hiv/aids and viral hepatitis in the criminal justice profession texas commission on law enforcement...
TRANSCRIPT
HIV/AIDS and Viral Hepatitisin the
Criminal Justice Profession
Texas Commission on Law Enforcement &
Texas Department of State Health Services

Unit One
1.0 Functional Area: This section will introduce the student to HIV/AIDS, HBV, and HCV. The student will be able to demonstrate on a written
examination an understanding of the relevant terms and definitions of HIV/AIDS, HBV and HCV.

Learning Objective
1.1 Learning Objective: The student will be able to write general
statements regarding HIV.

What is HIV?
H = Human
I = Immunodeficiency
V = Virus
General Statement (HIV)
• Virus that causes AIDS
• Once a person is infected, they can immediately transmit HIV to another person
• Destroys the body's ability to fight infections and certain cancers by killing or damaging cells of the body's immune system
• A person infected may remain without symptoms for a long period of time

General Statement (HIV)
• There is no cure for HIV
• Increased understanding of HIV disease progression, refinement and acceptance of holistic therapies, availability of sophisticated testing, ability to prevent or reduce the impact of opportunistic infections, and potent treatment therapies have made HIV an increasingly manageable chronic disease

Learning Objective
1.2 Learning Objective: The student will be able to list and describe the general stages of HIV
infection.

Stages of HIV Infection
• Infection
• Primary HIV Infection
• Sero-conversion (Response)
• Immune System Decline– Mild, non-specific Symptoms– More Severe Symptoms; Opportunistic
Infections and Diseases/AIDS

Learning Objective
1.3 Learning Objective: The student will be able to write general
statements regarding AIDS.

What is AIDS?
A = Acquired
I = Immuno-
D = deficiency
S = Syndrome

General Statements (AIDS)
• AIDS is the common abbreviation for Acquired Immunodeficiency Syndrome
• The term AIDS applies to the most advanced stages of HIV infection
• AIDS is the result of the natural progression of HIV infection
• The acquired immunodeficiency syndrome (AIDS) was first recognized in 1981

Learning Objective
1.4 Learning Objective: The student will be able to describe in
writing, the relationship between HIV and AIDS
Relationship between HIV & AIDS
• Individuals don’t transmit AIDS, they transmit HIV
• HIV progresses in each individual differently
• Immune system breakdown causes opportunistic infections/AIDS
• Common opportunistic infections (PCP, KS, MAC, TB)

How would I know if I have HIV?• The only sure way to know your status is to be
tested
• The most common test is an antibody test\
• The antibody test (EIA) detects infection in most persons within 6 weeks to 3 months
• Any positive antibody test must be confirmed with a second type of test, the Western Blot
• Both tests (EIA and Western Blot) must be positive for someone to be told s/he has HIV

Split Decision
Split Decision intends to open the lines of communication in relationships as it relates to the rapidly spreading HIV virus. This is a five minute short film of a longer piece of work directed by Sanedria Arne’ Porter, writer/director originally from Winston-Salem, N.C. currently residing in Atlanta, Georgia. This short film was written by Sanedria Arne' Potter & Kirk A. Moore.

Learning Objective
1.5 Learning Objective: The student will be able to write general
statements regarding Hepatitis A (HAV).

What is Hepatitis? Hepatitis is:
• A disease that causes inflammation of the liver
What does the liver do?
• The liver is an organ that helps your body digest food and acts as a filter for poisons or anything toxic in the body
Where is it located?
• It is located in the upper right quadrant of the abdomen, tucked up under your rib cage.
General Statements (Hepatitis A – HAV)
• Hepatitis A (HAV) is a liver disease caused by the Hepatitis A virus
• 1/3 of Americans have evidence of past HAV infection
• Hepatitis A is found in the stool (feces) or persons infected with HAV

General Statements (Hepatitis A – HAV)
• It is usually spread when a person eats food or drinks water that has been contaminated with the feces of someone with HAV
• It is important to wear gloves when handling inmate linen or clothing

Signs and Symptoms of HAV
• Persons may not have any symptoms
– Older persons are more likely to have symptoms than children
• If symptoms are present, they usually occur quickly and may include:
– Fever - Tiredness– Loss of appetite - Nausea– Abdominal Discomfort - Jaundice– Dark urine

Signs and Symptoms of HAV
• The average incubation time from exposure to symptoms is 28 days (15-50 days)
• Symptoms usually last less than 2 months

Long-term Effects of HAV
• There is no chronic (long-term) infection
• One you have had hepatitis A, you cannot get it again
• There is a vaccine for hepatitis A
• If you have been exposed, Immune globulin can be given to prevent infection (within 14 days of exposure)
• About 15% of people infected with HAV will have prolonged or relapsing symptoms over a 6-9 month period
Learning Objective
1.6 Learning Objective: The student will be able to write general
statements regarding Hepatitis B (HBV).
What is Hepatitis B?
• Hepatitis B is an inflammation of the liver caused by infection with the hepatitis B virus (HBV)
• Hepatitis B is spread through contact with infected blood (usually through sex or sharing needles/works)
• HBV has both acute (new, short-term) and chronic stages (ongoing, long-term)
• The severity of the disease can range from mild or unapparent to severe or even fatal
Transmission of HBV
• You can get infected with HBV by:
1. Contacting blood/body fluids containing blood if you are not immune (via vaccine/ prior infection)
2. Having sex with an infected person without using a condom
3. Sharing needles to inject drugs or “works” (spoons, cotton, water)
Signs and Symptoms of HBV
• If you have HBV, you may experience:
• Jaundice (eyes and/or skin)• Loss of appetite• Nausea, vomiting, fever, stomach or joint
pain• Fatigue lasting weeks or months
• The average incubation period (from exposure to symptoms) is approximately 4 months

Learning Objective
1.7 Learning Objective: The student will be able to describe the
relationship between acute and chronic HBV infection.

Relationship between Acute & Chronic HBV
• Acute hepatitis B occurs shortly after exposure to the virus
• Chronic hepatitis B is an infection that lasts longer than 6 months
• About 85% of people who are infected are able to fight off the virus so their infection never becomes chronic
• The younger you are when you become infected with the hepatitis B virus, the more likely you are to develop chronic hepatitis B

HBV Vaccine
• The Hepatitis B vaccine is the best protection against HBV
• Immune globulin can be given within 7 days if you are exposed to HBV and not vaccinated. You should also be given the first dose of HBV vaccine
• Three doses are needed for complete protection (0, 1-2, 4-6 months)
HBV Vaccine
• Most young adults and children have been vaccinated against HBV by the age of 2 (or 12-18 years of age if not vaccinated as a child)
• The CDC, the National Commission on Correctional Health Care and the Society of Correctional Physicians recommend that correctional officers and correctional health care workers be vaccinated against HBV

Learning Objective
1.8 Learning Objective: The student will be able to write general
statements regarding Hepatitis C (HCV).

What is Hepatitis C?• Hepatitis C (HCV) is an inflammation of the
liver caused by infection with the hepatitis C virus
• HCV is the most common chronic blood borne viral infection in the United States
• HCV is the #1 cause of chronic liver disease and liver transplants
• HCV has both acute and chronic stages
• There is not a vaccine to prevent hepatitis C
Transmission of HCV• HCV is transmitted through blood
• The most frequent risk for HCV is sharing needles/works to inject drugs (illicit as well as steroids, insulin, etc)
• At least 60% of the reported HCV cases are related to injecting drugs
• Sexual transmission does occur, but it is inefficient (20%)
• Inmates are 10x more likely to have HCV than the US population
Signs & Symptoms of Acute HCV
• Most persons with HCV do not have symptoms
• Many persons with chronic HCV have mild to moderate liver damage but do not feel sick
• Some people with an acute infection will have jaundice (skin and/or eyes) or mild flu-like symptoms

Signs and Symptoms of Chronic HCV infection
• Most people with chronic HCV will only have mild to moderate liver disease
• Symptoms may include:
– Jaundice - Fatigue– Loss of appetite - Nausea
Learning Objective
1.9 Learning Objective: The student will be able to describe the
relationship between acute and chronic HCV infection.

Relationship between Acute & Chronic HCV
• There is no treatment for acute hepatitis C
• Over time HCV may cause your liver to stop working and a new liver from a donor may be needed
• Antiviral medicines for chronic hepatitis C are available, but they are expensive and have significant side effects

Natural History of HCV Infection
100 People
Resolve (15)
15%
Chronic (85)
85%
Cirrhosis (17)Stable (68)
80%
75%
Stable (13)Mortality (4)
25%
Time
20%
Leading Indication for Liver Transplant

Unit Two
2.0 Functional Area: This section will introduce the student to HIV/AIDS, HBV, and HCV. The student will be able to demonstrate on a written
examination an understanding of the relevant terms and definitions of HIV/AIDS, HBV and HCV.

Learning Objective
2.1 Learning Objective: The student will be able to list the four methods of
transmission of HIV, HBV and HCV.
HIV, HBV & HCV Transmission
• HIV, HBV, and HCV have similar transmission routes and are spread by direct contact with body fluids:
• Body Fluids (confirmed risk)
– Blood– Semen– Vaginal/cervical secretions– Breast milk (HIV & HBV only)

HIV, HBV & HCV Transmission
• Body Fluids (theoretical risk)
– Saliva– Perspiration– Tears– Feces– Urine
HIV, HBV and HCV Transmission Blood
• Sharing needles/syringes and/or equipment “works” to inject drugs (IDU)
• Blood transfusions/blood products (all blood products have been screened for HIV and viral hepatitis B and C since 1992 so the chance of becoming infected through a transfusion is extremely rare).
• Occupational exposures
• Tattooing/piercing in unlicensed facilities

HIV, HBV & HCV Transmission Sexual Transmission
• Unprotected vaginal, anal, oral sex regardless of partners’ gender
• Sexual transmission of HCV is low or inefficient, although any sexual activity that involves blood-to-blood contact (including menstrual blood) with an infected person can potentially transmit HCV
• “High-risk” sexual activity (e.g. multiple partners, presence of other sexually transmitted disease, exchange of sex for drugs and/or money, etc.) appears to increase the risk of HCV transmission

HIV, HBV & HCV Transmission Birth
• From an HIV, HBV or HCV infected mother to her baby during pregnancy, birth, or breast-feeding (HIV & HBV only)
• A woman who tests positive for HIV during pregnancy can take medication to reduce the risk of transmission to the baby from approximately 20% without medication to as low as 2-8% with medication
• Breast-feeding is considered safe for HCV, but cracked and/or bleeding nipples could increase the risk of HCV transmission
• Transmission from an HCV infected mother to her baby occurs in less than 5% of births. At the same time, rates of infection can be as high as 20% if the mother is also HIV positive

Misconceptions • There is no risk of exposure from donating blood
• There is no evidence of transmission from human bites, insect bites, scratches, or spit (saliva)
• There is no evidence of transmission from casual contact; i.e. closed-mouth or “social kissing”
• There is no evidence of transmission from sharing food, drink, or handling food trays
• There is no evidence of transmission from sharing laundry facilities
• There is no evidence of transmission from toilet seats and/or insects
Unit Three
3.0 Functional Area: This section will introduce the student to personal and occupational practices that place individuals at risk of
exposure to HIV, HBV, and HCV.

Learning Objective
3.1 Learning Objective: The student will be able to identify personal behavior that places individuals at risk of exposure to HIV, HBV, and HCV.
Assessing HIV, HBV, and HCV Risk
• Factors in the “Formula” for assessing HIV, HBV, and HCV risk
– Which body fluid (blood, semen etc…)
– Route of entry into body (blood stream, mucous membranes)
– Dose of infected fluid
– How long fluid is out of body before another person has contact with it
– Number of exposures
– Condition of host (how high is their viral load)
– Condition of recipient (immune system, other STDs)
High Risk Individuals
High-risk individuals are those who engage in behaviors that increase the chance of exposure to HIV, HBV, and HCV
• Male to male sexual intercourse
• People who share needles and/or “works”
• People who have sex for money or drugs
• People who have multiple sex partners
• People who have sexual intercourse with any of the above

Substance Use
• The use of substances which impair judgment can result in the high-risk behaviors listed above. These substance include:
– intravenous drugs
– alcohol
– cocaine
– marijuana
– other substances that limit the brain’s ability to function normally
Learning Objective
3.2 Learning Objective: The student will be able to define occupational exposure, identify occupational risks to law enforcement and corrections personnel and the precautions that will reduce the chance of exposure.

Can Law Enforcement & Correctional Officers be Infected
on the Job? • Every agency should have an Occupational
Exposure Program (strategies & policies)
• There have been no reported cases of occupational exposure in the law enforcement or corrections
• Peace Officers and/or corrections personnel who have tested positive for HIV were infected through activities outside of the work environment
• Risk increases when blood/body fluids containing blood enter an open wound

Occupational Exposure• The exposure occurs during the performance of the
employee’s duties;
• There is a route of exposure—in other words, a way for the viruses to enter your body. This could happen in one or more of the following ways:
– A percutaneous injury (i.e., needle stick, puncture wound or cut with a contaminated object, or from a human bite that breaks the skin); or
– Contact with the mucous membrane linings of the eyes, nose and/or mouth; or
– Contact with the skin, especially if the exposed skin is chapped, abraded or afflicted with dermatitis, or the contact is prolonged or involving an extensive portion of the body.
Occupational Exposure
• If the employee is exposed to a body fluid to which universal precautions apply. These fluids include:
– Blood (including menstrual) – Semen – Vaginal secretions – Amniotic fluid – Cerebrospinal (brain and backbone) fluid – Synovial (joint) fluid – Pleural (chest) fluid – Peritoneal (abdominal) fluid – Pericardial (heart) fluid – Saliva (in a dental setting is considered a risk factor
for HIV exposure since it is possible that blood or tissue may be present in the saliva

What about Biting or other Fluids?
• Biting is not a common way to transmit HIV, HBV and/or HCV
• There have been numerous reports of bites that did NOT result in HIV infection
• Saliva, tears and/or sweat has never been shown to result in the transmission of HIV
• Exposure to saliva, urine and/or feces (or when fluids have been purposely contaminated with blood) have not resulted in any documented cases of HIV transmission
Learning Objective
3.3 Learning Objective: The student will be able to list specific criminal
justice job related behaviors that may put them at risk for occupational
exposure.
Occupational Risks • Occupational exposure is greatest in health
care workers who experience a hollow-borne needle stick from an HIV, HBV, or HCV infected person
• Law enforcement & corrections personnel may be at risk if they fail to utilize precautions:
– Encountering blood or potentially infectious body fluids, cleaning up body fluid spills
– Conducting body and cell searches, or handling evidence that results in a puncture of the skin
– Intervening in fights

Learning Objective
3.4 Learning Objective: The student will be able to list universal precautions for occupational exposure to HIV, HBV, and HCV.
Universal Precautions & Preventive Measures
• Gloves
• Cover cuts, sores or breaks in the skin
• Wash hands or other areas exposed to blood
• Clean all spills with 1:10 bleach: water mixture
• Avoid sharing objects that could have blood on them (razors, toothbrushes)
• Dispose of needles/sharp instruments
Learning Objective
3.5 Learning Objective: The student will be able to list the prevalence of reported HIV, HBV, and HCV cases.

Reported Cases
• To date there have been no reported cases of HIV in correctional or law enforcement personnel as a result of occupational exposure
• Published reports do not document any increased risk for HBV infection among public safety workers
• To date no reported HIV infections as a result of CPR, with or without a one way pocket mask
• To date no reported HIV infections as the result of contaminated surfaces or environment

Unit Four
4.0 Functional Area: In this unit of instruction the student will be able to list the infection control procedures and steps used to conduct searches and handling evidence during the performance of the job.
Learning Objective
4.1 Learning Objective: Students will be able to list the eight general infection control procedures as outlined by the Texas Commission on Law Enforce- ment, “Facts on AIDS: A Law
Enforcement Guide”.

Infection Control Procedures• Use disinfectants such as:
- 70% isopropyl alcohol- one part bleach to ten parts water- waterless soap
• Wash hands after contact with bodily fluids with hot, soapy water
• Clean and bandage all cuts and abrasions
• Body fluid spills should be wiped up immediately and the surface area should then be disinfected
Infection Control Procedures• Soiled clothing may be cleaned in hot, soapy water or
dry cleaned
• Instruments, padding, helmets, weapons, floors, vehicles and other soiled items can be cleaned with soap and water, while wearing disposable latex gloves. Sterilize with disinfectants like diluted bleach and water (1:10 ratio) or rubbing alcohol
• Dispose of used needles in puncture-proof containers. Do not break or try to re-cap a needle, as you may jab yourself.
Infection Control Procedures
• Prepare a first aid kit for your vehicle containing the following items:
- 70% isopropyl alcohol- sterile wipes- sterile gauze- tape- plastic sharps container- latex gloves- Ziploc plastic bags
Learning Objective
4.2 Learning Objective: Students will be able to describe five of seven precautions that should be taken that
with involved searches or evidence handling as outlined in the National Institute of Justice “AIDS Bulletin,”

Searches & Evidence Handling Precaution
• Use puncture proof containers to store sharp instruments and clearly marked plastic bags to store other possibly contaminated items
• Whenever possible ask suspects to empty their own pockets
• Whenever possible, use long-handled mirrors to search hidden areas
• If it is necessary to search manually, always wear protective gloves and feel very slowly and carefully

Searches & Evidence Handling Precaution
• Use tape – never metal staples – when packaging evidence
• Wash hands thoroughly with soap and running water when tasks are completed
• Use good personal hygiene and common sense

Unit Five
5.0 Learning Objective: The student will be able to list and briefly describe the State and Local laws that govern the communicable diseases identified in this curriculum.
Learning Objective
5.1 Learning Objective: The student will be able to describe provisions
of the federal law American Disability Act of 1990 and the Federal
Rehabili- tation Act of 1973.

Federal Laws & Legal Issues• American Disability Act 1990:
– In June of 1998, the high court stated that people infected with HIV/AIDS were entitled to protection under Americans with Disabilities Act, regardless if they were asymptomatic
– Employers must make reasonable accommodations for the infected person
– When criminal justice professionals learn about an individual’s HIV status through self-disclosure or other means, they must realize that if an individual exhibits no behavior for isolation, that the detention, booking and processing policies within their agency dictates how these individuals must be handled; HIV is no exception
– Some criminal justice professionals practice selective enforcement because of someone’s known HIV status, which is discriminatory
– Some peace officers also refuses to provide lifesaving first aid based on their opinion that the individual belongs to a high-risk group

Federal Laws & Legal Issues• Federal Rehabilitation Act of 1973:
– Section 504 PROTECTS QUALIFIED PERSONS WITH HIV INFECTION
– applies to employers and organizations which receive federal financial assistance from any Federal department or agency, including the DHHS. The DHHS Section 504 regulation can be found at 45 CFR Part 84.
– If a person with HIV infection have been terminated from their jobs, denied access to social services, or denied medical treatment solely because of their handicap. Individuals have been similarly treated because they have been perceived as having HIV infection. Such actions by an agency, institution, hospital, nursing home, drug treatment center, clinic, organization or other entity receiving Federal funds may constitute unlawful discrimination under Section 504.

Federal Laws & Legal Issues• OSHA 29CFR 1910.1030:
– The employer shall make available the at no cost to the employee hepatitis B vaccine and vaccination series to all employees at risk, who have been exposed, and post exposure evaluation and follow-up to all employees who have had an exposure incident
– Hepatitis B vaccination shall be made available after the employee has received training required in para (g)(92)(vii)(I) and within 10 working days of initial assignment of all employees who have occupational exposure unless the employee has received the complete hepatitis B vaccination series and antibody testing has revealed that the employee is immune or the vaccine is contraindicated for medical reasons
Federal Laws & Legal Issues• OSHA 29CFR 1910.1030:
– The employer shall not make participation in a prescreening program a prerequisite for receiving hepatitis B vaccination
– If an employee initially declines hepatitis B vaccination but at a later date while still covered under the standards decides to accept vaccination, the employer shall make available hepatitis B vaccination at that time
– The employer shall assure that employees who decline to accept hepatitis B vaccination offered by the employer sign the statement in Appendix A of 29CFR 1910.1030
Federal Laws & Legal Issues• OSHA 29CFR 1910.1030:
– Each employer having an employee(s) with occupational exposure as defined by paragraph (b) of this law shall establish a written Exposure Control Plan designed to eliminate or minimize employee exposure
– Employers shall ensure that a copy of the Exposure Control Plan is accessible to employees in accordance with 29CFR 1910.1020.
– Exposure plan shall be reviewed and updated at least annually and when ever necessary to reflect new or modified tasks and procedures
procedures.

Federal Laws & Legal Issues• OSHA 29CFR 1910.1030:
– When there is occupational exposure, the employer shall provide, at no cost to the employee, appropriate personal protection equipment such as gloves, gown, lab coats, face shields (masks) and eye protection, mouth pieces, resuscitation bags, etc

Learning Objective
5.2 Learning Objective: The student will be able to list and briefly
describe the state laws that govern the communicable diseases identified in this curriculum.
State Laws & Legal Issues
• Texas Health and Safety Code, Chapter 81- Subchapter A
– Prevention, Control and Reports of Diseases
• Code of Criminal Procedure, Chapter 46A
– AIDS and HIV Testing in County and Municipal Jails
• Government Code, Chapter 507- Subchapter A
– Inmate Welfare
• Government Code, Chapter 507- Subchapter A
– State Jail Felony Facilities
• Government Code, Chapter 607
– Benefits Relating to Certain Contagious Diseases

HIV Testing in Texas’ Prisons
• Across The Nation | Texas Attorney General Gregg Abbott Rules that State Law permits prison officials to mandate HIV Testing among State Prisoners
• The state prison system in August 2006 had proposed a change to its HIV testing policy from saying new inmates "should be tested" upon entering prison to saying they "shall be tested" unless they opt out of testing.
• Feb 05, 2007, Texas Attorney General Greg Abbott (R) ruled that state law permits the Texas Board of Criminal Justice to mandate HIV testing among inmates upon entry to state prisons, the Houston Chronicle reports (Babineck, Houston Chronicle, 2/2).
• Sponsored legislation approved last year that requires inmates to be tested for HIV before departing prison.

HIV Testing in Texas’ Prisons
• About 80% of inmates have agreed to take an HIV test upon entering prison since the state began its testing program, and prison system statistics show more than 38,700 inmates received HIV tests in 2005. Of those, 372 tested HIV-positive. Texas law mandates that HIV test results are confidential and that HIV-positive inmates are not separated from HIV-negative inmates.
• Advocates for mandatory HIV testing upon entry into the prison system say it would help prison officials properly treat HIV-positive people, would provide more accurate data on the spread of the disease and could help officials estimate how many people are becoming HIV-positive in prison.

HIV Testing in Texas’ Prisons
• July 2006 statistics show that of 154,000 prisoners in Texas, 2,627 are HIV-positive (Kaiser Daily HIV/AIDS Report, 8/24/06). Abbott's opinion, which leaves the decision regarding mandatory testing up to the Texas Department of Criminal Justice, says that TDCJ is "authorized to adopt a rule or policy requiring mandatory" HIV testing among "incoming offenders in both the institutional division and the state jail division." According to TDCJ spokesperson Jason Clark, there is no indication that the department is planning to make HIV testing among incoming prisoners mandatory anytime soon.
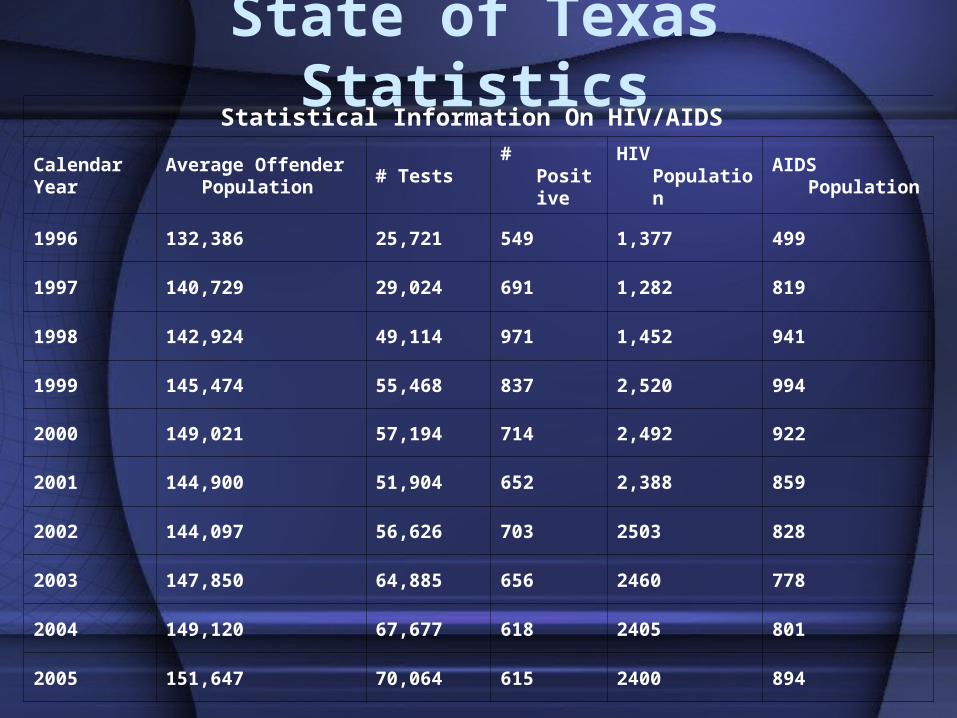
State of Texas StatisticsStatistical Information On HIV/AIDS
Calendar Year
Average Offender Population
# Tests # Positive HIV Population AIDS Population
1996 132,386 25,721 549 1,377 499
1997 140,729 29,024 691 1,282 819
1998 142,924 49,114 971 1,452 941
1999 145,474 55,468 837 2,520 994
2000 149,021 57,194 714 2,492 922
2001 144,900 51,904 652 2,388 859
2002 144,097 56,626 703 2503 828
2003 147,850 64,885 656 2460 778
2004 149,120 67,677 618 2405 801
2005 151,647 70,064 615 2400 894

Final Comments or Questions?
What other questions or concerns do you have?
• End-of-course exam
• Please fill out the course evaluation
• Be safe and remember, most HIV and Hepatitis infections can be prevented
• Thank you for your time and attention