glenn yiu, hms-iii gillian lieberman, mderadiology.bidmc.harvard.edu/learninglab/central/yiu.pdf ·...
TRANSCRIPT
Glenn Yiu, HMS-IIIGillian Lieberman, MD
Glenn YiuGillian Lieberman, MD
Imaging of the Orbit
March 2007
History: •
53 y/o
male with type II DM and history of
proptosis, who presents with visual complaints in the right eye
Exam: •
Bilateral proptosis
L>R
•
Visual acuity normal•
No relative afferent pupillary
defect bilaterally
•
Optic cup enlargement in R eye
Our Patient GB
Glenn YiuGillian Lieberman, MD
Inflammation/Infection•
Orbital pseudotumor
•
Thyroid ophthalmopathy•
Sarcoid
•
Orbital cellulitis•
Abscess
Glenn YiuGillian Lieberman, MD
Differential DiagnosisNeoplastic
•
Lymphoma•
Dermoid
•
Metastases
Vascular•
Hemangioma
•
Vascular malformations
RULE OUT:
• lid lag• relative enophthalmos• external swelling

Glenn YiuGillian Lieberman, MD
Orbit Anatomy
(Wichmann & Muller-Forell, Eur
J Radiol. 2004)
Eyeball
Zygomaticbone
Lateral rectus
Intraconal
fat
Optic nerve
Extraconal
fat
Medial rectus
Annulus of Zinn
Ethmoid
sinus
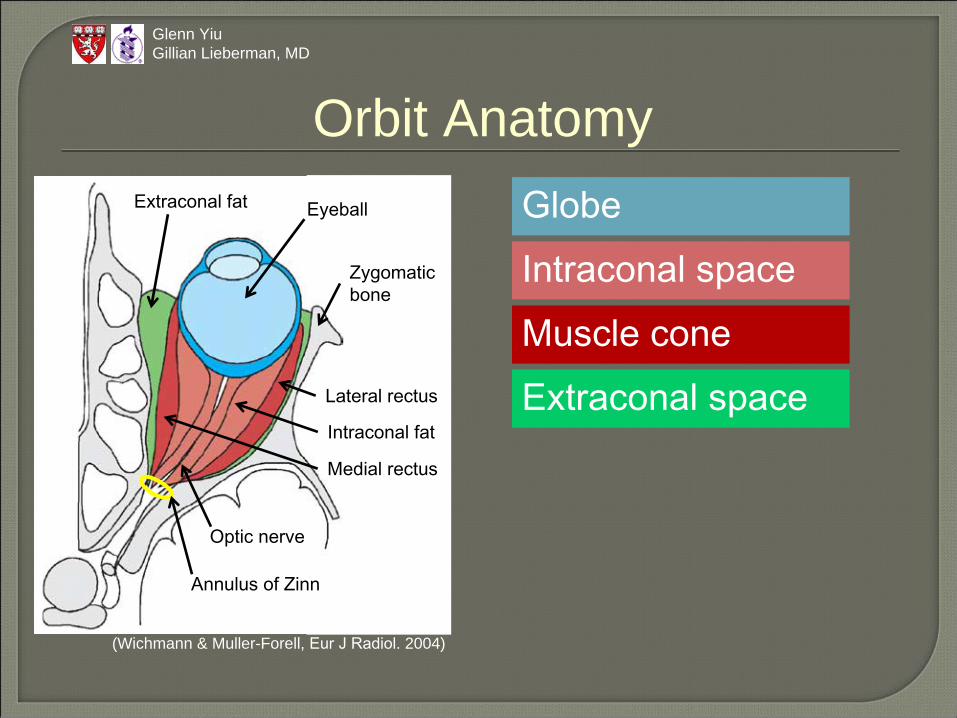
Globe
Glenn YiuGillian Lieberman, MD
Orbit AnatomyEyeball
Zygomaticbone
Lateral rectus
Intraconal
fat
Optic nerve
Extraconal
fat
Medial rectus
Annulus of Zinn
Intraconal
space
Muscle cone
Extraconal
space
(Wichmann & Muller-Forell, Eur
J Radiol. 2004)

Globe
Glenn YiuGillian Lieberman, MD
Orbit AnatomyEyeball
Zygomaticbone
Lateral rectus
Intraconal
fat
Optic nerve
Extraconal
fat
Medial rectus
Annulus of Zinn
Intraconal
space
Muscle cone
Extraconal
space
Optic nerve gliomaMeningiomaVarix
Orbital pseudotumorThyroid ophthalmopathy
Orbital cellulitis(Wichmann & Muller-Forell, Eur
J Radiol. 2004)
Glenn YiuGillian Lieberman, MD
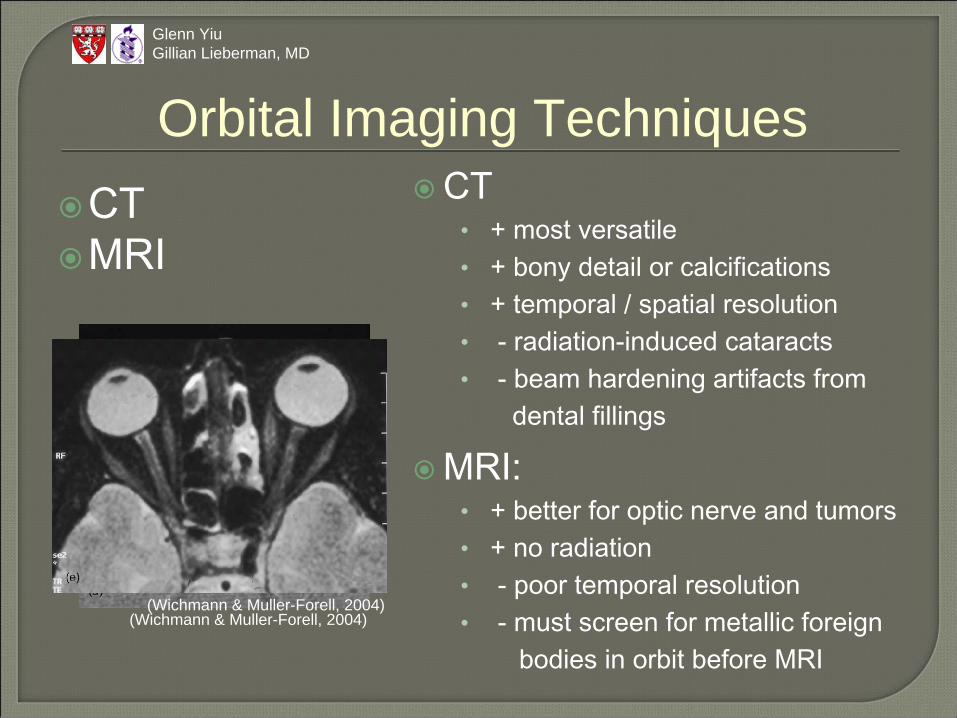
Orbital Imaging TechniquesCTMRI
CT•
+ most versatile•
+ bony detail or calcifications•
+ temporal / spatial resolution•
-
radiation-induced cataracts•
-
beam hardening artifacts from dental fillings
MRI:•
+ better for optic nerve and tumors•
+ no radiation•
-
poor temporal resolution•
-
must screen for metallic foreign bodies in orbit before MRI
(Wichmann & Muller-Forell, 2004)(Wichmann & Muller-Forell, 2004)
Glenn YiuGillian Lieberman, MD
Orbital Imaging TechniquesCTMRIUltrasoundPlain filmAngiography
Angiography:•
good for vascular malformations and vascularized
tumors•
invasive and time-consuming
Plain film:•
mainly for screening for metallic foreign bodies before MRI
•
useless for soft tissue details
Ultrasound:•
good for lesions within globe or foreign bodies in orbit
•
poor penetration

Glenn YiuGillian Lieberman, MD
Orbit Anatomy on CT
(Wichmann & Muller-Forell, Eur
J Radiol., 2004)
1.
Zygomatic
bone2.
Nasal septum3.
Lacrimal
gland4.
Sclera5.
Vitreous body6.
Optic nerve7.
Medial rectus8.
Lateral rectus9.
Superior orbital fissure10.
Optic canal11.
Pituitary gland12.
Ethmoid
sinus13.
Sphenoid sinus
123 4 5
67
8
910
11
12
13
Glenn YiuGillian Lieberman, MD
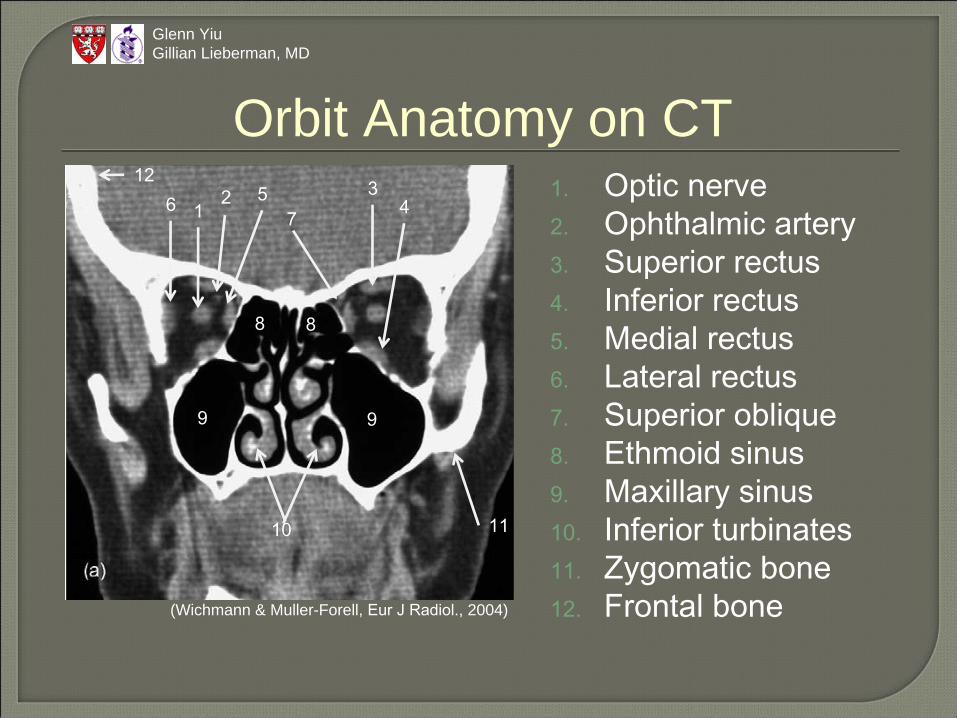
Orbit Anatomy on CT
(Wichmann & Muller-Forell, Eur
J Radiol., 2004)
1.
Optic nerve2.
Ophthalmic artery3.
Superior rectus4.
Inferior rectus5.
Medial rectus6.
Lateral rectus7.
Superior oblique8.
Ethmoid
sinus9.
Maxillary sinus10.
Inferior turbinates11.
Zygomatic
bone12.
Frontal bone
12
73
456
9 9
10
8 8
12
11
Glenn YiuGillian Lieberman, MD
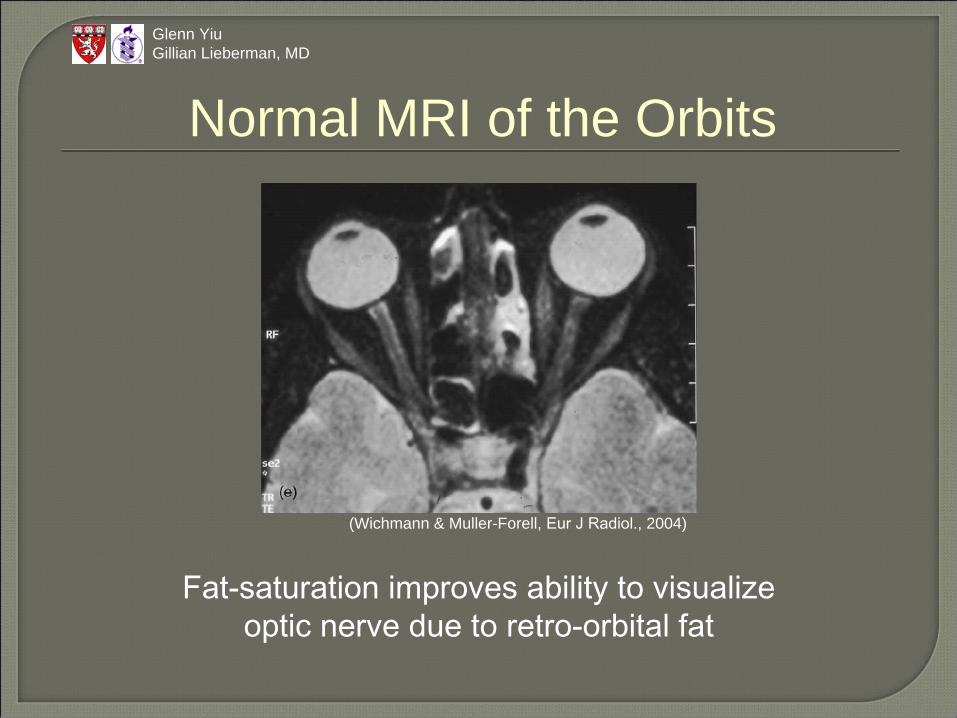
Normal MRI of the Orbits
(Wichmann & Muller-Forell, Eur
J Radiol., 2004)
Fat-saturation improves ability to visualizeoptic nerve due to retro-orbital fat
Axial and coronalnon-contrast CT of orbits
Radiological findings: Our Patient GB
Glenn YiuGillian Lieberman, MD

(Wichmann & Muller-Forell, 2004)
Normal
Glenn YiuGillian Lieberman, MD
Bilateral proptosis
(PACS, BIDMC, 2007)
Patient GB’s Findings on Axial CT

Glenn YiuGillian Lieberman, MD
Extra-occular muscle enlargement
(PACS, BIDMC, 2007)
* **
*
* *
Bilateral enlargement of all extra-occularmuscles, including superior obliques
Patient GB’s Findings on Coronal CT

Glenn YiuGillian Lieberman, MD
Extra-occular muscle enlargement
(PACS, BIDMC, 2007)
* *
Bilateral enlargement of all extra-occularmuscles, including superior obliques
Center enlargement with no involvement of tendons
Patient GB’s Findings on Axial CT

Glenn YiuGillian Lieberman, MD
Normal fat
(PACS, BIDMC, 2007)
* *
* *
No fat stranding
Patient GB’s Findings on Axial/Coronal CT

Glenn YiuGillian Lieberman, MD
Grave’s Ophthalmopathy
(PACS, BIDMC, 2007)
Proptosis
Extra-occular muscle enlargement
Central enlargement with sparing of tendons
I’M SLow (inferior, medial, superior, & lateral rectus)
Patient GB’s Findings on Axial CT
Glenn YiuGillian Lieberman, MD
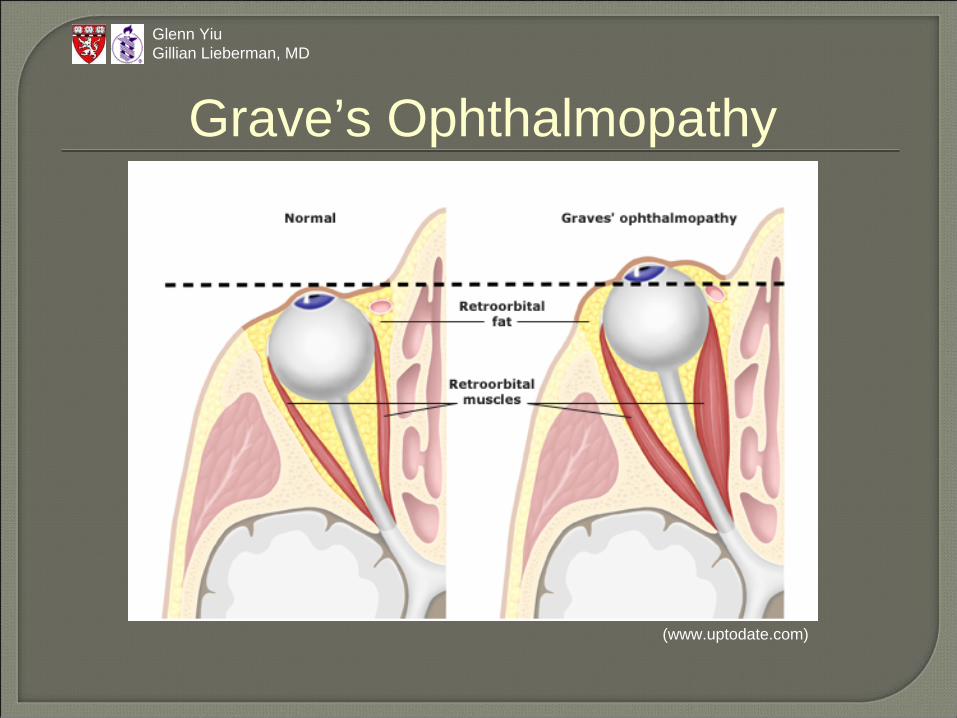
Grave’s Ophthalmopathy
(www.uptodate.com)

Glenn YiuGillian Lieberman, MD
Grave’s Ophthalmopathy: Pathogenesis
An autoimmune disease of retroorbital tissues that occurs in 20-25% of patients with Graves’ disease, more often in women than in men.
Antibodies activate TSH receptors not only in thyroid tissue, but also in orbital fibroblasts and adipocytes.
T-cell activation stimulates secretion of glycosamino-glycans (GAG), mostly hyaluronic acid, resulting in increased volume of both extraocular muscles and retroorbital connection/adipose tissues.
Risk factors include genetics, female sex, smoking, and radioiodine therapy.
Glenn YiuGillian Lieberman, MD
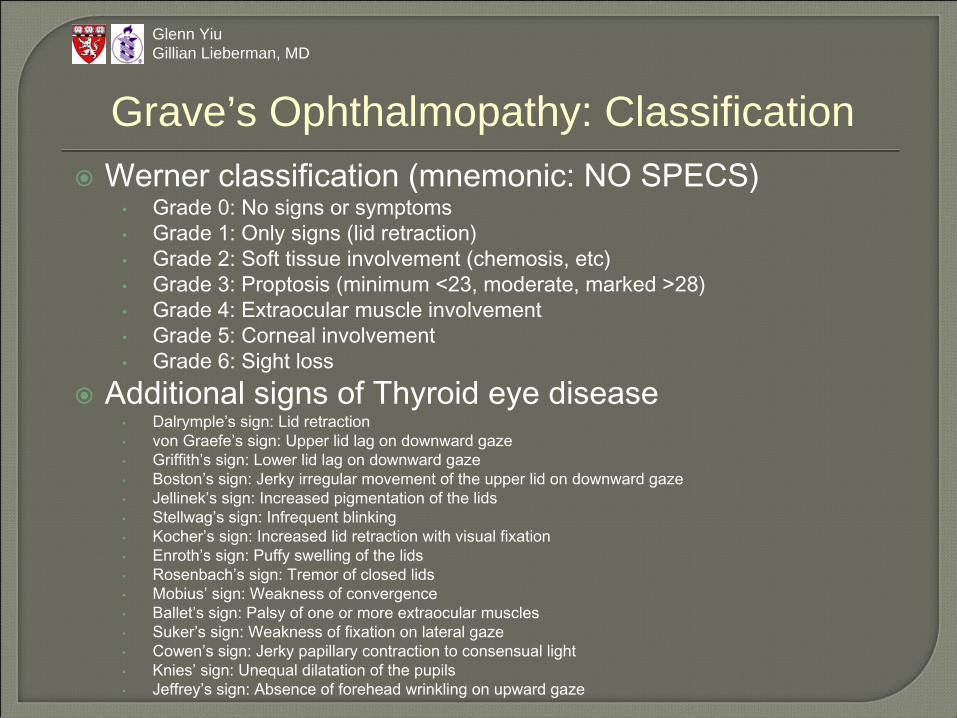
Grave’s Ophthalmopathy: ClassificationWerner classification (mnemonic: NO SPECS)
•
Grade 0: No signs or symptoms•
Grade 1: Only signs (lid retraction)•
Grade 2: Soft tissue involvement (chemosis, etc)•
Grade 3: Proptosis
(minimum <23, moderate, marked >28)•
Grade 4: Extraocular
muscle involvement•
Grade 5: Corneal involvement•
Grade 6: Sight lossAdditional signs of Thyroid eye disease
•
Dalrymple’s
sign: Lid retraction•
von Graefe’s
sign: Upper lid lag on downward gaze•
Griffith’s sign: Lower lid lag on downward gaze•
Boston’s sign: Jerky irregular movement of the upper lid on downward gaze•
Jellinek’s
sign: Increased pigmentation of the lids•
Stellwag’s
sign: Infrequent blinking•
Kocher’s sign: Increased lid retraction with visual fixation•
Enroth’s
sign: Puffy swelling of the lids•
Rosenbach’s
sign: Tremor of closed lids•
Mobius’
sign: Weakness of convergence•
Ballet’s sign: Palsy of one or more extraocular
muscles•
Suker’s
sign: Weakness of fixation on lateral gaze•
Cowen’s sign: Jerky papillary contraction to consensual light•
Knies’
sign: Unequal dilatation of the pupils•
Jeffrey’s sign: Absence of forehead wrinkling on upward gaze

(PACS, BIDMC, 2007)
Glenn YiuGillian Lieberman, MD
Grave’s Ophthalmopathy: TreatmentGlucocorticoid therapyExternal orbital radiationOrbital decompression surgery
Patient GB was s/porbital decompression
Patient GB’s Findings on Axial CT

Glenn YiuGillian Lieberman, MD
Differential DiagnosisInflammation/Infection
•Orbital pseudotumor•Thyroid ophthalmopathy•Sarcoid•Orbital cellulitis•Abscess
Neoplastic•Lymphoma•Dermoid•Metastases
Vascular•Hemangioma•Vascular malformations

Glenn YiuGillian Lieberman, MD
Orbital Pseudotumor
(Courtesy of Fabio Komlos, BIDMC)
Inflammation/Infection•Orbital pseudotumor•Thyroid ophthalmopathy•Sarcoid•Orbital cellulitis•Abscess
Neoplastic•Lymphoma•Dermoid•Metastases
Vascular•Hemangioma•Vascular malformations
*
Fat strandingTendon not spared
Companion Patient Findings on Axial/Coronal CT

Glenn YiuGillian Lieberman, MD
Inflammation/Infection•Orbital pseudotumor•Thyroid ophthalmopathy•Sarcoid•Orbital cellulitis•Abscess
Neoplastic•Lymphoma•Dermoid•Metastases
Vascular•Hemangioma•Vascular malformations
Preseptal & Postseptal Cellulitis
(Caruso et al., Radiology, 2006)
Unilateral Sinus involvement
Companion Patient Findings on Axial CT
Glenn YiuGillian Lieberman, MD
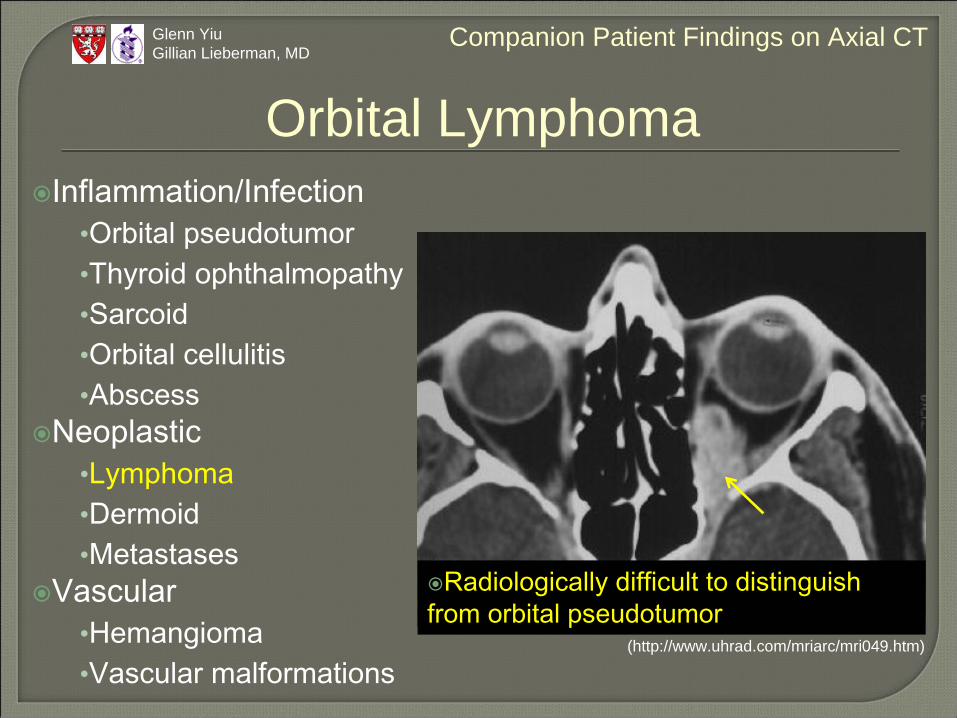
Orbital Lymphoma
(http://www.uhrad.com/mriarc/mri049.htm)
Inflammation/Infection•Orbital pseudotumor•Thyroid ophthalmopathy•Sarcoid•Orbital cellulitis•Abscess
Neoplastic•Lymphoma•Dermoid•Metastases
Vascular•Hemangioma•Vascular malformations
Radiologically difficult to distinguish from orbital pseudotumor
Companion Patient Findings on Axial CT

Glenn YiuGillian Lieberman, MD
Cavernous Hemangioma
(http://mni.mcgill.ca/neuroimage/nov2001/nov2001_p6.htm)
Inflammation/Infection•Orbital pseudotumor•Thyroid ophthalmopathy•Sarcoid•Orbital cellulitis•Abscess
Neoplastic•Lymphoma•Dermoid•Metastases
Vascular•Hemangioma•Vascular malformations
Well-defined massProgressive peripheral to
center enhancement post-gado
Companion Patient Findings on MRI
Agarwal A. Handbook of Ophthalmology. 2006.Aviv RI, Casselman J. Orbital imaging: Part 1. Normal anatomy. Clin Radiol. 2005 Mar;60(3):279-87. Aviv RI, Miszkiel K. Orbital imaging: Part 2. Intraorbital pathology. Clin Radiol. 2005 Mar;60(3):288-307. Belden CJ, Zinreich SJ. Orbital imaging techniques. Semin Ultrasound CT MR. 1997 Dec;18(6):413-22. Braffman BH, Naidich TP, Chaneles M. Imaging anatomy of the normal orbit. SeminUltrasound CT MR. 1997 Dec;18(6):403-12. Caruso PA, Watkins LM, Suwansaard P, Yamamoto M, Durand ML, Romo LV, Rincon SP, Curtin HD. Odontogenic orbital inflammation: clinical and CT findings--initial observations. Radiology. 2006 Apr;239(1):187-94. Davies TF. Pathogenesis and clinical features of Graves’ ophthalmopathy(orbitopathy). www.uptodate.com.Davies TF. Treatment of Graves’ ophthalmopathy (orbitopathy). www.uptodate.com.Wichmann W, Muller-Forell W. Anatomy of the visual system. Eur J Radiol. 2004 Jan;49(1):8-30.
References
Glenn YiuGillian Lieberman, MD

Fabio Komlos, MDMichael Geary, MDGillian Lieberman, MD
Pamela LepkowskiLarry Barbaras
Acknowledgements
Glenn YiuGillian Lieberman, MD