gnrh-a to trigger ovulation should be used in all pcos patients to prevent ohss dr. shahar kol
TRANSCRIPT

GnRH-a to trigger ovulation should be used in all PCOS patients to prevent OHSS
Dr. Shahar Kol
Disclaimer
• The following presentation reflects my own experience and opinion.
• The presentation does not necessarily reflect drug companies’ policies.
• I mention off-label use of medications, this use is not endorsed by drug companies.
IVM
• This option is thoroughly discussed in this meeting.
• If you adopt IVM you need not worry about OHSS.
• If you choose to stimulate your PCOS patient, please use the GnRH antagonist option.
• Mild stimulation is a great idea, not easy to implement.
AUGUST 2009 VOL 5 NO 8AUGUST 2009 VOL 5 NO 8
AUGUST 2009
AUGUST 2009 VOL 5 NO 8
If you choose a long GnRH agonist protocol, this what might happen
Basic clinical details
• 25-year-old, 2 years of primary infertility• Irregular cycles, facial hair• BMI=24, LH=14.9, Testo=2.5, FSH-normal• US: PCOS• Impaired glucose tolerance – started
Metformin 850 twice daily• Sperm-normal• FSH-normal
Pre-IVF treatment
• CC up to 100 mg daily – no ovulation• 5 cycles with recFSH 50 U daily. Four cycles
mono-ovulation, 1 cycle cancelled for multifollicular development. No pregnancy.
• Referral to IVF.
IVF – cycle I
• Long agonist protocol, continue metformin, daily gonadotropin dose of 112.5 U – no response, increase to 150 U – good response
• Trigger with hCG 10,000 U• OPU: 16 eggs from 20 follicles.• ET: 2 embryos, no pregnancy.

IVF-cycle II
• Same long protocol, continue metformin, starting dose 150 U.
• After 7 days: “unfortunately” 25 follicles<12 mm, 9 follicles 13-16 mm, dose reduced to 125 U, trigger with hCG 5,000 U.
• OPU: 41 eggs, 21 embryos frozen.• 2 days later: abdominal pain, vomiting.• US: large ovaries.• Hemoglobin -16.3, WBC-31,700. • Decision to hospitalize.
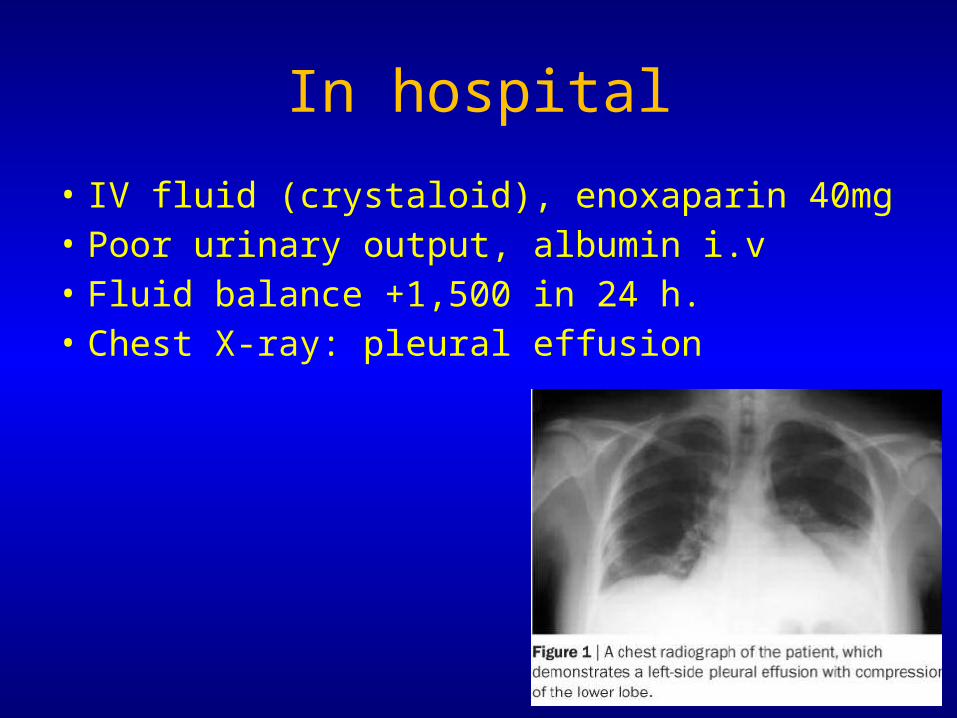
In hospital
• IV fluid (crystaloid), enoxaparin 40mg• Poor urinary output, albumin i.v• Fluid balance +1,500 in 24 h.• Chest X-ray: pleural effusion
Getting worse
• Chest and abdominal drains.• During 24h 2 L of ascitic fluid and 1 L pleuritic
fluid was drained.• Further deterioration: O2 sat <95%, X-ray:
bilateral pleural effusion and pulmonary edema.
ICU
• Risk of adult RDS – transferred to ICU• 2nd chest tube inserted• Central i.v. line• Continue albumin• Gradual improvement and discharge after a
few days.
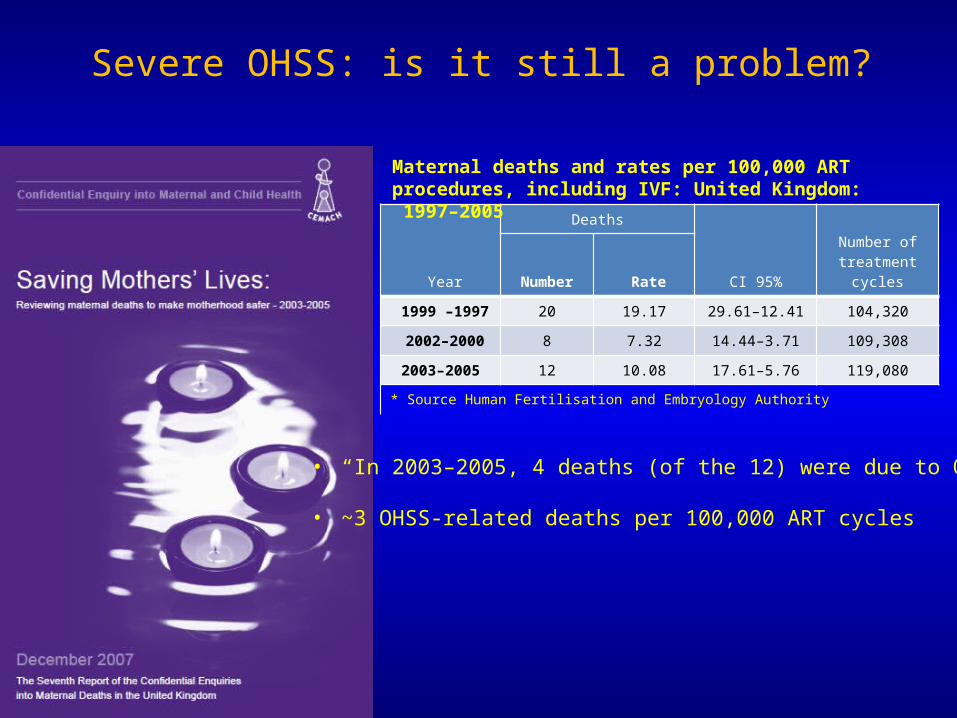
Severe OHSS: is it still a problem?
• “In 2003–2005, 4 deaths (of the 12) were due to OHSS”
• ~3 OHSS-related deaths per 100,000 ART cycles
Year
Deaths
95% CI
Number of treatment
cycles Number Rate
1997 –1999 20 19.17 12.41–29.61 104,320
2000–2002 8 7.32 3.71–14.44 109,308
2003–2005 12 10.08 5.76–17.61 119,080
* Source Human Fertilisation and Embryology Authority
Maternal deaths and rates per 100,000 ART procedures, including IVF: United Kingdom: 1997–2005
Three OHSS-related deaths (3:100,000), all had their embryos frozen
Braat DDM, et al. Hum Reprod 2010;25:1782–1786
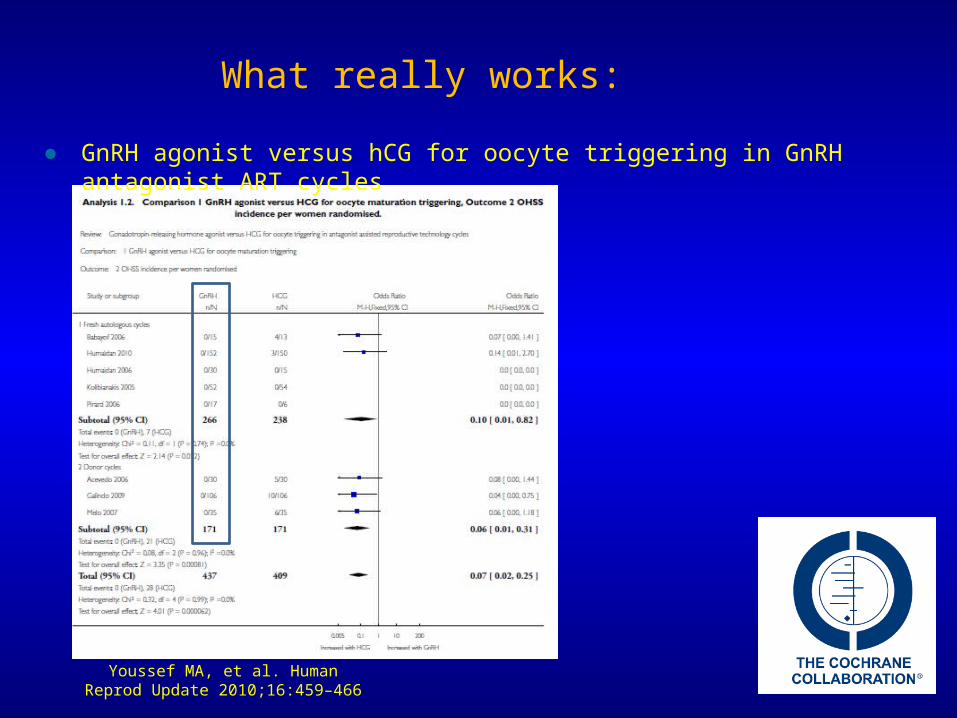
Youssef MA, et al. Human Reprod Update 2010;16:459–466
What really works:
● GnRH agonist versus hCG for oocyte triggering in GnRH antagonist ART cycles
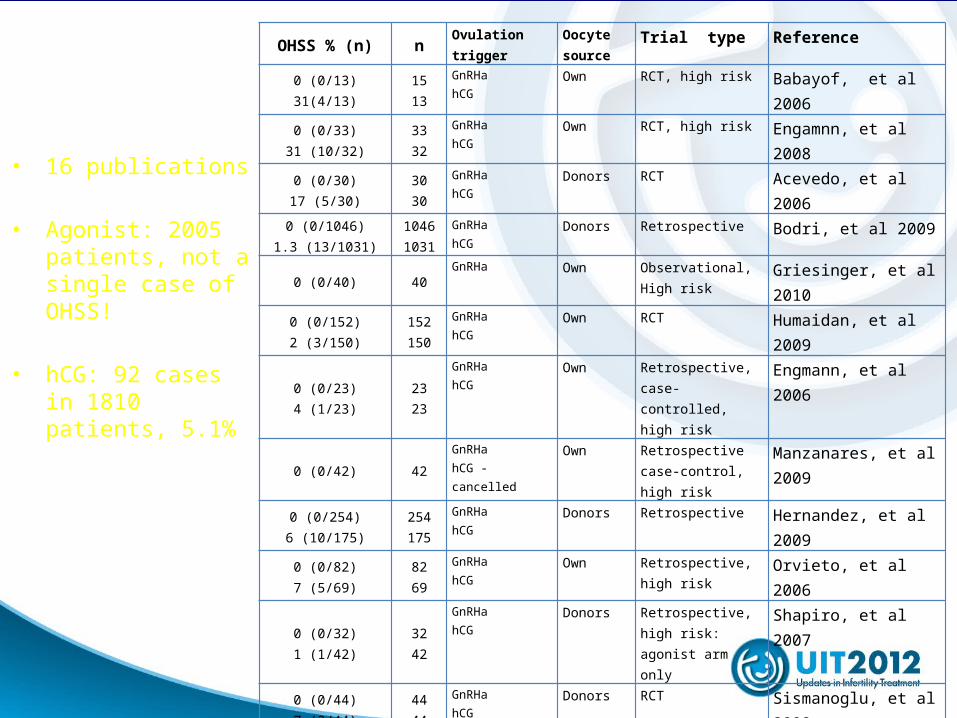
OHSS % (n) n Ovulation trigger
Oocyte source
Trial type Reference
0 (0/13)31(4/13)
1513
GnRHahCG
Own RCT, high risk Babayof, et al 2006
0 (0/33)31 (10/32)
3332
GnRHahCG
Own RCT, high risk Engamnn, et al 2008
0 (0/30)17 (5/30)
3030
GnRHahCG
Donors RCT Acevedo, et al 2006
0 (0/1046)1.3 (13/1031)
10461031
GnRHahCG
Donors Retrospective Bodri, et al 2009
0 (0/40) 40GnRHa Own Observational,
High riskGriesinger, et al 2010
0 (0/152)2 (3/150)
152150
GnRHahCG
Own RCT Humaidan, et al 2009
0 (0/23)4 (1/23)
2323
GnRHahCG
Own Retrospective, case-controlled, high risk
Engmann, et al 2006
0 (0/42) 42GnRHahCG - cancelled
Own Retrospective case-control, high risk
Manzanares, et al 2009
0 (0/254)6 (10/175)
254175
GnRHahCG
Donors Retrospective Hernandez, et al 2009
0 (0/82)7 (5/69)
8269
GnRHahCG
Own Retrospective, high risk
Orvieto, et al 2006
0 (0/32)1 (1/42)
3242
GnRHahCG
Donors Retrospective, high risk: agonist arm only
Shapiro, et al 2007
0 (0/44)7 (3/44)
4444
GnRHahCG
Donors RCT Sismanoglu, et al 2009
8 (1/12) 12GnRH, luteal rescue with hCG 1500IU
Own Observational, high risk
Humaidan, et al 2009
0 (0/106)8 (9/106)
106106
GnRHahCG
Donors RCT Galindo, et al 2009
0 (0/50)16(8/50)
5050
GnRHahCG
Donors RCT Melo, et al 2009
0 (0/45)15 (33)
445
GnRHahCG
Own RCT, high risk Shahrokh, et al 2010
• 16 publications
• Agonist: 2005 patients, not a single case of OHSS!
• hCG: 92 cases in 1810 patients, 5.1%
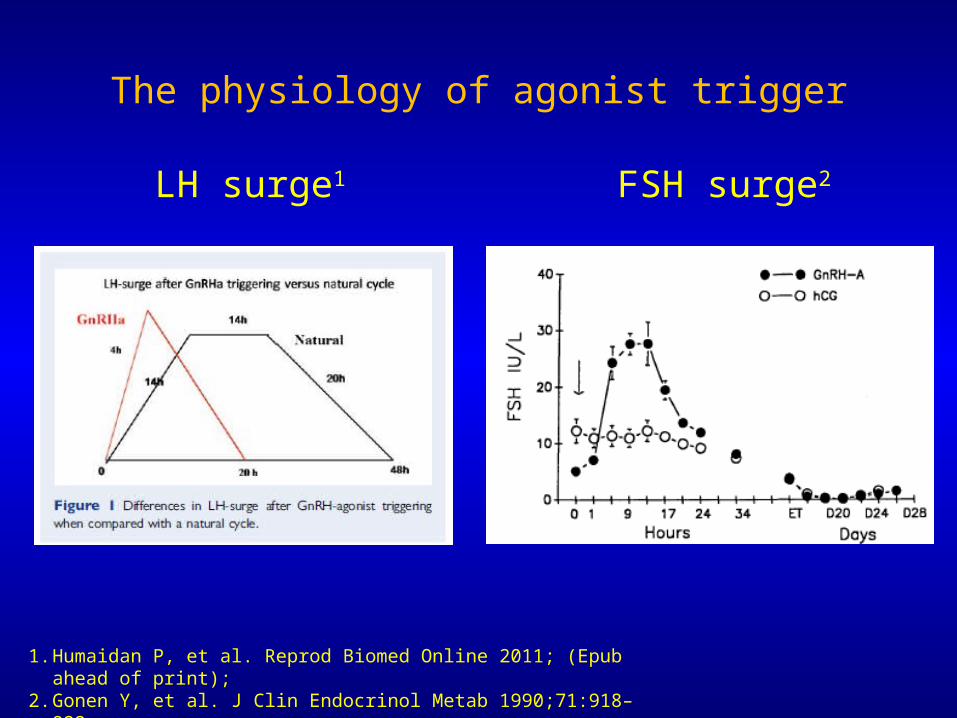
The physiology of agonist trigger
1. Humaidan P, et al. Reprod Biomed Online 2011; (Epub ahead of print);2. Gonen Y, et al. J Clin Endocrinol Metab 1990;71:918–922
LH surge1 FSH surge2

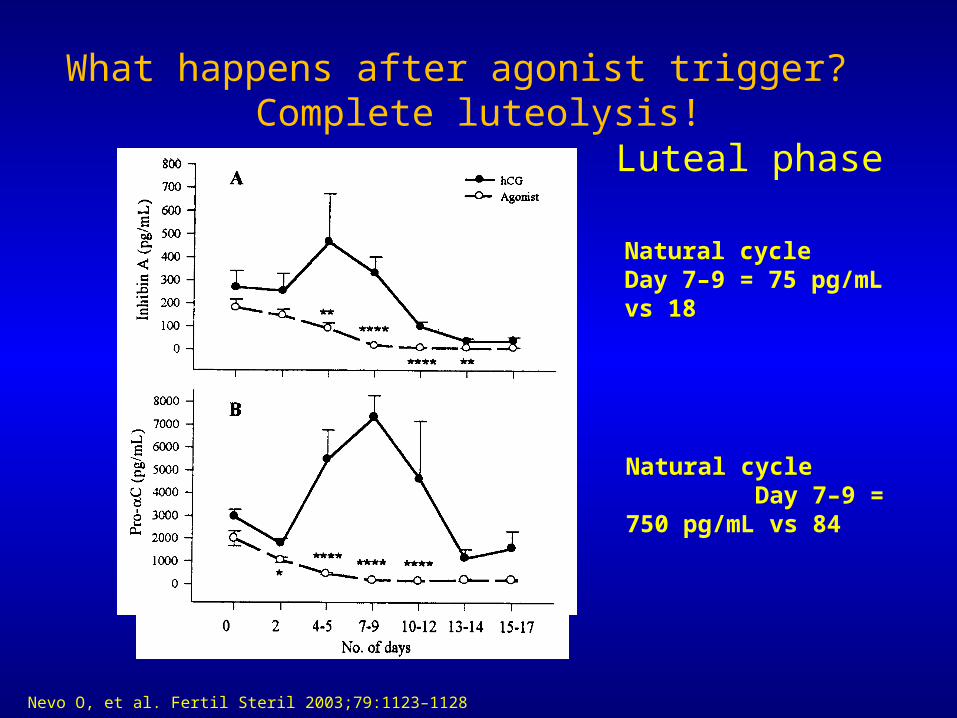
What happens after agonist trigger? Complete luteolysis!
Luteal phase
Natural cycle Day 7–9 = 75 pg/mL vs 18
Natural cycle Day 7–9 = 750 pg/mL vs 84
Nevo O, et al. Fertil Steril 2003;79:1123–1128
“The concept of an OHSS-Free Clinic has become a reality. This approach should include pituitary down-regulation using a GnRH antagonist, ovulation triggering with a GnRH agonist and vitrification of oocytes or embryos”
“…luteal phase supplementation with low-dose hCG has to be fine tuned.”
Devroey P, et al. Human Reprod 2011; 26: 2593–2597
OHSS prevention by GnRH agonist triggering of final oocyte maturation in a GnRH antagonist protocol in combination with freeze-all strategy: a prospective multicenter study
• Conclusions: “…a single case of a severe early onset OHSS occurred”
– E2 trigger day=47,877 pmol/L– 13 oocytes– The patient was hospitalized on day of OPU, with abdominal distension,
drastically enlarged ovaries (right and left ovarian volume 363 cm2 and 261 cm2, respectively), and lower abdominal pain.
– She received low molecular weight heparin, cabergoline (0.5 mg/d), and IV infusion therapy, including albumin.
Griesinger G, et al. Fertil Steril 2011;95:2029–2033
Failures?

Failures? (cnt’d)
– “drastic decrease of hemoglobin levels to 4.9 mmol/L” (8 grams/dL) patient received blood transfusion 2 days post OPU.
– Hematocrit: 41 trigger day, 37 OPU day, ‘,<35’ post blood transfusion.
– 3–4 days post trigger 3.9 litres of “blood-stained ascites which was indicative of a subacute intraperitoneal hemorrhage”.
How to secure good clinical outcome post agonist trigger?
• High risk fresh transfer: intensive E2+P luteal support
• High risk: ‘freeze-all’• Low risk: luteal rescue based on LH activity
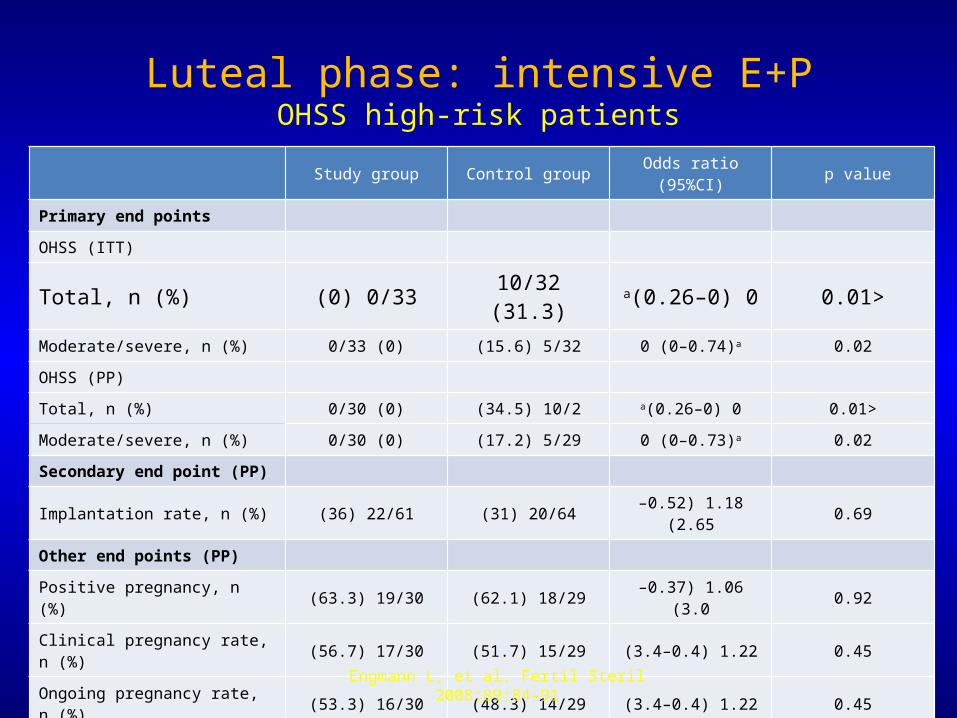
Luteal phase: intensive E+POHSS high-risk patients
Study group Control group Odds ratio (95%CI) p value
Primary end points
OHSS (ITT)
Total, n (%) 0/33( 0) 10/32( 31.3) 0( 0–0.26)a <0.01Moderate/severe, n (%) 0/33 (0) 5/32( 15.6) 0 (0–0.74)a 0.02
OHSS (PP)
Total, n (%) 0/30 (0) 10/2( 34.5) 0( 0–0.26)a <0.01
Moderate/severe, n (%) 0/30 (0) 5/29( 17.2) 0 (0–0.73)a 0.02
Secondary end point (PP)
Implantation rate, n (%) 22/61( 36) 20/64( 31) 1.18( 0.52–2.65) 0.69
Other end points (PP)
Positive pregnancy, n (%) 19/30( 63.3) 18/29( 62.1) 1.06( 0.37–3.0) 0.92
Clinical pregnancy rate, n (%) 17/30( 56.7) 15/29( 51.7) 1.22( 0.4–3.4) 0.45
Ongoing pregnancy rate, n (%) 16/30( 53.3) 14/29( 48.3) 1.22( 0.4–3.4) 0.45aThe estimates of these odds ratios are zero, because no patient developed OHSS in the study group; ITT=intention to treat; PP=per protocol
Engmann L, et al. Fertil Steril 2008;89:84–91
GnRHa Trigger and Total Freeze in High Risk Patients
Griesinger et al., 2007, observational, 20 high- risk patients (≥ 20 follicles ≥ 11mm)
- cumulative ongoing pregnancy rate 37%
Griesinger at al., 2011, observational, 51 high-risk patients (≥ 20 follicles ≥ 11mm)
- cumulative live bith rate 37%
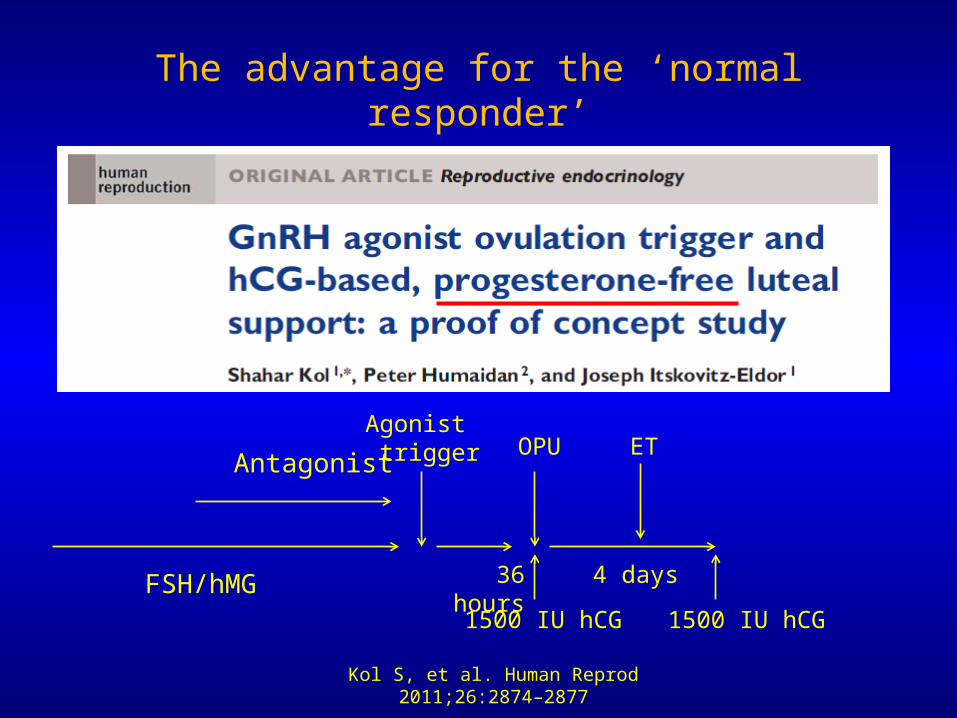
The advantage for the ‘normal responder’
Kol S, et al. Human Reprod 2011;26:2874–2877
FSH/hMG
AntagonistAgonist trigger
36 hours
OPU
1500 IU hCG
4 days
1500 IU hCG
ET
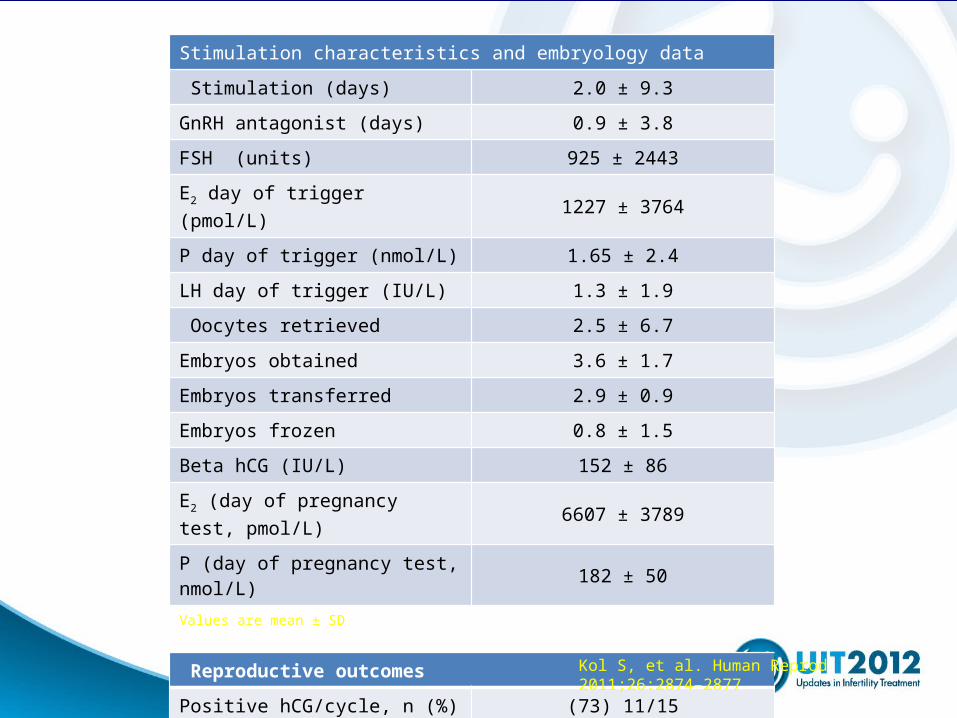
Stimulation characteristics and embryology data
Stimulation (days) 9.3 ±2.0
GnRH antagonist (days) 3.8 ±0.9
FSH (units) 2443 ±925
E2 day of trigger (pmol/L) 3764 ±1227
P day of trigger (nmol/L) 2.4 ±1.65
LH day of trigger (IU/L) 1.9 ±1.3
Oocytes retrieved 6.7 ±2.5
Embryos obtained 3.6 ± 1.7
Embryos transferred 2.9 ± 0.9
Embryos frozen 0.8 ± 1.5
Beta hCG (IU/L) 152 ± 86
E2 (day of pregnancy test, pmol/L) 6607 ± 3789
P (day of pregnancy test, nmol/L) 182 ± 50Values are mean ± SD
Reproductive outcomes
Positive hCG/cycle, n (%) 11/15( 73)
Clinical ongoing pregnancy, n (%) 7/15( 47)
Early pregnancy loss, n (%) 4/11( 36)
Kol S, et al. Human Reprod 2011;26:2874–2877

Side benefits
• Agonist trigger: more MII oocytes compared with hCG trigger1-4
• Potential benefit of FSH surge:5-9 – Promotes LH receptor formation in luteinizing
granulosa cells– Promotes nuclear maturation (i.e. resumption of
meiosis) – Promotes cumulus expansion
1. Humaidan P, et al. Reprod Biomed Online 2005;11:679–6842. Humaidan P, et al. Human Reprod 2009;24:2389–23943. Imoedemhe DA, et al. Fertil Steril 1991;55:328–3324. Oktay K, et al. Reprod Biomed Online 2010;20:783–788 5. Eppig JJ. Nature 1979;281:483–4846. Strickland and Beers. J Biol Chem 1976;251:5694–57027. Yding Andersen C. Reprod Biomed Online 2002;5:232–2398. Yding Andersen C, et al. Mol Hum Reprod 1999;5:726–7319. Zelinski-Wooten MB, et al. Human Reprod 1995;10:1658–1666

Anecdotal cases
• You may consider GnRH agonist trigger in the following cases:– Repeated IVF failure– “empty follicles” syndrome– Immature oocytes despite adequate follicular
diameter

Crystal ball: where are we heading?
Out In‘Long agonist’ protocols Antagonist-based protocols
hCG trigger Agonist trigger
1–2% severe OHSS Total OHSS elimination
OHSS-related death rate: 3:100,000 Total OHSS elimination