hepatocelular carcinoma
TRANSCRIPT
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 1/52
Page 1 of 52
[Type text] Page 1
Hepatocelular carcinoma
Introduction:
Hepatocellular carcinoma (HCC) is the third leading
cause of cancer-related death and accounts for as many
as 500 000 deaths annually being a considerable challenge
for surgeons[1]. The incidence of HCC varies by geographic
location from a relatively rare tumor, like those
found in North America and Europe, to a very common
and highly malignant tumor as occurs in sub-Saharan
Africa and Southeast Asia. HCC has been found to account
for 80% of all primary liver cancers, being the
fifth most common cancer worldwide[1,2]. Most patients
with HCC also suffer from coexisting cirrhosis, which
is the major clinical risk factor for hepatic cancer and is
correlated to hepatitis B virus or hepatitis C virus (HCV)
infection[3]. However, cirrhosis from non-viral causes
such as alcoholism, hemochromatosis and primary biliary
cirrhosis are also associated with an elevated risk
of HCC. Furthermore, concomitant risk factors such as
HCV infection in addition to alcoholism, tobacco use,
diabetes or obesity increase the relative risk of HCC development,
as numerous studies in humans and animal
models have shown[4-10]. The incidence of HCC varies
by geographic area worldwide. Research has shown that
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 2/52
Page 2 of 52
[Type text] Page 2
Southeast Asia and sub-Saharan Africa have an incidence
rate of HCC that ranges from 150 to 500 per 100 000
population, primarily because of the endemic nature of
hepatitis B and C in those regions[11-13].
HCV accounts for almost 90% of all cases of HCC
in Japan, and in China, hepatitis B infection is diagnosed
in about 80% of patients with HCC[12-14]. In Europe and
North America, however, despite a significantly lower incidence
rate of 3 to 4 per 100 000 population, a distinct
increase in cases of HCC has been reported as a result
of intravenous drug use, unsafe sexual practices, and
other causes[15-17]. Because of a lack of effective HCV
vaccination, underlying HCV infection is largely responsible
for that increase. As a result of the interval between
the onset of infection and the development of liver cirrhosis,
the incidence of HCV-related HCC will continue
to increase over the next few years[18]. In contrast to
Asian populations, the percentage of Western patients
with HCC but without underlying cirrhosis is considerable,
and the development of HCC in cirrhotic individuals
in the West is associated with a wider spectrum
of underlying diseases. In the West, the percentage of
virally engendered cirrhosis is lower than that in Asian
regions, but alcohol-toxic or cryptogenic hepatic dam-
age is observed more frequently in Western countries[14].
Thus, the etiologic pattern of HCC in Western regions
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 3/52
Page 3 of 52
[Type text] Page 3
of low risk for that disease differs appreciably from that
in Southeast Asia and sub-Saharan Africa.
Surgery, including liver transplantation (LT), still
remains the most important therapeutic approach for
patients with HCC. Over the past few decades, considerable
progress has been made in the diagnosis and surgical
treatment of HCC. In fact, tumors are now often identified
at an early stage[19,20], surgery is safer with an acceptable
overall mortality rate (in cirrhotic patients < 5%),
being characterized by a good long-term survival[21,22] and
results of LT have steadily improved because of careful
patient selection[23].
However, HCC is still associated with a high rate
of mortality and prognosis of this tumor is poor even
when treatment has been considered potentially curative[
24,25].
This brief report summarizes the current status of
the management of this disease and includes a short
description of a new pharmacological approach in HCC
treatment.
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 4/52
Page 4 of 52
[Type text] Page 4
STAGING:
Various classification systems are available for HCC. The
Barcelona Clinic Liver Cancer (BCLC) classification has
emerged during recent years as the standard classification
that is used for trial design and clinical management
of patients with HCC[26,27]. This classification has been
approved by EASL and the AASLD [24,28] and has subsequently
been corroborated in clinical studies [29,30]. The
BCLC staging system was constructed on the basis of
the results obtained in the setting of several cohort studies
and randomized controlled trials by th e Barcelona
group.
The main prognostic factors of this s taging system
are related to tumor status (defined by the number and
size of nodules, the presence or absence of vascular
invasion, and the presence or absence of extrahepatic
spread), liver function (defined by the Child-Pugh score
system, serum bilirubin and albumin levels, and portal
hypertension), and general health status [defined by
the Eastern Cooperative Oncology Group (ECOG),
classification and presence of symptoms]. On the other
hand, aetiology is not an independent prognostic factor.
The BCLC classification links stage stratification with a
recommended treatment strategy and defines standard

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 5/52
Page 5 of 52
[Type text] Page 5
of care for each tumor stage (Figure 1).
Patients with very early HCC (stage 0) are optimal
candidates for resection. Patients with early HCC (stage A)
should be considered for radical therapy [rese ction, LT,
or local ablation via percutaneous ethanol injection (PEI)
or radiofrequency (RF) ablation]. Patients with intermed iate
HCC (stage B) have been found to benefit from
transarterial chemoembolization (TACE). Patients with
advanced HCC, defined as the prese nce of macroscopic
vascular invasion, extrahepatic spread, or cancer-related
symptoms (ECOG performance status 1 or 2) (stage
C), have recently been found to benefit from Sorafenib
treatment[31,32]. Patients with end-stage disease (stage D)
will receive symptomatic treatment.
Treatment strategy will transition from one stage to
another on treatment failure or contraindications for the
procedures.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 6/52
Page 6 of 52
[Type text] Page 6
HCC TREATMENT OPTIONS:
Liver resection:
Pre-treatment imaging studies such as computed tomography
and magnetic resonance imaging, either with
or without angiography, can be used to match patients
with their most appropriate treatment. Positron emission
tomography is also useful in the identification of
extrahepatic metastases which considerably influence
clinical decision-making. These types of studies aid in
detecting intrahepatic and extrahepatic disease as well
as vascular invasion. Knowledge about the relation of
the tumour to regional anatomic structures su ch as large
vessels is crucial because it provides valuable information
about resectability. Furthermore, volumetric studies
can be used to define the residual parenchyma exactly.
The determination of hepatic reserve is also significant
when resection is considered. The he althy liver has a
great capacity for regeneration and adjusts to the metabolic
requirements of the host after liver resection due
to hypertrophy of the residual live r. Partial hepatectomy
usually ensures a safety margin of at least one centimeter
and is associated with an operative mortality rate of less
than 5%[33,34]. For patients with inadequate or borderline
remnant parenchyma, hypertrophy of the prospective
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 7/52
Page 7 of 52
[Type text] Page 7
liver remnant can be induced by preoperative portal
vein embolization[35]. However, the use of portal vein
embolization to induce compensatory hypertrophy of
healthy liver before major resection is controve rsial. Uncontrolled
tumour progression as a result of the proliferation
of malignant cells stimulated by this me thod and
the risk of variceal bleeding resulting from acute portal
hypertension should be carefully considere d and for that
reason this procedure raises some concerns[36]. In certain
circumstances, an unfavourable location of the tumour
and involvement of the confluence of the three he patic
veins and either the caval vein or the re trohepatic caval
vein can render resection by conventional techniques impossible.
In these rare cases, special techniques such as
in situ or ante situm resection can be used[37].
The overall long-term results after resection are favourable.
However, only 20% to 30% of patients with
HCC are eligible for resection because of advanced or
multifocal disease or inadequate functional hepatic reserve[
38]. In patients with solitary lesions of less than 5 cm,
no vascular invasion, and a negative surgical margin of
at least 1 cm, the 5-year survival rate after resection has
been reported to be greater than 70%[39]. In a series consisting
of 68 patients with HCC and non-cirrhotic liver,
an overall 5-year survival rate of 40% was achieved even
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 8/52
Page 8 of 52
[Type text] Page 8
when extensive resection had been performed[40]. Similar
results were observed in a large series in which patients
with HCC and non-cirrhotic liver demonstrated a survival
rate of 58% after 3 years and 42% after 5 years[41].
Despite earlier detection, safer surgical procedures
and more aggressive treatment of HCC, recurrence, as a
result of multicentric carcinogenesis or intrahepatic metastases
from the primary tumour may occur. In selected
patients, repeat resection provides good long-term benefits
and is an option for those with solitary peripheral
tumors that can be treated with segmental or atypical
resection. In patients with adequate functional reserve
capacity and no extrahepatic tumour growth, the 5-year
survival rate after repeat resection has be en reported to
be as high as 86%[42].
Liver Transplant:
LT is one of the best treatment approaches for HCC
in patients who fulfil the selection criteria (solitary tumors
of less than 5 cm and up to three tumour nodules,
each of which is smaller than 3 cm)[23]. First, it removes
the tumour with the widest margin together with any
intrahepatic metastasis. Second, it cures the underlying
cirrhosis that is responsible for both hepatic decompensation
and metachronous tumour after partial he patectomy.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 9/52
Page 9 of 52
[Type text] Page 9
Finally, it allows the histologic examination of
the entire liver explant for the most accurate pathologic
staging.
Study results have generally shown a significantly
higher probability of survival in patients with incide ntally
discovered tumors, no vascular invasion, a negative
nodal status, a tumour size of less than 5 cm, and a tumour
of lower histologic grade[43-48]. The 5-year reported
survival rate is around 26% after resection and 69% after
transplantation in cirrhotic patients with HCC[43]. The
decisive prognostic factor for patients with HCC is vascular
invasion, which no system of medical imaging can
accurately demonstrate at this time[49]. Therefore, the preoperativ e
prognosis is still based on the number and size
of tumour nodes demonstrated, due to the evide nce that
vascular invasion has been found to be correlated to tumour
size and number[44]. Because of the present lack of
organs available, an accurate estimation of the patie nts
prognosis is important and not every patient with HCC
and cirrhosis can be treated with LT. Thus the need to
obtain the optimal benefit from the limited number of
organs available has prompted adherence to strict selection
criteria, so that only those patients with early HCC
and the highest likelihood of survival after transplantation
are listed to undergo that procedure (Figure 1).
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 10/52
Page 10 of 52
[Type text] Page 10
Excellent 5-year post-transplant patient survival of
at least 70% has been reported from many centres[50,51].
In another study, excellent results were achieved in patients
with solitary lesions of a maximum diameter of 6.5
cm, patients with a maximum of three lesions (the largest
of which was no larger than 4.5 cm), and those who
had no more than 8 cm in diamete r in all tumour nodes.
The 1-year and 5-year survi val rates of these patients
were as high as 90% and 72%, respectively[52].
Even if the selection criteria for LT to treat HCC
could be expanded, the current shortage of liver grafts
and the lack of data defining the new limits for LT in
patients with HCC makes the attempt t o expand the
listing criteria a very controversial issue. As a result of
expanded listing criteria, the inclusion of patients with
more advanced cancer may result in a higher dropout
rate that in turn leads to poor survival rates in an intentto-
treat analysis[53,54].
In their recent publication, Mazzaferro and colleagues[
55] developed a new prognostic model that could
be used to expand the Milan criteria and help identify
patients whose odds of survival could be improved b y
having a liver transplant. Using the up-to-seven criteria,
where seven is the maximum number obtained by
adding the size of the largest tumour (in centimeter) to

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 11/52
Page 11 of 52
[Type text] Page 11
the total number of tumors, the report indicates that the
5-year survival in patients without microvascular invasion
was 71.2%, similar to patients who met the Milan
criteria. The researchers conclude: more patie nts with
HCC could be candidates for transplantation if the current
dual (yes/no) approach to candidacy, based on the
strict Milan criteria, was replaced with a more precise
estimation of survival contouring individual tumour
characteristics and use of the up-to-seven criteria.
Stage 0
PST 0, Child-Pugh A
Stage A-C
PST 0-2, Child-Pugh A-B
Stage D
PST > 2, Child-Pugh C
Early stage (A)
Single or 3 nodules < 3 cm, PS 0
Intermediate stage (B)
Multinodular, PST 0
Advanced stage (C)
Portal invasion, N1, M1, PST 1-2
Very early stage (0)
Single < 2 cm
Carcinoma in situ
End stage (D)

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 12/52
Page 12 of 52
[Type text] Page 12
HCC
Single
Portal pressure/bilirubin
Normal
Resection
Increased Associated diseases
3 nodules 3 cm
No Yes
Liver transplantation
(CLT/LDLT)
PEI/RF TACE Sorafenib
Curative treatments (30%)
5-yr survival: 40%-70%
Randomized controlled trials (50%)
Median survival 11-20 mo
Symptomatic treatment (20%)
Survival < 3 mo
Figure 1 Barcelona Clinic Liver Cancer staging classification and
treatment schedule[27].
3212 ISSN 1007-9327 CN 14-1219/R World J Gastroente rol July 14,
2009 Volume 15 Number 26
www.wjgnet.com
Therefore, the ultimate therapeutic choice should
always result from the analysis of each individual case
and should be based on the experience and judgment of

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 13/52
Page 13 of 52
[Type text] Page 13
the transplant team and not just on the statistical results
derived from the literature.
The wait for a graft to become available still presents
the greatest challenge. Methods of neoadjuvant therapy
(PEI, RF, TACE) may be used to provide tumour
control in patients on a waiting list for LT.
Patients can reach a prognostically unfavourable
stage because of tumour progression with subsequent
deterioration of their clinical profile while waiting and
may no longer fulfil the criteria for LT[52]. As a result,
these patients should be removed from the waiting list,
indeed about 50% of HCC patients who were initially
candidates for LT will become ineligible for transplantation
if the median waiting period exceeds 1 ye ar[53,56].
Strategies to increase the donor pool and diminish
the tumour progression rate have become a priority in
many centres. In the United States, the United Network
for Organ Sharing proposed a new system to allocate patients
on the list according to the Mode l for End-Stage
Liver Disease score[57]. This change give s priority to patients
to minimize drop-out rates and has improved the
access to timely liver transplant for patients with HCC[58].
Recent advances in adult living-donor liver
transplantation (LDLT) may produce a drastic change
in the role of transplantation surgery for HCC. This

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 14/52
Page 14 of 52
[Type text] Page 14
option enables patients to avoid the long waiting time
before transplantation and consequently to reduce the
dropout rate. The keynote of living donation in patients
with HCC and cirrhosis is supported by these factors:
(1) Better graft function, because each graft is obtained
from a healthy person;
(2) Better clinical condition of the patient at the time of
transplantation;
(3) Optimal organ harvest, conservation, and reduced cold ischemia
time;
(4) A significantly reduced waiting time.
Whether LDLT is indicated in patients with HCC
that exceeds the Milan criteria remains controversial[59,60].
A recent survey of transplant surgeons from North
America, Europe, and Asia revealed that 41% of the respondents
favoured LDLT for use in patients with HCC
that exceeds the Milan criteria[61]. Patients who no longer
fulfil the criteria because of tumour size or the number
of tumour nodes may still retain the option of LDLT.
Because a potential 5-year survival rate of around 50%
in patients whose LT is justified by exte nded criteria has
been described[53], transplantation would offer a better
chance of survival than would all other therapeutic options.
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 15/52
Page 15 of 52
[Type text] Page 15
However, evidence-based universal guidelines for
this important issue have not been established. Pri mary
graft failure and the risk to the donor present ethical
concerns that cannot be disregarded. Donor deaths and
other complications, such as insufficiency of the donors
remaining liver (which required subsequent transplantation),
have been reported[62]. Furthermore, some data
also suggest the need to have a better evaluation of the
donor, including liver histology[63]. The complication rate
for LT in North America and Europe ranges between
9.2% and 40% for the donor, and the mortality risk in
donors is still 0.3% to 0.61%[64,65 ]. In contrast, data
in Japan showed a complication rate of 12% with no
perioperative deaths in living liver donors[66]. Meticu lous
surgical techniques and perioperative management, lean
body mass in individual Japanese donors, and genetic
factors were given as possible explanations for the zero
transplant-related mortality rate in Japan. In general,
however, morbidity after living liver donation strongly
correlates with the expertise of the staff of the transp lant
centre. Therefore, a combination of surgical expertise
and thorough, individualized medical and psychological
evaluations is vital to ensure the lowest morbidity
rate and best outcome, not only in the recipient, but also
in the donor.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 16/52
Page 16 of 52
[Type text] Page 16
Locoregional procedures and
chemotherapy:
Percutaneous ablation:
For patients who are not candidates
for liver resection or transplantation, percutaneous
ablation offers the best treatment option. However,
to our knowledge, there are no randomized controlled
clinical trials that have compared the results of this treatment
option with those of surgical therapy for HCC,
and none of the ablation techniques have been shown
to offer a definitive surviv al advantage. The principle of
ablation is based on the destru ction of tumour cells by
the application of chemical substances, su ch as ethanol,
or by using RF or laser to modify the temperature in the
tumour via the delivery of heat. Of all those technique s,
PEI has been the most investigated[67]. In individuals
who do not fit the optimal surgical profile, PEI is as effective
as surgery and is associated with a 5-year surviv al
rate as high as 72% if the accurate selection of patients
is performed[68,69]. The low rate of procedure-re lated
complications and the low cost of PEI a re additional
advantages. The main drawback of this technique is the
need for repeated injections in separate sessions and the
inability to achieve complete necrosis in larger tumors.
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 17/52
Page 17 of 52
[Type text] Page 17
In that regard, RF ablation has be en shown to be more
effective in achieving complete necrosis in tumors larger
than 2 cm and to require fewer treatment sessions[70]. RF
ablation involves the delivery of energy created by RF
waves to tumors to induce thermal da mage and coagulative
necrosis. Study results have shown that RF ablation
is superior to PEI in terms of causing complete tumour
necrosis (90% vs 80%) and in the number of required
treatments (1.2 vs 4.8)[71]. However, RF ablation causes
more complications such as pleural effusion, bleeding,
and tumour seeding than does PEI[71,72]. In addition, the
effectiveness of RFA decreases as the tumour size exceeds
3 cm.
Chemoembolization:
This approach can be used before
liver resection to improve resectability, as a bri dge
to LT while awaiting organ availability, or as a palliative
treatment, and it may offer patients with preserved liv er
function and no evidence of ascites a surviv al advantage[
73]. Chemoembolization is based on the principle of
arterial obstruction (obstruction of the hepatic artery
during angiography via the use of agents such as an absorbable
gelatin sponge, alcohol, etc, to induce ischemic
tumour necrosis). This technique is effective because the
growth of HCC depends primarily on the hepatic artery

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 18/52
Page 18 of 52
[Type text] Page 18
blood supply, but the healthy hepatic parenchyma has a
dual blood supply (85% is supplied by the portal vein,
and the remainder is supplied by the he patic artery). The
injection of a chemotherapeutic agent [usually cisplatin,
doxorubicin hydrochloride (Adriamycin), or mitomycin
C] before arterial obstruction (transcatheter arterial embolization)
results in TACE, a method by which regionally
elevated levels of these agents in the live r can be
achieved while concomitant systemic toxicity is avoided.
When compared with controls, patients treated with
TACE exhibited a decrease in tumour size of 16% to
61% and a 1-year survival advantage as high as 82%[74-77].
Systemic treatment:
A number of systemic chemotherapies have been evaluated
in many clinical trials. Unfortunately, no sing le agent
or combination of agents given systemically leads to reproducible
response rates that show beneficial effe ct of
systemic chemotherapy on survival rates[78]. Tamoxifen,
octreotide, interferon, and interleukin-2 have not been
shown to be effective in treating HCC in randomized
controlled clinical trials[79,80]. The increasing knowledge in
the molecular structure of HCC as well as the introduction
of molecular targeted therapies in oncology have
created an encouraging trend in the management of this

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 19/52
Page 19 of 52
[Type text] Page 19
disease[81]. These targeted molecular therapies are aimed
at growth factors and their receptors, intracellular signal
transduction and cell cycle control. Recent positive results
from a preliminary study of the receptor tyrosine
kinase inhibitor, sorafenib, have bee n reported in the
treatment of HCC[31,32]. This oral multikinase inhibitor
action of several kinases (VEGF, PDGF, c-kit receptor,
Raf) involved in both tumour cell proliferation (tumour
growth) and angiogenesis (tumour blood supply).

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 20/52
Page 20 of 52
[Type text] Page 20
CONCLUSION:
Novel treatment options based on an improved understanding
of the molecular pathogenesis of HCC have
been proposed. Nonetheless a substantial improvement
in the outcomes of intermediate and advanced stage
HCC is expected with the advent of these targeted the rapies,
used in combination with surgical or locoregional
therapies.
LT still remains an important treatment approach f or
HCC and is a well-documented and proven treatment
modality for this disease. However, early unsatisfactory
results have emphasized that only a highly selected
patient population would benefit from transplantation.
Pretransplantation therapies and the deve lopment of
novel agents to prevent progression of HCC in patients
awaiting LT are neede d. Promotion of organ donation
is necessary, the role of new systemic therap y is now
becoming a new and interesting option in the treatment
of patients with HCC, but LDLT as the dominant
strategy will continue to escalate.
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 21/52
Page 21 of 52
[Type text] Page 21
REFERENCES
1 Parkin DM, Bray F, Ferlay J, Pisani P. Estimating the world
cancer burden: Globocan 2000. Int J Cancer 2001; 94: 153-156
2 Befeler AS, Di Bisceglie AM. Hepatocellular carcinoma:
diagnosis and treatment. Gastroenterology 2002; 122:
1609-1619
3 Liu JH, Chen PW, Asch SM, Busuttil RW, Ko CY. Surgery
for hepatocellular carcinoma: does it improve survival? Ann
Surg Oncol 2004; 11: 298-303
4 Fong TL, Kanel GC, Conrad A, Valinluck B, Charboneau F,
Adkins RH. Clinical significance of concomitant hepatitis C
infection in patients with alcoholic liver disease. Hepatology
1994; 19: 554-557
5 Ming L, Thorgeirsson SS, Gail MH, Lu P, Harris CC,
Wang N, Shao Y, Wu Z, Liu G, Wang X, Sun Z. Dominant
role of hepatitis B virus and cofactor role of aflatoxin in
hepatocarcinogenesis in Qidong, China. Hepatology 2002; 36:
1214-1220
6 Hassan MM, Hwang LY, Hatten CJ, Swaim M, Li D,
Abbruzzese JL, Beasley P, Patt YZ. Risk factors for
hepatocellular carcinoma: synergism of alcohol with
viral hepatitis and diabetes mellitus. Hepatology 2002; 36:
1206-1213
7 Ohata K, Hamasaki K, Toriyama K, Matsumoto K, Saeki
A, Yanagi K, Abiru S, Nakagawa Y, Shigeno M, Miyazoe
S, Ichikawa T, Ishikawa H, Nakao K, Eguchi K. Hepatic
steatosis is a risk factor for hepatocellular carcinoma in
patients with chronic hepatitis C virus infection. Cancer
2003; 97: 3036-3043
8 El-Serag HB, Richardson PA, Everhart JE. The role of
diabetes in hepatocellular carcinoma: a case-control study
among United States Veterans. Am J Gastroenterol 2001; 96:

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 22/52
Page 22 of 52
[Type text] Page 22
2462-2467
9 Davila JA, Morgan RO, Shaib Y, McGlynn KA, El-Serag
HB. Diabetes increases the risk of hepatocellular carcinoma
in the United States: a population based case control study.
Gut 2005; 54: 533-539
10 Chokshi MM, Marrero JA. Hepatocellular carcinoma. Curr
Opin Gastroenterol 2001; 17: 276-280
11 Kew MC. The development of hepatocellular cancer in
humans. Cancer Surv 1986; 5: 719-739
12 Di Bisceglie AM. Hepatitis C and hepatocellular carcinoma.
Semin Liver Dis 1995; 15: 64-69
13 El-Serag HB. Hepatocellular carcinoma and hepatitis C in
the United States. Hepatology 2002; 36: S74-S83
14 Beasley RP. Hepatitis B virus. The major etiology of
hepatocellular carcinoma. Cancer 1988; 61: 1942-1956
15 Wingo PA, Tong T, Bolden S. Cancer stati stics, 1995. CA
Cancer J Clin 1995; 45: 8-30
16 El-Serag HB, Mason AC. Rising incidence of hepatocellular
carcinoma in the United States. N Engl J Med 1999; 340:
745-750
17 Allen J, Venook A. Hepatocellular carcinoma: epidemic and
treatment. Curr Oncol Rep 2004; 6: 177-183
18 Tanaka Y, Hanada K, Mizokami M, Yeo AE, Shih JW,
Gojobori T, Alter HJ. Inaugural Article: A comparison of the
molecular clock of hepatitis C virus in the United States and
Japan predicts that hepatocellular carcinoma incidence in
the United States will increase over the next two decades.
Proc Natl Acad Sci USA 2002; 99: 15584-15589
19 Bolondi L, Sofia S, Siringo S, Gaiani S, Casali A, Zironi
G, Piscaglia F, Gramantieri L, Zanetti M, Sherman M.
Surveillance programme of cirrhotic patients for early
diagnosis and treatment of hepatocellular carcinoma: a cost
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 23/52
Page 23 of 52
[Type text] Page 23
effectiveness analysis. Gut 2001; 48: 251-259
20 Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma.
Lancet 2003; 362: 1907-1917
21 Makuuchi M, Sano K. The surgical approach to HCC: our
progress and results in Japan. Liver Transpl 2004; 10: S46-S52
22 Shimozawa N, Hanazaki K. Longterm prognosis after
3214 ISSN 1007-9327 CN 14-1219/R World J Gastroenterol July 14, 2009 Volume 15 Number 26
www.wjgnet.com
hepatic resection for small hepatocellular carcinoma. J Am
Coll Surg 2004; 198: 356-365
23 Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti
A, Bozzetti F, Montalto F, Ammatuna M, Morabito A,
Gennari L. Liver transplantation for the treatment of small
hepatocellular carcinomas in patients with cirrhosis. N Engl
J Med 1996; 334: 693-699
24 Bruix J, Sherman M. Management of hepatocellular
carcinoma. Hepatology 2005; 42: 1208-1236
25 Tang ZY. Hepatocellular carcinoma--cause, treatment and
metastasis. World J Gastroenterol 2001; 7: 445-454
26 Tang ZY. Hepatocellular carcinoma. J Gastroenterol Hepatol
2000; 15 Suppl: G1-G7
27 Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni
R, Zhu AX, Sherman M, Schwartz M, Lotze M, Talwalkar
J, Gores GJ. Design and endpoints of clinical trials in
hepatocellular carcinoma. J Natl Cancer Inst 2008; 100: 698-711
28 Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni
R, Burroughs AK, Christensen E, Pagliaro L, Colombo M,
Rodés J. Clinical management of hepatocellular carcinoma.
Conclusions of the Barcelona-2000 EASL conference.
European Association for the Study of the Liver. J Hepatol
2001; 35: 421-430
29 Marrero JA, Fontana RJ, Barrat A, Askari F, Conjeevaram
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 24/52
Page 24 of 52
[Type text] Page 24
HS, Su GL, Lok AS. Prognosis of hepatocellular carcinoma:
comparison of 7 staging systems in an American cohort.
Hepatology 2005; 41: 707-716
30 Cillo U, Vitale A, Grigoletto F, Farinati F, Brolese A, Zanus
G, Neri D, Boccagni P, Srsen N, D'Amico F, Ciarleglio
FA, Bridda A, D'Amico DF. Prospective validation of the
Barcelona Clinic Liver Cancer staging system. J Hepatol 2006;
44: 723-731
31 Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc
JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz
M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz
JF, Borbath I, Häussinger D, Giannaris T, Shan M, Moscovici
M, Voliotis D, Bruix J. Sorafenib in advanced hepatocellular
carcinoma. N Engl J Med 2008; 359: 378-390
32 Llovet JM, Bruix J. Molecular targeted therapies in
hepatocellular carcinoma. Hepatology 2008; 48: 1312-1327
33 Buell JF, Rosen S, Yoshida A, Labow D, L imsrichamrern
S, Cronin DC, Bruce DS, Wen M, Michelassi F, Millis JM,
Posner MC. Hepatic resection: effective treatment for
primary and secondary tumors. Surgery 2000; 128: 686-693
34 De Carlis L, Giacomoni A, Pirotta V, Lauterio A, Slim AO,
Sammartino C, Cardillo M, Forti D. Surgical treatment of
hepatocellular cancer in the era of hepatic transplantation. J
Am Coll Surg 2003; 196: 887-897
35 Vauthe y JN, Cha oui A, Do KA, Bi l imo r i a MM,
Fenstermacher MJ, Charnsangavej C, Hicks M, Alsfasser
G, Lauwers G, Hawkins IF, Caridi J. Standardized
measurement of the future liver remnant prior to extended
liver resection: methodology and clinical associations.
Surgery 2000; 127: 512-519
36 Farges O, Belghiti J, Kianmanesh R, Regimbeau JM,
Santoro R, Vilgrain V, Denys A, Sauvanet A. Portal vein
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 25/52
Page 25 of 52
[Type text] Page 25
embolization before right hepatectomy: prospective clinical
trial. Ann Surg 2003; 237: 208-217
37 Oldhafer KJ, Lang H, Malagó M, Testa G, Broelsch CE. [Ex
situ resection and resection of the in situ perfused liver: are
there still indications?] Chirurg 2001; 72: 131-137
38 Tsuzuki T, Sugioka A, Ueda M, Iida S, Kanai T, Yoshii H,
Nakayasu K. Hepatic resection for hepatocellular carcinoma.
Surgery 1990; 107: 511-520
39 Yamanaka N, Okamoto E, Toyosaka A, Mitunobu M,
Fujihara S, Kato T, Fujimoto J, Oriyama T, Furukawa K,
Kawamura E. Prognostic factors after hepatectomy for
hepatocellular carcinomas. A univariate and multivariate
analysis. Cancer 1990; 65: 1104-1110
40 Bismuth H, Chiche L, Castaing D. Surgical treatment of
hepatocellular carcinomas in noncirrhotic liver: experience
with 68 liver resections. World J Surg 1995; 19: 35-41
41 Fong Y, Sun RL, Jarnagin W, Blumgart LH. An analysis of
412 cases of hepatocellular carcinoma at a Western center.
Ann Surg 1999; 229: 790-799; discussion 799-800
42 Marín-Hargreaves G, Azoulay D, Bismuth H. Hepatocellular
carcinoma: surgical indications and results. Crit Rev Oncol
Hematol 2003; 47: 13-27
43 Ringe B, Weimann A, Tusch G, Pichlmayr R. Resection
versus transplantation for malignancy of liver and bile
duct. In: Wanebo HJ, ed. Surgery for gastrointestinal cancer.
Philadelphia: Lippincott-Raven, 1997: 513-524
44 Pawlik TM, Delman KA, Vauthey JN, Nagorney DM, Ng IO,
Ikai I, Yamaoka Y, Belghiti J, Lauwers GY, Poon RT, Abdalla
EK. Tumor size predicts vascular invasion and histologic
grade: Implications for selection of surgical treatment for
hepatocellular carcinoma. Liver Transpl 2005; 11: 1086-1092
45 Bismuth H, Chiche L, Adam R, Castaing D, Diamond T,

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 26/52
Page 26 of 52
[Type text] Page 26
Dennison A. Liver resection versus transplantation for
hepatocellular carcinoma in cirrhotic patients. Ann Surg
1993; 218: 145-151
46 Achkar JP, Araya V, Baron RL, Marsh JW, Dvorchik I,
Rakela J. Undetected hepatocellular carcinoma: clinical
features and outcome after liver transplantation. Liver
Transpl Surg 1998; 4: 477-482
47 Ojogho ON, So SK, Keeffe EB, Berquist W, Concepcion W,
Garcia-Kennedy R, Imperial J, Esquivel CO. Orthotopic
liver transplantation for hepatocellular carcinoma. Factors
affecting long-term patient survival. Arch Surg 1996; 131:
935-939; discussion 939-941
48 Molmenti EP, Klintmalm GB. Liver transplantation in
association with hepatocellular carcinoma: an update of the
International Tumor Registry. Liver Transpl 2002; 8: 736-748
49 Plessier A, Codes L, Consigny Y, Sommacale D, Dondero F,
Cortes A, Degos F, Brillet PY, Vilgrain V, Paradis V, Belghiti
J, Durand F. Underestimation of the influence of satellite
nodules as a risk factor for post-transplantation recurrence
in patients with small hepatocellular carcinoma. Liver
Transpl 2004; 10: S86-S90
50 Jonas S, Bechstein WO, Steinmüller T, Herrmann M, Radke
C, Berg T, Settmacher U, Neuhaus P. Vascular invasion
and histopathologic grading determine outcome after liver
transplantation for hepatocellular carcinoma in cirrhosis.
Hepatology 2001; 33: 1080-1086
51 Bruix J, Fuster J, Llovet JM. Liver transplantation for
hepatocellular carcinoma: Foucault pendulum versus
evidence-based decision. Liver Transpl 2003; 9: 700-702
52 Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook
A, Ascher NL, Roberts JP. Liver transplantation for
hepatocellular carcinoma: expansion of the tumor size limits

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 27/52
Page 27 of 52
[Type text] Page 27
does not adversely impact survival. Hepatology 2001; 33:
1394-1403
53 Yao FY, Bass NM, Nikolai B, Davern TJ, Kerlan R, Wu
V, Ascher NL, Roberts JP. Liver transplantation for
hepatocellular carcinoma: analysis of survival according
to the intention-to-treat principle and dropout from the
waiting list. Liver Transpl 2002; 8: 873-883
54 Roayaie S, Haim MB, Emre S, Fishbein TM, Sheiner PA,
Miller CM, Schwartz ME. Comparison of surgical outcomes
for hepatocellular carcinoma in patients with hepatitis B
versus hepatitis C: a western experience. Ann Surg Oncol
2000; 7: 764-770
55 Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M,
Mariani L, Camerini T, Roayaie S, Schwartz ME, Grazi GL,
Adam R, Neuhaus P, Salizzoni M, Bruix J, Forner A, De
Carlis L, Cillo U, Burroughs AK, Troisi R, Rossi M, Gerunda
GE, Lerut J, Belghiti J, Boin I, Gugenheim J, Rochling
F, Van Hoek B, Majno P. Predicting survival a fter liver
transplantation in patients with hepatocellular carcinoma
beyond the Milan criteria: a retrospective, exploratory
analysis. Lancet Oncol 2009; 10: 35-43
56 Sarasin FP, Giostra E, Mentha G, Hadengue A. Partial
hepatectomy or orthotopic liver transplantation for the
treatment of resectable hepatocellular carcinoma? A cost-
Rampone B et al . Hepatocellular carcinoma 3215
www.wjgnet.com
effectiveness perspective. Hepatology 1998; 28: 436-442
57 Saab S, Wang V, Ibrahim AB, Durazo F, Han S, Farmer DG,
Yersiz H, Morrisey M, Goldstein LI, Ghobrial RM, Busuttil
RW. MELD score predicts 1-year patient survival postorthotopic
liver transplantation. Liver Transpl 2003; 9: 473-476
58 Yao FY, Bass NM, Ascher NL, Roberts JP. Liver transplantation

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 28/52
Page 28 of 52
[Type text] Page 28
for hepatocellular carcinoma: lessons from the first year
under the Model of End-Stage Liver Disease (MELD) organ
allocation policy. Liver Transpl 2004; 10: 621-630
59 Helton WS, Di Bisceglie A, Chari R, Schwartz M, Bruix
J. Treatment strategies for hepatocellular carcinoma in
cirrhosis. J Gastrointest Surg 2003; 7: 401-411
60 Bruix J, Llovet JM. Prognostic prediction and treatment
strategy in hepatocellular carcinoma. Hepatology 2002; 35:
519-524
61 Van Kleek EJ, Schwartz JM, Rayhill SC, Rosen HR, Cotler
SJ. Liver transplantation for hepatocellular carcinoma: a
survey of practices. J Clin Gastroenterol 2006; 40: 643-647
62 Pomfret EA. Early and late complications in the right-lobe
adult living donor. Liver Transpl 2003; 9: S45-S49
63 Cuomo O, Perrella A, Pisaniello D, Marino G, Di Costanzo
G. Evidence of liver histological alterations in apparently
healthy individuals evaluated for living donor liver
transplantation. Transplant Proc 2008; 40: 1823-1826
64 Broering DC, Wilms C, Bok P, Fischer L, Mueller L, Hillert
C, Lenk C, Kim JS, Sterneck M, Schulz KH, Krupski G,
Nierhaus A, Ameis D, Burdelski M, Rogiers X. Evolution
of donor morbidity in living related liver transplantation:
a single-center analysis of 165 cases. Ann Surg 2004; 240:
1013-1024; discussions 1024-1026
65 Trotter JF, Wachs M, Everson GT, Kam I. Adult-to-adult
transplantation of the right hepatic lobe from a living donor.
N Engl J Med 2002; 346: 1074-1082
66 Umeshita K, Fujiwara K, Kiyosawa K, Makuuchi M, Satomi
S, Sugimachi K, Tanaka K, Monden M. Operative morbidity
of living liver donors in Japan. Lancet 2003; 362: 687-690
67 Livraghi T, Giorgio A, Marin G, Salmi A, de Sio I,
Bolondi L, Pompili M, Brunello F, Lazzaroni S, Torzilli G.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 29/52
Page 29 of 52
[Type text] Page 29
Hepatocellular carcinoma and cirrhosis in 746 patients:
long-term results of percutaneous ethanol injection.
Radiology 1995; 197: 101-108
68 Ryu M, Shimamura Y, Kinoshita T, Konishi M, Kawano
N, Iwasaki M, Furuse J, Yoshino M, Moriyama N, Sugita
M. Therapeutic results of resection, transcatheter arterial
embolization and percutaneous transhepatic ethanol
injection in 3225 patients with hepatocellular carcinoma: a
retrospective multicenter study. Jpn J Clin Oncol 1997; 27:
251-257
69 Lau H, Fan ST, Ng IO, Wong J. Long term prognosis after
hepatectomy for hepatocellular carcinoma: a survival analysis
of 204 consecutive patients. Cancer 1998; 83: 2302-2311
70 Lin SM, Lin CJ, Lin CC, Hsu CW, Chen YC. Radiofrequency
ablation improves prognosis compared with ethanol
injection for hepatocellular carcinoma < or =4 cm.
Gastroenterology 2004; 127: 1714-1723
71 Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L,
Gazelle GS. Small hepatocellular carcinoma: treatment with
radio-frequency ablation versus ethanol injection. Radiology
1999; 210: 655-661
72 Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern
EF, Goldberg SN. Treatment of focal liver tumors with
percutaneous radio-frequency ablation: complications
encountered in a multicenter study. Radiology 2003; 226:
441-451
73 Llovet JM, Real MI, Montaña X, Planas R, Coll S, Aponte J,
Ayuso C, Sala M, Muchart J, Solà R, Rodés J, Bruix J. Arterial
embolisation or chemoembolisation versus symptomatic
treatment in patients with unresectable hepatocellular
carcinoma: a randomised controlled trial. Lancet 2002; 359:
1734-1739
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 30/52
Page 30 of 52
[Type text] Page 30
74 Llovet JM, Bruix J. Systematic r eview of randomized trials for
unresectable hepatocellular carcinoma: Chemoembolization
improves survival. Hepatology 2003; 37: 429-442
75 Poon RT, Fan ST, Tsang FH, Wong J. Locoregional therapies
for hepatocellular carcinoma: a critical review from the
surgeon's perspective. Ann Surg 2002; 235: 466-486
76 Lo CM, Ngan H, Tso WK, Liu CL, Lam CM, Poon RT, Fan
ST, Wong J. Randomized controlled trial of transarterial
lipiodol chemoembolization for unresectable hepatocellular
carcinoma. Hepatology 2002; 35: 1164-1171
77 Ferrari FS, Stella A, Pasquinucci P, Vigni F, Civeli L,
Pieraccini M, Magnolfi F. Treatment of small hepatocellular
carcinoma: a comparison of techniques and long-term
results. Eur J Gastroenterol Hepatol 2006; 18: 659-672
78 Schwartz JD, Schwartz M, Mandeli J, Sung M. Neoadjuvant
and adjuvant therapy for resectable hepatocellular
carcinoma: review of the randomised clinical trials. Lancet
Oncol 2002; 3: 593-603
79 Chow PK, Tai BC, Tan CK, Machin D, Win KM, Johnson PJ,
Soo KC. High-dose tamoxifen in the treatment of inoperable
hepatocellular carcinoma: A multicenter randomized
controlled trial. Hepatology 2002; 36: 1221-1226
80 Yuen MF, Poon RT, Lai CL, Fan ST, Lo CM, Wong KW,
Wong WM, Wong BC. A randomized placebo-controlled
study of long-acting octreotide for the treatment of
advanced hepatocellular carcinoma. Hepatology 2002; 36:
687-691
81 Villanueva A, Newell P, Chiang DY, Friedman SL, Llovet
JM. Genomics and signaling pathways in hepatocellular
carcinoma. Semin Liver Dis 2007; 27: 55-76
S- Editor Cheng JX L- Editor Webster JR E- Editor Zheng XM
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 31/52
Page 31 of 52
[Type text] Page 31
J Gastroenterol 2009; 44[Suppl XIX]:136±141DOI 10.1007/s00535-008-2252-z
Molecular targeted therapy f or
hepat o
cell
ul
ar carcinom
aM ELANIE T HOMAS
Di vi s i on of Hematology/ O n cology Hol l i n gs Can cer Cen ter , Medi cal Un i vers i ty of S ou th Carol i n a ,
Charleston , S C 29425, US A
A majority of patients with HCC present with advanced
disease and are not candidates for liver transplantation,
surgical resection, or regional therapy. Systemic
cytotoxic chemotherapy agents are minimally effective,
can have significant toxicity, and have not been
shown to improve patient survival. Hepatocellular carcinomas
are inherently chemotherapy-resistant tumors
and are known to overexpress the multidrug resistance
genes. Hepatocellular carcinoma is a very heterogeneous
disease in terms of its etiology, molecular carcinogenic
mechanisms, and biological behavior, which
complicate our ability to identify rational molecular
therapeutic targets. Nearly every pathway involved
in carcinogenesis is altered to some degree in HCC.
Changes in hepatocyte growth factor expression, intracellular
signaling, protease and matrix metalloproteinase
expression, and oncogene expression are seen in
HCC. The recent demonstration, in randomized clinical
trials, of survival benefit for HCC patients treated with
the oral agent sorafenib is encouraging progress in the
development of molecularly targeted anticancer agents in HCC.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 32/52
Page 32 of 52
[Type text] Page 32
Key words: hepatocellular carcinoma, HCC, chemotherapy,
targeted therapy
Introduction
Hepatocellular carcinoma (HCC) is potentially curable
by surgical resection and liver transplantation. However,
the majority of patients present with advanced-stage
disease, which is most commonly accompanied by severe
background liver disease. Hence, surgery is feasible for
only a small fraction of patients with localized disease,
and liver transplantation is severely limited by the availability
of liver donors. Systemic cytotoxic therapies
have demonstrated a very limited impact on the natural
history of advanced HCC (Table 1). A 1997 metaanalysis
evaluating the results of 37 randomized clinical
trials of systemic and regional chemotherapy in 2803
HCC patients concluded that nonsurgical therapies
were ineffective or minimally effective at best.1
Chemotherapy resistance in HCC
Cancer cells, including HCC cells, often have intrinsic
drug resistance mediated via enhanced cellular drug
effl ux of several cytotoxic agents. This phenomenon is
associated with increase in a drug transporter family,
the adenosine triphosphate-binding cassette proteins
that include MDR1, p-glycoprotein (p-gp), and the
multidrug resistance protein (MRP). 2,3 Both these are
upregulated in HCC. 2,4 Upregulation of MDR1 accompanied
by a decrease in doxorubicin accumulation levels
has been reported in certain HCC cell lines. 5 Th e H19

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 33/52
Page 33 of 52
[Type text] Page 33
gene is thought to induce p-gp expression and MDR1-
associated drug resistance in HCC cells through
regulating MDR1 promoter methylation.5 Also, coexpression
of p53 and p-gp may contribute to HCC chemoresistance
in HCC cell lines. 6 In addition, recent
evidence suggests that hypoxia, MDR1 expression, and
an angiogenic HCC phenotype may be interacting. 7, 8
Topoisomerase IIa encodes an enzyme that is the
target for anticancer chemotherapeutic agents such as
doxorubicin, and mutations are associated with resistance.
9 There is upregulation of topoisomerase IIa in
doxorubicin-resistant HCC cell lines, and its expression
is associated with an aggressive tumor phenotype. 10
Finally, large HCCs commonly develop areas of central
necrosis, which may interfere with drug delivery to the
growing tumor.
Received: June 24, 2008 / Accepted: July 3 , 2008
Reprint requests to: M. Thomas
M. Thomas: Molecular targeted therapy for HCC 137
Thus, to improve the outcome for patients with
advanced HCC, alternatives to traditional cytotoxic
chemotherapy agents are clearly needed. Recently,
molecular characterization of HCC has led to the
recognition of defined aberrant signaling pathways,
which helped in subsequent development of targeted
agents as potential choices for the treatment of this
disease.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 34/52
Page 34 of 52
[Type text] Page 34
M olecular therapeutic targets in
hepatocellular carcinoma
In HCC, several crucial intracellular signaling pathways
such as the Ras/Raf/Mek/Erk pathway and PI3k/Akt/
mTOR pathway, in addition to several growth and
angiogenic factors/receptors such as epidermal growth
factor receptor (EGFR), platelet-derived growth factor
receptor (PDGFR), fibroblast growth factor receptor
(FGFR), and vascular endothelial growth factor receptor
(VEGFR), have been recognized. Subsequently,
targeted agents have entered clinical trials in HCC
patients, and this is of particular signifi cance for HCC
in light of the lack of existing effective systemic therapy
for this cancer.
The growth of HCC depends on stimulatory effects
of various growth factors, which bind to tyrosine kinase
receptors and hence activate various intracellular signaling
pathways that subsequently lead to tumor cell
proliferation, survival, migration, and metastasis. Both
the extracellular growth factors and the intracellular
signaling pathways represent potential molecular targets
for therapy of HCC. H owever, the antiangiogenic
pathway looks promising in HCC.
T argeting growth factors in hepatocellular carcinoma
The epidermal growth factor receptor (EGFR) is frequently
expressed in human hepatoma cells, and EGF
may be one of the mitogens needed for the growth of

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 35/52
Page 35 of 52
[Type text] Page 35
hepatoma cells.11,12 Several strategies have been tested
in HCC: one is through using a neutralizing monoclonal
antibody such as cetuximab, and another is using a small
molecule tyrosine kinase inhibitor such as gefi tinib
and erlotinib, as demonstrated in HCC cell cultures.13,14
Erlotinib is an orally active and selective inhibitor of the
EGFR/HER1-related tyrosine kinase enzyme. EGFR/
HER1 expression was detected in 88% of the patients
in a phase II study of erlotinib. 15 In two phase II studies
T able 1. Summary of selected cl inical trials in patients with advanced hepatocel lular carcinoma
(HCC)
Study Regimen Phase Sample size
Response rate
(% )
Median survival
(months)
Cytotoxic chemotherapy
Y eo et al . 59 PIAF vs. adriamycin 3 94/94 20.9 vs . 10.5 8 .6 vs . 6 .83
Mok et al . 60 Nolatrexed vs .
doxorubicin
2 37/17 0 4.9 vs . 3 . 7
Posey et al . 61 TI38067 vs. adriamycin 2/3 169/170 NA 5.7 vs . 5 .6
Gish et al . 62 Nolatrexed vs .
doxorubicin
3 444 1.4 vs . 4 .0 5 .5 vs . 8 ( P ! 0.0068)
Patt et al . 30 Thalidomide 2 37 6% 6.8
Pastorel l i et al . 63 Pegylated doxorubicin
gemcitabine
2 35 23% 8.8
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 36/52
Page 36 of 52
[Type text] Page 36
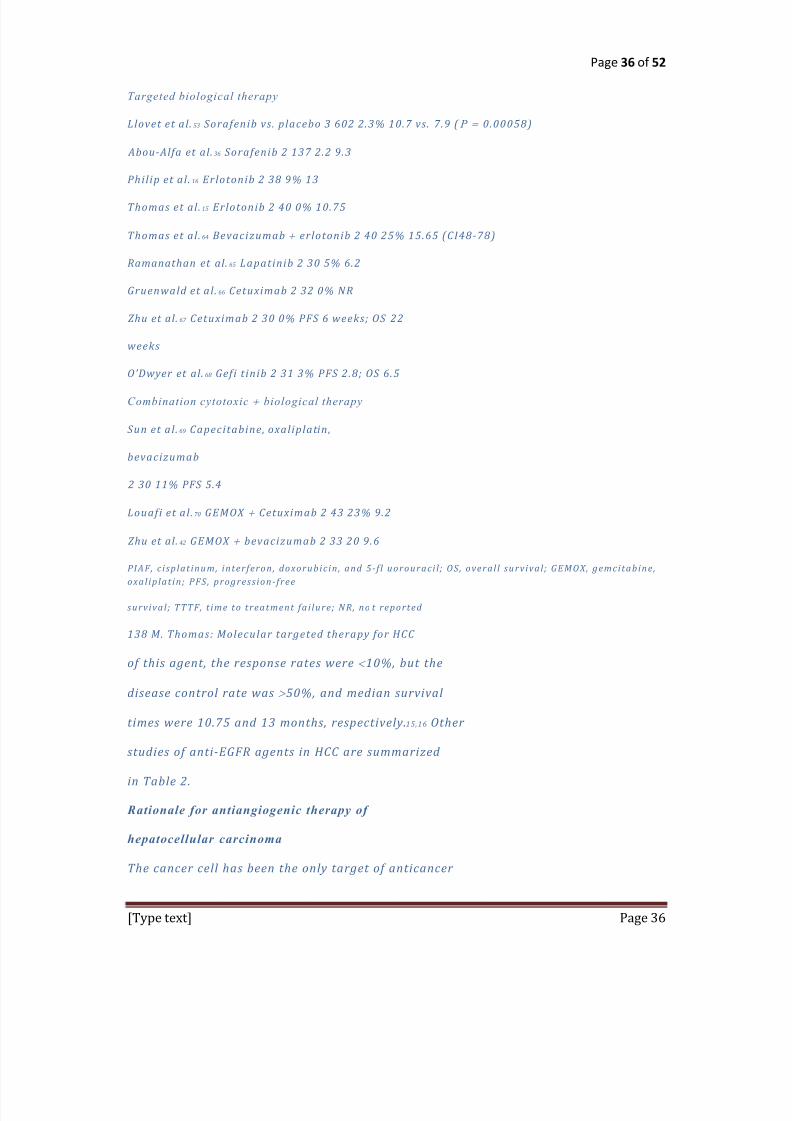
Targeted biological therapy
Llovet et al . 53 Sorafenib vs . placebo 3 602 2.3% 10.7 vs . 7 .9 ( P !0.00058)
Abou-Alfa et al . 36 Sorafenib 2 137 2.2 9 .3
Phil ip et al . 16 Erlotonib 2 38 9% 13
Thomas et al . 15 Erlotonib 2 40 0% 10.75
Thomas et al . 64 Bevacizumab erlotonib 2 40 25% 15.65 (CI48-78)
Ramanathan et al . 65 Lapatinib 2 30 5% 6.2
Gruenwald et al . 66 Cetuximab 2 32 0% NR
Zhu et al . 67 Cetuximab 2 30 0% PFS 6 weeks; OS 22
weeks
ODwyer et al . 68 Gefi t inib 2 31 3% PFS 2.8; OS 6.5
Combination cytotoxic biological therapy
Sun et al . 69 Capecitabine, oxal iplatin,
bevacizumab
2 30 11% PFS 5.4
Louafi et al . 70 GEMOX Cetuximab 2 43 23% 9.2
Zhu et al . 42 GEMOX bevacizumab 2 33 20 9.6
PIAF, c i splat i n u m, i n terferon , dox oru bi c i n , an d 5-f l u orou raci l ; O S , overal l su rvi val ; GE MO X, gemci tabi n e ,ox al i plat i n ; PFS , progress i on -free
su rvi val ; TTTF, t i me to treatmen t fai lu re; NR, n o t reported
138 M. Thomas: Molecular targeted therapy for HCC
of this agent, the response rates were 10%, but the
disease control rate was " 50%, and median survival
times were 10.75 and 13 months, respectively.15,16 Other
studies of anti-EGFR agents in HCC are summarized
in Table 2.
Rationale for antiangiogenic therapy of
hepatocellular carcinoma
The cancer cell has been the only target of anticancer
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 37/52
Page 37 of 52
[Type text] Page 37
therapy for more than 50 years. However, the cancer
cell is genetically unstable, and mutations accumulate.
On the other hand, antiangiogenic therapy targets
endothelial cells that are genetically stable. The genetic
stability of endothelial cells may make them less
susceptible to acquired drug resistance. As a result,
angiogenesis inhibitors are emerging as a new class of
therapeutic agents.
The role of angiogenesis in the initial progression
from a premalignant tumor to a cancer prompted investigators
to study the role of VEGF in the natural history
of HCC.17 In 1999, a group of researchers suggested that
the degree of tissue VEGF expression increased according
to the stepwise development of HCC. 18 In addition,
studies have shown that VEGF was frequently expressed
in HCC. In a quantitative analysis study, VEGF expression
was demonstrated in 63.9% of encapsulated HCC
and 78.3% of nonencapsulated HCC. 19 Another stud y
reported VEGF tissue expression in HCC of 88.8%. 20
Notably, studies have suggested a correlation between
the degree of tissue VEGF expression and the intensity
of both the magnetic resonance signal and the computed
tomographic enhancement of the hepatic artery,
which represent radiologic vascular signals. 2123 Hence,
the hypervascular nature of HCC has led to increasing
interest in exploring the potential of antiangiogenic
therapy in this disease.
T able 2. Ongoing cl inical trials of systemic antiangiogenic therapy in HCC

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 38/52
Page 38 of 52
[Type text] Page 38
Regimen
Study
phase Patient population Trial #/s ponsor
AZD2171 II Unresectable or metastatic HCC NCT00238394
NC I
AZD-2171 II Unresectable local ly advanced or
metastatic HCC
NCT00427973a
Massachusetts General Hospital/NCI
Bevacizumab II Unresectable or m etastatic HCC NCT00162669
Institute Gusatve Roussy
Bevacizumab Erlotinib II Unresectable HCC N CT00242502
M.D. Anderson Cancer Center
Bevacizumab Erlotinib II Unresectable or metastatic HCC NCT00287222
University of Arkansas/Genentech
Bevacizumab Erlotinib II Advanced unresectable HCC NCT 00365391
Mayo Cl inic/NCI
Bevacizumab Sirol imus I Unresectable local ly advanced or
metastatic HCC
NCT00467194
NC I
BMS-582664 vs. Doxorubicin II Unresectable, local ly advanced or
metastatic HCC
NCT00355238
Bristol-Myers Squibb
BMS-582664 I Advanced HCC with varying
levels of hepatic impairment
NCT00437424a
Bristol-Myers Squibb
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 39/52
Page 39 of 52
[Type text] Page 39
Sorafenib tegafur/uracil
(UFUR)
II Unresectable local ly advanced or
metastatic HCC
NCT00464919
National Taiwan University Hospital
Doxorubicin ssorafenib II Unresectable or metastatic HCC NCT00108953b
Bayer
Pazopanib I HCC NCT00370513
GlaxoSmithKline
Sunitinib II Unresectable local ly advanced or
metastatic HCC
NCT00361309
Massachusetts General Hospital
Sunitinib II Unresectable HCC NCT00247676
Pfi zer
Thalidomide III Local ly advanced or metastatic
HC C
NCT00225290
TT Y Biopharm
Thalidomide tegafur/uracil
(UFUR)
II Unresectable local ly advanced or
metastatic HCC
NCT00384800
Far Eastern Memorial Hospital
a Not open yet
b No lon ger recru i t i n g pat i en ts
M. Thomas: Molecular targeted therapy for HCC 139
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 40/52
Page 40 of 52
[Type text] Page 40
Clinical trials of antiangiogenic agents in
hepatocellular carcinoma
Several vascular targeted agents, including thalidomide,
sunitinib, sorafenib, and bevacizumab, have been tested
in advanced HCC (see Tables 1, 2). The thalidomide
mechanism was not clearly known but was thought to
be partly based on its antiangiogenic effects. 2426 Nevertheless,
several clinical trials of thalidomide alone or in
combination with epirubicin or interferon showed rare
responses ranging from 0% to 6.3%. 2733 A recent report
in abstract form of 19 patients treated with oral thalidomide
200 mg/day continuously showed a 6-month
progression-free survival of 41%.34
Sunitinib, an oral multikinase inhibitor, exerts an
antiangiogenic effect by targeting VEGFR and plateletderived
growth factor receptor (PDGFR) tyrosine
kinases. A phase II study of sunitinib alone in 19 patients
with unresectable or metastatic HCC reported a partial
response in 1 patient.35
Sorafenib, an oral multikinase inhibitor, exerts an
antiangiogenic effect by targeting VEGFR and PDGFR
tyrosine kinases. It exerts its effect through targeting
Raf/MEK/ERK signaling at the level of Raf kinase and
exerts an antiangiogenic effect by targeting VEGFR-2/
-3. A phase II study of Sorafenib alone in advanced
HCC showed 2.2% partial and 5.8% minor response.36
Recently, a randomized, placebo-controlled phase III
trial of Sorafenib in advanced HCC reported a 2.8-

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 41/52
Page 41 of 52
[Type text] Page 41
month improvement in median overall survival [hazard
ratio (HR), 0.69; 95% confi dence interval (CI), 0.55
0.87; P !0.0006] along with increased time to progression
and disease control rate. 37
Bevacizumab is a recombinant, humanized monoclonal
antibody that targets VEGF and may augment chemotherapy
administration by making tumor vasculature
less permeable and decreasing the elevated tumor interstitial
pressure.38,39 Two recent phase II trials of bevacizumab
alone in advanced HCC suggested an improved
disease control, with one reporting a partial response
rate of 12.5% with a disease control rate (PR SD) of
67%.40,41 Bevacizumab was also combined with gemcitabine
and oxaliplatin in a phase II trial of advanced
HCC with an overall response rate of 20%. 42 A phase
II trial of bevacizumab capecitabine as a fi rst-line
treatment for advanced HCC recently reported a
response rate (CR PR) of 16% (95% CI, 4.5%36.1%)
and disease control rate (CR PR SD) of 60% (95%
CI, 38.7%78.9%), with a median overall survival of
10.7 months (95% CI, 5.314.7) and median progression-
free survival (PFS) o f 4.1 months. 43 In addition, a
phase II study of advanced or unresectable metastatic
HCC treating 30 patients with bevacizumab, oxaliplatin,
and capecitabine reported an 11% response rate with
mean PFS of 5.4 months.44 An ongoing phase II, singlearm,
open-label trial of bevacizumab and erlotinib in 29
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 42/52
Page 42 of 52
[Type text] Page 42
patients with unresectable HCC recently showed a 22%
response rate.45
There is a number of ongoing clinical trials of different
vascular targeted agents in HCC (see Table 2). Preclinical
studies of agents that target other foci which
interact with VEGF, such as hypoxia-inducible factor
(HIF)-1 alpha and APRIL (a proliferation-inducing
ligand), have shown promising results with reduced
VEGF expression in HCC cell cultures.46,47
Additional molecular pathways targeted in HCC
clinical trials
Mitogen-activated protein kinase pathway
The mitogen-activated protein kinase (MAPK) pathway
includes a cascade of phosphorylation of four major
cellular kinases, ras, raf, mitogen-activated protein
kinase (MAP), and extracellular signal-regulated kinase
(ERK), which is responsible mainly for cellular differentiation
and proliferation signal transduction. These
intermediates are found to be high in both HCC cell
lines and human specimens.4851 Notably, for Ras proteins
to be competent for signal transduction, posttranslational
modifi cation by incorporation of farnesyl and
geranylgeranyl groups is required. One of the inhibitors
of farnesyl transferase has been developed to prevent
prenylation of Ras proteins: ABT-100, which has
been shown to prevent the development of chemically
induced HCC in rats. 52 Raf kinase inhibitor Bay-439006
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 43/52
Page 43 of 52
[Type text] Page 43
(sorafenib), a therapeutic agent that targets this pathway,
is currently the most promising molecular targeting
drug for HCC that has undergone phase I, II, and III
trials. It targets both raf and vascular endothelial growth
factor receptor (VEGFR). A phase II trial of sorafenib
demonstrated antitumor activity in advanced HCC
patients. This study did not meet its primary endpoint
of response on the basis of World Health Organization
(WHO) criteria, with a response rate of 2.2%.
However, 33.6% of patients had stable disease for at
least 4 months, with many showing central tumor necrosis.
36 On the basis of the encouraging overall survival of
9.2 months reported in the phase II trial, a placebocontrolled
international trial was completed in HCC
patients with ChildsPugh A cirrhosis.53 The results
concluded that sorafenib offers a survival advantage
compared with placebo (10.7 months vs. 7.9 months,
HR 0.69; 95% CI, 0.55 to 0.87). This may be comparable
to survival observed with other biological agents (see
Table 2).
140 M. Thomas: Molecular targeted therapy for HCC
PI3K/AKT/mTOR pathway (phosphoinositid e-3 kinase/
protein kinase B/mammalian target
of rapamycin)
Activation of PI3K subsequently activates Akt kinase,
which phosphorylates and inactivates several proapoptotic
proteins. This activity in turn leads to a number of
downstream events that are responsible for cellular proliferation
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 44/52
Page 44 of 52
[Type text] Page 44
and apoptosis and is closely linked to the cell
cycle.54,55 This pathway is known to be upregulated in a
subset of HCC patients. Furthermore, mTOR is a downstream
of Akt that regulates cellular translational activities
through the eukaryotic initiation factor 4E-binding
protein-1 (4E-BP1) and the 40s ribosomal protein S6
kinase (p70s6k); these are linked with the translation of
mRNAs of genes regulating cell proliferation and angiogenesis,
such as c-my c , cyclin D1, a nd HIF-1£ .56 Rapamycin
is an antibiotic that inhibits mTOR and is clinically
used as an immunosuppressive drug to prevent graft
rejection. It was shown to possess activity against HCC
cell lines.57,58
References
1. S i mon ett i RG, L i berat i A , An gi ol i n i C , et a l . Treatmen t of hepato cel lu lar
carc i n oma: a systemati c revi ew of ran domi zed con trol led
tr i als . An n O n col 1997;8:117 36.
2 . Ng IO , L i u CL , Fan S T , et a l . E x p ress i on of P-g lycopro tei n
i n hepatocel lu lar carc i n oma. A determi n an t of chemotherapy
respon se . Am J C l i n Pathol 2000;113:355 63.
3 . E n di cott JA , L i n g V . The b i ochemi stry of P-g lycopro tei n medi ated
mu lt i dru g res i s tan ce . An n u Rev Bi ochem 1989;58:137
71 .
4 . Park JG, Lee S K , Hon g IG, et a l . MDR1 gen e ex press i on : i t s
ef fect on dru g res i s tan ce to dox oru bi c i n i n hu man hepatocel lu lar
carc i n oma cel l l i n es . J Nat l Can cer In st 1994;86:700 5.
5 . Tsan g WP, K w ok TT. R i boregu lator H19 i n du ct i on of MDR1-
assoc i ated dru g res i s tan ce i n hu man hepatocel lu lar carc i n oma
cel ls . O n cogen e 2007;26:4877 81.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 45/52
Page 45 of 52
[Type text] Page 45
6. Chan K T, Lu n g ML. Mu tan t p53 ex press i on en han ces dru g res i s tan ce
i n a hepatocel lu lar carc i n oma cel l l i n e . Can cer Chemother
Pharmacol 2004;53:519 26.
7 . Lasagn a N, Fan tappi e O , S olazzo M, et a l . Hepatocyte grow th
factor an d i n du ci b le n i tr i c ox i de syn th ase are i n volve d i n mu lt i dru g
res i s tan ce- i n du ced an gi ogen es i s i n hepatocel lu lar carc i n oma
cel l l i n es . Can cer Res 2006;66:2673 82.
8 . Zhu H, Chen XP , Lu o S F , et a l . In volve men t of hypox i a- i n du ci b le
factor-1-alpha i n mu lt i dru g res i s tan ce i n du ced by h ypox i a i n
HepG2 cel ls . J E x p C l i n Can cer Res 2005;24:565 74.
9 . O k a d a Y , Tosaka A , Ni mu r a Y , e t a l . Atypi cal mu l t i dru g res i s tan ce
may be assoc i ated w i th catalyt i cal ly ac t i ve mu tan ts of
hu man DNA topoi somerase I I a lpha. Gen e (Amst) 2001;272:
141 8.
10. Watan u ki A , O hw ada S , Fu ku sa to T , et a l . Progn ost i c s i gn i f i can ce
of DNA topoi somerase I I a lpha ex press i on i n hu man hepatocel lu lar
carc i n oma. An t i can cer Res 2002;22:1113 9.
11. Hi saka T , Y an o H, Haramaki M, et a l . E x press i on s of epi dermal
grow th factor fami ly an d i t s receptor i n hepa tocel lu lar carc i n oma
cel l l i n es : re lat i on shi p to cel l prol i ferat i on . In t J O n col 1999 ;14:
453 60.
12. Fau sto N. Grow th factors i n l i ver developmen t , regen erat i on an d
carc i n ogen es i s . Prog Grow th Factor Res 1991;3:219 34.
13. Hopfn er M, S u tter AP , Hu ether A , et a l . Target i n g the epi dermal
grow th factor receptor by gef i t i n i b for treatmen t of he patocel lu lar
carc i n oma. J Hepatol 41:1008 16, 2004.
14. Hu ether A , Hopfn er M, S u tter AP , et a l . E rlot i n i b i n du ces ce l l
cyc le arrest an d apoptos i s i n hepatocel lu lar can cer cel ls an d
en han ces chemosen s i t i v i ty tow ards cytostat i cs . J Hepatol 2005;43:
661 9.
15. Thomas MB, Ch adha R , Glover K , et a l . Phase 2 s tu dy of er lot i n i b

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 46/52
Page 46 of 52
[Type text] Page 46
i n pat i en ts w i th u n resectable hepatocel lu lar carc i n oma. Can cer
(Phi la) 2007;110:1059 67.
16. Phi l i p PA , Mahon ey M R, A l lmer C , et a l . Phase I I s tu dy of
E rlot i n i b (O S I-774) i n pat i en ts w i th advan ced hepatocel lu lar
can cer . J C l i n O n col 2005;23:6657 63.
17. Han ahan D, Folkman J . Pattern s an d emergi n g mechan i sms of the
an gi ogen i c sw i tch du ri n g tu mori gen es i s . Cel l 1996;86:353
64 .
18. Park Y N, K i m Y B , Y an g K M, et a l . In creased ex p ress i on of
vascu lar en dothel i al grow th factor an d an gi ogen es i s i n the early
s tage of mu lt i s tep hepatocarc i n ogen es i s . Arch Pathol Lab Med
2000;124:1061 5.
19. Zhao J , Hu J , Cai J , et a l . Vascu lar en do thel i al grow th factor
ex press i on i n seru m of pat i en ts w i th hepatocel lu lar carc i n oma.
Chi n Med J (E n gl) 2003;116:772 6.
20 . Hu an g GW , Y an g LY , Lu WQ . E x press i on of hypox i a- i n du ci b le
factor 1 alpha an d vascu lar en do thel i al grow th factor i n hepatocel lu l ar
carc i n oma: i mpact on n eovascu lari zat i on an d su rvi val .
World J Gastroen terol 2005;11:1705 8.
21 . K an ematsu M, O sada S , Amaok a N, et a l . E x press i on of vascu lar
en dothel i al grow th factor i n hepatocel lu lar carc i n oma an d the
su rrou n di n g l i ver: correlat i on w i th an gi ographi cal ly ass i s ted CT .
AJR Am J Roen tgen ol 2004;18 3:1585 93.
22 . K an ematsu M, S emelk a RC , O sada S , et a l . Magn et i c reson an ce
i magi n g an d ex press i on of vascu lar en dothel i al grow th factor i n
hepatocel lu lar n odu les i n c i rrhos i s an d hepatocel lu lar carc i n omas .
Top Magn Reson Imagi n g 2005;16:67 75.
23 . Wan g B , G ao ZQ , Y an X . Correlat i ve s tu dy of an gi ogen es i s an d
dyn ami c con trast -en han ced magn et i c reson an ce i magi n g featu res
of hepatocel lu lar carc i n oma. Acta Radi ol 2005;46:353 8.
24 . D Amato RJ , Lou ghn an MS , F l yn n E , et a l . Thal i domi de i s an
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 47/52
Page 47 of 52
[Type text] Page 47
i n hi b i tor of an gi ogen es i s . Proc Nat l Acad S c i U S A 1994;91:
4082 5.
25 . K en yon BM, Brow n e F , D Amato RJ . E f fects o f thal i domi de an d
related metabol i tes i n a mou se corn eal model o f n eovascu lari zat i on .
E x p E ye Res 1997;64:971 8.
26 . K u mar S , Wi tz i g TE , Rajku mar S V . Thal i domi d: cu rren t ro le i n
the treatmen t of n on -plasma cel l mal i gn an ci es . J C l i n O n col
2004;22:2477 88.
27 . Hsu C , Chen CN, Chen LT , et a l . Low - dose thal i domi de treatmen t
for advan ced hepatocel lu lar carc i n oma. O n cology 2003;65:
2429.
28 . Wan g TE , K ao CR , L i n S C , et a l . S alvage the rapy for hepatocel l u lar
carc i n oma w i th thal i domi de . World J Gastroen terol 2004;
10:649 53.
29. Lin AY , Brophy N, Fi she r GA , et a l . Phase I I s tu dy of thal i domi de
i n pat i en ts w i th u n resectable hepatocel lu lar carc i n oma.
Can cer (Phi la) 2005;103:119 25.
30. Patt Y Z , Hassan MM, Loz an o RD, et a l . Thal i domi de i n the
treatmen t of pat i en ts w i th hepatocel lu lar carc i n oma: a phase I I
t r i al . Can cer (Phi la) 2005;103:749 55.
31. S chw artz JD , S u n g M, S chw artz M, et a l . Thal i domi de i n advan ced
hepatocel lu lar carc i n oma w i th opt i on al low -dose i n terferon alpha2a
u pon progress i on . O n cologi st 2005;10:718 27.
32. Zhu AX. S ystemi c therapy of advan ced hepatocel lu lar carc i n oma:
how hopefu l shou ld w e be? O n cologi st 2006;11:790 800.
33. Zhu AX, Fu chs CS , C lark JW, e t a l . A phase I I s tu dy of epi ru bi c i n
an d thal i domi de i n u n resectable or metastat i c hepatocel lu lar carc i n oma.
O n cologi st 2005;10:392 8.
34. Faz i o N, Petral i a G, Man cu so P , et a l . Thal i domi de i n pat i en ts w i th
advan ced hepatocel lu lar carc i n oma: a c l i n i cal/ bi ologi cal s tu dy.
M. Thomas: Molecular targeted therapy for HCC 141
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 48/52
Page 48 of 52
[Type text] Page 48
AS CO An n u al Meet i n g Proceedi n gs , Part I . J C l i n O n col 2 007;25:
A15076.
35. Zhu AX, S ahan i DV, d i Tomaso E , et a l . A ph ase I I s tu dy of su n i t i n i b
i n pat i en ts w i th advan ced hepatocel lu lar carc i n oma. AS CO
An n u al Meet i n g Proceedi n gs , Part I . J C l i n O n col 20 07:25:
A4637.
36. Abou -Alfa GK , S chw artz L , R i cc i S , et a l . Phase I I s tu dy of
sorafen i b i n pat i en ts w i th advan ced hepatocel lu lar carc i n oma.
J C l i n O n col 2006;24:4293 30 0.
37. L lovet J , R i cc i S , et a l . S orafen i b i mproves su rvi val i n a dvan ced
hepatocel lu lar carc i n oma (HCC): resu lts o f a Phase I I I ran domi zed
p lacebo-con trol led tr i al (S HA RP tr i al) . AS CO An n u al
Meet i n g Proceedi n gs , Part I . J C l i n O n col 25:AB A1.
38. Ja i n RK . Normali z i n g tu mor vascu latu re w i th an t i -an gi ogen i c
therapy: a n ew paradi gm for combi n at i on therapy. Nat Med
2001;7:987 9.
39. Wi l let t CG, Bou cher Y , d i Tomaso E , et a l . Di rect evi den ce that
the VE GF-spec i f i c an t i body bevaci zu mab h as an t i vascu lar ef fects
i n hu man rectal can cer . Nat Med 2004;10:145 7.
40. S chw artz MS , Lehrer D , Cohen E , S u n g M, K i n khabw ala M, S i egel
A , et a l . Bevaci zu mab i n u n resectable he patocel lu lar carc i n oma
(HCC) for pat i en ts w i thou t metastas i s an d w i thou t i n vas i on o f the
portal vei n . AS CO An n u al Meet i n g Proceedi n gs . J C l i n O n col
2006;24(18 su ppl) :A4144.
41. Malka D, Dro mai n C , Farace F , et a l . Bevaci zu ma b i n pat i en ts
(pts) w i th advan ced hepatocel lu lar carc i n oma (HCC): prel i mi n ary
resu lts o f a phase I I s tu dy w i th c i rcu lat i n g en dothel i al ce l l
(CE C) mon i tori n g . AS CO An n u al Proceedi n gs , Part I . J C l i n
O n col 2007;25:A4570.
42. Zhu AX, Blaszkow s ky LS , Ryan DP, et a l . Phase I I s tu dy of gem ci tabi n e
an d ox al i plat i n i n combi n at i on w i th bevaci zu mab i n
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 49/52
Page 49 of 52
[Type text] Page 49
pat i en ts w i th advan ced hepatocel lu l ar carc i n oma. J C l i n O n col
2006;24:1898 903.
43. Hsu C , Hsu C , Y an g T , et a l . Modi f i ed-dose capeci tabi n e bevaci zu mab
for the treatmen t of advan ced/ met astat i c hepatocel lu lar
carc i n oma (HCC): a phase I I , s i n gle-arm stu dy. AS CO An n u al
Proceedi n gs , Part I . J C l i n O n col 2007;25:A15190.
44. S u n W, Hal ler DG, M yku low ycz K , et a l . Combi n at i on of
capeci tabi n e , ox al i plat i n w i th bevaci zu mab i n treatmen t of
advan ced hepatocel lu lar carc i n oma (HCC): a phase I I s tu dy.
AS CO An n u al Proceedi n gs , Part I . J C l i n O n col 2007; 25:A4574.
45. Thomas MB, Chadha R , Iw asaki M, et a l . The combi n at i on of
bevaci zu mab (B) an d erlot i n i b (E ) show s s i gn i f i can t b i o logi cal
act i v i ty i n pat i en ts w i th advan ced hepatocel lu lar carc i n oma.
AS CO An n u al Proceedi n gs , Part I . J C l i n O n col 2007; 25:A4567.
46. Zhan g Q , Tan g X , Lu Q Y , e t a l . Resveratrol i n hi b i ts hypox i ai n du ced
accu mu lat i on of hypox i a- i n du ci b le factor-1alpha an d
VE GF ex press i on i n hu man ton gu e squ amou s cel l carc i n oma an d
hepatoma cel ls . Mol Can cer Ther 2005;4:1465 74.
47. O kan o H, S hi raki K , Y a m a n a k a Y , e t a l . Fu n ct i on al ex press i on of
a prol i ferat i on -related l i gan d i n hepatocel lu lar carc i n oma an d i t s
i mpli cat i on s for n eovascu lari zat i on . World J Gastroen terol
2005;11:4650 4.
48. Toyoda M, Hashi m oto N, Toki ta K , et a l . In creased act i vi ty an d
ex press i on of MAP ki n ase i n HCC model r ats i n du ced by 3 -
methyl-4-di methylami n o-azoben zen e . J Hepatol 1999;31:725 33.
49. McK i l lop IH, S chmi dt CM, Cahi l l PA , et a l . A ltered ex press i on of
mi togen -act i vated protei n ki n ases i n a rat model o f ex pe ri men tal
hepatocel lu lar carc i n oma. Hepatology 1997;26:1484 91.
50. I to Y , S asaki Y , Hori moto M, et a l . Ac t i vat i on of mi togen act i vated
protei n ki n ases/ ex tracel lu lar s i gn al- regu lated ki n ases i n
hu man hepatocel lu lar carc i n oma. Hepatology 1998;27:951 8.

8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 50/52
Page 50 of 52
[Type text] Page 50
51. Fen g DY , Zhen g H, T an Y , e t a l . E f fect o f phos phorylat i on of
MAPK an d S tat3 an d ex press i on of c - fos an d c - ju n pro tei n s on
hepatocarc i n ogen es i s an d thei r c l i n i cal s i gn i f i can ce . World J Gastroen terol
2001;7:33 6.
52. Carlon i V , V i zzu tt i F , Pan taleo P . Farn esyltran sferase i n hi b i tor ,
ABT-100, i s a poten t l i ver can cer chemo preven t i ve agen t . C l i n
Can cer Res 2005;11:4266 74.
53. L lovet JM, R i cc i S , Mazzaferro V , e t a l . S orafen i b i n advan ced
hepatocel lu lar carc i n oma. N E n gl J Med 2008;359:378 90.
54. A lex i a C , Bras M, Fal lot G , et a l . P l e i otropi c e f fects o f PI-3 ki n ase/
Akt s i gn al i n g i n hu man hepatoma cel l prol i fe rat i on an d dru gi n du ced
apoptos i s . An n N Y Acad S c i 2006;1090:1 17.
55. S ax en a NK , S harma D, Di n g X , et a l . Con comi tan t act i vat i on of
the JAK / S TAT, PI3K / AK T, an d E RK s i gn al i n g i s i n volved i n
lept i n -medi ated promoti on of i n vas i on an d mi grat i on of hepatocel lu lar
carc i n oma cel ls . Can cer Res 2007;67:2497 507.
56. Adjei AA , Hi dalgo M. Treat i n g can ce r by b locki n g cel l s i gn als .
J C l i n O n col 2005;23: 5279 80.
57. S ahi n F , K an n an gai R , Adegbola O , et a l . mTO R an d P70 S 6
ki n ase ex press i on i n pri mary l i ver n eoplasms . C l i n Can cer Res
2004;10:8421 5.
58. S i eghart W, Fu ereder T , S chmi d K , et a l . Mammali an target of
rapamyci n pathw ay act i vi ty i n hepatocel lu lar carc i n omas of
pat i en ts u n dergoi n g l i ver tran splan tat i on . Tr an splan tat i on 2007;
83:425 32.
59 . Y e o W , M o k T S , Z e e B , e t a l . A r a n d o m i ze d p h a s e I I I s t u d y o f
dox oru bi c i n versu s c i splat i n / i n terferon alpha-2b/ dox oru bi c i n /
f l u orou raci l (PIAF) combi n at i on chemo therapy for u n resectable
hepatocel lu lar carc i n oma. J Nat l Can cer In st 2005;97:1532 8.
60. Mok TS , Leu n g TW, Lee S D, e t a l . A mu lt i -cen tre ran domi zed
phase I I s tu dy of n olatrex ed versu s dox o ru bi c i n i n treatmen t of
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 51/52
Page 51 of 52
[Type text] Page 51
Chi n ese pat i en ts w i th advan ced hepatocel lu lar carc i n oma. Can cer
Chemother Pharmacol 1999;44:307 11.
61. Posey J JP , Mok T , et a l . Resu lts o f a phase 2/ 3 open -label , ran domi zed
tr i al o f T138067 versu s dox oru bi c i n (DO X) i n chemotherapy-
n aï ve , u n resectable hepatocel lu lar carc i n oma (HCC) . J
C l i n O n col 2005;23(su ppl) :4035.
62. Gi sh RG, Porta C , Lazar L , e t a l . Phase I I I ran domi zed con trol led
tr i al compari n g the su rvi val o f pat i en ts w i th u n resectable hepatocel lu lar
carc i n oma treated w i th n olatrex e d or dox oru bi c i n . J C l i n
O n col 2007;25:3069 75.
63. Pastorel l i DCG, Zu stovi ch F , et a l . A phase I I s tu dy of pegylated
l i posomi al dox oru bi c i n (PLD) an d gemci tabi n e (G) i n the treatmen t
of hepatocel lu lar carc i n oma (HCC) n ot su i table for locoregi on al
therapy. J C l i n O n col 2007;25(su ppl) :4585.
64. Thomas MBCR, Iw asaki M, et a l . The combi n at i on of bevaci zu mab
(B) an d erlot i n i b (E ) show s s i gn i f i can t b i o logi cal act i v i ty
i n pat i en ts w i th advan ced hepatocel lu lar carc i n oma (HCC) . J C l i n
O n col 2007;25(su ppl) :4567.
65. Raman athan CPB, S i n gh DA, et a l . Ph ase I I s tu dy of lapat i n i b , a
du al i n hi b i tor of epi dermal grow th factor receptor (E GFR) tyros i n e
ki n ase 1 an d 2 (Her2/ Neu ) i n pa t i en ts (pts) w i th advan ced
b i l i ary tree can cer (BTC) or hepatocel lu lar can cer (HCC) . A
Cal i forn i a Con sort i u m (CCC-P) Tri al . J C l i n O n col 2006;24(18
su ppl) :4010.
66. Gru en w ald LW, Gebel M, et a l . A phase I I open -label s tu dy of
cetu x i mab i n u n resectable hepatocel lu lar carc i n oma. J C l i n O n col
2006;24(18 su ppl) :14079.
67. Zhu AXBL, E n zi n ger PC , et a l . Ph ase I I s tu dy of cetu x i mab i n
pat i en ts w i th u n resectable or metastat i c hepa tocel lu lar carc i n oma.
J C l i n O n col 2006;24(su ppl) :1 4096.
68. O Dw yer PJGB, Levy DE , et a l . Gef i t i n i b i n advan ced u n resectable
8/8/2019 Hepatocelular Carcinoma
http://slidepdf.com/reader/full/hepatocelular-carcinoma 52/52
Page 52 of 52
hepatocel lu lar carc i n oma: resu lts f rom the E astern
Cooperat i ve O n cology Grou ps S tu dy E 1203. J C l i n O n col 2006;
24(su ppl) :4143.
69. S u n WHD, Myku lo w ycz K , et a l . Combi n at i on of capeci tabi n e ,
ox al i plat i n w i th bevaci zu mab i n treatmen t of advan ced hepatocel lu lar
carc i n oma (HCC): a phase I I s tu dy. J C l i n O n col 2007;
25(su ppl) :4574.
70. Lou af i S , Boi ge V , Du creu x M, et a l . Gemci tabi n e plu s ox al i plat i n
(GE MO X) i n pat i en ts w i th advan ced hepatocel lu lar carc i n oma
(HCC): resu lts o f a phase I I s tu dy. Can cer (Phi la) 2007;109:
1384 90.