goal directed therapy - emergency laparotomy...
TRANSCRIPT

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Goal Directed Therapy
Dr Maurizio Cecconi MD FRCA FFICM MD(Res) Consultant and Reader
Anaesthesia and Intensive Care Medicine St George’s University Hospital NHS Foundation Trust
St George’s University of London

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Disclosure
• Edwards Lifesciences
• LiDCO
• Cheetah Medical
• Masimo
• Bmeye
• Deltex
• Applied Physiology
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
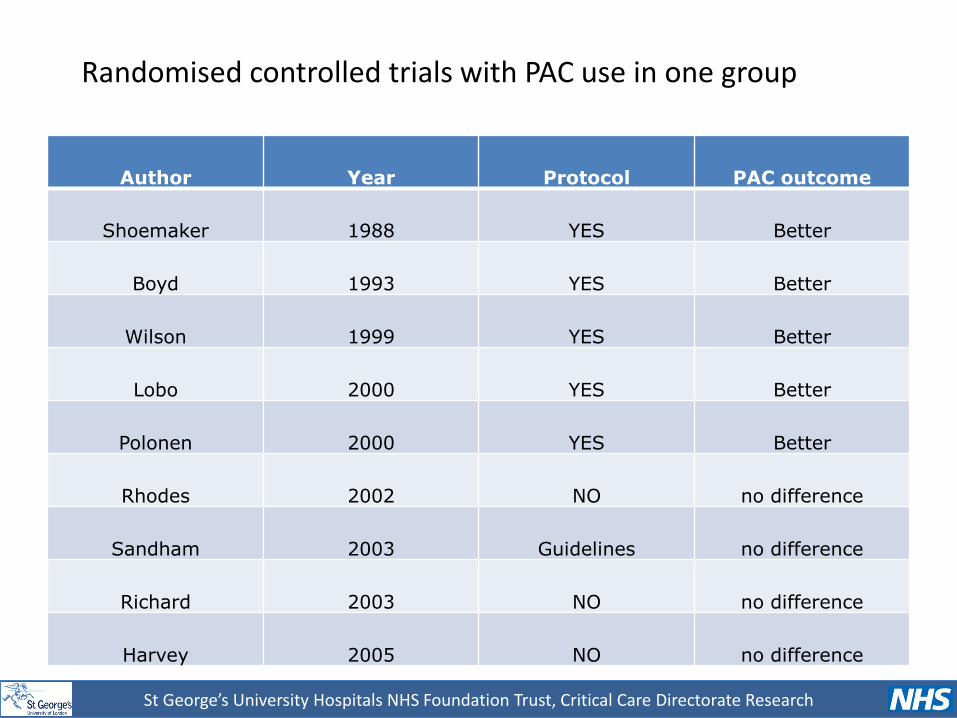
Author Year Protocol PAC outcome
Shoemaker 1988 YES Better
Boyd 1993 YES Better
Wilson 1999 YES Better
Lobo 2000 YES Better
Polonen 2000 YES Better
Rhodes 2002 NO no difference
Sandham 2003 Guidelines no difference
Richard 2003 NO no difference
Harvey 2005 NO no difference
Randomised controlled trials with PAC use in one group

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
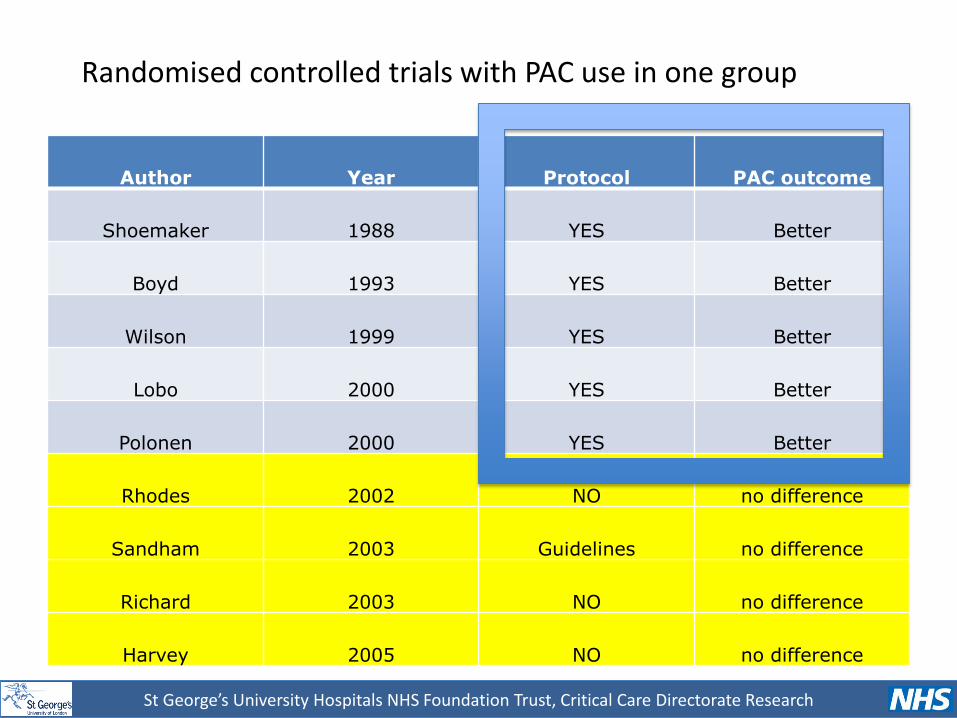
Author Year Protocol PAC outcome
Shoemaker 1988 YES Better
Boyd 1993 YES Better
Wilson 1999 YES Better
Lobo 2000 YES Better
Polonen 2000 YES Better
Rhodes 2002 NO no difference
Sandham 2003 Guidelines no difference
Richard 2003 NO no difference
Harvey 2005 NO no difference
Randomised controlled trials with PAC use in one group
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Author Year Protocol PAC outcome
Shoemaker 1988 YES Better
Boyd 1993 YES Better
Wilson 1999 YES Better
Lobo 2000 YES Better
Polonen 2000 YES Better
Rhodes 2002 NO no difference
Sandham 2003 Guidelines no difference
Richard 2003 NO no difference
Harvey 2005 NO no difference
Randomised controlled trials with PAC use in one group
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Identification of a high risk population Haemodynamic monitoring + Strategy
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
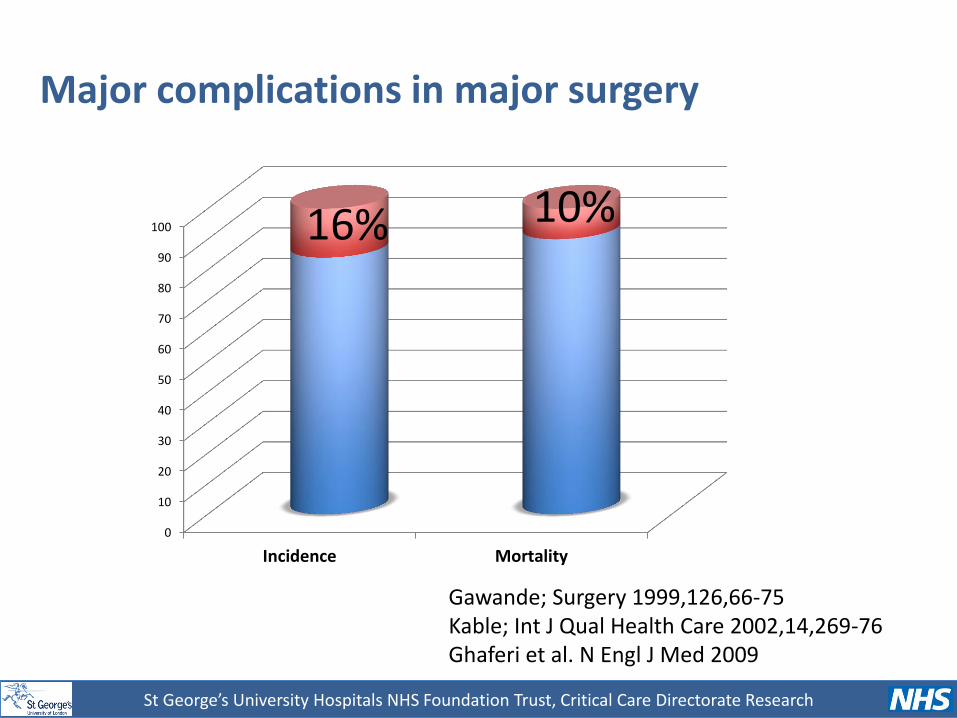
Major complications in major surgery
0
10
20
30
40
50
60
70
80
90
100
Incidence Mortality
16%
10%
Gawande; Surgery 1999,126,66-75 Kable; Int J Qual Health Care 2002,14,269-76 Ghaferi et al. N Engl J Med 2009
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
438 Elective operations:
Major orthopedic Major general Major urological Major vascular Major gynecological
Incidence of complications?

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research Bennett-Guerrero Anesth Analg 1999
0
5
10
15
20
25
30
Mortality Complications
1.6%
27%

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Consequencies of a postoperative complication?

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Ann Surg 2005;242: 326–343
8 Operations
• AAA
• Infrainguinal Vascular reconstruction
• Carotid endarterectomy
• Colectomy
• Open Cholecystectomy
• Laparoscopic Cholecystectomy
• Lobectomy/Pneumonectomy
• Total Hip replacement

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Khuri et al. Ann Surg 2005;242: 326–343

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Khuri et al. Ann Surg 2005;242: 326–343
Patients with no complications Patients with complications

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Khuri et al. Ann Surg 2005;242: 326–343
Patients with no complications Patients with complications
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
“The occurrence of a 30 day postoperative complication is more important than preoperative patient risk and intraoperative factors in determining survival after major surgery”
Khuri et al. Ann Surg 2005;242: 326–343

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Dimick et al J Am Coll Surg 2004

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Mortality Hamilton MA, Cecconi M, Rhodes A Anaesthesia & Analgesia 2011
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
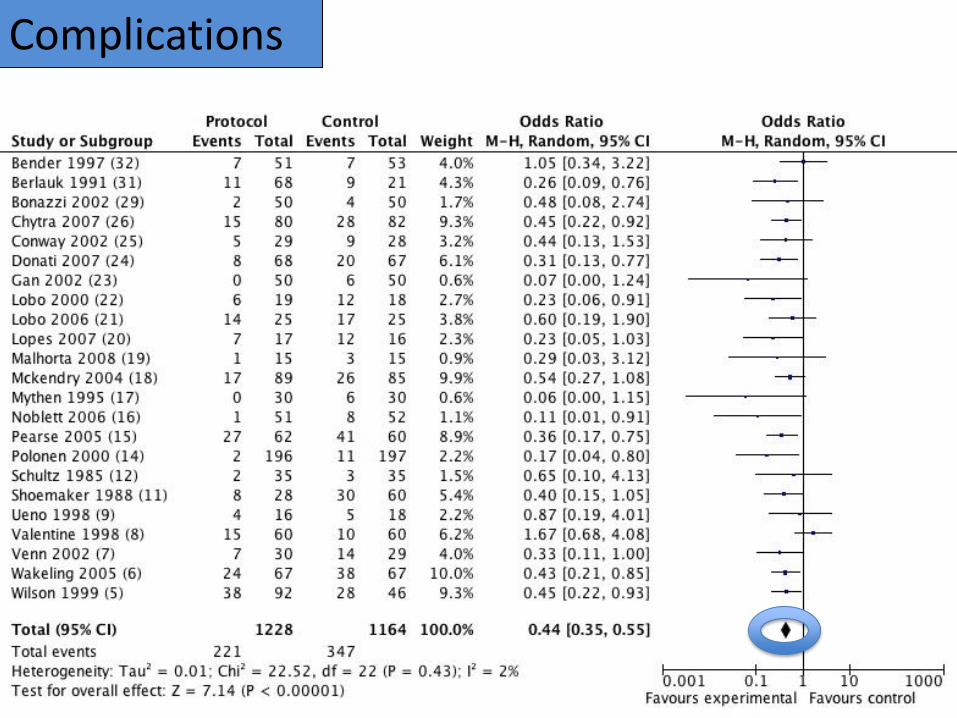
Complications

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Control Group Mortality
Hamilton MA, Cecconi M, Rhodes A Anaesthesia & Analgesia 2011
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Goal directed therapy: what is the
evidence in surgical patients?
The effect on different risk groups
Maurizio Cecconi, Carlos Corredor, Nishkantha Arulkumaran, Gihan Abuella,
Jonathan Ball, Michael R Grounds,
Mark Hamilton and Andrew Rhodes
Crit Care 2013

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Cecconi et al. Crit Care 2013
Mortality effect
based on risk group
Mortality 5 to 20%
Mortality less than 5 %
Mortality higher than 20%

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Mortality 5 to 20%
Mortality less than 5 %
Mortality higher than 20%
Morbidity effect
based on risk group
Cecconi et al. Crit Care 2013

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
15 years survival Protocol vs Control
Rhodes A, Cecconi M, Hamilton M et al ICM 2011
Median increase in survival 1107 days (> 3 years) Hazard ratio 1.8 (95% CI 1.2 to 2.8)

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Cost Effectiveness Analysis
• QALY
• Cost effectiveness Ratio
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
QALY
Scale from 0 to1 0 equates to death
1 to full health
Hip replacement
0.7 first year post recovery
0.8 for 2 years
0.9 for next 2 years
4.1 = 0.7 x 1 + 0.8 x 2 + 0.9 x 2
Ebm C, Sutton L, Rhodes A and Cecconi M In Press JCVA 2014

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
QALY
Scale from 0 to1 0 equates to death
1 to full health
No Hip replacement
3.85 = 0.77 x 5 Surgery vs no Surgery
total QALY 4.1 vs 3.85
Ebm C, Sutton L, Rhodes A and Cecconi M In Press JCVA 2014

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research Ebm C, Sutton L, Rhodes A and Cecconi M In Press JCVA 2014
Costs
Effect
Less Cost More Benefit:
Cost Saving
Less Cost Less Benefit
More Cost Less Benefit
More Cost More Benefit
If the ICER is below an accepted threshold we accept the new therapy
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
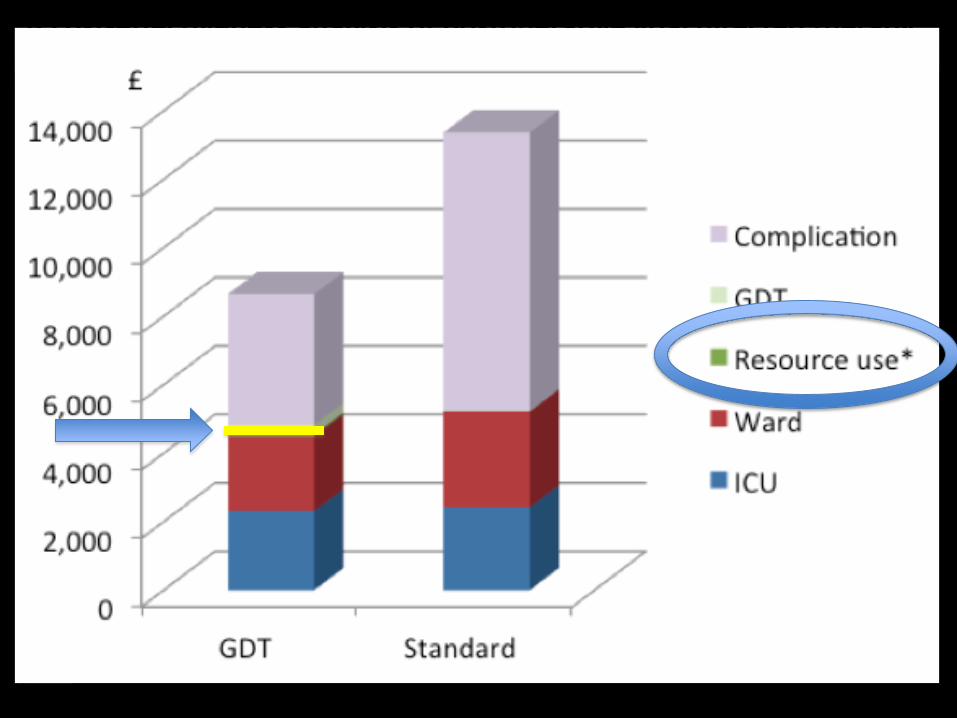
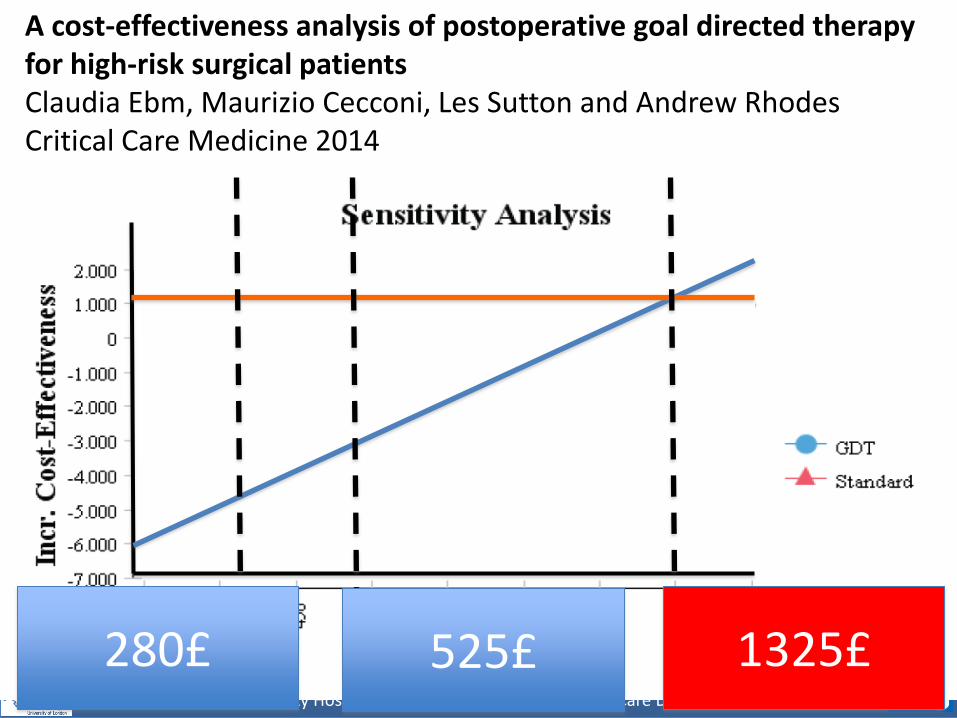
Cost effectiveness A cost-effectiveness analysis of postoperative goal directed therapy for high-risk surgical patients Claudia Ebm, Maurizio Cecconi, Les Sutton and Andrew Rhodes Critical Care Medicine 2014
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Cost effectiveness
1325£ 280£ 525£
A cost-effectiveness analysis of postoperative goal directed therapy for high-risk surgical patients Claudia Ebm, Maurizio Cecconi, Les Sutton and Andrew Rhodes Critical Care Medicine 2014

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Randomized controlled trial of intraoperative goal directed fluid therapy in aerobically fit and unfit patients having major colorectal surgery C Challand et al BJA 2011
• Patients undergoing CPEX testing preop
• Intraop GDT vs CTRL
• Analysis for GDT vs CTRL in overall/fit and unfit
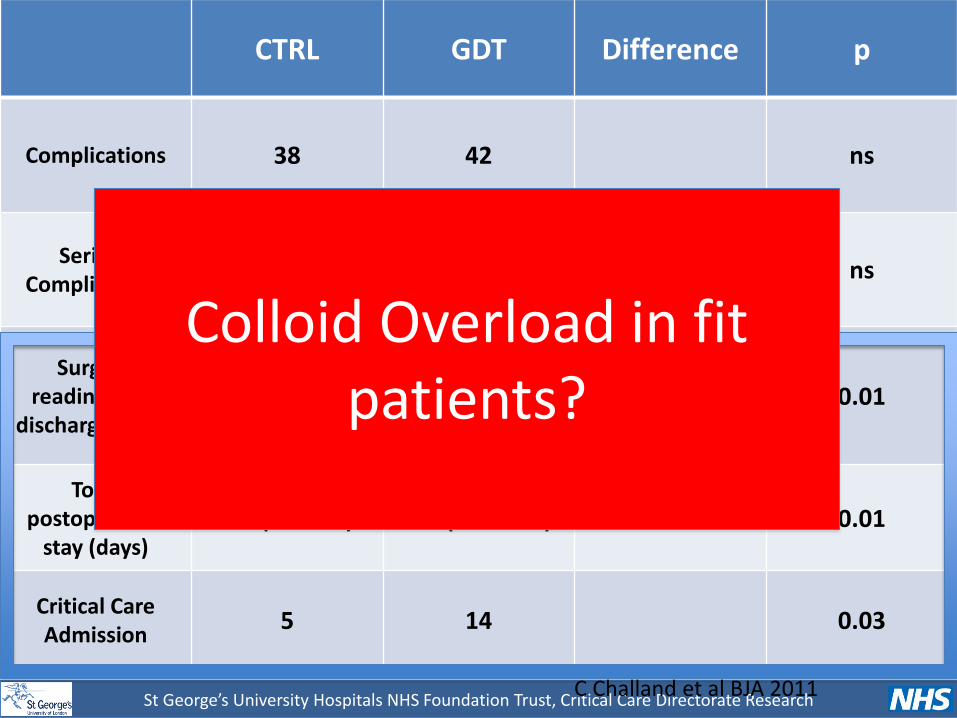
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research C Challand et al BJA 2011
CTRL GDT Difference p
Complications 38 42 ns
Serious Complications
6 6 ns
Surgical readiness for
discharge (days) 4.7 (3.0-7.8) 7.0 (4.7-9.6) +2.3 0.01
Total postoperative
stay (days) 6.0 (4.1-9.8) 8.8 (6.8-11.0) +2.8 0.01
Critical Care Admission
5 14 0.03
Colloid Overload in fit patients?

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Effect of a Perioperative, Cardiac Output–Guided Hemodynamic Therapy Algorithm on Outcomes Following Major Gastrointestinal Surgery A Randomized Clinical Trial and Systematic Review Rupert M.Pearse,MD; DavidA. Harrison,PhD; Neil MacDonald,FRCA; Michael A.Gillies,FRCA; Mark Blunt,FRCA; Gareth Ackland,PhD; Michael P.W.Grocott,MD; Aoife Ahern,BSc; Kathryn Griggs,MSc; Rachael Scott,PhD; Charles Hinds,FRCA; Kathryn Rowan,PhD; for the OPTIMISE Study Group JAMA 2014
Difference Non significant

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research Pearse et al. JAMA 2014
“A prespecified analysis of timing of recruitment suggested that a learning curve may have existed”
removing first 10 patients per site the results are significant
Timing recruitment
GDT Standard care OR p
First 10 patients 33 (42.3%) (n=78)
28 (34.1%) (n=82)
1.51 (0.75-3.01)
Without first 10 patients
100 (35.0%) (n=286)
129 (46.7%) (n=276)
0.59 (0.41-0.84) 0.019

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research Pearse et al. JAMA 2014
“A prespecified analysis of timing of recruitment suggested that a learning curve may have existed”
removing first 10 patients per site the results are significant
Timing recruitment
GDT Standard care OR p
First 10 patients 33 (42.3%) (n=78)
28 (34.1%) (n=82)
1.51 (0.75-3.01)
Without first 10 patients
100 (35.0%) (n=286)
129 (46.7%) (n=276)
0.59 (0.41-0.84) 0.019

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Cardiac complications associated with goal-directed therapy in high-risk surgical patients: a meta-analysis N. Arulkumaran, C. Corredor, M. A. Hamilton, J. Ball, R. M. Grounds, A. Rhodes and M. Cecconi BJA 2014
Is GDT safe?

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
ELPQuiC Emergency Laparotomy Pathway Quality Improvement Care-Bundle
48%
16%
29%
5%
90%
54%
83%
49%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Site 1 Site 2 Site 3 Site 4
Intra-op GDFT (%)
Pre-ELPQuiC
Post-ELPQuiC
Courtesy of Nial Quiney

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
ELPQuiC Emergency Laparotomy Pathway Quality Improvement Care-Bundle
20.4%
14.0% 13.6% 13.3% 14.9%
13.5% 13.2%
8.2% 7.8%
11.2%
0%
5%
10%
15%
20%
25%
Site 1 Site 2 Site 3 Site 4 All
30-day mortality
Pre-ELPQuiC
Post-ELPQuiC
25% reduction
Courtesy of Nial Quiney

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Bundles Treatments: Marginal gain theory
“There's fitness and conditioning, of course, but there are other things that
might seem on the periphery: like sleeping in the right position
having the same pillow when you are away and training in
different places…”

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
November 7th 2013 62 Countries from all continents 1794 Patients
Top Countries 1. USA 2. United Kingdom 3. Malaysia 4. Spain 5. India 6. Italy 7. China 8. Brazil 9. Greece 10. Belgium
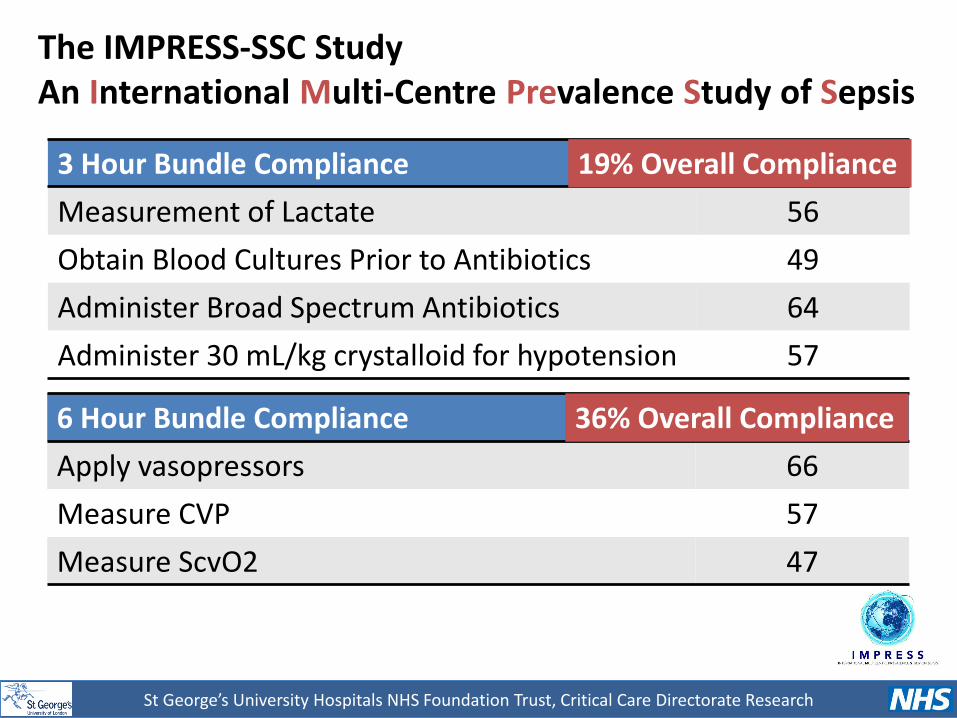
The IMPRESS-SSC Study An International Multi-Centre Prevalence Study of Sepsis
St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
3 Hour Bundle Compliance % Compliance
Measurement of Lactate 56
Obtain Blood Cultures Prior to Antibiotics 49
Administer Broad Spectrum Antibiotics 64
Administer 30 mL/kg crystalloid for hypotension 57
6 Hour Bundle Compliance % Compliance
Apply vasopressors 66
Measure CVP 57
Measure ScvO2 47
19% Overall Compliance
36% Overall Compliance
The IMPRESS-SSC Study An International Multi-Centre Prevalence Study of Sepsis

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Hospital Mortality (%) by Bundle Compliance
P<0.001 P<0.001

St George’s University Hospitals NHS Foundation Trust, Critical Care Directorate Research
Conclusions
• No specific RCTS in Emergency Laparotomies
• Evidence suggests consistent benefit in highest mortality risk groups (>5%)
• Unlikely to cause harm
• Cost-effectiveness?
• No magic bullet, only as part of high quality care