goal-directed fluid therapy: a new way of thinking · goal-directed fluid therapy: a new way of...
TRANSCRIPT

Goal-Directed Fluid
Therapy: A New Way of
Thinking
Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN
DNP Candidates
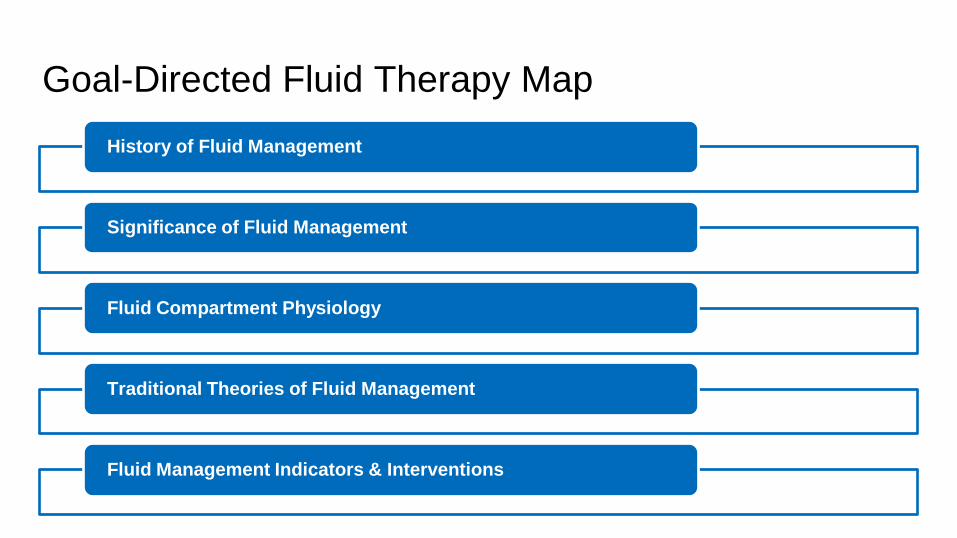
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
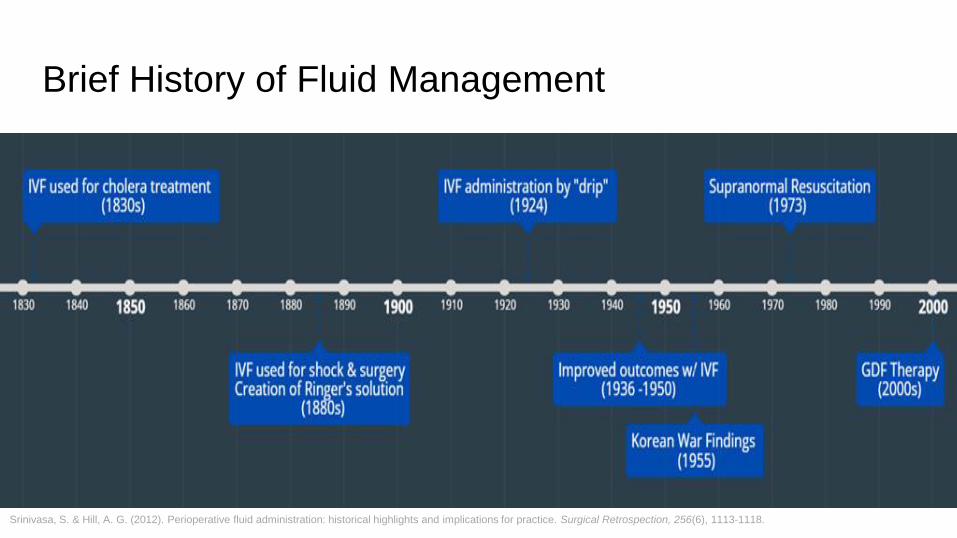
Brief History of Fluid Management
Srinivasa, S. & Hill, A. G. (2012). Perioperative fluid administration: historical highlights and implications for practice. Surgical Retrospection, 256(6), 1113-1118.
Why Should I Care?
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
Hypovolemia Hypervolemia
Hypovolemia Complications
Low cardiac output
Decreased tissue perfusion
Shock/organ failure
Hypovolemia
Chappell, D., Jacob, M., Hofmann-Kiefer, K., Conzen, P., & Rehm, M. (2008). A rational approach to
perioperative fluid management. Anesthesiology, 109(4): 723
Brandstrup, B. (2006). Fluid therapy for the surgical patient. Best Practice Research Clinical
Anaesthesiology, 20(2), 265.
Hypervolemia Complications Respiratory
effects
GI effects
Coagulation
Wound healing
Hypervolemia
Joshi, G. P. (2018). Intraoperative fluid management. UpToDate. Retrieved February 26, 2018, from
https://www.uptodate.com/contents/intraoperative-fluid-management
Thacker, J. K., Mountford, W. K., Ernst, F. R., Krukas, M. R., & Mythen, M. M. (2016). Perioperative fluid utilization
variability and association with outcomes: considerations for enhanced recovery efforts in sample US surgical
populations. Annals of Surgery, 263(3), 502-510.
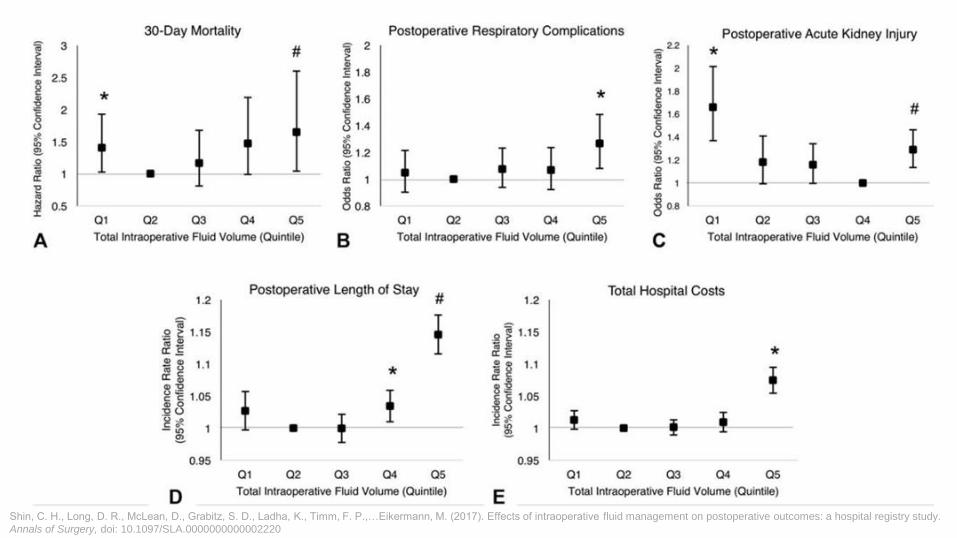
Shin, C. H., Long, D. R., McLean, D., Grabitz, S. D., Ladha, K., Timm, F. P.,…Eikermann, M. (2017). Effects of intraoperative fluid management on postoperative outcomes: a hospital registry study.
Annals of Surgery, doi: 10.1097/SLA.0000000000002220
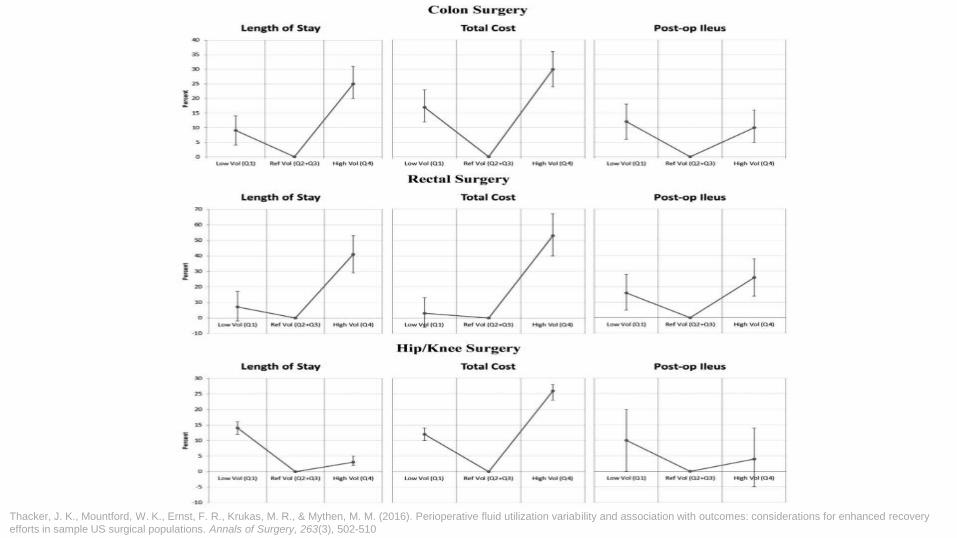
Thacker, J. K., Mountford, W. K., Ernst, F. R., Krukas, M. R., & Mythen, M. M. (2016). Perioperative fluid utilization variability and association with outcomes: considerations for enhanced recovery
efforts in sample US surgical populations. Annals of Surgery, 263(3), 502-510
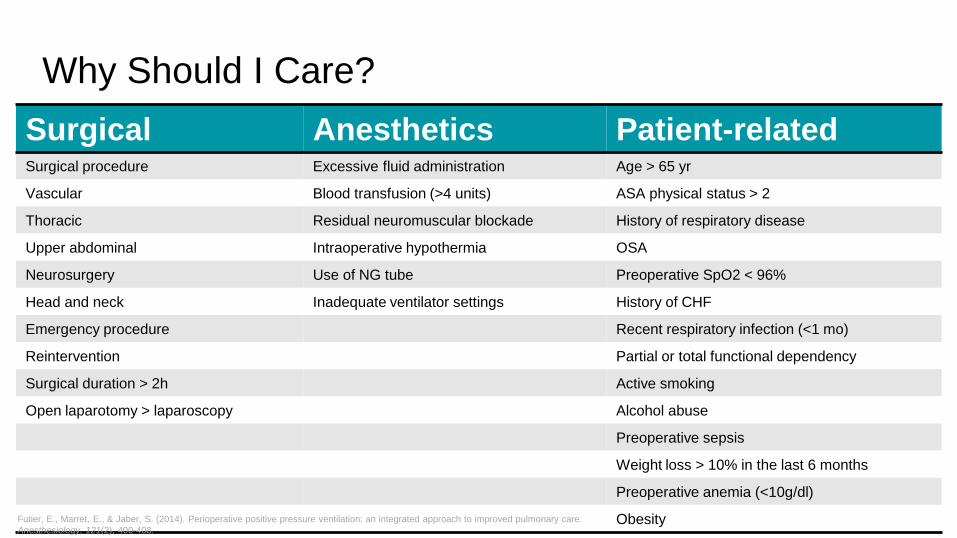
Why Should I Care?
Surgical Anesthetics Patient-related Surgical procedure Excessive fluid administration Age > 65 yr
Vascular Blood transfusion (>4 units) ASA physical status > 2
Thoracic Residual neuromuscular blockade History of respiratory disease
Upper abdominal Intraoperative hypothermia OSA
Neurosurgery Use of NG tube Preoperative SpO2 < 96%
Head and neck Inadequate ventilator settings History of CHF
Emergency procedure Recent respiratory infection (<1 mo)
Reintervention Partial or total functional dependency
Surgical duration > 2h Active smoking
Open laparotomy > laparoscopy Alcohol abuse
Preoperative sepsis
Weight loss > 10% in the last 6 months
Preoperative anemia (<10g/dl)
Obesity Futier, E., Marret, E., & Jaber, S. (2014). Perioperative positive pressure ventilation: an integrated approach to improved pulmonary care.
Anesthesiology, 121(2), 400-408.
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
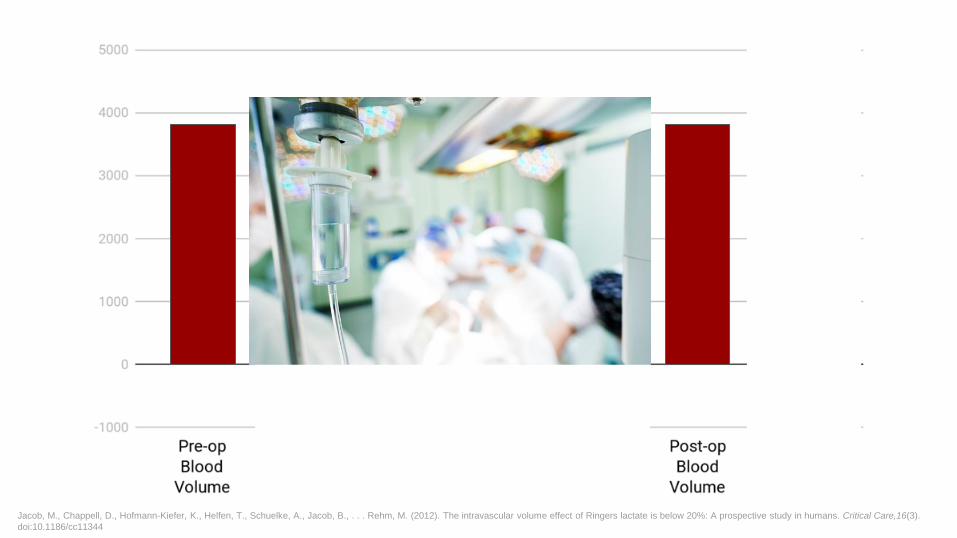
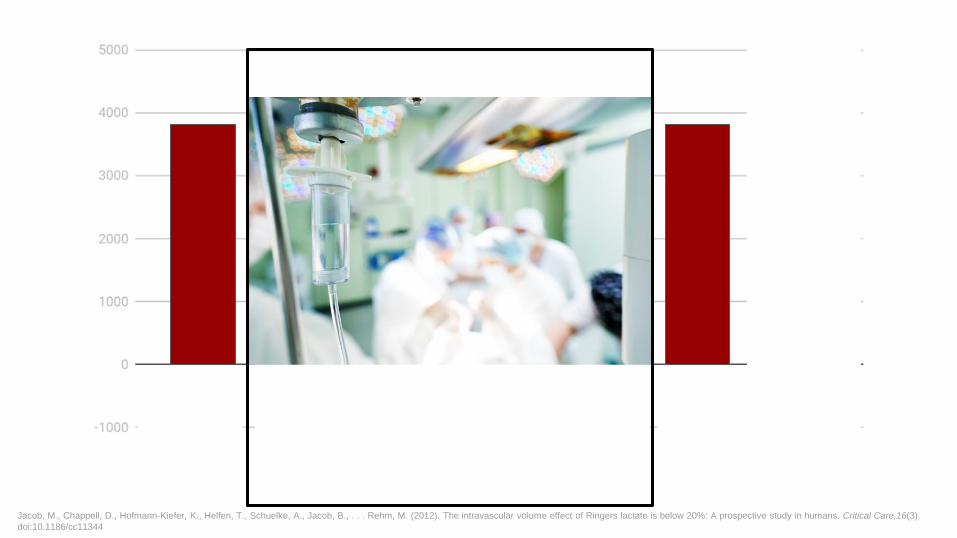
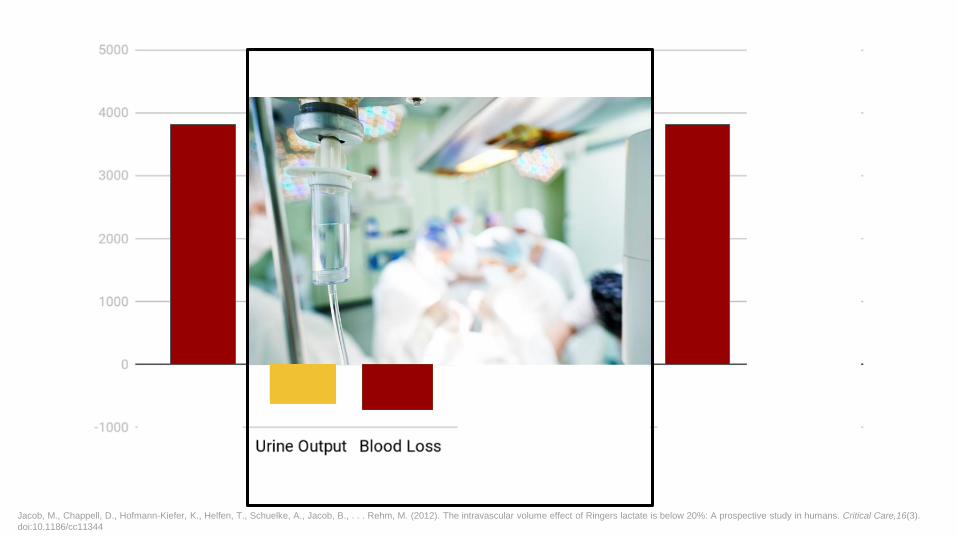
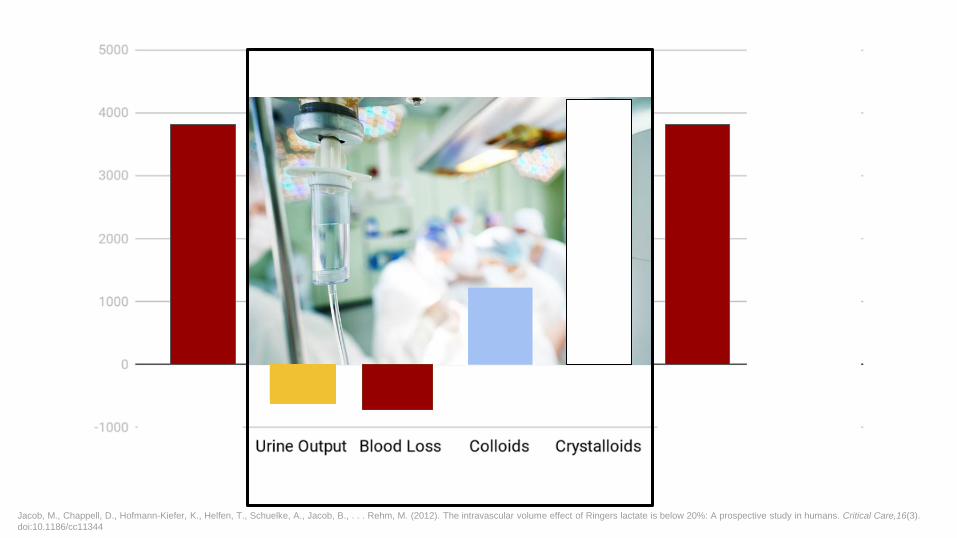
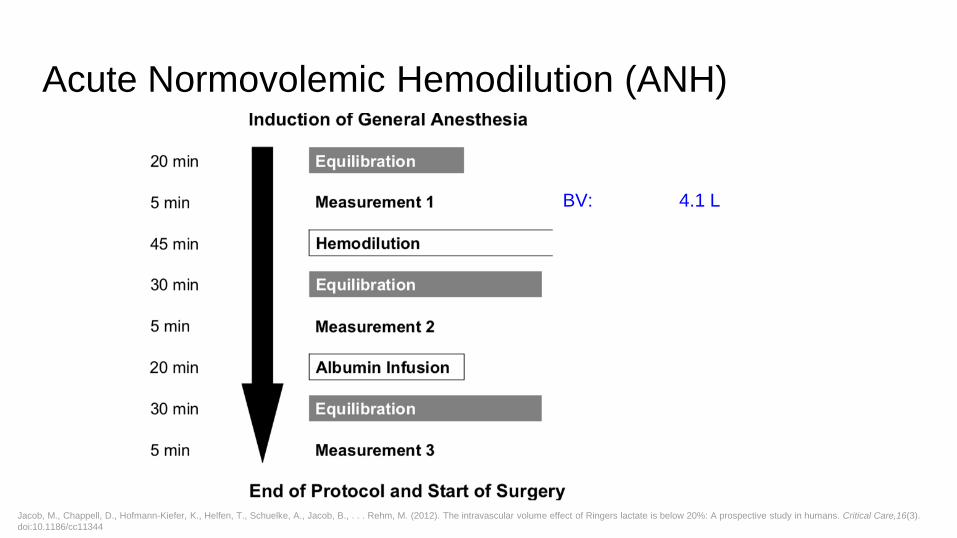
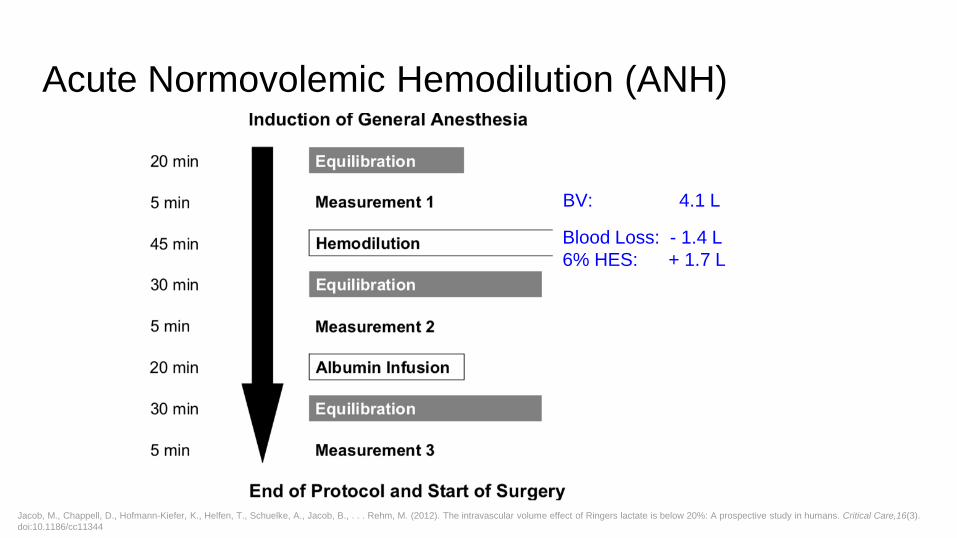
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
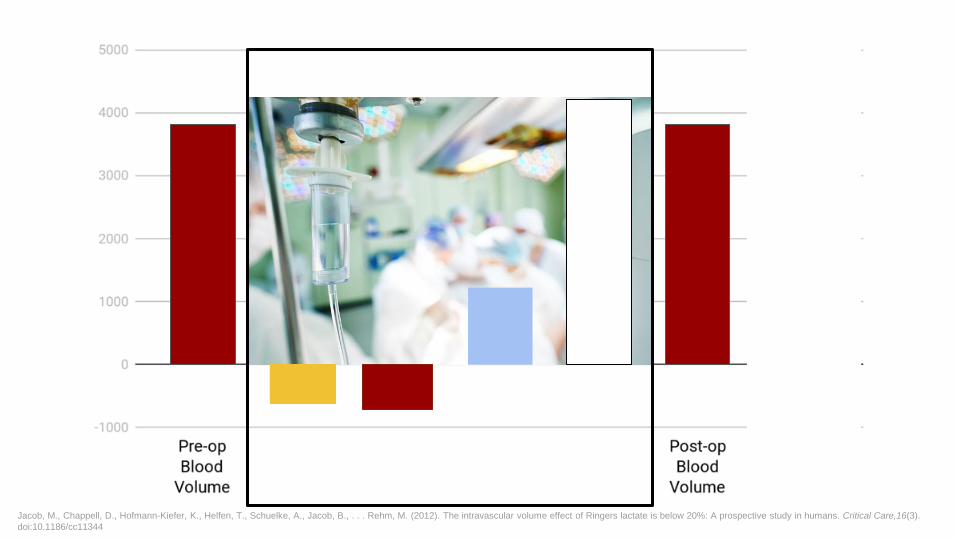
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
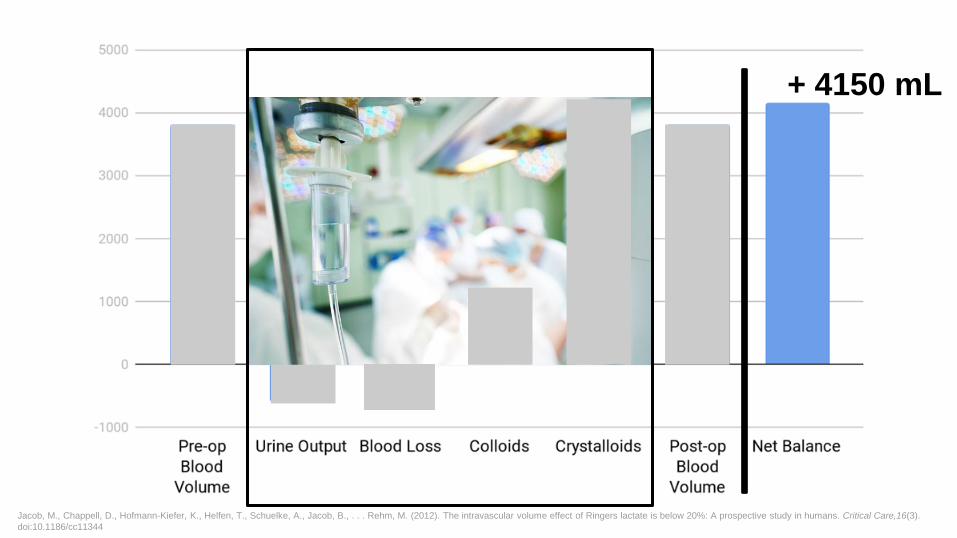
+ 4150 mL
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
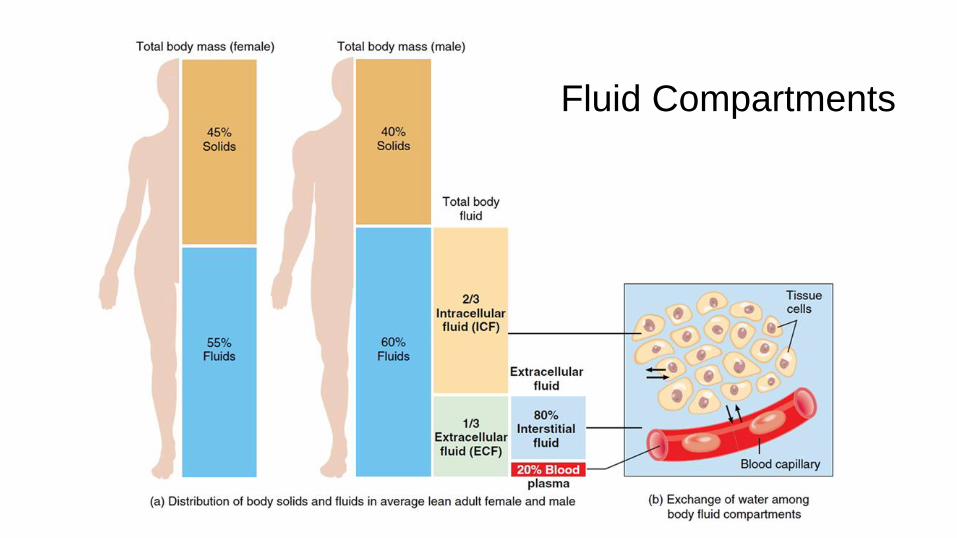
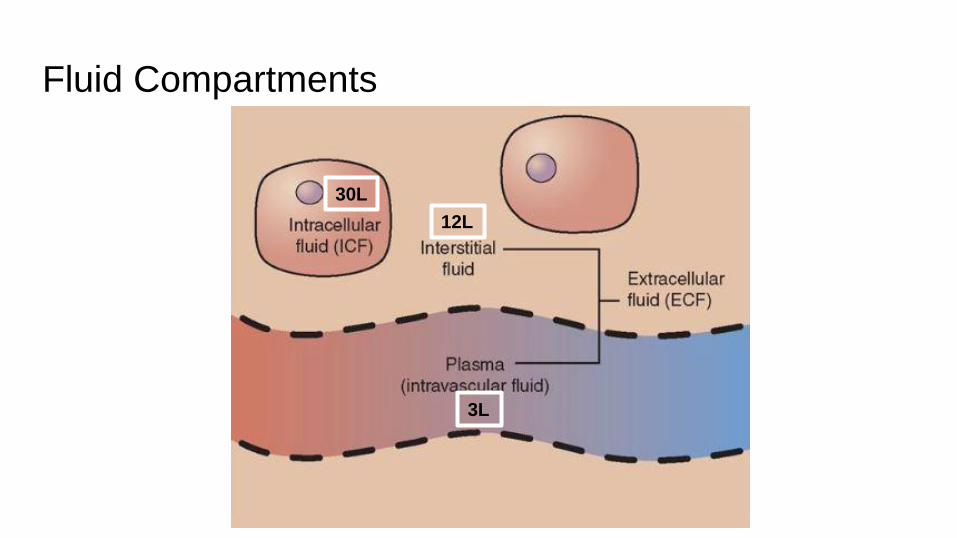
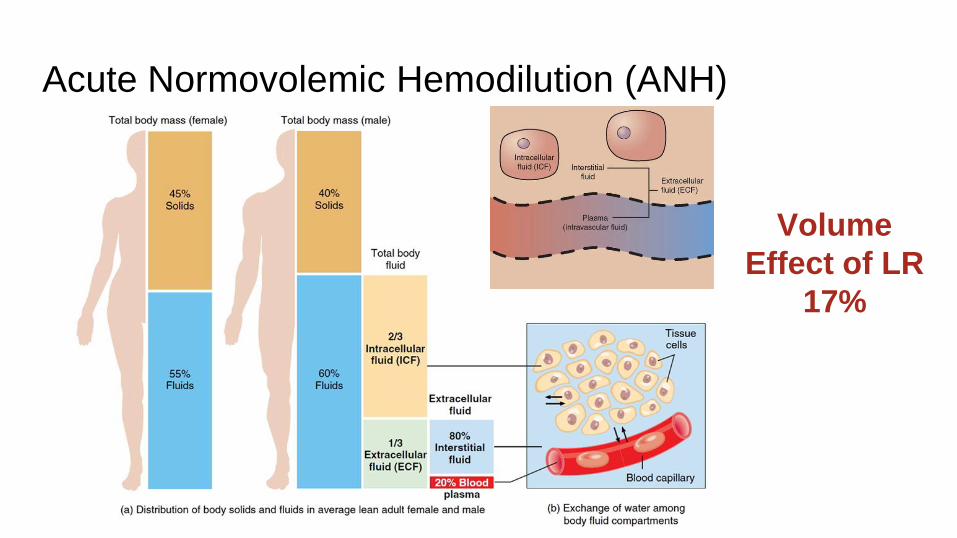
Fluid Compartments
Fluid Compartments
30L
12L
3L
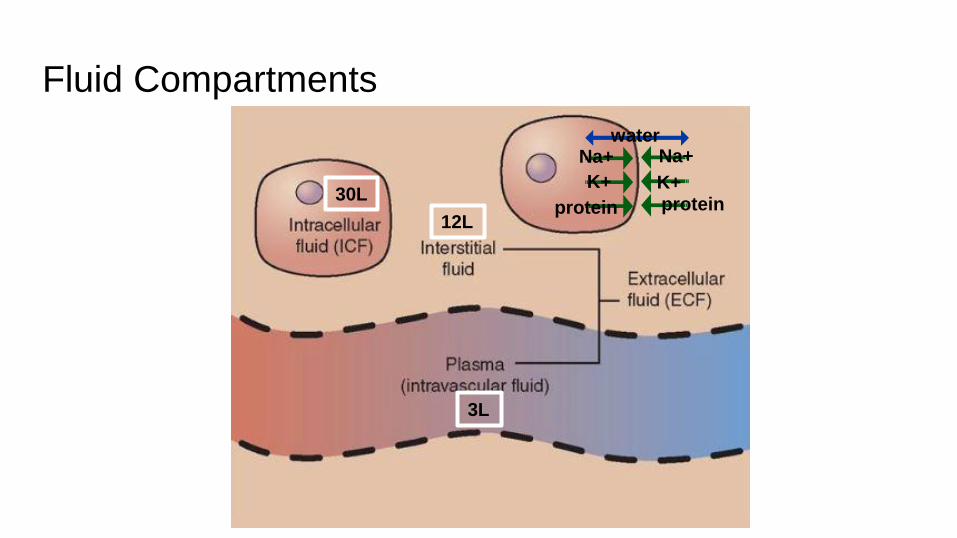
Fluid Compartments
30L
12L
3L
water Na+ Na+
K+ K+ protein protein
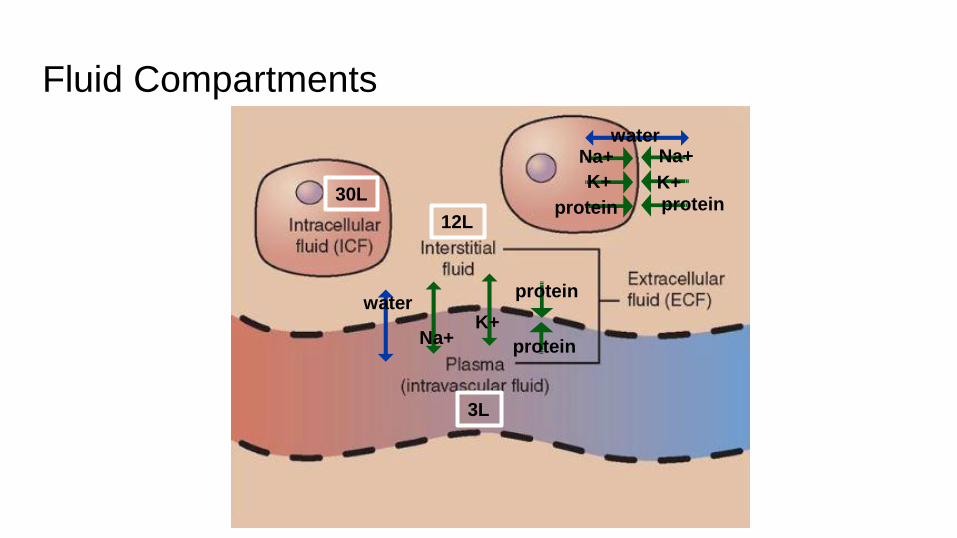
Fluid Compartments
30L
12L
3L
water Na+ Na+
K+ K+ protein protein
water
Na+ K+
protein
protein
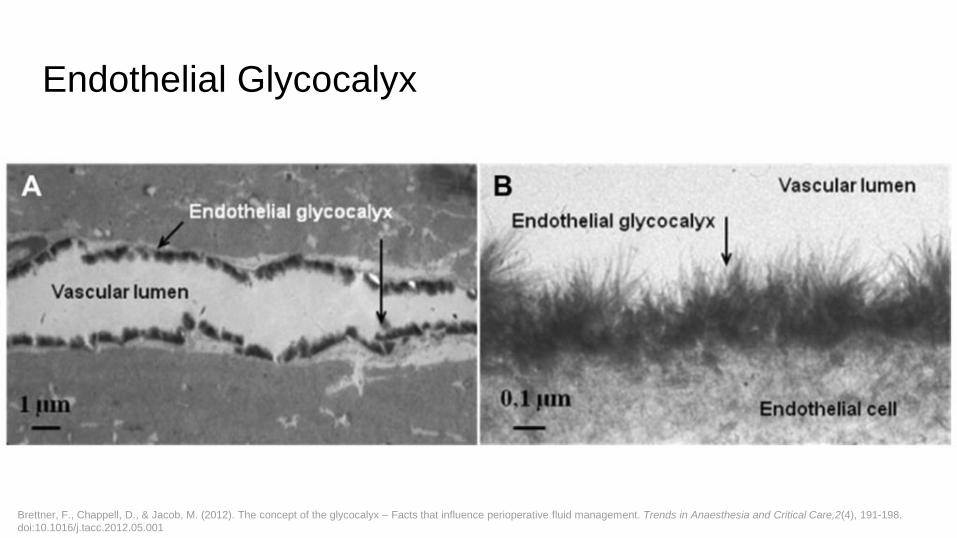
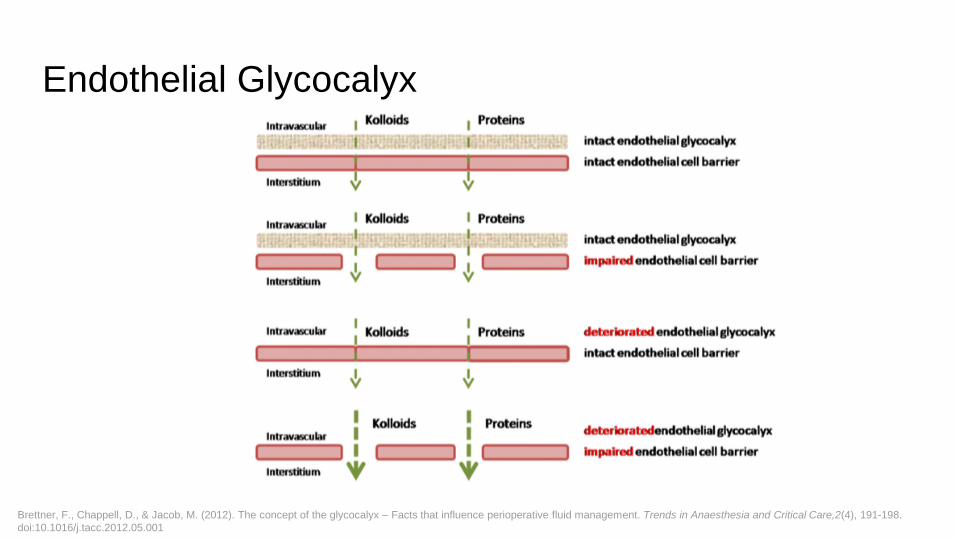
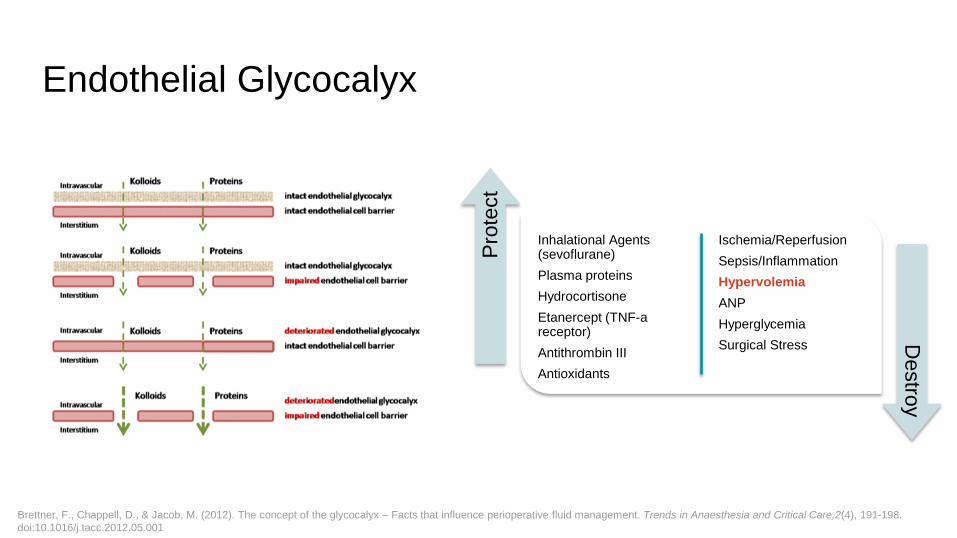
Endothelial Glycocalyx
Brettner, F., Chappell, D., & Jacob, M. (2012). The concept of the glycocalyx – Facts that influence perioperative fluid management. Trends in Anaesthesia and Critical Care,2(4), 191-198.
doi:10.1016/j.tacc.2012.05.001
Endothelial Glycocalyx
Brettner, F., Chappell, D., & Jacob, M. (2012). The concept of the glycocalyx – Facts that influence perioperative fluid management. Trends in Anaesthesia and Critical Care,2(4), 191-198.
doi:10.1016/j.tacc.2012.05.001
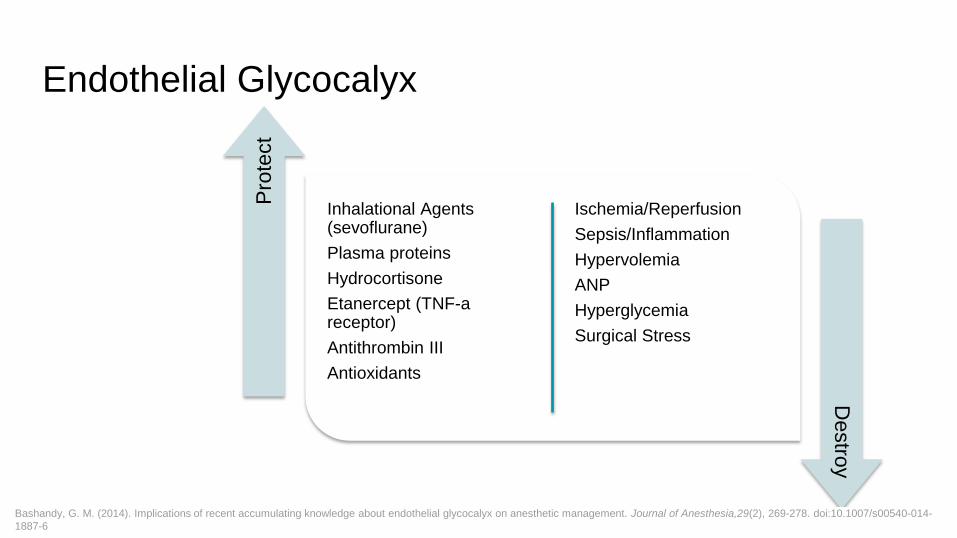
Endothelial Glycocalyx
Inhalational Agents (sevoflurane)
Plasma proteins
Hydrocortisone
Etanercept (TNF-a receptor)
Antithrombin III
Antioxidants
Ischemia/Reperfusion
Sepsis/Inflammation
Hypervolemia
ANP
Hyperglycemia
Surgical Stress
Pro
tect
Destro
y
Bashandy, G. M. (2014). Implications of recent accumulating knowledge about endothelial glycocalyx on anesthetic management. Journal of Anesthesia,29(2), 269-278. doi:10.1007/s00540-014-
1887-6
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
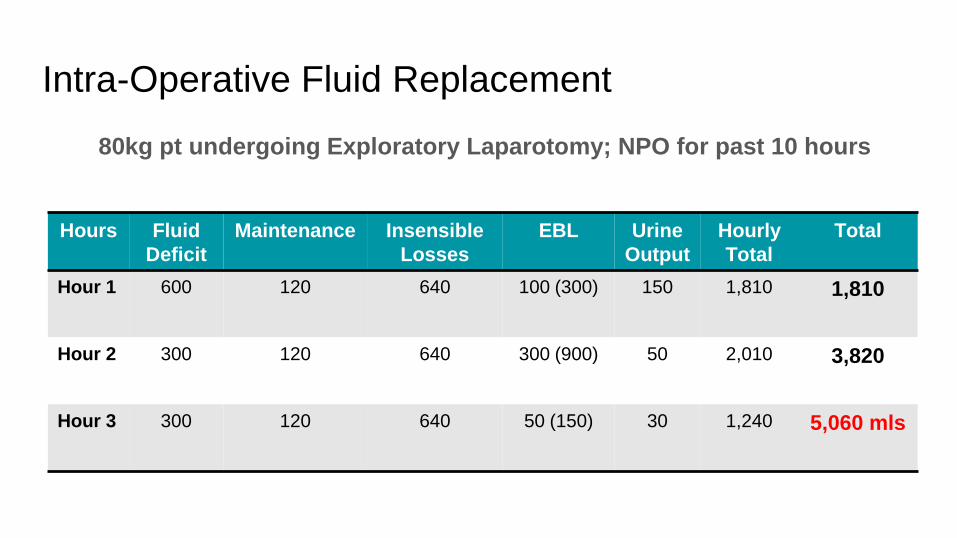
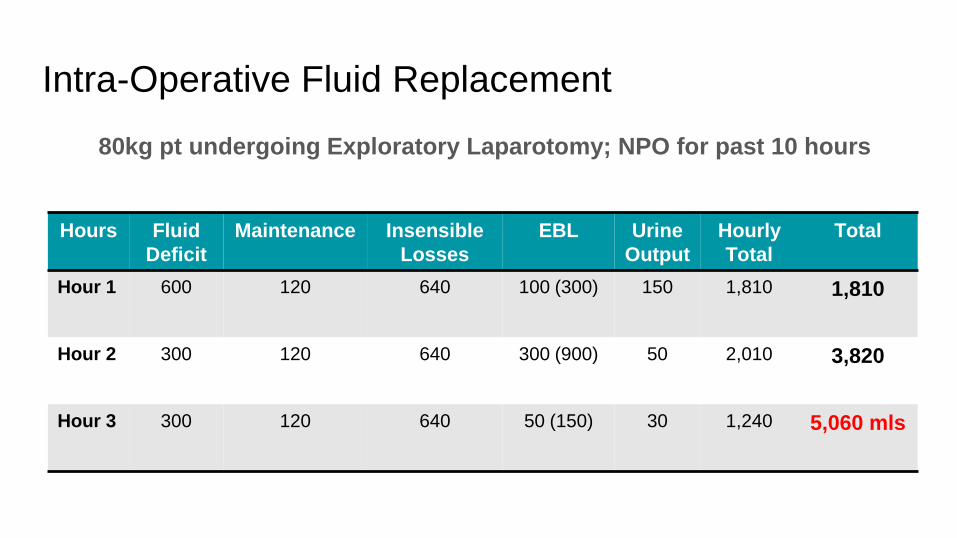
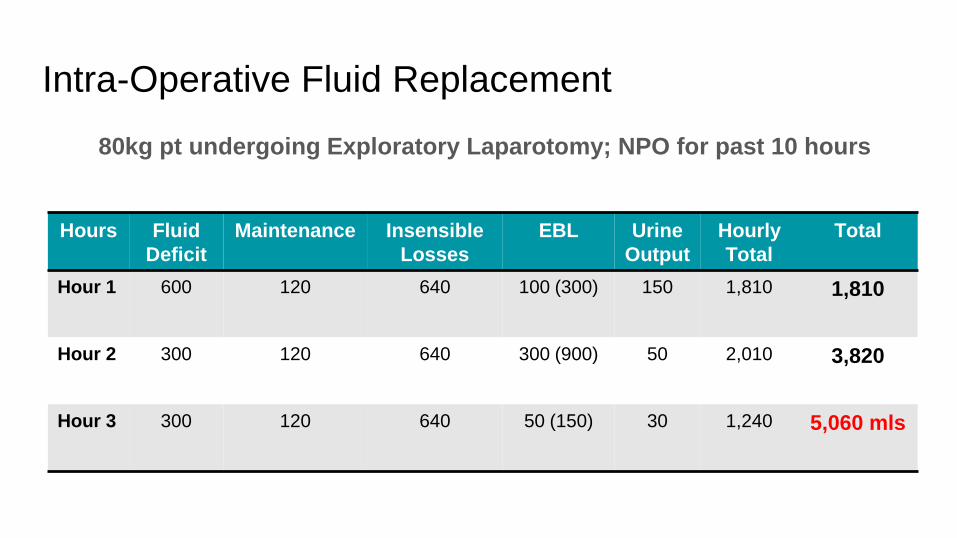
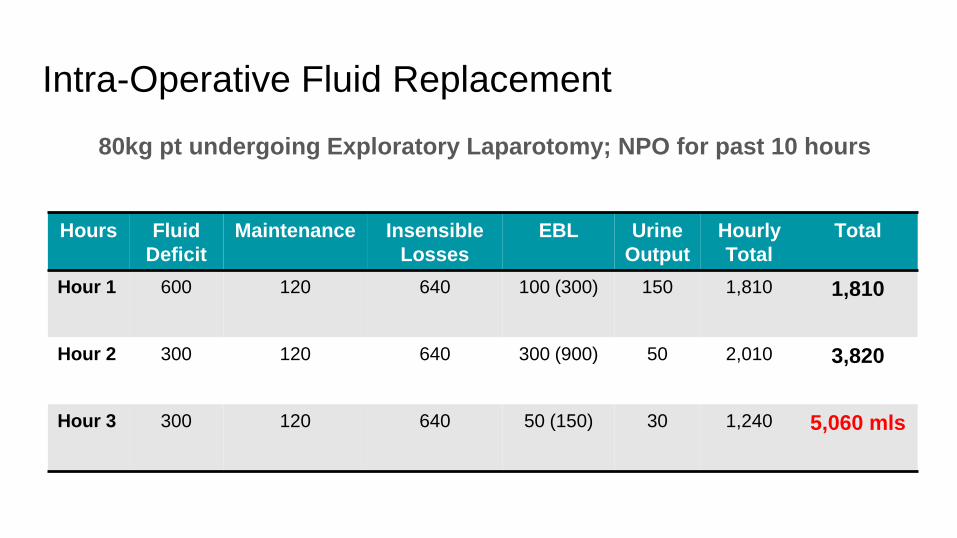
Intra-Operative Fluid Replacement
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
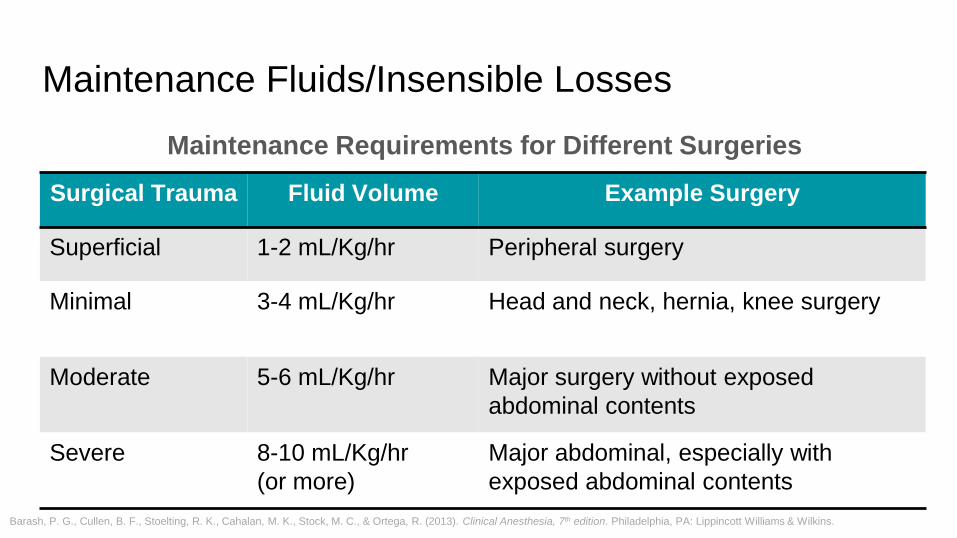
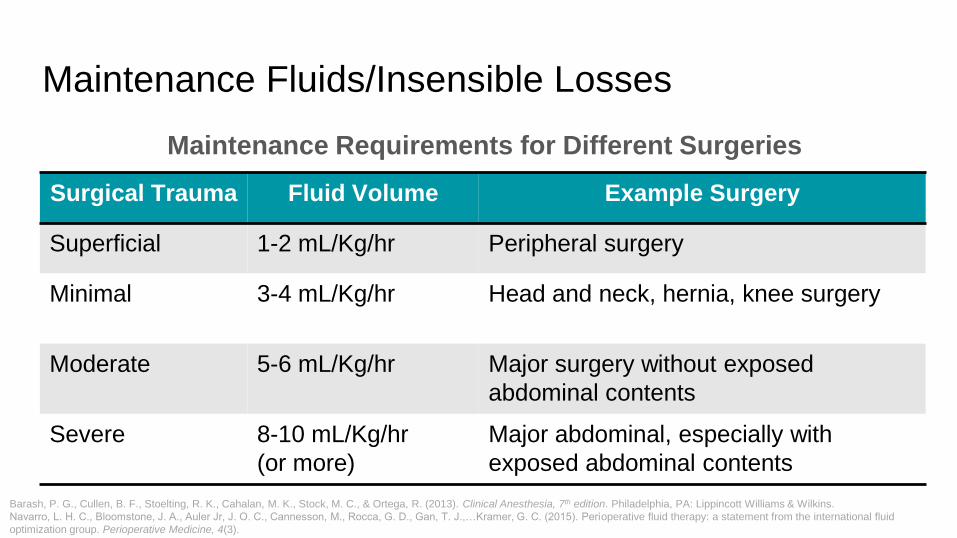
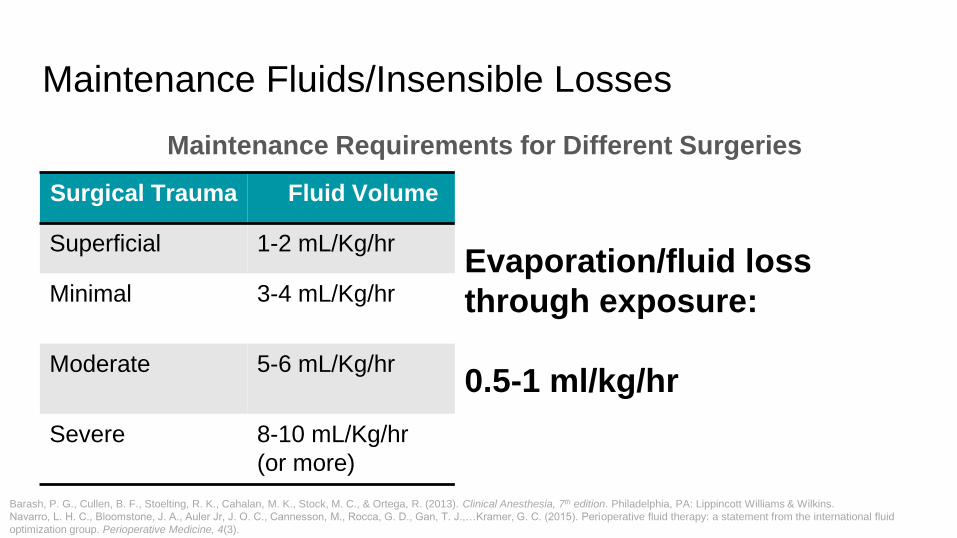
Maintenance Fluids/Insensible Losses
Maintenance Requirements for Different Surgeries
Surgical Trauma Fluid Volume Example Surgery
Superficial 1-2 mL/Kg/hr Peripheral surgery
Minimal 3-4 mL/Kg/hr Head and neck, hernia, knee surgery
Moderate 5-6 mL/Kg/hr Major surgery without exposed
abdominal contents
Severe 8-10 mL/Kg/hr
(or more)
Major abdominal, especially with
exposed abdominal contents
Barash, P. G., Cullen, B. F., Stoelting, R. K., Cahalan, M. K., Stock, M. C., & Ortega, R. (2013). Clinical Anesthesia, 7th edition. Philadelphia, PA: Lippincott Williams & Wilkins.
Intra-Operative Fluid Replacement
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
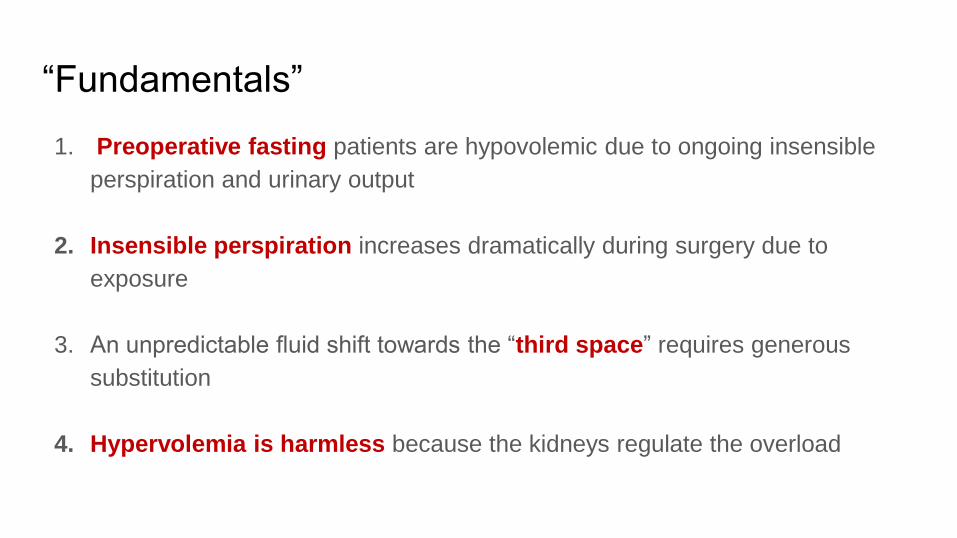
“Fundamentals”
1. Preoperative fasting patients are hypovolemic due to ongoing insensible
perspiration and urinary output
2. Insensible perspiration increases dramatically during surgery due to
exposure
3. An unpredictable fluid shift towards the “third space” requires generous
substitution
4. Hypervolemia is harmless because the kidneys regulate the overload
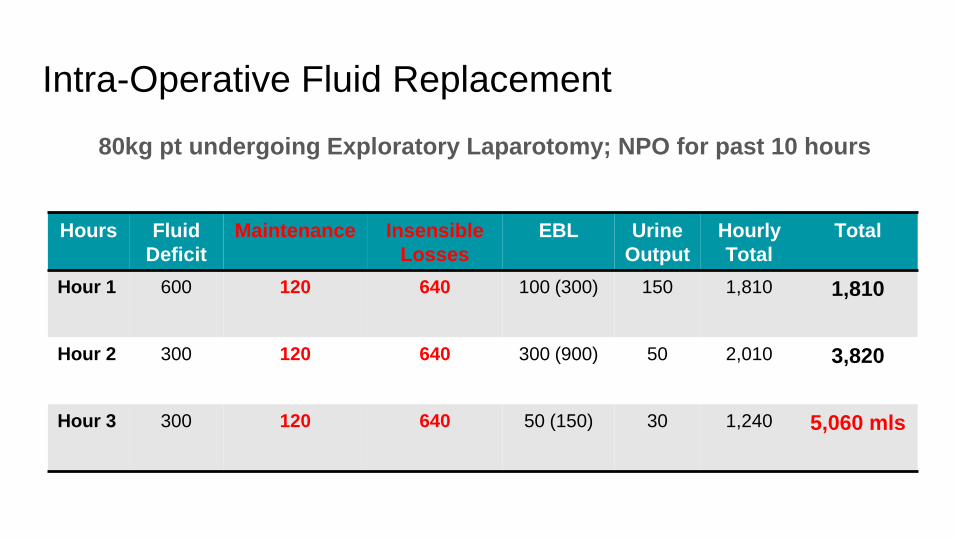
Intra-Operative Fluid Replacement
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
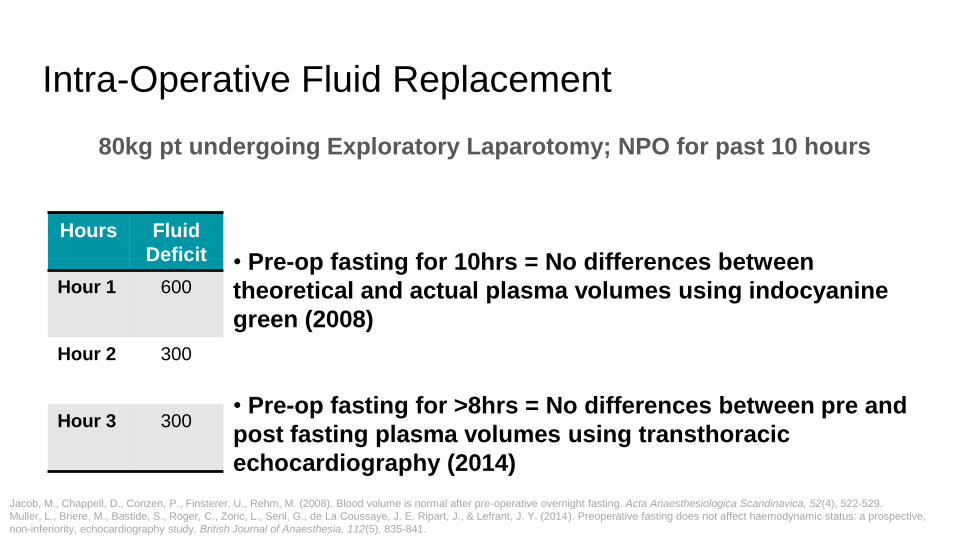
Intra-Operative Fluid Replacement
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
• Pre-op fasting for 10hrs = No differences between
theoretical and actual plasma volumes using indocyanine
green (2008)
• Pre-op fasting for >8hrs = No differences between pre and
post fasting plasma volumes using transthoracic
echocardiography (2014)
Jacob, M., Chappell, D., Conzen, P., Finsterer, U., Rehm, M. (2008). Blood volume is normal after pre-operative overnight fasting. Acta Anaesthesiologica Scandinavica, 52(4), 522-529.
Muller, L., Briere, M., Bastide, S., Roger, C., Zoric, L., Seni, G., de La Coussaye, J. E. Ripart, J., & Lefrant, J. Y. (2014). Preoperative fasting does not affect haemodynamic status: a prospective,
non-inferiority, echocardiography study. British Journal of Anaesthesia, 112(5), 835-841.
Intra-Operative Fluid Replacement
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
Maintenance Fluids/Insensible Losses
Maintenance Requirements for Different Surgeries
Surgical Trauma Fluid Volume Example Surgery
Superficial 1-2 mL/Kg/hr Peripheral surgery
Minimal 3-4 mL/Kg/hr Head and neck, hernia, knee surgery
Moderate 5-6 mL/Kg/hr Major surgery without exposed
abdominal contents
Severe 8-10 mL/Kg/hr
(or more)
Major abdominal, especially with
exposed abdominal contents
Barash, P. G., Cullen, B. F., Stoelting, R. K., Cahalan, M. K., Stock, M. C., & Ortega, R. (2013). Clinical Anesthesia, 7th edition. Philadelphia, PA: Lippincott Williams & Wilkins.
Navarro, L. H. C., Bloomstone, J. A., Auler Jr, J. O. C., Cannesson, M., Rocca, G. D., Gan, T. J.,…Kramer, G. C. (2015). Perioperative fluid therapy: a statement from the international fluid
optimization group. Perioperative Medicine, 4(3).
Maintenance Fluids/Insensible Losses
Maintenance Requirements for Different Surgeries
Surgical Trauma Fluid Volume Example Surgery
Superficial 1-2 mL/Kg/hr Peripheral surgery
Minimal 3-4 mL/Kg/hr Head and neck, hernia, knee surgery
Moderate 5-6 mL/Kg/hr Major surgery without exposed
abdominal contents
Severe 8-10 mL/Kg/hr
(or more)
Major abdominal, especially with
exposed abdominal contents
Barash, P. G., Cullen, B. F., Stoelting, R. K., Cahalan, M. K., Stock, M. C., & Ortega, R. (2013). Clinical Anesthesia, 7th edition. Philadelphia, PA: Lippincott Williams & Wilkins.
Navarro, L. H. C., Bloomstone, J. A., Auler Jr, J. O. C., Cannesson, M., Rocca, G. D., Gan, T. J.,…Kramer, G. C. (2015). Perioperative fluid therapy: a statement from the international fluid
optimization group. Perioperative Medicine, 4(3).
Evaporation/fluid loss
through exposure:
0.5-1 ml/kg/hr
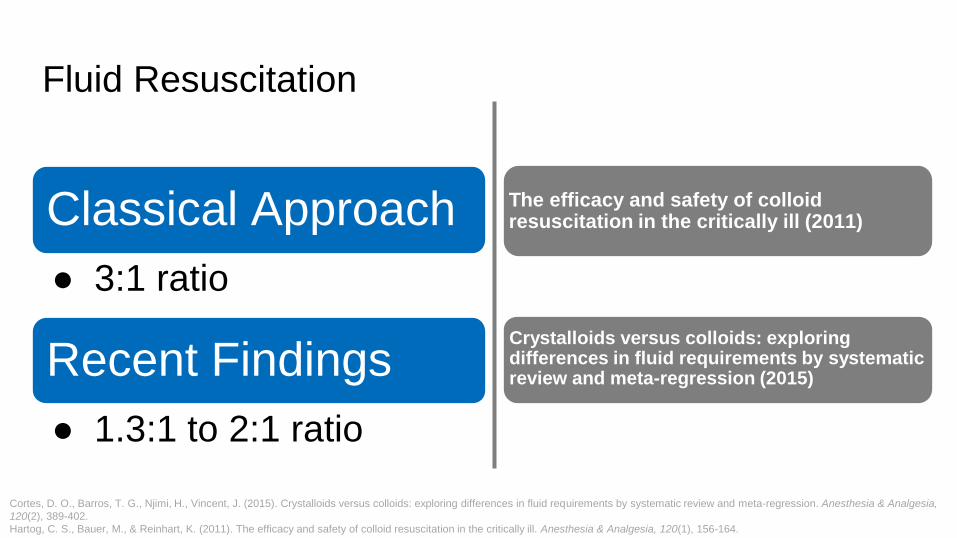
Fluid Resuscitation
Classical Approach
● 3:1 ratio
Recent Findings
● 1.3:1 to 2:1 ratio
Cortes, D. O., Barros, T. G., Njimi, H., Vincent, J. (2015). Crystalloids versus colloids: exploring differences in fluid requirements by systematic review and meta-regression. Anesthesia & Analgesia,
120(2), 389-402.
Hartog, C. S., Bauer, M., & Reinhart, K. (2011). The efficacy and safety of colloid resuscitation in the critically ill. Anesthesia & Analgesia, 120(1), 156-164.
The efficacy and safety of colloid resuscitation in the critically ill (2011)
Crystalloids versus colloids: exploring differences in fluid requirements by systematic review and meta-regression (2015)
Intra-Operative Fluid Replacement
80kg pt undergoing Exploratory Laparotomy; NPO for past 10 hours
Hours Fluid
Deficit
Maintenance Insensible
Losses
EBL Urine
Output
Hourly
Total
Total
Hour 1 600 120 640 100 (300) 150 1,810 1,810
Hour 2 300 120 640 300 (900) 50 2,010 3,820
Hour 3 300 120 640 50 (150) 30 1,240 5,060 mls
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
Goal-Directed Fluid Therapy Map
History of Fluid Management
Significance of Fluid Management
Fluid Compartment Physiology
Traditional Theories of Fluid Management
Fluid Management Indicators & Interventions
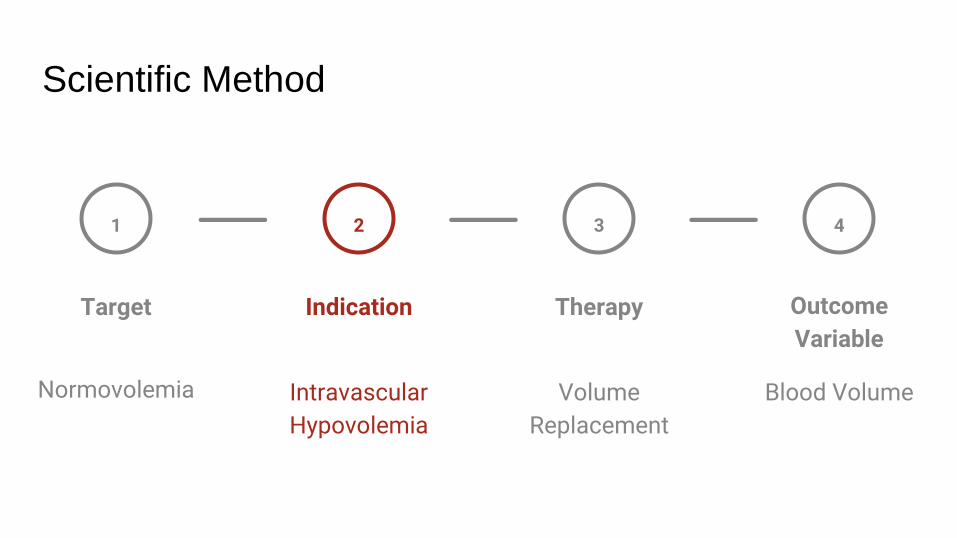
● Scientific Method
● Traditional Indicators
● Advanced Indicators
● Pharmacokinetic Indicator: Volume Effect
● Crystalloid vs. Colloid
Indications and Interventions
Volume
Replacement
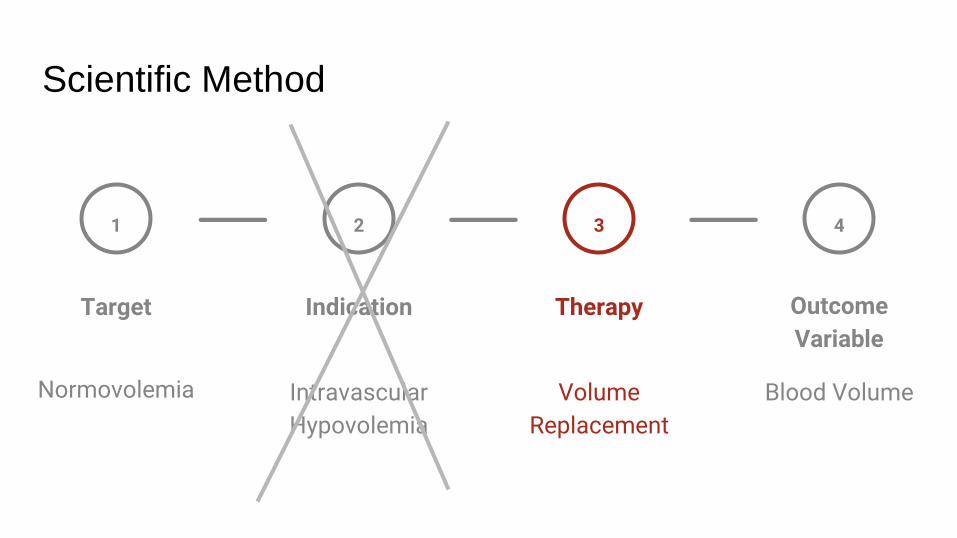
Scientific Method
1
Target
Normovolemia
Indication
Intravascular
Hypovolemia
2
Therapy
3
Outcome
Variable
Blood Volume
4
Volume
Replacement
Scientific Method
1
Target
Normovolemia
Indication
Intravascular
Hypovolemia
2
Therapy
3
Outcome
Variable
Blood Volume
4
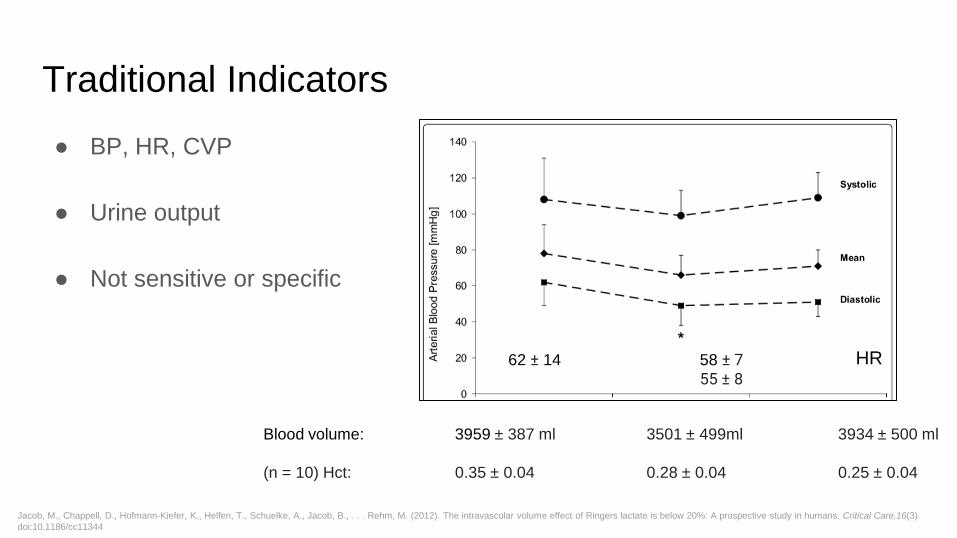
Traditional Indicators
● BP, HR, CVP
● Urine output
● Not sensitive or specific
62 ± 14 58 ± 7 55 ± 8
HR
Blood volume: 3959 ± 387 ml 3501 ± 499ml 3934 ± 500 ml
(n = 10) Hct: 0.35 ± 0.04 0.28 ± 0.04 0.25 ± 0.04
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
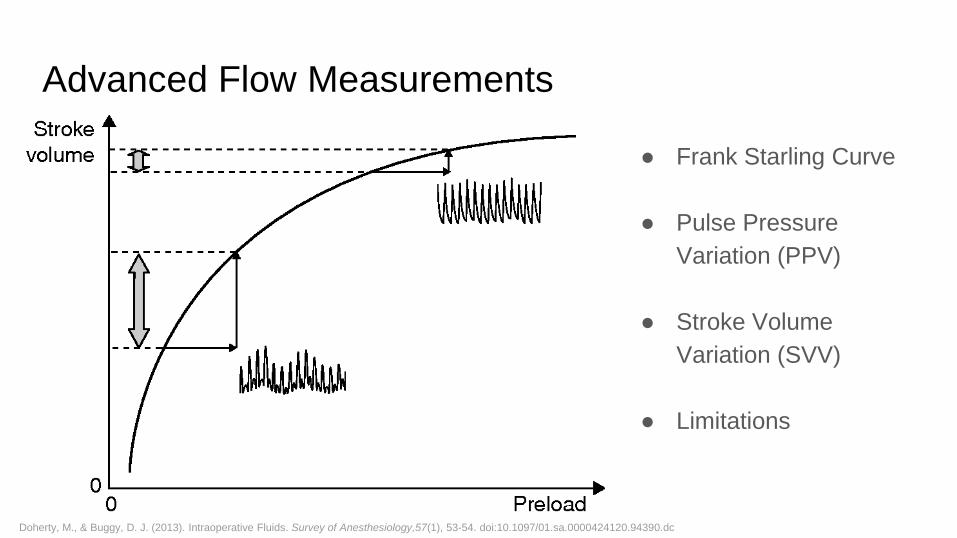
Advanced Flow Measurements
● Frank Starling Curve
● Pulse Pressure
Variation (PPV)
● Stroke Volume
Variation (SVV)
● Limitations
Doherty, M., & Buggy, D. J. (2013). Intraoperative Fluids. Survey of Anesthesiology,57(1), 53-54. doi:10.1097/01.sa.0000424120.94390.dc
✓ Scientific Method
✓ Traditional Indicators
✓ Advanced Indicators
● Pharmacokinetic Indicator: Volume Effect
● Crystalloid vs. Colloid
Indications and Interventions
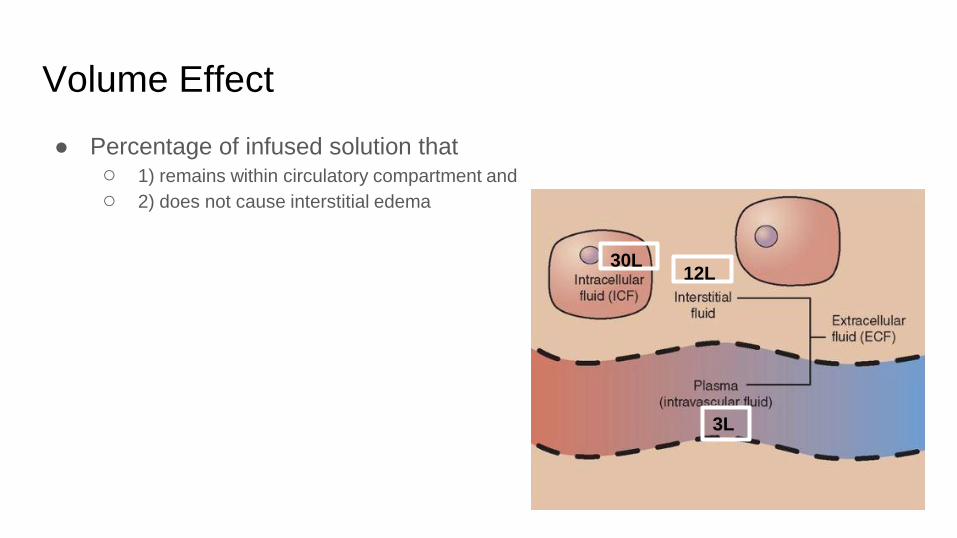
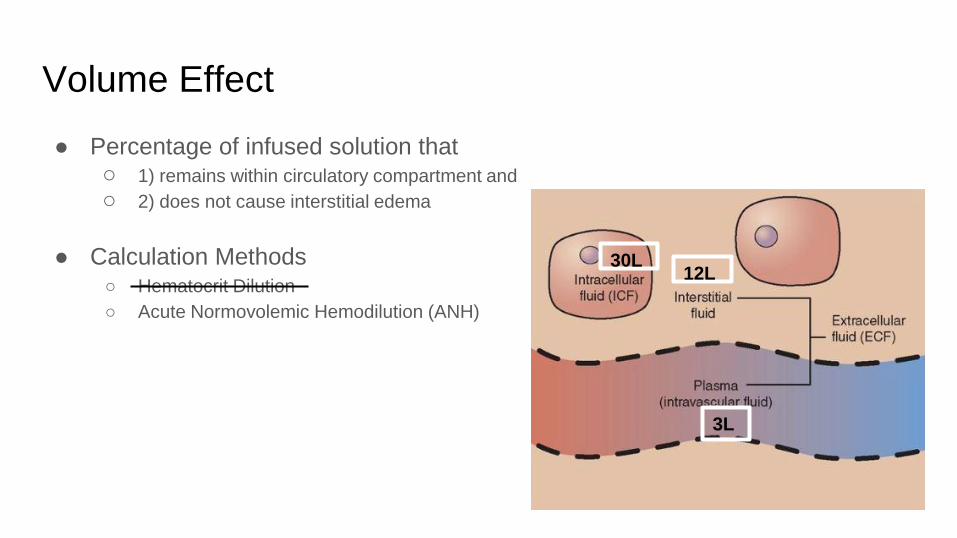
● Percentage of infused solution that ○ 1) remains within circulatory compartment and
○ 2) does not cause interstitial edema
Volume Effect
30L 12L
3L
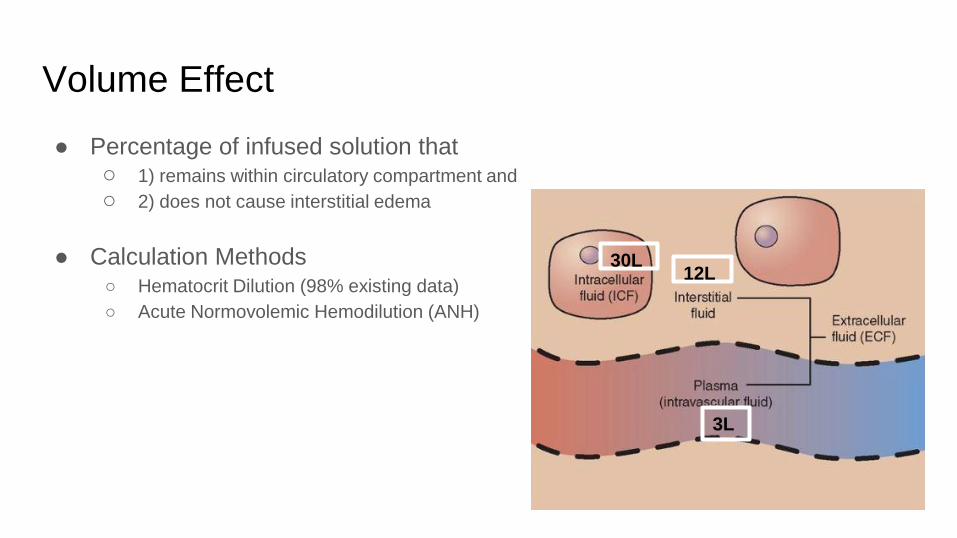
● Percentage of infused solution that ○ 1) remains within circulatory compartment and
○ 2) does not cause interstitial edema
● Calculation Methods ○ Hematocrit Dilution (98% existing data)
○ Acute Normovolemic Hemodilution (ANH)
Volume Effect
30L 12L
3L
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
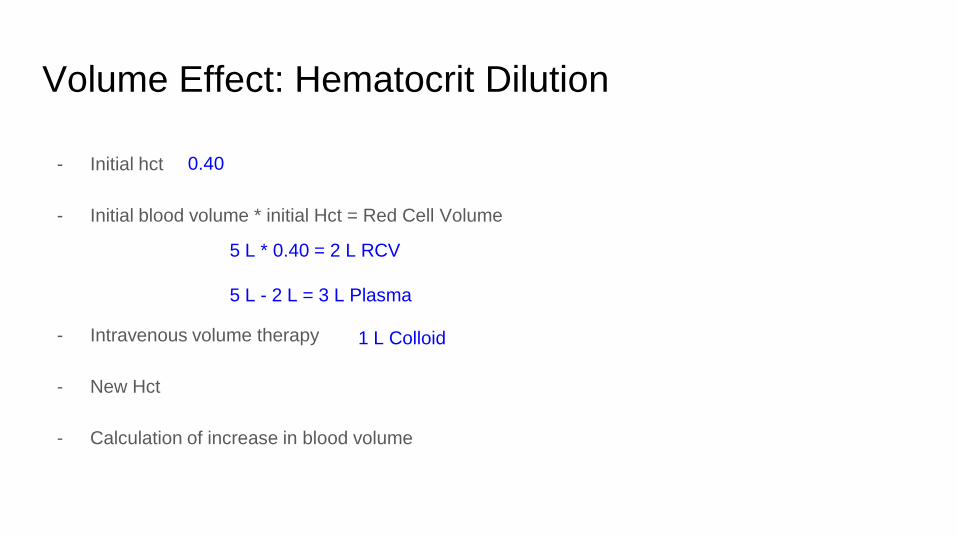
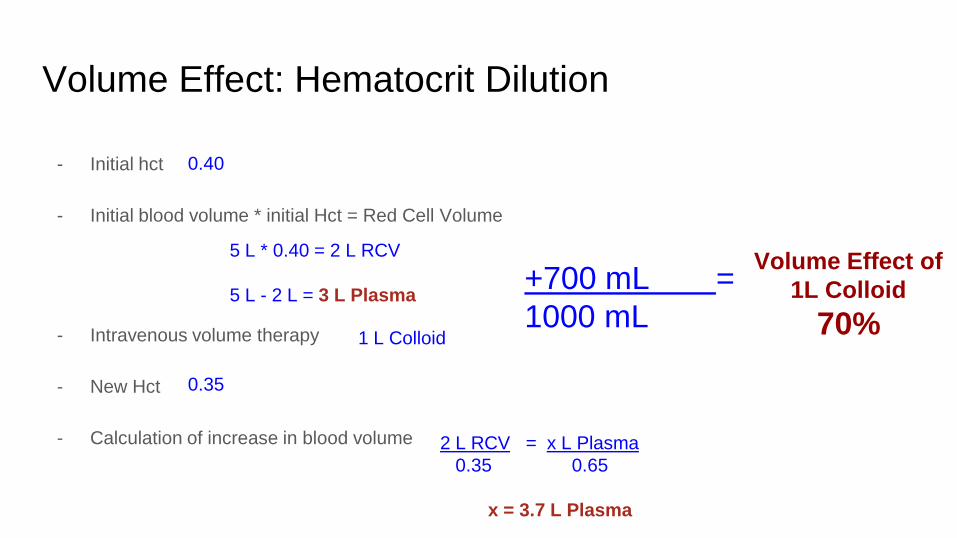
Volume Effect: Hematocrit Dilution
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
Volume Effect: Hematocrit Dilution
0.40
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
Volume Effect: Hematocrit Dilution
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
0.40
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
Volume Effect: Hematocrit Dilution
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
1 L Colloid
0.40
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
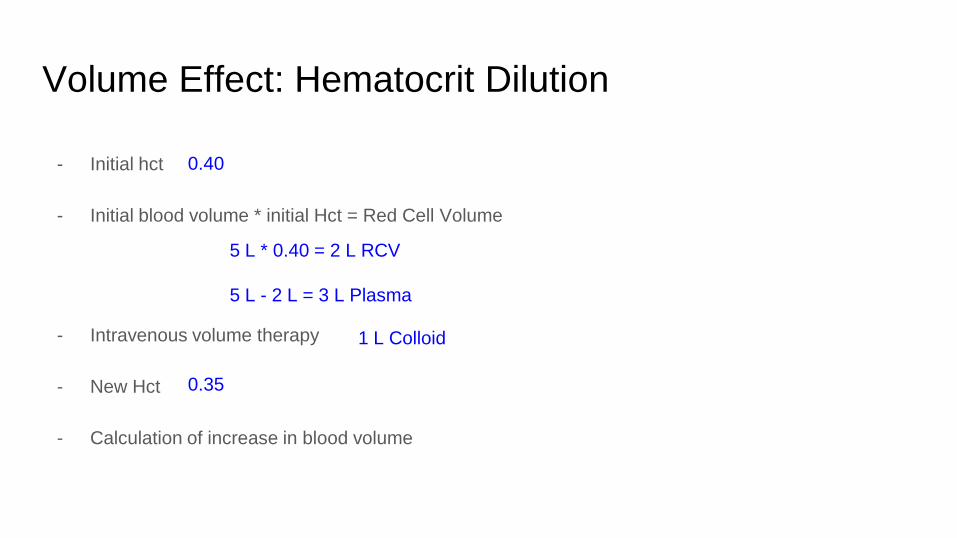
Volume Effect: Hematocrit Dilution
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
1 L Colloid
0.35
0.40
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
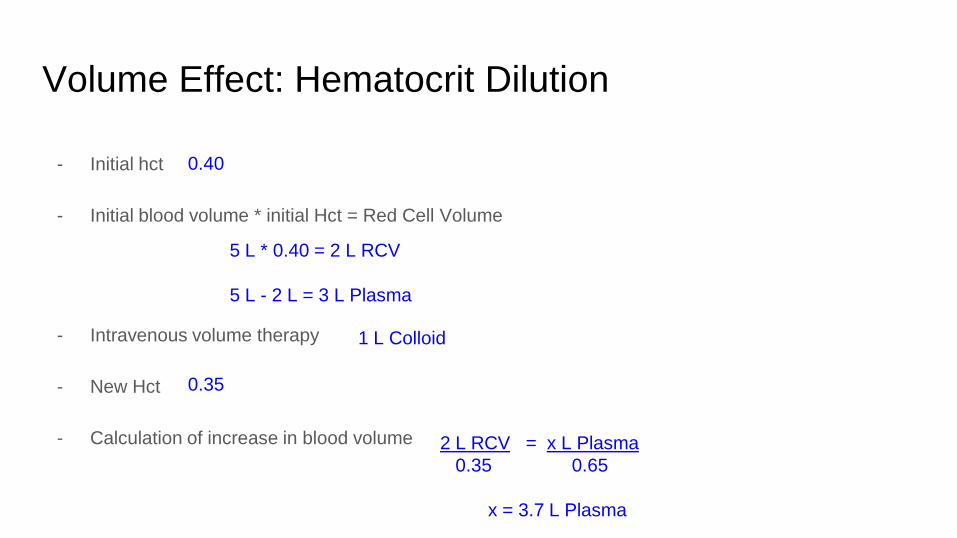
Volume Effect: Hematocrit Dilution
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
1 L Colloid
0.35
2 L RCV = x L Plasma
0.35 0.65
x = 3.7 L Plasma
0.40
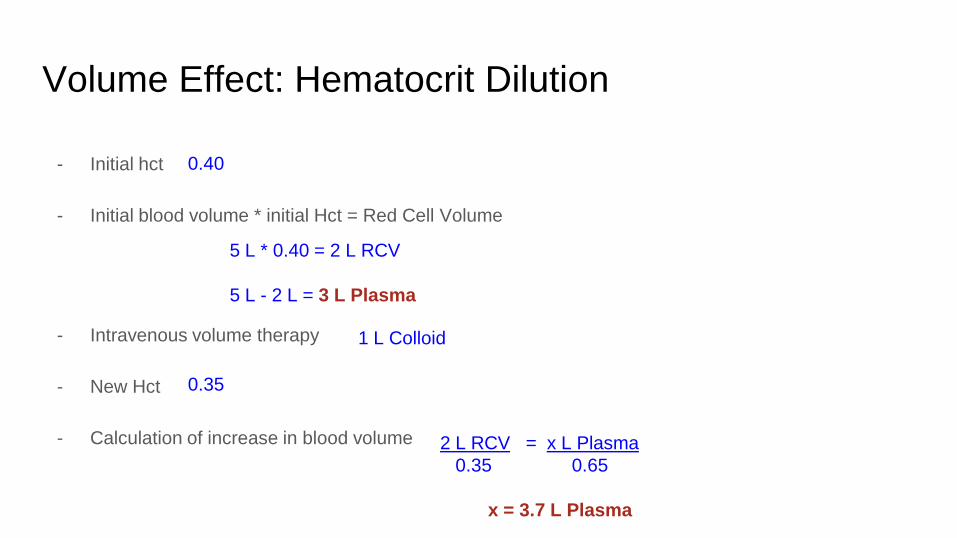
Volume Effect: Hematocrit Dilution
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
1 L Colloid
0.35
2 L RCV = x L Plasma
0.35 0.65
x = 3.7 L Plasma
0.40
Volume Effect: Hematocrit Dilution
Volume Effect of
1L Colloid
70%
- Initial hct
- Initial blood volume * initial Hct = Red Cell Volume
- Intravenous volume therapy
- New Hct
- Calculation of increase in blood volume
+700 mL =
1000 mL
5 L * 0.40 = 2 L RCV
5 L - 2 L = 3 L Plasma
1 L Colloid
0.35
2 L RCV = x L Plasma
0.35 0.65
x = 3.7 L Plasma
0.40
Endothelial Glycocalyx
Inhalational Agents (sevoflurane)
Plasma proteins
Hydrocortisone
Etanercept (TNF-a receptor)
Antithrombin III
Antioxidants
Ischemia/Reperfusion
Sepsis/Inflammation
Hypervolemia
ANP
Hyperglycemia
Surgical Stress
Pro
tect
Destro
y
Brettner, F., Chappell, D., & Jacob, M. (2012). The concept of the glycocalyx – Facts that influence perioperative fluid management. Trends in Anaesthesia and Critical Care,2(4), 191-198.
doi:10.1016/j.tacc.2012.05.001
● Percentage of infused solution that ○ 1) remains within circulatory compartment and
○ 2) does not cause interstitial edema
● Calculation Methods ○ Hematocrit Dilution
○ Acute Normovolemic Hemodilution (ANH)
Volume Effect
30L 12L
3L
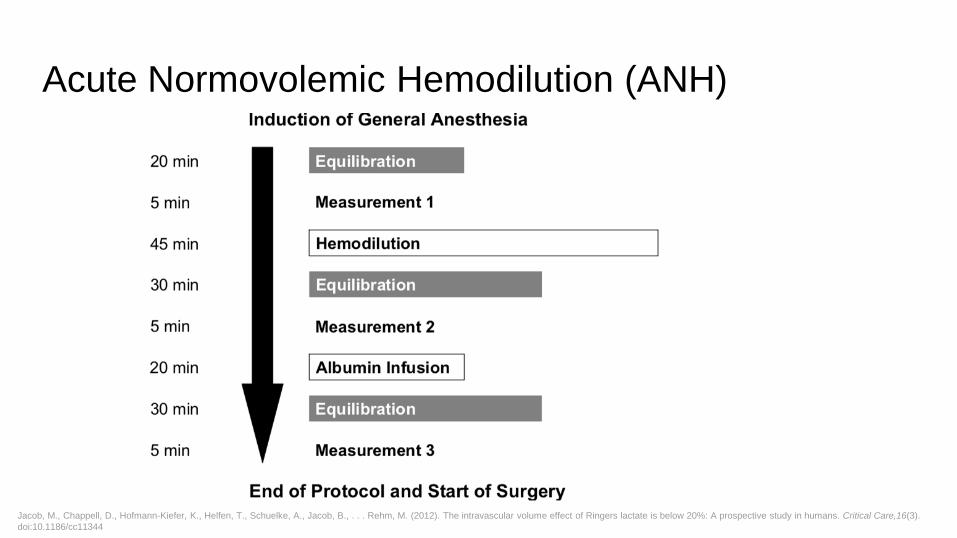
Acute Normovolemic Hemodilution (ANH)
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
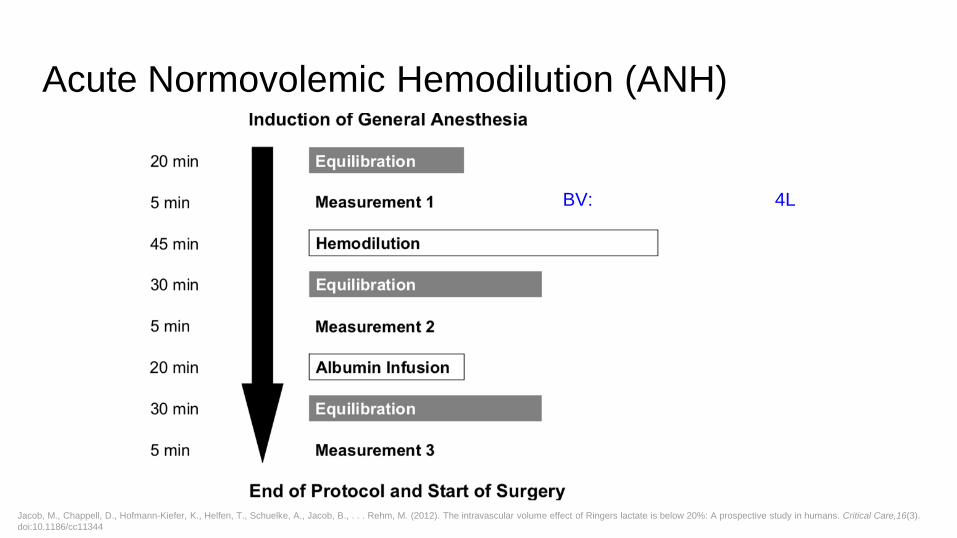
Acute Normovolemic Hemodilution (ANH)
BV: 4L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
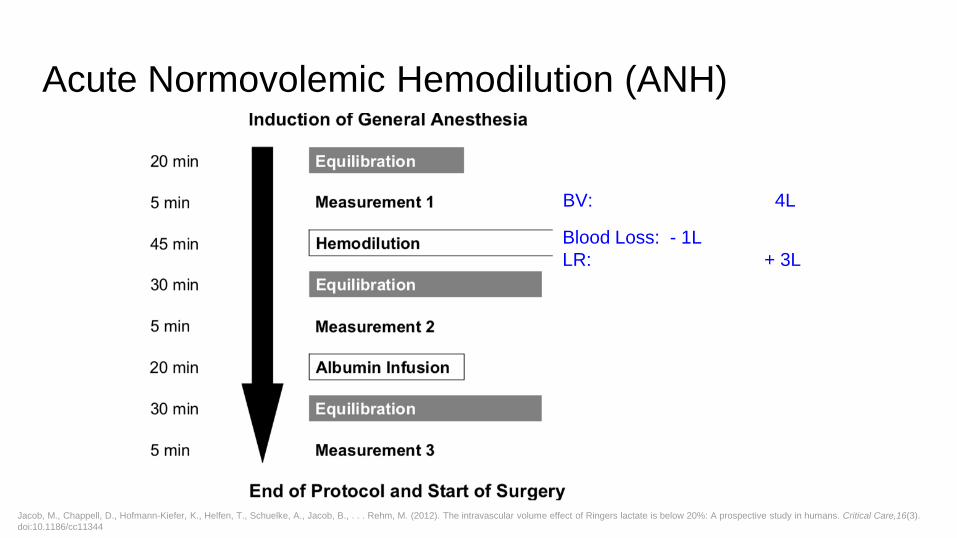
Acute Normovolemic Hemodilution (ANH)
BV: 4L
Blood Loss: - 1L
LR: + 3L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
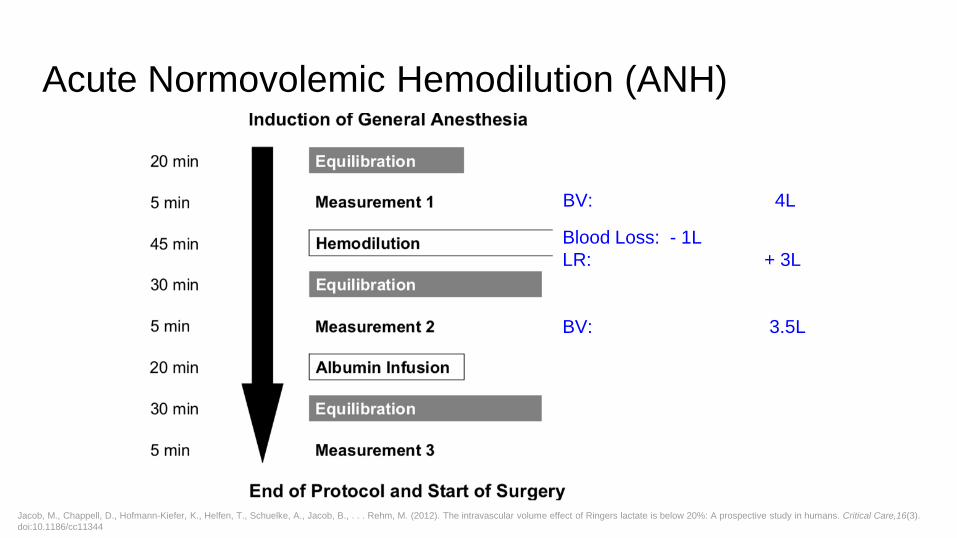
Acute Normovolemic Hemodilution (ANH)
BV: 4L
Blood Loss: - 1L
LR: + 3L
BV: 3.5L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
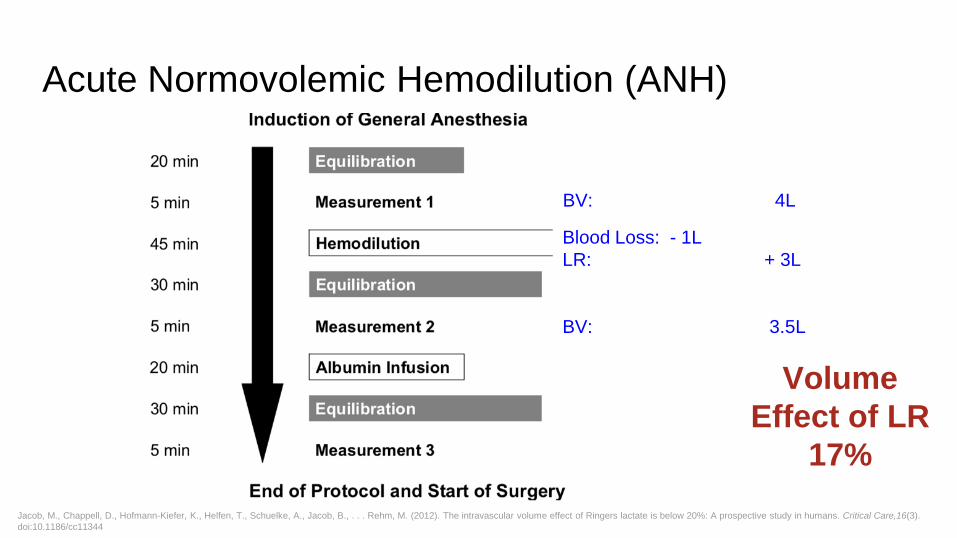
Acute Normovolemic Hemodilution (ANH)
BV: 4L
Blood Loss: - 1L
LR: + 3L
BV: 3.5L
Volume
Effect of LR
17%
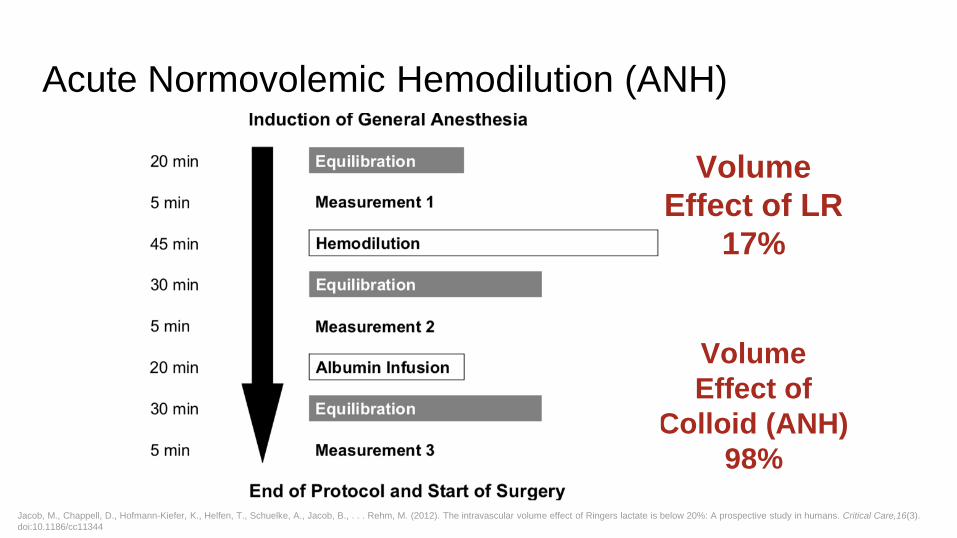
Acute Normovolemic Hemodilution (ANH)
BV:
4L Blood Loss: - 1L
LR:
+ 3L
BV:
3.5L
Volume
Effect of LR
17%
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Acute Normovolemic Hemodilution (ANH)
BV: 4.1 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
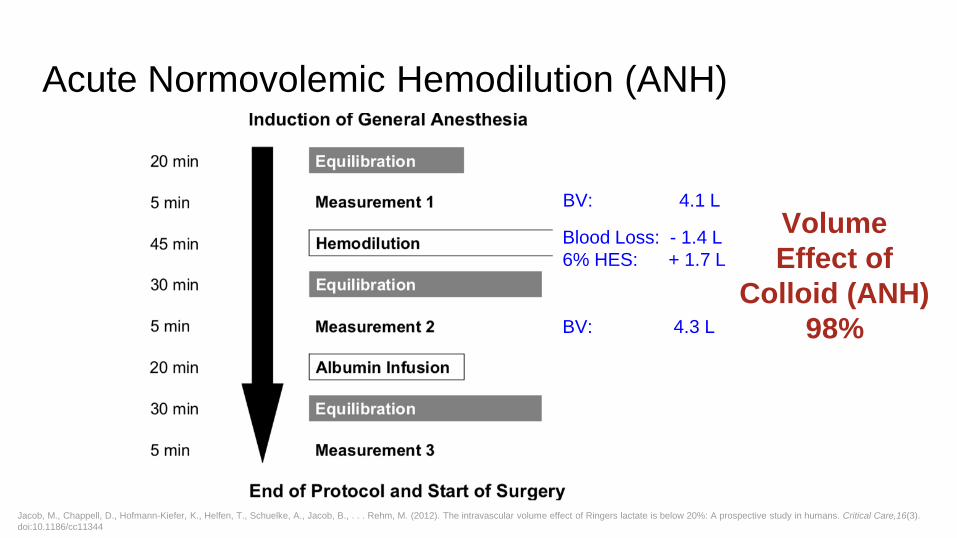
Acute Normovolemic Hemodilution (ANH)
BV: 4.1 L
Blood Loss: - 1.4 L
6% HES: + 1.7 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
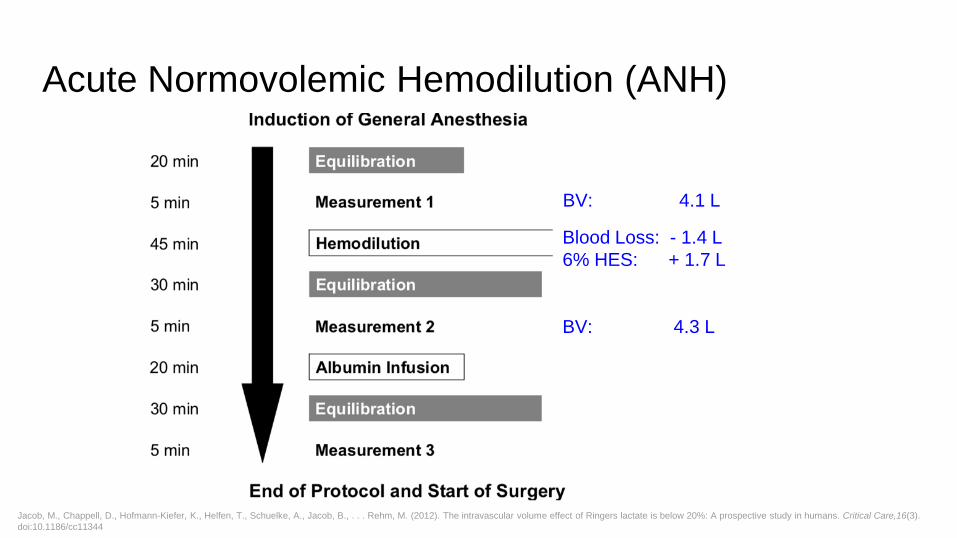
Acute Normovolemic Hemodilution (ANH)
BV: 4.1 L
Blood Loss: - 1.4 L
6% HES: + 1.7 L
BV: 4.3 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Acute Normovolemic Hemodilution (ANH)
BV: 4.1 L
Blood Loss: - 1.4 L
6% HES: + 1.7 L
BV: 4.3 L
Volume
Effect of
Colloid (ANH)
98%
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
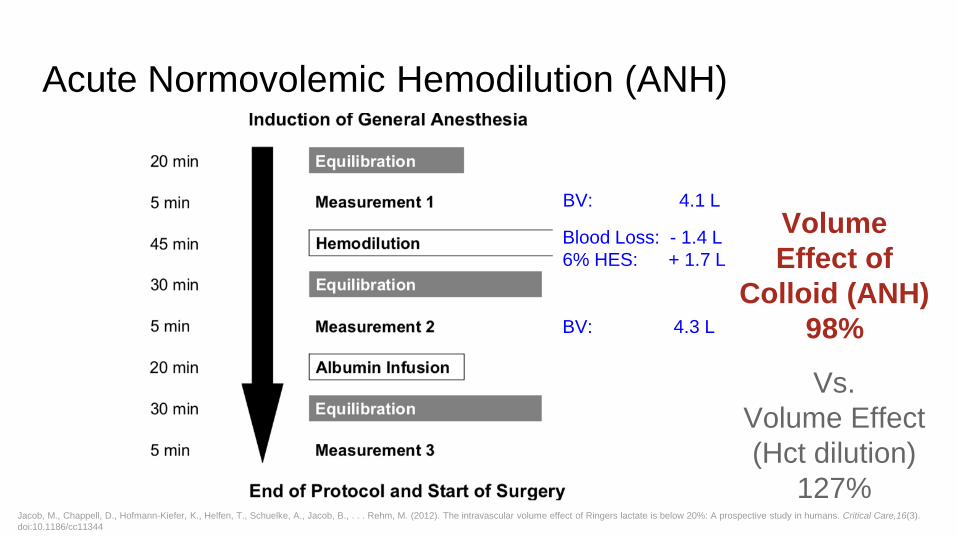
Acute Normovolemic Hemodilution (ANH)
BV: 4.1 L
Blood Loss: - 1.4 L
6% HES: + 1.7 L
BV: 4.3 L
Volume
Effect of
Colloid (ANH)
98%
Vs.
Volume Effect
(Hct dilution)
127%
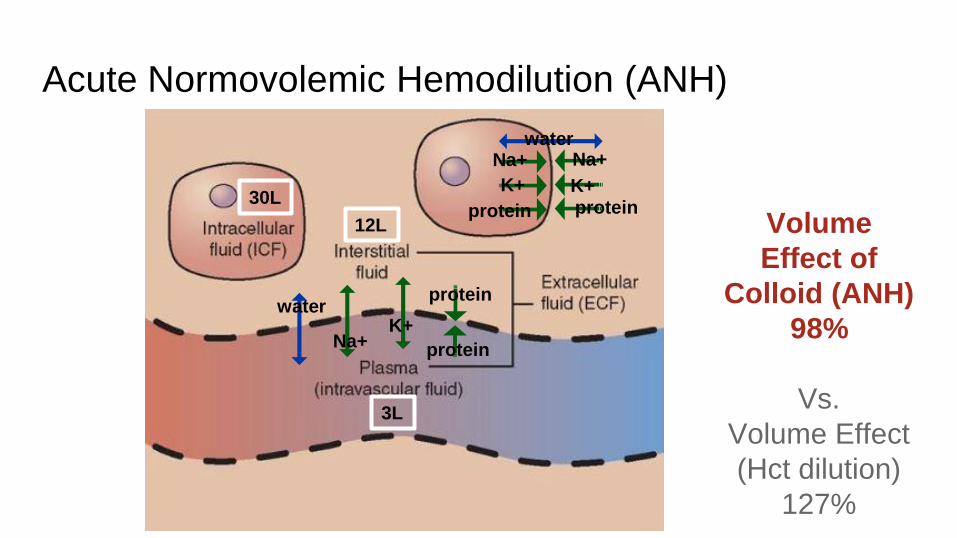
Acute Normovolemic Hemodilution (ANH)
Volume
Effect of
Colloid (ANH)
98%
Vs.
Volume Effect
(Hct dilution)
127%
30L
12L
3L
water Na+ Na+
K+ K+ protein protein
water
Na+ K+
protein
protein
Acute Normovolemic Hemodilution (ANH)
Volume
Effect of LR
17%
Volume
Effect of
Colloid (ANH)
98%
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Volume
Replacement
Scientific Method
1
Target
Normovolemia
Indication
Intravascular
Hypovolemia
2
Therapy
3
Outcome
Variable
Blood Volume
4
Scientific Method
Volume
Replacement
1
Target
Normovolemia
Indication
Intravascular
Hypovolemia
2
Therapy
3
Outcome
Variable
Blood Volume
4
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
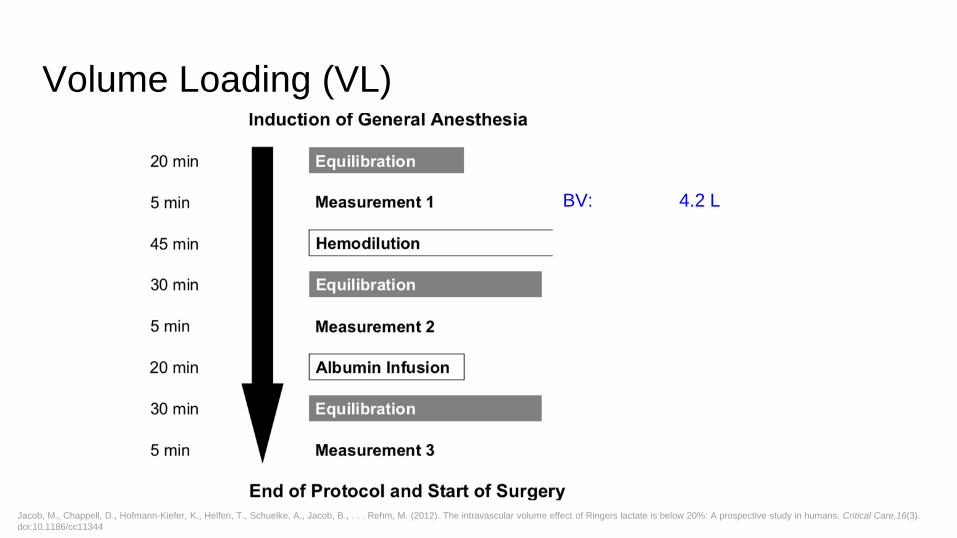
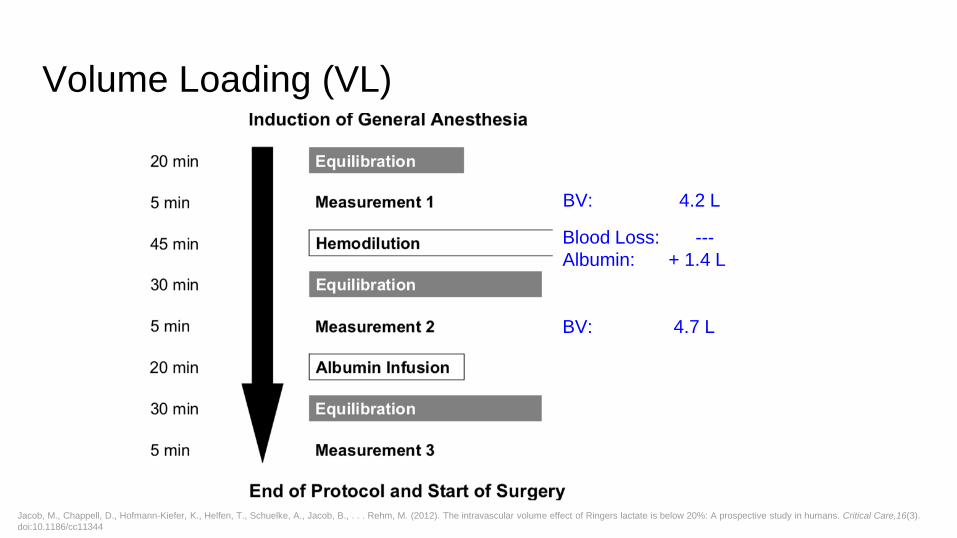
Volume Loading (VL)
BV: 4.2 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
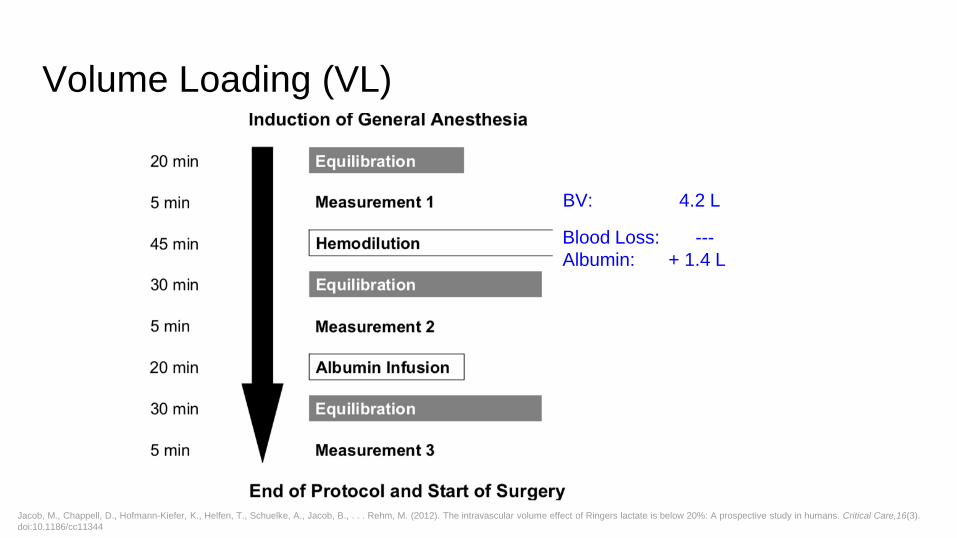
Volume Loading (VL)
BV: 4.2 L
Blood Loss: ---
Albumin: + 1.4 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
Volume Loading (VL)
BV: 4.2 L
Blood Loss: ---
Albumin: + 1.4 L
BV: 4.7 L
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
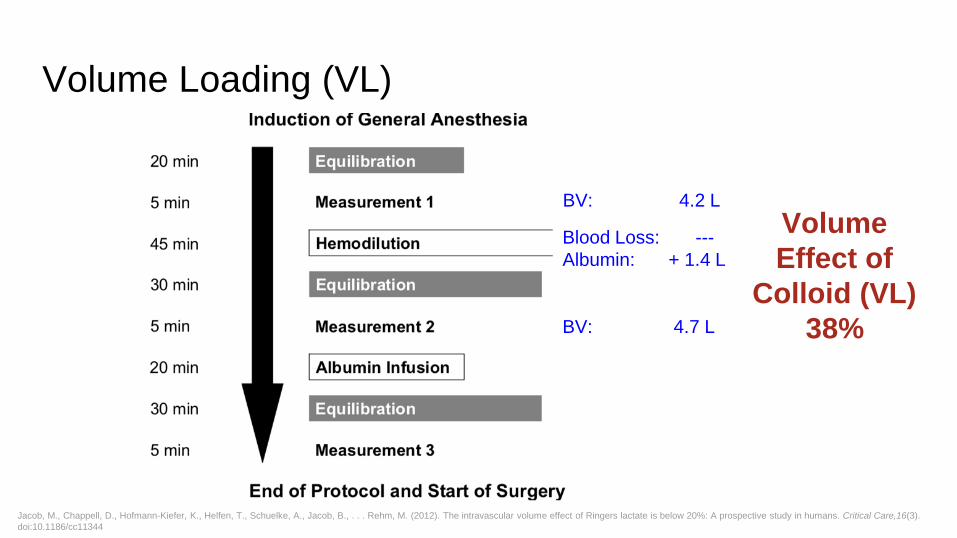
Volume Loading (VL)
BV: 4.2 L
Blood Loss: ---
Albumin: + 1.4 L
BV: 4.7 L
Volume
Effect of
Colloid (VL)
38%
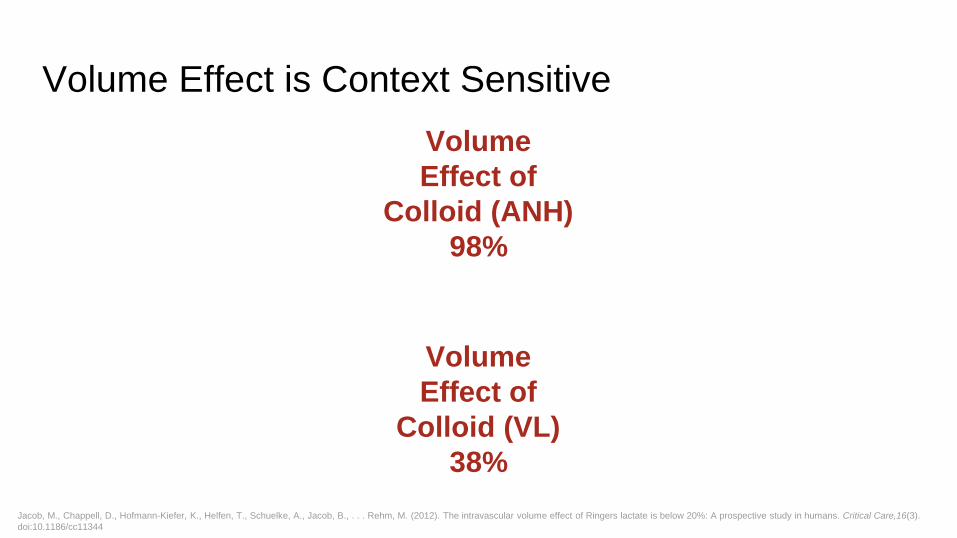
Volume Effect is Context Sensitive
Volume
Effect of
Colloid (VL)
38%
Volume
Effect of
Colloid (ANH)
98%
Jacob, M., Chappell, D., Hofmann-Kiefer, K., Helfen, T., Schuelke, A., Jacob, B., . . . Rehm, M. (2012). The intravascular volume effect of Ringers lactate is below 20%: A prospective study in humans. Critical Care,16(3).
doi:10.1186/cc11344
✓ Scientific Method
✓ Traditional Indicators
✓ Advanced Indicators
✓ Pharmacokinetic Indicator: Volume Effect
● Crystalloid vs. Colloid
Indications and Interventions
Crystalloid Colloid
Why Should I Care?
- Hypervolemia and hypovolemia are not benign.
- Evidence challenges traditional theories of fluid replacement and indicators.
- Integrity of the EGL has many implications for perioperative fluid therapy
(namely, hypervolemia, surgical stress, ischemia).
- Volume effect is context sensitive. Proper indications matter.
THANK YOU!