health system and its financial aspects nouf aloudah, m.s clinical pharmacy lecturer king saud...
Post on 21-Dec-2015
214 views
TRANSCRIPT
Health System And its Financial Aspects
Nouf Aloudah, M.SClinical Pharmacy Lecturer
King Saud University

Health system
A health system comprises all organizations, institutions and resources devoted to producing actions whose primary intent is to improve health.
Most national health systems include public, private, traditional and informal sectors. The four essential functions of a health system have been defined as service provision, resource generation, financing and stewardship

لعالمية الصحة منظمةWHO
الصحي؟ • النظام هو ماالرامية • والموارد والمؤسسات المنظمات مجموع هو الصحي النظام
. وأموال موظفين إلى النظام ذلك ويحتاج الصحة تحسين إلى ) أساسا . وال عامة واتجاهات وتوجيهات واتصال نقل ووسائل وإمدادات ومعلوماتمنصفة بأسعار القائمة االحتياجات 7ي تلّب خدمات توفير من النظام لذلك بد
. الئق نحو الناسعلى معاملة إلى ذاته، الوقت في والسعي،الناسبشكل • حياة تحسين في يسهم الذي ذلك هو الجيد الصحي والنظام
. تمنيع بضرورة 7رها تذّك رسالة تتلقى التي فاألم يوم بعد ) يوما ملموسنظام من الواقع في تستفيد هي حياته يتهد7د مرض ضد الصغير طفلها
مياه. على الحصول ) أخيرا وسعها في أسرة على ) أيضا ذلك وينطّبق صحي ) مشروعا مو7لت الحكومة ألّن7 قريتها بالغرضفي وافية مضخة من نقيةيستفيد بفيروسه والعدوى األيدز متعايشمع شخص على أو (؛ إصحاحيا. التكلفة ميسورة عيادة في منتظمة وفحوص غذائية نصائح و أدوية من

لعالمية الصحة منظمةWHO
•) تكملة ) الصحي؟ النظام هو ماالصحي • للنظام اإلجمالي األداء يخص فيما األولى المسؤولية وتقع
مستوى على 7د الجي اإلشراف أّن7 غير الحكومة، عاتق على الوطنيمن ّكذلك ي̀عد الصحية المؤسسات وفرادى والّبلديات المناطق
. األهمية الحاسمة األمورمن • ) إنصافا أّكثر وجعلها الصحية الن̀ظم تعزيز بأّن7 االعتراف وتم
. التنمية وتعزيز الفقر لمكافحة األساسية االستراتيجياتالّبلداّن • في محصورة ليست الصحية بالن̀ظم المرتّبطة والمشاّكل
ال. واسعة سكانية فئات الغنية الّبلداّن بعض في فهناك الفقيرةالخاصة المنصفة غير الترتيّبات بسّبب الرعاية خدمات من تستفيد
. تغطية أجل من تكافح أخرى فئات وهناك االجتماعية بالحماية. فعال غير نحو على الموارد استخدام بسّبب الخدمات تلك تكاليف
Spending On Health
• Total global expenditure for health US$ 4.1 trillion • Total global expenditure for health per person per year:
US$ 639• Country with highest total spending per person per year on
health: United States (US$ 6103) • Country with lowest total spending per person per year on
health: Burundi (US$ 2.90) • Country with highest government spending per person per
year on health: Norway (US$ 4508) • Country with lowest government spending per person per
year on health: Burundi (US$ 0.70) • WHO estimate of minimum spending per person per year
needed to provide basic, life-saving services: US$35 to US$50

WHO And Health System Financing
• WHO works with countries to devise ways of raising more funds for health equitably, to use the available funds efficiently, and to monitor the use of funds. It works with the international community to try to raise more, and more predictable funds for health.
• Many countries need to use available funds more efficiently and raise more funds from domestic sources, but these measures would be insufficient to fill the current gap in the poorest countries. Only an increased and predictable flow of donor funding will allow them to meet basic health needs in the short to medium term.
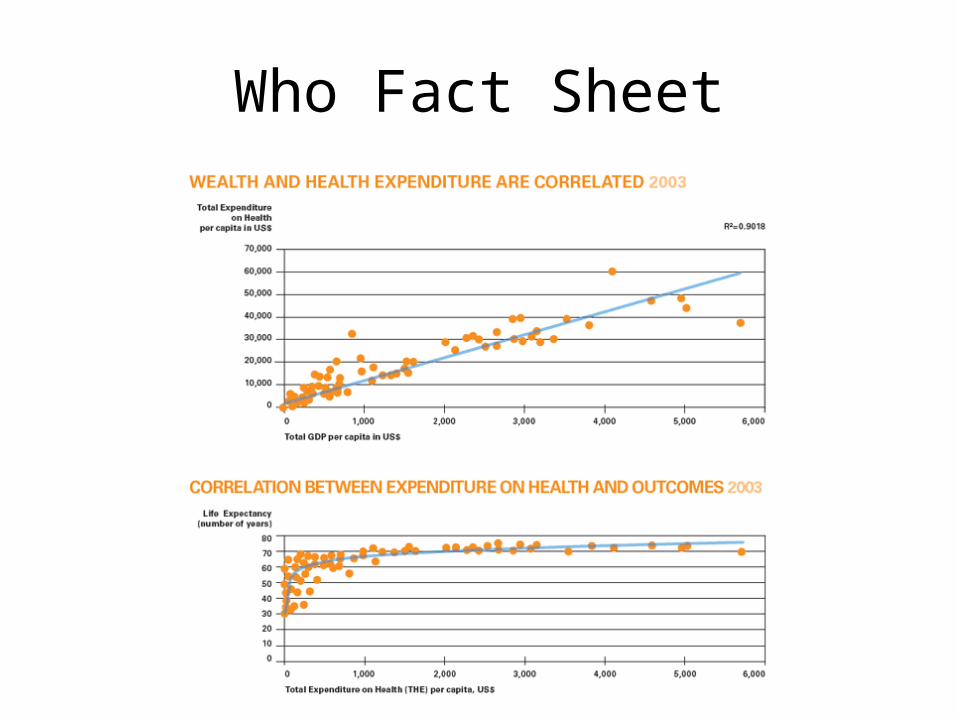
Who Fact Sheet
Paying For Health Services
• In most low-income countries, people pay a high proportion of their health costs directly to health care providers out of their own pockets. In 47 countries, out-of-pocket payments represent more than half of total health expenditures.

Paying For Health Services (cont)
• In most of the world’s wealthiest countries, individuals pay little out of pocket. In Germany, for example, where the GDP is $32,860 per capita, 11.3 percent of all medical expenses nationwide are borne by households and the rest by social health insurance or by the government. In the Democratic Republic of the Congo, by contrast, where GDP per capita is only $120, about 90% of the money spent on the health system is paid directly by households to providers.
Paying For Health Services (cont)
• High out-of-pocket payments for health care can have a variety of harmful effects. Some people are deterred from using health services or from continuing treatment because they cannot afford to pay. People who use services may need to cut spending on basic needs such as food, clothing, housing and children's education to meet health costs. Each year, approximately 150 million people experience financial catastrophe, meaning they are obliged to spend on health care more than 40 percent of the income available to them after meeting their basic needs. An additional 100 million people are driven below the poverty line

Paying For Health Services (cont)
• The best approach is to develop a system through which people contribute to the health system before they are ill - through taxes, some form of insurance or some mix - then draw on services funded by these sources when they are ill rather than paying out of pocket for them. In general, the greater the extent of prepayment in overall health financing, the more are households protected from financial catastrophe and impoverishment.

Paying For Health Services (cont)
• Estimates of how much is required to provide a basic package of health services vary from somewhere around $30 per person per year, up to $50. A recent paper suggested that low- and middle-income countries, governments and individuals would have to jointly contribute US$ 341 per person per year for essential preventive and curative services. US$ 11 to $25 would have to come from international donors

Paying For Health Services (cont)
• WHO works with countries to help identify ways of moving away from a heavy reliance on out-of-pocket payments to prepayment. It provides information on best practices and technical support to countries engaged in this process. It also works with the international community to encourage help for recipient countries in developing and strengthening financial institutions and capacities that will allow prepayment mechanisms to be successful

Social Health Protection
• There are different approaches to social health protection, but all have one thing in common: they create a system, called a risk pool, that allows a large group of people to share the risk that they may become ill and need expensive care. That means funds dedicated for healthcare are collected through prepayment, and managed in such a way as to ensure that the risk of having to pay for healthcare is borne by all the members of a pool and not by each contributor individually. In a risk pool, at any given time healthy people, who are in need of limited healthcare, are subsidizing the sick, who must draw more heavily on available health resources.

categories of social health protection systems
• Tax-funded health financing. In this type of system a government makes use of general tax revenue to finance healthcare. All citizens (and sometimes residents) are entitled to services.
• Social health insurance. With this second approach, contributions targeted specifically for healthcare are collected from workers, self-employed people, enterprises and the government. These monies are pooled into a social health insurance fund or funds. Universal coverage can be achieved with this type of financing scheme only if contributions are made on behalf of each member of the population. For this reason most social health insurance schemes combine different sources of funds, with the government often contributing on behalf of people who cannot afford to pay themselves.
• Mixed systems. In some countries, part of the population is covered directly through general taxes, while others are required to make contributions to a social health insurance fund or another type of health insurance, which may be private.


Migration Of Health Workers
• Health workers are all people whose main activities are aimed at enhancing health. They include the people who provide health services -- such as doctors, nurses, pharmacists, laboratory technicians -- and management and support workers such as financial officers, cooks, drivers and cleaners. Worldwide, there are 59.8 million health workers. About two-thirds of them (39.5 million) provide health services; the other one-third (19.8 million) are management and support workers. Without them, prevention and treatment of disease and advances in health care cannot reach those in need

Migration Of Health Workers
• Workers tend to go where the working conditions are best. Income is an important motivation for migration, but not the only one. Other reasons include better working conditions, more job satisfaction, career opportunities and the quality of management and governance. Political instability, war, and the threat of violence in the workplace also are strong drivers in many countries.
• Migration is often stepwise. People sometimes move from the poorest regions to richer cities within a country and then to high-income countries. In most countries, there is also movement from the public to the private sector, particularly if there are considerable differences in income levels.

Migration Of Health Workers
• Globalization certainly has helped to drive migration abroad. At the same time, demand for health workers has increased in high-income countries because wealthy countries are not producing enough health workers locally and their existing workforce is ageing; yet there is a growing need for health care because of the ageing of populations and the rise of chronic illnesses like diabetes and heart disease. Another stimulus to migration is the growth of professional recruitment agencies.

Migration Of Health Workers
• In a number of middle-income countries with good medical education systems--such as Fiji, Jamaica, Mauritius and the Philippines--a significant proportion of students, especially in nursing school, enter their education with the intention of migrating, usually in search of a good income. Some countries, notably the Philippines, are seeking to capitalize on the demand for imported health workers by deliberately producing graduates for international export.
Impact Of Migration
• The movement of health workers abroad has positive features. Each year, migration generates billions of dollars in remittances (the money sent back to home countries by migrants) to low-income countries and has therefore been associated with a decline in poverty. Health workers also may return, bringing significant skills and expertise back to their home countries.
• Nonetheless, when significant numbers of doctors and nurses leave, the countries that financed their education lose a return on their investment and become unwilling donors to the wealthy countries to which their health personnel have migrated.

Impact Of Migration
• Financial loss is not the most damaging outcome, however. When a country has a fragile health system, the loss of its workforce can bring the whole system close to collapse, with the consequences measured in lives lost. In these circumstances, the calculus of international migration shifts from brain drain/gain to "fatal flows."
• Health systems in a number of industrialized countries depend heavily on doctors and nurses who have been trained abroad. English-speaking countries draw the lion's share of health workers from overseas. In Canada, New Zealand, the United Kingdom and the United States, a quarter or more of all physicians have been imported from other countries.

Impact Of Migration
• On average one in four doctors and one nurse in 20 trained in Africa is working in OECD countries. Some countries have been hit harder than others. For example, 29% of Ghana’s physicians are working abroad, as are 34% of Zimbabwean nurses.
• What is OECD?

Reasons For Migration

Global Health Workers Shortage
• Health workers are all people whose main activities are aimed at enhancing health. They include the people who provide health services -- such as doctors, nurses, pharmacists, laboratory technicians -- and management and support workers such as financial officers, cooks, drivers and cleaners. Worldwide, there are 59.8 million health workers. About two-thirds of them (39.5 million) provide health services; the other one-third (19.8 million) are management and support workers. Without them, prevention and treatment of disease and advances in health care cannot reach those in need

Extent of the shortage and its consequences
• Fifty-seven countries, most of them in Africa and Asia, face a severe health workforce crisis. WHO estimates that at least 2 360 000 health service providers and 1 890 000 management support workers, or a total of 4 250 000 health workers, are needed to fill the gap. Without prompt action, the shortage will worsen.
• Health workers are inequitably distributed throughout the world, with severe imbalances between developed and developing countries. This global workforce shortage is made even worse by imbalances within countries. In general, there is a lack of adequate staff in rural areas compared to cities.

Extent of the shortage and its consequences
• Sub-Saharan Africa faces the greatest challenges. While it has 11 percent of the world's population and 24 percent of the global burden of disease, it has only 3 percent of the world's health workers.
• There is a direct relationship between the ratio of health workers to population and survival of women during childbirth and children in early infancy. As the number of health workers declines, survival declines proportionately.

World Distribution Of Health Workers

Health Workers Shortage

What is needed?
• A threat to global health• Outbreaks• Natural disasters• Conflicts• Care of aging populationWhat is needed?

•
Tackling the crises
more direct investment in the training and support of health workers
• Initial funds will be for training more health workers. As they graduate and enter the workforce, more funds will be needed to pay their salaries. To educate and pay the salaries of the four million health workers needed in the 57 countries with severe shortages, health budgets will have to increase at least US$ 10 per person per year by the year 2025. To meet that target within 20 years is an ambitious but reasonable goal.

National plan for the health work force and an increase in the number of health workers in all countries with serious shortages
• That will take political leadership, a comprehensive plan for an effective health workforce, and commitment of the necessary funds. Funding must not only cover health service providers, but also the management and support workers who provide crucial services to the health system. Governments also need to invest in training existing health workers, to keep them up to date with changing priorities.

More efficient use of the existing health work force
• Simple, inexpensive measures like improving management and supervision and writing clear job descriptions would help. Another helpful strategy is "piggy-backed" services -- meaning that workers delivering one specific service, such as a vaccine during an immunization campaign, can simultaneously deliver others, such as a needed dose of vitamins.

Some simple health care tasks now assigned to highly skilled personnel delegated to less skilled workers able to deliver them competently
• With sufficient supervision and support, volunteers, community health workers and workers, with limited training can improve efficiency of health services.

Protection and fairer treatment of health
• They face difficult and often dangerous working conditions and poor pay in many developing countries

Access to effective prevention and treatment for all health workers
• H I V has disproportionately affected health workers in many countries. It is vital that they receive these services under confidential conditions.

Encouragement of women to enter health professions
• Their needs should be accommodated through flexible work arrangements and leadership career tracks adapted to family life.

Decreased incentives for early retirement
• Countries with serious shortages also should provide opportunities for retirees to go back to work.
السعودية في الصحي النظام
هـ 1423•

الصحي الضماّن نظلم
هـ 1420

الخاصة الصحية المؤسسات نظام
هـ 1423•

الصحية المهن مزاولة نظلم
هـ1426•

Health System And its Financial Aspects
• Definition– Access– Diagnostic related groups– Delivery– E prescribing– Health care facilities– Health literacy– Managed care
Health System And its Financial Aspects
• Definition– Multidisciplinary– National health care– Price– Reimbursement– Utilization– Utilization review

Health System And its Financial Aspects
• Background– Historical overview of us health care system and
evolution of care services– Health care from civil war to early 1900s– Attempts at national health care– Health care statistics– Public perception of the health car system

Health System And its Financial Aspects
• Access of health care personnel– Distribution of health care personnel– Distribution of facilities

Health System And its Financial Aspects
• Delivery of health care– Managed care– Quality of care/ interdisciplinary teams

Health System And its Financial Aspects
• Utilization of health care– Patient population– Health literacy– Chronic disease management

Health System And its Financial Aspects
• Price and reimbursement of health care– Other cost containment mechanisms– Pharmacist reimbursement– Medicare modernization ACT/MEDICAID

Health System And its Financial Aspects
• Legislative and regulatory changed– Technology advancement– Hints on how to monitor legislative and regulatory
changes

Health System And its Financial Aspects
• summery

Health System And its Financial Aspects
References• World health organization www.who.int • www. ncda.gov.sa المحفوظات و للوثائق الوطني المرّكز