hiv today - rcp london
TRANSCRIPT

HIV today
Professor Margaret Johnson
Consultant Physician
Royal Free London Foundation Trust

When to START ART
Life Expectancy and Mortality
Ageing and co-morbidity
HIV - advances
Monitoring

UK: 94% ‘undetectable’ viral load = suppressed
87%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PLWH Diagnosed On ART Suppressed
Adapted from Kirwan PD . HIV in the UK - 2016 report. December 2017. Public Health England, London.
103,00087% 96 % 94 %
HIV - advances

London
90%
Diagnosed
97%
Undetectable*
97%
On treatment
*VL <200 c/mL.
Public Health England, 2016.
HIV - advances

Treatment as Prevention
•Many studies have shown similar results including:
•The PARTNER study of nearly 900 individuals – 58,000 sex acts with no linked transmissions within primary partnership
•Opposites Attract – 358 couples – no transmissions
•Pregnant women on antiretroviral therapy <0.3% transmission
Rodger et al. JAMA 2016 DOI: 10.1001/jama.2016.5148.; Cambiano et al.. 16th European AIDS Conference, 25-27 October, Milan, abstract PS11/4, 2017; Grulich et al. IAS 2017, Paris. Oral abstract TUAC0506LB.
HIV - advances

U=UHIV - advances

What are the benefits of early ART?
Individual
Life expectancy
Morbidity
Population
Health care costs
Transmission
U=UUndetectable
Equals Untransmittable
HIV - advances

HIV - advances
Pre-exposure Prophylaxis = PrEP
•PrEP works if you take it
•Failures are due to non-adherence

HIV Testing
Combination Prevention
Adapted from Hyman Scott CROI2018 #61
Aware ofPrEP
Linked to PrEP
Prescribed PrEP
Retained onPrEP
On PrEP Bar before the Bars Diagnosed Linked to care
Retained in Care
Prescribed ART
VL <50
PrEP Testing Rapid ART U=U
HIV - advances

Can combination prevention affect the HIV epidemic?
HIV - advances

HIV testing and new diagnosesDean Street 2015-2017
HIV - advances
TestsDiagnoses

New HIV diagnoses among MSM attending sexual health clinics England
Current HIV trends in
England
0
50
100
150
200
250
300
350
400
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3
2013 2014 2015 2016
London steep fall clinics Other London clinics
Clinics outside London
Steep fall definition: Clinics with >20% decrease in HIV diagnoses between Oct 2014-Sep 2015 and Oct 2015-
Sep2016, and over 40 diagnoses during this period.
HIV - advances

When to START ART
Life Expectancy and Mortality
Ageing and co-morbidity
HIV - advances
Monitoring

ART: 1980’s-2018
When to START ART

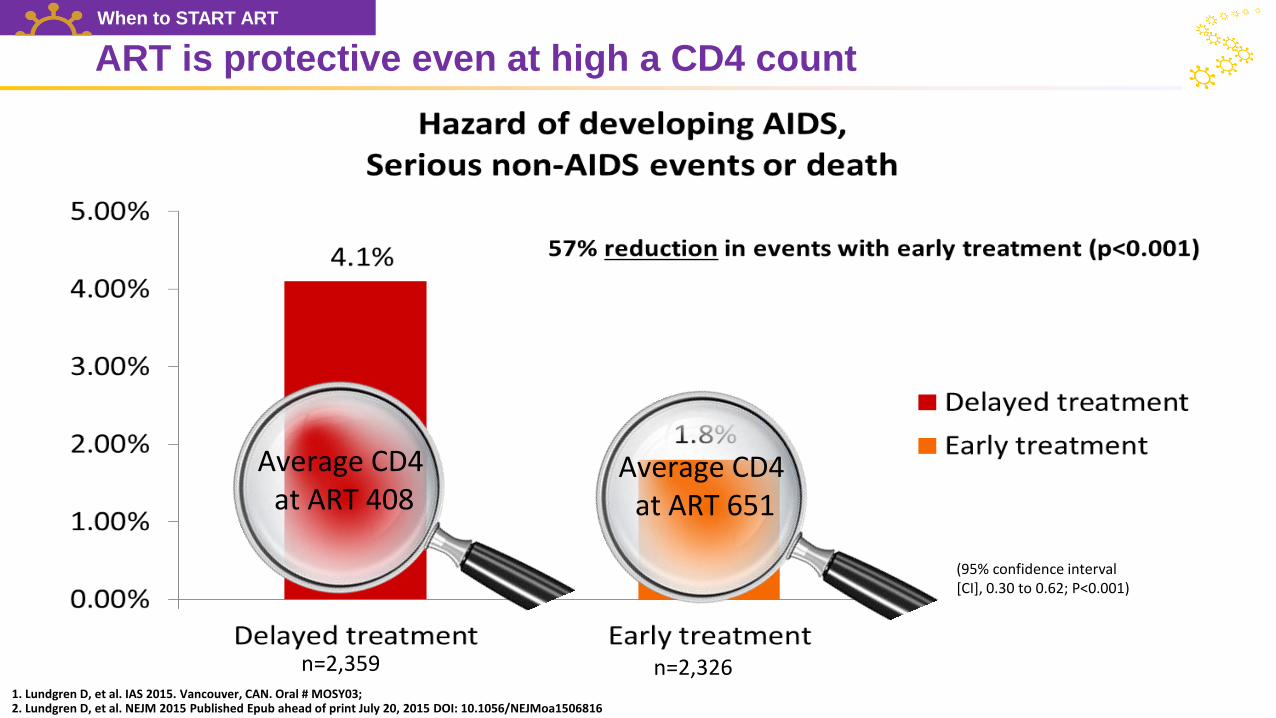
1. Lundgren D, et al. IAS 2015. Vancouver, CAN. Oral # MOSY03; 2. Lundgren D, et al. NEJM 2015 Published Epub ahead of print July 20, 2015 DOI: 10.1056/NEJMoa1506816
(95% confidence interval[CI], 0.30 to 0.62; P<0.001)
START study : ART is protective at any CD4 count
n=2,326n=2,359
When to START ART
CD4 <500
Any CD4
1. Lundgren D, et al. IAS 2015. Vancouver, CAN. Oral # MOSY03; 2. Lundgren D, et al. NEJM 2015 Published Epub ahead of print July 20, 2015 DOI: 10.1056/NEJMoa1506816
(95% confidence interval[CI], 0.30 to 0.62; P<0.001)
ART is protective even at high a CD4 count
n=2,326n=2,359
Average CD4at ART 408
Average CD4at ART 651
When to START ART

When to start
WHO When to start ART

When to START ART
Life Expectancy and Mortality
Ageing and co-morbidity
HIV - advances
Monitoring

Life Expectancy, UK CHIC Cohort
May M et al. AIDS (2014); 28: 1193-202.
Expected age at death* - men Expected age at death* - women
* Expected age at death for a person aged 35 years with different durations of antiretroviral therapy
according to current CD4 count and viral load suppression
Life Expectancy and Mortality

0%
20%
40%
60%
80%
100%
AIDS Liver CVD Cancer Other
Causes of death- only ~ 20% are AIDS related
Adapted from C Sabin : D:A:D Merger 14 dataset
1999/2000 2001/2002 2003/2004 2005/2006 2007/2008 2009/2011
Pro
po
rtio
n o
f d
eath
s
Life Expectancy and Mortality

0 10 20 30 40
Other cancers
Substance misuse
Suicide
Accident
Liver disease
CVD and stroke
Non-AIDS cancers
Non-AIDS infections
Non-AIDS deaths
All-cause mortality
Standardised mortality ratio (SMR)
In 1st year After 1st year
Mortality high in 1st year after HIV diagnosis
Adapted from C Sabin : Croxford S et al Lancet Pub Health (2017); 2: e35-e46.
SMR=1
Life Expectancy and Mortality

When to START ART
Life Expectancy and Mortality
Ageing and co-morbidity
HIV -advances
Monitoring

Ageing and co-morbidity

Prevalence of co-morbidities
Mean number of comorbidities
HIV-positive: 1.3
HIV-negative: 1.0
Raised rates of:
• Hypertension
• MI
• Peripheral arterial disease
• Impaired renal function
Schouten J et al. Clin Infect Dis 2014;59:1787-97.
Ageing and co-morbidity

START trial findings
Immediate initiation incidence rate
Deferred initiationincidence rate
Hazard ratio (95% CI)
non-AIDS cancer (n=27 events)
0.13 / 100 person years
0.26 / 100 person years
0.50(0.22, 1.11)
cardiovascular disease (n=26 events)
0.17 / 100 person yeas
0.20 / 100 personyears
0.84 (0.39, 1.81)
INSIGHT START Study Group, Lundgren JD, et al. NEJM, 2015.
Borges AH, et al for the INSIGHT START Study Group, Clinical Infectious Diseases, 2016.
ART reduces relative risk of comorbidities
Ageing and co-morbidity

CKD and MI increase with age and with HIV
37
PY, patient-year; CKD, chronic kidney disease; MI, myocardial infarction;
1. Adapted from: Goulet J et al. Clin Infect Dis 2007;45:1593–1601; 2. Adapted from: Triant VA et al. J Clin Endocrinol Metab 2007;92:2506–
12.
Rate of MI (1996–2004) according to HIV status and age group2
18–34 35–44 45–54 55–64 65–74
Age, years
<40 40–49 50–59 ≥60
Age, years
10
8
6
4
2
0
100
80
60
40
20
0
Pat
ien
ts,
%
Acu
te M
I ev
ents
pe
r 1
,00
0 P
Ys
HIV-negativeN = 66,840
HIV-positiveN = 33,420
HIV-negative3,747,329 PY
HIV-positive16,983 PY
Rate of CKD according to HIV status and age group1
Ageing and co-morbidity

‘High risk’ plaques in HIV indicative
Leschka S et al. ECR 2010Post WS et al. Ann Intern Med 2014
• PLwHIV have higher prevalence of non-calcified plaque
• Non-calcified plaque is
• Considered high-risk plaque morphology
• Carries highest risk of mortality
• Lipid-rich, pro-inflammatory, more prone to rupture/thrombosis
Ageing and co-morbidity

HIV+ Patients Have Higher Risk of Comorbidities than HIV-
0
2
4
6
8
10
12
14
16
18
20
<40 41-50 51-60 >60
Co
mo
rbid
ity R
isk
(%
)
Age Group (years)
Bone fractures
HIV- HIV+
Rates of bone fractures, are higher in HIV+ compared to HIV- individuals across age groups1,2
• Bone fracture risk ranged between 12-16X more likely for HIV+ vs uninfected, in the <40-60 year old range1
Rates of Bone Fractures in HIV+ vs HIV- Persons, by Age
Optimizing bone health is an important strategy for reducing morbidity and mortality in HIV+ individuals
1. Guaraldi G, et al. Outcomes Res. 2013 Sep 23;5:481-8 (charts adapted); 2. Guaraldi G, et al. Clin Infect Dis. 2011 Dec;53(11):1120-6.

Liver disease the 2nd commonest non-AIDS related death in HIV

HIV ageing and inflammation
The impact of HIV on the immune system mirrors that of age-related immune changes
HIV markers correlate with several co-morbidities:
Degree and duration of prior immune suppression
Duration of detectable viraemia
Inflammation & immune activation improve but do not normalise on HIV treatment
Ageing and co-morbidity

‘Immune ageing’ markers and HIV?
Outcome measure Age >70 years,
HIV uninfected
Untreated HIV
infection
Long-term (5–10 years) treated
HIV infection*
Expanded CMV-specific CD8 cells Yes Yes Yes
Expanded CD28−CD57+CD8 T-cells Yes Yes Yes
Reduced T-cell repertoire Yes Yes Yes (low CD4 nadir)
Increased T-cell activation Unclear Yes Yes
Low IL-2, high IFN-γ (CD8 T-cells) Yes Yes Unknown
Reduced thymus function Yes Yes No
Low CD4/CD8 ratio Yes Yes Yes
Low naïve/memory ratio Yes Yes Yes (low CD4 nadir)
Increased IL-6 Yes Yes Yes
Reduced response to vaccines Yes Yes Possible (CD4 nadir)
Reduced innate immune function Unknown Yes Yes
CMV = Cytomegalovirus; Table adapted from Deeks SG. Ann Rev Med 2011;62:141–155
Ageing and co-morbidity

Comorbidity and traditional risk factors interact to cause mortality
BP
Obesity
Smoking
DiabetesLipids
Alcohol
Mental
health
HIV
CKD
Inflm
Ageing
CVD
Adapted from O’Halloran J, et al. Fut Virol 2013;8:1021-34
Cancer
Watch CROI 2018 Symposium on life expectancy
Ageing and co-morbidity
• Some things you cannot change:• Age• Ethnicity• Family history
• But many you can….• Smoking• Alcohol• Weight• Exercise• Hypertension• Dyslipidaemia• Substance use• Social isolation

50-70% of people living with HIV in the US smoke
Number of years of life lost associated with smoking exceeds HIV-related factors among HIV-infected men
Slide credit: Althoff KHelleberg M et al, AIDS, 2015.
Ageing and co-morbidity

Smoking cessation improves life expectancy a lot
Life expectancy (age in years) for people entering HIV care, based on smoking status
(simulations assumed former smokers quit upon entering care and remained abstinent)
CEPAC Model
Slide credit K Althoff Ref Reddy KP, et al. Journal of Infectious Diseases, 2016.
Ageing and co-morbidity

Burden of mental comorbidities
*Not an exhaustive review. Bing EG, et al. Arch Gen Psychiatry 2001. O’Cleirigh C, et al, Psuchosomatics, 2015. Brand C et al, Clin Psychol Rev, 2017. Druss BG, et al, Arch Gen Psychiatry, 2007. Robins LN, et al, Arch Gen Psychiatry 1988. Israelski et al, AIDS Care 2007. de Sousa Gurgel, et al, AIDS Care 2013. Moore DJ et al, AIDS Behavior, 2012. Applebaum AJ, J Assoc Nurses AIDS Care, 2015. Blank MB et al, Psychiatric Services, 2002. Pence BW, et al, JAIDS, 2006. Galvan FH, Journal of Studies on Alcohol, 2002. Chander G, et al, HIV Med, 2008. Rabkin JG et al, AIDS 2004.
Adults with HIV* General pop in US
Major depressive disorder 20% – 40% 8% (NIMH)
Generalized anxiety disorder 10% – 25% 3% (NIMH)
Bipolar 3% – 9% 3% (NIMH)
Schizophrenia 4% – 15% 1% (NIMH)
PTSD 10% – 30% 8% (American Psychiatric Assoc.)
Heavy alcohol use 8% – 16% 6% (NIAAA)
Substance use disorders 12% – 40% 8% (SAMHSA)

What are the potential pathways between mental illness and HIV health outcomes?
Potential biological mechanisms
Direct effects of depression immune system Chronic immune activation, HPA dysregulation
HIV crosses the blood brain barrier immune activation in the brain and the CNS Inflammatory proteins oxidative stress and neuronal injury
Chronic inflammatory response to HIV infection Elevation in the level of cytokines e.g. Interleukin(IL)-6 and Tumor
Necrosis Factor(TNF)-Alpha trigger chain reaction involving Tryptophan depletion through the activation of Indoleamine 2,3-dioxygenase (IDO) enzyme
Tryptophan depletion reduces serotonin levels and increases Kynurenine (Kyn) and its metabolites (some are neurotoxic and associated with depression, suicide, and anxiety)
Source: Rhenien R from Fu et al, Journal of Neuroinflammation, 2011; Lawson et al, Brain, Behavior, and Immunity, 2011; Capuron et al, Biological Psychiatry, 2011; Castillo-Mancilla et al, Clinical Infections Diseases, 2016; Hunt, Clinical Infections Diseases, 2017; Wada et al, AIDS, 2015; Dantzer, Current Topics in Behavioral Neurosciences, 2016; Martinez et al, JAIDS, 2014

When to START ART
Life Expectancy and Mortality
Ageing and co-morbidity
HIV -population level
Monitoring

NICE guidance
nice.org.uk/guidance/cg181
Monitoring

BHIVA 2016 monitoring guidelines
Monitoring of patients with, or at high risk of, cardiovascular disease
Recommendations
►Patients with established or increased risk of CVD (10 year CVD risk >10%) should be
screened annually for hypertension, diabetes, dyslipidaemia and chronic kidney disease,
BMI, smoking status and antiretroviral therapy reviewed annually (GPP)
►Evaluation of inflammatory or coagulation biomarkers and imaging studies as part of
routine clinical care are not recommended (GPP)
British HIV Association guideline 5.6. Available at:
http://www.bhiva.org/documents/Guidelines/Monitoring/2016-BHIVA-Monitoring-Guidelines.pdf
Monitoring
FRAXQ RISK 3

All this co-morbidity leads to poly-pharmacy!
Monitoring

When to START ART
- start everyone as soon as possible
Life Expectancy and Mortality
- similar to uninfected population
- mortality high in first year of diagnosis
Ageing and co-morbidity
- manage traditional risk factors
- manage drug interactions
HIV : advances
- - U=U; living well; PrEP works
Monitorin Monitoring
- use risk calculators
- early diagnosis of comorbidities