hep b and c: updates and resources john scott, md, msc asilomar aetc conference october 6, 2006
Post on 20-Dec-2015
215 views
TRANSCRIPT

Hep B and C: Updates and Resources
John Scott, MD, MSc
Asilomar AETC Conference
October 6, 2006

Outline
• Hepatitis C– Background & natural history – Treatment of Hep C/HIV coinfection
• New drugs• Guidelines and Internet resources
• Hepatitis B– Natural history w/ and w/o HIV– Treatment of Hep B monoinfection– Treatment of Hep B/HIV coinfection
• New drugs• Guidelines and Internet resources

Biology
• ss RNA virus• RNA-dependent RNA
polymerase, lacks proofreading function
• Flaviviridae• 6 genotypes, type 1
accounts for 70% of infections in US, types 2,3 account for rest
• No easy culture system!
www.hepcprimer.com/3dmodel.html






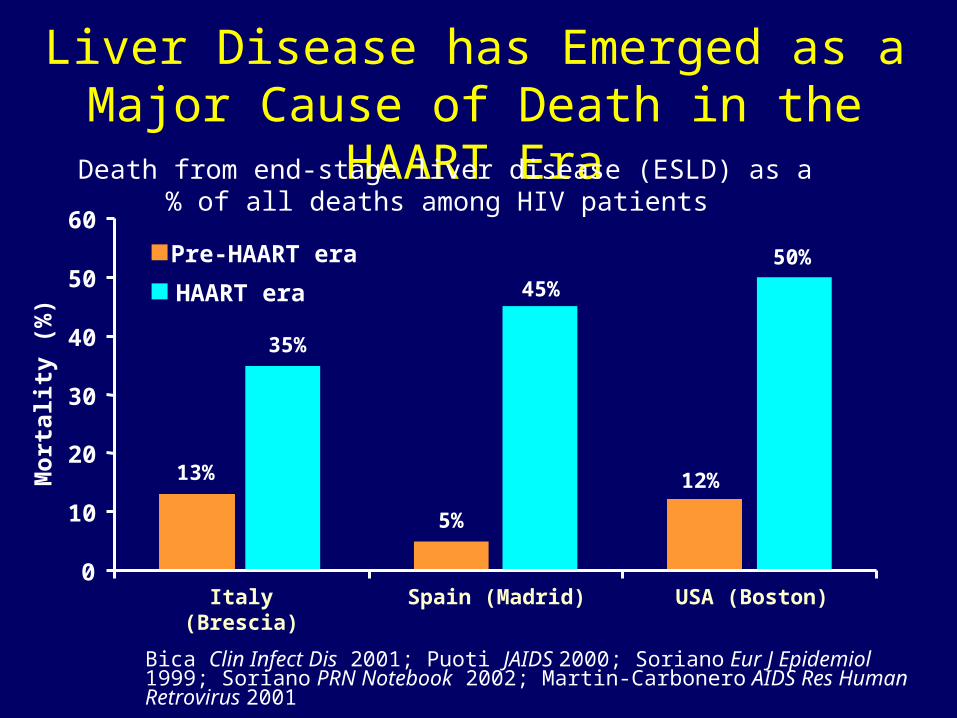
Liver Disease has Emerged as a Major Cause of Death in the HAART Era
Bica Clin Infect Dis 2001; Puoti JAIDS 2000; Soriano Eur J Epidemiol 1999; Soriano PRN Notebook 2002; Martin-Carbonero AIDS Res Human Retrovirus 2001
0
10
20
30
40
50
60
Mo
rtal
ity
(%)
Death from end-stage liver disease (ESLD) as a% of all deaths among HIV patients
Italy (Brescia) Spain (Madrid) USA (Boston)
13%
35%
5%
12%
45%
50%Pre-HAART era
HAART era

Impact of HIV on HCV
Cirrhosis Decompensation
Makris
Soto
Pol
Benhamou
Combined
0.76 1.0 2.07 10.83
Eyster
Telfer
Makris
Lesens
Combined
0.61 1.0 6.14 175.32
Graham CID 2001Relative Risk (95% CI)
A B

AASLD Guidelines
• Anti-HCV testing on all HIV+ pts• HCV RNA to confirm Ab+ and all Ab- w/
unexplained liver disease• Treat HIV/HCV patients in whom likelihood of
serious liver dz and tx response outweigh the side effects of tx
• PegIFN-alfa + ribavirin x 48 wks• Closely monitor pts on therapy• Use RVN carefully in pts on AZT or d4T. Avoid
RVN and ddI• Decompensated liver dz -> liver transplant eval
Strader D. Hepatology 2004.
Workup
• H&P: date HCV diagnosed, risk factors, earliest exposure, signs and symptoms of hepatitis and cirrhosis, alcohol hx, prior treatment and response
• Candidate for tx: depression, poorly controlled DM, CAD, cytopenias, autoimmune dz, pregnant
• EIA (TPR>99%, TNR=99%)• If EIA+, sensitive PCR assay• LFTs, CBC, chem 7, TSH, hepatitis serologies, CD4 and
HIV RNA, pregnancy test, eye exam, utox?• If treatment contemplated, then HCV genotype and viral
load, +/- liver biopsy
Liver Biopsy
• Currently the best way to determine how much scarring is present, but imperfect
• Needle, local anesthetic
• Risks: bleeding
• Scar Stages: 0-1-2-3-4 (Batts-Ludwig)
• VA guidelines recommend bx for all patients

Progression of Fibrosis on BiopsyProgression of Fibrosis on Biopsy
No FibrosisNo Fibrosis
Stage 1: Fibrous Stage 1: Fibrous expansion of expansion of some portalsome portal areasareas
Stage 3: Stage 3: Fibrous Fibrous expansion of expansion of most portal most portal areas areas with occasional with occasional portal to portal portal to portal bridgingbridging
StageStage 4: Fibrous 4: Fibrous expansion of expansion of portal areas with portal areas with marked bridging marked bridging (portal to portal (portal to portal and portal to and portal to central)central)
Stage 4: CirrhosisStage 4: Cirrhosis
Cirrhotic liver: Cirrhotic liver: Gross anatomy Gross anatomy of cadaverof cadaver
Courtesy of Gregory Everson, MD.Courtesy of Gregory Everson, MD.

• ACTG 5071 (Chung RT, NEJM 2004; 351:451-9)
• RIBAVIC (Carrat F, JAMA 2004; 292:2839-48)
• APRICOT (Torriani F, NEJM 2004: 351:438-50)
– All compared standard with pegylated IFN– All treated for 48 weeks, regardless of
genotype– All used low-dose RBV (avg dose 800 mg/d)
• Laguno et al (AIDS 2004: 18:27-36).
– Higher dose RBV, 24 weeks for GT2 or 3
Prospective, Randomized Multicenter Trials of Pegylated Interferons in
HIV/HCV

HIV/HCV Coinfection TrialsACTG RIBAVIC APRICOT Laguno
# pts 134 412 860 95
% genotype 1 78% 66% 61% 49%
fibrosis score 2.5 2.3 16% cirrhotic 30% st 3 or 4
Mean CD4 475 515 530 560
Overall SVR 27% 26% 40% 44%
SVR GT 1 5% 15% 29% 38%
SVR non-1 30% 43% 62% 53%
d/c rate (ea arm)
12% 42% 30-40% 17%

Side Effects of PegIFN/Ribavirin
• Depression ranging from mild to suicidality• Irritability, aggressive behavior• Worsening of mania• Fatigue• Insomnia• Myalgias, fever, flu-like symptoms• Hair loss• Cytopenias“Interferon Man”

0
1
2
3
4
5
6
7
8
0 1 2 3 4 12 24 48 72
Time (wks)
Lo
g (
10)
HC
V R
NA
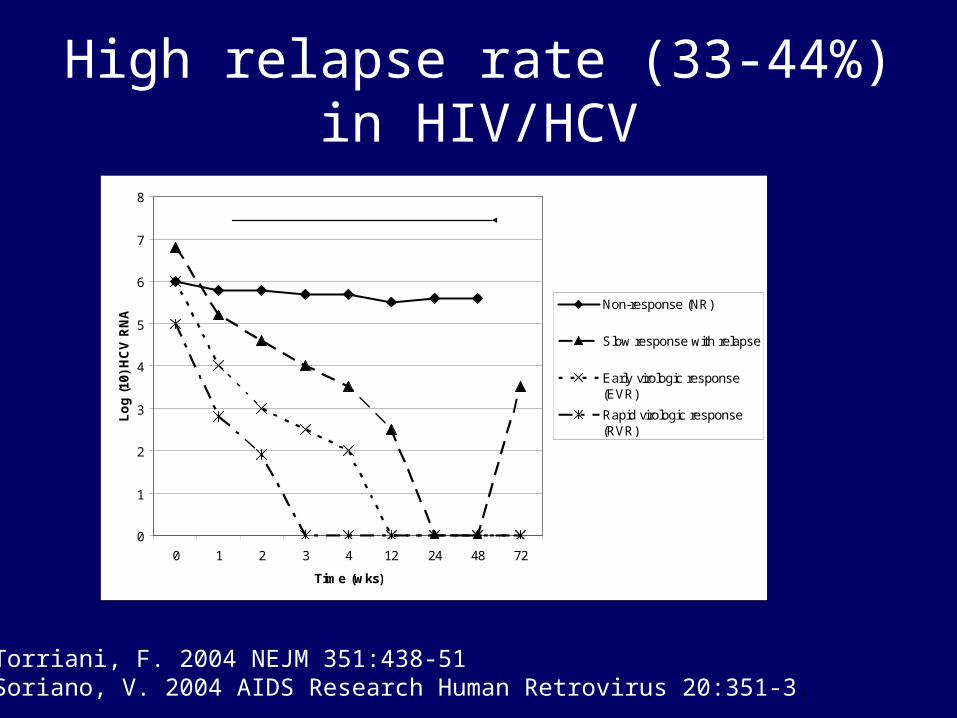
Non-response (NR)
Slow response with relapse
Early virologic response(EVR)
Rapid virologic response(RVR)
Therapy
High relapse rate (33-44%) in HIV/HCV
Torriani, F. 2004 NEJM 351:438-51Soriano, V. 2004 AIDS Research Human Retrovirus 20:351-3.

Extended treatment for HCV
• Mathematical models show that viral suppression necessary for at least 36 weeks
• HCV monoinfected trial showed that if HCV RNA + at wk 12 but – at wk 24, SVR increased from 17% to 29% with add’l 24 weeks of therapy
• Goal: reduce relapse rateDrusano GL. 2004 J Infect Dis 189:964-70Berg T. 2006 Gastro 130:1086-97.
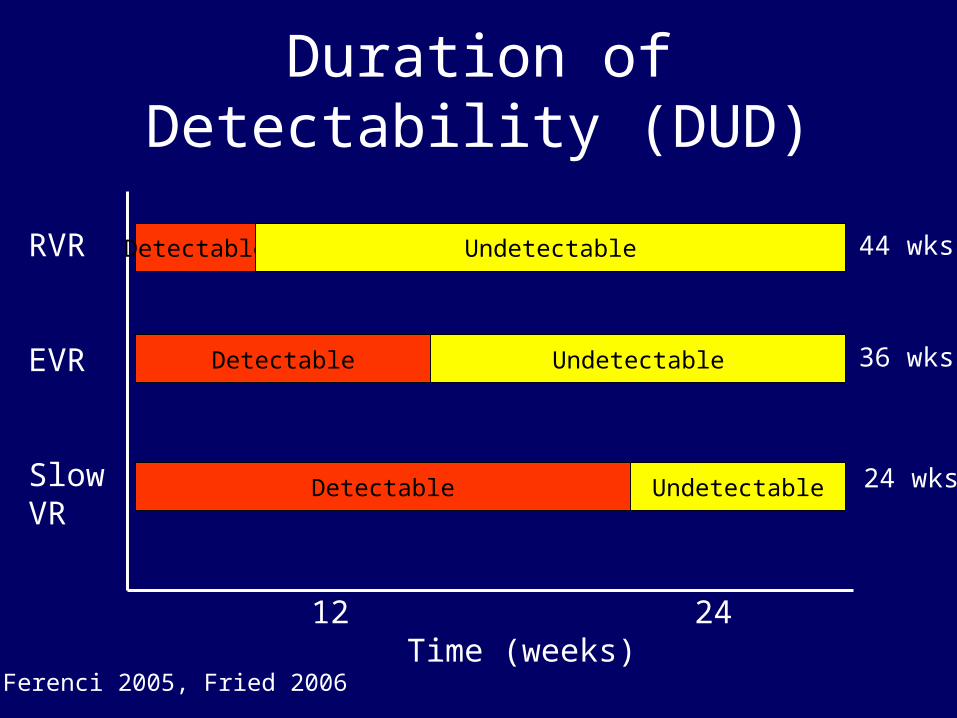
Duration of Detectability (DUD)
4 12 24 48 Time (weeks)
RVR
EVR
SlowVR
Detectable
Detectable
Detectable
Undetectable
Undetectable
Undetectable
44 wks
36 wks
24 wks
Ferenci 2005, Fried 2006
PRESCO
• Ongoing Spanish study of 398 stable coinfected pts (mean CD4 562 cells/mm3)
• All are receiving 180 mcg PegIFNα2a (Pegasys) and wt-based RBV (1000 or 1200 mg/d)
• Comparing extended tx w/ std tx:– 48 weeks for GT non-1– 72 weeks for GT 1
Soriano, et. al., 44th Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC) October 30 - November 2, 2004, Washington, DC (abstract)


% HCV Responders at Week 4
Genotype Study # patients HCV-RNA reduction> 1 log10
HCV-RNA reduction> 2 log10
SerumHCV-RNA-negative
Genotype 1
PRESCO 94 69.2 46.2 33.8
Fried 298 78.8 55.3 31.2
APRICOT 176 68 40 13
Genotype 3
PRESCO 70 93.8 89.6 85.4
Fried 140 95 90.7 84.2
APRICOT 96 87 80 37
Soriano V. 2nd Intl Workshop on HIV and HCV 2006

PRESCO: Interim Analysis
• End-of-treatment results for 181 pts:– Overall, 63% response rate– 50% for GT 1– 85% for GT 2/3
• Highest response rates reported so far for coinfected pts.

HRN-004 SLAM-C ENDURE
Patient population Nonresponse F > 0/CPT < 6
AnyF > 0/CPT < 6
AnyCPT ≤ 8
Number of patients 100 300 468
Endpoint Histology/clinical
Histology/clinical
Clinical
Arm 1 PEG-IFN alfa2a 90 mcg
PEG-IFN alfa-2a 180 mcg
PEG-IFN alfa2b 0.5 mcg/kg
Arm 2 Observation Observation Observation
Treatment duration (years)
1.5 1.5 1.5
Recruitment status Complete Enrolling Launch 2006
2nd Intl Workshop on HIV and HCV 2006
Maintenance Therapy Trials for Prior Non-responders

Drugs in development
• Serine protease inhibitors• Polymerase inhibitors• Helicase inhibitors• Antisense therapy• siRNA• Toll-like receptor
agonists• Therapeutic vaccination• Cyclosporine analog• Improved Ribavirin and
Interferon Review: McHutchison JG. 2006 J Hepatol 44:411-21
Source: www.clinicalcareoptions

Hepatitis B: Epidemiology
• HBV very common worldwide, ~350 million infected
• 1.25 million Americans chronically infected
• 70,000 new cases annually in US
• HBV is 10x more common in HIV+ than in general population
• Highest rates among HIV+ seen in MSM (6-10%)
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2006.Nunez M, et al. Lancet Infect Dis 2005.

Clinical-Epidemiologic CorrelationsHBV Endemicity
LocationAge of
InfectionMode of
TransmissionChronicity
HCC Risk
High 10-15%Asia
Sub-Sahara Africa
BirthToddler
PerinatalHorizontal
Likely High
Low < 2%N. AmericaW. Europe
Scandinavia
EarlyAdulthood
PercutaneousSexual
Rare Low
Available at: http://www.who.int/mediacentre/factsheets/fs204/en/. Accessed February 6, 2006.Designed by Jules Dienstag, MD
clinicaloptions.com/hep
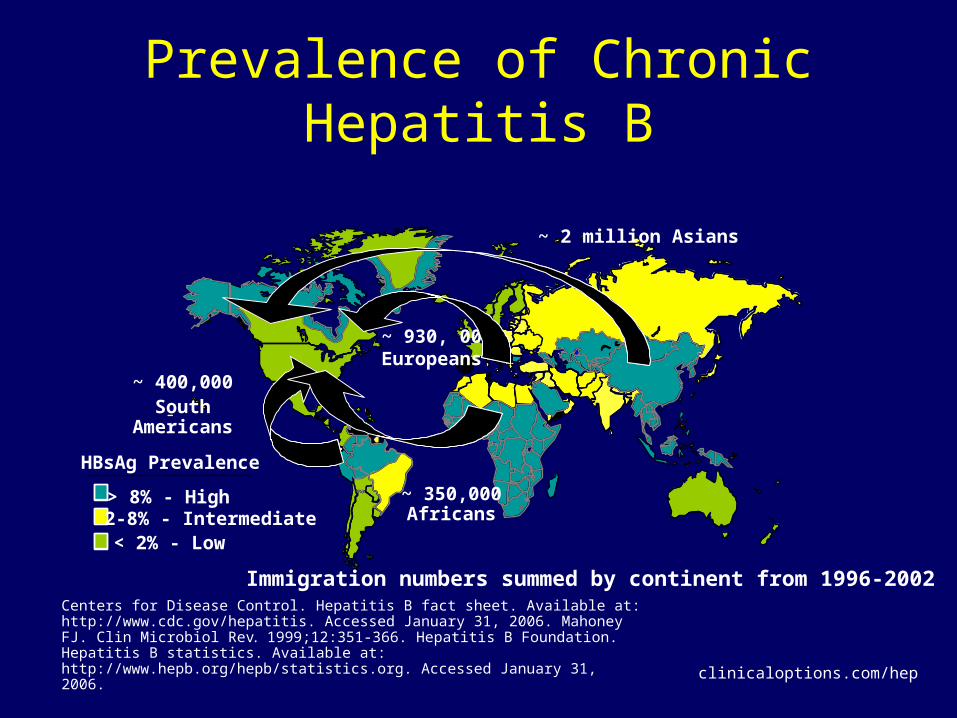
Prevalence of Chronic Hepatitis B
HBsAg Prevalence
> 8% - High 2-8% - Intermediate< 2% - Low
Immigration numbers summed by continent from 1996-2002
~ 2 million Asians
~ 400,000South Americans
~ 350,000 Africans
~ 930, 000 Europeans
Centers for Disease Control. Hepatitis B fact sheet. Available at: http://www.cdc.gov/hepatitis. Accessed January 31, 2006. Mahoney FJ. Clin Microbiol Rev. 1999;12:351-366. Hepatitis B Foundation. Hepatitis B statistics. Available at: http://www.hepb.org/hepb/statistics.org. Accessed January 31, 2006.
clinicaloptions.com/hep
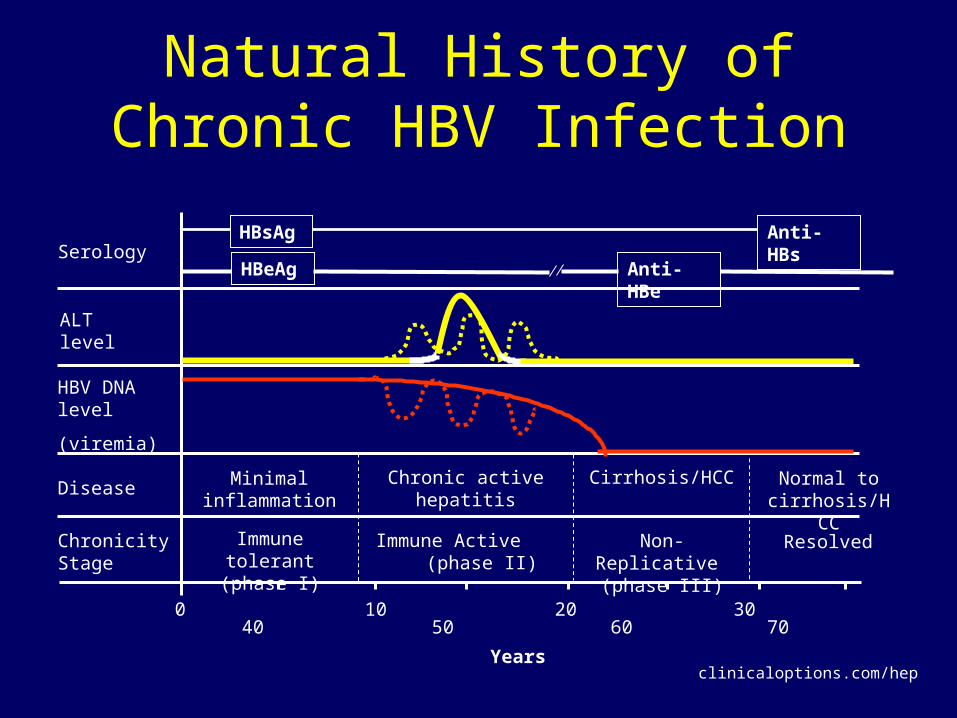
Natural History of Chronic HBV Infection
0 10 20 30 40 50 60 70
Years
SerologyHBeAg Anti-HBe
ALT level
HBV DNA level
(viremia)
DiseaseChronic active
hepatitisCirrhosis/HCC
Immune tolerant (phase I)
Immune Active (phase II)
Non-Replicative (phase III)
Chronicity Stage
Minimal inflammation
Resolved
Normal to cirrhosis/HCC
HBsAg Anti-HBs
clinicaloptions.com/hep
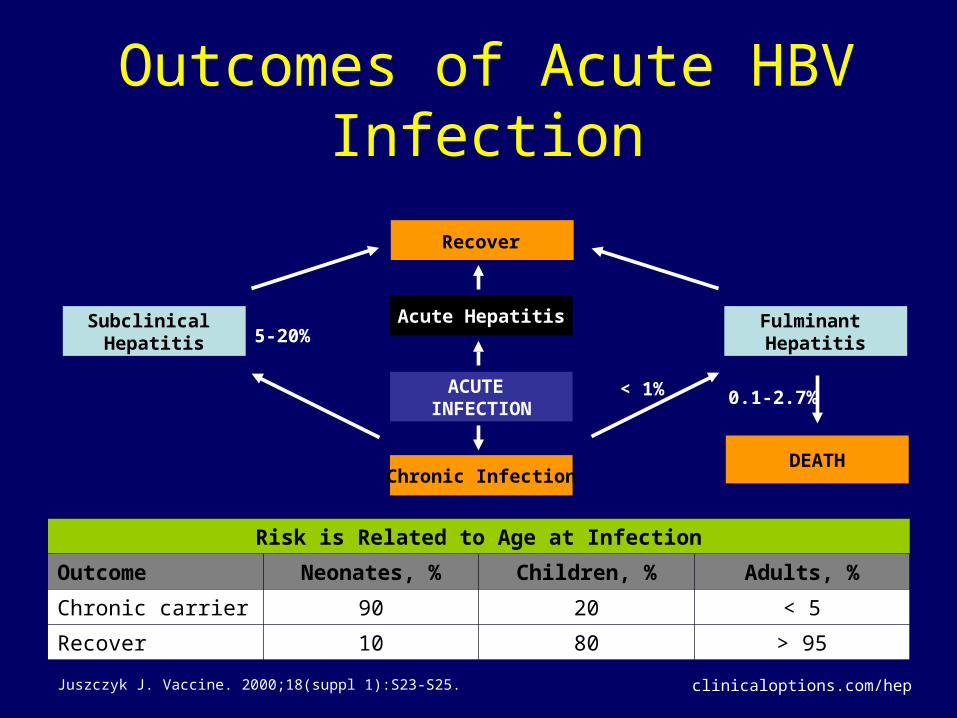
Outcomes of Acute HBV Infection
Recover
Subclinical Hepatitis
Fulminant Hepatitis
Acute Hepatitis
ACUTE INFECTION
Chronic InfectionDEATH
< 1% 0.1-2.7%
5-20%
Risk is Related to Age at Infection
Outcome Neonates, % Children, % Adults, %
Chronic carrier 90 20 < 5
Recover 10 80 > 95
Juszczyk J. Vaccine. 2000;18(suppl 1):S23-S25. clinicaloptions.com/hep

Possible Outcomes of HBeAg+ Chronic HBV Infection
Patient Populations in Chronic Hepatitis B
MarkerImmuneTolerant
HBeAg+ CHB
Inactive HBsAg Carrier
HBeAg– CHB(Precore Mutant)
HBsAg + + + +
HBeAg + + – –
Anti-HBe – – + +
ALT Normal Normal
HBV DNA (copies/mL)
> 105 > 105 < 103 > 104
Histology Normal/Mild Active Normal Active
Lai CL, et al. Lancet. 2003:362:2089-2094. Lok AS, et al. Gastroenterology. 2001;120:1828-1853.
clinicaloptions.com/hep

Annual Risk of HBV Progression
HBeAg+ chronic hepatitis B
HBeAg-Neg chronic hepatitis B
Cirrhosis
Decompensation HCC
5.0%
1.0%-2.0%
3.0% 2.0%
All HBsAg +individuals
0.4%
Factors linked with progression
– Duration of “active”disease– Heavy alcohol use– Immune suppression (HIV)
Juszczyk J. Vaccine. 2000;18(suppl 1):S23-S25. clinicaloptions.com/hep
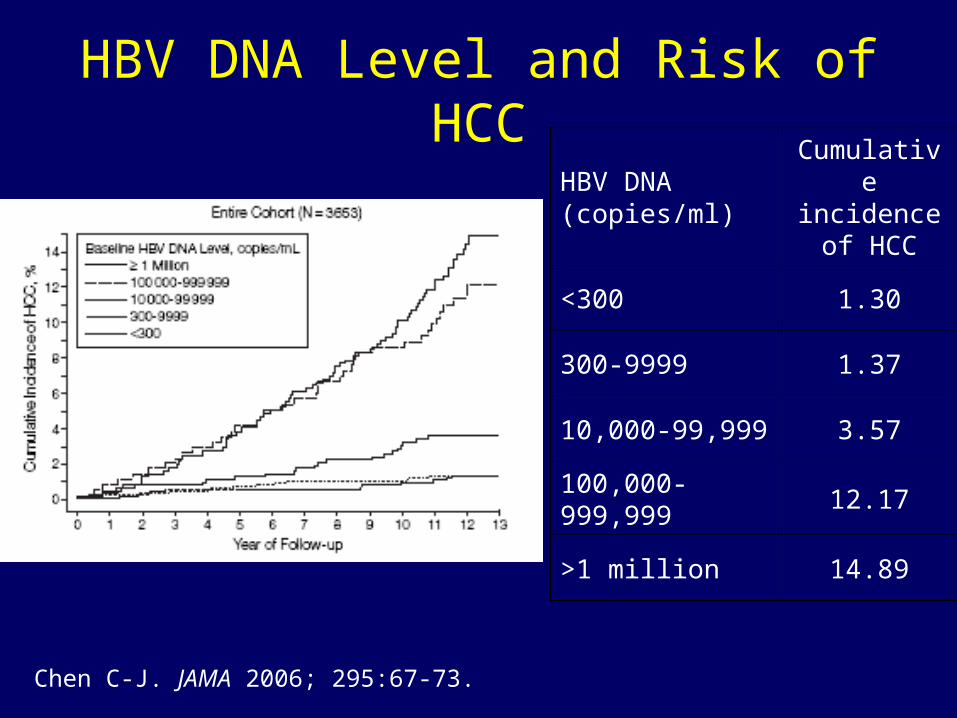
HBV DNA Level and Risk of HCCHBV DNA (copies/ml)
Cumulative incidence of
HCC
<300 1.30
300-9999 1.37
10,000-99,999 3.57
100,000-999,999 12.17
>1 million 14.89
Chen C-J. JAMA 2006; 295:67-73.

HBV Treatment Guidelines
HBeAgHBV DNA(IU/ml)*
ALT Management
+< 20,000 Normal#
Follow, no treatment
+≥ 20,000 Normal
Consider biopsy;treat if diseased
+ ≥ 20,000 Elevated Treat
–< 2,000 Normal
Follow, no treatment
–≥ 2,000 Normal
Consider biopsy;treat if diseased
– ≥ 2,000 Elevated Treat
*1 IU = 5.6 copies; #Normal ALT for men = 30 U/ml and for women = 19 U/mlKeeffe EB, et al. Clin Gastroenterol Hepatol.2006.
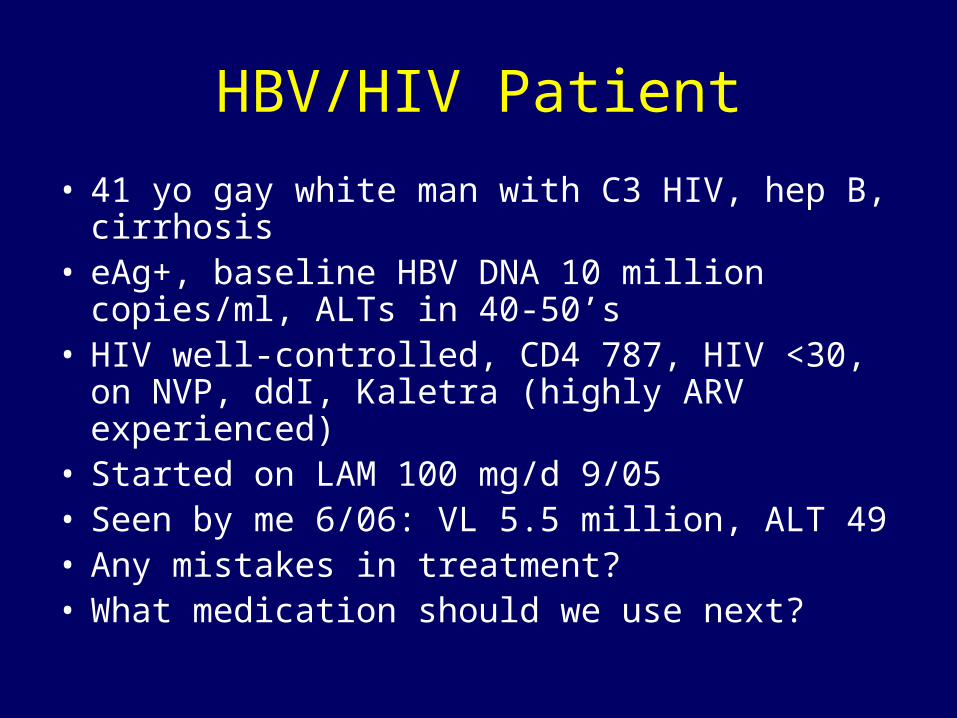
HBV/HIV Patient
• 41 yo gay white man with C3 HIV, hep B, cirrhosis
• eAg+, baseline HBV DNA 10 million copies/ml, ALTs in 40-50’s
• HIV well-controlled, CD4 787, HIV <30, on NVP, ddI, Kaletra (highly ARV experienced)
• Started on LAM 100 mg/d 9/05• Seen by me 6/06: VL 5.5 million, ALT 49• Any mistakes in treatment?• What medication should we use next?
Goals of Therapy in Patients With Chronic HBV Infection
• Eradication of infection– HBsAg seroconversion– Undetectable HBV DNA
• Prevent complications of liver disease– Histologic progression to cirrhosis– Decompensated liver disease– Liver cancer
clinicaloptions.com/hep

Therapeutic Endpoints• HBeAg-positive patients (wild type)
– HBeAg seroconversion is KEY– Sustained suppression of HBV DNA to low or
undetectable levels– ALT normalization– Reduced necroinflammation on biopsy
• HBeAg-negative patients (precore and core promoter mutants)– HBeAg seroconversion not an endpoint– Sustained suppression of HBV DNA to low or
undetectable levels– ALT normalization– Reduced necroinflammation on biopsy
clinicaloptions.com/hep
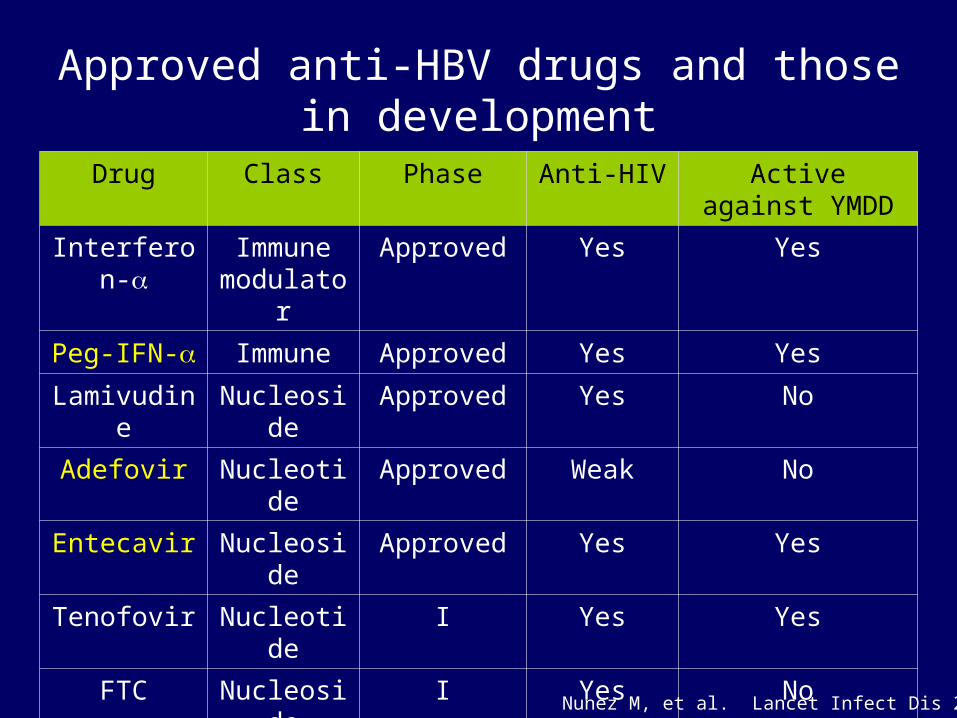
Approved anti-HBV drugs and those in development
Drug Class Phase Anti-HIV Active against YMDD
Interferon- Immune modulator
Approved Yes Yes
Peg-IFN- Immune Approved Yes Yes
Lamivudine Nucleoside Approved Yes No
Adefovir Nucleotide Approved Weak No
Entecavir Nucleoside Approved Yes Yes
Tenofovir Nucleotide I Yes Yes
FTC Nucleoside I Yes No
Telbivudine Nucleoside III No No
Clevudine Nucleoside III No Yes
DAPD Nucleoside II Yes Yes
Nunez M, et al. Lancet Infect Dis 2005.

Responses to anti-HBV agents in HIV/HBV coinfected patients
IFN LAM ADV ETV FTC TDF
# pts 87 230 35 51 33 200
HBV DNA ↓
26% 2.7 log 4.7-6 log 3.6 log - 4.4 log
E sero-
Convert
9% 11% 7% - - 4%
ALT normalize
12-20% 30-50% 35-66% 49% - -
Histology
improve
- - 33-50% - - -
Benhamou Y. J Hepatol 2006.
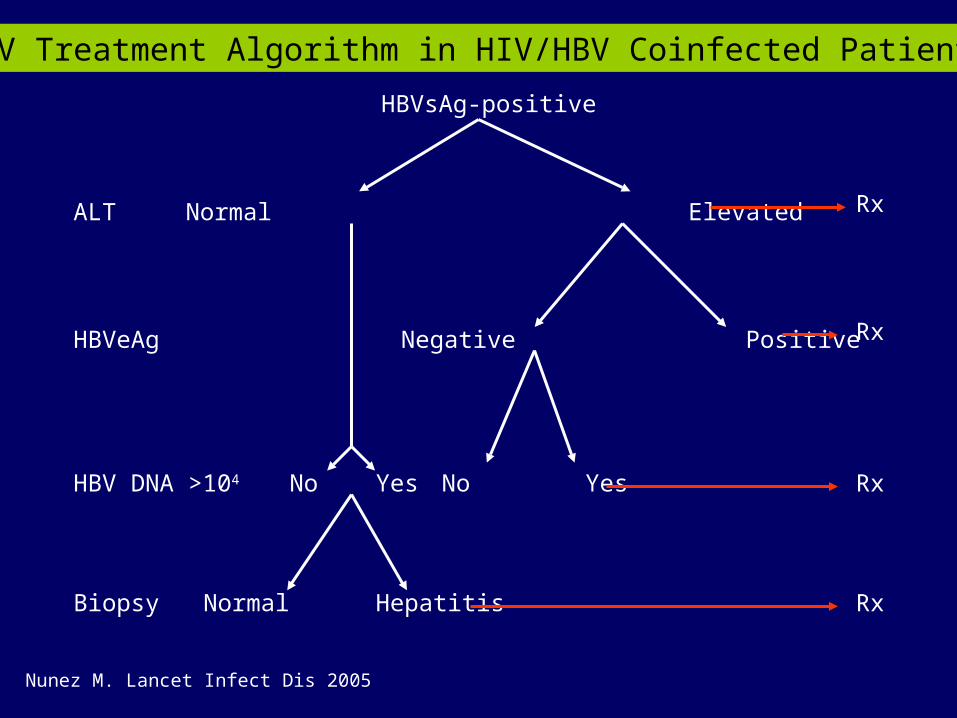
HBV Treatment Algorithm in HIV/HBV Coinfected Patients
HBVsAg-positive
ALT
HBVeAg
HBV DNA >104
Biopsy
Normal Elevated
Negative Positive
No Yes No Yes
Normal Hepatitis
Rx
Rx
Rx
Rx
Nunez M. Lancet Infect Dis 2005
Lamivudine (3TC, Epivir)
• Nucleoside analog• Different dose for HBV (100 mg)
monotherapy, use 300 mg for HIV+ and never alone
• Well-tolerated and cheap• eAg conversion rate b/t 21-28%• High rates of resistance!
– 47% develop YMDD mutation at 2 yrs, 90% at 4 yrs

Adefovir (Hepsera)
• Nucleotide analog
• At 10 mg/d dose, no HIV activity
• Effective for LAM resistant HBV, no cross-resistance
• Side effects: renal toxicity, Fanconi’s Syndrome

Tenofovir (Viread)
• Nucleotide analog not approved for HBV
• Perhaps more potent than Adefovir– 48 wk mean decline in HBV DNA (log10) 4.4
vs 3.2
• 63% had HBV suppression by wk 48, 15% had anti-HBe seroconversion
• Rare cases of ADV resistance but TDF sensitivity
Schildgen O. 2006 N Engl J Med 354:1807-12Peters M. CROI 2005; Abstract 124.

Entecavir (Baraclude)
• Nucleoside analog
• No HIV activity
• Good for LAM failures– 84% of patients had 2 log decline or <400
copies/ml after 24 wks
• Cross-resistance can occur w/ LAM
• Start w/ higher dose (1.0 mg/d) Entecavir in HIV/HBV patients

Peg-interferon (Pegasys)
• Long acting form of IFN, once weekly• Pros: defined duration (48 wks), low resistance• Cons: Many side effects, expensive, not for
decompensated cirrhosis• No data in HIV+, probably lower response than
in HIV-• In HIV-, PEG better than LAM
– 27% seroconversion, 4.5 log HBV DNA reduction, 3% sAg loss

Treatment Options for HIV/HBV Coinfected Patients
Only HBV therapy indicated
HBeAg-positive Pegylated IFN
Entecavir
Adefovir
HBeAg-negative Entecavir
Adefovir
HIV and HBV therapy indicated
HAART including TDF +/- LAM or FTC
HAART + (ADV or ETV)
Only HIV therapy At least one HBV active drug to avoid flares
Nunez. Lancet Infect Dis 2005.

Back to the patient
• 41 yo gay white man with C3 HIV, hep B, cirrhosis
• eAg+, baseline HBV DNA 10 million copies/ml, ALTs in 40-50’s
• HIV well-controlled, CD4 787, HIV <30, on NVP, ddI, Kaletra (highly ARV experienced)
• Started on LAM 100 mg/d 9/05• Seen by me 6/06: VL 5.5 million, ALT 49• Any mistakes in treatment?• What medication should we use next?

Web Resources• www.aasld.org• www.hivandhepatitis.org• www.hepwebstudy.org• www.cdc.gov/ncidod/
diseases/hepatitis/c/index.• www.idsociety.org

Good Reviews
• Sulkowski MS. Treatment algorithm for the management of hepatitis C in HIV-coinfected person. 2006. J Hepatol 44:S49-55
• Nunez M, Soriano V. Management of patients coinfected with hepatitis B virus and HIV. 2005. Lancet Infect Dis 5:374-82
• Tien P, Wright T. Management and treatment of hepatitis C virus infection in HIV-infected Adults: Recommendations from the Veterans Affairs Hepatitis C Resource Center Program and National Hepatitis C Program Office. 2005. Am J Gastro 100: 2338-54.
• Benhamou Y. Treatment algorithm for chronic hepatitis B in HIV-infected patients. 2006. J Hepatol 44:S90-94.

Thanks!