hematopoietic stem cell transplantation for sickle cell...
TRANSCRIPT

Hematopoietic stem cell
transplantation for sickle cell
disease
Hazza Al-zahrani
KFSHRC-Riyadh

SCD major Health Burden in KSA
• endemic in southern and eastern
• prevalence remains higher than that in other countries
- Per 10,000 population
• East prov. 145 cases
• South 24 cases
• Western 12 cases
• central 6 cases Al-Qurashi Saudi Med J 2008
• SCD trait carriers: 2–27% of the population of KSA
Jastaniah Ann Saudi Med 2011

Challenges in Controlling SCD in Saudi Arabia
consanguineous marriages (57.7%->80% )
• How to overcome this issue?
- Awareness programs:
• Education of people regarding the effects of consanguineous marriages
- Premarital Screening Program and the Genetic Counseling Program
• mandatory for all couples
• free at all government facilities
• Results:
• Adult 4.2% carriers
• 0.26% of the population is affected by SCD
• reduced the number of voluntary cancelations of at-risk marriage
proposals by 60%
• increased by 5-fold over 6 years
Memish Six-year outcome of the national
premarital screening and genetic
counseling program for sickle cell disease
and b thalassemia in Saudi Arabia Ann
Saudi Med (2011)
Ann Saudi Med 2011



Disability-Adjusted Life Year (DALY)
One DALY
one lost year of "healthy" life
Sum: measurement of the gap between current health status and an ideal
health situation where the entire population lives to an advanced age, free of
disease and disability.
Feb 2017 Journal of Epidemiology and Global Health M Alosaimi

Feb 2017 Journal of Epidemiology and Global Health M Alosaimi

KFSHRC Experience:
• SCD adults have many comorbidities
- Many are ineligible to full intensity Conditioning
- Repeated transfusion + chr Inflam. Rejection risk
• Intensifying conditioning loose the patient
• Reducing conditioning loose the graft
• Anything in the middle medium size results
Background-Challenges

Hypothesis:
SCD is a chronic inflammatory
Needs Anti-inflammatory
induction before BMT Needs MAC or close to MAC to
prevent relapse
Hypothesis:
SCD is a stem cell disease
Adults with Tx-dependent SCA
may be alloimmunized
Adults with high Risk SCA
cannot tolerate MAC
Pre-BMT Steroids
ATG with conditioning
Reduced Toxicity Condtioning
“RTC)

AIM OF THE STUDY: assess safety & efficacy of
1. Pre-conditioning: Steroids+ HU & HyperTransfusion
2. Reduced Toxicity Conditioning : FLA, iv-Bu + LD-ATG
in young adults with Sickle Cell Anemia (SCA).
Patient population :
• Adolescents and Adults (>14 years)
• Sickle Cell Anemia

Indications for Transplantation 1. Recurrent severe VOC
2. Recurrent ACS
3. Stroke (none-debilitating)
4. AVN
5. Tx-dependence
6. Pulm . HTN (Mod)

Eligibility for Transplantation 1. The presence of matched Sib or EF-
donor
2. Age > 14
3. Performance: (KPS <=2 ; ECOG >70%)
4. NO Chr. active hepatitis due to HBV/HCV
5. NO HIV/AIDS
6. Consent


SCD SCT at KFSHRC
Patients
• Started 2011
• 38 cases of high risk SCD
- 5 cases per year
- Age: 14-35 yrs
- Median age 17 years
- Comorbidities
• Non : 26%
• 1 patient had also smoldering Myeloma

Patients: Indications of HSCT
• Recurrent severe VOC (n:25; 100%)
• Acute chest syndrome (n: 10; 40% )
• stroke or silent brain insult (8; 32% )
including Moya Moya (2; 8%)
• AVN (n; 8; 32%)
• Moderately severe (O2-dependent)
pulmonary HTN in 1 patient

Sex distribution of the 39 donors Sex distribution of the 39 patients
56% females and 44% males
Donor and Recipient Sex

91.2
5.9
2.9
ABO Compatibility
Compatible
Minor
Major

Donors
• HLA-matching was 10/10 in all pairs (100%)
• 8 donors (32%) SCA trait
• Identical siblings (20 BM, 4 PB and 1 BM+PB)
• CD34+ cell dose
- 4.7 x106/kg (2.7-7.81 ) for Marrow
- 7 x106/kg for the peripheral blood

Comorbidities
score 0 score 1 score 2 score 3 score 4
Score 0
Score 1 Score 2
Score 3
Score 4
https://qxmd.com/calculate/calculator_108/hematopoietic-cell-transplantation-specific-comorbidity-index-hct-ci

Comorbidities
https://qxmd.com/calculate/calculator_108/hematopoietic-cell-transplantation-specific-comorbidity-index-hct-ci

• Conditioning
- IVBU14/FLU/ATG
- Gvhd PROPHYLAXIS :
• MTX +CSA
• Stem cell dose average 6.12 X106/Kg
- 3.2-8 X106/Kg
• Jan 2011\till Jan 2018
• 3 required boost and 3 required DLI
SCD SCT at KFSHRC

MAC
CSA CSA
HIT+RTC
TRM
TRT
GVHD !
• Less/No delay
• Less/No crisis
• Less TRT
• No TRM
• Less Rejection &
• Less GVHD
• Well Being !!!!
• Outpatient BMT ?
• Fertility: Better ?
Change of paradigm of Conditioning
H. I. T.
RTC

Total WBC during pre-conditioning
phase
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9
To
tal W
BC
(x
10^
9/L
)
-8 week -6week -4week -2week

ALLOGENEIC PROGENITOR STEM CELL TRANSPLANT
PROGRAM
ADULT HEMATOLOGY/ BMT UNIT
DATE 1 Feb
2015
2 Feb
2015
3 Feb
2015
4 Feb
2015
5 Feb
2015
6 Feb
2015
7 Feb
2015
8 Feb
2015
9 Feb
2015
10 Feb
2015
11 Feb
2015
Days Mon Tue Wed Thurs Fri Sat Sun Mon Tue Wed Thurs
BMT/PBSCT DAY -10 -9 -8 -7 -6 -5 -4 -3 -2 -1 0
FLUDARA 40mg/m2
x x x x
IV-
BUSULFAN 0.8 mg/kg q6hx
14 doses
4 doses
4 doses
4 doses
2 . Doses
.
ATG Thymoglobulin; Genzyme
1.5 mg/kg
x x x
PHENYTOIN
X X X X X X
“Keppra”
Levetiracetam x
Rest Day
X
HSCT
X
SICKLE CELL-BMT IV-BUSULFAN/FLUDARABINE and ATG o HEIGHT: _________cm WEIGHT: _________kg BSA: _________
o ALLERGIES: _________
o NOTE: This regimen is for the exclusive use for Sickle Cell Conditioning.
ALLOGENEIC PROGENITOR STEM CELL TRANSPLANT PROGRAM ADULT HEMATOLOGY/ BMT UNIT- KFSHRC, Riyadh, SA
160 mg/m2
11.2 mg/kg
4.5 mg/kg
.

Engreftment
• Granulocytes
- Median day 19
• Platelets
- Median day 20

Figure 1A. Kinetics of Neutrophil drop and engraftment after RTC-conditioning for Allo-sib
HSCT in adults with severe SCA .
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
d0 d2 d+4 d+6 d+8 d+10d+12d+14d+16d+18d+20d+22d+24d+26d+28
Ne
utr
op
hil c
ou
nt/
ul

Figure 1B. Kinetics of platelet drop and engraftment after RTC conditioning for
Allo-sib HSCT adults with severe SCA (n=21)
0
50
100
150
200
250
300
350
400
450
500
d0 d2 d+4 d+6 d+8 d+10 d+12 d+14 d+16 d+18 d+20 d22 d+24 d+26 d+28 d+30
Pla
tele
t c
ou
nt
(x1000/u
l)
Complications of SCT in SCD
KFSHRC experience
• Fungal infections
- 11%
• Varicella zoster Infection:
- 14.7%
• CMV pcr detection:
- 70% pre-emptively treated
- 0% CMV disease

Peri-transplant complications
• Mucositis
- grade I in 6 (24)%
- grade II in 2 (8) %
- Grade III in 2( 8)%)
• one (4%) patient bled due to gastritis and possible pulmonary invasive fungal disease in one (4)
• New minor stroke with monoparesis in a patient with Moya Moya disease that recovered in a few days
• One patient developed severe hypertension
• PRESS in 2 patients, fits in 3 patients
- one other patient developed PRES-like syndrome at Hb S of 32% treated and recovered after exchange transfusion.
• TMA in 1 patient treated with Fresh frozen plasma infusion, fits with change level of consciousness in one treated with Exchange transfusion and resolved within a few hours,
Mohamed S.Y, 2017

Complications of SCT in SCD
KFSHRC experience
• Mucositis:
- 70%
• Hemorrhagic cystitis :
- 1 patient 2.9%
• Veno-occlusive Disease of the liver
1 patient 2.9%

SCD SCT KFSHRC
Acute GVHD
70% are grade I-II
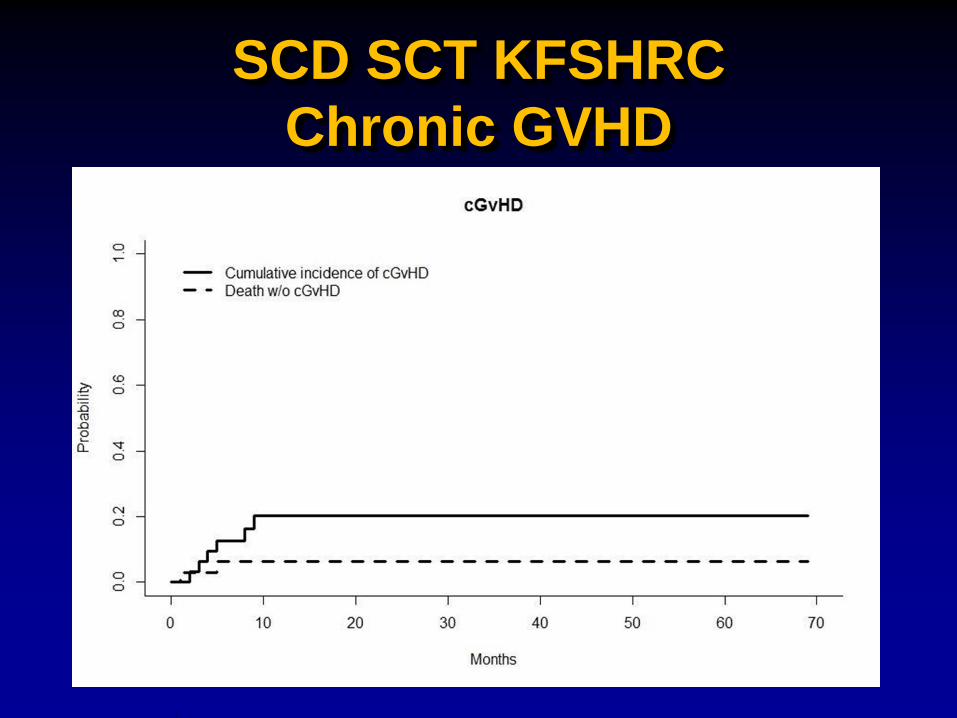
SCD SCT KFSHRC
Chronic GVHD

Graft Stability
Boost 3
DLI 3


Boost+DLI Boost+DLI
Fig 2. Kinetics of Myeloid (M) and lymphoid (L) Chimerism after RTC conditioning for Allo-Sib HSCT in adults with severe SCA
N:1
8

0
20
40
60
80
100
120
1 Mo 2Mo 3Mo 4mo 6Mo 1Y 15 mo 18mo 21 mo 24mo 30 mo

0
20
40
60
80
100
120 Cyclosporine


1980s-2007 SCA transplant
experience
Study US
collaborati
ve
French Belgian CIBMTR
n 59 87 50 67
Median age
(y) 9.9 9.5 7.5 10
EFS 85 85 86 82
GVHD 12 12.6 20 22
Horan JT et al., 2005
Bernaudin F et al., 2007
Krishnamurti m et al.,2007
Angelucci E et al.,2009

Pre- HU & pre BMT fertility preservation
HU naïve (pre –HU) On HU & pre BMT
Semen analysis (SA)
optimal Suboptimal Suboptimal optimal
Exchange
Hold HU
Qmo SA
Up to 6moif if
improving
Collect
Resume HU
Transfuse
or
Exchange
qMo SA
Up to 3 mo
Collect
Start HU

1Death
• 16-year-old male SCD
• History of TB lymphadenitis and he completed ant tuberculous therapy June 2016
• post neurosurgery for Moya-Moya
• Dec 2016 AlloSCT well for 4 months
• Secondary graft failure, S/P Stem cell boost on March 30th & 31st
• septic shock ARDS
• Medivac transfer
- Severe sepsis, septic shock
- Acute respiratory failure, ARDS
- Bilateral pneumothoraces
- CNS hemorrhage
- HLH
- Chronic hypernatremia

Af. Fi. 16 year old girl SCD
Acute chest syndrome mechanical ventilator subglottic stenosis
Laparoscopic cholecystectomy
Tonsillectomy
History of recurrent chest infection, community-acquired pneumonia
hydroxyurea 6 tables
History of pancytopenia secondary to hydroxyurea overdose
Frequent admission
History of AVN of Rt shoulder
11 January 2011 for allogenic sibling SCT
The donor: 3-year-old sister ABO incomp. (AO)
pre-implantation genetic diagnosis for selection





Conclusion
HSCT remains the only curative therapy for SCD
HLA-identical sibling transplantation in patients with SCD
offers excellent overall and disease free survival
Risk of GVHD, infections, infertility, and other long-term
transplant complications, limits widespread use of SCT but our
results are relatively low toxicity allowing SCT in patients with
significant morbidity
Post SCT cyclophosphamide is being explored at our
center
graft failure rate was low and manageable with boost and DLI
long-term follow up is needed
