getting the most from clinical data through physiological modelling & medical decision support...
Post on 19-Dec-2015
216 views
TRANSCRIPT

Getting the Most from Clinical Data through Physiological Modelling & Medical Decision Support
Bram Smith
Stephen Rees, Toke Christensen,
Dan Karbing, Steen Andreassen
Center for Model-based Medical Decision Support, Aalborg University, Denmark

Introduction
EXISTING TECHNOLOGY
• Clinical databases allowing easy, automated storage and retrieval of patient data.
• Medical equipment allowing data collection on a PC.
• Physiological models and decision support systems.
BUT:
• Doctors are still faced with interpreting large amounts of data to diagnose patients.
PROPOSED SOLUTION:
• An architecture that combines existing database technology with physiological models and decision support algorithms to assist clinicians in diagnosing and treating patients.

Systems architecture
• Clients on the architecture can be divided into 3 types:
– Inputs – User inputs, or data taken automatically from medical equipment.
– Interpretation – Uses equations and physiological models to expand knowledge about the patient.
– Decision support – Uses decision support algorithms to assisting in choosing suitable treatment strategies.
DatabaseDatabase
InputsVentilator (Paw, Flow,…)Gas analysis (O2, CO2)Clinical monitor (ECG, HR,…)
InputsVentilator (Paw, Flow,…)Gas analysis (O2, CO2)Clinical monitor (ECG, HR,…)
InterpretationMetabolic (VO2, VCO2,…)Lung (Shunt, V/Q,…)Blood (Base excess, DPG,…)
InterpretationMetabolic (VO2, VCO2,…)Lung (Shunt, V/Q,…)Blood (Base excess, DPG,…)
Decision supportMonitoringVentilator controlGlucose regulation
Decision supportMonitoringVentilator controlGlucose regulation
Architecture is compartmentalised to allow independent development of each client.

Input clients
• Many monitors allow data logging on a computer for automated data collection.
• The user interface also allows clinicians to add data that can not be logged automatically.
DatabaseDatabase
ECG,SaO2,…
CO2,Vt,...
CO, MAP,…
ALL data input is written to the database.
Vt, Paw, …Values,Events

Interpretation clients
• Physiological models and more basic calculations are carried out on data in the database to determine more abstract measurements or patient condition and extend the knowledge of the patient.
• Some clients can be automatic, carrying out calculations when ever new data is available, while more complex clients may require user control.
DatabaseDatabase
Body surface area
Body surface area
WeightHeight
BSA
Cardiac Index
Cardiac Index
BSACO
CI
Oxygen Consumption
Oxygen Consumption
FetO2,
Vt,…VO2
ALPEALPE
VO2,
CI,…Shunt,PO2
Automatic Requires user control
Decision support clients
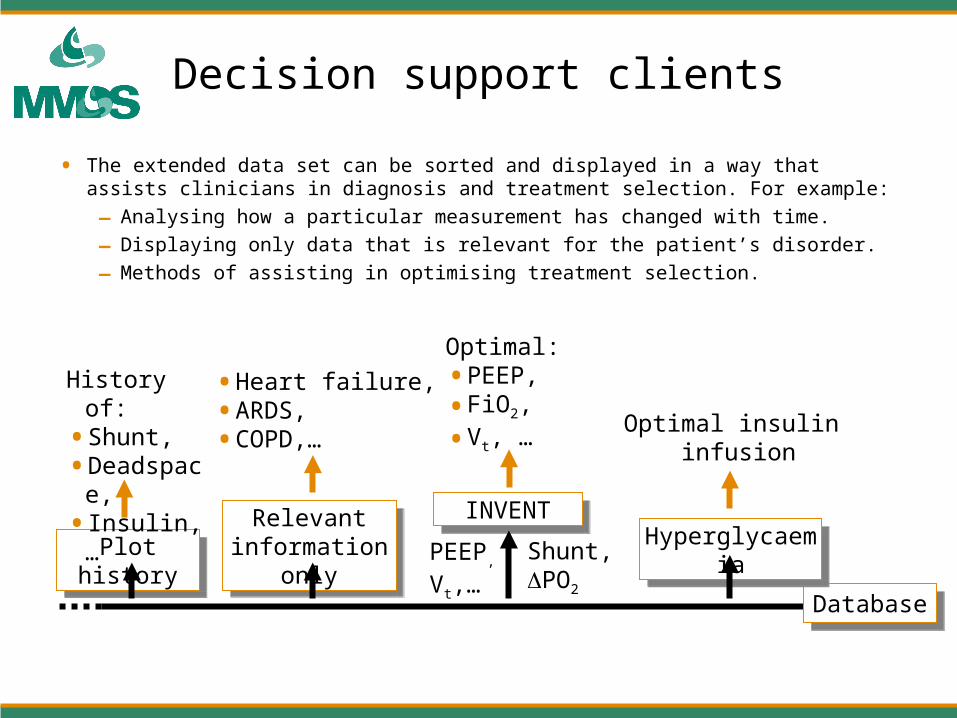
• The extended data set can be sorted and displayed in a way that assists clinicians in diagnosis and treatment selection. For example:
– Analysing how a particular measurement has changed with time.
– Displaying only data that is relevant for the patient’s disorder.
– Methods of assisting in optimising treatment selection.
DatabaseDatabase
Plot historyPlot historyRelevant
information only
Relevant information only
INVENTINVENT
PEEP,
Vt,…Shunt,PO2
HyperglycaemiaHyperglycaemia
Optimal insulin infusion
• Heart failure,• ARDS,• COPD,…
History of:• Shunt,• Deadspace,• Insulin,…
Optimal: • PEEP,
• FiO2,
• Vt, …
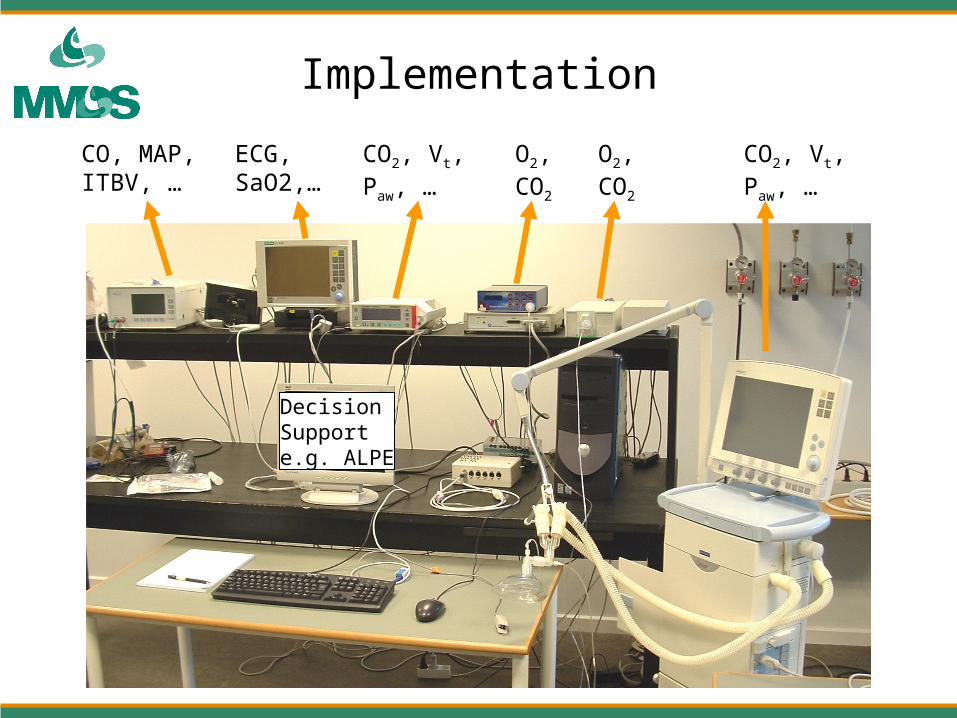
Implementation
CO, MAP, ITBV, …
ECG,SaO2,…
CO2, Vt, Paw, …
O2, CO2
O2, CO2
CO2, Vt,Paw, …
DecisionSupport e.g. ALPE
Conclusions
• A generic architecture has been implemented for development of new calculation methods, physiological models and decision support systems.
• The compartmental design means that clients can be developed and function independently, yet interact if possible to improve functionality (eg, cardiopulmonary interaction, VO2).
• This architecture presents a method for moving information systems from audit to clinical support tools, through:
– Calculation of abstract representations of patient condition (e.g. cardiac index, shunt).
– Assistance in interpreting patient information and choosing optimal treatment strategies (e.g. optimising ventilator settings).