hdl: still a target for therapy? paacc annual chapter meeting november 2, 2008 daniel j. rader, md...
TRANSCRIPT

HDL: Still a target for therapy?
PaACCAnnual Chapter Meeting
November 2, 2008
Daniel J. Rader, MDUniversity of Pennsylvania
School of [email protected]

Lipoproteins and Atherosclerosis
Chol
Arterial macrophage
B
LDL
Chol
Oxidation, modification, aggregation
CE

LDL goals keep going down
Grundy SM, et al. Circulation. 2004;110:227-239.
High Risk
CHD or CHD risk equivalents
(10-yr risk >20%)
LD
L-C
lev
el
100 -
160 -
130 -
190 -
Lower Risk
<2 risk factors
Moderately High Risk
≥2 risk factors
(10-yr risk 10–20%)goal
160mg/dL
goal
130mg/dL
70 -
goal
100 mg/dL
70 mg/dL*
Moderate Risk
≥2 risk factors
(10-yr risk <10%)
goal
130 mg/dL
100 mg/dL*
Previous LDL-C goals
New LDL-C goals

TNT: Stable CAD PatientsMajor Cardiovascular Events
*CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke
(HR = 0.78 95% CI 0.69, 0.89)P=0.0002
Pro
po
rtio
n o
f p
atie
nts
exp
erie
nci
ng
m
ajo
r ca
rdio
vasc
ula
r ev
ent
0
0.05
0.10
0.15
Atorvastatin 10 mg LDL 100 LDL 100
Atorvastatin 80 mg LDL 77LDL 77
0 1 2 3 4 5 6Time (years)
Relative risk
reduction = 22%
LaRosa JC, et al. N Eng J Med. 2005;352

Lipoproteins and Atherosclerosis
Chol
Arterial macrophage
B
LDL
CE
Oxidation, modification, aggregation
CE
HDL
A-I
CE


0
2
4
6
8
10
12
14
Atorva 10 Atorva 80
<40
>40-50
>50-60
>60
On treatmentHDL-C (mg/dL)
Barter et al. ACC 2006. Abstract 914-203.
Major Cardiovascular Events
%
Mean LDL-C73 mg/dL
Mean LDL-C99 mg/dL
“On-treatment” HDL-C Predicts Cardiovascular Events: TNT

Is HDL causally related to atherosclerosis and CHD risk
or simply a very good integrator and biomarker of CHD risk?

Low HDL is often accompanied by other cardiovascular risk factors
Insulin resistanceInflammationHypertensionHigh triglycerides
↑ Cardiovascular Disease
↓HDL

Low HDL is often accompanied by other cardiovascular risk factors
Insulin resistanceInflammationHypertensionHigh triglycerides
↑ Cardiovascular Disease
↓HDL
?

Hepatic expression of apoA-I reduces and even regresses atherosclerosis in mice
Liver
A-I
HDL
AdapoA-I

HDL Metabolism and Reverse Cholesterol Transport
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEFC

Quantitation of macrophage to feces reverse cholesterol transport in vivo
Plasma 3H-cholesterol,AcLDL
3H-CholBile
Feces
3H-FC
3H-chol
3H-BA
3H-BA
3H-BA 3H-FC
3H-FC

ApoA-I overexpression promotes macrophage to feces reverse cholesterol transport
Plasma 3H-cholesterol,AcLDL
3H-CholBile
Feces
3H-FC
3H-chol
3H-BA
3H-BA
3H-BA 3H-FC
3H-FC
ApoA-I adenovirus

HDL-C levels are not a marker of the rate of reverse cholesterol transport
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEFC
SR-BI HDL RCT atherosclerosis
SR-BI HDL RCT atherosclerosis
Zhang, et al, J Clin Invest, 2004

A-I
Liver
CE FCFCLCAT
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
TG
FC
ABCG1
FCLXRLXR
PPARαPPARγPPARδFC
BA
PLTP
HL, EL M
Intestine
Anti-oxidant, anti-inflammatory, anti-thrombotic, other
Targeting HDL metabolism for therapeutic reasons is complex

Clinical studies have not definitively confirmed the HDL hypothesis
• Niacin: Coronary Drug Project, HATS
• Fibrates: VA-HIT, BIP, FIELD
• ApoA-I: IVUS studies

Nicotinic Acid (Niacin)
N
C
O
OH

LDLR
apoB
TG
BVLDL
BLDL
Niacin acts on adipose to reduce FFA release and flux to liver
MTP
FFA
FFA
Niacin

Niacin receptor (GPR109A)
• Highly expressed in adipose tissue
• Mediates the anti-lipolytic effects of niacin

Adipocyte lipolysis generating FFA
ATP cAMP
AdenylateCyclase
InactiveHSL
Active HSL
PKA
FFA
FFA
TG
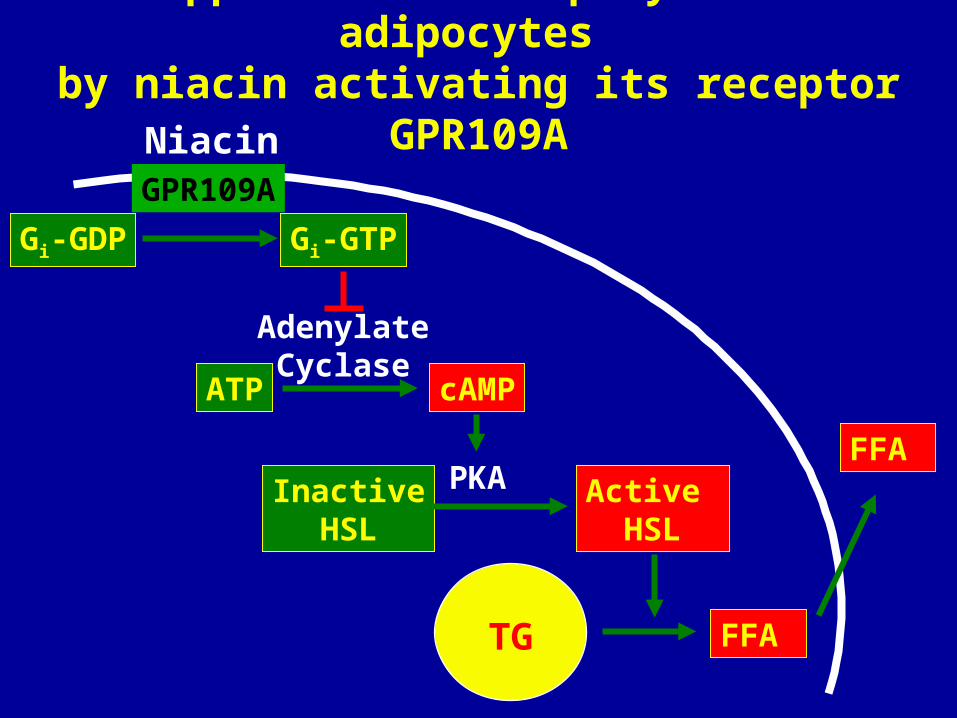
Suppression of lipolysis in adipocytes by niacin activating its receptor GPR109A
GPR109A
Gi-GDP
Niacin
Gi-GTP
ATP cAMP
AdenylateCyclase
InactiveHSL
Active HSL
PKA
FFA
FFA
TG

Niacin activates its receptor GPR109A in adipose to reduce FFA release and flux to liver
LDLR
apoB
TG
BVLDL
B LDL
MTP
FFA
FFA
Niacin
GPR109A

Mechanism of Niacin-induced Flushing
Adapted from Pike NB. J Clin Invest. 2005;115:3400-3403.
Nicotinic Acid–Induced Flush
Undesirable effects
Arachidonic acid
COX-1
EP2 or EP4
DP1
Smooth muscle cell or other
cell type
Dermal macrophages
PGE2
PGD2
PGE2
PGD2
Cutaneousvasodilation and
burning sensationon face andupper body

A-I
Liver
CE
A-I
TG
Kidney
PL
Mechanisms of niacin’s HDL raising effects?
?
Niacin

Data are needed proving that adding niacin to a statin reduces CV outcomes
to a greater extent than statin alone

Vascular Dz.Age >45 years
Atherogenic Dyslipidemia (HDL<40 or 50; TGL>149; LDL<160)
Simvastatin
Simvastatin + niaspan
3-5 yr
3300 patients from 60 sites (U.S. and Canada
CV DeathNFMIStrokeACS
AIM-HIGHStudy Overview
LDL-C target <80 mg/dl both groups (may add ezetimibe if needed)
Hypothesis-30% event rate with Simva -23% event rate with simva-nia - 50% relative reduction based on ~46% placebo rate
2 year enrollment

HPS2-THRIVE: A Randomized Trial of the Long-term Clinical Effects of Raising HDL
With Niacin and Laropiprant
THRIVE=Treatment of HDL to Reduce the Incidence of Vascular Events.
Patients aged 50-80 years with pre-existing atherosclerotic disease receiving
simvastatin 40 mg qd and, if indicated,ezetimibe/simvastatin 10/40 mg qd
N=20,000
Niacin 2 g + Laropiprant 40 mg
Placebo
Randomization
An international collaboration, with a Central Office in Oxford and 3 Regional Coordinating Centers in the UK, China and Scandinavia, will conduct the trial in about 200 hospitals
Follow-up visits at 3 and 6 months, then every 6 months thereafter
Does niacin combined with Laropiprant prevent vascular events in high-risk patients receiving intensive LDL-lowering therapy?

CETP inhibition:
the definitive test of the HDL hypothesis?

HDL Metabolism: Role of CETP
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
CE
TG
FC

CETP Deficiency is Associated with Markedly Increased HDL-C Levels
Liver
CEFCFC
LCATFC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
CE
TG
A-I
CE
FC
XX

CETP Inhibition as a Novel Strategy to Raise HDL-C
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
CE
TG
FC
X
Feces
CETP inhibitor

Treatment with the CETP inhibitor torcetrapib substantially raiseed HDL-C levels in patients with low HDL
0
10
20
30
40
50
60
70
80
90
100
Untreated 120 mg 240 mg
HD
L C
ho
les
tero
l (m
g/d
l)
Brousseau, et al. NEJM 350:1505-1515; 2004


Barter P et al. N Engl J Med 2007
ILLUMINATE: Increased mortality and major cardiovascular events in subjects randomized to
torcetrapib therapy despite favorable lipid changes
HDL 72%LDL 25%

Torcetrapib Phase III Imaging Program:Efficacy
• One coronary IVUS and two carotid IMT trials
• Torcetrapib resulted in increases in HDL-C of 50-63% and decreases in LDL-C of ~ 20%
• No significant impact on atherosclerosis progression by carotid IMT or coronary IVUS
Torcetrapib Phase III Imaging Program:Blood pressure
• Carotid IMT trial in heterozygous FH patients (RADIANCE 1): Mean BP increase 2.1 mmHg
• Carotid IMT trial in mixed hyperlipidemia (RADIANCE 2): Mean BP increase 5.1 mmHg
• Coronary IVUS study in CHD patients (ILLUSTRATE): Mean BP increase 4.6 mmHg

Is the BP increasing effect of torcetrapib
- a mechanism-based effect of CETP inhibition
-or a molecule-specific effect of torcetrapib?

Barter P et al. N Engl J Med 2007
ILLUMINATE: Increased mortality and major cardiovascular events in subjects randomized to
torcetrapib therapy

Rader D. N Engl J Med 2007
Potential Mechanisms of Adverse Outcomes Associated with Torcetrapib

Could CETP inhibition impair reverse cholesterol transport?
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
CE
TG
FC
X
Feces
CETP inhibitor

Potential beneficial effects of CETP inhibition
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
CE
TG
FC
X
Feces
CETP inhibitor
ABCG1

Increasing HDL-C levels is neither adequate nor necessary for predicting cardiovascular benefit of an HDL-targeted therapeutic approach
Improving HDL function will be the focus of new therapies
Better and standardized methods to assess HDL function will be required
HDL-targeted therapeutics in the post-torcetrapib era:
focus on HDL function

Targeting HDL: Promote Reverse Cholesterol Transport
A-I
Liver
CECE
FCFCLCAT
FC
Bile
SR-BI
A-I
ABCA1
Macrophage
CEFC

A-I
CE FCFCLCAT
SR-BI
A-I
Macrophage
CEB
LDLR
VLDL/LDL
CETP
TG
FCFCBA
Increasing lipid-poor apoA-I as an acceptor for cholesterol efflux via ABCA1
ABCA1

• ApoA-I Milano/phospholipid complexes• ApoA-I (wild-type)/PL complexes• ApoA-I mimetic peptides• Large unilamellar vesicles (LUVs)• Delipidated HDL
Increasing lipid-poor apoA-I as an acceptor for cholesterol efflux:
parenteral approaches

Increasing endogenous apoA-I production via transcriptional
enhancement
A-I
LiverIntestine
HDL

Chol
A-I ABCA1
A-I
CEABCG1
Regulation of Cholesterol Efflux in the Macrophage by LXR
LXR

Chol
A-I ABCA1
A-I
CEABCG1
LXR
Agonist
Pharmacologic Promotion of Pharmacologic Promotion of Macrophage Cholesterol Efflux by Macrophage Cholesterol Efflux by
Synthetic LXR AgonistsSynthetic LXR Agonists

% C
PM
In
ject
ed
The LXR agonist GW3965 significantly The LXR agonist GW3965 significantly increased macrophage to feces reverse increased macrophage to feces reverse
cholesterol transport in vivocholesterol transport in vivo
0.0
0.5
1.0
1.5
2.0
2.5
*
Control LXR agonistNaik, et al, Circulation 2005

LDLR
apoB
TG
BVLDL
BLDL
LXR agonists can cause steatosis, hypertriglyceridemia, and elevated LDL-C
MTP
LXR
SREBP1c
TG

TGLipase
LPL HL EL
Phospholipase
TG-rich lipoproteins HDL
Endothelial Lipase: a member of the lipoprotein lipase gene family
Jaye M, et al, Nature Genetics 21:424; 1999

A-I
Liver
CECE
FC
Bile
SR-BI
A-I
TG
Kidney
PL
EL
Endothelial lipase promotes catabolism of apoA-I and reduces HDL levels

Endothelial lipase is upregulated by inflammation in metabolic syndrome
and mediates low HDL-C levels
Cytokines
↓HDL
↑EL

Mutations in endothelial lipase cause high HDL
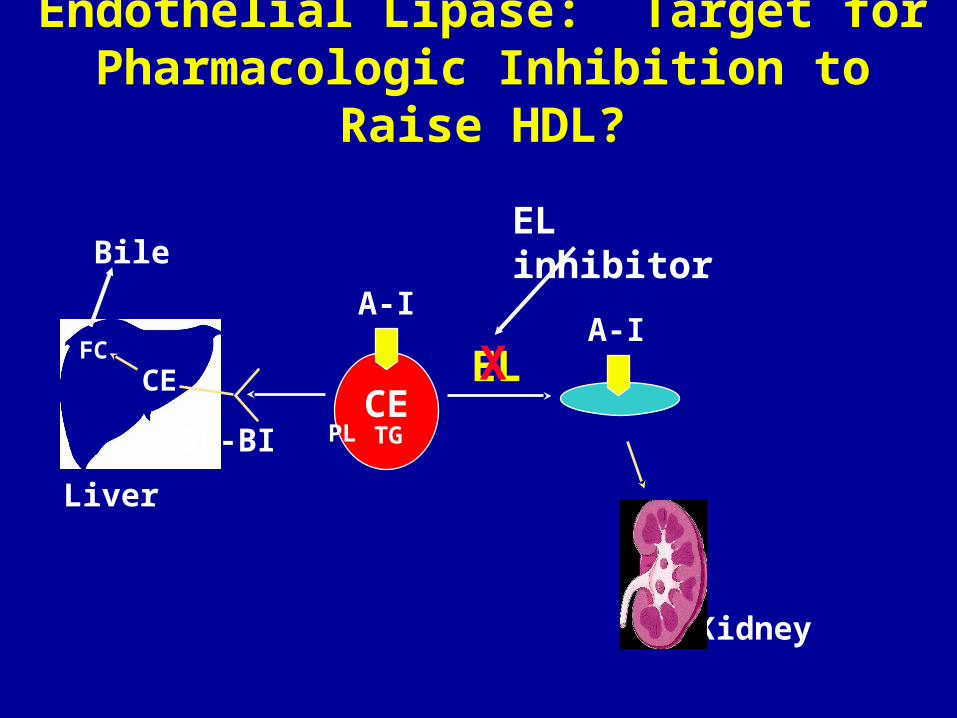
A-I
Liver
CECE
FC
Bile
SR-BI
A-I
Endothelial Lipase: Target for Pharmacologic Inhibition to Raise HDL?
TG
Kidney
PL
EL
EL inhibitor
X

A-I
Liver
CE FCFCLCAT
SR-BI
A-I
ABCA1
Macrophage
CEB
LDLR
VLDL/LDL
CETP
TG
FC
ABCG1
FCLXRLXR
PPARαPPARγPPARδFC
BA
PLTP
HL, EL M
Intestine
Anti-oxidant, anti-inflammatory, anti-thrombotic, other
Targeting HDL metabolism for therapeutic reasons is complex