Incorporate education of the public

Screening Guidelines for early detection of cancerTest or Procedure Disease
Breast Self Examination Clinical Breast Examination Mammography Breast Cancer
Cancer Fecal Occult blood test (FOBT) or Fecal Immunochemical Test Flexible Sigmoidoscopy Annual (FOBT) or (FIT) Colonoscopy Double contrast Barium Enema
Colorectal Cancer
Digital rectal exam or Prostate Specific Antigen Prostate Cancer
Pap Test or liquid based test Cervical Cancer
Information on health risks and symptoms Endometrial Cancer
Health counseling and physical examination Cancer related check Up

Adapted from tables 130-5 and 130-6, Pharmacotherapy, A pathophysiologic approach, 7th Edition
Basic Principles of Oncology Pharmacotherapy Screening- Presenting Signs and Symptoms
In Adults• Change in bowel or bladder habits • A sore that does not heal • Unusual bleeding or discharge • Thickening or lump in breast or
elsewhere • Indigestion or difficulty in
swallowing • Obvious changes in wart or mole • Nagging cough or hoarseness
In Children• Continued, unexplained weight loss• Headaches with vomiting in the morning • Increased swelling or persistent pain in the
bones or joints • Lump or mass in abdomen, neck, or
elsewhere• Development of a whitish appearance in
the pupil of the eye • Recurrent fevers not caused by infections • Excessive bruising or bleeding • Noticeable paleness or prolonged tiredness

Basic Principles of Oncology PharmacotherapyScreening
• Loss of appetite and Pain also common symptoms • Warning signs of cancer in children differ and reflect the types of
tumors more common in this patient population • Even with increased public awareness, the fear of a cancer diagnosis
can deter people from seeking medical attention.

Basic Principles of Oncology PharmacotherapyDiagnosis and staging
• Diagnosis • MUST get tissue for pathologic diagnosis• Cytogenetics, Tumor markers ???????• Lab • Complete blood cell count, electrolytes, renal & liver function • Radiology • X-rays, CT scans, MRI.

Basic Principles of Oncology Pharmacotherapy Diagnosis and staging
• Grading: Measures the extent to which tumor cells differ from their parent tissue • Grade 1= well differentiated
cells, function most like parent tissue least malignant • Grade 4 =least differentiated
cells, not like parent tissue most rapidly increasing in number
• Staging (TMN) Refers to extent of disease and relative size of tumor. • T: (0-4) =tumor size (primary) N:
(0-3)= degree or regional lymph node involvement • M: ( 0-3) = presence or absence
of distant metastases
Staging

Basic Principles of Oncology Pharmacotherapy
Treatment Modalities
Surgery Radiation Pharmacotherapy (Chemotherapy & Biologic therapy)

Basic Principles of Oncology Pharmacotherapy Treatment• Surgery: Oldest modality • Plays a major role in the diagnosis and treatment of cancer • Can reduce a tumor or totally remove it in early stages • Radiation: First used for cancer treatment in late 1800s • Is a mainstay in cancer management to this day • Receive treatment for multiple sites simultaneously • Effective for many kinds of cancer
Surgery and Radiation are local treatments

Basic Principles of Oncology Pharmacotherapy Treatment• Surgery and radiation can not treat completely if the cancer has
metastasized, and usually cancer is diagnosed at late stages. • Thus to completely eliminate the cancer will need other modalities
with localized treatment.
This is where pharmacotherapy comes in.(Drug therapy) consisting of chemotherapy and biologic agents.
Pharmacotherapy can be indicated as a primary, palliative, adjuvant, or Neoadjuvant treatment modality.
Basic Principles of Oncology Pharmacotherapy Treatment Pharmacotherapy:
• Targets systemic malignancies such as leukemia that can not be cured with a localized modality • Chemotherapy and hormonal therapy can access the systemic
circulation and can theoretically treat the primary tumor and any metastatic disease • therapies are currently considered in the broader sense of
immunotherapy or “targeted therapies” • Systemic therapy is given either as adjuvant therapy to surgery or
radiation, pre operatively, post operatively.
Basic Principles of Oncology Pharmacotherapy Treatment• Micrometastases- cancer appears to be eliminated by surgery or
radiation. However, there is recurrence of cancer. This implies that the primary tumor began to metastasize before it was removed. • These early metastases are too small to detect with current diagnostic
tests and are known as micrometastases

Basic Principles of Oncology Pharmacotherapy Treatment- Applications
• Primary chemotherapy • First line treatment and, in the case of leukemia, it is referred to as
induction chemotherapy • Choice of primary chemotherapy is governed by observations made
from clinical trials that demonstrate that a given regimen has the highest known activity against the tumor• Can be either curative or palliative, depending on specific type of
tumor

Basic Principles of Oncology Pharmacotherapy Treatment- Applications
• Second line or salvage chemotherapy • Is administered after the tumor has become refractory to primary
therapy or if the patient is unable to tolerate first line therapy • Chemotherapy is the primary treatment modality used for
hematologic malignancies as well as a number of solid tumors that have metastasized at the time diagnosis or have recurred at metastatic sites after initial therapy.

Basic Principles of Oncology Pharmacotherapy Treatment- Applications
• Adjuvant therapy : is defined as the use of systemic agents to eradicate micrometastatic disease following localized modalities• Goal is to reduce subsequent recurrence rates and prolong long term
survival• Neoadjuvant or Preoperative Setting • The goal is to make other treatment modalities more effective by
reducing tumor burden and to destroy micrometastases• E.g. to shrink large tumors and make them more amenable to later
surgery resection and possibly spare critical organs

Basic Principles of Oncology Pharmacotherapy Treatment- Applications• Combined Modalities • The management of most types of cancer involves the use of
combined modalities

Basic Principles of Oncology Pharmacotherapy Treatment
• Primary curative modality • Treatment with cytotoxic drugs, e.g. testicular cancer, leukemias • Palliative chemotherapy • Often solid tumors are not curable with chemotherapy alone, either
because of the biology of the tumor or because of advanced disease at presentation • With palliative chemotherapy it is often possible to decrease tumor
size or to retard growth enough to reduce untoward symptoms caused by the tumor.

Basic Principles of Oncology Pharmacotherapy Treatment-• Factors that influence response
to chemotherapy• In the clinical setting tumor cells
do not always decrease predictably with each successive course of chemotherapy, This is because the growth fraction of human tumors is not 100% and because the cell population is not heterogeneous; and some are resistant to chemotherapy.
• The objective of successive chemotherapy courses is a further decrease in size of tumor mass. • Factors influence response: Dose
intensity • schedule • drug resistance • tumor site • A patients performance status

Tumor growth

Basic Principles of Oncology Pharmacotherapy Treatment
• Dose intensity: The chemotherapy dose per unit time over which treatment is given ( e.g., mg/m 2 /week) • Drug resistance might be overcome by escalating the dose intensity of
drugs. This can be achieved by: • Increasing the dose of chemotherapy per cycle • Shortening the interval between cycles Unnecessary lengthening of the interval between successive courses or decreasing the dose can negatively affect treatment outcomes The dose intensity for most chemotherapy regimens is limited by the major dose related toxicity

Basic Principles of Oncology Pharmacotherapy Treatment- Factors that influence response to chemotherapy
• Schedule dependency: The schedule of chemotherapy administration is an important determinant of response. • It influences dose intensity largely by affecting toxicity. • In some circumstances, changing the administration schedule can
reduce the toxicity sufficiently to allow patients to receive higher total doses or more frequent courses of therapy, thereby increasing the dose intensity • E.g., IV bolus vs. frequent IV infusion or continuous IV infusion

Basic Principles of Oncology Pharmacotherapy Treatment • Drug Resistance: • Biochemical resistance to
chemotherapy is the major impediment to successful treatment with most cancers• Resistance can occur de novo
in cancer cells or develop during cell division as a result of mutation
• Possible Mechanisms of anti- cancer cells drug resistance include: • Proficiency in repair of DNA • In drug activation • In drug inactivation • In cellular uptake of drug • In efflux of drug (multidrug
resistance) • Alterations in target enzymes (DHFR,
topoisomerase)

Basic Principles of Oncology Pharmacotherapy Treatment
• Tumor site:• The cytotoxic effects of chemotherapy agents are related to the time
the tumor is exposed to an effective concentration of the agent (i.e., concentration X time [C×T]). • The dosage regimen, including the dose, infusion rate, route of
administration, lipophilicity, and protein binding, can influence the concentration-time product. • Tumors located in sites of the body with poor drug penetration may
not receive a sufficient concentration of medication to eradicate cancerous cells.
Basic Principles of Oncology Pharmacotherapy Treatment
• Patients performance status • Specific patient factors such as presence of genetic polymorphisms
affect antitumor activity and adverse effects of chemotherapy agents. • E.g., a prodrug that needs to be metabolized to the active form by a
glucuronidating enzyme.• Patients with decreased activity of this enzyme experience
accumulation of drug and are at increased risk for potential side effects.

Basic Principles of Oncology Pharmacotherapy Treatment
Response Criteria for Evaluating Effects of Chemotherapy of Target Lesion:
Complete Response (CR): Disappearance of all target lesions
Partial Response (PR): At least a 30% decrease in the sum of the longest diameter (LD) of target lesions, taking as references the baselines sum LD Progressive Disease ( PD): At least a 20% increase in the sum of the LD of target lesions, taking as reference the smallest sum LD recorded since the treatment started or the appearance of one or more new lesions Stable Disease (SD): Neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD, taking as reference the smallest sum LD since the treatment started Disease free survival : Time from documentation of complete response until disease relapse or death
Overall survival: Time from treatment until time of death.
Basic Principles of Oncology Pharmacotherapy Treatment
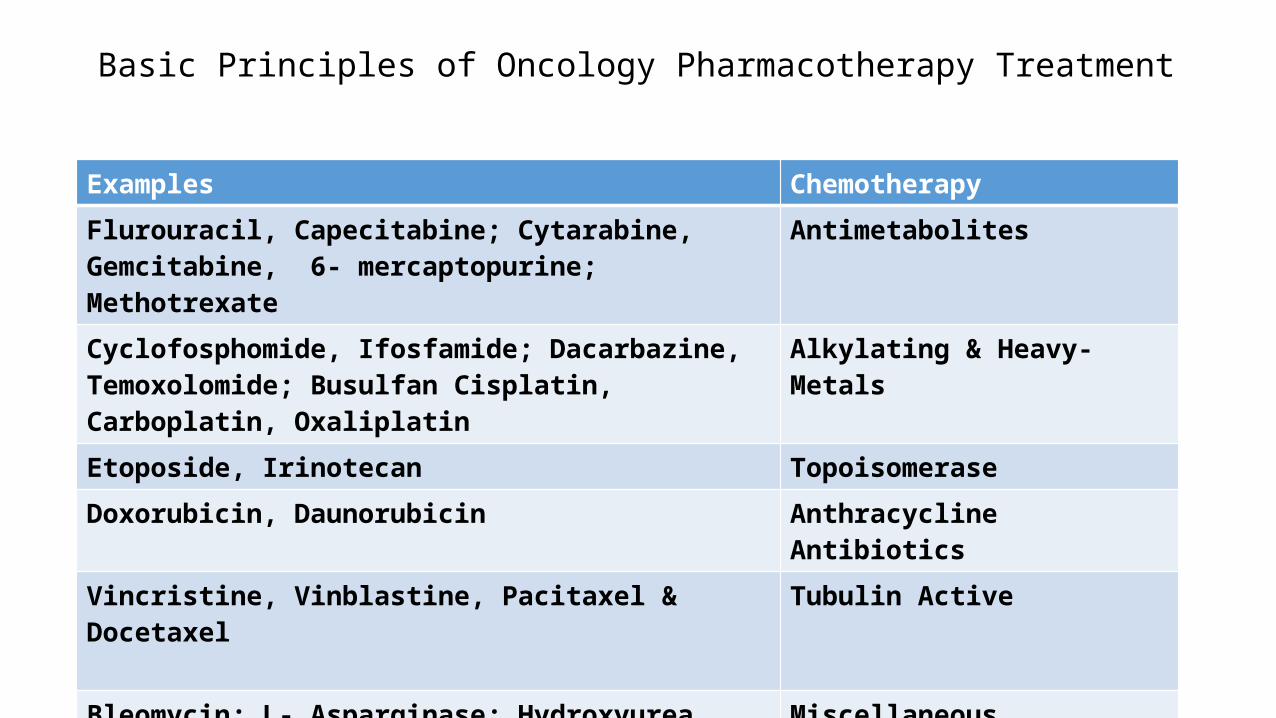
Examples Chemotherapy
Flurouracil, Capecitabine; Cytarabine, Gemcitabine, 6- mercaptopurine; Methotrexate
Antimetabolites
Cyclofosphomide, Ifosfamide; Dacarbazine, Temoxolomide; Busulfan Cisplatin, Carboplatin, Oxaliplatin
Alkylating & Heavy-Metals
Etoposide, Irinotecan Topoisomerase
Doxorubicin, Daunorubicin Anthracycline Antibiotics
Vincristine, Vinblastine, Pacitaxel & Docetaxel Tubulin Active
Bleomycin; L- Asparginase; Hydroxyurea, Tretinoin, Thalidomide
Miscellaneous
Bicalutamide, Flutamide; Anastrozole, Tamoxifen Hormonal
Interferon, Aldesleukin Immune Therapy

Basic Principles of Oncology Pharmacotherapy Treatment
Examples Targeted BiologicalRituximab Monoclonal Antibodies “Mabs”Imatinib Tyrosine-Kinase Inhibitors “Nibs”

Basic Principles of Oncology Pharmacotherapy Treatment
Examples Chemotherapy
Flurouracil, Capecitabine; Cytarabine, Gemcitabine, 6- mercaptopurine; Methotrexate
Antimetabolites
Cyclofosphomide, Ifosfamide; Dacarbazine, Temoxolomide; Busulfan Cisplatin, Carboplatin, Oxaliplatin
Alkylating & Heavy-Metals
Etoposide, Irinotecan Topoisomerase
Doxorubicin, Daunorubicin Anthracycline Antibiotics
Vincristine, Vinblastine, Pacitaxel & Docetaxel Tubulin Active
Bleomycin; L- Asparginase; Hydroxyurea, Tretinoin, Thalidomide
Miscellaneous
Bicalutamide, Flutamide; Anastrozole, Tamoxifen Hormonal
Interferon, Aldesleukin Immune Therapy
Basic Principles of Oncology Pharmacotherapy Treatment
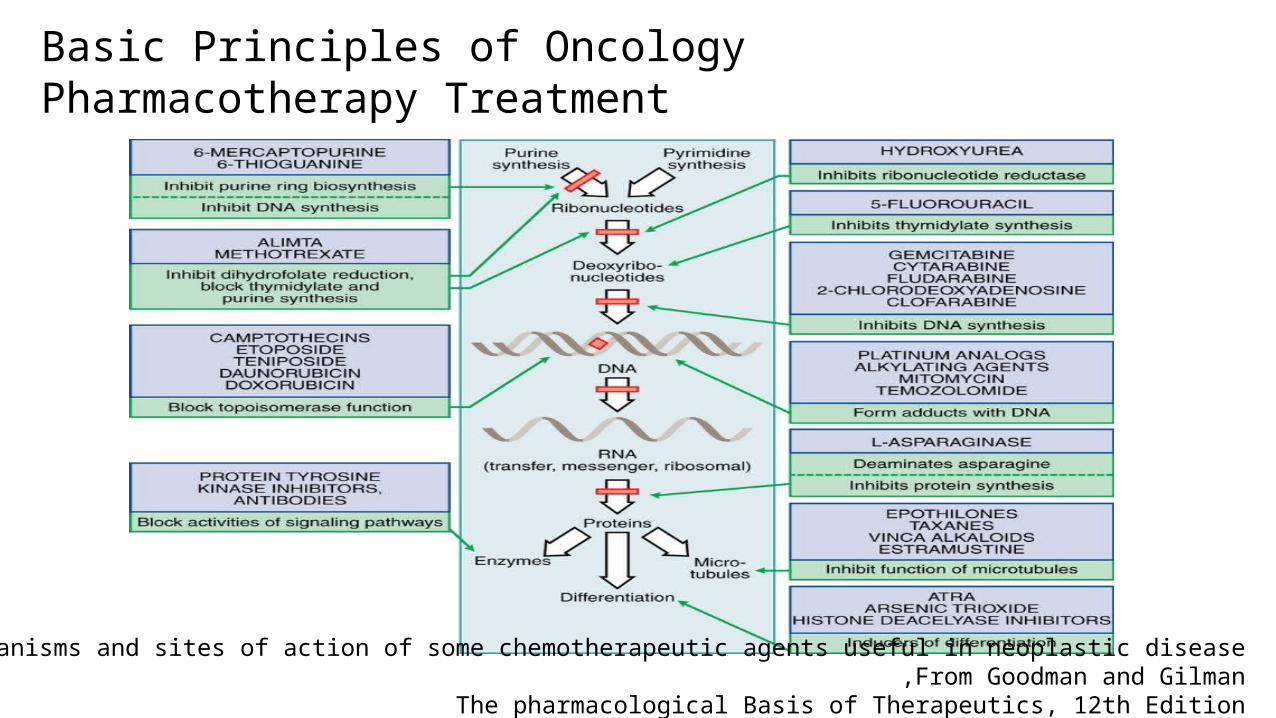
Figure 60.1 Summary of the mechanisms and sites of action of some chemotherapeutic agents useful in neoplastic disease .From Goodman and Gilman ,
The pharmacological Basis of Therapeutics, 12th Edition

Basic Principles of Oncology Pharmacotherapy Treatment
Figure60–2. Cell cycle specificity of antineoplastic agents. From Goodman and Gilman, -The pharmacological Basis of Therapeutics

Basic Principles of Oncology PharmacotherapyCell cycle specificity
• S-Phase: DNA synthetic phase • M-Phase: Formation of mitotic spindle, Mitosis , most vulnerable part of
the cell cycle • Leukemias and lymphomas have high percentage of proliferating cells, and
are the neoplasms most susceptible to chemotherapeutic measures. • Slowly growing tumors with a small growth fraction (e.g., carcinomas of the
colon or non small cell lung cancer ) are less responsive to cycle specific drugs • More effective are agents that inflict high levels of DNA damage (e.g.,
alkylating agents) or those that remain at high concentrations inside the cell for extended periods of time (e.g., fluoropyrimidines)

Basic Principles of Oncology Pharmacotherapy Treatment –cell cycle specificity
• Works on reproducing (non-resting) cells• There will always be some cells
still alive• Schedule dependent• Usually (but not always) as
infusion
• Works on all cells• Dose Dependent• Bolus (probably better but not
always) or infusion
Specific Non specific

Basic Principles of Oncology Pharmacotherapy Treatment -Toxicity and other adverse effects
• Toxicity targets rapidly dividing cells: • Narrow therapeutic range and distinctive toxicity • Bone marrow/myelosuppression (WBC, RBC, PLTs) • Mucus membrane and skin (esophagitis, diarrhea and alopecia) –• Nausea and vomiting via CTZ •

Basic Principles of Oncology Pharmacotherapy Treatment -Toxicity and other adverse effects
• Other adverse effects • Promalignant • Extravasation • Hypersensitivities • Gonadal effects ( hypogonadism, sterility) • Organ-Drug specific ( lungs, heart)
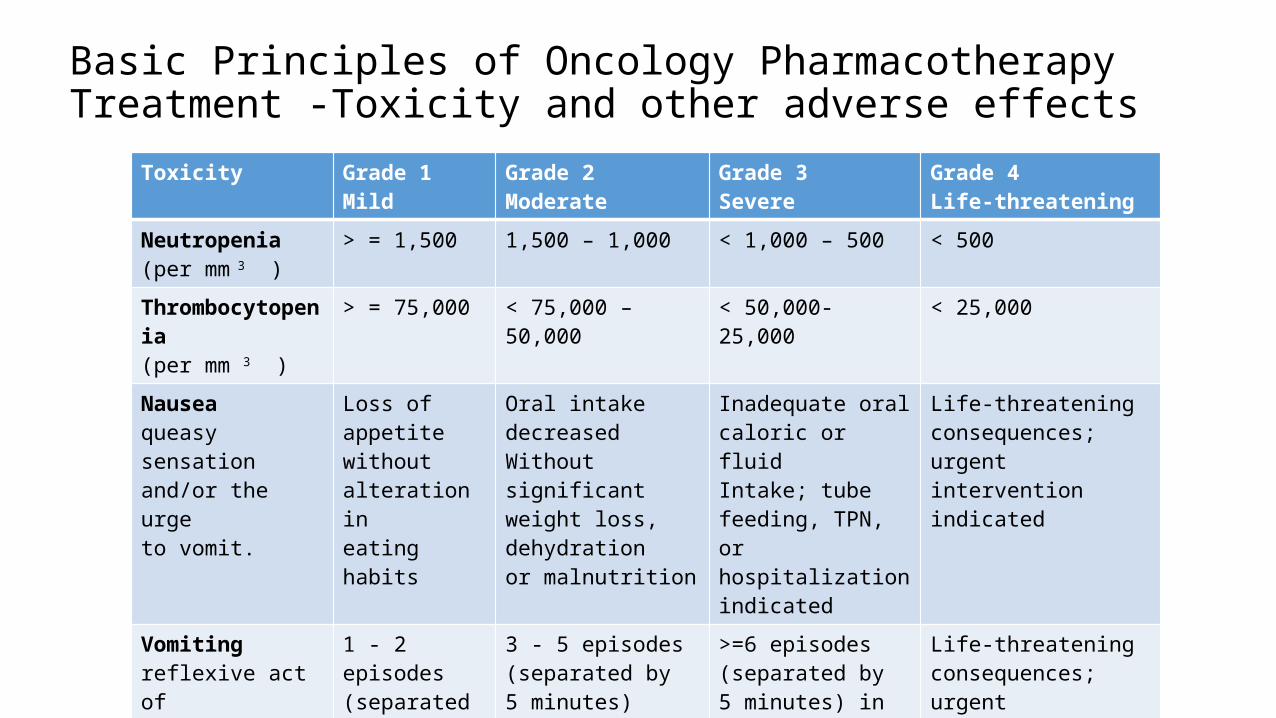
Basic Principles of Oncology Pharmacotherapy Treatment -Toxicity and other adverse effects
Toxicity Grade 1Mild
Grade 2Moderate
Grade 3Severe
Grade 4Life-threatening
Neutropenia(per mm 3 )
> = 1,500 1,500 – 1,000 < 1,000 – 500 < 500
Thrombocytopenia(per mm 3 )
> = 75,000 < 75,000 – 50,000 < 50,000- 25,000 < 25,000
Nauseaqueasy sensationand/or the urgeto vomit.
Loss of appetitewithoutalteration in eating habits
Oral intake decreasedWithout significantweight loss, dehydrationor malnutrition
Inadequate oral caloric or fluid Intake; tube feeding, TPN,or hospitalizationindicated
Life-threatening consequences;urgent intervention indicated
Vomitingreflexive act of Ejecting contents of stomach throughmouth.
1 - 2 episodes (separated by 5 minutes) in 24 hrs
3 - 5 episodes(separated by5 minutes)in 24 hrs
>=6 episodes (separated by 5 minutes) in 24 hrs; tube feeding, TPNor hospitalization indicated
Life-threatening consequences;urgent intervention indicated

Basic Principles of Oncology Pharmacotherapy Treatment –Designing specific clinical regimens
• Drugs in combination
• Ideally, drug combinations should not overlap in major toxicities• Cytotoxic drugs are used as close as possible to their maximally
tolerated individual doses AND • should be given as frequently as tolerated to discourage tumor
growth
•Negate effects of resistance mechanism specific for a single agent •May be synergistic because of their biochemical interactions

Basic Principles of Oncology Pharmacotherapy Treatment- Administration
• Systemic chemotherapy is most commonly administered by the IV route.
IV Administration
Bolus injection <15 min A short Infusion 15min to several hrs
Continuous infusion (24 hrs to several weeks)

Basic Principles of Oncology Pharmacotherapy Treatment- Administration
• No matter what the route of administration, the individual administering the chemotherapy should be: • experienced and expert in administration of the particular agent by
the chosen route • Aware of the most common toxicities associated with the
chemotherapy ( both acute and chronic) • Proper education of patient to know what to expect throughout
therapy • Printed educational materials in addition to oral instructions

Basic Principles of Oncology Pharmacotherapy Treatment- Administration• Currently most patients receive chemotherapy through a central
venous catheter to reduce some of the potential problems associated with the recurrent IV administration • Some chemotherapeutic agents are potent vesicants or irritants if
they extravasted from vein • Other agents can produce severe irritation and pain to peripheral
veins (sclerosis and thrombosis) • Other potential problems associated with IV therapy are
unsatisfactory venous access due to obesity, prior IV therapy with irritant drugs, or advanced age.

Basic Principles of Oncology Pharmacotherapy Treatment- Administration• A peripherally inserted central catheter (PICC) is non permanent but it
can be maintained and used for venous access for extended periods of time • In patients undergoing chemotherapy permanent central venous
access devices are commonly used. Central Venous access devices
Tunneled central venous catheter [CVC] e.g.,
Broviac, Hickman Subcutaneous Ports e.g., Port a Cath or
Infuse-A- Port



Basic Principles of Oncology Pharmacotherapy Treatment- Administration
• Techniques have been developed to locally administer agents to specific sites of the body affected by the tumor • Regional or local chemotherapy allows high concentrations of agents
to be achieved at the site of the tumor • The aim is to reduce systemic exposure and thus subsequent toxicity.• Downside is undetectable metastases at distant sites may not be
exposed to the chemotherapy, allowing continued growth of the mass

Basic Principles of Oncology Pharmacotherapy Treatment
Examples Chemotherapy
Flurouracil, Capecitabine; Cytarabine, Gemcitabine, 6- mercaptopurine; Methotrexate
Antimetabolites
Cyclofosphomide, Ifosfamide; Dacarbazine, Temoxolomide; Busulfan Cisplatin, Carboplatin, Oxaliplatin
Alkylating & Heavy-Metals
Etoposide, Irinotecan Topoisomerase
Doxorubicin, Daunorubicin Anthracycline Antibiotics
Vincristine, Vinblastine, Pacitaxel & Docetaxel Tubulin Active
Bleomycin; L- Asparginase; Hydroxyurea, Tretinoin, Thalidomide
Miscellaneous

Basic Principles of Oncology Pharmacotherapy Treatment - Antimetabolites
• False or faulty substrates that inhibit form, function or maintenance of DNA• Cell-cycle specific
Antimetabolites SubstrateFlurouracil, Capecitabine; Pyrimidine
Cytarabime, Gemcitabine Cytosine
6-mercaptopurine Purine
Methotrexate Folate

Basic Principles of Oncology Pharmacotherapy Treatment-Antimetabolites – Pyrimidine Uracil analouge
• 5-fluorouracil (5-FU) • Prodrug; Hepatic Elimination• Activity increased by folinic acid• Colorectal, breast, other GI & Head and Neck CA• Side effects:
• Bolus: Stomatitis, Esophagitis; neutropenia• Infusion: Diarrhea• Uncommon: Neuro, Cardiotoxicity.

Basic Principles of Oncology Pharmacotherapy Treatment-Antimetabolites – Pyrimidine Uracil analouge
• Capecitabine• Oral prodrug of 5-FU• Like 5-FU, more myelosuppression & palmar-plantar erythrodyesthesia;
Affects INR
• Used in treatment of metastatic breast cancer either as a single agent or in combination with the taxane docetaxel

Basic Principles of Oncology Pharmacotherapy Treatment ANTIMETABOLITES Cytosine Analogs
• Cytarabine- s phase specific • Renal elimination • – IV as low dose continuous infusion, OR high-dose intermittent infusion • Used for: Hematological malignancies only. Has no effect for solid tumors • –Toxicity is dose dependent called delayed toxicity, doesn’t appear as
acute toxicity • Myelosuppression • neurotoxicitiy as Cerebellar syndrome ( nystagmus, ataxia)
Basic Principles of Oncology Pharmacotherapy Treatment ANTIMETABOLITES Cytosine Analogs
• Gemcitabine • – Non-renal elimination • Used For: Originally approved for pancreatic cancer. Now used Non
Squamous Cell Lung cancer, Bladder & GI cancers • Adverse events- Myelosuppression (anemia), flu-like symptoms, rash

Basic Principles of Oncology Pharmacotherapy Treatment- ANTIMETABOLITES Purine Antagonists
• Purine antimetabolites: 6 mercaptopurine • Given orally, excreted in urine • Catabolized by thiopurine S-methyltransferase (TPMT)• Some people with genetic polymorphisms will have differing
pharmacokinetics • Allopurinol interaction • 6 mercaptopurine is used for : Acute lymphocytic and chronic
myelogenous leukemia • Toxicity: Myelosuppression, immunosuppression mild nausea, skin rash

Basic Principles of Oncology Pharmacotherapy Treatment-Folate Antimetabolites: Methotrexate (MTX)
• Inhibits dihydrofolate reductase ( DHFR) • Renal elimination and nephrotoxic { adjust dose, vigorous
hydration, and alkylation of urine} • Used for: Lymphoma, gastric, esophageal, bladder, ALL • MTX has wide variety of uses, namely psoriasis, rheumatoid
arthritis (immunosuppressant effects and doses vary) • Toxicity- Myelosuppression, N/V, mucositis; drug
interactions, diarrhea

Basic Principles of Oncology Pharmacotherapy Treatment-Folate Antimetabolites: Methotrexate (MTX)
• Activity is blocked by folinic acid (leucovorin)- used as rescue therapy after high MTX doses • Leucovorin is started at 24 hours and titrated to MTX levels

Alkylating & Heavy-Metals
• Oldest group• Alkylating: add group to DNA, inhibit replication• Heavy Metals: reactive platinum complex binds cell
Chemotherapy Examples
Alkylating&Heavy-Metals
Cyclofosphomide, Ifosfamide; Dacarbazine, Temoxolomide; BusulfanCisplatin, Carboplatin, Oxaliplatin

Basic Principles of Oncology PharmacotherapyTreatment- Alkylating agents and Heavy Metals
• Alkylating agents have direct vesicant effects and can damage tissues at the site of injection as well as produce systemic toxicity• Toxicities are usually dose related and occur particularly in rapidly
growing tissues such as bone marrow, GI tract, and reproductive system• Nausea and vomiting begin as early as 30-60 minutes after IV
injection with some of the alkylating agents

Basic Principles of Oncology PharmacotherapyTreatment- Alkylating agents and Heavy Metals
• Cyclophosphamide most widely used• Wide range of activity; given PO or IV• Toxicity: (12h) N/V, myelosuppression, leukopenia, thrombocyopenia,
alopecia, Hemorrhagic cystitis• Hemorrhagic cystitis– Activation of cyclophosphamide to cytotoxic
forms produces nephrotoxic substance (acrolein)• Prevent with vigorous hydration +/ - dose dependent MESNA ( 2
mercaptoethanesulfonate)

Basic Principles of Oncology PharmacotherapyTreatment- Alkylating agents and Heavy Metals
• Ifosphamide• More CNS toxicity and cystitis ALWAYS give MESNA• ALL, ( Acute lymphoblastic leukemia), lymphoma, breast, ovarian,
lung cancers• Busulfan:• Oral administration• Major specificity for granulocytes therefore great value in treatment
of chronic myelogenous leukemia

Basic Principles of Oncology PharmacotherapyTreatment- Alkylating agents and Heavy Metals
Heavy Metals( Platinum)
Efficacy Safety
CisplatinIV, Renal
Wide range V. High N/VNephrotoxic
CarboplatinIV, Renal
Ovary, lung, breastTesticular, esophagealhead & neck
Moderate N/VMore myelosuppression, Thrombocytopenia,otherwise less toxic vs CisplatinHypersensitivity
OxaliplatinIV
Colorectal CA Moderate N/VNeuropathy
Basic Principles of Oncology PharmacotherapyTreatment- Plant Alkaloids - Topoisomerases
• Epidophyllotoxin e.g. Etopside, Teniposide :• Cell cycle specific ( late S phase of cell cycle)• Inhibit topoisomerase II• Give divided doses over several days• Both are water insoluble and have to be formulated in Cremophor®
vehicle before use. (polyethoxylated castor oil)• IV over 30-60 minutes• Renal excretion• Myelosuppression, alopecia

Basic Principles of Oncology PharmacotherapyTreatment- Plant Alkaloids - Topoisomerases
• Teniposide use limited mainly to acute lymphoblastic leukemia
• Etopside has clinical activity in small cell and non small cell lung cancer, Hodgkin’s and Non-Hodgkins lymphomas, and gastric cancer and as high dose therapy for breast cancer

Basic Principles of Oncology PharmacotherapyTreatment- Anthracyclines
• Antibiotics- Topoisomerases• Doxorubicin (adriamycin)• (i)Inhibit Topo II (ii) generate free radicals (iii) binding and altering ion
transport (iv) Intercalating to DNA• Antitumor antibiotics

Basic Principles of Oncology PharmacotherapyTreatment- Anthracyclines
• Side effects- - Extravasations• Cardiotoxic: ( due to generation of free radicals)• Total cumulative dose to be calculated• Method or schedule of administration• Concurrent therapy• Pre existing heart disease• Previous use of other anthracyclines
Basic Principles of Oncology PharmacotherapyTreatment
• Daunorubicin still used in treatment of acute myeloid leukemia• Doxorubicin has a broad spectrum of clinical activity against
hematologic malignancies and a wide range of solid tumors- cancers of breast, endometrium, ovary, testicle, bladder, liver, lung• Administered IV• Metabolized extensively in the liver• Every three week schedule, alternative schedules:• Low dose weekly / 72-96 hour continuous infusions (identical efficacy,
less overall toxicity)

Basic Principles of Oncology PharmacotherapyTreatment- Tubulin Active Plant alkaloids
Mechanism: Inhibit tubulin polymerization, inhibit mitosis, halting cell division, thus bringing about cell death. Cell cycle specific for M phase
Hodgkins disease, Non-hodgkin’slymphomas,Vinblastine-breast cancerVincristine- combined with prednisonefor remission of pediatric ALL
VinblastineVincristine
Vinca alkaloids(Periwinkle plantVinca rosea)
Paclitaxel 1st line, Docetaxel 2nd lineAdvanced Breast, ovarian, NSCL andSCL, head and neck, esophageal,prostate, bladder cancers
PaclitaxelDocetaxel
Taxanes ( yew trees)

Basic Principles of Oncology Pharmacotherapy-Treatment- Tubulin Active Plant alkaloids
• Vincristine , Vinblastine- Hepatic elimination• Potent vesicant• Neurotoxicity , nausea vomiting, bone marrow• suppression, alopecia, paralytic ileus• Fatal if given intrathecal• Paclitaxel ,Docetaxel- Hepatobiliary route• Paclitaxel: hypersensitivity (premedicate with dexamethazone,
diphenhydramine, and a H 2 Blocker)• Peripheral Sensory neuropathy• Docetaxel: Neurotoxicity, fluid retention

Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents
• Miscellaneous• Bleomycin, Hydroxyurea, Tretinoin, Thalidomide,• Asparaginase

Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents• Bleomycin:• Hypersensitivity reactions ,fever• Pulmonary toxicity with cumulative doses < 400 IU• Used in Treatment of Hodgkins and non-hodgkins lymphoma, head
and neck cancer squamous cell cancer of the skin, cervix and vulva• Can be given subcutaneously, intramuscularly, or intravenously
Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents• L-Asparaginase• Unique mechanism- L asparaginase hydrolyzes aspargine to aspartic
acid and ammonia. Tumor cells lack asparagine synthetase, and require an exogenous
source of L-asparagine. Thus depletion of l-asparagine causes effective inhibition of protein synthesis• –Treatment: Acute Lymphocytic Leukemia & childhood Acute Myeloid
Leukemia.

Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents• Severe allergic reactions ( test dose before give IV)• Blood glucose abnormalities• Pancreatitis• Blood clotting abnormalities

Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents• Tretinoin & Thalidomide• – Tretinoin: retinoic acid syndrome (like pneumonia), Vitamin A
toxicity• Against acute promyelocytic leukemia {APL}• Thalidomide: used for Multiple Myeloma• Chemically unrelated, both severe teratogens
Basic Principles of Oncology PharmacotherapyTreatment- Miscellaneous Agents• Hydroxyurea: Analog of urea• This drug exerts its effects in the S-phase of the cell cycle, involves
inhibition of DNA synthesis• Administered orally (Almost 100% bioavailability)• Mainly used in chronic myelogenous leukemia and treatment of the
blast crises of acute myeloid leukemia• Also used as adjunct to radiation in cancers of head and neck, and
treating thrombocytosis and polycythemia vera

Basic Principles of Oncology PharmacotherapyTreatment- Endocrine Therapy
• Endocrine Therapy can be used to treat several common cancers, including breast, prostate, and endometrial cancers which arise from hormone sensitive tissues• These tumors grow in response to endogenous hormones that trigger
growth signals by binding to specific receptors located on a cell membrane or within cytoplasm of a cell• Current endocrine therapies inhibit tumor growth by blocking the
receptors or by eliminating the endogenous hormone feeding the tumor

Basic Principles of Oncology PharmacotherapyTreatment- Endocrine Therapy
• Interruption of hormonal secretion can also be achieved by surgical removal of hormone producing organs• Not all tumors arising from hormone sensitive tissues respond to
endocrine manipulation
Basic Principles of Oncology PharmacotherapyTreatment- Signal Transduction Pathway inhibitors
• By understanding the mechanisms by which cancer cells exhibit unregulated growth and immortality, and posses the ability to invade tissue and metastasize, it has been possible to design drugs to inhibit these processes• The following signaling pathways:• EGFR (epidermal growth factor receptor) ,• HER2/ NEU (Human Epidermal growth factor Receptor 2)• and VEGF (vascular endothelial growth factor) :

Basic Principles of Oncology PharmacotherapyTreatment- Signal Transduction Pathway inhibitors
• Epidermal Growth Factor Receptors (EGFR): HER-2• HER-2 over expressed in 30% of breast cancer ( aggressive disease,
high risk of relapse, poor survival)• Trastuzumab:• Recombinant humanized monoclonal antibody targeting HER-2• 4 different mechanisims• Standard of care for HER-2 + breast cancer• Distinctive toxicities• Cardiac and pulmonary

EEGFR, HER2/neu, VEGF Blocked or Inhibited by
Blocked by monoclonal antibodies that inhibit receptor tyrosine kinase
activation by binding to the extracellular domain
Small molecules that directly inhibit tyrosine kinase activation
by competing with ATP for binding to the intracellular
tyrosine kinase domain have been developed as well

Basic Principles of Oncology Pharmacotherapy Treatment • Because of their mechanism of action, their effects are exerted
primarily through inhibition of cell growth rather than cytotoxicity• Bone marrow suppression is not a frequent dose limiting factor of
signal transduction pathway inhibitors • Treatment regimens that incorporate the use of these class with
cytotoxic drugs are most likely to have the greatest impact on patient outcomes in cancer treatments

Basic Principles of Oncology Pharmacotherapy Treatment
• Angiogenesis inhibition: • Starve tumors of nutrients and oxygen • Not able to form new vessels • Act on migration, proliferation, differentiation and tubule formation • E.g. Bevacizumab is an antibody molecule

Current biologic response modifiers aim to bolster an individuals immune response, as well as provide a direct cytotoxic effect
Biologic response modifiers
Proteins ( Vaccines )
Antibodies (monoclonal and polyclonal)
Growth Factors

Basic Principles of Oncology Pharmacotherapy Treatment• Interferon-α - first recombinant cytokine to become available for the
treatment of cancer Interleukin -2 is a recombinantly reproduced lymphokine that has numerous immunoregulatory functions

Interferons
• Interferons are three families; each has different receptor structures • Type I consists of IFN- α and IFN- β • Type II comprises of IFN- γ • Type III, IFN- λ the newest discovered family, subtypes IFN- λ1, IFN-
λ2, IFN- λ3 exist• Type III Interferons could have distinct functions from Type I
Interferons

Interferons
• Type III INFs have multiple functions including antiviral, immunomodulatory, and anti-proliferative actions, and the majority of the actions overlap with those of the type I IFNs • Recombinant type I interferons have been tested for antitumour
effects against a variety of tumors in clinical settings • However limited efficacy partly due to toxicity in systemic
administrations

Tyrosine kinase inhibitors
• Imantib was the first in the class of tyrosine kinase inhibitors • Inhibits Bcr-Abl tyrosine kinase which results in apoptosis of Bcr-Abl
positive cells • Used for Chronic Myelogenous Leukemia • Dasatinib used for patients resistant to imantib

Tyrosine kinase inhibitors
• Erlotinib and Gefitinib • Inhibit tyrosine kinases associated with transmembrane surface
receptors • Therefore growth, invasion, metastasis, angiogensis, and resistance
to apoptosis cancerous cells • Used for: NSCLC • Toxicities: Diarrhea, rash, acne, NV, dry skin

Vaccines
• Vaccines • Cervical cancer is causally related to infection with human papilloma
virus (HPV) • This is a sexually transmitted virus • Theoritically, cervical cancer is a preventable disease • HPV subtypes 16 and 18 in particular are oncogenic or cause genital
warts • Vaccines to reduce incidence of HPV infection
Vaccines
• Gardasil- • The first HPV vaccine (quadrivalent) • Inactivated viral vaccine • Targets HPV types 6, 11,( cause genital warts) 16, and 18 Three
doses are given over a period of six months to females aged 9-26 years • Guidelines for administration to males are variable • CDC indicates routine administration for all boys aged 11-12 years

Vaccines
• Indicated for prevention of anal cancer caused by HPV types 6, 11, 16, 18, regardless of gender from age 9-26 years