traumatic brain injury - rcp london
TRANSCRIPT

www.stgeorges.nhs.uk
Traumatic Brain Injury
Dr Colette Griffin
Consultant Neurologist

www.stgeorges.nhs.uk
What is a TBI?
“Non degenerative, non congenital insult to the brain from an external mechanical force, possibly leading to permanent or temporary impairments of cognitive, physical, and psychosocial functions with an associated diminished or altered state of consciousness”
(Dawodu, 2005)

www.stgeorges.nhs.uk
www.stgeorges.nhs.uk
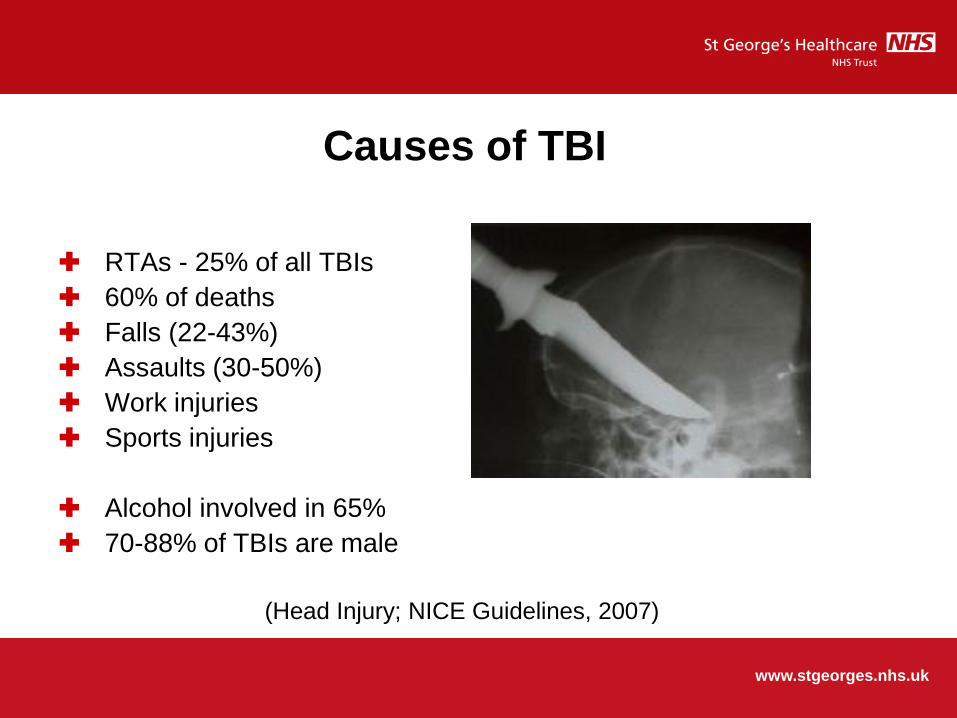
Causes of TBI
RTAs - 25% of all TBIs
60% of deaths
Falls (22-43%)
Assaults (30-50%)
Work injuries
Sports injuries
Alcohol involved in 65%
70-88% of TBIs are male
(Head Injury; NICE Guidelines, 2007)

www.stgeorges.nhs.uk
Why is this important?
Reconfiguration of trauma services pan UK
Major Trauma Centres developed
Trauma Units developed
NICE guidelines on head injury (2007)
NCEPOD “Trauma: who cares?” (2007)
Socially and economically catastrophic
www.stgeorges.nhs.uk
TBI pathway
Referral straight to neurosurgery SPR 24 hours a day
Referral then straight to neurology / dedicated TBI SPR
Dedicated TBI MDT team
Head injury coordinator 8am daily e mail
Immediate availability of TBI MDT team
MDT screening tool
Follow up with consultant and psychologist

www.stgeorges.nhs.uk
Why intervene early?
Intensive intervention leads to earlier gains Turner-Stokes L et al Cochrane
review 2005
Earlier rehabilitation improves functional outcome and lowers
rehabilitation and acute hospitalisation costs Cowen TD et al 1995
www.stgeorges.nhs.uk
Neuroplasticity
Brain remodelling in response to external factors
Structural redundancies
Neural recovery
Neural compensation
Enlargement of dendrites and axons
Increase in neuronal density

www.stgeorges.nhs.uk
Role of A&E
Trauma team
Imaging
Observation of patients overnight
Head injury booklet
Advice for GP follow up within one week (NICE)
Onward referral
Transfer to MTC as necessary
www.stgeorges.nhs.uk
Imaging
NICE guidelines 2007
Canadian CT head rule
GCS <13 on presentation
GCS <15 two hours post trauma
Focal signs, vomiting, severe headaches
If intubated or GCS <13 also need spinal imaging
Spinal cord clearance

www.stgeorges.nhs.uk
Discuss with neurosurgery
NICE guidelines 2007
Abnormal CT head
GCS 8 or below
Deteriorating GCS
Progressive neurology
Penetrating trauma
CSF leak

www.stgeorges.nhs.uk
Classifications
Severity (mild/moderate/severe)
Isolated vs poly trauma
Mode of injury
Pathology
www.stgeorges.nhs.uk
Classifications
90% of TBIs presenting to A&E have GCS 13-14 (mild TBI)
5% GCS 9-12 (moderate)
5% GCS 8 or below (severe)

www.stgeorges.nhs.uk
Pathophysiology
Primary tissue disruption at the time of injury is generally
irreversible
Secondary insults over hours and days may well be reversible
Cellular ischaemia
Activation of inflammatory cascades
Neuronal and astrocytic swelling
Vasogenic oedema

www.stgeorges.nhs.uk
White matter changes
Corpus callosum very vulnerable to shear and strain effects McAllister
et al 2012
Reduction in size and integrity of the corpus callosum, even in mild
TBI Aoki et al 2012
Loss of overall brain connectivity
TBI and dementia association may relate to selective white matter
damage and the role this plays in the expression of dementia via a
breakdown in neural connectivity

www.stgeorges.nhs.uk
Chronic atrophy
Mechanical deformation
Axonal shearing
Focal lesional effects
Ischaemia
Pathological neuroexcitatory effects
Pathological neuroinflammatory reactions
Overlapping trauma induced neurodegenerative effects occur in the
same frontotemporolimbic areas associated with age related
neurodegenerative disorders

www.stgeorges.nhs.uk
Erin D Bigler 2013

www.stgeorges.nhs.uk
Common Presentations These can be many and varied
Confusion
Agitation
Aggression
Loss of memory
Hemiplegia
Poor problem solving
Inappropriate behaviour
Altered social skills Reduced insight
Reduced sensation
Emotional lability
Altered communication
Difficulty eating/drinking
Loss of balance
Altered level of consciousness
Fatigue

www.stgeorges.nhs.uk
Post-Traumatic Amnesia
‘The period of post-traumatic amnesia is usually defined as
the time between receiving a head injury and the
resumption of normal continuous memory’
King et al 1997

www.stgeorges.nhs.uk
Why is PTA important?.. Can assist in predicting the severity of TBI
Used along side GCS score to predict severity of injury (Teasdale and
Jennett, 1979)
Research suggests it can be used to predict rehab outcomes
PTA duration Severity of Injury
< 5 mins Very mild
5-60 mins Mild
1-24 hours Moderate
1-7 days Severe
1-4 weeks Very severe
>4 weeks Extremely severe
Jennett, 1976
Russell and Smith, 1961

www.stgeorges.nhs.uk
Neuropsychiatric Management
Drug treatment of the neurobehavioural sequelae of TBI is common practice
There is limited evidence to guide drug treatment choices
Guidelines are based on consensus and some common principles between disorders
Presentation based on time course and common symptoms/disorders
See Chew & Zafonte 2009; Warden et al. 2006
www.stgeorges.nhs.uk
Post Traumatic Amnesia
Avoid typical antipsychotics and/or Benzodiazepines
• May delay recovery and neuroplasticity Arcienegas & Silver,
2006
Atypical antipsychotics as effective as Haloperidol
• Less interference with dopaminergic function and may
normalise cholinergic function
• Have fewer adverse effects Arcienegas & McAllister, 2008

www.stgeorges.nhs.uk
Management of PTA
Limit no. of visitors and their length of stay
Avoid restraints, consider one to one nursing
Allow patients to wander on ward with supervision
Try and keep patients in the same bed for orientation
Provide external structure (e.g. timetable, routine)
Allow frequent rest breaks
Keep instructions simple

www.stgeorges.nhs.uk
KEEP CALM
AND
BE NICE (EVEN IF YOU DON’T FEEL LIKE IT)

www.stgeorges.nhs.uk
PTA & Capacity
A patient is deemed NOT to have capacity when they are in PTA
Implications for the treating team:
Cannot be discharged
Have to ensure that patient stays on the ward
If a patient absconds they need to be brought back
Not ready for rehabilitation (historically)

www.stgeorges.nhs.uk
The Absconding Patient
Mental Capacity Act – MDT approach
Deprivation of Liberties - the least restrictive method of restraint must be used
Use of family / friends
Usually gentle guidance, explanation of risks and effective communication help
Use of pictorial and other external aids
www.stgeorges.nhs.uk
Key “take home” points
Reduce stimulation
Limit visitors to two at a time
Quiet environment
Stay calm with the person
Reassure them
Orientate them
Don’t encourage/allow any negative behaviour – whole team must have a consistent approach

www.stgeorges.nhs.uk
Seizures
Early post traumatic (<one week later): 25% develop epilepsy
Late post traumatic (>one week later): 80% develop epilepsy
65% of bullet induced TBIs develop seizures
20% of closed TBIs develop seizures
Over 35% of patients who have at least two neurosurgical
procedures post TBI develop late onset seizures
Immediate provoked single seizure: no AEDs
Seizure within first week: rapid titration and withdrawal
Late seizures: Lamotrigine or Levitiracetam
Epilepsy information and referral to epilepsy services

www.stgeorges.nhs.uk
Endocrinology
SIADH
Cerebral salt wasting
Chronic changes: hypopituitarism
Testing more useful at a later point in time
Most patients do not need replacement therapy

www.stgeorges.nhs.uk
VTE
TBI is a prothrombotic state
Patients are often totally immobile
Local trust VTE policies
“Individual patient based decision making”
Haemorrhage is a contra-indication
Heparin and TEDs
Personal experience
www.stgeorges.nhs.uk
Herb A Phelan Pharmacologic Venous Thromboembolism Prophylaxis
after Traumatic Brain Injury: A Critical Literature Review J Neurotrauma
2012;29(10):1821-1828

www.stgeorges.nhs.uk

www.stgeorges.nhs.uk
Headaches
Should usually settle with time
Do not use Paracetamol or Codeine containing products
Ibuprofen is typically contra-indicated
Personal experience
Associated loss of sleep-wake cycle: use of Melatonin

www.stgeorges.nhs.uk
Vertigo
Can be problematic clinically
Again should settle with time
Vestibular physiotherapy is often very helpful

www.stgeorges.nhs.uk
Pre-hospital neurosurgery…………..

www.stgeorges.nhs.uk
TBI Top tips
These patients are not a new invention
There will already be a fair number in the trust
They can be managed within a Trauma Unit or District General
Hospital setting
The hub and spoke model is the correct model of care
SGH service can be replicated elsewhere
www.stgeorges.nhs.uk
TBI Top tips
The first planned Trauma Unit TBI pilot will be Frimley Park
Hospital
Patient cohorting within the Trauma Unit is critical
Acute Stroke Unit model of care
No funding……………….
Rearrangement of services
Consultant responsible for service
Alteration in distribution of AHPs
www.stgeorges.nhs.uk
TBI Top tips
These are NICE and NCEPOD targets from almost a decade
ago…………………
Current care is not ideal
Patient care has to be utmost priority
The days of playing “pass the parcel” are over

www.stgeorges.nhs.uk
Kamp MA et al. Traumatic Brain Injuries in illustrated literature:
experience from a series of over 700 head injuries in the Asterix comic
books. Acta Neurochir (Wein) 2011;153(6):1351-1355

www.stgeorges.nhs.uk
Risk factors for TBI
Roman nationality (TBIs caused by Gauls)
Lost helmet
Ingestion of the “magic potion”
Forgot to call for help

www.stgeorges.nhs.uk
References
NICE guideline CG56. Triage, assessment, investigation and early
management of head injury in infants, children and adults. 2007
NCEPOD Trauma; who cares? 2007
Turner-Stokes L et al. Multi-disciplinary rehabilitation for acquired
brain injury in adults of working age. Cochrane Database Sys Rev
2005;(3):CD004170
Cowen TD et al. Influence of early variables in traumatic brain
injury on functional independence measure scores and
rehabilitation length of stay and charges. Arch Phys Med Rehabil
1995;76:797-803

www.stgeorges.nhs.uk
References
Teasdale GM et al. Analysing outcome of treatment of severe head
injury: a review and update on advancing the use of the Glasgow
Outcome Scale. J Neurotrauma 1998;15:587-97
Erin D Bigler. Traumatic brain injury, neuroimaging and
neurodegeneration. Frontiers In Human Neuroscience 2013

www.stgeorges.nhs.uk
Thank you