grievance form - ponca city public schools / ponca ... · web viewany administrator who becomes...
TRANSCRIPT
APPENDIX
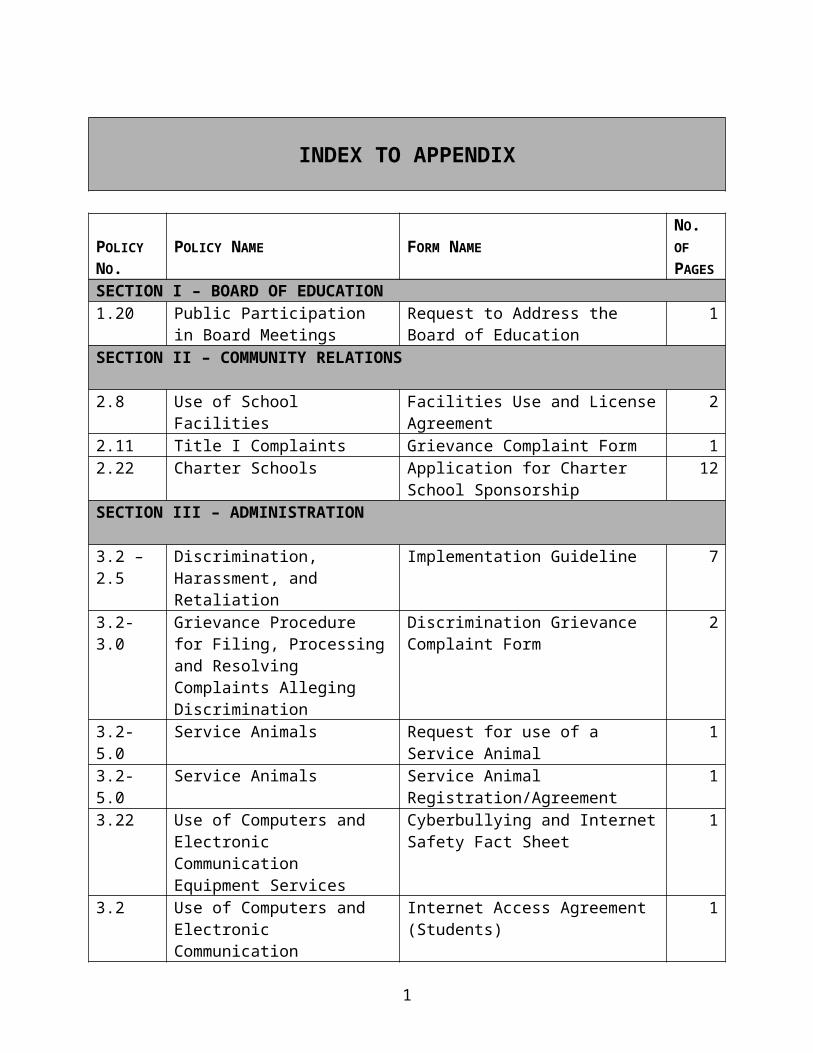
INDEX TO APPENDIX
POLICY NO.
POLICY NAME FORM NAMENO. OF PAGES
SECTION I – BOARD OF EDUCATION1.20 Public Participation in Board
MeetingsRequest to Address the Board of Education
1
SECTION II – COMMUNITY RELATIONS
2.8 Use of School Facilities Facilities Use and License Agreement 22.11 Title I Complaints Grievance Complaint Form 12.22 Charter Schools Application for Charter School
Sponsorship12
SECTION III – ADMINISTRATION
3.2 – 2.5 Discrimination, Harassment, and Retaliation
Implementation Guideline 7
3.2-3.0 Grievance Procedure for Filing, Processing and Resolving Complaints Alleging Discrimination
Discrimination Grievance Complaint Form
2
3.2-5.0 Service Animals Request for use of a Service Animal 13.2-5.0 Service Animals Service Animal
Registration/Agreement1
3.22 Use of Computers and Electronic Communication Equipment Services
Cyberbullying and Internet Safety Fact Sheet
1
3.2 Use of Computers and Electronic Communication Equipment Services
Internet Access Agreement (Students) 1
3.2 Use of Computers and Electronic Communication Equipment Services
Internet Access Agreement (Employees)
1
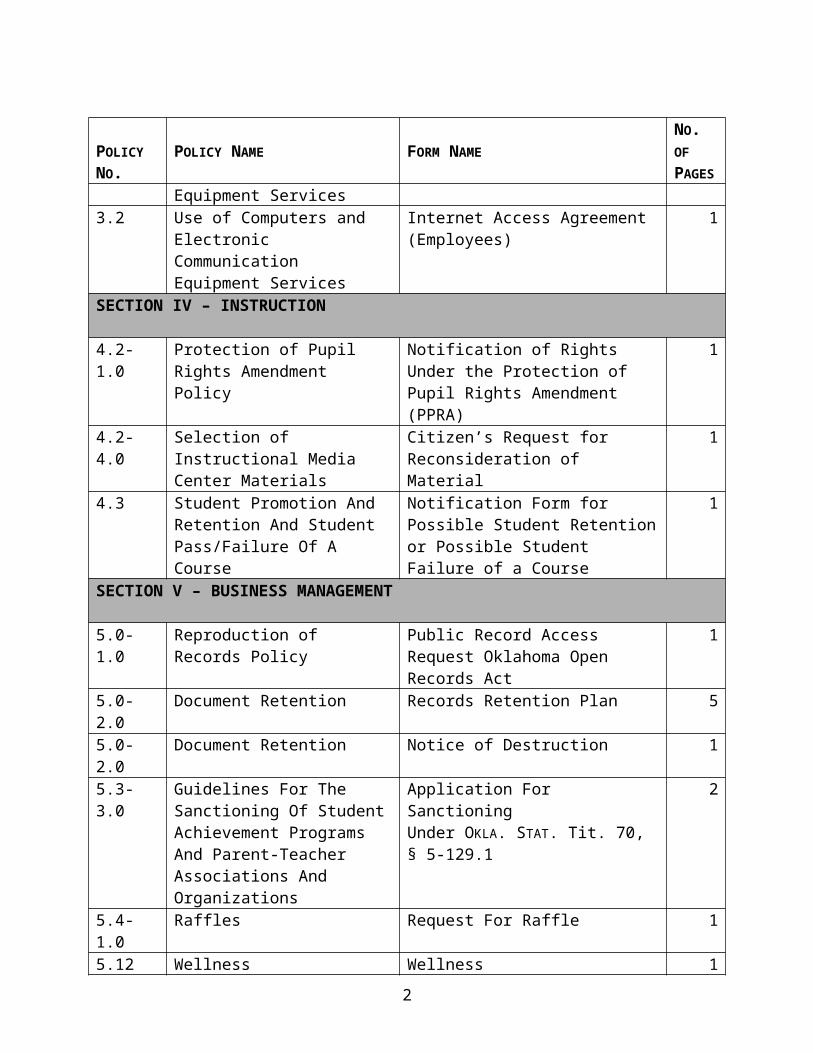
SECTION IV – INSTRUCTION
4.2-1.0 Protection of Pupil Rights Amendment Policy
Notification of Rights Under the Protection of Pupil Rights Amendment (PPRA)
1
4.2-4.0 Selection of Instructional Media Center Materials
Citizen’s Request for Reconsideration of Material
1
4.3 Student Promotion And Retention And Student Pass/Failure Of A
Notification Form for Possible Student Retention or Possible Student Failure
1
1
POLICY NO.
POLICY NAME FORM NAMENO. OF PAGES
Course of a CourseSECTION V – BUSINESS MANAGEMENT
5.0-1.0 Reproduction of Records Policy Public Record Access Request Oklahoma Open Records Act
1
5.0-2.0 Document Retention Records Retention Plan 55.0-2.0 Document Retention Notice of Destruction 15.3-3.0 Guidelines For The Sanctioning
Of Student Achievement Programs And Parent-Teacher Associations And Organizations
Application For SanctioningUnder OKLA. STAT. Tit. 70, § 5-129.1
2
5.4-1.0 Raffles Request For Raffle 15.12 Wellness Wellness 1SECTION VI – PERSONNEL
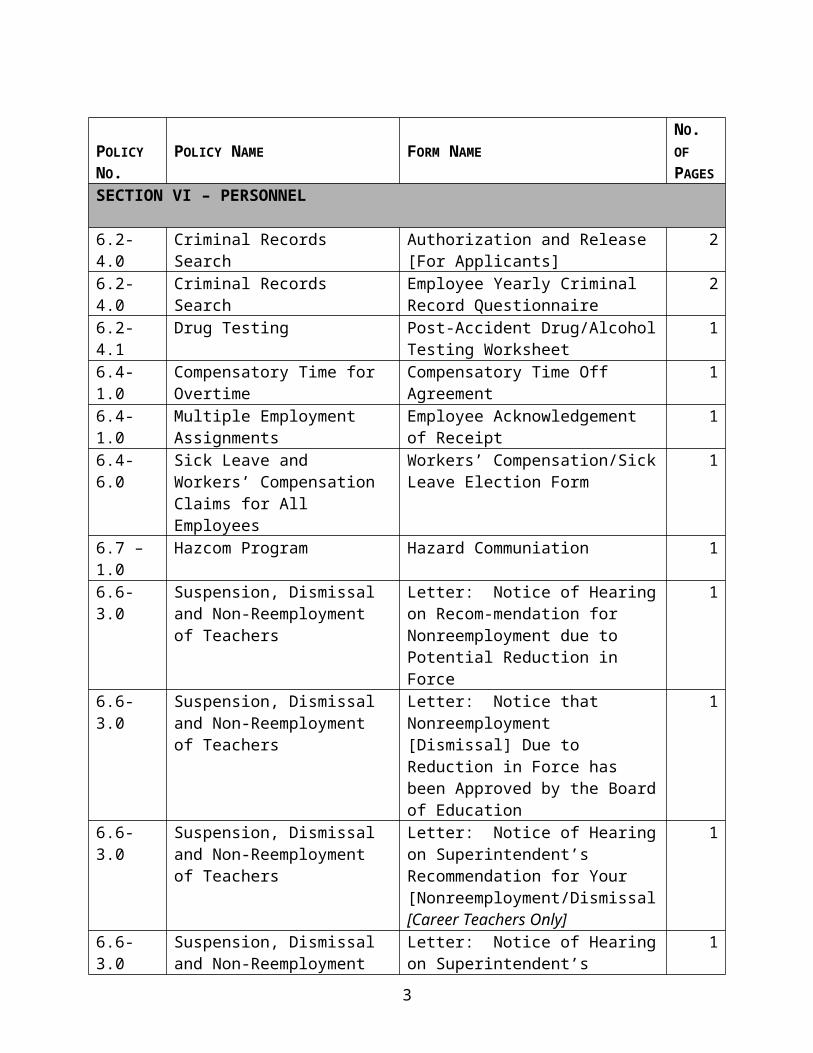
6.2-4.0 Criminal Records Search Authorization and Release[For Applicants]
2
6.2-4.0 Criminal Records Search Employee Yearly Criminal Record Questionnaire
2
6.2-4.1 Drug Testing Post-Accident Drug/Alcohol Testing Worksheet
1
6.4-1.0 Compensatory Time for Overtime Compensatory Time Off Agreement 16.4-1.0 Multiple Employment
AssignmentsEmployee Acknowledgement of Receipt
1
6.4-6.0 Sick Leave and Workers’ Compensation Claims for All Employees
Workers’ Compensation/Sick Leave Election Form
1
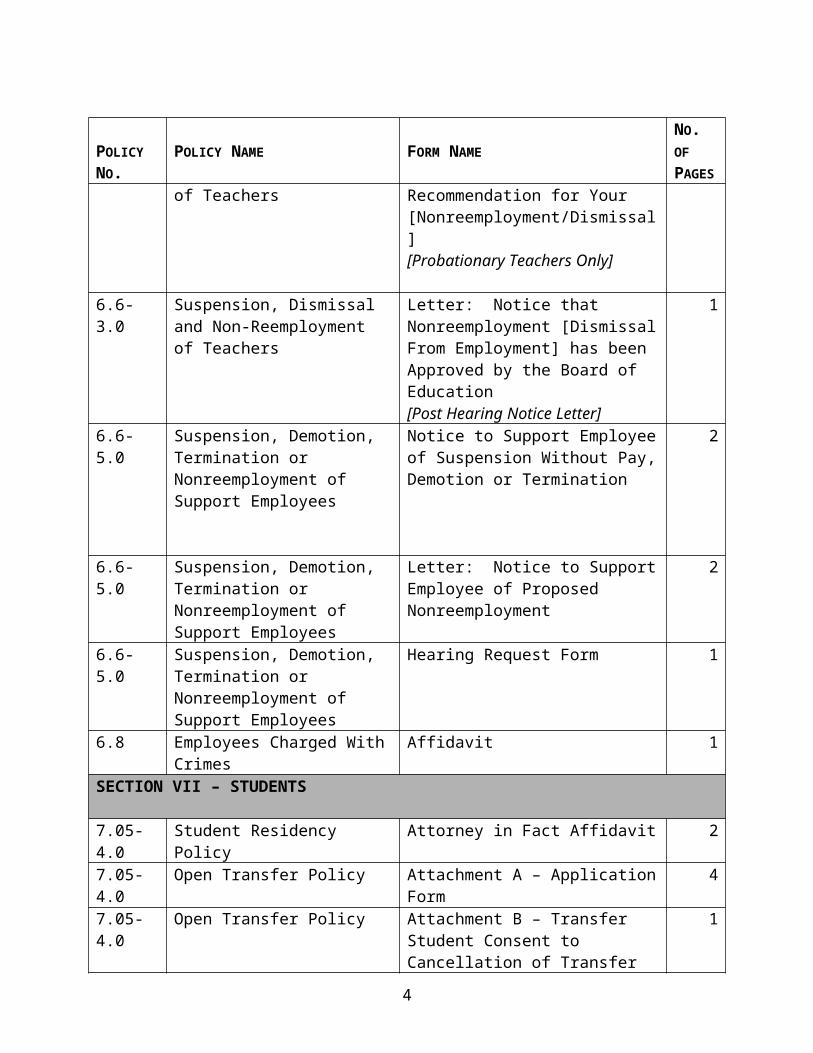
6.7 – 1.0 Hazcom Program Hazard Communiation 16.6-3.0 Suspension, Dismissal and Non-
Reemployment of TeachersLetter: Notice of Hearing on Recom-mendation for Nonreemployment due to Potential Reduction in Force
1
6.6-3.0 Suspension, Dismissal and Non-Reemployment of Teachers
Letter: Notice that Nonreemployment [Dismissal] Due to Reduction in Force has been Approved by the Board of Education
1
6.6-3.0 Suspension, Dismissal and Non-Reemployment of Teachers
Letter: Notice of Hearing on Superintendent’s Recommendation for Your [Nonreemployment/Dismissal[Career Teachers Only]
1
6.6-3.0 Suspension, Dismissal and Non-Reemployment of Teachers
Letter: Notice of Hearing on Superintendent’s Recommendation for Your [Nonreemployment/Dismissal]
1
2
POLICY NO.
POLICY NAME FORM NAMENO. OF PAGES
[Probationary Teachers Only]
6.6-3.0 Suspension, Dismissal and Non-Reemployment of Teachers
Letter: Notice that Nonreemployment [Dismissal From Employment] has been Approved by the Board of Education[Post Hearing Notice Letter]
1
6.6-5.0 Suspension, Demotion, Termination or Nonreemployment of Support Employees
Notice to Support Employee of Suspension Without Pay, Demotion or Termination
2
6.6-5.0 Suspension, Demotion, Termination or Nonreemployment of Support Employees
Letter: Notice to Support Employee of Proposed Nonreemployment
2
6.6-5.0 Suspension, Demotion, Termination or Nonreemployment of Support Employees
Hearing Request Form 1
6.8 Employees Charged With Crimes Affidavit 1SECTION VII – STUDENTS
7.05-4.0 Student Residency Policy Attorney in Fact Affidavit 2
7.05-4.0 Open Transfer Policy Attachment A – Application Form 4
7.05-4.0 Open Transfer Policy Attachment B – Transfer Student Consent to Cancellation of Transfer
1
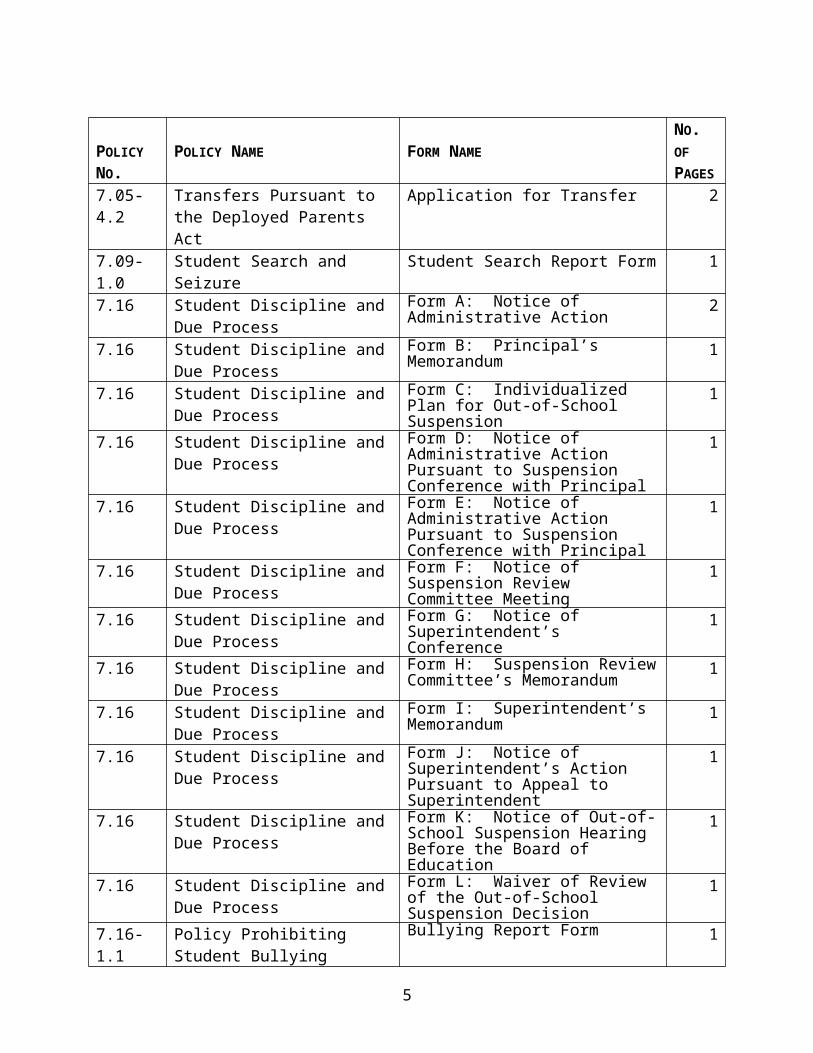
7.05-4.2 Transfers Pursuant to the Deployed Parents Act
Application for Transfer 2
7.09-1.0 Student Search and Seizure Student Search Report Form 17.16 Student Discipline and Due
ProcessForm A: Notice of Administrative Action
2
7.16 Student Discipline and Due Process
Form B: Principal’s Memorandum 1
7.16 Student Discipline and Due Process
Form C: Individualized Plan for Out-of-School Suspension
1
7.16 Student Discipline and Due Process
Form D: Notice of Administrative Action Pursuant to Suspension Conference with Principal
1
7.16 Student Discipline and Due Form E: Notice of Administrative 13
POLICY NO.
POLICY NAME FORM NAMENO. OF PAGES
Process Action Pursuant to Suspension Conference with Principal
7.16 Student Discipline and Due Process
Form F: Notice of Suspension Review Committee Meeting
1
7.16 Student Discipline and Due Process
Form G: Notice of Superintendent’s Conference
1
7.16 Student Discipline and Due Process
Form H: Suspension Review Committee’s Memorandum
1
7.16 Student Discipline and Due Process
Form I: Superintendent’s Memorandum
1
7.16 Student Discipline and Due Process
Form J: Notice of Superintendent’s Action Pursuant to Appeal to Superintendent
1
7.16 Student Discipline and Due Process
Form K: Notice of Out-of-School Suspension Hearing Before the Board of Education
1
7.16 Student Discipline and Due Process
Form L: Waiver of Review of the Out-of-School Suspension Decision
1
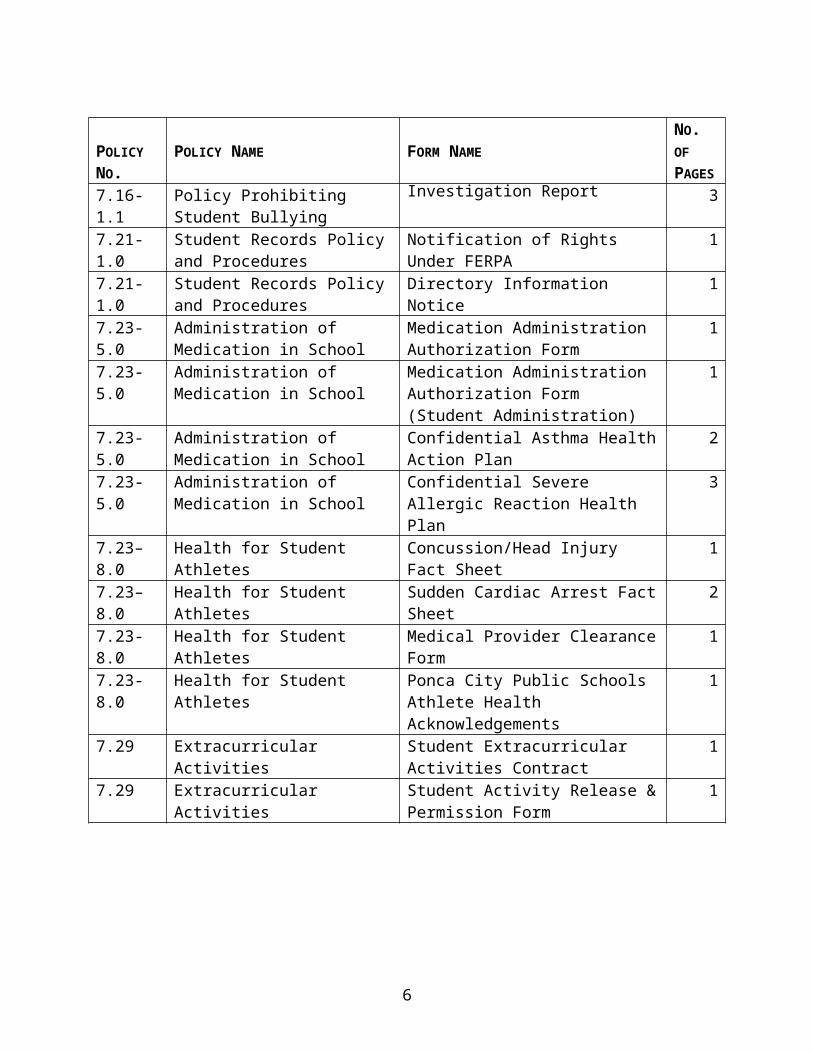
7.16-1.1 Policy Prohibiting Student Bullying
Bullying Report Form 1
7.16-1.1 Policy Prohibiting Student Bullying
Investigation Report 3
7.21-1.0 Student Records Policy and Procedures
Notification of Rights Under FERPA 1
7.21-1.0 Student Records Policy and Procedures
Directory Information Notice 1
7.23-5.0 Administration of Medication in School
Medication Administration Authorization Form
1
7.23-5.0 Administration of Medication in School
Medication Administration Authorization Form (Student Administration)
1
7.23-5.0 Administration of Medication in School
Confidential Asthma Health Action Plan
2
7.23-5.0 Administration of Medication in School
Confidential Severe Allergic Reaction Health Plan
3
7.23–8.0 Health for Student Athletes Concussion/Head Injury Fact Sheet 17.23–8.0 Health for Student Athletes Sudden Cardiac Arrest Fact Sheet 27.23-8.0 Health for Student Athletes Medical Provider Clearance Form 17.23-8.0 Health for Student Athletes Ponca City Public Schools Athlete
Health Acknowledgements1
7.29 Extracurricular Activities Student Extracurricular Activities Contract
1
7.29 Extracurricular Activities Student Activity Release & Permission 1
4
POLICY NO.
POLICY NAME FORM NAMENO. OF PAGES
Form
FORMS FOR
SECTION IBOARD OF
EDUCATION
5
Request to Address the Board of Education(Non-Action Agenda Item)
I request to address the board of education on the following topic:
I understand and agree that if my request is approved, the superintendent will prepare an appropriate agenda item for inclusion on the board’s upcoming meeting agenda. I agree to adhere to the following guidelines:
▪ My comments will be limited to 3 minutes and must be made in a civil and courteous manner.
▪ In accordance with applicable legal requirements, I will not make comments on issues subject to remediation under board policies and district procedures – including positive or negative comments about staff or others connected with the district unless those items have reached the board through the proper administrative procedures.
▪ I will not use this as an opportunity for campaigning for or against a candidate for public office or any ballot measure.
Name:
Organization name:
Address:
Phone:
Email:
Please notify me of approval / rejection of my request by: phone / email
6
FORMS FOR
SECTION IICOMMUNITY RELATIONS
7
FACILITIES USE AND LICENSE AGREEMENT
THIS AGREEMENT is entered into between Independent School District No. 71 of Kay County, Oklahoma ("School District") and ("Licensee").
RECITALS:
Licensee desires to use on a temporary basis certain facilities owned by the School District. The School District desires to allow Licensee to use and occupy designated portions of those facilities at specific times and for specific purposes.
WHEREFORE, in consideration of the following mutual promises, covenants and conditions and intending to be legally bound the parties agree as follows:
1) The School District agrees to allow Licensee to use and occupy the facilities and portions thereof described in paragraph 6 below at the times designated in said paragraph 6 below and for the specific uses described in paragraph 6.
2) Licensee agrees to pay the School District $ as and for rentals and all required cleaning and janitorial expense involved in Licensee's use and occupancy of the facilities.
3) Licensee agrees to release, hold harmless and indemnify the School District, its agents and employees from any and all liability regardless of the source and regardless of the type of claim which may occur arising out of, directly or indirectly, the Licensee's occupancy and use of the below-described facilities. In addition to the foregoing release and indemnity, and not in lieu thereof, Licensee agrees to furnish School District with a certificate or certificates of insurance coverage in such amounts as the superintendent of schools requires as will insure the School District against any and all liability or actions that can arise by virtue of the Oklahoma Governmental Tort Claims Act, and naming the School District, its agents and representatives as additional parties insureds.
4) Licensee warrants and represents that it is authorized to sign this Agreement and by signing this Agreement binds itself, its affiliates, members, successors and assigns.
5) This Agreement is terminable at the will of the School District upon thirty (30) days advance notice.
6) a) Designated building:
b) Designated portion:
c) Designated use:
d) Designated date(s):
e) Designated time:
7) Licensee will take care to use all facilities and equipment of the School District in a careful and prudent manner so as to prevent any loss, defacement or damage to them. Licensee is liable to the School District for the damages, repair or replacement of any items damaged during its use of the School District's facilities.
DATED this day of , 20__.
"SCHOOL DISTRICT"
INDEPENDENT SCHOOL DISTRICT NO. 71 OF KAY COUNTY, OKLAHOMA
By: President of the Board of Education
"LICENSEE"
By: Authorized Representative
GRIEVANCE COMPLAINT FORM
Name and Address of Charging Party (Grievant):
Date:
Phone numbers where Grievant may be reached:
Home: __________________________ Office: _____________________________Cell: __________________________ Other: _____________________________
Statement of grievance (please provide as detailed a statement as is possible and attach supplemental pages so that we may have a complete understanding of your concerns):
Who is your grievance against?
District Individual(s):
Please identify any documents or other materials which support your grievance.If documents or materials are in your possession, please attach copies to this grievance. If documents are not in your possession, please indicate where they are located.
Please identify what action or relief you are seeking as a result of this grievance.
_______________________________Signature of Grievant
If, as a result of a disability, you need assistance in completing this form, please contact the district’s ADA Coordinator, or superintendent, for assistance or accommodation.
Application forCharter School Sponsorship
Type all answers.Answer all questions completely and accurately. Attach additional pages if more space is needed.
Proposed School Name:
Proposed Sponsor:
Organization Background Data
Note: this information is required for each individual applicant. If the applicant is a corporation, LLC, or partnership, this information is required for the entity and for each officer/director/partner/member/manager.
Applicant: Address: Phone: Email:
Tax Information
Applicant’s 501(c)(3) status
Currently established Currently seeking Previously sought but denied by IRS Never sought
Other Affiliations
Will the school be associated in any manner with a sectarian school or religious institution?
Yes No
Litigation
Identify all civil and criminal litigation in which the applicant is or has been a party. State the litigation’s potential to adversely affect the charter school’s operation.
Case No.: Venue: Plaintiff: Defendant: Potential impact:
Case No.: Venue: Plaintiff: Defendant: Potential impact:
Case No.: Venue: Plaintiff: Defendant: Potential impact:
Proposed Timeline
1st school year for classes: Grades to be served: Max school enrollment: Max per grade enrollment: Max per class enrollment:
2nd school year for classes: Grades to be served: Max school enrollment: Max per grade enrollment: Max per class enrollment:
3rd school year for classes: Grades to be served: Max school enrollment: Max per grade enrollment: Max per class enrollment:
4th school year for classes: Grades to be served: Max school enrollment: Max per grade enrollment: Max per class enrollment:
5th school year for classes: Grades to be served: Max school enrollment: Max per grade enrollment: Max per class enrollment:
Governing Body
The applicant agrees that it will not permit individuals to serve on the governing body if the individual has a felony conviction or misdemeanor criminal conviction involving moral turpitude within the past 15 years (10 years for the president).
Yes No
Process to be used to appoint/elect members
Minimum qualifications required to be a member
Number of individuals initially serving on governing body:
Min/max positions on governing body: Min: Max:
Officer positions, lengths of terms, and responsibilities
Initial members of the governing body:
Name: Title: Address: Phone: Email: Relevant experience:
Name: Title: Address:

Phone: Email:
Relevant experience:
Name: Title: Address: Phone: Email: Relevant experience:
Name: Title: Address: Phone: Email: Relevant experience:
Name: Title: Address: Phone: Email: Relevant experience:
Name: Title: Address: Phone: Email: Relevant experience:
Name: Title:
Address: Phone: Email:
Relevant experience:
Meetings of the Governing Body
The governing body will meet at least quarterly, in state, during the first year:
Yes No
The majority of members of the governing body are residents within the geographic boundary of the district:
Yes No
The governing body will follow the requirements of Oklahoma’s Open Meeting Act:
Yes No
The governing body will follow the requirements of Oklahoma’s Open Records Act:
Yes No
During the first year, the governing body anticipates the following meetings:
Date Time Location
Records of the governing body’s meetings and deliberations will be maintained at:________________________________________________________________________________________________________________________________________________________________________________________________________________________
Name of the individual and/or position responsible for complying with the Open Meeting Act and Open Records Act:________________________________________________________________________
Detailed description of the governing body’s authority:________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Facilities
The Charter School has secured, or will secure by the time operations are to begin, the following facilities in which to house school operations:________________________________________________________________________________________________________________________________________________________________________________________________________________________
The owner of the above facilities and the owner’s address:________________________________________________________________________________________________________________________________________________________________________________________________________________________
Financial Information
Identify the name of the individual with primary responsibility for managing the charter school’s finances, including but not limited to education, credentials, relevant experience, and the name/address and phone number of every school district in which the individual has worked.________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Name / address of the charter school’s depository bank:________________________________________________________________________________________________________________________________________________________________________________________________________________________
Mission / Goals
What is the charter school’s mission?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What are the specific educational goals of the charter school?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
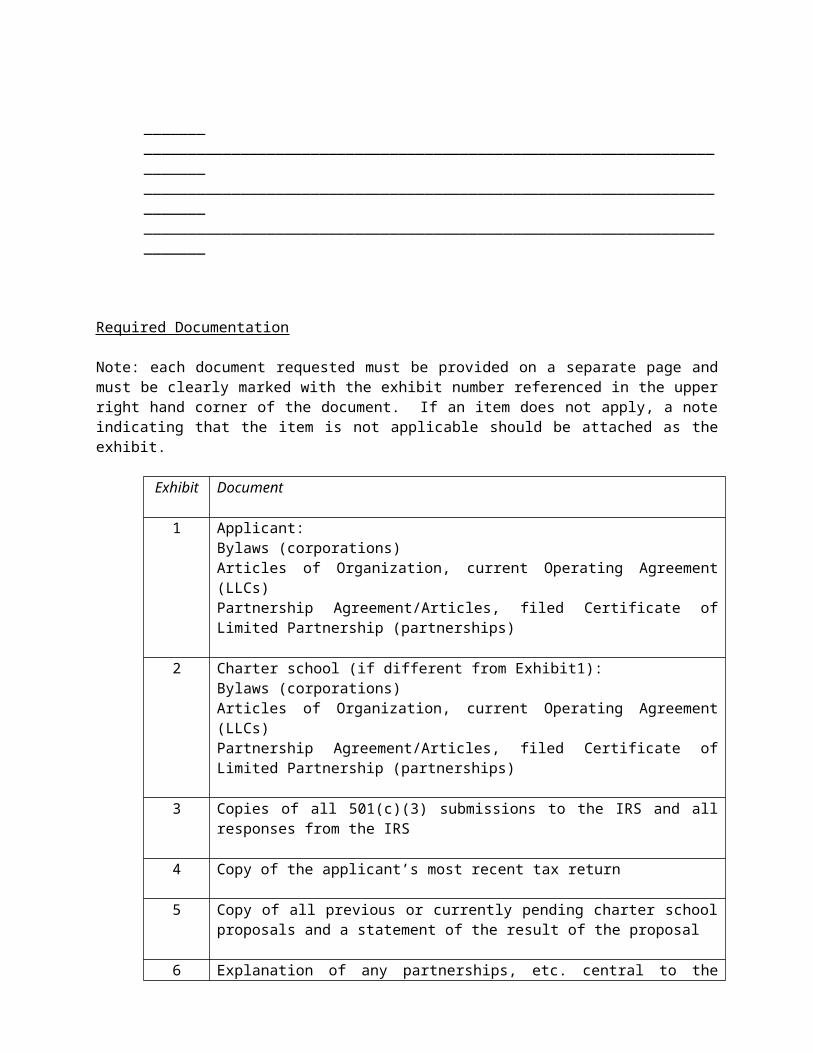
Required Documentation
Note: each document requested must be provided on a separate page and must be clearly marked with the exhibit number referenced in the upper right hand corner of the document. If an item does not apply, a note indicating that the item is not applicable should be attached as the exhibit.
Exhibit Document
1 Applicant:Bylaws (corporations)
Articles of Organization, current Operating Agreement (LLCs)Partnership Agreement/Articles, filed Certificate of Limited Partnership (partnerships)
2 Charter school (if different from Exhibit1):Bylaws (corporations)Articles of Organization, current Operating Agreement (LLCs)Partnership Agreement/Articles, filed Certificate of Limited Partnership (partnerships)
3 Copies of all 501(c)(3) submissions to the IRS and all responses from the IRS
4 Copy of the applicant’s most recent tax return
5 Copy of all previous or currently pending charter school proposals and a statement of the result of the proposal
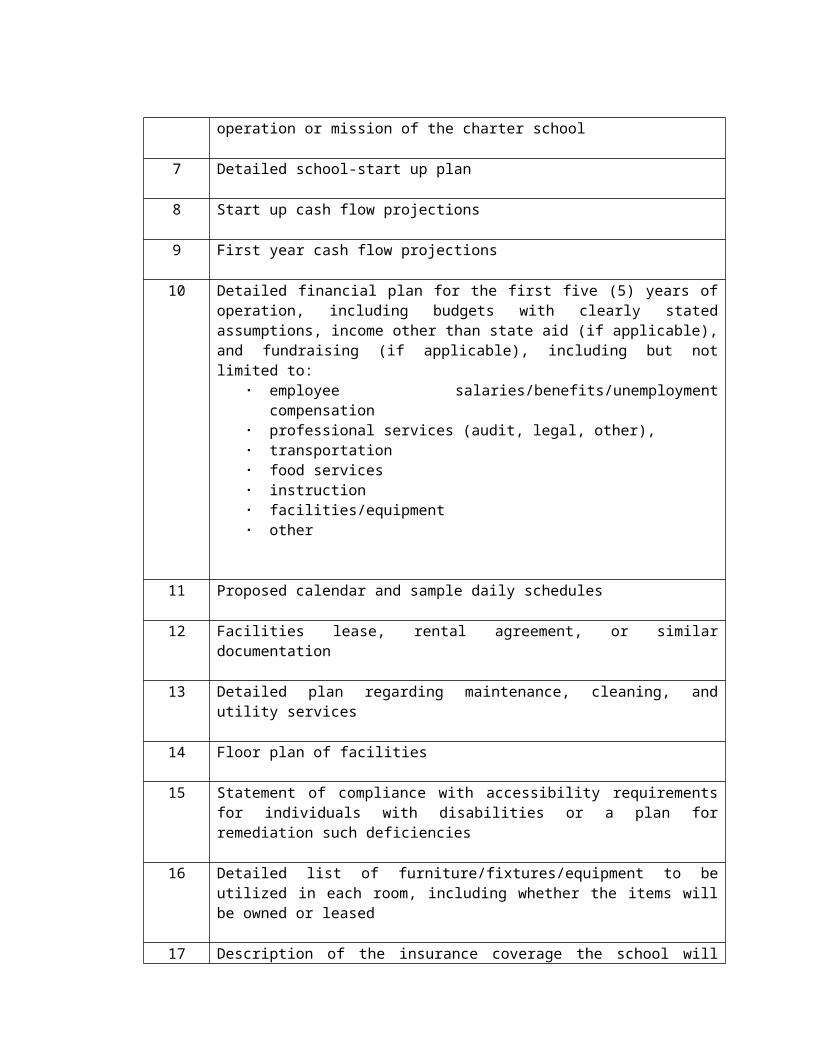
6 Explanation of any partnerships, etc. central to the operation or mission of the charter school
7 Detailed school-start up plan
8 Start up cash flow projections
9 First year cash flow projections
10 Detailed financial plan for the first five (5) years of operation, including budgets with clearly stated assumptions, income other than state aid (if applicable), and fundraising (if applicable), including but not limited to:
employee salaries/benefits/unemployment compensation professional services (audit, legal, other), transportation food services instruction facilities/equipment other
11 Proposed calendar and sample daily schedules
12 Facilities lease, rental agreement, or similar documentation
13 Detailed plan regarding maintenance, cleaning, and utility services
14 Floor plan of facilities
15 Statement of compliance with accessibility requirements for individuals with disabilities or a plan for remediation such deficiencies
16 Detailed list of furniture/fixtures/equipment to be utilized in each room, including whether the items will be owned or leased
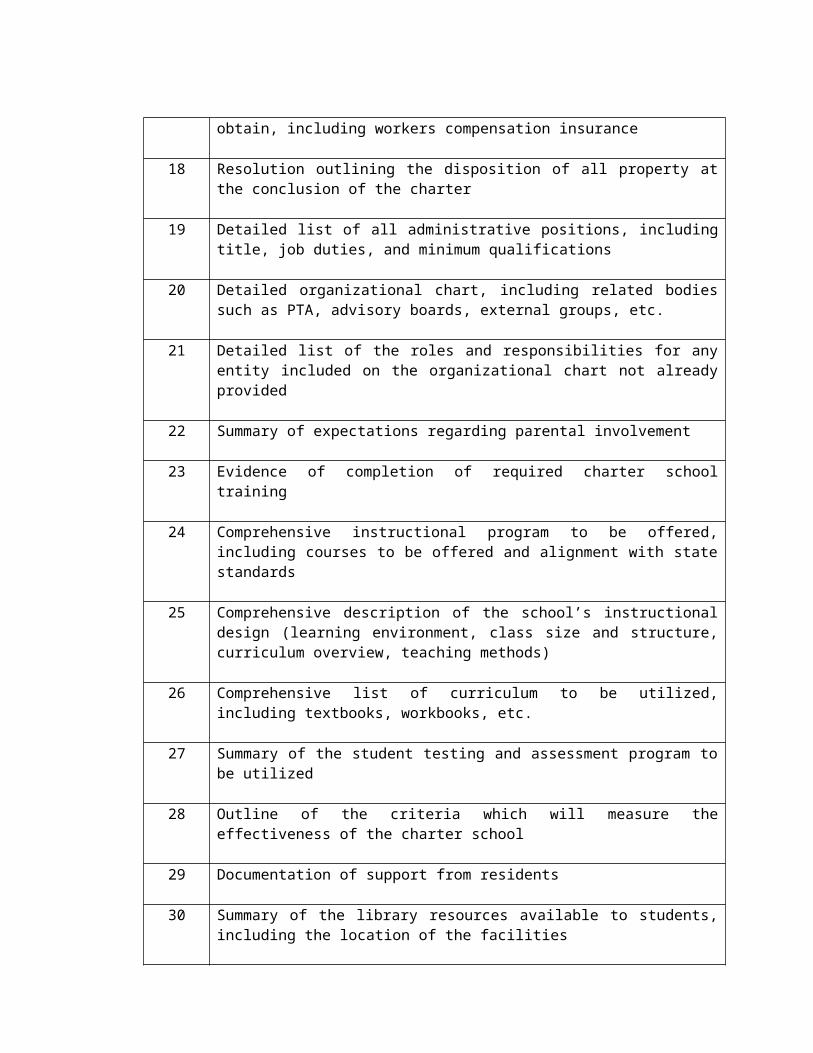
17 Description of the insurance coverage the school will obtain, including workers compensation insurance
18 Resolution outlining the disposition of all property at the conclusion of the charter
19 Detailed list of all administrative positions, including title, job duties, and minimum qualifications
20 Detailed organizational chart, including related bodies such as PTA, advisory boards, external groups, etc.
21 Detailed list of the roles and responsibilities for any entity included on the organizational chart not already provided
22 Summary of expectations regarding parental involvement
23 Evidence of completion of required charter school training
24 Comprehensive instructional program to be offered, including courses to be offered and alignment with state standards
25 Comprehensive description of the school’s instructional design (learning environment, class size and structure, curriculum overview, teaching methods)
26 Comprehensive list of curriculum to be utilized, including textbooks, workbooks, etc.
27 Summary of the student testing and assessment program to be utilized
28 Outline of the criteria which will measure the effectiveness of the charter school
29 Documentation of support from residents
30 Summary of the library resources available to students, including the location of the facilities
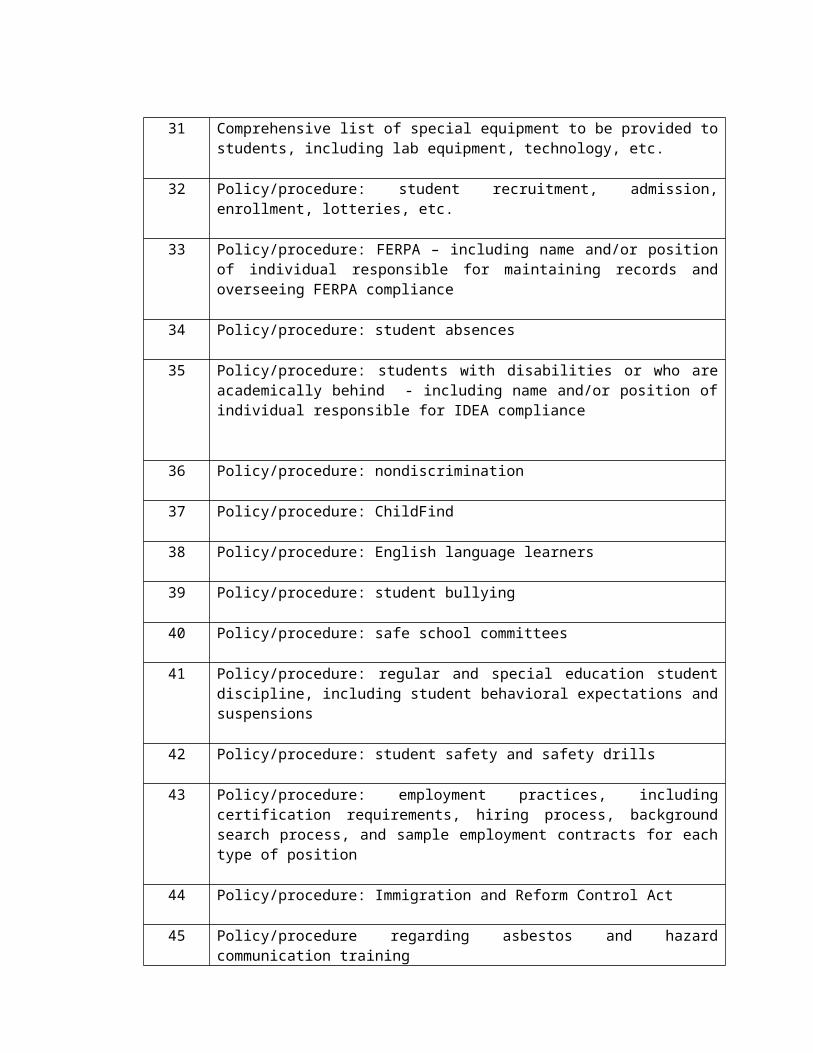
31 Comprehensive list of special equipment to be provided to students, including lab equipment, technology, etc.
32 Policy/procedure: student recruitment, admission, enrollment, lotteries, etc.
33 Policy/procedure: FERPA – including name and/or position of individual responsible for maintaining records and overseeing FERPA compliance
34 Policy/procedure: student absences
35 Policy/procedure: students with disabilities or who are academically behind - including name and/or position of individual responsible for IDEA compliance
36 Policy/procedure: nondiscrimination
37 Policy/procedure: ChildFind
38 Policy/procedure: English language learners
39 Policy/procedure: student bullying
40 Policy/procedure: safe school committees
41 Policy/procedure: regular and special education student discipline, including student behavioral expectations and suspensions
42 Policy/procedure: student safety and safety drills
43 Policy/procedure: employment practices, including certification requirements, hiring process, background search process, and sample employment contracts for each type of position
44 Policy/procedure: Immigration and Reform Control Act
45 Policy/procedure regarding asbestos and hazard communication training
46 Policy/procedure: transportation (including transportation for students with disabilities)
47 Policy/procedure: food services
48 Policy /procedure: business office operations, including but not limited to compliance with OCAS, adopting an annual budget and compliance with the Oklahoma Public School Audit Law
49 Policy/procedure: how the charter school will comply with all federal regulations and state and local rules/statutes related to health, safety, civil rights, insurance, students, and faculty – if not provided above
Other Services To Be Provided
Yes NoAP classesIB programGifted and talented programGuidance and counseling services(provide a detailed description)
Cocurricular activities(list, by grade, including funding sources and delivery method)
Extracurricular activities(list, by grade, including funding sources and delivery method)
Services to students at risk of dropping out(provide a detailed description)
Other:Other:Other:
Other Information
Please provide any additional information not already included which would be helpful as the district evaluates this application:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Certification
The information contained in this application is true and correct to the best of my knowledge and belief. I am individually authorized to submit this application on behalf of the applicant.
Individual Printed Name
_______________________________________________________________________ Individual Signature
________________________________________________________________________ Date Contact Number
FORMS FOR
SECTION IIIADMINISTRATION
Implementation Guideline forCombatting Sex/Gender Based Discrimination
The district is committed to ensuring equity in all its programs. This document is designed to help the administration avoid claims of sex/gender based discrimination and to ensure all students and employees are treated fairly.
Education - Students
The district’s anti-bullying and anti-discrimination education efforts will include education to students regarding the following topics:
Identifying bullying and cyberbullying
Identifying all forms of discrimination, including sex discrimination based on gender stereotypes, gender nonconformity, and transgender status
Concrete and age appropriate examples of harassment, intimidation, discrimination and bullying – and appropriate responses
Outline of the district’s conduct expectations
Ways in which prohibited conduct adversely affects the education environment
Identification of bullying and discrimination coordinators
Explanation of how to file a claim of harassment, intimidation, discrimination or bullying
Education – Staff
All school personnel have a responsibility to understand the district’s commitment to eliminate all forms of discrimination in all its programs. The district will provide basic training to school personnel to ensure success, including information about who to contact in regard to potential discrimination. The district will also provide additional training to personnel who are designated program coordinators.
Handbooks
All school site handbooks must contain the following language:
There will be no discrimination in the district because of race, color, sex, pregnancy, gender, gender expression or identity, national origin, religion, disability, veteran status, sexual orientation, age, or genetic information in its programs, services, activities and employment. The following people have been designated to handle inquiries regarding the district’s non-discrimination policies:
Section 504/Title II of the Americans with Disabilities Act Coordinator (for questions or complaints based on disability)
Director of Special Services613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Title VI of the Civil Rights Act Coordinator (for questions or complaints based on race, color and national origin)
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Title IX Coordinator (for questions or complaints based on sex, pregnancy, gender, gender expression or identity)
Director of Operations613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Age Act Coordinator (for questions or complaints based on age)
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Any individual who has experienced some other form of discrimination, including discrimination not listed above, may contact:
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Outside Assistance may be obtained from:
U.S. Department of EducationOffice for Civil RightsOne Petticoat Lane1010 Walnut Street, Suite 320Kansas City, MO 64106(816) 268-0550(816) 268-0599 (Fax)(877) 521-2172 (TTY)E-mail: [email protected]
All district employees and students will be provided with age appropriate education regarding types of discrimination, harassment and bullying. Students and employees will also be advised of the district’s expectations regarding appropriate conduct. Any student who is experiencing difficulty fully accessing the district’s education programs should contact the appropriate coordinator so a success plan can be developed for the student.
Administrator Responses
Any administrator who becomes aware that a student is pregnant or transitioning to a different gender must meet privately with the student, or with the student and another administrator of the student’s gender, to discuss the situation. The meeting must include discussion of whether the student’s parent/guardian can be contacted (no student may be “outed” to his/her parent or guardian) and creation of a transition plan. The plan is not to be punitive/exclusionary in nature and must be designed to ensure the student’s educational success.
Each student must be provided with information regarding the district’s nondiscrimination policies and procedures and the name/contact information for the district’s nondiscrimination coordinators. The student must also be provided with the name/number of a staff liaison in the event the student encounters any difficulties with his/her education.
Placement and Other Education ConsiderationsFor Special Circumstances
In an attempt to meet individual student needs, the district will consider all placement and related education options at times when traditional instruction and other access may not be in a student’s best interests. This worksheet will guide the administrator, parent/guardian (if authorized by the student), and student in making the best decision possible given the totality of the circumstances. This placement will be reviewed as often as needed but at least once per semester.
Placement Options1
Retain Current PlacementThe student retains his/her current schedule at his/her current school.
Current School / New ScheduleThe student continues at his/her current school but with a different class schedule.
In-District TransferThe student is transferred to another school within the district.
Out-of-District TransferThe district consents to the student transferring to another school district. This option requires the consent of the receiving school district, which is outside this district’s control.
Blended LearningThe student receives educational services by taking supplemental online courses or participating in an online program. This option is available for secondary students only.
Dropout PreventionThe student receives all education services via online instruction. This option is available for secondary students only.
Alternative SchoolThis option requires an application process prior to placement.
Health Considerations / IEPThese options include partial school days, 504 Plans, and homebound instruction. Additional evaluations may be required prior to placement with these options.
Information Dissemination
The following personnel have a need to know this information:
Staff Member Information to be Disclosed, if any
1 No student will be excluded from regular classes or segregated in any way based on special or unique circumstances alone. All educational placements, including extracurricular activities, will be considered based on the entirety of the student’s unique circumstances. Regardless of the placement option agreed upon between the school and the family, additional supportive services may be added as deemed appropriate.
Temporary Leave
The student will be on leave from school the following dates: To
The student will make up work related to this absence:
Supportive Services
The following additional services and special considerations are needed:
Schedule a meeting with the principal prior to returning to class to discuss any potential
obstacles and how to successfully navigate those challenges
Designate an individual for the student to report any difficulties to, including any concerns about bullying, retaliation, or other inappropriate conduct
School counseling sessions
Consulting with the student’s private counselor to ensure a unified approach
Coordinating the student’s class schedule to maximize successful goal completion
Other:
Decisions / Action Plan
After considering each of the options and categories outlined above, the administration, parent/guardian (if authorized) and student have selected those options and choices which are marked. The reasons for these decisions are:
Acknowledgment
We have jointly agreed to the options noted above as the best choice for the student given the totality of the circumstances. We agree to review this decision as needed, but at least once per semester.
Student Signature Date
Parent/Guardian Signature (if authorized) Date
Administrator Signature Date
A copy of this plan will be provided to the student, authorized parent/guardian, and authorized school personnel.
Additional Options & Discussion PointsGender Transitioning Students Only
Name / Gender Identification
Name the student will use (unofficial records):
Gender pronoun the student will use:
Will official school records be changed (court order required):
Restroom & Locker Room Access
Student will use group restrooms associated with the preferred gender
Student will use a private restroom located
Student will use restrooms associated with the preferred gender but will also have access to a private restroom located
Gender Based Activities
Student will participate in the following activities consistent with the preferred gender identity or expression:
Health classes PE classes Club/intramural athletics
Extracurricular Activities
Student is participating in the following extracurricular activities:
Notes from OSSAA on student’s eligibility and participation:
Other Needs
Describe:
DISCRIMINATION GRIEVANCE COMPLAINT FORM
Name and Address of Charging Party (Grievant):
_____________________________________________________________________________________
_____________________________________________________________________________________
Date: ___________________________
Phone numbers where Grievant may be reached:
Home: __________________________ Office: _____________________________
Cell: ____________________________ Other: _____________________________
Statement of grievance (please provide as detailed a statement as is possible and attach additional pages so that we may have a complete understanding of your concerns):
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Please identify any documents or other materials that support your grievance. If documents or materials are in your possession, please attach copies to this grievance. If documents or materials are not in your possession, please indicate where they are located.
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Please identify what action or relief you are seeking as a result of this grievance.
_____________________________________________________________________________________
_____________________________________________________________________________________
_______________________________________Signature of Grievant
You may contact the District’s Compliance Coordinators as follows:
Section 504/Title II of the Americans with Disabilities Act Coordinator (for questions or complaints based on disability)
Director of Special Services613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Title VI of the Civil Rights Act Coordinator (for questions or complaints based on race, color and national origin)
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Title IX Coordinator (for questions or complaints based on sex, pregnancy, gender, gender expression or identity)
Director of Operations613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Age Act Coordinator (for questions or complaints based on age)
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Any individual, who has experienced some other form of discrimination, including discrimination not listed above, may contact:
Executive Director of Human Resources/TLE613 E. Grand Ave., Ponca City, OK 74601(580) 767-8000
Outside Assistance may be obtained from:
U.S. Department of EducationOffice for Civil RightsOne Petticoat Lane1010 Walnut Street, Suite 320Kansas City, MO 64106(816) 268-0550(816) 268-0599 (Fax)(877) 521-2172 (TTY)E-mail: [email protected]
If, as a result of a disability, you need assistance in completing this form, please contact the District’s Section 504/Title II Coordinator for assistance or accommodation.
PONCA CITY SCHOOL DISTRICTREQUEST FOR USE OF A SERVICE ANIMAL
Date: ________________________
Staff Member or Student's Name: ________________________________________________
Parent's Name (for Students only): _________________________ Building: _______________
Identify whether the service animal is required because of a staff member or student’s disability, and if so, identify and describe the manner in which the service animal will meet the individual’s particular need(s):
Type of Service Animal: Dog Miniature Horse Name of Animal:______________________
Documentation attached that the Service Animal is: Properly and currently vaccinated Under the control of a properly trained handler. Name of handler:______________________ Covered by adequate liability insurance
Submit request to the Director of Special Services613 E. Grand Ave.
Ponca City, OK 74601
Annual Application Required
PONCA CITY SCHOOL DISTRICTSERVICE ANIMAL REGISTRATION/AGREEMENT
___________________________________ ___________________________________Owner Student (if applicable)
Type of Service Animal: Dog Miniature Horse Name of Animal: _____________________
Request Approval Form is attached
Documentation attached that the Service Animal is: Properly and currently vaccinated Under the control of a properly trained handler Name of handler: _____________________ Covered by adequate liability insurance
I have read and understand the District’s Service Animals Policy. I will abide by the terms of the Policy.
I understand that if my Service Animal is: out of control and/or the animal’s handler does not effectively control the animal’s behavior; not housebroken or the animal’s presence or behavior fundamentally interferes in the functions of the District; or poses a direct threat to the health or safety of others that cannot be eliminated by reasonable modifications, the District has the discretion to exclude or remove my Service Animal from its property.
I agree to be responsible for any and all damage to District property, personal property, and any injuries to individuals caused by my Service Animal. I agree to indemnify, defend and hold harmless Ponca City Public Schools from and against any and all claims, actions, suits, judgments and demands brought by any party arising on account of, or in connection with, any activity of or damage caused by my Service Animal.
OWNER
___________________________Signature
Date:_______________________
Note: This Registration/Agreement is valid until the end of the current school year. It must be renewed prior to the start of each subsequent school year or whenever a different Service Animal will be used.

Cyber Bullying and Internet Safety Fact Sheet
People can be bullied in lots of ways, including through cyber bullying. Cyber bullying is when someone sends or posts things (words, pictures, recordings) that are mean, embarrassing or make people feel scared, embarrassed or uncomfortable. Even if they don't do this at school sometimes cyber bullying makes things at school hard. No student is allowed to disrupt school through cyber bullying.
Cyber bullies work in lots of ways, but here's some of their most common:
▪ Send or post mean messages▪ Make up websites or accounts with stories, cartoons, pictures or "jokes" that are
mean to others▪ Take embarrassing pictures or recordings (without asking first)▪ Send or post stuff to embarrass others▪ Hack into other people's accounts or read their stuff▪ Hack into other people's accounts and send or post their private stuff▪ Pretend to be somebody else to get someone to give them private info▪ Send threats
If you're a cyber bully knock it off! Ask your principal/counselor how you can make things right.
If someone is cyber bullying you, there's something you can do about it:
▪ Don't respond to and don't ignore a cyber bully. Instead, tell an adult you trust. If cyber bullying follows you to school, tell your teacher, counselor or principal.
▪ Even if what the bully does is embarrassing, don't delete it. Instead, get a copy so you can prove what happened.
▪ Have an adult help you contact a company representative (cell phone company, Yahoo, Facebook, Twitter, etc.) about blocking or removing the bad stuff.
You can't always stop people from being mean, but there are ways to help yourself:
▪ Don't give out your personal info in electronic or digital communications ▪ Don't tell anyone but your parents what your login name, password or PIN
number is▪ Don't post or send embarrassing pics or recordings (even on your own sites) -
bullies love to copy your stuff
Suggestions for Parents:
▪ Help your child understand how permanent electronic or digital communications are
▪ Talk to your child about understanding, preventing and responding to cyber bullying
▪ Contact your student's school for help if you suspect your child is being cyber bullied – or if you suspect your child is engaging in cyber bullying
INTERNET ACCESS AGREEMENT(STUDENTS)
STUDENT SECTION:
Student Full Name:
School Site: ___________________________________ Grade:
Home Address:
Home Phone No.:
I have received a copy of the policy titled Acceptable Use of Internet and Electronic and Digital Communications Devices, including the attachment regarding cyber bullying, and a copy of the Student Handbook. I have read and agree to abide by their provisions. I understand that any violation of the policy or handbook provisions may result in disciplinary action including, but not limited to, suspension and/or revocation of network privileges and suspension from school.
Student Signature Date
SPONSORING PARENT OR GUARDIAN SECTION (Required):
I have received a copy of the policy titled Acceptable Use of Internet and Electronic and Digital Communications Devices, including the attachment regarding cyber bullying, and a copy of the Student Handbook Parent Laptop Handbook. I have read and discussed these provisions with my child. My child and I understand that any violation of the policy or handbook provisions may result in disciplinary action including, but not limited to, suspension and/or revocation of network privileges and suspension from school.
I understand that the school district has taken reasonable precautions to ensure that access to controversial material is limited to the extent possible, but I realize that it is not possible to guarantee that my child will never encounter objectionable material. I hereby release the school district from liability in the event that my child acquires inappropriate material through use of the district's technology resources, including the Internet.
I request that the district issue an account for my child and certify that the information contained on this form is correct.
Parent Signature Date
Student Access Agreement must be renewed each academic year.
INTERNET ACCESS AGREEMENT(EMPLOYEES)
Employee Name:
Position:
School or Site:
Home Address:
Home Phone No.:
I have received a copy of the policy titled Acceptable Use of Internet and Electronic and Digital Communications Devices. I have read and agree to abide by its provisions. I understand that any violation of the use provisions may result in disciplinary action including suspension and/or revocation of network privileges as well as any discipline allowed by law including termination of employment.
Employee Signature Date
FORMS FOR
SECTION IVINSTRUCTION
PONCA CITY SCHOOL DISTRICTNOTIFICATION OF RIGHTS UNDER THE
PROTECTION OF PUPIL RIGHTS AMENDMENT (PPRA)
PPRA affords parents certain rights regarding our conduct of surveys, collection and use of information for marketing purposes, and certain physical exams. These include the right to:
Consent before students are required to submit to a survey that concerns one or more of the following protected areas (“protected information survey”) if the survey is funded in whole or in part by a program of the U.S. Department of Education (ED) -
1. Political affiliations or beliefs of the student or student’s parent;2. Mental and psychological problems of the student or student’s family;3. Sex behavior or attitudes;4. Illegal, anti-social, self-incriminating or demeaning behavior;5. Critical appraisals of others with whom respondents have close family relationships;6. Legally recognized privileged relationships, such as with lawyers, doctors, or ministers;7. Religious practices, affiliations, or beliefs of the student or parents; or8. Income, other than as required by law to determine eligibility.
Receive notice and an opportunity to opt a student out of –
1. Any other protected information survey, regardless of funding;2. Any non-emergency, invasive physical exam or screening required as a condition of attendance;
administered by the school or its agent, and not necessary to protect the immediate health and safety of a student, except for hearing, vision, or scoliosis screenings, or any physical exam or screening permitted or required under State law; and
3. Activities involving collection, disclosure, or use of personal information obtained from students for marketing or to sell or otherwise distribute the information to others.
Inspect, upon request and before administration or use –
1. Protected information surveys of students;2. Instruments used to collect personal information from students for any of the above marketing, sales, or
other distribution purposes; and 3. Instructional material used as part of the educational curriculum.
These rights transfer from the parents to a student who is 18 years old or an emancipated minor under State law.
The School District will develop and adopt policies, in consultation with parents, regarding these rights, as well as arrangements to protect student privacy in the administration of protected information surveys and the collection, disclosure, or use of personal information for marketing, sales, or other distribution purposes. The School District will directly notify parents of these policies at least annually at the start of each school year and after any substantive changes. The School District will also directly notify, such as through U.S. Mail or email, parents of students who are scheduled to participate in the specific activities or surveys noted below and will provide an opportunity for the parent to opt his or her child out of participation of the specific activity or survey. The School District will make this notification to parents at the beginning of the school year if the District has identified the specific or approximate dates of the activities or surveys at that time. For surveys and activities scheduled after the school year starts, parents will be provided reasonable notification of the planned activities and surveys listed below and be provided an opportunity to opt their child out of school activities and surveys. Parents will also be provided an opportunity to review any pertinent surveys. Following is a list of the specific activities and surveys covered under this requirement:
Collection, disclosure, or use of personal information for marketing, sales or other distribution. Administration of any protected information survey not funded in whole or in part by ED. Any non-emergency, invasive physical examination or screening as described above.
Parents who believe their rights have been violated may file a complaint with:
Family Policy Compliance Office U.S. Department of Education400 Maryland Avenue, SWWashington, D.C. 20202-5901
CITIZEN’S REQUEST FOR RECONSIDERATION OF MATERIAL
Name
Address
Telephone
Type of Material
Title
Author
State specific objections: (Please cite pages or portions) Attach additional pages as needed.
What do you believe might result from using this material?
What do you believe is the theme or purpose of this material?
Have you reviewed the entire material?
Have you reviewed other material by this person?
If yes, please list the material
What material dealing with same subject would you recommend as a replacement?
(Date) (Signature)
NOTIFICATION FORM FOR POSSIBLE STUDENT RETENTIONOR POSSIBLE STUDENT FAILURE OF A COURSE
TO: ______________________________________________________________[Name of Parent]
FROM: ______________________________________________________________[Name of Administrator or Teacher]
RE: ______________________________________________________________[Name of Student]
DATE: ______________________________________________________________
[Check the following items, as appropriate]:
_____ This is to advise you that the above-named student is in danger of being retained in his/her current grade because his/her performance is insufficient.
PLEASE CONTACT ME AS SOON AS POSSIBLE TO DISCUSS THIS ISSUE.
____ This is to advise you that the above-named student is in danger of being retained in his/her current grade because his/her performance on reading sufficiency tests has demonstrated a reading deficiency.
PLEASE CONTACT ME AS SOON AS POSSIBLE TO DISCUSS THIS ISSUE.
____ This is to advise you that the above-named student is in danger of failing the following course: ________________________________________________.
[Name of course]
PLEASE CONTACT ME AS SOON AS POSSIBLE TO DISCUSS THIS ISSUE.
FORMS FOR
SECTION VBUSINESS
MANAGEMENT
PUBLIC RECORD ACCESS REQUESTOKLAHOMA OPEN RECORDS ACT
TO: PONCA CITY SCHOOL DISTRICT613 East GRAND AVENUEPONCA CITY, OKLAHOMA 74601-5211
1. Pursuant to the Oklahoma Open Records Act, the undersigned hereby requests access to the following School District records:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
[Describe records as specifically as possible; attach additional sheets if necessary.]
2. The undersigned requests access to the foregoing records for the following purpose:
________________________________________________________________________________________________________________________________________________________________________________________________________________________
3. If copies of the documents are requested, the undersigned agrees to pay the per page fee for copies identified in the School District’s Oklahoma Open Records Act policy. If a search is necessary to furnish the documents and if this request is solely for commercial purposes, the undersigned agrees to pay the hourly search fee identified by District policy.
4. The undersigned is acting as representative or agent for ______________________.
(Signature)
Date:
Address:
Received by:Ponca City School Districton ____________________, ______.Record Request No. _____
PONCA CITY SCHOOL DISTRICTRECORDS RETENTION PLAN
Warning: If a record pertains to ongoing or anticipated litigation, do not destroy it!Records need not be maintained in original form unless a claim or lawsuit is suspected.
Student Records
Record Retention Period ReferenceTranscriptsIncludes: name, address, phone, birth date/place, courses (with grades), GPA and/or class rankMay include: academic & extracurricular honors & awards, degrees, extracurricular or after-school activities
80 years from student’s last date of enrollment
70 O.S. § 24-114.C
Screening results(from a regional education service center)
Must destroy when information no longer needed or when student turns 18, whichever is earlier
70 O.S. § 1210.277
Records of access 5-7 years from student’s last date of enrollment
20 U.S.C. § 1232g (b)(4)(A)70 O.S. § 24-114.D
Special education records 5 years from student’s last date of special education services, with 60 day notice to parents or student
All other student records 5-7 years from student’s last date of enrollment
70 O.S. § 24-114.D
Teacher Records
Record Retention Period ReferenceGrade and plan books Recommended: keep until
no longer needed
Incident / anecdotal notes Recommended: keep 5 years
Board Records
Record Retention Period ReferenceAgendas and minutes Permanent 25 O.S. § 312
Real property deeds and titles Recommended: permanent
Payroll Records
Record Retention Period ReferencePayroll statements and affidavits Permanent 62 O.S. § 304.1(C)
Payroll records of non-exempt employees, including:1. Full name;2. Social Security number;3. Identifying symbol or number used on payroll records in place of name;4. Home address, including zip code;5. Date of birth, if under 19;6. Sex and occupation in which employed7. Time of day and day of week in which an employee’s work week begins or the starting time and length of each employee’s work period;8. Regular hourly rate of pay for any work week in which overtime compensation is due, including the basis of the pay by showing the amount paid per hour, per day, per week, or other basis;9. Hours worked each work day and total hours worked each work week;10. Total daily or weekly straight-time earnings or wages due for hours worked during the work day or work week, exclusive of overtime;11. Total pay for overtime hours;12. Total additions or deductions from wages paid each pay period;13. Total wages paid each pay period;14. Date of payment and wages and pay period covered by those wages; and,15. If retroactive payment of wages is made, the employer must record and preserve as an entry on pay records the amount of payment to each employee, the period covered by the
3 years 29 C.F.R. § 516.229 C.F.R. § 516.5
payment, and the date of the payment
Payroll records of bona fide executive, administrative, or professional employees, including all records containing the information in items 1 – 7 and 12 – 15 above, plus the basis on which wages are paid, fringe benefits, and any prerequisites for pay or benefits
3 years 29 C.F.R. § 516.329 C.F.R. § 516.5
Collective bargaining agreements 3 years 29 C.F.R. § 516.5
Employment contracts 3 years 29 C.F.R. § 516.5
Certificates of employment 3 years 29 C.F.R. § 516.5
Sales and purchase records (not related to real property)
3 years 29 C.F.R. § 516.5
Basic employment and earnings records, including time sheets
2 years 29 C.F.R. § 516.6
Wage rate tables 2 years 29 C.F.R. § 516.6
Order, shipping, and billing records 2 years 29 C.F.R. § 516.6
Records of additions to or deductions from wages paid
2 years 29 C.F.R. § 516.6
General Employment Records
Record Retention Period ReferencePersonnel records, including:1. Requests for accommodation2. Applications & records related to hiring3. Evaluations4. Admonishments and reprimands5. Supervisor anecdotal notes6. Sick leave records
2 years from the conclusion of the employee’s employment
29 C.F.R. § 1602.40
Personnel or employment records relating to a charge of discrimination
Through the final disposition of the charge
29 C.F.R. § 1602.40

Drug / Alcohol Testing Records
Record Retention Period ReferenceEmployee drug and alcohol testing record obtained from Department of Transportation regulated employees
3 years from date employee first performs safety-sensitive duties
49 C.F.R. § 40.25(i)
Results of employee alcohol test indicating alcohol concentration of .02 or greater
5 years 49 C.F.R. § 40.333
Results of positive employee drug test 5 years 49 C.F.R. § 40.333
Documentation of an employee’s refusal to take a drug and alcohol test (including substituted or adulterated test results)
5 years 49 C.F.R. § 40.333
SAP reports 5 years 49 C.F.R. § 40.333
Follow up tests /schedules for follow up tests
5 years 49 C.F.R. § 40.333
Negative drug and alcohol test results 1 year 49 C.F.R. § 40.333
Information on drug and alcohol tests obtained from previous employers
3 years 49 C.F.R. § 40.333
Records of inspection, maintenance, and calibration of evidential breath testing apparatuses
2 years 49 C.F.R. § 40.333
Financial Records
Record Retention Period ReferenceFinancial records, including claims, warrants, contracts, purchase orders, and any other financial records or documents – except those from competitively bid projects
5 years 51 O.S. § 24A.470 O.S. § 5-122
Records related to the Competitive Bidding Act, including both successful and unsuccessful bids and all resulting contracts and required bonds
5 years from the date of opening bids or 3 years from the date of completion of the contract, whichever is longer
61 O.S. § 112
Activity fund records 5 years 70 O.S. § 5-122
Report of an audit conducted pursuant to the Oklahoma Public School Audit Law
5 years 70 O.S. § 22-108(B)
Federal and State Programs
Record Retention Period ReferenceRecords pertaining to federal funds, including records disclosing amount and disposition of funds, total cost of activity, share of cost from non-federal sources, and other records that would facilitate an audit
3 years after the completion of the activity for which the funds were used
20 U.S.C. § 1232f(a)
Records pertaining to federal funds which are the subject of litigation, claim, negotiation, or audit ongoing at end of three year retention period
Keep until the issue is resolved
34 C.F.R. § 80.42
Records pertaining to the National School Lunch Program
3 complete, prior school years
7 C.F.R. § 210.20 (b) (12)
PONCA CITY SCHOOL DISTRICTNOTICE OF RECORDS DESTRUCTION
Date
NAMEADDRESSADDRESS
Re: Destruction of Education Records
Dear Parent / Student:
In response to the mandates contained in OKLA. STAT. tit. 70 § 24-114.D please be advised that the district will destroy STUDENT NAME’s non-transcript education records on DATE, which is at least 30 days after this notice is being sent. However, instead of having the records destroyed you may pick up the records on or before the destruction date at the district’s SITE / ADDRESS.
OPTION 1: For records stored in hard copyThese records are maintained as paper copies and there is no charge for you to pick up the records if you want them. You may also request that these records be mailed to you. Retrieving the records by mail requires advance payment of postage costs. Contact NAME / NUMBER to determine the amount of postage to remit.
OPTION 2: For records stored electronicallyThese records are stored electronically and a copy charge will be assessed in accordance with the district’s posted fee schedule prior to releasing records if you want them. You may also request that these records be mailed to you. Retrieving the records by mail requires advance payment of postage costs and copy costs. Contact NAME / NUMBER to determine the fees associated with your request for records.
Again, this notice is being sent to you to fulfill the mandates of Oklahoma law regarding routine student record destruction. No action is required on your part unless you wish to retrieve the records prior to their destruction.
Sincerely,
Name
APPLICATION FOR SANCTIONINGUNDER O KLA . S TAT . tit. 70, § 5-129.1
This is a request for sanctioning by the Applicant to the Board of Education of Ponca
City School District pursuant to which the funds collected by the Applicant are exempt from the
statutory controls over school activity funds. The Applicant is a student achievement program or
a parent-teacher association or organization.
Name of applicant:
Applicant's Address:
Applicant's Taxpayer I.D. No.:
Applicant's Representative fromwhom additional information maybe obtained: ____________________________________
Applicant's Telephone Number: ____________________________________
Applicant's Purpose, Goals andOrganizational Structure: ____________________________________
Describe how the School Districtand its Students will Benefit ifthe Applicant is Sanctioned. ____________________________________
Attach the most recent financial audit report, if any, for the Applicant issued by an independent accounting firm.
Applicant certifies that it does not and will not discriminate with respect to its benefits,
membership, programs, operation or organization on the basis of race, color, sex, pregnancy,
gender, gender expression or identity, national origin, religion, disability, veteran status, sexual
orientation, age, or genetic information.
Applicant acknowledges that the Board of Education has the discretion to sanction or
decline to sanction the Applicant, and the decision of the Board of Education is final and
nonappealable. Applicant further acknowledges that (a) the Board of Education may, at any
time, request the records maintained by the Applicant, which records Applicant will promptly
make available, and (b) the Board of Education may, at any time it believes it is in the best
interest of the School District to do so, withdraw sanctioning, and the decision of the Board of
Education is final and nonappealable.
Applicant also acknowledges that, in order for the School District to consider whether to
maintain the sanctioning action of Applicant, Applicant shall provide to the Board of Education,
upon request, on an annual basis, by July 1 of each year, the audit report, if any, for Applicant's
recently ended fiscal year, prepared by an independent accounting firm.
Instructions to Applicant:
Complete this application. Please print or type. If necessary, please use additional sheets of paper.
Attach Applicant's most recent audit report, if any.
Sign and date this application.
Deliver this application to:
Superintendent
[Address]
(Name of Applicant)
Dated:
By:
PONCA CITY SCHOOL DISTRICTREQUEST FOR RAFFLE
To be completed by requestor.
Date: School:
Group :
Description of item(s) to be raffled with their respective fair market values:
Purpose of fundraising:
Suggested Voluntary Contribution Amount for Ticket (if any): $
Expected Drawing Date, if approved:
Signature of Organization’s Representative:
To be completed by District Personnel:
Request is: Approved Denied
Date:
Signature:
Wellness ResourcesThis list is provided for the administration’s reference only and should not be adopted with the policy.
For: Go to this address:
School level assessments http://www.schools.healthiergeneration.org
USDA nutrition standards http://www.fns.usda.gov/school-meals/nutrition-standards-school-meals
USDA training requirements http://professionalstandards.nal.usda.gov/
Tips to promote health http://smarterlunchrooms.org/ideas
USDA Smart Snacks in Schoolstandards & food lists
www.healthiergeneration.org/smartsnacks
www.healthiergeneration.org/live_healthier/eat_healthier/alliance_product_navigator/browse_products/?product_category_id=720
https://www.healthiergeneration.org/take_action/schools/snacks_and_beverages/celebrations/
http://healthymeals.nal.usda.gov/local-wellness-policy-resources/wellness-policy-elements/healthy-celebrations
Non-food rewards & discipline
https://www.healthiergeneration.org/take_action/schools/snacks_and_beverages/non-food_rewards/
http://cspinet.org/new/pdf/constructive_classroom_rewards.pdf
Fundraising https://www.healthiergeneration.org/take_action/schools/snacks_and_beverages/fundraisers/
http://healthymeals.nal.usda.gov/local-wellness-policy-resources/wellness-policy-elements/healthy-fundraising
Food guidance http://www.choosemyplate.gov/
Free materials, plans http://www.fns.usda.gov/tn/team-nutrition
Let’s Move! Active Schools www.letsmoveschools.org
Shared use agreements http://changelabsolutions.org/shared-use
Fitness and activity assessments
http://www.pyfp.org/
Ideas for physical activity breaks
http://healthymeals.nal.usda.gov/resource-library/physical-activity-school-aged-children/activities-and-tools
https://www.healthiergeneration.org/take_action/schools/physical_activity/physical_activities/
FORMS FOR
SECTION VIPERSONNEL
[FOR APPLICANTS]AUTHORIZATION AND RELEASE
This Authorization and Release is executed under penalty of perjury on the day of , 20 by , an applicant for employment ("Applicant") with the Ponca City School District (“School District”).
Applicant understands that School District's receipt of a national criminal history record check is a condition of employment with School District, and that the record check must reveal that the applicant has not had any felony conviction(s) within the past ten (10) years, or at any time if the conviction shows a tendency to be a danger to the health/safety of students or if the conviction indicates a potential conflict with the duties to be performed by the applicant, unless after review of the facts and circumstances of each situation the administration decides to recommend employment. Because Applicant desires employment with School District, Applicant authorizes School District to request and obtain the results of a national felony record search of Applicant's name, fingerprints, if applicable, social security number and any other lawful means of obtaining such results. Applicant hereby releases Applicant's record check results to School District. Applicant also releases School District of any and all liability relating to its request for, receipt and use of the search results.
APPLICANT ACKNOWLEDGES THAT APPLICANT HAS BEEN FURNISHED AND UNDERSTANDS ALL OF THE REQUIREMENTS OF SCHOOL DISTRICT'S FELONY RECORD CHECK POLICY AND AGREES TO BE BOUND BY ALL OF ITS TERMS AND CONDITIONS.
Applicant also agrees to truthfully answer the following questions:
Have you ever:Yes No
Entered a plea of guilty or nolo contendere to a state (any state) or federal felony charge? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Been convicted of a state (any state) or federal felony offense?
Been charged with a state (any state) or federal felony offense which was reduced to a misdemeanor offense to which you entered a plea of guilty or nolo contendere? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Entered a plea of guilty or nolo contendere to, or been convicted of, a state (any state) or federal misdemeanor charge involving illegal chemical substances or illegal sexual activity? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Entered into a deferred prosecution agreement with a state (any state) or federal prosecutor?
Applicant understands that if Applicant is hired by School District prior to receipt of the results of
the national criminal history record check, Applicant will be classified as a temporary employee until notified otherwise by the superintendent. Furthermore, Applicant understands that if School District does not receive the results of the national criminal history record check within sixty (60) days, the check reveals a prior felony offense conviction that occurred within the past ten (10) years, or at any time if the conviction shows a tendency to be a danger to the health/safety of students or if the conviction indicates a potential conflict with the duties to be performed by the applicant, or if Applicant provides a false response to one or more of the above questions, then Applicant will be deemed to have resigned. The board of education may accept Applicant's resignation at any time within thirty (30) days after the date School District was notified of either the unsatisfactory search results or the false response, whichever is later; and Applicant waives Applicant's right to any and all due process procedures to which Applicant might otherwise be entitled under federal and state law and School District policies and procedures.
APPLICANT UNDERSTANDS AND AGREES THAT IF HIRED BY SCHOOL DISTRICT, THEN APPLICANT IS SUBJECT TO A FELONY RECORD SEARCH AT ANY TIME DURING HIS/HER EMPLOYMENT WITH SCHOOL DISTRICT AND THIS AUTHORIZATION AND RELEASE SHALL REMAIN IN FULL FORCE AND EFFECT THROUGHOUT APPLICANT'S EMPLOYMENT WITH SCHOOL DISTRICT.
"Applicant"
VERIFICATION
STATE OF OKLAHOMA )) ss.
COUNTY OF )
, Applicant, of lawful age and being first duly sworn upon oath, deposes and states: that Applicant is familiar with the statements set forth above; that Applicant has read and fully understood the foregoing Authorization and Release; and Applicant states that all the matters therein set forth are true and correct.
"Applicant"
SUBSCRIBED AND SWORN to before me this day of , 20 .
Notary PublicMy Commission expires:
(SEAL)
[FOR CURRENT EMPLOYEES]
AUTHORIZATION AND RELEASE
This Authorization and Release is executed under penalty of perjury on the day of , 20 by an employee ("Employee") with the Ponca City School District (“School District”).
Employee understands that School District’s receipt of a clear national criminal history record check has been requested by the superintendent and/or board of education. Employee hereby releases his/her felony record check results of his/her name, fingerprints, social security number and any other lawful means of obtaining such results to School District. Employee also releases School District of any and all liability relating to its request for, receipt and use of the search results.
Employee acknowledges that he/she has been furnished and understands all of the requirements of School District's Felony Record Search Policy and agrees to be bound by all of its terms and conditions.
Employee also agrees to truthfully answer the following questions and to promptly report to the Human Resources Director any change in Employee’s criminal history occurring after the answers to questions below are made:
Have you ever:Yes No
Entered a plea of guilty or nolo contendere to a state (any state) or federal felony charge? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Been convicted of a state (any state) or federal felony offense?
Been charged with a state (any state) or federal felony offense which was reduced to a misdemeanor offense to which you entered a plea of guilty or nolo contendere? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Entered a plea of guilty or nolo contendere to, or been convicted of, a state (any state) or federal misdemeanor charge involving illegal chemical substances or illegal sexual activity? (This question includes non-sealed criminal records involving a “deferred sentence” or “deferred judgment.”)
Entered into a deferred prosecution agreement with a state (any state) or federal prosecutor?
Employee understands that if the felony record search reveals a prior felony offense conviction(s) within the past ten (10) years, or at any time if the conviction shows a tendency to be a danger to the health/safety of students or if the conviction indicates a potential conflict with the duties to be performed by the applicant , or if Employee has provided a false response to one or more of the above questions, then Employee's employment by School District will be reviewed to determine whether there is a basis for non-reemployment or dismissal. In any event, the board of education may accept Employee's resignation at any time within thirty (30) days
after the date School District was notified of either the unsatisfactory search results or the false response, whichever is later.
"Employee"
VERIFICATION
STATE OF OKLAHOMA )) ss.
COUNTY OF )
, Employee, of lawful age and being first duly sworn upon oath, deposes and states: that Employee is familiar with the statements set forth above; that Employee has read and fully understood the foregoing Authorization and Release; and Employee states that all the matters therein set forth are true and correct.
"Employee"
SUBSCRIBED AND SWORN to before me this day of , 20 .
Notary PublicMy Commission expires:
(SEAL)
PONCA CITY SCHOOL DISTRICTPOST-ACCIDENT DRUG/ALCOHOL TESTING WORKSHEET
Accident DetailsAttach a detailed description of the accident from all workers injured and/or involved.
Date: Time: .m.Location: Injured Worker(s): Others Involved: Property Damage: Witnesses:
Testing Considerations
Could employee drug/alcohol use have contributed to the accident?
Yes, because:
Testing is permitted, but also see the next consideration.
NoDoes the employee perform hazardous or dangerous duties?
Yes, because:
Testing is permitted, but also see the next consideration.
NoDo not test.
Did other workers contribute to the accident?
YesMake arrangements to test all workers contributing to the incident.
NoNo additional action is needed.
Testing Conclusions
I received notice of a workplace accident/injury on / / at o’clock __.m. from .
I sent the following workers: for testing on / / at the district’s testing facility.
I did not send any workers for testing.
Supervisor Signature Date
PONCA CITY SCHOOL DISTRICTCOMPENSATORY TIME OFF AGREEMENT
In accordance with the Fair Labor Standards Act, the Ponca City School District has a policy of granting employees compensatory time off in lieu of compensation for hours worked in excess of 40 hours a week, or, in the District’s discretion, providing the employee monetary overtime compensation. A copy of this policy has been provided to me. I understand that the compensatory time will be granted at time and one-half for all hours worked in excess of 40 hours per week. I further understand that the compensatory time may be limited, preserved, used or cashed out consistent with the provisions of that policy and applicable law and regulations of the U.S. Department of Labor.
I knowingly agree to this provision of time off as compensation for overtime work as a condition of my employment and consent to the use of compensatory time in accordance with the District’s policy. I further understand that in the event any portion of the policy is interpreted to conflict with the FLSA or its regulations, that the conflicting portion shall be struck and the remainder of the policy shall continue in full force and effect.
__________________________________Employee Signature
__________________________________Date
__________________________________Supervisor Signature
__________________________________Date
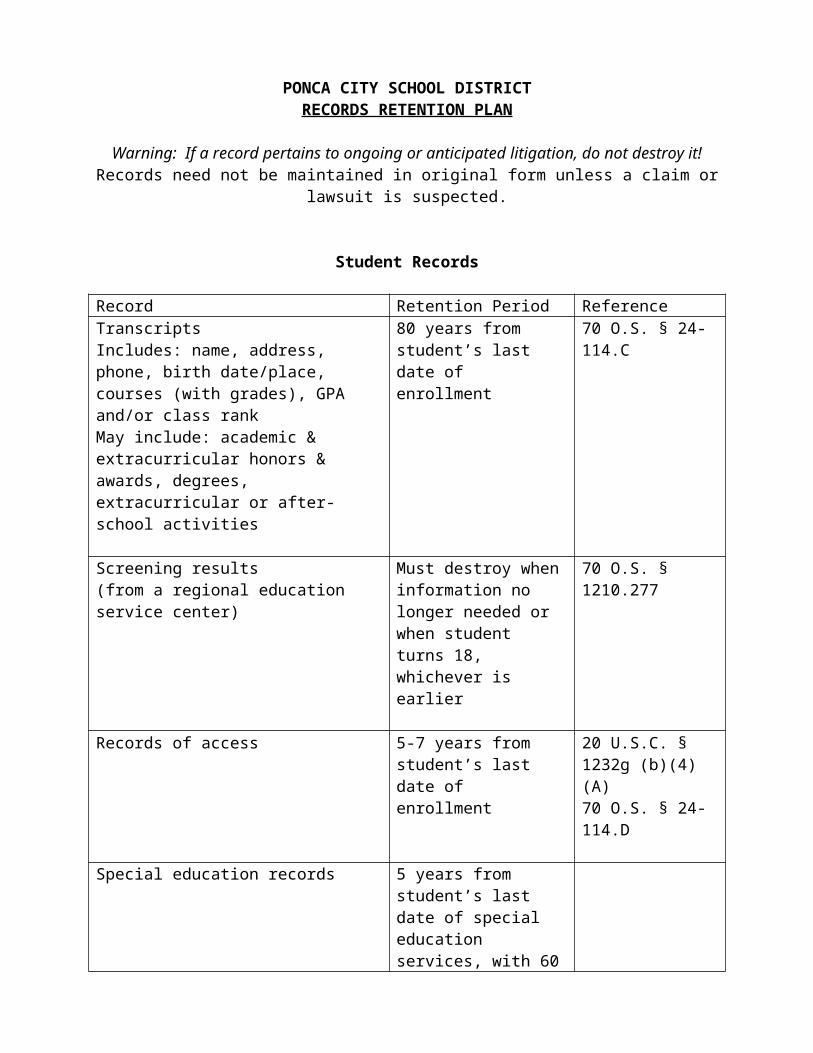
EMPLOYEE ACKNOWLEDGEMENT OF RECEIPT
I acknowledge that I received the following policies:
Policy for Classification of Employees and Rights and Responsibilities Involving Nonexempt Employees;
Policy Regarding Multiple Employment Assignments; and
Compensatory Time for Overtime Policy
I further acknowledge that I have read these policies, any questions I may have had regarding these policies have been answered to my satisfaction, that I understand these policies and agree to comply with these policies.
Employee Signature Date
The supervisor’s signature below verifies that the above named support employee was furnished with the District’s FLSA policies.
Supervisor’s Signature Date
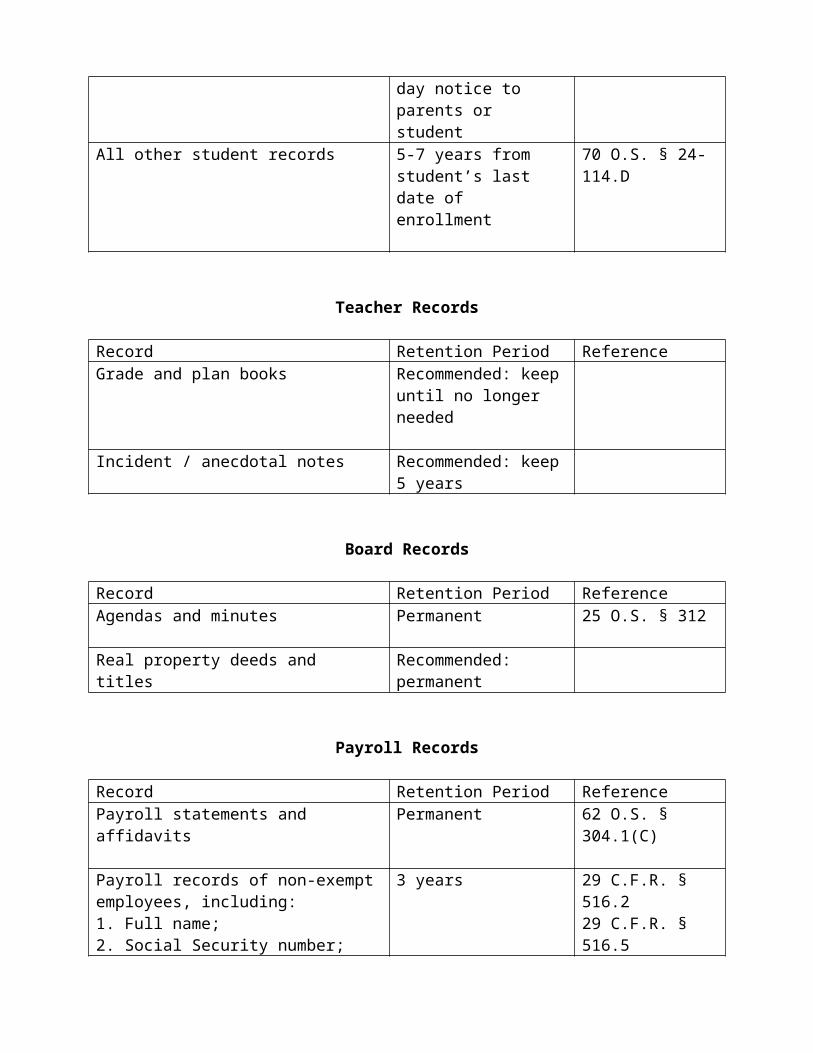
Workers' Compensation/Sick Leave Election Form
The School District shall provide the benefits established under the Oklahoma Workers’ Compensation Act to all School District employees who are injured in on-the-job accidents.
All regular employees who are injured in on-the-job accidents shall receive statutory benefits including medical expenses, temporary compensation and benefits for permanent disability or death.
Certificated Support Personnel
I suffered an on-the-job injury on (month, day, year) , while working for the School District. As a result of the injury, I am entitled to receive temporary disability compensation according to the Workers' Compensation laws of Oklahoma. I understand that I am entitled to receive such compensation for a period of time as may be provided for by law. I have accumulated certain sick leave/personal leave benefits, because of my employment, which are available to me when I am unable to work because of illness or injury.
PLACE AN "X" IN THE APPROPRIATE ELECTION BLANK OR BLANKS
I would prefer only to have:
Sick Leave Compensation/Personal Leave Supplementation --
Number of days (To be filled in by a Human Resources representative)
I understand that by choosing to be paid my accumulated sick leave/personal leave in addition to the temporary disability provided by law, I will be paid my sick leave/personal leave on a prorated basis to the extent that I will receive my full wages until I return to work or the number or sick leave/personal leave days I have are exhausted.
I understand that after the number of specified sick leave/personal leave days are exhausted, I will receive temporary disability compensation for a period of time as may be provided for by law.
I understand that my accrued sick leave/personal leave benefits will be decreased on a prorated basis by those days I use as a result of making this election.
OR
I would prefer only to have:
Under the Workers' Compensation Act, temporary benefits begin the fourth day off work due to an on-the-job injury. The first three days are considered a waiting period during which time temporary benefits are not paid, but I request that I be paid my accrued but unused sick leave/personal leave to cover these three days. I understand that by making this election, I will NOT be paid any sick leave/personal leave benefits beyond the first three days of the waiting period.
(IF YOU PREFER TO RECEIVE YOUR SUPPLEMENTAL BENEFITS UNDER NUMBER 1 ABOVE AND YOUR SICK LEAVE/PERSONAL LEAVE FOR THE FIRST THREE DAYS OF YOUR DISABILITY AS PROVIDED FOR IN NUMBER 2 ABOVE, CHECK BOTH 1 AND 2 ABOVE.)
OR
I would prefer to not use any of my sick leave/personal leave benefits while I am off work due to my on-the-job injury.
Name Social Security # Last First Middle
Address Number & Street City State Zip Code
Job Title School or Department
Dated this day of , 20 .
Employee
Witness:
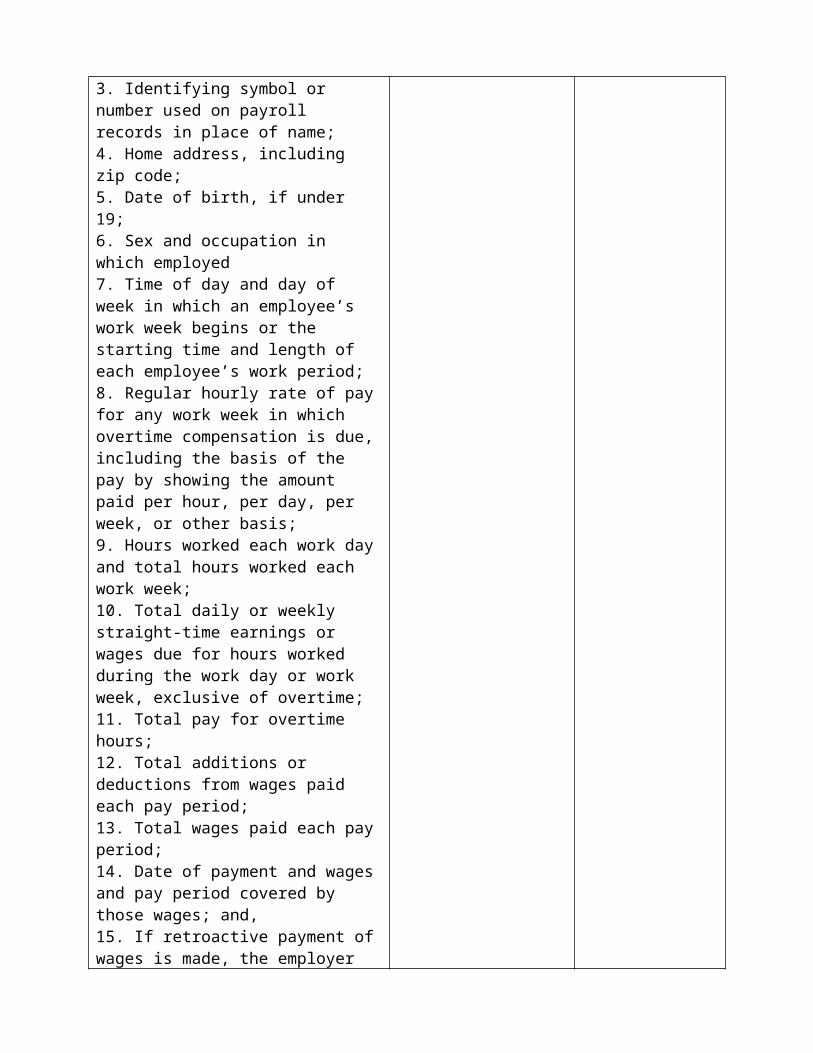
School District Representative
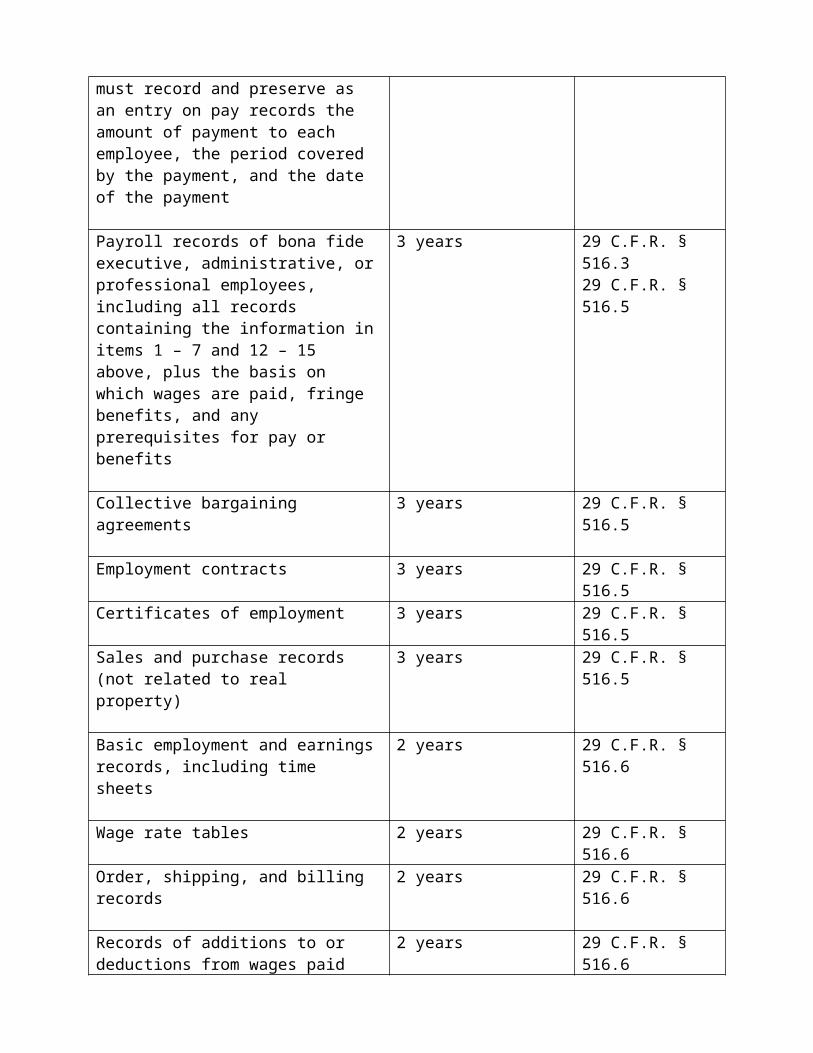
Hazard Communication
Prior to June 1, 2016 the district must develop a new labeling and HazCom program, and provide appropriate training to all employees. The Occupational Safety and Health Administration provides a number of excellent resources and compliance documents, and RFR suggests using OSHA documents as the template for the district’s revised program. OSHA’s website can be accessed at:
https://www.osha.gov/workers.html
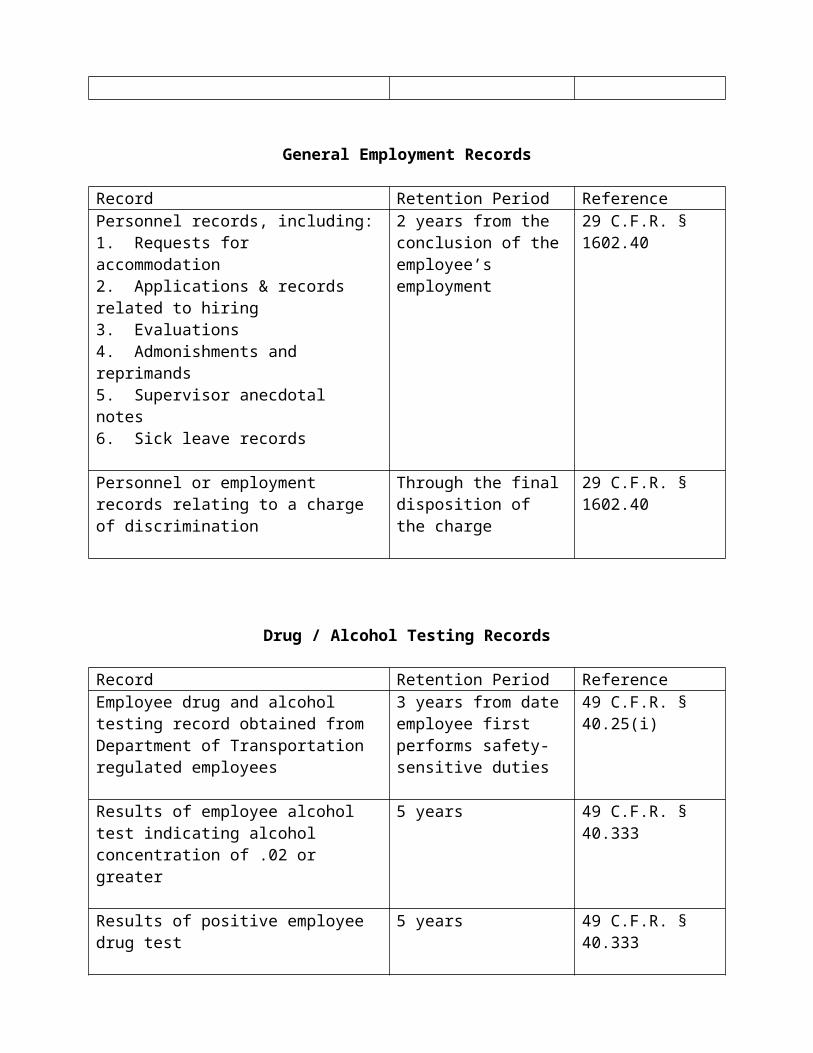
Date
[Name][Address]
Re: Notice of Hearing on Recommendation for Nonreemployment due to Potential Reduction in Force
Dear :
This is to notify you that on the ____ day of __________, _____, at p.m., the Board of Education will hold a hearing at [address] , at which time the Board will consider and determine whether to accept the superintendent’s recommendation that your position be eliminated and that your contract not be renewed for the _____ - _____school year due to a reduction in force.
Enclosed with this letter is a copy of the superintendent’s recommendation which sets out the cause or causes and underlying facts on which the recommendation is based and which is incorporated herein by reference.
You have the right to appear before the Board at the hearing and present your position, and witnesses and other evidence, as to why a reduction in force is not necessary, why your specific teaching position should not be eliminated and why your teaching contract for the _____ - _____ school year should be renewed. You will be given an adequate opportunity to present your side of the matter to the Board of Education.
If you have any questions concerning the procedures to be followed at the hearing, please feel free to contact the superintendent of schools.
Very truly yours,
Clerk of the Board of Education
Enclosure
[TO BE PERSONALLY DELIVERED TO TEACHER ANDTO BE MAILED BY CERTIFIED MAIL,
RETURN RECEIPT REQUESTED, ADDRESSEE ONLY]
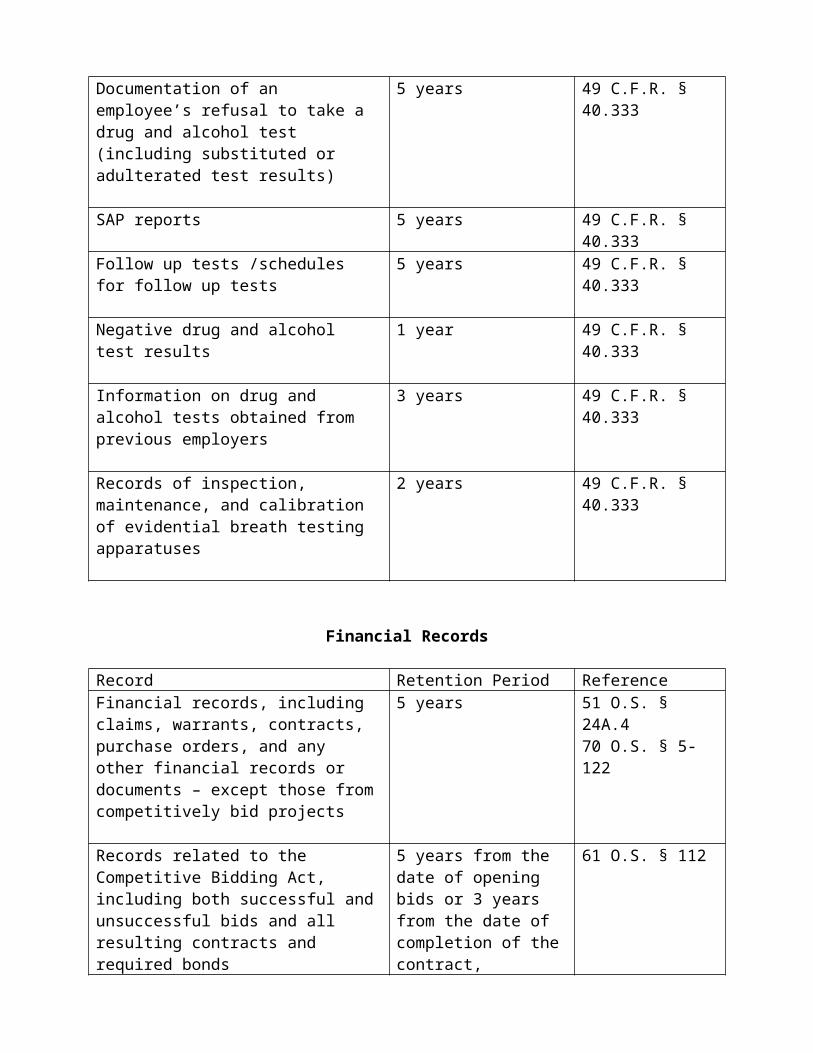
[DATE]
[NAME OF TEACHER][ADDRESS OF TEACHER]
Re: Notice that Nonreemployment [Dismissal] Due to Reduction in Force has been Approved by the Board of Education.
Dear [Mr. or Ms.] :
On the a_____ day of __________, _____, the Board of Education of the __________ School District voted to eliminate your employment position and to [not renew] [dismiss you from] your contract for the _____ - _____ school year because of a reduction in force.
The basis for the Board’s decision is:
The decision of the Board of Education is final and non-appealable.
If the Board decides to reinstate your specific position within the next school year, you will be notified and may be eligible to be reemployed.
Very truly yours,
Superintendent of Schools
[TO BE PERSONALLY DELIVERED TO TEACHER AND TO BE MAILED BYCERTIFIED MAIL, RETURN RECEIPT REQUESTED, ADDRESSEE ONLY]
[IF A PROBATIONARY TEACHER IS DISMISSED UNDER THIS POLICYRATHER THAN NONREEMPLOYED THEN THE LANGUAGE OF THIS
LETTER NEEDS TO BE REVISED TO REFLECT A DISMISSAL]
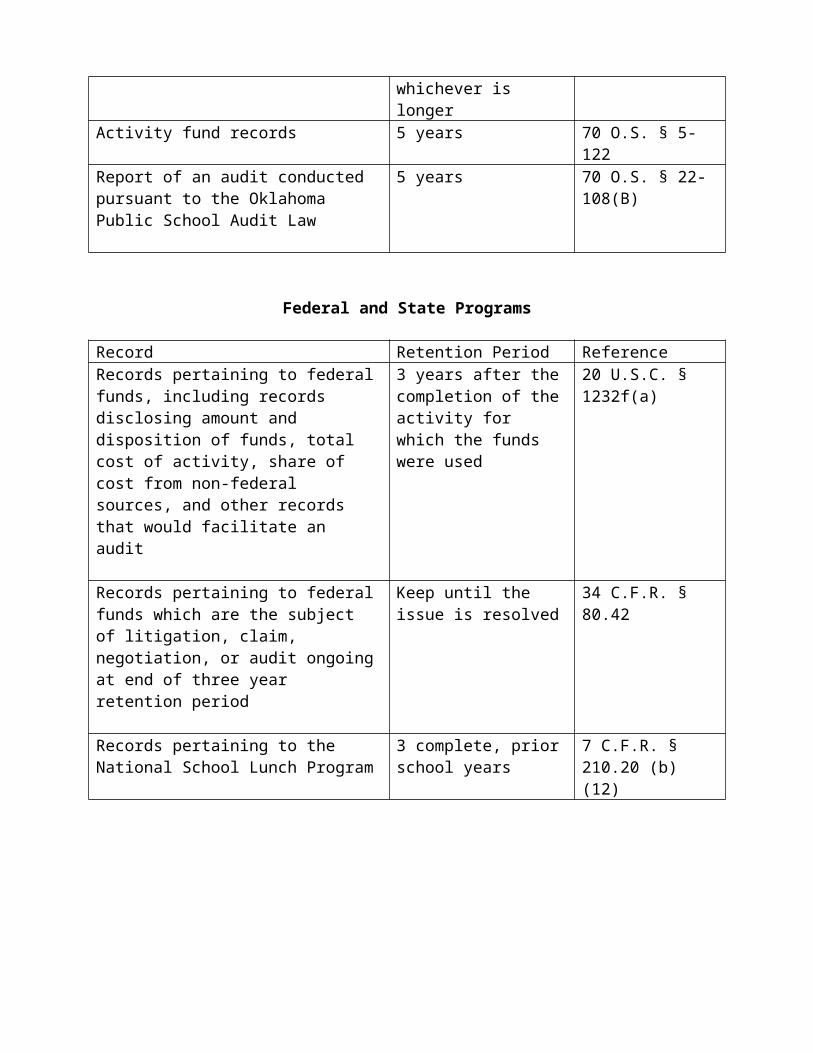
[CAREER TEACHERS ONLY]
[School District Letterhead]
[DATE]
[To be delivered by:Certified Mail, Restricted Delivery,Return Receipt Requested; orPersonal Delivery with a SignedAcknowledgement of Receipt; orProcess Server]
[name][address]
Re: Notice of Hearing on Superintendent's Recommendation for Your [Nonreemployment/Dismissal]
Dear :
This letter will notify you that the Board of Education has received a recommendation from the Superintendent of Schools for your [nonreemployment/ dismissal] from employment in this School District. Enclosed with this letter is a copy of the Superintendent's recommendation which is incorporated herein and which sets out the statutory causes on which the recommendation is based and specifies the underlying facts supporting the recommendation.
This is to further notify you that on the day of , 20 , at p.m., the Board of Education will hold a pre-termination hearing at [ADDRESS OF BOARD] at which time the Board will consider and determine whether to accept the recommendation of the Superintendent that you be [nonreemployed/dismissed] from your employment based on the statutory cause(s) and the underlying facts specified in the Superintendent's recommendation.
You have the right to appear before the Board at the hearing. At the pre-termination hearing the superintendent or his designee will, in person or in writing or both, specify the statutory grounds upon which the recommendation is based and shall also specify the underlying facts and provide an explanation of the evidence supporting the recommendation. You will have a meaningful opportunity to present reasons, in person or writing or both, as to why the proposed action should not be taken. After you respond to the superintendent’s recommendation the board will vote to decide whether to accept or reject the recommendation of the superintendent.
This notice with the accompanying recommendation is sent at the direction of the Board of Education.
Yours very truly,
Clerk of the Board of Education
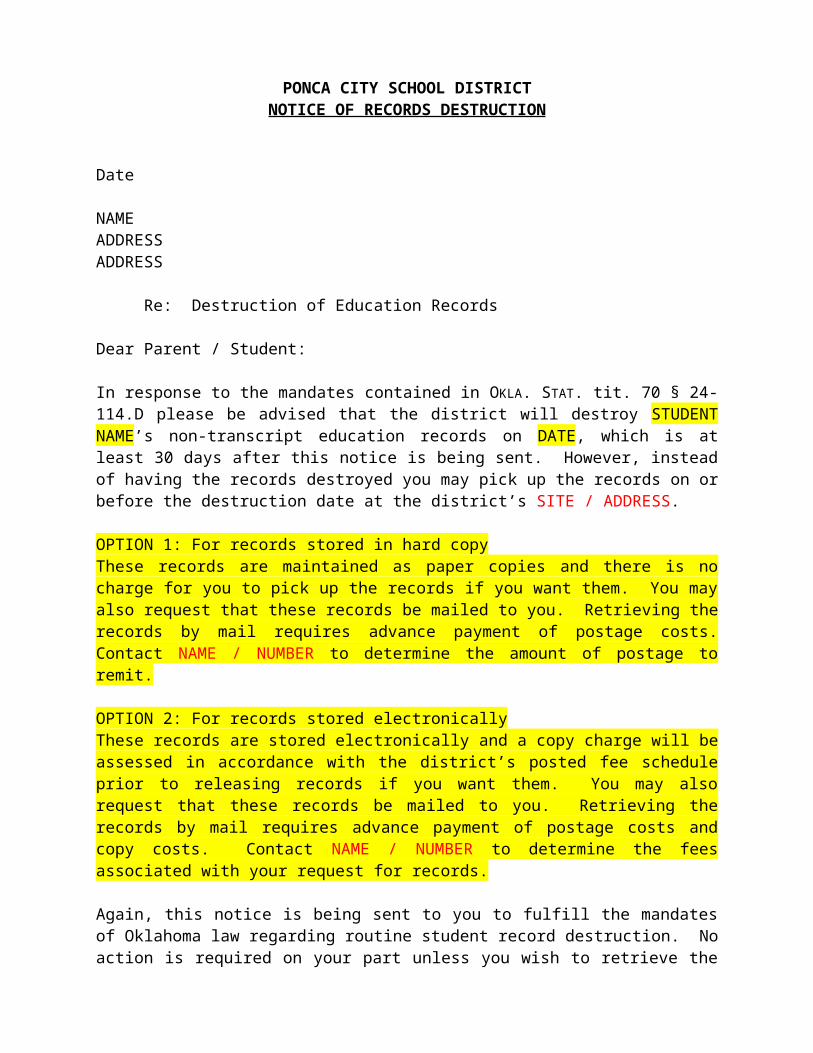
[PROBATIONARY TEACHERS ONLY]
[School District Letterhead]
[DATE]
[To be delivered by:Certified Mail, Restricted Delivery,Return Receipt Requested; orPersonal Delivery with a SignedAcknowledgement of Receipt; or(3) Process Server]
[name][address]
Re: Notice of Hearing on Superintendent's Recommendation for Your [Nonreemployment/Dismissal]
Dear :
This letter will notify you that the Board of Education has received a recommendation from the Superintendent of Schools for your [nonreemployment/ dismissal] from employment in this School District. Enclosed with this letter is a copy of the Superintendent's recommendation which is incorporated herein and which sets out the causes on which the recommendation is based and specifies the underlying facts supporting the recommendation.
This is to further notify you that on the day of , 20 , at p.m., the Board of Education will hold a hearing at [ADDRESS OF BOARD], at which time the Board will consider and determine whether to accept the recommendation of the Superintendent that you be [nonreemployed/dismissed] from your employment based on the causes and the underlying facts specified in the Superintendent's recommendation.
You have the right to appear before the Board at the hearing. The school administration will explain and present evidence regarding the charges against you. You are entitled to be represented by legal or other counsel, to ask questions of the witnesses presented by the administration, to present witnesses on your behalf and to present any relevant evidence or statement which you desire to offer.
If the Board of Education determines the preponderance of the evidence supports the Superintendent's recommendation and warrants your [nonrenewal/dismissal], then the Board of Education can vote to [nonreemploy/dismiss] you.
The decision of the Board of Education is final and nonappealable.
This notice with the accompanying recommendation is sent at the direction of the Board of Education.
Yours very truly,
Clerk of the Board of Education
[POST HEARING NOTICE LETTER]
[School District Letterhead]
[DATE]
[name][address]
Re: Notice that Nonreemployment [Dismissal From Employment] has been Approved by the Board of Education.
Dear [Mr. or Ms.] :
On , 20___, the Board of Education of the School District, meeting in (regular/ special) session and having heard and duly considered all matters required by law to be considered, voted to [immediately dismiss you from your employment as a teacher with the School District] [not renew your teaching contract for the school year]. The specific cause and underlying facts for your nonrenewal [dismissal] which serve as the basis for the Board's decision are set forth in the attached motion adopted by the Board.
Sincerely yours,
______________________________Superintendent of Schools
[TO BE MAILED BY CERTIFIED MAIL,RESTRICTED DELIVERY, WITH RETURN RECEIPT REQUESTED
AND A COPY HAND DELIVERED TO TEACHER, IF POSSIBLE]
NOTICE TO SUPPORT EMPLOYEE OFSUSPENSION WITHOUT PAY, DEMOTION OR TERMINATION
TO:
On the ____ day of _________________ , 20_____, an initial hearing was held concerning your employment status. This will notify you of: [Mark the Applicable Item]
A. Suspension Without Pay as a Disciplinary Measure.
You have been suspended from your employment without pay and other benefits as a disciplinary measure from _________________ , 20_____, to _________________ , 20_____.
B. Demotion Action.
You have been demoted from ________________________ to ________________________, with appropriate reduction in pay and other benefits, effective _________________ , 20_____.
C. Termination Action.
You have been terminated, effective as of _________________ , 20_____.
The above action has been taken for the following cause or causes:
You are entitled by law to a hearing before the Board of Education on this action. If you desire to exercise this right, you must notify the Board of Education in writing within ten (10) working days of the postmark on the envelope in which this notice is sent. FAILURE TO REQUEST A HEARING WITHIN THE ABOVE TIME WILL RESULT IN THE LOSS OF YOUR RIGHT TO A HEARING. ENCLOSED FOR YOUR CONVENIENCE IS A HEARING REQUEST FORM. IF YOU DESIRE A HEARING ON THE ABOVE ACTION, THE ENCLOSED HEARING REQUEST FORM SHOULD BE DELIVERED TO THE CLERK OF THE BOARD OF EDUCATION AT THE PONCA CITY SCHOOL DISTRICT, 613 E. GRAND AVENUE,
1
PONCA CITY, OKLAHOMA, 74601-5211, OR MAILED BY CERTIFIED MAIL TO THE SAME PERSON AT THE PONCA CITY SCHOOL DISTRICT, 613 E. GRAND AVENUE, PONCA CITY, OKLAHOMA, 74601-5211.
If you request a hearing you will be notified in writing of the date, time and place of the hearing. The hearing will be conducted at the next, or next succeeding, regularly scheduled meeting of the Board of Education if the hearing request is received at least 10 days prior to the next, or the next succeeding regularly scheduled Board of Education meeting. However, you have the right to request a special board meeting to conduct the hearing, which special meeting will be held no earlier than 10 days nor later than 30 days after receipt of your hearing request.
You have the following hearing rights: the right to be present in person; the right to be represented by counsel of your choice; the right to present evidence and witnesses on your behalf; and the right to confront and cross-examine witnesses on behalf of the school administration. The Board of Education at the hearing may affirm, modify or reverse the above action and may increase or decrease the severity of the above action. The decision of the Board of Education will be final.
Yours very truly,
Superintendent of Schools
Enclosure: Hearing Request Form
2
[DATE]
[NAME OF EMPLOYEE][ADDRESS]
Re: Notice to Support Employee of Proposed Nonreemployment
Dear Mr./Ms.________________________:
This is to advise you that the Board of Education intends to consider and act on whether you should not be reemployed with the School District for the 20__-20__ fiscal year. The cause for your possible nonreemployment is as follows:
You are entitled by law to a hearing before the Board of Education on this proposed action. If you desire to exercise this right, you must notify the Board of Education in writing within ten (10) WORKING days of the postmark on the envelope in which this notice is sent. FAILURE TO REQUEST A HEARING WITHIN THE ABOVE TIME WILL RESULT IN THE LOSS OF YOUR RIGHT TO A HEARING. ENCLOSED FOR YOUR CONVENIENCE IS A HEARING REQUEST FORM. IF YOU DESIRE A HEARING ON THE ABOVE PROPOSED ACTION, THE ENCLOSED HEARING REQUEST FORM SHOULD BE DELIVERED TO THE CLERK OF THE BOARD OF EDUCATION AT THE PONCA CITY SCHOOL DISTRICT, 613 E. GRAND AVENUE, PONCA CITY, OKLAHOMA, 74601-5211, OR MAILED BY CERTIFIED MAIL TO THE SAME PERSON AT THE PONCA CITY SCHOOL DISTRICT, PONCA CITY, OKLAHOMA, 74601-5211.
If you request a hearing you will be notified in writing of the date, time and place of the hearing. The hearing will be conducted at the next, or next succeeding, regularly scheduled meeting of the Board of Education if the hearing request is received at least 10 days prior to the next, or the next succeeding regularly scheduled Board of Education meeting or at a special meeting called by the Board, at the Board's discretion. However, you have the right to request a special board meeting to conduct the hearing, which special meeting will be held no earlier than 10 days nor later than 30 days after receipt of your hearing request.
You have the following hearing rights: the right to be present in person; the right to be represented by counsel of your choice; the right to present evidence and witnesses on your behalf; and the right to confront and cross-examine witnesses on behalf of the school administration. At the conclusion of the hearing, the Board of Education will vote to reemploy
1
or nonreemploy you for the ensuing fiscal year. The decision of the Board of Education is final and nonappealable.
Yours very truly,
Superintendent of Schools
Enclosure: Hearing Request Form
[TO BE SENT BY CERTIFIED MAIL, RETURN RECEIPT REQUESTED, RESTRICTED DELIVERY]
2
HEARING REQUEST FORM
TO: Clerk of Board of Education
I hereby request a hearing before the Board of Education on the ___ suspension without pay as a disciplinary measure ___ demotion ___ termination action ___ proposed nonreemployment concerning my employment. I acknowledge receipt of the Notice dated _________, 20__, concerning such action. I understand that the hearing will be conducted at the next, or next succeeding, regularly scheduled meeting of the Board of Education if the hearing request is received at least 10 days prior to the next, or the next succeeding regularly scheduled meeting of the Board, or at a special meeting of the Board, at the Board's discretion, unless I check the item below requesting a special meeting of the Board of Education.
I request a special meeting of the Board of Education, to be held no earlier than 10 days nor later than 30 days after receipt of this hearing request.
Support Employee Date
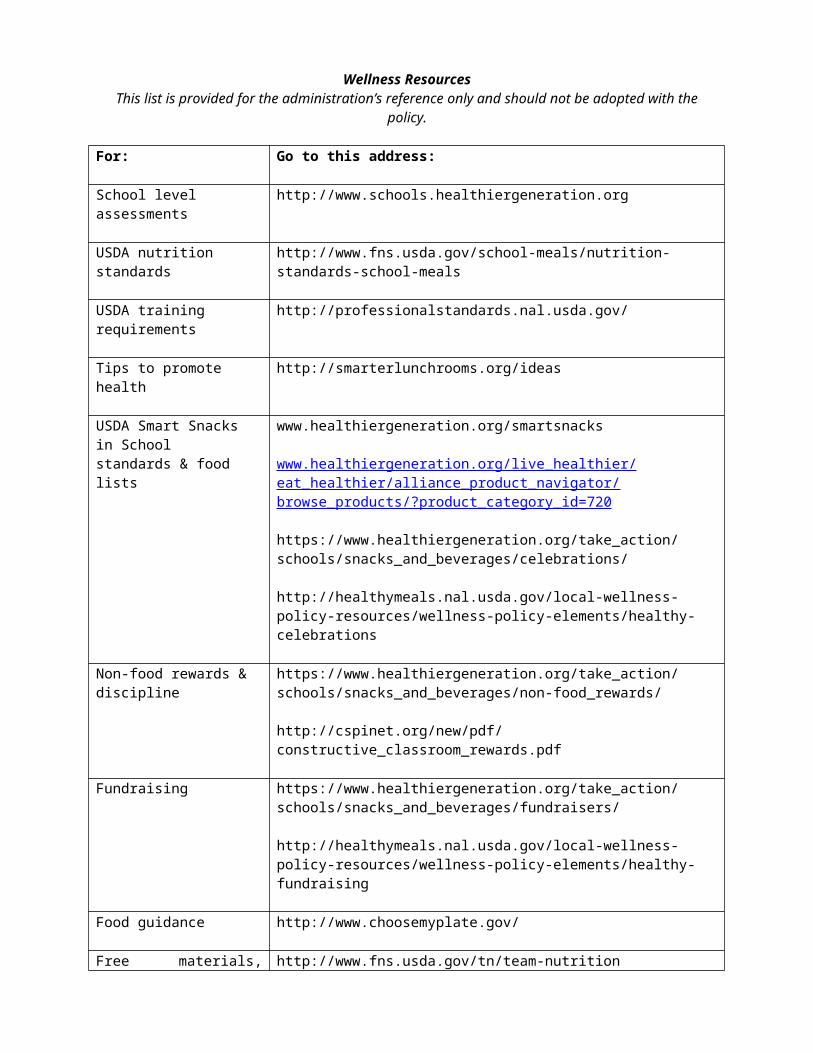
AFFIDAVIT
STATE OF OKLAHOMA )) ss:
COUNTY OF _______ )
The undersigned, under the penalties of perjury, certifies to the Ponca City School District (“District”) as follows:
1. The undersigned:_____ has a contract with the District; OR_____ is the duly authorized representative of a business (“entity”) having a contract with the
District,to perform work on District premises on a full-time or part-time basis, which work would not otherwise be performed by District employees.
2. The undersigned hereby certifies that the undersigned will not allow any employee of the undersigned or of the entity, or of any subcontractor, to perform work on District premises on a full-time or part-time basis that would otherwise be performed by District employees if such employee is or has been convicted in this state, the United States or another state of any felony offense unless ten (10) years has elapsed since the date of the criminal conviction or the employee has received a pardon for the offense.
3. No employee of the undersigned, or the entity, who performs any work on District property is currently registered or required to register under the Oklahoma Sex Offenders Registration Act or the Mary Rippy Violent Crime Offenders Registration Act.
4. The undersigned, or the entity _____ has OR _____ has not conducted a felony record search of employees who would be assigned to work on a part-time or full-time basis on District property.
5. This Affidavit is intended to comply with Okla. Stat. tit. 70, § 6-101.48.
EXECUTED AND DELIVERED this _____ day of _______________, 20___.
____________________________________________AFFIANT SIGNATURE
____________________________________________(Print Name and Title)
Representing:
____________________________________________(Name of Entity)
Subscribed and sworn to before me this _____ day of _____________, 20__.
My Commission expires: _______________________________________________________________ Notary Public
[SEAL]
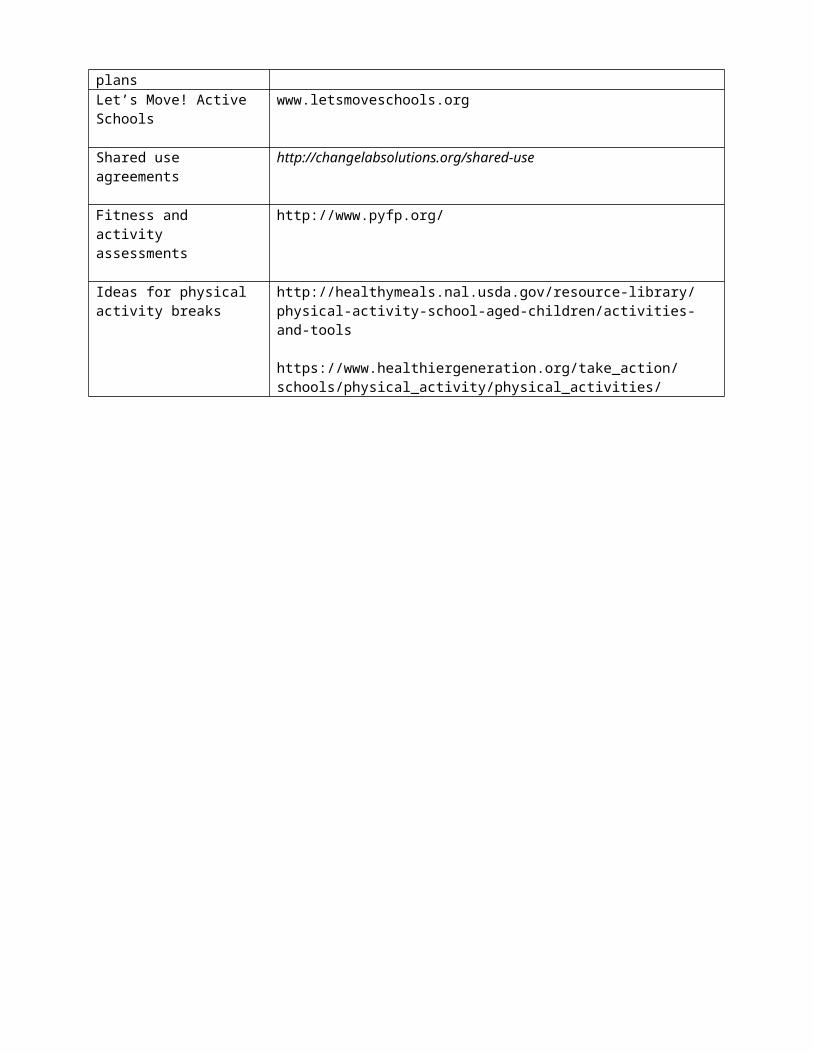
FORMS FOR
SECTION VIISTUDENTS
ATTORNEY-IN-FACT AFFIDAVIT2
I certify that I am the parent or legal custodian of:
Full name of minor child Date of birth
Full name of minor child Date of birth
Full name of minor child Date of birth
I designate the following individual as the attorney-in-fact for each minor child named above:
Full name of attorney-in-fact
Street address, city, state and zip code of attorney-in-fact
Home phone, attorney-in-fact Work phone, attorney-in-fact
I provide the attorney-in-fact the following authority:
I delegate to the attorney-in-fact all of my power and authority regarding the care, custody and property of each minor child named above, including but not limited to the right to enroll the child in school, inspect and obtain copies of education records and other records concerning the child, the right to attend school activities and other functions concerning the child, and the right to give or withhold any consent or waiver with respect to school activities, medical and dental treatment, and any other activity, function or treatment that may concern the child. This delegation shall not include the power or authority to consent to marriage or adoption of the child, the performance or inducement of an abortion on or for the child, or the termination of parental rights to the child.
OR
2 Student residency cannot be established through an attorney-in-fact relationship without this fully completed document.
I delegate to the attorney-in-fact the following specific powers and responsibilities:
This delegation shall not include the power or authority to consent to marriage or adoption of the child, the performance or inducement of an abortion on or for the child, or the termination of parental rights to the child.
Effective Dates
This power of attorney is effective for a period not to exceed one year (12 calendar months), beginning on , 20 and ending , 20 . I reserve the right to revoke this authority at any time. I understand that in order to extend this power of attorney beyond one year I must execute and deliver to the district a new power of attorney.
Signatures
I hereby make these designations as specified above.
Parent signature Date
I hereby accept my designation as attorney-in-fact for the minor child(ren) specified in this power of attorney.
Attorney-in-fact signature Date
Acknowledgment
Before me, the undersigned, a Notary Public, in and for said County and State on this day of , 20 , personally appeared (name of parent/legal custodian) and (name of attorney-in-fact) to me known to be the identical persons who executed this instrument and acknowledged to me that each executed the same as his or her free and voluntary act and deed for the uses and purposes set forth in the instrument.
Witness my hand and official seal the day and year above written.
Signature of notarial officer
My commission expires(Seal)
ATTACHMENT AApplication Form
Completion of this form is required of each applicant for a transfer in order to apply the criteria of this policy. Failure to fully and truthfully complete and timely submit this form to the district will result in a denial of the transfer. Completion of this form will be in addition to completion of any form required by the State Board of Education.
1. Full name of student as it appears on the student’s birth certificate:
2. Date of student’s birth:
3. Current address of student:
4. Full names of parent(s), guardian(s), or custodian(s) of the student:
5. Educational history of the student:
A. School district in which student currently resides:
B. School in which the student is currently enrolled, if different from above.
C. If the student has not exclusively attended the school district in which the student is currently enrolled, list the name of each school district and addresses, if known, in which student has ever been enrolled:
School: Dates of Attendance: Grade Completed Upon Leaving District:
School: Dates of Attendance: Grade Completed Upon Leaving District:
School: Dates of Attendance: Grade Completed Upon Leaving District:
6. Current or last completed grade of student:
7. Grade in which the student desires to enroll:

8. Courses in which the student desires to enroll in each semester in the coming school year:
9. Has the student a disciplinary record for violating school regulations?
Yes _____ No _____
If Yes, state school(s) in which each violation occurred and approximate date(s) of violation(s):
10. Has the student ever been suspended from school or placed in a alternative education program or setting for disciplinary reasons?
Yes _____ No _____
If Yes: For each suspension and alternative program or setting, state the school which suspended or placed the student; the nature of the offense; and approximate date of the suspension or placement, if different from the above:
11. Has the student been adjudicated as a delinquent for either a violent or nonviolent offense under relevant Oklahoma law?
Yes _____ No _____
If Yes: State the name of the court making the adjudication; the time of such adjudication; the nature of offense; whether the student is still under any court supervision; and, if so, the name of the person overseeing such supervision:
12. Has the student been convicted as an adult for either a violent or nonviolent offense as defined in relevant Oklahoma law ?
Yes _____ No _____
If Yes: State the name of the court in which the conviction was entered; the time of the conviction; the nature of the offense; the sentence imposed; whether the student is still under any court supervision; and, if so, the name of the parole officer or other supervisor:
13. Has the student committed on school property, in school transportation, or at a school event, a violent act or an act showing deliberate or reckless disregard for the health or safety of faculty or others?
Yes _____ No _____
If Yes: State the school district attended when the act occurred; the approximate date of the act; and describe what occurred:
14. Has the student possessed on school property, in school transportation, or at a school event, an alcoholic beverage; low-point beer, as defined by relevant Oklahoma law; or been involved with missing or stolen property found to have been taken from a student, school employee, or the school during school activities?
Yes _____ No _____
If Yes: State, for each separate act, the school district attended when the act occurred; the approximate date of the act; and describe what occurred:
15. Has the student possessed on school property, while in school transportation, or at a school event, a dangerous weapon or a controlled dangerous substance, as defined by relevant Oklahoma law, or a prescription or non-prescription mood altering substance?
Yes _____ No _____
If Yes: State, for each separate act, the school district attended when the act occurred; the approximate date of the act; and describe what occurred:
16. Has the student ever been removed from any school for making an electronic communication with the intent to terrify, intimidate, harass, or threaten injury or harm to faculty or other students?
Yes _____ No _____
If Yes: State, for each separate act, the school district attended when the act occurred; the approximate date of the act; and describe what occurred:
17. If the student has been identified as a child with a disability, this district will need to review all such records to make a reasonable determination of whether the district has the facilities, programs, staff, and space to implement the student’s current or anticipated Individualized Education Program (IEP) or Section 504 Accommodation Plan, and, if preliminary approval of a transfer is made, to conduct the statutorily-required joint IEP or Section 504 conference with the resident school district. Is the student currently, or has the student been, a child with a disability who received an IEP or Section 504 Accommodation Plan?
Yes _____ No _____
If Yes: Brief describe the nature of the disability; the approximate time period in which the student has been, or was, under an IEP or Section 504 Accommodation Plan; and the names of the school districts which implemented the student’s plan:
18. Do you agree to complete the Consent For Release Of Confidential Information, allowing this district to review all educational records of the student from all previous schools attended by the student?
Yes _____ No _____
ATTACHMENT BTransfer Student Consent to Cancellation of Transfer
The undersigned, who is not a resident of this district, recognizes:
1. That the undersigned non-resident student has a right by law to attend the school district of residence;
2. That the non-resident student desiring to enroll in this district has no statutory right to attend this district;
3. That the district is not required to accept this transfer application; and,4. That the district does not desire to accept a transfer of a student who will detract from the
educational process of resident students or take the place of another transfer applicant who would not detract from that process.
The undersigned hereby agrees that if the district approves a transfer allowing the undersigned student to enroll in this district, the administration of the district has the consent of the undersigned to cancel the transfer during the approved enrollment school year if:
1. The student fails to comply with student behavior rules set by the district, school, or teacher;2. The parent(s), or student 18 years of age or older, fails to promptly pay financial obligations
owed to the district, including payments owed, but not limited to, school lunches and for lost or destroyed district property; or,
3. The student does not have a valid excuse for failure to attend school.4. The superintendent or board determine that due to a financial shortfall
occurring at any time or over-enrollment causing crowded classrooms or programs that it is necessary to cancel any transfer for the best interests of the students who reside in the district.
The undersigned also is informed that this consent to cancellation is a necessary component for continued enrollment after transfer acceptance, and thus the consent may not be withdrawn at any time in the future.
The undersigned also understands that although the administration will notify the parent(s), or student 18 years of age or older, of any cancellation, the undersigned understands and agrees that the determination of the administration that a cancellation is to be effected will be final, that the undersigned will have no right to appeal that determination to the board of education, and that after cancellation, the administration will send the educational records of the student to the student’s resident school district or to such other school district as the undersigned directs.
By signing this agreement, I affirm that I have read and understand the above conditions concerning acceptance of the transfer application and my consent to district authority to cancel the transfer, if granted, for the reasons stated above.
EXECUTED this _____ day of _____________________, 2________.
Signature of Parent (or Adult Student) Applying for Transfer
Printed Name of Parent (or Adult Student) Applying for Transfer
APPLICATION FOR TRANSFER UNDER THE DEPLOYED PARENTS SCHOOL ACT OF 2013
1. Full name of student as it appears on the student’s birth certificate:
2. Date of student’s birth:
3. Current address of student:
4. Full name(s) of student’s parent(s):
5. Name of parent on active duty (copy of Department of Defense ID card required):
6. Full name of student’s custodian(s) during parent’s active duty:
7. Address of custodian(s):
8. Period of parent’s active duty (copy of orders required):
9. School district in which student currently resides:
10. School district which student attends, if different from above:
11. Current or last completed grade of student:
12. Grade in which the student desires to enroll:
13. Courses in which the student desires to enroll in each semester in the coming school year:
14. If the student has been identified as a child with a disability, this district will need to review all such records to implement the student’s current or anticipated Individualized Education Program (IEP) and conduct the statutorily-required joint IEP conference with the resident school district. Is the student currently, or has the student been, a child with a disability who received an IEP?
Yes _____ No _____
If Yes: Briefly describe the nature of the disability; the approximate time period in which the student has been, or was, under an IEP; and the names of the school districts which implemented the student’s IEP:
15. Do you agree to complete the Consent for Release of Confidential Information, allowing this district to review all educational records of the student from all previous schools attended by the student?
Yes _____ No _____

STUDENT SEARCH REPORT FORM
Student searched:_________________________________________________________________
Date of search:___________________Approximate time:_________________________
Person conducting the search:________________________________________________________
Person witnessing the search:________________________________________________________
Grounds for reasonable suspicion that the student should be searched:
_______________________________________________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
What kinds of items were the object of the search:_______________________________________
_______________________________________________________________________________
What was searched (pockets, purse, wallet, coat, etc.): ____________________________________
_______________________________________________________________________________
What was found and where:_________________________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
What was done with any items found:_________________________________________________
_______________________________________________________________________________
Date:____________________________ ______________________________________Person Conducting the Search
______________________________________Witness
______________________________________Principal
PONCA CITY PUBLIC SCHOOLSNOTICE OF ADMINISTRATIVE ACTION
TO: _______________________________________ DATE: ______________________
SUBJECT: ___________________________________________________________________(Name of Student)
Please be advised that your child has violated the school district’s discipline policy by:
For violating the school district’s discipline policy the following action is hereby taken:
1. Short-term out-of-school suspension for _____ days beginning ____________________. 2. Long-term out-of-school suspension for _____ days beginning ____________________. 3. Long-term out-of-school suspension for balance of semester. 4. Long-term out-of-school suspension for balance of this semester and succeeding
semester.
SHORT-TERM OUT-OF-SCHOOL SUSPENSION APPEAL
You are entitled to appeal an out-of-school suspension to the building Suspension Review Committee (SRC). If you desire review by the SRC, please advise this office in writing no later than five (5) calendar days from the receipt of the principal’s decision, and you will be promptly advised as to when the SRC meeting will beheld.
LONG-TERM OUT-OF-SCHOOL SUSPENSION APPEAL
You are entitled to appeal an out-of-school suspension decision to the Superintendent and the Board of Education. If you desire an appeal to the Superintendent, please advise the Superintendent in writing no later than five (5) calendar days from the receipt of the principal’s decision, and you will be promptly advised as to when the Superintendent’s conference will be held.
The student may return to school: ___________________________________________.
_________________________________________Principal/Assistant Principal
Receipt acknowledged this _____ day of _____________, 20__.
____________________________________ ____________________________________Parent or Guardian Student
*Notice to Parents/Guardians Due Process is located on the back of this form.FORM A
1

NOTICE TO PARENTS/GUARDIANSDUE PROCESS
The student has:
The opportunity to know these policies or any other school regulations or procedures; Been informed of the policy, rule or regulation allegedly violated; Sufficient opportunity to give his/her version of the alleged violation; The right to a conference with the principal; The right to appeal a suspension of ten (10) days or less to the Suspension Review Committee (SRC), and if over ten (10) days, to the Superintendent
and the Board of Education
SPECIAL NOTICE: A disabled student and his or her parent/guardian are entitled to the procedural protection of Section 504 and/or IDEA-B before the student’s placement is changed for disciplinary reasons.
APPEAL
The student suspended out of school shall have the right to appeal the principal’s suspension action by following the procedures outlined below:
IF THE OUT-OF-SCHOOL SUSPENSION IS FOR TEN (10) DAYS OR LESS (SHORT-TERM)
A student who has been given a short-term out-of-school suspension and the student’s parent/guardian have the right to appeal the out-of-school suspension decision to a building SRC.
Within five (5) calendar days from the date the principal’s decision is received by the parent/guardian or student, the student or the student’s parent/guardian may request, in writing, a review by the building SRC. The SRC is composed of teachers and/or administrators.
The SRC will meet to review the suspension action as soon as possible. The principal will notify the student’s parent/guardian of the date, time and place of the hearing not less than 24 hours in advance of the hearing.
The student and the student’s parent/guardian will have a right to be present at the hearing and to present evidence and witnesses to support their position. Either party wishing to have legal counsel present must give the other party 24 hours advance notice or he/she may not have counsel present. The SRC will determine the guilt or innocence of the student and the reasonableness of the term of the out-of-school suspension.
The SRC will sustain, rescind, or modify the out-of-school suspension action. THE DECISION OF THE SRC WILL BE FINAL AND NONAPPEALABLE.
IF THE OUT-OF-SCHOOL SUSPENSION IS FOR MORE THAN TEN (10) DAYS (LONG-TERM)
A student and/or parent/guardian may appeal the out-of-school suspension decision of the principal to the Superintendent of Schools and the Board of Education.
Within five (5) calendar days from the date the principal’s decision is received by the parent/guardian or student, the student’s parent/guardian may request, in writing, a review of the out-of-school suspension by the Superintendent.
The Superintendent will schedule a hearing as soon as possible, notify the parent/guardian of the date, time and place of the hearing at least 24 hours prior to the hearing and notify the parent/guardian that they and the student have a right to be present at the hearing.
The Superintendent will review the facts, determine the guilt or innocence of the student, the reasonableness of the term of the suspension and decide to sustain, rescind, or to modify the out-of-school suspension. The Superintendent will notify the student’s parent/guardian of the decision at the conclusion of the hearing.
If the student and/or parent/guardian is not satisfied with the action of the Superintendent, the student and/or parent/guardian may appeal that decision to the Board of Education by written notice to the Superintendent or Board Clerk within five (5) calendar days after the Superintendent’s decision. The student and/or parent/guardian will be notified in writing of the date, time and place of the Board of Education hearing at least 24 hours prior to the hearing. The student and the student’s parent/guardian will have a right to be present in person at the hearing. Both the administration and the student or student’s parent/guardian will have the right to present evidence and witnesses to support their position and to be represented by legal counsel. The Board of Education will determine the guilt or innocence of the student and the reasonableness of the term of the out-of-school suspension. The Board will sustain, rescind or modify the out-of-school suspension action. THE DECISION OF THE BOARD OF EDUCATION WILL BE FINAL AND NONAPPEALABLE.
All appeal hearings are based on the following criteria:
Is the student guilty or innocent of a violation of a school rule, policy, or regulation? Is the term of the out-of-school suspension reasonable and in keeping with the severity of the infraction?
SPECIAL NOTICE: Students who are disabled and are subject to out-of-school suspension will be afforded the same treatment as provided to students who are not disabled in accordance with Section 504 and its implementing regulations at 34 C.F.R. § 104.4(a), (b) (1) (vii). Specifically, suspension and appeal procedures will be the same as for students who are disabled. These procedures could be altered if the administration makes a determination that the student will be a danger to other students, staff, or school property, or would substantially interfere with the educational process at the school.
2
PONCA CITY PUBLIC SCHOOLS
PRINCIPAL'S MEMORANDUM
Re: Student Conference
Student:
Date and Time of Conference:
Persons Present:
Policy, Rule, or Regulation Violated:
Summary of Conduct:
Student's Response:
Decision (set forth length of suspension and beginning date):
Factors considered in decision:
Date Signature
Form B
3
PONCA CITY PUBLIC SCHOOLS
INDIVIDUALIZED PLANFOR
OUT-OF-SCHOOL SUSPENSION
(To be used for out-of-school suspensions in excess of five (5) school days that do not involve possession of a dangerous weapon or controlled dangerous substance.)
TO: DATE: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
The named student has been suspended out of school in compliance with the policy of the Ponca City Public Schools. Because of the out-of-school suspension, the student has been placed in a home-based school work assignment setting or another appropriate work assignment setting. This Plan will provide for the core units in which the student is enrolled. Under state law, core units consist of the minimum English, mathematics, science, social studies and art units required by the Oklahoma State Department of Education for grade completion in grades kindergarten through eight and for high school graduation in grades nine through twelve. As the student’s parent or guardian, you are responsible for providing him/her with and placing him/her in a supervised, structured environment. You also bear the responsibility for monitoring the student’s educational progress until he/she returns to school.
The following Plan will be in effect from , 20 through , 20 .
(Use additional pages if necessary.)
All assigned work completed and returned according to this Plan will be graded for full credit, and no absences will be charged to the student’s attendance record. The student’s failure to comply with this Plan by not completing and returning all assigned school work according to this Plan will result in a grade of 0 for each such assignment.
Principal
Receipt acknowledged this day of , 20 .
Student Parent or Guardian
Form C
1
PONCA CITY PUBLIC SCHOOLS
NOTICE OF ADMINISTRATIVE ACTIONPURSUANT TO SUSPENSION CONFERENCE WITH PRINCIPAL
(For Out-of-School Suspensions of 10 Days or Less)
TO: DATE: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
Please be advised that pursuant to a suspension conference held this date between the principal, you, and your child, who was previously charged with:
the following action is hereby taken1:
1. No action. 2. Out-of-school suspension for days beginning _______________ 3. Other (describe)
You are entitled to appeal the principal’s out-of-school suspension decision to the building Suspension Review Committee (SRC). If you desire review by the SRC, please advise this office in writing no later than five (5) calendar days from the receipt of the principal's decision, and you will be promptly advised as to when the SRC meeting will be held.
Principal
Receipt acknowledged this _______ day of , 20 .
Parent or Guardian
Student
Form D
PONCA CITY PUBLIC SCHOOLS
NOTICE OF ADMINISTRATIVE ACTIONPURSUANT TO SUSPENSION CONFERENCE WITH PRINCIPAL
(For Out-of-School Suspensions of More Than 10 Days)
TO: DATE: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
Please be advised that pursuant to a suspension conference held this date between the principal, you, and your child, who was previously charged with:
the following action is hereby taken2:
1. No action 2. Out-of-school suspension for days beginning ______________ 3. Out-of-school suspension for balance of this semester 4. Out-of-school suspension for balance of this semester and succeeding semester 5. Other (describe)
You are entitled to appeal the principal’s out-of-school suspension decision to the Superintendent and the Board of Education. If you desire an appeal to the Superintendent, please advise the Superintendent in writing no later than five (5) calendar days from the receipt of the principal's decision, and you will be promptly advised as to when the Superintendent’s conference will be held.
Principal
Receipt acknowledged this day of , 20 .
Parent or Guardian
Student
Form E
PONCA CITY PUBLIC SCHOOLS
NOTICE OF SUSPENSION REVIEWCOMMITTEE MEETING
TO: DATE: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
Please be advised that a meeting of the Suspension Review Committee has been scheduled for the ______day of , 20 , at .m. at .
You have previously been furnished with a copy of your appeal rights.
Please contact me if you have any questions.
Principal
Form F
PONCA CITY PUBLIC SCHOOLS
NOTICE OF SUPERINTENDENT'S CONFERENCE
TO: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
DATE:
Please be advised that a conference before the Superintendent has been scheduled for the day of , 20 , at , .m. in the Superintendent's office.
If the Superintendent’s decision is adverse to you, you are advised that pursuant to Title 70, Section 24-101.3 of the Oklahoma Statutes, as amended, and School District policy, you are entitled to a hearing before the Board of Education. You have previously been furnished with a copy of your appeal rights.
Please contact me if you have any questions.
Superintendent
Form G
PONCA CITY PUBLIC SCHOOLS
SUSPENSION REVIEW COMMITTEE'S MEMORANDUM
Re: Appeal Conference
Student:
Date and Time of Conference:
Persons Present:
Policy, Rule, or Regulation Violated:
Summary of Conduct:
Student's Response:
Decision (if student is to be suspended, set forth length of suspension and beginning date):
Factors considered in decision: ______
Date Signature
Form H

PONCA CITY PUBLIC SCHOOLS
SUPERINTENDENT'S MEMORANDUM
Re: Appeal Conference
Student:
Date and Time of Conference:
Persons Present:
Policy, Rule, or Regulation Violated:
Summary of Conduct:
Student's Response:
Decision (if student is to be suspended, set forth length of suspension and beginning date):
Factors considered in decision:
Date Signature
Form I
PONCA CITY PUBLIC SCHOOLS
NOTICE OF SUPERINTENDENT'S ACTIONPURSUANT TO APPEAL TO SUPERINTENDENT
TO: DATE: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
Please be advised that pursuant to the appeal conference before the Superintendent the following action is hereby taken3:
1. No action 2. Out-of-school suspension for days beginning ______________ 3. Out-of-school suspension for balance of this semester 4. Out-of-school suspension for balance of this semester and succeeding semester 5. Other (describe)
You have previously been advised of the reason(s) for the out-of-school suspension. Further, you are advised that pursuant to Title 70, Section 24-101.3 of the Oklahoma Statutes, as amended, and School District policy, you are entitled to a hearing before the Board of Education, if the Superintendent’s action is adverse to you. If you desire a hearing, please notify this office or the Clerk of the Board in writing within five (5) calendar days of your receipt of the Superintendent's decision.
Superintendent
Receipt acknowledged this day of , 20 .
Parent or Guardian
Student
Form J
PONCA CITY PUBLIC SCHOOLS
NOTICE OF OUT-OF-SCHOOL SUSPENSION HEARINGBEFORE THE BOARD OF EDUCATION
TO: (Name of Parent or Guardian)
SUBJECT: (Name of Student)
DATE:
Please be advised that pursuant to your request as received by the Superintendent or the Clerk of the Board of Education, a hearing before the Board of Education has been set for .m. on the day of , 20 , in the Board conference room, at which time evidence will be heard and a final determination rendered as to the action taken by the administration of this school.
Please contact me if you have questions.
Superintendent
Form K
PONCA CITY PUBLIC SCHOOLS
WAIVER OF REVIEW OF THEOUT-OF-SCHOOL SUSPENSION DECISION
(Select Proper Paragraph)
I agree with the principal's decision to suspend my child out of school. I understand that I have the right to appeal the principal's decision to the Suspension Review Committee (for an out-of-school suspension of ten days or less) or to the Superintendent and ultimately the Board of Education (for an out-of-school suspension of more than ten days). I hereby waive my right to appeal review of the decision.
Parent/Guardian Signature
Student’s Name
Date
I agree with the Superintendent's decision to uphold the suspension of my child from school. I understand that I have the right to appeal the Superintendent's decision to the Board of Education. I hereby waive my right to appeal review of the decision.
Parent/Guardian Signature
Student’s Name
Date
Form L
Bullying Report FormInstructions
Complete the form below with as much information as possible. If you need assistance completing this form, contact the district’s bullying coordinator (Contact information here). Return the completed form to (Contact information here).
Anonymous reports will be investigated to the best of the district’s ability, but full information allows the district to conduct a more thorough inquiry. No individual will be retaliated against for filing a good faith bullying report.
Individual Making the Report
Name: Report Date: School: Grade / Job Title: Contact Numbers:
Incident Information:
Date of Incident: Time: Location of Incident: Describe Incident: Use additional pages as necessary, and attach any relevant documents
Other Witnesses:
The information in this report is true and correct to the best of my knowledge. I understand that the district will not tolerate retaliation for filing a good-faith report of bullying. I also understand that if I knowingly file a false report of bullying, I may face disciplinary consequences.
Reporter’s Signature Date

Investigation Report
Investigator: Position/Title: Date report received: Date investigation begun:
Required Notifications
Date target’s parent notified of a report received: Method: Date target’s parent notified of completed inquiry: Method: Date bully’s parent notified of a substantiated report: Method: Date reported to district’s bullying coordinator: Method: Date reported to law enforcement, if applicable: Method:
Investigation Process
Individuals interviewed: (attach additional pages if needed)
Name: Date: Interview summary:
Name: Date: Interview summary:
Name: Date: Interview summary:
Name: Date: Interview summary:
Name: Date: Interview summary:
Documents reviewed: (attach additional pages if needed)Note: attach copies of all documents reviewed, including witness statements.
Document: Date: Document: Date: Document: Date: Document: Date: Document: Date: Document: Date: Document: Date:
Conclusions reached:
Actions taken:
Conclusions reached:
Bullying did /did not occur
Bullying (or perceived bullying) appeared to be motivated by:
Age Disability, genetic information Gender, gender expression or identity, sexual orientation, pregnancy Race, color, national origin Religion Sex Veteran status Other:
Actions taken (referrals, education, discipline, etc.) :Note: If the target is a student on an IEP or Section 504 Plan, the team must be convened, regardless of whether the bullying appeared to be motivated by the student’s disability.
OJA Referral: Yes No
Demographics – Target (or alleged target)
Race
Hispanic / Latino American Indian / Alaska Native Asian Native Hawaiian / Pacific Islander Black or African American White Multiracial Other:
Gender
Male Female Transgender
Religion
Disability Status
None known IDEA 504 Plan
English Proficiency Proficient LEP
Demographics – Bully (or alleged bully)
Race
Hispanic / Latino American Indian / Alaska Native Asian Native Hawaiian / Pacific Islander Black or African American White Multiracial Other:
Gender
Male Female Transgender
Religion
Disability Status
None known IDEA 504 Plan
English Proficiency Proficient LEP
Signature of Investigator Date
PONCA CITY SCHOOL DISTRICTNOTIFICATION OF RIGHTS UNDER FERPA
The Family Educational Rights and Privacy Act (FERPA) (20 U.S.C. § 1232g; 34 CFR Part 99) is a Federal law that affords parents and “eligible students” over 18 years of age certain rights with respect to the student's education records. They are:
1. The right to inspect and review the student's education records within 45 days from the day the School District receives a request for access.
Parents or eligible students must submit a written request to the school principal or appropriate school official that identifies the record(s) they wish to inspect. This school administrator will make arrangements for access to the education records and will notify the parent or eligible student of the time and place where these records may be inspected.
2. The right to request correction of the student's education records that the parent or eligible student believes are inaccurate, misleading or otherwise in violation of the student’s privacy rights.
Parents or eligible students may ask the School District to amend a record they believe is inaccurate, misleading or otherwise in violation of the student’s privacy rights. They must submit a written request to the school principal or appropriate school official, clearly identify the part of the record they want changed, and specify why it is inaccurate, misleading or otherwise in violation of the student’s privacy rights.
If the School District decides not make changes in the record as requested, the School District must notify the parent or eligible student of the decision and advise them of their right to a hearing regarding the request for correction. Additional information about hearing procedures will be provided to the parent or eligible student at the time of this notification.
3. The right to consent to disclosures of personally identifiable information contained in the student's education records, except to the extent that FERPA authorizes disclosure without consent (34 CFR § 99.31).
School officials with legitimate educational interests are permitted disclosure without consent. A school official is a person employed by the School District as an administrator, supervisor, instructor, or support staff member, including health or medical staff and law enforcement unit personnel; a person serving on the School Board; a person or company with whom the School District has contracted to perform a special task, such as an attorney, auditor, medical consultant or therapist; or a parent or student serving on an official committee, such as a disciplinary or grievance committee, or assisting another school official in performing his or her tasks.
A school official has a legitimate educational interest if the official needs to review an education record in order to fulfill his or her professional responsibility.
Upon request, the School District will disclose education records without consent to officials of another school district in which a student seeks or intends to enroll.
School districts may disclose, without consent, “directory” information; however, the School District must inform parents and eligible students about directory information, allowing them a reasonable amount of time to request that the School District not disclose directory information about that student.
School districts must notify parents and eligible students annually of their rights under FERPA by means of a special letter, inclusion in a Parent/Teacher Association (PTA) bulletin, student handbook and/or other means left to the discretion of each school district.
4. The right to file a complaint with the U.S. Department of Education concerning alleged failures by the School District to comply with the requirements of FERPA. The name and address of the Office that administers FERPA are Family Policy Compliance Office, U.S. Department of Education, 400 Maryland Avenue, SW, Washington, D.C. 20202-5920.
PONCA CITY SCHOOL DISTRICTDIRECTORY INFORMATION NOTICE
The Family Educational Rights and Privacy Act (FERPA), a Federal law, requires that the School District, with certain exceptions, obtain your written consent prior to the disclosure of personally identifiable information from your child’s education records. However, the School District may disclose appropriately designated “directory information” without written consent, unless you have advised the District to the contrary in accordance with District procedures. The primary purpose of directory information is to allow the School District to include this type of information from your child’s education records in certain school publications. Examples include:
A playbill, showing your student’s role in a drama production; The annual yearbook; Honor roll or other recognition lists; Graduation programs; and Sports activity sheets, such as for wrestling, showing weight and height of team members.
Directory information, which is information that is generally not considered harmful or an invasion of privacy if released, can also be disclosed to outside organizations without a parent’s prior written consent. Outside organizations include, but are not limited to, companies that manufacture class rings or publish yearbooks. In addition, two federal laws require local educational agencies (LEAs) receiving assistance under the Elementary and Secondary Education Act of 1965 (ESEA) to provide military recruiters, upon request, with three directory information categories – names, addresses and telephone listings – unless parents have advised the LEA that they do not want their student’s information disclosed without their prior written consent.
If you do not want the School District to disclose directory information from your child’s education records without your prior written consent, you must notify the Superintendent in writing. The School District has designated the following information as "directory information," and it will disclose that information without prior written consent:
1. The student's name;2 The names of the student's parents;3 The student's address;4. The student's telephone listing;5. The student's date and place of birth;6. The student’s dates of attendance;7. The student's grade level (i.e., first grade, tenth grade, etc.);8. The student's participation in officially recognized activities and sports;9. The student's degrees, honors and awards received;10. The student's weight and height, if a member of an athletic team;11. The most recent educational agency or institution attended;12. The student’s photograph; and13. The student’s electronic mail address.
The School District will notify parents and eligible students annually of the designated items of directory information by means of a District newsletter, newspaper notice, school handbook or individual notice. Parents and eligible students have the right to exclude directory information from public access by notifying the Superintendent’s office in writing of any or all of the items they refuse to permit the School District to designate as directory information about that student within two weeks of receiving the notice. At the end of the two-week period, each student's records will be appropriately marked to indicate the items the School District will not designate as directory information about that student. This designation will remain in effect until it is modified by the written direction of the student's parent or the eligible student.
MEDICATION ADMINISTRATION AUTHORIZATION FORM(Medication Administered by School Personnel)
Student Name:
Student D.O.B.:
TO: (Administrator) (School)
I am the parent, guardian or legal custodian with legal custody of , a minor student attending this school. This student requires medication at intervals during the school day.
I hereby give my consent and authorize school personnel who are authorized by Ponca City Public Schools to administer medicine to administer:
Nonprescription Medication (name of drug), a non-prescription medication which I am hereby supplying you, in accordance with my written instructions and the label directions and manufacturer’s guidelines or the written instructions of a physician which are attached hereto.
Prescription Medication (name of drug), a filled prescription medication which I am hereby supplying you, in accordance with the directions for the administration of the medicine listed on the prescription label.
Prescription Medication (name of drug), a filled prescription medication which I am hereby supplying you, in accordance with the written instructions of the physician prescribing the medicine, which is attached hereto.
I agree to abide by all of the terms of the school district’s policy on the Administration of Medicine to Students, a copy of which will be given to me on my request.
Date Signature Address Parent with legal custody/guardian
MEDICATION ADMINISTRATION AUTHORIZATION FORM(Medication Administered by Student)
Student Name:
Student D.O.B.:
TO: (Administrator) (School)
I am the parent, guardian or legal custodian with legal custody of , a minor student attending this school. This student has a condition which may require medication during the school day. The student’s physician and I believe it is in the student’s best interest that the medication, including any specialized equipment to deliver the medication, be transported and administered by my child in accordance with the district’s policy.
I hereby give my consent and authorize my child to self-administer the following medicine, subject to the district’s policies and procedures regarding self administration of medication:
Prescription Medication (name of drug), a filled prescription medication which I am hereby supplying, in accordance with the directions for the administration of the medicine listed on the prescription label.
Prescription Medication (name of drug), a filled prescription medication which I am hereby supplying, in accordance with the written instructions of the physician prescribing the medicine, which is attached hereto.
I agree to abide by all of the terms of the school district’s policy on the administration of medicine to students, a copy of which will be given to me on my request. I specifically confirm that my child has been instructed on the proper use of the medication and that the district is not liable for any adverse reaction as a result of self-administration.
Date Signature
Address Parent with legal custody/guardian
CONFIDENTIAL ASTHMA HEALTH ACTION PLAN
Student: Date: Date of Birth: Grade: School:
You have checked on school records that your child has Asthma.It is important to have current health information and direction when your child needs help during school. Please check with your child’s doctor for assistance in completing this form. Both parent and physician signatures are required. Return to your student’s school or to the Office of School Nurse Consultant’s at 613 East Grand Avenue Ponca City, OK 74601.
ASTHMA HISTORY:
How long has your child had asthma? How often do the asthma attacks occur? Has hospitalization been needed in the past year? No / Yes When: Is a peak flow meter used: No / Yes. Best flow rate is: How many days would you estimate he/she missed school last year due to asthma? Physician (who is treating asthma): Address: Phone Number:
CHECK THE CONDITIONS THAT TRIGGER AN ASTHMA ATTACK:_____ Emotional Stress _____ Seasonal (Spring Summer Fall Winter)_____ Respiratory infection _____ Exposure to cold air_____ Exercise (describe, e.g. after running) _____ Cough (constant, nagging) Animals_____ Foods (describe) _____ Other (describe)
CHECK THE SIGNS THAT MAY BE PRESENT IN AN ASTHMA ATTACK:_____ Shortness of Breath _____ Wheezing_____ Unable to get a deep breath _____ Coughing_____ Cyanosis (Blue color to lips) _____ Other _____ Anxiety, fearfulness
MEDICATION:
EMERGENCY CONTACTS AND PHONE NUMBERS
Name: Relationship: Numbers: H: ___________________ W __________________ C
Name: Relationship: Numbers: H: ___________________ W __________________ C
a.
EMERGENCY MEDICATIONS:
Medication: Dosage: Frequency: Medication: Dosage: Frequency:
COMMENTS/SPECIAL INSTRUCTIONS:
In my opinion, this student shows capability to self-carry and self-administer the above stated medication(s) or perform the above described procedure without supervision or monitoring of school personnel unless in an emergency situation. ________________________________________________________________________
Health Care Provider Signature Date
Parent/Guardian Signature Date
STEPS TO BE TAKEN DURING AN ASTHMA ATTACK
1. Assist student with prescription medication.2. Encourage student to relax (take slow deep breaths & stay in a sitting position).3. Stay with the student and observe for inadequate breathing.4. Do not give any food or liquid.5. CALL 911 if:
a. No improvement in 15-20 minutes after initial treatment with medication and a relative cannot be reached.b. Peak flow of _______________.c. Trouble walking or talking.d. Lips or fingernails are gray or blue.
e. Hard time breathing: Chest and neck muscles pull with breathing. Child is hunched over to breathe.
Child is struggling to breathe.
CONFIDENTIAL SEVERE ALLERGIC REACTION HEALTH PLAN
Student: Date: Date of Birth: Grade: School:
You have checked on school records that your child has It is important to have current health information and direction when your child needs help during school. Please check with your child’s doctor for assistance in completing this form. Both parent and physician signatures are required. Return to your student’s school or to the Office of School Nurse Consultants at 613 East Grand Avenue Ponca City, OK 74601.
HISTORY
How long has your child had this condition? Is the child routinely seen by a doctor? No / Yes Doctor’s Name: Address: Phone Number:
Does your child need any special activity adaptations/protective equipment at school? Activity restrictions will require written direction from the student’s physician. Yes No If Yes please list
Has your child been hospitalized in the past year for severe allergic reactions? No / Yes
When/Where: Treatment:
CHECK ANY SEVERE ALLERGY YOUR CHILD PRESENTLY HAS:
_____ Bee Stings/Wasp Stings/Bug Bites_____ Pollens (Spring Summer Fall Winter)_____ Food Allergy – List Type ___________________ Other
MEDICATIONS:
Medication: Dosage: Frequency: Medication: Dosage: Frequency:
Check Signs Usually Present During Allergic Reaction:
□ Itching, feeling of tingling or swelling of the lips, tongue or mouth
□ Itching and/or a sense of tightness to the throat, hoarseness and hacking cough□ Hives, itchy rash, feeling of tingling and/or swelling to the face and extremities□ Nausea and Vomiting□ Abdominal cramping and/or diarrhea (runny stools)□ Shortness of breath□ Repetitive coughing and/or wheezing□ “Thready and/or weak “ pulse, passing out , extreme paleness, clammy skin□ Anxiety; feeling of apprehension or fear
EMERGENCY TREATMENTDO NOT HESITATE TO CONTACT 911
IF STUDENT EXPERIENCESSeveral hivesItchy skinSwelling at site of an insect sting OR if an ingestions (or sting) is suspected:Treatment:
1. Send student to office ACCOMPANIED by an adult.2. Give student IMMEDIATELY.3. Contact the parent or emergency contact person.4. Stay with student, keep student quiet and monitor symptoms until parent/emergency contact person
arrives.5. Watch student for more serious symptoms listed below.6. DO NOT HESITATE TO CONTACT 911.
SEVERE ALLERGIC REACTION□ Itching, feeling of tingling or swelling of the lips, tongue or mouth□ Itching and/or a sense of tightness to the throat, hoarseness and hacking cough□ Hives, itchy rash, feeling of tingling and/or swelling to the face and extremities□ Nausea and Vomiting□ Abdominal cramping and/or diarrhea (runny stools)□ Shortness of breath□ Repetitive coughing and/or wheezing□ “Thready and/or weak “ pulse, passing out , extreme paleness, clammy skin□ Anxiety; feeling of apprehension or fear
Treatment:1. Have student use their EpiPen, or give EpiPen immediately by holding against upper outer thigh
(may be given through clothes).2. Call 911 immediately Paramedics should always be called if EpiPen is given3. Contact parents or emergency contact person.4. If possible, copy student’s – record of event –signs, symptoms of distress, emergency measures
instituted student’s response to measures and time lines.Directions for use of EpiPen
Pull off gray cap Place black tip against upper outer thigh Press hard into outer thigh, until it clicks. HOLD in place 10 seconds, then remove
*SAVE EPI-PEN AND GIVE TO PARAMEDICS
Emergency Phone Numbers:Name Relationship Phone Number
In my opinion, this student shows capability to self-carry and self-administer the above stated medication(s) or perform the above described procedure without supervision or monitoring of school personnel unless in an emergency situation.
Healthcare Provider Signature Date
Parent Signature Date
Concussion/Head Injury Fact Sheet
What is a concussion?A concussion is a brain injury that: Is caused by a bump or blow to the head Can change the way your brain normally works Can occur during practice or games in any sport Can happen even if you have not been knocked
out Can be serious even if you have just been
“dinged”All concussions are serious. A concussion can affect your ability to do schoolwork and other activities like playing video games, working on a computer, studying, driving or exercising. Most people with a concussion get better, but it is important to give your brain time to heal.
What are the symptoms of a concussion?Signs and symptoms of a concussion can show right up after the injury or may not appear to be noticed until days or weeks after the injury.
Signs Observed by Parents or GuardiansIf your child has experienced a bump or blow to the head during a game or practice, look for any of the following signs and symptoms of a concussion: Appears dazed or stunned Is confused about assignment or position Forgets an instruction Is unsure of game, score or opponent Moves clumsily Answers questions slowly Loses consciousness (even briefly) Shows behavior or personality changes Cannot recall event prior to hit or fall Cannot recall events after hit or fall
Symptoms Reported by Athletes: Headache or “pressure” in head Nausea or vomiting Balance problems or dizzinesss; double or blurry
vision Sensitivity to light or noise Feeling sluggish, hazy, foggy or groggy Concentration or memory problems Confusion Does not “feel right”
What should you, the student athlete, do if you think you have a concussion? Tell your coaches or parents. Never ignore a bump or
blow to the head even if you feel fine. Also, tell your coach if one of your teammates may have a concussion.
Get a medical checkup. A doctor or health care professional can tell you if you have a concussion and when you are OK to return to play.
Give yourself time to get better. If you have had a concussion, your brain needs time to heal. While your brain is still healing, you are much more likely to have a second concussion. Additional concussions can cause damage to your brain. It is important to rest until you get approval from a doctor or health care professional to return to play.
What should parents/guardians do if they think their child has a concussion? Seek medical attention right away. A health care
professional will be able to decide how serious the concussion is and when it is safe for your child to return to sports.
Keep your child out of play. Concussions take time to heal. Don’t let your child return to play until a health care professional says it’s OK. Children who return to play too soon—while the brain is still healing—risk a greater chance of having a second concussion. Second or later concussions can be very serious. They can cause permanent brain damage, affecting your child for a lifetime.
Tell your child’s coach about any recent concussion. Coaches should know if your child had a recent concussion in ANY sport. Your child’s coach may not know about a concussion your child received in another sport or activity unless you tell the coach.
How can you prevent a concussion? Follow the coach’s rules for safety and the rules of the
sport. Practice good sportsmanship. Use the proper equipment, including personal protective
equipment (such as helmets, padding, shin guards and eye and mouth guards –IN ORDER FOR EQUIPMENT TO PROTECT YOU, it must be the right equipment for the game, position and activity; it must be worn correctly and used every time you play.)
Learn the signs and symptoms of a concussion
If you think you have a concussion:Don’t hide it. Report it. Take time to recover.
It’s better to miss one game than the whole season.For more information about concussions visit:
www.cdc/concussion www.cdc.gov/TraumaticBrainInjury www.oata.net www.ossaa.com www.nfhslearn.com
Athlete Release
To: Athletic DirectorAddress
My signature below certifies the following:
▪ I am a:______ medical doctor doctor of osteopathy licensed athletic trainer advanced registered nurse practitioner physician assistant
licensed to practice in the State of Oklahoma.
I evaluated , a student-athlete, on the following date: . This occurred after the student-athlete:
______ sustained a head injury / suspected concussion______ collapsed or fainted without sustaining a head injury
▪ If I have evaluated/treated the student athlete for a head injury, I have been trained in the evaluation and management of head concussions.
▪ It is my professional opinion, based on my training and experience, that the student-athlete named above may return to participation in the district’s athletics program on the following date: .
__________________________________________ Signature of Medical Provider Date
Athlete Health Acknowledgments
In compliance with Oklahoma Statute Sections 24-155 and 156 of Title 70, this acknowledgement form confirms that you have read and understand the Concussion/Head Injury Fact Sheet and the Sudden Cardiac Arrest Fact Sheet provided to you by the School District related to these potential adverse health conditions which may occur during participation in athletics.
I, _____________________________________________________________ (please print student-athlete’s name) as a student-athlete who participates in athletics and I, _________________________________ (please print parent/guardian’s name) as the parent/legal guardian, have read the information material provided to us by the School District related to sudden cardiac arrest and concussions and head injuries occurring during participation in athletic programs and understand the content and warnings.
_______________________________ ______________________Signature of Student-Athlete Date
________________________________ _______________________Signature of Parent/Legal Guardian Date
This form should be completed annually prior to the athlete’s first practice and/or competition and be kept on file for one year beyond the date of signature in the principal’s office or the office designated by the principal.
Ponca City School DistrictStudent Extracurricular Activities Contract
Statement of Purpose and Intent:
Participation in school sponsored extracurricular activities at the Ponca City School District is a privilege and not a right. Such privilege is governed by the attached Ponca City School District Policy on Student Possession or Use of Alcohol, Tobacco and Illegal Drugs and Participation in Extracurricular Activities (the “Policy”). Alcohol, tobacco and illegal drug use of any kind is incompatible with participation in extracurricular activities on behalf of the Ponca City School District. Students who participate in these activities are respected by the student body and are expected to hold themselves as good examples of conduct, sportsmanship and training. Accordingly, student extracurricular activity participants carry a responsibility to themselves, their fellow students, their parents and their school to set the highest possible examples of conduct, which includes avoiding the use or possession of alcohol, tobacco or illegal drugs.
Participation in Extracurricular Activities:
For the safety, health and well-being of the students of the Ponca City School District, the Ponca City School District has adopted the attached Policy and this Student Extracurricular Activities Contract (the “Contract”) which shall be read, signed and dated by the student participant, parent or custodial guardian and coach/sponsor before such student participant shall be eligible to practice or participate in any extracurricular activity. No student shall be allowed to practice or participate in any extracurricular activity unless the student has returned the properly signed Contract.
Student's Last Name First Name Middle Initial Student ID Number
I understand after having read the Policy and this Contract that, out of care for my safety and health, the Ponca City School District enforces the rules applying to the consumption or possession of alcohol, tobacco, and/or illegal drugs. As a member of a public school organization, I realize that the personal decision that I make daily in regard to the consumption or possession of alcohol, tobacco and/or illegal drugs may affect my health and well-being as well as the possible endangerment of those around me and reflect upon any organization with which I am associated. If I choose to use or possess alcohol, tobacco and/or other illegal drugs any time during the school year, I understand upon determination of that violation I will be subject to the restrictions of my participation as outlined in the Policy.
Signature of Student Date
We have read and understand the Policy and this Contract. We desire that the student named above participate in the extracurricular activity programs of the Ponca City School District and we hereby agree to abide by all provisions of the Ponca City School District's Policy.
Signature of Parent or Custodial Guardian Date
BELOW PLEASE OBTAIN THE SIGNATURES OF ALL COACHES/SPONSORS FOR EXTRACURRICULAR ACTIVITIES/TEAMS/ORGANIZATIONS IN WHICH YOU ARE INVOLVED:
Signature of Sponsor or Coach Activity/Team/Organization
Signature of Sponsor or Coach Activity/Team/Organization
Signature of Sponsor or Coach Activity/Team/Organization
Signature of Sponsor or Coach Activity/Team/Organization
PONCA CITY SCHOOL DISTRICTSTUDENT ACTIVITY RELEASE & PERMISSION FORM
Event Details
Description: Sponsor: Date: Start Time: End Time: Cost: Items to Bring: Other Info:
Transportation
School vehicles. The district will provide transportation to/from the event. All students are required to use school transportation to/from the event. The bus will leave from promptly at the start time. Students should arrive minutes in advance to check in. The bus will return as close to the end time as possible. Please arrive promptly to pick up your child from .
Volunteer vehicles. Parent volunteers will transport students to/from the event in their personal vehicles. Parent vehicles will leave from promptly at the start time. Students should arrive minutes in advance to check in. Parent vehicles will return as close to the end time as possible. Please arrive promptly to pick up your child from .
Personal transportation. All students are individually responsible for arranging and providing their own transportation to and from the event. The district is not supervising transportation in connection with this event.
Emergency Info
Contacts
Parent/Guardian: #:
Name: #:
Name: #:
Medical
My child does not have any known allergies or other health conditions. My child has the following known allergies or health conditions:
During this event my child will not need any medication. During the event my child will need medication. A completed copy of the
district’s authorization to administer medication is attached.
Permission
I give permission for my child, , to attend the event described above in accordance with the terms outlined in this form. I understand that participation in this event is voluntary and I agree to hold the district and any parent volunteers harmless from liability for their good faith acts connected with this event. In case of emergency, I authorize the event sponsor to obtain medical treatment on behalf of my child. I agree to be financially responsible for those costs.
Parent/Guardian Signature Date