glutathione s-transferases and cytochrome p450 detoxifying enzyme distribution in human cerebral...
TRANSCRIPT

Journal of Neuro-Oncology 25: 1-7, 1995. �9 1995 Kluwer Academic Publishers. Printed in the Netherlands.
Laboratory Investigation
Glutathione S-transferases and cytochrome P450 detoxifying enzyme distribution in human cerebral glioma
Robert Grant 1 and James W. Ironside 2 1 Department of Clinical Neurosciences, Western General Hospital, Edinburgh, UK; : Neuropathology Lab- oratory, University Department of Pathology, Western General Hospital, Edinburgh, UK
Key words: glioma, glutathione S-transferase, cytochrome P450, chemotherapy
Abstract
Malignant astrocytomas are frequently resistant to cytotoxic chemotherapy A possible mechanism of chemo- resistance is drug inactivation within malignant astrocytes by detoxifying enzymes (glutathione transferases (GST) and cytochrome P450's). The aim of this study was to assess whether there was differential expression of these detoxifying enzymes in the central nervous system and any relationship to histological grade (WHO) of the tumours.
Immunostaining was performed in 30 consecutive glioma samples, using class specific polyclonal antibodies to subtypes of GST (pi, alpha, mu) and to human cytochrome P450 reductase.
GST immunostaining was evident in astrocytes and endothelium but not neurones or oligodendrocytes in normal brain. Immunostaining for GST increased in intensity from well differentiated tumours to glioblasto- ma. Staining was least evident in surrounding normal brain, strong in reactive astrocytes and astrocytic tu- mour cells and very intense in gemistocytic and giant tumour cells. Small anaplastic tumour cells had very little GST staining. Where endothelial proliferation was evident, GST staining in endothelial cells was increased. Pi was always the predominant subclass, although GST alpha and mu were also expressed in some tumours.
Cytochrome P450 reductase immunostaining was present in normal neurones and malignant astrocytes. Gemistocytic astrocytic tumour cells stained intensely Further work is necessary to see if there is any correla- tion between immunostaining intensity survival or response to chemotherapy.
Introduction
Cerebral gliomas are one of the most chemoresist- ant tumours found in man. There are several pos- sible mechanisms of intrinsic cytotoxic drug resist- ance [1, 2]. Molecular mechanisms such as multi- drug resistance due to the overexpression of P gty- coprotein, an energy dependent drug efflux pump [3], or inactivation and increased intracellular me- tabolism due to detoxifying enzymes. Intracellular drug inactivation or metabolism may be as a result of increased concentrations of detoxifying enzymes such as .to glutathione S-transferase (GST's) or cy-
tochrome P450's. Glutathione S-transferases are multifunctional proteins found in the cytoplasm of most human tissues that catalyse the conjugation of glutathione with various electrophiles, including some anti-cancer drugs. They are known to partici- pate in the mechanisms of chemoresistance to cer- tain cytotoxic drugs including nitrosoureas [4-6]. Concentrations of GST in resistant glioma cell lines are increased when compared with the parent cell line [7] and expression of GST pi has been reported to correlate with the degree of resistance to BCNU in malignant astrocytoma cell lines.
Carder et aL [8] have studied GST expression in

2
normal and developing brain and Strange et aL [9] have used chromatofocusing of some glioma sam- ples to measure GST expression. The cytochrome P450's are multifunctional oxidases found in mito- chondria and microsomes that also play a role in de- toxification of certain cytotoxic agents. Cyto- chrome P450 enzyme distribution in human glio- mas has not yet been reported.
The aim of this study was to assess whether there was any differential expression of these detoxifying enzymes in the central nervous system and to study expression related to grade of malignancy in a series of surgically sampled gliomas.
Methods
Brain tumour samples
Paraffin embedded tumour samples from 30 con- secutive patients with different grades of cerebral glioma were identified in the Neuropathological Laboratory. Histological interpretation of tumour type, grade and descriptive analysis of the staining pattern was performed by JI; Distribution and in- tensity of immunostaining were arbitrarily graded by RG and JI. Tumours were graded as well differ- entiated astrocytoma, anaplastic astrocytoma or glioblastoma multiforme based on the revised WHO classification [10]. Fourteen patients had glioblastoma multiforme, 7 had anaplastic astrocy- toma and 9 had well differentiated astrocytoma. Twenty nine specimens were from the first ever op- erative procedure and one was taken at the time of relapse. The latter patient was the only one to have received radiation therapy. Twenty one patients
Table 1. Primary antibody dilutions and incubation details
were male and 9 female of age range 15 to 74 years (median 45 years).
Immunohistochemistry staining techniques
a) Glutathione S-transferase immunostaining tech- nique Immunohistochemistry was performed on paraffin embedded sections, using the avidin biotin perox- idase (ABC kit; Dako Ltd., High Wicombe, Bucks, U.K.). Five micron sections were cut from the paraf- fin wax blocks and dewaxed with alcohol. Sections were treated with 3 % hydrogen peroxide in metha- nol for 30 min to block endogenous peroxidase ac- tivity, then washed three times with Tris buffered saline (pH 7.6) with 0.02% Tween (TBST). The tis- sue sections were not pre-treated with trypsin. Sec- tions were then treated with 20% normal swine se- rum (NSS) (Sigma Chemical Co. Ltd., Poole Dor- set, U.K.) for 10 min (Dilution 1:5 NSS/TBS). The tissue sections were then incubated with primary antibody. Dilution and incubation times are shown in Table 1. After three further 5 min washes with TBST, sections were incubated in biotinylated swine anti-rabbit immunoglobulin (Dako Ltd., High Wicombe, Bucks. U.K.) (Dilution 1:200 in 1:5 NSS/TBS) for 30 min. Normal swine serum (20%) was used in place of primary antibody for negative controls. After two further TBST rinses, the sec- tions were incubated for 30 min with Avidin Biotin Complex. After two further rinseswith Tris buf- fered saline (TBS pH 7.6). The sections were then developed using diaminobenzidine (DAB) (Sigma Chemical Co. Ltd., Poole Dorset, U.K.) incorporat- ing 0.01 M imidazole in Tris HC1 buffer pH 7.6. Sec-
Antibody Nature Dilution Incubation
GST pi Rabbit polyclonal 1:400 30 min; room temp GST alpha Rabbit polyclonal 1:200 30 min; room temp GST mu Rabbit polyclonal 1:200 30 min; room temp P450 red Rabbit polyclonal 1:100 Overnight: - 4 ~ C
GST = Glutathione S-transferase, P450 = Cytochrome P450 reductase, min = minutes, temp = temperature, C = Celsius. (All primary antibodies were kindly supplied by Dr. J.D. Hayes and Prof. C.R. Wolf, Imperial Cancer Research Fund, Molecular Pharma-
cology Lab, Ninewells Hospital).
tions were then washed in water for 5 min and coun-
terstained in Mayer 's haematoxylin, washed in wa-
ter then dehydrated and mounted.
Cytochrome P450 reductase staining technique
A similar technique was used for the cytochrome
P450 reductase immunostaining, but the sections
were incubated with primary antibody overnight at
- 4 ~ The tissue sections were not pre-treated with
trypsin.
Immunostaining assessment
We used the ABC technique because of its high sen-
sitivity at determining the presence of these en-
zymes in brain tumours and to record the distribu-
tion of immunostaining within each tumour, with
regard to the highly heterogenous tumour cell pop-
ulations. Each section was subjectively scored on
staining distribution in the most evident immunos-
tained section, taking into account any variations in
staining intensity, as: 0 = no immunostaining,
+ =mild (focal) immunostaining, ++ = moderate
distribution of immunostaining, t i t = marked (widespread) immunostaining.
Resul t s
Descriptive analysis a) GST immunostaining GST pi immunostaining was present in astrocytes
and endothelium but not neurones or oligodendro-
cytes. Staining was least evident in surrounding
'normal ' brain, strong in 'reactive' astrocytes (Fig.
la) and astrocytic tumour cells and very intense in
gemistocytic and giant tumour cells (Fig. lb). Small
anaplastic tumour cells had very little staining.
Where endothelial proliferation was evident, GST
staining in endothelial cells was increased (Fig. lc).
GST pi was always the predominant subclass, al-
though GST alpha and mu were also expressed in some tumours.
b) Cytochrome [450 immunostaining Cytochrome P450 reductase was most conspicuous
in neurones and axons. There was minimal staining
in some reactive astrocytes and tumour cells and ve-
ry intense staining in gemistocytic astrocytes (Fig. ld).
Immunostaining intensity a) Glutathione S-transferases Immunostaining for GST pi, increased in intensity
from well differentiated tumours to glioblastoma
(Table 2). All sections histologically graded as glio-
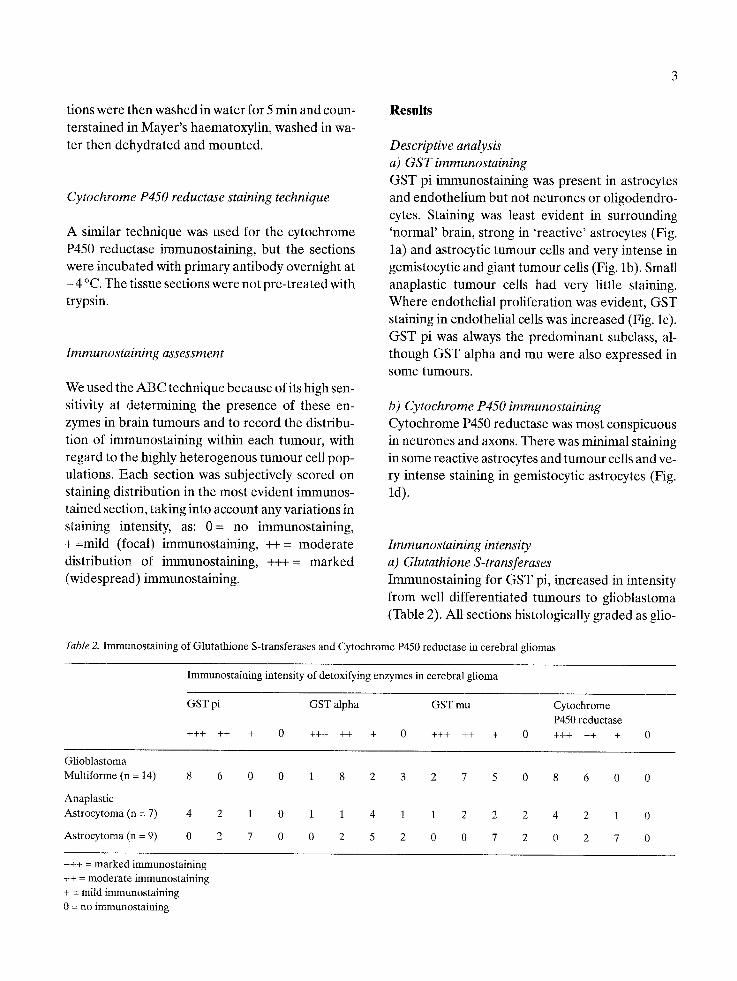
Table 2. Immunostaining of Glutathione S-transferases and Cytochrome P450 reductase in cerebral gliomas
Immunostaining intensity of detoxifying enzymes in cerebral glioma
GST pi GST alpha GST mu Cytochrome P450 reductase
+++ ++ + 0 +++ ++ + 0 +++ ++ + 0 +++ ++ + 0
Glioblastoma Multiforme (n = 14) 8 6 0 0 1 8 2 3 2 7 5 0 8 6 0 0
Anaplastic Astrocytoma (n = 7) 4 2 1 0 1 1 4 1 1 2 2 2 4 2 1 0
Astrocytoma (n = 9) 0 2 7 0 0 2 5 2 0 0 7 2 0 2 7 0
+++ = marked immunostaining ++ = moderate immunostaining + = mild immunostaining 0 = no immunostaining
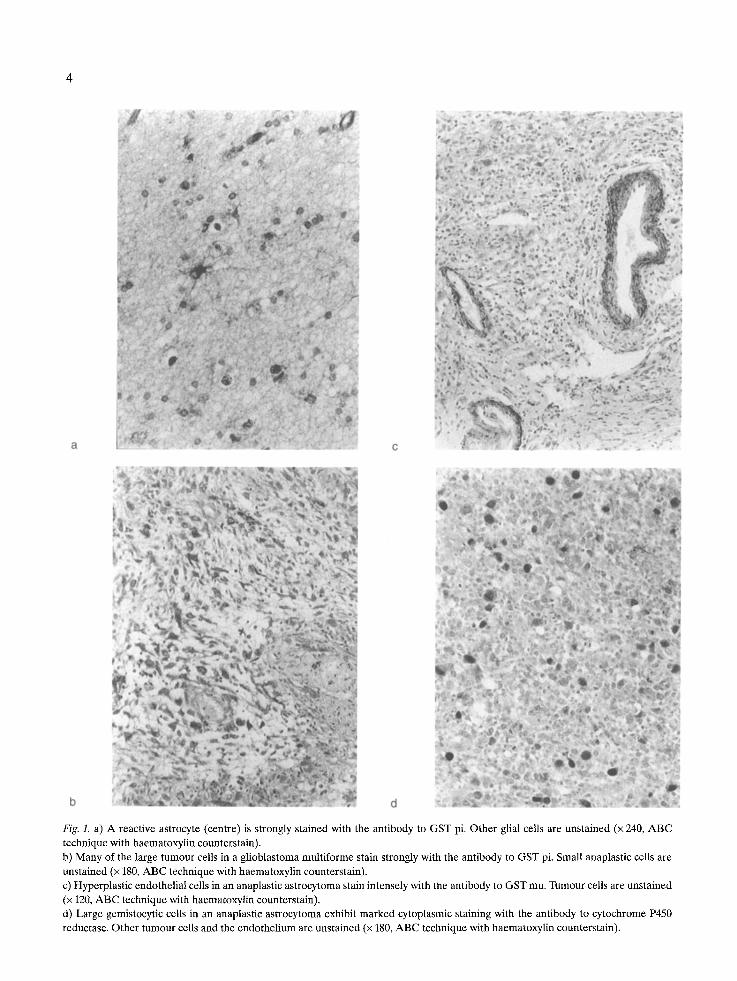
Fig. 1. a) A reactive astrocyte (centre) is strongly stained with the antibody to GST pi. Other glial cells are unstained (x 240, ABC technique with haematoxylin counterstain). b) Many of the large tumour cells in a glioblastoma multiforme stain strongly with the antibody to GST pi. Small anaplastic cells are unstained (x 180, ABC technique with haematoxylin counterstain). c) Hyperplastic endothelial cells in an anaplastic astrocytoma stain intensely with the antibody to GST mu. Tumour cells are unstained (x 120, ABC technique with haematoxylin counterstain). d) Large gemistocytic cells in an anaplastic astrocytoma exhibit marked cytoplasmic staining with the antibody to cytochrome P450 reductase. Other turnout cells and the endothelium are unstained (x 180, ABC technique with haematoxylin counterstain).
blastomas and 86% of sections graded as anaplastic astrocytoma had moderate or marked immunos- taining in malignant astrocytes or endothelium us- ing GST pi antibody. Seventy eight percent of pa- tients with well differentiated astrocytoma had only mild immunostaining with GST pi. There was quite a wide variation in immunostaining intensity with GST alpha and GST mu and histological tumour grading.
b) Cytochrome P450 reductase Immunostaining intensity also tended to increase with tumour grade. All GBM sections and 86% of anaplastic astrocytoma sections had marked or moderate immunostaining intensity whereas 55% of well differentiated astrocytomas had mild or no immunostaining with cytochrome P450 reductase (Table 2).
Discussion
Malignant gliomas (glioblastoma multiforme and anaplastic astrocytoma) are refractory to most forms of chemotherapy [11], although, some pre- dominantly young patients will have a clinical and radiological response to chemotherapy for a limited period [12]. Age at the time of chemotherapy is cer- tainly an important factor, irrespective of the tu- mour grade; other reasons why some patients re- spond and others do not remain unclear. Any meth- od that would help predict which patients are likely to respond to chemotherapy would be a significant advance in management. Molecular mechanisms such as the central role of GST's and cytochrome P450's in detoxification raises the possibility that differences in GST and cytochrome P450 expres- sion may give rise to differences in chemoresistance to nitrosoureas.
It is widely accepted that the multi-drug resist- ance gene (MDRI), which is expressed in some hu- man glial tumours, confers resistance to certain che- motherapy agents (alkaloids, anthracyclines and antibiotics) [3]. There is increasing circumstantial, as well as genetic evidence which indicates that glu- tathione transferases (GST's) and cytochrome P450's are also determinants in the sensitivity of tu-
mour cells to anticancer drugs, particularly nitro- soureas [13, 14]. 1,3-Bis(2-chloroethyl)-l-nitrosou- rea (BCNU) is the most commonly used nitrosou- rea in treatment of malignant astrocytomas. BCNU is inactivated by a glutathione dependent denitro- sation reaction [15,16] and increased levels of GST activity play a major role in chlorambucil resistance [17] and adriamycin resistance [18]. In laboratory experiments certain tumours that develop drug re- sistance overexpress GST. Intracellular GST is pre- sent in resistant tumours up to 40 times that of che- mosensitive cells, and the increase may not be sub- type specific [19, 20]. Studies have demonstrated an elevation in GST expression in drug resistant glio- ma cell lines [7, 21]. All three classes of cytosolic GST have been shown to be overexpressed in cell lines resistant to cytotoxic agents [2]. In breast can- cer, a correlation of erythrocyte GSH concentra- tion with response rate to chemotherapy suggests that this measurement may be helpful in predicting the response to therapy [22]. An alternative view is that pi class GST may simply act as a marker for neoplastic lesions and simply reflects the degree of cellular damage [23].
We have confirmed that GST pi immunostaining is evident in human astrocytes and endothelium but not neurones or oligodendrocytes and that immu- nostaining for GST, increased in intensity from well differentiated tumours to glioblastomas. While we did observe a variability in intensity of immunos- taining within different cell types (e.g. between re- active astrocytes and large gemistocytic tumour cells) which might reflect the relative quantity of enzyme present in these cells, we wish to emphasise that the ABC technique is highly sensitive but it can not be used as a semiquantitative estimation of en- zyme load in the cells. There is also GST immunos- taining within proliferation vascular endothelium. As in previous studies GST pi was always the pre- dominant subclass, although GST alpha and mu were also expressed in most tumours to a lesser ex- tent. It is known that between 40-45 % of individu- als do not express mu class GST [24, 25] and it has been suggested that such individuals may be more prone to certain cancers, possibly because of failure to detoxify mutagenic epoxides [26, 27]. Smith et al. [21] have demonstrated that GST mu is involved in

denitrosation of BCNU in rat brain tumour cells. If patients have no GST mu in their tumours, it is also possible that they cannot detoxify chemotherapy agents raising the possibility that patients with low GST may have better responses to chemotherapy. This paper confirms some of Hara's findings [13], and extends the observation with regard to GST subclasses in the wider range of tumours examined in the current study.
The presence of cytochrome P450 in the brain is of interest to neurobiologists, neuropharmacolo- gists and neurotoxicologists. In animals, most cyto- chrome P450 is in the microsomes [28] or mitochon- dria [29]. Cytochrome P450's have a different mechanism and site of action from glutathione S- transferases. They are brain phase 1 enzymes that result in intracellular oxidative biotransformation. There is some evidence that cytochrome P450 re- ductase may actually activate certain chemother- apeutic drugs through oxidative biotransformation. Cytochrome P450 reductase immunostaining was present in normal neurones, reflecting mitochon- drial number and activity in these cells, and malig- nant astrocytes but not within normal astrocytes. Gemistocytic astrocytic tumour cells stained inten- sely.
There is growing evidence that GST/cytochrome P450's play an important role in tumour cell resist- ance. Further work is necessary to see if there is any correlation between immunostaining intensity and response to chemotherapy.
Acknowledgements
Primary antibodies were kindly provided by Dr. J. Hayes/Prof CR Wolf of the Imperial Cancer Re- search Fund Molecular Biology Unit at Ninewells Hospital, Dundee, Scotland, U.K.
References
1. Hayes JD, Wolf CR: Molecular mechanisms of drug resist- ance. Biochemical Journal 272: 1-15,1990
2. Wolf CR, Wareing CJ, Black SM, Hayes JD: Glutathione S-transferases in resistance to chemotherapeutic drugs. In:
Hayes JD, Pickett CB, Mantle TJ (eds) Glutathione S-trans- ferases and Drug Resistance, pp 296-307. Taylor and Fran- cis, London
3. Becker I, Becket K-F, Meyermann R, Holt V: The multidrug resistance gene MDR1 is expressed in human glial tumors. Acta Neuropathol 82: 516-519, 1991
4. Smith MT, Evans CG, Doane-Setzer E Castro VM, Tahir MK, Mannervik B: Denitrosation of 1,3-Bis(2-chloroeth- yl)-l-nitrosourea by class mu glutathione transferases and its role in cellular resistance in rat brain tumor cells. Cancer Res 49: 2621-2625, 1989
5. Hayes JD, Wolf CR: The role of glutathione transferase in drug resistance. In: Seis H, Ketterer B (eds) Glutathione Conjugation: Mechanisms and Biological Significance, pp 316-355. Academic Press, London
6. Black SM, Wolf CR: The role of glutathione-dependent en- zymes in drug resistance. Pharmac Ther 51: 139-154, 1991
7. Ali-Osman F, Caughlin J, Gray GS: Decreased DNA inter- strand crosslinking and cytotoxicity induced in human brain tumor cells by 1,3-Bis(2-chloroethyl)-l-nitrosourea after in
vitro reaction with glutathione. Cancer Res 49: 5954-5959, 1989
8. Carder PJ, Hume R, Fryer AA, Strange RC, Lauder J, Bell JE: Glutathione S-transferase in human brain. Neuropath Appl Neurobio116: 293-303, 1990
9. Strange RC, Fryer AA, Matharoo B, Zhao L, Broome J, Campbell A, Jones P, Pastor IC, Singh RVP: The human Glutathione S-transferases: Comparison of isoenzyme ex- pression in normal and astrocytoma brain. Biochem Bio- phys Acta 1139(3): 222-228, 1992
10. World Health Organization International Classification of Tumours: Histological typing of turnouts of the central nerv- ous system. In: Kleihues P, Burger PC, Scheithauer BW (eds) Second Edition. Springer Verlag, Berlin 1993
11. Yung WKA, Levin VA: Chemotherapy: Current and future role and expectations. In: Apuzzo MLJ (ed) Neurosurgical Topics: Malignant Cerebral Glioma. American Association of Neurological Surgeons: Park Ridge, Illinois, USA
12. Grant R, Liang B, Page M, Greenberg H, Junck L: Age influ- ences chemotherapy response in glioma, irrespective of tu- mor grade. Ann Neurol 32(2): 289-290, 1992
13. Hara A, Yamada H, Sakai N, Hirayama H, Tanaka T, Mori H: Immunohistochemical demonstration of the placental form of glutathione S-transferase, a detoxifying enzyme in human gliomas. Cancer 66: 2563-2568, 1990
14. Evans CG, Bodell WJ, Tokuda K, Doane-Setzer R Smith MT: Glutathione and related enzymes in rat brain tumor cell resistance to 1,3,Bis(2-chloroethyl)-l-nitrosourea and nitro- gen mustard. Cancer Res 49: 2523-2530, 1989
15. Hill DR: N,N'-bis(2-chloroethyl)-N-nitrosourea, a substrate for glutathione S-transferase. Proc Am Assoc Cancer Res 17: 52,1976
16. Castro VM: Significance of glutathione transferases in the resistance of tumor cells to alkylating cytostatic drugs. Doc- torial dissertation Stockholm 1991, Department of Bio-

chemistry, Stockholm University. ISBN 91-7146-876-5. Aka- demitryck AB, Edsbruk 1991
17. Yang WZ, Begleiter A, Johnstone JB, Israels LG, Mowat MR: Role of glutathione and glutathione S-transferase in chlorambucil resistance. Mol Pharmacol 41(4): 625-630, 1992
18. Peters WH, Roelofs HM: Biochemical characterization of resistance to mitoxantrone and adriamycin in caco-2 human colon adenocarcinoma cells: a possible role for glutathione S-transferase. Cancer Res 52(7): 1886-1890, 1992
19. Sato K, Kitahara A, Satoh K, Ishikawa T, Tatematsu M, Ito N: The placental form of glutathione s-transferase as a new marker protein for pre-neoplasia in rat chemical hepatocar- cinomatosis. Cancer Research 44: 2698-2703, 1984
20. Shiratori Y, Soma Y, Maruyama H, Sato S, Takano A, Sato K: Immunohistochemical detection of the placental form of glutathione s-transferase in dysplastic and neoplastic human uterine cervix lesions. Cancer Research 47: 6806-6809,1987
21. Smith MT, Evans CG, Doane-Setzer R Castro VM, Tahir MK, Mannervik B: Denitrosation of 1,3-Bis(2-chloroeth- yl)-l-nitrosourea by class mu glutathione transferases and its role in cellular resistance in rat brain tumor cells. Cancer Res 49: 2621-2625, 1989
22. Hercbergs A, Brok-Simoni F, Holtzman F, Bar-Am J, Leith JT, Brenner JH: Erythrocyte glutathione and tumour re- sponse to chemotherapy. Lancet 339(8801): 1074-1076,1992
23. Beckett G J, Howie AF, Hussey A J, Hayes PC, Miller WR, Hayes JD: Radioimmunoassay measurements of the human glutathione S-transferases. In: Hayes JD, Pickett CB, Man-
tie TJ (eds) Glutathione S-transferases and drug resistance. 1990: p309. Taylor and Francis, London
24. Strange RC, Faulder CG, Davis BA, Hume R, Brown JAH, Cotton W, Hopkinson DA: The human glutathione S trans- ferases: studies on the distribution and genetic variation of GST-I, GST-2, and GST-3 isoenzymes. Ann Hum Genet 48: 11-20, 1984
25. Hussey AJ, Hayes JD, Beckett GJ: Measurement of human neutral glutathione S transferase (GST) concentrations in plasma and biopsy tissue using radioimmunoassay. Biochem Pharmacop 36: 40134015, 1987
26. Seidegard J, Pero RW, Miller DG, Beattie EJ: A glutathione transferase in human leukocytes as a marker for the suscep- tibility to lung cancer. Carcinogenesis 7: 751-753, 1986
27. Seidegard J, Pero RW, Markowitz MM, Roush G, Miller DG, Beattie E J: Isozyme(s) of glutathione transferase (class mu) as a marker for the susceptibility to lung cancer: a fol- low-up study. Carcinogenesis 11: 33-36, 1990
28. Warner M, Ahlgren R, Zaphiropoulos PG, Hayashi S-I, Gustafsson J-A. In: Methods in Enzymology: Identification of P450s in the brain. 206: 631-640, 1991
29. Walther B, Ghersi-Egea JF, Minn A, Siest G: Subcellular distribution of cytochrome P-450 in the brain. Brain Res 375: 338-344, 1986
Address for offprints: R. Grant, Neurology Unit, Department of Clinical Neurosciences, Western General Hospital, Crewe Road, Edinburgh EH4 2XU, UK