hospital planning and project manegment (1)
DESCRIPTION
testTRANSCRIPT

Study MaterialOn
PGDHHM Correspondence Course
HOSPITAL PLANNING AND PROJECT MANAGEMENT
COMPILED BYDr. Vivek Desai
POST GRADUATE DIPLOMA INHOSPITAL AND HEALTCARE MANAGEMENT (PGDHHM)
M.B.B.S, DHA, DBM, M.Phil

Symbiosis Centre of Health Care (SCHC)
AUTHOR
Printed and Published on behalf of the Symbiosis Centre of Health Care byDr. Rajiv Yeravdekar, Hon. Director, SCHC.
Printed at Bhagyashri Printers, Pune - 411 051.
2 SCHC HOSPITAL PLANNING AND PROJECT MANAGEMENT
Dr Vivek DesaiM.B.B.S, DHA, DBM, M.PhilVisiting Faculty SIMS
All rights reserved. No part of this work may be reproduced in any form, by mimeograph or any other means, without permission in writing from the Symbiosis Centre of Health Care.

PREFACE
The future of healthcare industry in India will see a continued strong demand for construction of health care facilities, including completely new or replacement facilities and projects involving major additions and modernization. The annual value of healthcare construction projects will see a upward trend in the immediate years ahead owing to various factors like opening up of the insurance sector, privatization initiatives etc. Therefore planning and design will continue to merit prime emphasis among several responsibilities of hospital officials. Because of the changing character of facilities and continuing increase in their complexity, planning and design will assume greater importance than ever before. Thus planners, architects, builders, hospital executives, board members, medical staff representatives, and others who possess responsibility for undertaking hospital construction projects should have basic understanding of planning process and of appropriate concepts of hospital and related healthcare facility design objectives.
There are very few areas where human factors and human requirements play such a critical role as they do in hospital design. The need for collaboration between those who care for the sick and those who plan healthcare facilities is of the most critical importance. A close look at almost any hospital department today demonstrates how far short we fall in meeting the human factor goals of well being and general efficiency in hospital facility planning. It was Florence Nightingale who so succinctly pointed out “the very first requirement of a hospital is that it should do no harm to the sick.” She was referring not only to the clinical care of the sick, but also to the general psychological well being of the patient. There have been numerous instances in modern day hospital care whereby hospital acquired infections owing to faulty air-conditioning, inadequate water supply/drainage etc. have resulted in patient morbidity and even mortality.
One should define planning as the specification of the means necessary for accomplishment of goals and objectives before action toward those goals has begun. Planning involves a particular kind of decision making in which one has to specify alternatives and choose among them. Once the goals are set, alternative plans can be examined in the context of the opportunities and constraints facing the promoters. In undertaking any complex project, it is advisable to examine the experience of others in similar situations and hence such information should be elicited and properly interpreted. The basic design of a hospital usually is carried out by one or two individuals, who reflect the labor of the entire planning team in a series of drawings. The quality of the facility planning effort is ultimately dependent upon designers, who, it is to be hoped, are capable of interpreting complex relationships, internal traffic flows, technological requirements, and operational procedures to the extent that a facility of beauty, reasonable cost, and optimal utility will result. No other activity is in the planning continuum is more important than that occurring in the design phase.
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 3

Like any other industrial venture, proper planning of hospitals is vital for success of the venture. It is beyond doubt that if hospitals are properly planned and professionally, there can be substantial surplus/profit that could be made. The first step is proper project conceptualization with the right mix of beds and facilities to generate sufficient income and to attract maximum clientele. For this a comprehensive market research may be required to assess the need, demand, and supply for health care services apart from evaluating competition. A detailed financial feasibility report would then show the promoters the viability of the project subject to various scenarios like effect on profitability with change in the debt/equity ratios, project cost escalation, etc. Such studies if conducted, will go a long way in avoiding financial mishaps, which have taken heavy toll in many a project.
Once the decision is taken to build a hospital, the next step is its architectural design. A detailed architect's brief has to be first prepared to enable the architect in drawing up his plans. The landscape, facility mix, bed mix, availability of utilities in the vicinity will have to be considered. Considerable inputs from the other agencies like air-conditioning, electrical, plumbing, etc. will be required to finalize the working plan for the building. Inputs from the equipment vendors especially in specialty areas like cardiac catheterization laboratories, CT-scanners, MRI's, linear accelerators, operation theatres etc will be essential. One thing very common in India is the lack of emphasis given to support services like kitchen, laundry, CSSD, back up electricity and so forth. Not only are these services vital, but these also have high capital cost and recurrent expense and hence should be properly planned.
This module is divided into three parts in order to stress the concept of an integrated and
coordinated hospital planning.
(1) The first section is devoted to conceptualizing a hospital project in terms of the
facilities to be planned in the center. This will deal with understanding the regional
demographics and requirements of health care delivery systems in the defined
geographic service area. It entails undertaking secondary data collection and
conducting market research surveys. This will enable the student to understand the
nuances of technical and financial feasibility of a hospital project.
(2) The second section deals with the planning and design aspects of hospital
buildings and will also trace historical and future development in the field of
hospital infrastructure. There will be descriptive narration to assist the student in
understanding the important planning criteria for hospital departments.
HOSPITAL PLANNING AND PROJECT MANAGEMENT4 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT
CONTENTS
No. Chapter Page No.
1. Planning Process and Market Research ...............................................7
2. Feasibility Study...................................................................................11
3. Hospital Planning Historical Growth ..............................................15
4. Essentials of Hospital Design .............................................................22
5. Steps Involved in Hospital Design ....................................................35
6. The Design Process...............................................................................54
7. Planning of Inpatient Wards ...............................................................62
8. Planning of Clinical Departments ......................................................68
9. Planning Support Services in a Hospital..........................................126
10. The Hospital Project Team ...............................................................144
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 5

About the Author :
Dr Vivek DesaiM.B.B.S, DHA, DBM, M.Phil
HOSPITAL PLANNING AND PROJECT MANAGEMENT6 SCHC

CHAPTER 1
PLANNING PROCESS AND MARKET
RESEARCH
Healthcare in India
Healthcare in India is in a developing stage and it needs a radical policy shift at
government level to propel in the future to face the challenges of the future. Under the
umbrella of health care providers are outpatient set-ups, nursing homes, hospitals,
medical colleges, health spas, diagnostic centers, ayurvedic and naturopathy centers,
hospices, old age homes etc. Most of theses institutions will have varied needs, which
will differ vastly in terms of their planning needs. Health care provision in India is
different in rural and semi urban settings where it is more unorganized to modern day
super specialty centers where it more institutionalized. The sector suffers form long
years of neglect by the government in terms of priority funding despite being a basic
need of the community. The mechanisms for funding are fast changing to the private
sector involvement thereby pushing up the cost of both setting up hospitals as well as
availing health care in these hospitals. The lowering of interest rates over the years have
no doubt helped the cause of the private sector wherein more entrepreneurs are coming
forward to set up hospitals as it has become affordable to take loans and repay them. The
burgeoning growth of the insurance sector is equally helping the community to face the
problem pf spiraling health care costs.
Stakeholders
There are innumerable stakeholders in the health care delivery domain including the
government, philanthropic trusts, educational institutions, corporate sector, insurance
companies, bio-medical vendors, architects, construction companies, patients,
relatives, the pharmaceutical industry, professionals like doctors and other para-medical
staff, and the funding agencies. Given the wide spectrum of stakeholders, the industry
growth will benefit many in the population.
The hospital ownership pattern can be basically three types:
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 7

i) Government owned - central / state / district / autonomous like army, railways etc
ii) Not For Profit Managed by Trusts / Societies
iii) For Profit Corporate Sector
The opening up of the economy has definitely helped the cause by brining in the
accountability on various stakeholders. Even the government funding is now aided by
multi-lateral agencies like the World Bank, UNICEF, European Commission, WHO etc
wherein sustainability of the initial capital expenditure is the main concern. This is no
doubt helping us to improve the delivery mechanisms. The private sector too is
developing, aided by growth in health insurance and the industry per se is moving
towards a market economy concept throwing up cafeteria choice for the consumer.
Adding fuel to growth is the concept of medical tourism wherein Indian hospitals are
gearing up for the challenge of treating foreign patients. This needs a definite focus on
hospital planning as we have to meet the global standards, which by far exceed the ones
followed until the recent past.
Project Conceptualization
The first step in hospital planning is to freeze the project concept in terms of :
?Identification of the market needs
?Finalization of the facility mix
?Deriving the appropriate size of the project
?Determining the possibility of getting skilled manpower
All the above factors have a bearing on the project cost and its viability in future. This
process understands the need of the community that will be served by the hospital in the
given geographic location. For doing this, one needs to undertake a detailed Market
Survey by collecting secondary data from various sources like the internet, libraries,
media publications, news paper archives, ministry of health and district health
departments records etc. Unfortunately India does not have a reliable mechanism for
capturing health related data especially in the private sector. Hence, one needs to
undertake primary data search by conducting interviews with house holds, practicing
doctors and visiting existing institutions. There can be three types of surveys required:
HOSPITAL PLANNING AND PROJECT MANAGEMENT8 SCHC

a) House Hold Survey : This is essentially done to understand the health care seeking
behavior pattern of the community as a whole. Sampling techniques are used to map
the statistically significant number of households. The basic information which
should be collected and analyzed is as follows:
- Demographic details of the family- Education & Income details- Disease profile in last three years- Choice of health care provider for minor & major ailments with reasons - Method of payment for availing healthcare- Their feel on deficiency in health care market- Critical success factor for the proposed project
b) Doctor's Survey : Medical professionals are normally the best judge of the
deficiency in the health care market and need to be interviewed carefully to identify
the project concept that would succeed in the geographic service area. The sample of
doctors to be interviewed should include professionals from all possible faculties in
medicine and surgery including those from diagnostic divisions like laboratories,
imaging, physiotherapy etc. The basic information to be collected and analyzed
from them would be :
- Personal details on specialty, qualification, experience etc- Area of practice and hospital attachments- Patients seen and their drainage area- Referrals to other hospitals/diagnostic centers with reasons for referring- Views on deficiency in health care market and solutions for same- Patient's capability to pay- Critical success factors for a hospital project in the service area
c) Institutional Survey : Getting a basic feedback on the competitors in the primary
service area of say 5-10 km radius would be important to assess the strengths and
weakness of major players. One would also need to know the productivity, tariffs,
salary structure etc which would help us in preparation of the feasibility report. The
important information to be collected would be as under:
- Ownership with historical growth pattern- Service Mix (diagnostic, therapeutic, medical, surgical, support services)- Bed mix - Productivity of major services
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 9

- Tariffs of major services- Bed to manpower ratio- Technology level- Annual revenue/expense in last 2-3 years to understand growth pattern
Data Analysis :
The data collected through secondary and primary sources is then analyzed to identify a
proper facility mix for the proposed project. It will also determine the scale pf the project
in terms of its bed size. In case it identifies some atypical need like cancer treatment, it
would perhaps need more research to understand the profitability of such capital
intensive specialty. The end result should give definitive information on the following:
i) Specialties to be practiced in the proposed projectii) Number of OPD rooms
iii) Bed mix with break up
iv) No of operation theatres
v) Diagnostic services
vi) Blood bank
vii) Support services
In case the project is to be developed in phases the facilities to be phased should be
clearly identified as the engineering services and areas for the phased development will
have to be carefully planned.
HOSPITAL PLANNING AND PROJECT MANAGEMENT10 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 11
CHAPTER 2
FEASIBILITY STUDY
After finalizing the Project Concept in terms of its facilities and size, the next important step is to analyze its financial viability. This will also help the promoter in planning the means of financing the project based on its profitability and capability of servicing the debt proportion.
The first step of the feasibility process is to identify the cost of the project in a realistic manner. Many projects have failed midway through construction process wherein it was identified that the cost overrun would be in more than 50% of the estimated budget. Hospital buildings are very complex in terms of its engineering needs and hence specialized agencies are required to plan these and identify the cost. The cost of the project should be broken down under the following heads:
i) Civil Works including RCC, masonry, doors, windows, interior, and façade treatment
ii) Electrical Works
iii) Plumbing and fire fighting
iv) Air Conditioning
v) Landscape and site development
vi) Elevators
vii) Medical equipment broken down under departmental heads
viii) Non medical equipment like kitchen, laundry, computer hardware & software etc
ix) Hospital furniture and fixtures
x) Professional fees
xi) Pre Operative Expenses
xii) Municipal Taxes & deposits
xiii) Interest during construction
xiv) Contingency
The estimates for all the above should be compiled meticulously after detailed discussions with experts and undertaking adequate research. Financial institutions also required sufficient back up data to accept the costs before accepting the project for funding.
Income Assumptions:
After compiling the project cost, the next important step is to ascertain the income from the project from various heads. Whilst doing this, one would rely heavily on the institutional market research to understand the industry benchmarks for making assumptions. Income assumptions will need to be made for the following income heads:
i) Room rents for all categories of beds like general ward, twin/single rooms, ICU, NICU etc.
ii) Departmental income for diagnostic services (lab, radiology, EEG, EMG, non-invasive cardiology, audiology, cath lab, refraction etc)
iii) Income from OPD & IPD consultations
iv) Income from surgical operations (major and day care surgeries)
v) Health check schemes
vi) Pharmacy
vii) Emergency
viii) Dialysis
ix) Deliveries
x) Blood Bank
xi) Emergency
xii) Any specialty service like LINAEC, IVF, Angioplasty, Minimal Invasive surgery, organ transplant etc. will need to be separately assessed
For calculating the income some important assumptions will need to be made with regards to the number of OPD/IPD days in a year, bed days available depending on the bed capacity, average length of stay (ALOS), number of admissions, number of operation theatres, number of OPD rooms etc. These assumptions form the important basis for assuming a realistic productivity for various departments which when multiplied with an average tariff rate will give the income on an annual basis. An example for assumption is given below:
HOSPITAL PLANNING AND PROJECT MANAGEMENT12 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 13
Number of beds - 100
Number OPD days - 300
Number of IPD days - 365
Bed Days available - 100 x 365 = 36,500
ALOS - 5 days therefore no of admissions
= 36500/5 = 7300/annum
Number of theatres - 4 , No of surgeries / OT / day
= 4, therefore surgeries/annum = 4 x 4 x 300
Number of OPD - 10, no of patients / OPD / hr = 4,
No of OPD/annum = 10 x 4 x 10 hrs = 400
Number of X-ray - 1 per admission for IPD and
10% of all OPD cases
One has to assume such productivity for all departments by using sound logic and keep cross checking it with some industry benchmark. All income is calculated on 100% capacity utilization and then adjusted for year wise utilization as % in year 1, year 2, year 3, till year 10. It is important to include all heads of income as may be possible.
Expense Assumptions:
The next important step is to compute all the important expenditure heads for the project operations. These heads would include the following:
i) Salaries and wages these should be computed on a cost to company basis and should take into a staffing pattern inclusive of those for leaves, contract labors etc.
ii) Departmental expenses in terms of consumables. This could be arrived as percentage expense to the departmental income by taking industry benchmarks
iii) Professional fee payable to doctors for rendering clinical services. This would differ from assuming a flat salary to incentive based remuneration. Again industry benchmarks will have to be followed for same. Some hospitals have a mix of both the options

iv) Energy costs in terms of electricity, water, medical gases, generator
v) Food expenses for patients and staff
vi) Laundry & linen expenses for patients and staff
vii) Housekeeping expenses can be calculated on a per sq ft basis for the building
viii) Stationery expenses
ix) Telecommunication
x) Conveyance and car maintenance
xi) Marketing expenses
xii) Repairs and maintenance
xiii) Insurance, Legal and Audit charges
xiv) Miscellaneous expenses
xv) Depreciation
xvi) Interest cost for loans taken
xvii) Taxes for corporate hospital
Financial Statements:
After computing the income and expense statements as mentioned above, one arrives at the various financials such as Profit & Loss statement, Balance Sheet, Cash Flow, break even analysis. After computing these statements once can undertake sensitivity analysis by subjecting the project assumptions certain changes and evaluating the impact on profitability like:
- Change in debt to equity ratio
- Change in interest rates on the loan taken
- Change in capacity utilization over the five year period
- Effect of cost escalation
Such meticulous financial analysis will give the promoter confidence to decide on whether to undertake the project or not. This also helps them to arrive at a proper debt to equity ratio for the project.
HOSPITAL PLANNING AND PROJECT MANAGEMENT14 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 15
CHAPTER 3
HOSPITAL PLANNING - HISTORICAL GROWTH
The hospital as an institution offering care to those who need it is of great antiquity. The
modern word is derived from the Latin hospes (“host”), which is also the root for the
words 'hotel', 'hospice', and 'hospitality'. The earliest examples approximating the
institutions we call hospitals, however, were the Egyptian temples of 4000 years ago.
The association of religion and medicine was a natural one in many ancient cultures.
Originating in the time of the matriarchal goddess religions, when the cyclical process
of nature and women's ability to give birth were revered, the relationship between the
midwife and the woman giving birth was the first healer-patient relationship. In
primitive societies those seen as holding mystical powers came to acquire more formal
ones. Thus healing and believing brought forth the faith healer.
Early knowledge was gained both from intuition, as well as from watching animals and
then passing on the accumulated knowledge down through the generations. Apart from
primitive tools there was no technology and medicine was based upon touch, comfort
and belief.
The early Egyptians identified over 250 diseases and combined medicine with magic
and religion. As they developed the science of medicine, treatment and drugs, there was
parallel development in improvements to public hygiene and sanitation. The
Babylonians further developed medicine and records show that fees were charged for a
healer's service. Yet it was the Greeks who gave us Hippocrates and the famous oath.
Greek buildings used for medical care were still similar to temples. The Greeks however
viewed healthcare in a natural and totally holistic framework. The Greeks assumed, as
only natural, that healthcare treatment should include music, poetry, arts and good
cuisine. Temples dedicated to Asclepius were noted for their cures.
The idea of an institution created specifically to care for the sick appeared in Hindustan
in the third century B.C., and in first century Rome. In Hindustan, the king Ashoka is
credited with establishing some 18 centers for treating the ill. There were physicians and
a nursing staff, and the expense was borne by the royal treasury. Hospital style
institutions appeared in China in the first millennium A.D., as part of a state supported

care system, while in Rome there were special institutions for slaves, gladiators, and
soldiers.
From about 500 BC to 475 AD the Romans assimilated medical cultures from the
territories that they inhabited. Generally, the Romans, as the Greeks, provided
healthcare in the community. The Roman hospital was built upon a military regime
within a rigid institutional setting. Thus the early example of what has become known as
the medical model was indeed based upon the military model, that is, the provision of
care within an ordered and military setting.
The early Christian era, between 1 and 500 AD brought the return of women in the role
of healers through the Church and convents. It was the Christian commitment to care for
the sick, to comfort the lonely, and to feed the hungry which motivated the prodigious
growth of hospices, orphanages, old age retreats and hospitals proper throughout the
medieval world. The first Christian Hospital was completed between 368 and 372 AD.
During the chaos that followed the collapse of the Roman Empire between 500 and
1000 AD, monasteries retained the teachings of the early Greek texts. Monks used their
knowledge of medicine and herbs to care for the sick and the term hospital was
synonymous with offering hospitality, i.e., refuge from the ravages of the outside world.
Clarity of form was lost during the medieval Christian period, and hospitals once again
became indistinguishable from medieval architectural forms.
In the medieval west, as in the east, the church bore primary responsibility for
developing institutions of care. Among the hospitals built by it was the Hotel Dieu,
founded by the Bishop of Paris in the seventh century, which today is the oldest working
hospital in existence. Hospital facilities expanded radically from the eleventh through
the fourteenth centuries. The Crusades were in part responsible. The crusading orders
built hospitals in Germany and throughout the Mediterranean world. Royal and noble
families also contributed to the growth. England's first hospital was built at York in 937
by Athelstan, a grandson of King Alfred the Great. In the twelfth and thirteenth
centuries, when Europe was in the grip of a vast leprosy epidemic, hundreds of leper
asylums or leprosaria were built. It has been estimated that in 1225 there were 19,000
leprosaria in Europe. As leprosy declined, some of these leprosaria became hospitals.
Thus the Hospital des Petits Maisons outside Paris which began as a leprosaria was alter
used for indigent syphilitics and mentally disordered pilgrims. When the bubonic plague
struck Europe in the fourteenth century, the leprosaria were the first plague hospitals.
During the seventh century, the rise of Islam led to the Muslim conquest of many
HOSPITAL PLANNING AND PROJECT MANAGEMENT16 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 17
countries. Islam inherited a rich medical tradition, and by the ninth century it had
established a sophisticated medical system. Hospital complexes were constructed at
Baghdad in the ninth and tenth centuries which employed up to 25 staff physicians,
which maintained separate wards for different conditions, and which gave medical
instruction. Thirty-four such hospitals have been identified in Muslim cities from
Mughal India to Spain. Islam, like Christianity, emphasized the community's
responsibility for those who needed help.
Byzantium's political resurgence under the powerful Macedonian dynasty in the ninth
and tenth centuries brought further hospital construction. The famous Pantocrator,
which was begun by John II Comnenus in 1136 was built as part of a complex of
buildings which included a sumptuous church, tombs for the ruling dynasty, and a
monastery. This hospital was the greatest achievement of the long Byzantium tradition.
The hospital comprised 50 rooms which were divided into 5 departments. There were 5
rooms for surgical cases, 8 for acute illnesses, 10 each for men and women with various
complaints, and 12 for gynecological cases. The remaining 5 were available for
miscellaneous use, including emergencies. Each department had a staff of two
physicians, five surgeons and two nurses or attendants. There were also an out-patient
department for ambulatory cases, a pharmacy, baths, a mill and a bakery.
Later, in classical antiquity, the rational processes of thought were reflected in the plan
form, which gradually evolved a character of its own. Order and clarity became evident
and clear patterns of circulation were delineated and attention was paid to functional
groupings. More scientific methods of healing appeared throughout the Renaissance
period, 1400 - 1700 Ad. This was also the time of Michelangelo and Leonardo da Vinci
who saw the integration of art, invention and medicine.
In England the traditional role of the Catholic Church in healing and medicine declined
as Henry VIII broke away from Rome. The closure of monasteries by him and the
resulting loss of there medical expertise was a spur to the development of the medical
profession, which then developed outside it's religious origins. He encouraged and gave
authority to physicians, granting the College of Physicians a charter in 1518. The years
1550 to 1850 were the dark period of nursing. Women were assigned nursing duty in lieu
of a jail sentence. Many hospitals fell into decay, and unsanitary conditions, epidemics
and diseases were common. The hospital was seen as a place to warehouse the sick and
dying and not necessarily a place for care and treatment.
By the end of the sixteenth century, monarchs and municipalities had become the prime

movers in hospital development. In France, as in most continental European states, the
central government took responsibility. In 1656 the Cardinal Mazarin created the
Hospital General in Paris. These hospitals showed the evolution of the medieval concept
of care into the secularized one of the sixteenth and seventeenth centuries. Though much
larger and administratively complex than their medieval predecessors, these institutions
were similar in that social functions were fundamental, while treatment was of minor
importance. A further change, however, was coming. Vesalian anatomy, William
Harvey's circulation theory, and a growing interest in clinical medicine were giving
hospitals a new significance. It was there that the actual sick could be observed, that
medical applications of scientific discoveries could be made most conveniently, and
that students could be taught. Bedside observation and teaching began in 1626 at
Leyden and Utrecht, won support from leading English scientists including Sir Francis
Bacon, and through the work of Hermann Boerhaave, the Leyden clinician and one of
Europe's greatest teachers, gained a European following. Even so, the transformation of
the hospital into a medical institution was not complete for another century and a half.Between 1700 and 1850 the foundations of the modern hospital system were
established. The number of hospitals increased, the quality of medical practice
improved, specialization advanced, and the emphasis shifted from care towards
treatment and cure. The process was most rapid in England, whose 18th century
development was phenomenal, but by the middle of the 19th century most European
societies as well as the United States had established a basic hospital system. In the
American colonies the first hospital was founded in Pennsylvania in 1751, with
Benjamin Franklin as a Trustee. Throughout the entire period of development, two
contrasting systems for planning and financing hospitals appeared. In England and
America, private funds and independent boards were the norm. On the Continent,
central governments and public funds led the way. The American hospitals served a
social need, but their staffing with trained physicians as both house physicians and
consultants showed an orientation from the beginning towards treatment and cure.
The brilliance of French medical scientists both before and after the revolution was
unconnected with the state of hospitals or other institutions. At this time, hospital
reformers, activated by a humanitarian concern over the real suffering of those
unfortunate enough to be hospitalized and convinced that an enlightened age had the
means to relieve it, began to agitate for changes. John Howard, an English prison
reformer who became interested in hospitals, was probably the person who did the most
to popularize reform ideas on the Continent. He was particularly emphatic about the
need for cleanliness and fresh air to combat the deadly miasmic vapors which were
thought to be responsible for illness, infection, and high mortalities.
HOSPITAL PLANNING AND PROJECT MANAGEMENT18 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 19
Probably the most important 18th century Continental hospital was Vienna's
Allgemeine Krankenhaus (general hospital) built by the order of the emperor Joseph II
in 1784. This hospital epitomized the Enlightenment absolutist's approach to medical
care and public health through administrative centralization and rationalization of
function. It also showed the growing conviction that hospitals were primarily
institutions for treating sick people, while its provision to accommodate both the poor
and paying patients struck a modern note. Vienna's influence was also significant
throughout other parts of Europe, appearing in a series of 100- to 200-bed hospitals built
between 1784 and 1850.
The combination of further scientific study and epidemics such as cholera in the United
States from 1830 to 1850 created a demand for more hospitals. As hospitals grew larger,
so the incidence of cross-infection became greater. A big turning point for health-care
was the Crimean War. In Crimea, Florence Nightingale gained fame for her nursing
skills. At the end of the war Nightingale became committed to designing hospitals. She
devised a series of concepts that had to do with light, air and cleanliness. She understood
the need to plan care buildings to avoid cross-infection. The dramatically low
mortalities in her temporary barracks at Scutari made her a nearly irresistible influence
on questions of hospital organization and architecture. She introduced a regime of
greater cleanliness and order and the now famous Nightingale ward, born out of the need
for a stricter regime of care and discipline, left an indelible mark on the subsequent
planning of healthcare buildings.
Both in the Crimean War and in the American Civil War, a need was recognized to
improve medical care through cleanliness, discipline and scientific rationality. Both
sides built large temporary military hospitals which were considered models of
organization and further proof for the 'fresh air' thesis. Treatment on the battlefield
became the generator for new models of care planning. Surgery until then was always
seen as a last resort. The outcome was invariably poor due to cross-infection and pain
must have been horrendous without proper anesthetic. Yet towards the end of the 19th
century, with Louis Pasteur's and Joseph Lister's understanding of living organisms and
methods of antiseptic, the surgeon came to the fore. As it became understood that
surgery was best undertaken in antiseptic conditions, the importance of the hospital as
the focus of healthcare treatment became further established. X-ray technology, which
developed first as a diagnostic tool, became a form of therapy requiring special
instrumentation and facilities; while advances in biochemistry opened a wide variety of
treatments and diagnostic tests which only a fully equipped laboratory could perform. In
much the same way that manufacturing technology shaped the factories and shops

necessary to its efficient use, medical technology influenced the development of the
modern hospital. The key dates may said to be :
! 1846- The discovery of anesthetics, which spread throughout the Western world
within a few years.
! 1866-9 - Lister's use of carbolic sprays for antiseptic surgery, which by combating
infection enormously reduced the number of post-operative fatalities.
! 1886 - Von Bergman's introduction of aseptic techniques, the sterilizing of
instruments and the use of autoclaves.
! 1895 - Roentgen used X-rays as an aid to diagnosis. Instead of relying on their five
senses, doctors now had the possibility of confirmation in black and white.
Laboratories similarly added a new dimension to medicine and enormously
extended the use of pharmaceuticals.
Not until the late 18th and early 19th centuries was hospital planning treated on a
functional and scientific basis. Then the 'pavilion' type plan evolved, segregating
patients into small groups and ensuring natural light and ventilation. Two other factors
led to this kind of planning. Fear of contagion led to segmentation into increasingly
isolated pavilions, and differentiation of the medical profession led to the organization
of many pavilions into specialty departments. The period from the turn of the century to
the present day has seen the architectural forms of hospitals change from low horizontal
pavilions to a vertical mono-block.
With the discoveries of X-rays and radium, the diagnostic approach to healthcare
became bound to a building rather than being brought to the people. Technological
advances accelerated throughout the 20th century. Each bore the need for new
equipment, with technology further centralizing and emphasizing the place of the
hospital as the main focus of medical skills.
After World War II, major factors influencing the evolution of hospitals in the US were
primarily internal in nature. Major design influences related to changes occurring within
a particular hospitals medical staff or those produced by new treatment modalities and
equipment. External forces played a relatively minor role in influencing design, and the
evolution of one hospitals facility was little influenced by any other institution, except
during periods of competitive action.
During the 1960's, architectural firms in the US specializing in hospital design directed
!
!
!
HOSPITAL PLANNING AND PROJECT MANAGEMENT20 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 21
their efforts to developing new programming techniques, applying systems theory to
planning, and updating departmental planning through functional analysis. The space
age that flowered in the 1960s was another turning point for hospital design. Electronic
devices developed for NASA included CRTs (cathode ray tubes) for monitors and
imaging devices. With the 1970's came several changes in the health care system which
shifted emphasis in hospital design. The most important factors influencing the physical
organization of the hospital were no longer internal changes but external constraints. Important forces of change were :
! Federal government's participation in the health field.! Changing patterns of illness and new modalities of treatment.! A new emphasis on the treatment of chronic diseases.! Extension of health care benefits to employees through OSHA.
The principal areas in which these changes made their impact on the physical plan of the
hospital were :!! Size, type and distribution of inpatient care units.! Growth of outpatient services and increased emphasis on ambulatory care.! Role and design of emergency departments.! Inter-relationships of the various departments within a hospital.! Overall relation of the hospital to the community it serves.! Regionalization of the health care system.
Scientific medicine administered through hospitals has proved to be very costly.
Publicly funded insurance and compensation plans and state-funded free medical care
have helped to ease this problem in Europe. In the United States private health insurance
has been the favored method. In the course of the 1970's, it became clear that private
insurance protection against high hospital costs was inadequate, and the creation of a
further national health insurance program has become a political issue. It is also widely
believed, however, that insurance programs have underwritten the rising costs of
hospital medicine while promoting unnecessary use of hospital facilities. At the same
time, rising costs have produced cutbacks in hospital services as well as hospital
closures, raising again the problem of accessibility to care for the poorest groups in
society.
Today, the weight of economics, social values, and futurist ideas necessitates a
reassessment of this series of “gifts” of history. Some of these gifts have become
liabilities. The reasons for original design are important; if they are understood, it will be

ESSENTIALS OF HOSPITAL PLANNING
CHAPTER 4
Choosing a Site
(1) The first consideration in choosing the site of a hospital is convenience for the
patients. In view of the increasing importance of the outpatient service given by
the hospital, convenience of access to patients is absolutely essential, and should
take priority over other factors in the selection of the site.
(2) The next most important consideration is that the site should be large enough to
enable the hospital to expand and develop in the future. Central positions, in urban
areas, are in great demand; it is often difficult, to find a site big enough for a
hospital in a central area. Sometimes there is a fairly well developed main
residential area, and the hospital can be sited in a central position in relation to this.
Sometimes it is known that the town is going to expand in a particular direction;
and it may be possible to find a large site fairly near the periphery of the present
town that will, in due course, become central to the major residential area.
(3) Close collaboration with town-planning authorities is necessary in choosing the
hospital site. In determining the area for the hospital, preliminary calculations are
necessary. These will show the approximate total volume of the building, and the
site area must be related to this. The degree of crowding on a site can be considered
in terms of “plot ratio”. This is the ratio of the total area of the building on all floors
to the area of the site. A “plot ratio” of one represents a building whose total floor
area is equal to the area of these site that is to say, if the hospital is to be a two-storey
structure, half of the site will be covered with buildings and the other half will be
available for open space, access roads, car parking, and so forth. For purpose of
reference, it may be assumed that a plot ratio of two to one is the greatest that
should be considered for hospital development, and that this ratio is acceptable
only in the centers of cities, where a high density of building is the rule. Generally
speaking, it will be found that hospitals developed at a plot ratio of two to one will
give a crowded site, high buildings close to one another, very little open space, and
a certain amount of overshadowing and overlooking between the buildings. In
suburban and rural areas, a site should be sought and given plot ratios of 0.5 to one
or less. The degree to which a site may be built up will depend, to some extent, on
HOSPITAL PLANNING AND PROJECT MANAGEMENT22 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 23
whether the hospital is in an urban or rural area, on the climate, and on the general
character of buildings in the neighborhood.
(4) In most cases a site should be accepted only if it provides room for substantial
future growth.
(5) In principle, the site should be at least double the area required for the hospital as it
is originally planned.
(6) As soon as one or more possible sites satisfying the requirements as set out above
have been found, they should be surveyed by the architect, assisted by an engineer.
(7) The site will need to have available, from public services, supplies of water,
electricity, and, perhaps, gas.
(8) It should also have main sewerage that is capable of carrying the hospital effluent.
If main sewerage is not available, the suitability of the soil for the installation of an
effective sewage plant will have to be investigated.
(9) It should also be established that the site is free from air pollution from adjoining
industries or other sources and free from insect vectors of disease.
(10) The proximity of sources of noise should be avoided.
(11) In hot climates, it is important that the site be exposed to breezes, and in harsh
climates, it should be reasonably sheltered.
(12) The bearing qualities of the soil will also require investigation; the risk of earth
movements, geological faults, or underground mine workings has to be considered.
The Master Plan
The first task of the architect is to prepare a master plan for the site as a whole. This plan
should take into account foreseeable future developments of the hospital as well as the
buildings erected in the first project. An architect who has specialized in hospital
construction will be able to prepare a hospital plan once the results of the early studies,
previously discussed, are available. At this stage there will be no schedules of
accommodation or detailed plans of the individual buildings, but an architect with
sufficient experience will be able to calculate the approximate volume of each building
from the general data that are available.
The master plan is the equivalent of an exercise in town planning. It is mainly

concerned with establishing the circulation routes on the site and the relative disposition
of the various departments and buildings that make up the hospital. The circulation
routes on the site are of prime importance, and the success of the hospital plan depends
very largely on getting them right. A hospital has two independent sets of circulation
routes external and internal.
All the major departments need to be linked by internal traffic routes for the use of
patients and staff and for the delivery of supplies from the supply areas to their points of
use. A great deal of the interior traffic in a hospital involves the use of trolleys. Bedfast
patients are moved on beds or trolleys; food and supplies are generally also moved on
trolleys. Trolleys cannot be pushed up stairs, and all vertical circulation points within
the hospital therefore have to be provided with lifts. Much of hospital planning stems
from the problems of internal circulation and, in particular, the need to localize vertical
circulation, so far as possible, at certain key points. It is very much more economical
and efficient to concentrate lifts than to distribute them among different parts of the
building. Four lifts banked together will give the same service as eight individual lifts
distributed at separate points.
The external traffic within the site is considerable. Ambulances and delivery vehicles
need access to the buildings at various points. Staff and visitors to patients need car-
parking facilities. There is likely to be a point, or points, where the majority of deliveries
are made for the hospital as a whole, it is also desirable to have road access to all major
sections of the hospital, and certainly to any independent buildings that there may be.
This access will facilitate the bringing of heavy items of equipment close to the point
where they are to be installed. It is also necessary for the use of fire engines in the event
of fire in the hospital, and will facilitate the maintenance of the fabric of the buildings.
In developing the master plan, areas have to be allotted within the site for each major
department of the hospital. These areas should always be large enough to allow for each
department to expand by additional building while remaining properly connected to the
circulation networks. Only if this is done will it be possible for the hospital to grow in an
orderly manner.
Certain broad principles for establishing the departmental zones may be set forth. The
parts of the hospital that are most closely linked to the community should be allotted
positions closest to the main entrance to the site.
These include the outpatient, casualty services and such offices or other facilities as are
needed to provide a base for domiciliary services. Next in order of distance from the
entrance should be a zone allotted to the medical service departments, such as radio
HOSPITAL PLANNING AND PROJECT MANAGEMENT24 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 25
diagnosis and the laboratories. These departments receive a great deal of work directly
from the outpatient department and need to be close to it. Beyond this is the area allotted
for inpatient care. Apart from the areas of the hospital used by the patients, there is a
substantial area required for the housekeeping and domestic services stores, laundry,
kitchens, and boiler house. These departments are best grouped together around a
service yard, to which most of the delivery vehicles will go. This service area should be
independent of, the main hospital entrance. Staff housing, which will take up a
substantial proportion of the site, can best be placed around the perimeter, to give the
staff easy access to roads and public transport.
The considerations set out above will need to be related to the nature of the site. In many
climates the orientation of buildings in relation to sunlight or to the prevailing breeze
will determine many aspects of the master plan. Many sites are sloping, and this may
provide both difficulties and opportunities in planning
Planning for Growth and Change
The first requirement in providing for growth and change is room for expansion in the
master plan, but there are other factors that need consideration. The master plan can
develop in the form of (1) A very concentrated building, making use, where necessary,
of multi-storey blocks; (2) Or it can be comparatively loose, occupying more area on the
ground and employing lower buildings.
The former approach will lead to a hospital, which is compact and in which the distance
from point to point within the hospital is minimized. There are many advantages in a
compact hospital,
(1) It saves the time of the staff,
(2) It helps to promote collaboration by making it easy for members of the staff to meet
one another.
(3) But the more the hospital is planned as a single, massive block, the more difficult
will it be to make effective provision for growth and change
(4) The concentration of all departments close to one another means that only a very
little space is available for each to expand
(5) Further concentration makes it inevitable that the buildings go up to a fair number
of storeys; and to add to a department on the fourth or fifth floor of a block is always

difficult, and sometimes impossible. If such a department needs to be extended, it
means taking over space from some adjoining department above or below it. This
will involve massive redistribution and reorganization of many departments. It is
therefore necessary to weigh very carefully the advantages and disadvantages of
concentrated versus diffuse types of structure.
The principal factor in the decision will be the prediction of the amount of change and
growth likely to occur. It may be that some sacrifice in concentration during the early
years of the hospital's life will be justified in the interests of allowing for future growth
and change. The preparation of a master plan at an early stage will being this
consideration forward and enable the advantages to be weighed and a rational decision
to be reached.
It is essential to consider which parts of the hospital are most likely to require room for
growth and which are relatively static.
The increase in cases coming into the hospital results directly from the increase in
motor traffic, and sometimes from mechanization in industry; and there seems no
reason to suppose that further development in these directions will not cause continued
increase in casualty rates.
The medical service departments, particularly the radio-diagnostic service and the
laboratories, will generally need to be extended. The demand for these services by the
clinical staff is continually increasing as new methods of diagnosis and treatment
become available. Therefore, these departments should be planned to allow for
substantial growth and should, if possible be at ground level, or in two-storey buildings.
The accommodation for in-patients may, as the services required on each in-patient
floor can be conveniently and economically designed to run up and down in a vertical
building, e.g., lifts can be planned to deliver food trolleys to the ward pantries of every
floor. The lavatories, bathrooms and sanitary rooms can be replaced one above the
other, making use of vertical ducts for plumbing services.
It may not be necessary to increase the total amount of in-patient accommodation
within a hospital. It will almost certainly be necessary to redistribute the
accommodation among the different clinical departments, whose relative requirements
for beds are likely to change within the life of the building. This can best be provided
for by having on each floor a single, general- purpose arrangement, capable of taking
any category or patient; then, shifting a user from, say, medicine to surgery on a
particular floor will not involve any structural change. Certain in-patient
accommodation - for children, maternity, infectious diseases, and psychiatry will
HOSPITAL PLANNING AND PROJECT MANAGEMENT26 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 27
require special planning, As a result, the in-patient accommodation for these services
may best be planned as separate wings apart from the main block.
Considerations Based on Climate
This is important criteria in country like India wherein there is diverse climate as we
move from North to South and East to West. In certain climates, building have to be
heated in winter or cooled in summer; and, in some areas, buildings may need both
heating and cooling, at different times of the year. Wherever this is the case,
concentrating the buildings as much as possible can reduce running costs. The more
spread out the hospital, the larger is the surface available for heat loss or heat gain and
the more expensive is the maintenance by artificial means of the desired internal
conditions.
The expense of cooling by air- conditioning is very great, far exceeding that of heating
in most climates. Therefore, wherever air- conditioning is deemed to be necessary, the
building should be designed in as compact a manner as possible. The cooling costs will
be directly proportional to the volume of the building, so the volume should be kept
down by the use of low ceiling and by restricting the size of rooms to the absolute
minimum. It is of vital importance that the decision should be taken at an early stage as
to whether cooling by air- conditioning is required, as the whole design of the building
will be affected by this decision. When in a hot climate it is concluded that air-
conditioning is unnecessary or impracticable, the design of the building must be
carefully considered in order to get the maximum natural cooling. In hot climates, air-
conditioning will always be needed for operating theatres and, very often, for recovery
wards, labor rooms, X- ray rooms, and other special areas.
There has been considerable research on the design of buildings for various tropical
conditions, and the results are available in the form of recommendations. It is worth
noting that the design of a building for comfort in a hot, humid climate is totally
different from that in a hot, dry climate. Broadly speaking, in the former air movement
past the body is the main objective. The buildings should be light and open and planned
so that even the slightest breeze can pass right through the buildings at low level to cool
the occupants. It is impossible to plan highly concentrated hospitals for use in hot,
humid climates without recourse to air- conditioning. In hot, dry climates, the nights are
cool, and the object of the building design is to protect the occupants from the fierce heat
during the day. Buildings in these climates are therefore massive, with heavy walls and
small windows. The heavy walls absorb the daytime heat and dissipate it at night. The

small windows keep the amount of radiation entering the building to a minimum.
In developing the master plan, attention must be given to the relation of building to each
other with regard to sunlight and shade. In cool climates, where sunlight is desirable,
buildings should not be planned so as to cut off one another's light. In hot climates, the
buildings can be planned to shade each other to some extent. The shadows cast by the
sun can be studied by means of models on a device known as the heliodon, which
simulates the movement of the sun. Architects concerned with the building of hospitals
in tropical climates should take care to familiarize themselves with the great mass of
valuable information now available on design for comfort.
In temperate climates, where the winters are not very long or very severe, it will not be
necessary to give great weight to the problem of heating in relation to the general plan of
the hospital, which can be designed primarily with other considerations in mind. But in
climates of extreme cold and long winters, where the cost of heating is heavy, some
thought should be given to making sure that the general plan results in a reasonably
compact building.
The methods used for heating and ventilation of the hospital are important, as bad design
can increase the risks of cross-infection. Massive ventilation is very advantageous in
reducing this risk. In warm climates, massive natural ventilation is easily obtained and
is desirable, for comfort. It will therefore be wise to rely, in hot climates, on natural
ventilation as much as possible and to have recourse to air-conditioning only under
extreme conditions.
In cold climates, the ventilation of hospitals during the winter presents difficulties, as
sufficient ventilation is apt to cause undue cooling by the introduction of cold air from
the outside. Any proposal for artificial ventilation or air-conditioning in hospital
buildings must, therefore, be submitted to expert bacteriological criticism before
adoption.
Certain areas of the hospital must always be provided with artificial ventilation or air-
conditioning. These include the operating theatres and any other areas where open
wounds are exposed to the air. These areas must be ventilated by special means to give a
high degree of air hygiene. The design of a ventilating plant for these purposes is highly
specialized, and must be entrusted to an expert.
Light and Color
Windows light most hospitals. It is important that patients lying in bed should not be
HOSPITAL PLANNING AND PROJECT MANAGEMENT28 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 29
exposed to too large an area of sky in direct view through the windows. Control of glare
from windows requires great care in design, and various special arrangements have
been proposed for this purpose. It is therefore important for the architect to consider the
design of the windows in the light of criteria that are now known to be good for hospital
purposes.
Criteria for the artificial lighting of hospitals by night have also now been established.
A note of caution is in order with regard to fluorescent lights: these may give rise to
difficulty for doctors and nurses who have to assess a patient's condition partly by
reference to his skin color.
Emergency arrangements for providing artificial lighting by a stand-by plant, in the
event of a failure of electric power from the main source, are always essential.
The color used internally on the walls, ceiling, and floors of a hospital is an integral part
of the design of the building and should be determined by the architect. The general
lighting of a room is greatly affected by the color scheme, and it is necessary for the
colors to be considered simultaneously with the design of the windows if the best effect
is to be achieved. Color can make all the difference between a depressing or disquieting
atmosphere and a restful or a pleasantly stimulating one. There now exists an
international color notation, and colors can be specified in relation to this.
Visual Impact of the Hospital
Hospital buildings are very large. As the hospital is very often set in a residential area
among buildings of a domestic scale and character, the contrast between its size and the
small, scattered houses around it may be very violent.
Consideration of planning for growth and change tends to soften the visual impact of the
hospital. The parts of it that form its front door or shop windows are the buildings for
outpatient care, reception, and emergency care. These will almost certainly be located
nearest to the entrance to the site, and may very well be planned as comparatively low
buildings, in the interests of future growth and flexibility.
The architectural handling of the design will also affect the visual impact of the hospital.
The architect has the opportunity, in planning the hospital, to give visual expression to
the human units of which the hospital is composed, or to suppress these divisions in the
interests of uniformity. For instance, in designing a ward building, he could allow each
nursing unit individual expression on the façade of the building; or by giving each unit
an identical series of windows, he could carry uniform architectural treatment over the
whole.

Hospital Engineering
More than a third of the cost of hospital building goes into the mechanical engineering
services heating and ventilating, electricity, lifts, and communications. These services
form the circulation and nervous systems without which the hospital cannot function.
Therefore, the contribution of engineers to the design is of capital importance. Their
help will be needed at an early stage, when the approximate demand for water, electric
power, fuel, gas, and sewerage is being estimated. Their advice will be needed on the
choice of site and on the master plan for the hospital. Later, they will have to design
systems of heating and ventilation, lifts and telephonic and other communications.
Engineers will have to concern themselves with the installation of all the mechanical
equipment also with its subsequent maintenance. They should advise the hospital
authority on maintenance problems at a very early stage in the design. They should
advise against the installation of any machinery or equipment for which maintenance
arrangements cannot be guaranteed. Decisions on these matters may affect the master
plan of the hospital, and they should be considered at an early stage.
The engineers must also collaborate with and advise the architect on the space that will
be needed in the building to house the mechanical services. This space must be of
sufficient size to allow not just for present services, but also for any future services that
may be required. The mechanical services must be planned so that easy access can be
obtained to all equipment for repairs and maintenance without disruption of the daily
function of the hospital. Provision must be made for stand-by power in the event of a
general power failure at the main source.
All these considerations point to the fact that a modern hospital can be built and operated
only if the town in which it is located is sufficiently well equipped with electric power,
potable water, sewers, and other technical infrastructures. In addition, competent
personnel must be available to maintain the mechanical and electrical equipment; and
spare parts and other essentials for repair must be obtainable. All these resources must
be fully developed and at the disposal of other institutions as well as the hospital; it
would be unrealistic to think that an isolated and self-supporting hospital could bear the
cost of such technical services only for itself.
Hospital Hygiene
Another important factor is hospital design is the special attention that must be given to
conditions of hygiene. Hospitals exist to treat illness, and often act as reservoirs of
HOSPITAL PLANNING AND PROJECT MANAGEMENT30 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 31
infections. Surveys have found that a substantial proportion of patients acquire
infections during their stay in hospital. The cost of extra patient-days in hospitals as a
result of cross-infection, bears heavily on the patients, sickness insurance and on the
national health budget. It is therefore essential to take reasonable precaution in the
design and organization of hospitals to minimize the risk of infection.
In addition to the risk to patients and staff, hospitals can also prove a danger to the
community if the arrangements for waste disposal are inadequate. The hospital's
sewage may contain dangerous organisms. Outbreaks of typhoid have been traced back
to pollution of the water supply by hospital effluents. The approval of health authorities
should be sought with regard to hospital sewerage and disposal installations.
Introduction of antibiotic drugs substantially reduced the dangers of infection within the
hospital. As a result, many precautions in the design of the buildings and in the methods
of work by the hospital staff were abandoned or neglected. Strains, particularly of
Staphylococcus, have developed resistance to nearly all antibiotics known at the present
time. These resistant organisms tend to establish themselves in hospitals, hospitals,
whose staff often become carriers. It is therefore, more necessary than ever to pay the
strictest attention to all available methods of control of infections.
The first line of defense must be appropriate training of all staff in correct methods of
work. Staff must be trained in aseptic techniques for use in all surgical procedures and
in “barrier” nursing of infectious patients. It may be extremely useful to secure the
permanent advice of a technician with an engineering background in order to control
and periodically survey all the vulnerable points of the hospital, such as sewers, drains,
faucets, lavatories, sinks, and so forth. The design of the buildings can also do a great
deal to facilitate safe working by the staff.
One of the most important matters in planning a hospital is to consider the disposal
routes of all waste and infected material. In every part of the hospital where patients are
treated, there will be infected material to be disposed of. In wards there will be the
patients' bedding and infected utensils, and other waste material of various kinds.
Operating rooms and surgical treatment areas will have infected dressings, dirty
instruments, and soiled linen to dispose of. In principle, it should be possible to take
infected material away from its point of use without contact with any clean supplies
coming into the unit and with minimum handling by hospital personnel. In the nursing
units, soiled linen should preferably be taken immediately from the patient's room to a
disposal room, from which a lift or other special route is available to a reception point
where the linen can be sterilized or otherwise dealt with to make it safe. Dirty materials

should, in general, go into a bin, bag, or other disposal container at its point of origin and
remain in that container until it reaches a point at which it is sterilized or incinerated.
It has been demonstrated that chutes are to be avoided at any cost, because they cannot
be cleaned and disinfected. Moreover, because of the possible difference in
atmospheric pressure between the upper floors and the basement, clouds of dust can
circulate through the chutes. Small lifts or vertical conveyors of the “dumb-waiter”
type should replace chutes.
It should noted that under no circumstances should nurses or other persons concerned
with the care of patients be required to sort or count soiled linen. The disposal route
from the wash-up room serving the operating theatre should be direct to the central
sterilizing department, and should not pass through the operating room or any other
room in the operating suite.
Blankets used on patients' beds are a special problem, as the wool blankets traditionally
used cannot be sterilized or laundered without becoming felted and rapidly destroyed.
Therefore, it is preferable to use blankets of cotton or other material that can be boiled.
Cleaning methods can help or hinder hygiene. Sweeping and dusting as traditionally
performed are dangerous. They spread dust in the air and raise the bacterial count. Wet
cleaning by approved methods and vacuum cleaning by approved types of machine with
special filters must be the methods adopted.
Surgical instruments and bowls have, until fairly recently, been sterilized in boiling-
water sterilizers at various points in the hospital; and dressings have traditionally been
sterilized in drums in autoclaves. These methods have not proved adequate however,
and in recent years this type of sterilization has given place to sterilization in a central
department serving the whole hospital. It is recommended that new hospitals should be
planned, from the start, with facilities for central sterilization. Under this system, all
objects that require sterilization are supplied in sealed packages from the central
department to the point of use. After use, non-disposable items are returned to the
central sterilizing department for re-sterilization. In recent years many new disposable
articles of equipment (e.g. syringes and needles, surgical bowls, and sputum mugs) have
come on the market. It may be found more economical to use these items than to incur
the cost of cleaning and re-sterilizing the conventional equipment after each use.
The planning and operation of the central sterile supply service require expert technical
advice. However, several authoritative reports that give guidance on the subject are
available. It should be noted that the adoption of a central sterile supply service, which
has gained favor on grounds of improved safety may have economic advantages as well.
HOSPITAL PLANNING AND PROJECT MANAGEMENT32 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 33
It affects the planning of the hospital radically, inasmuch as it eliminates the need to
provide sterilization facilities in the nursing units, outpatient and casualty departments,
and many other points within the hospital. In addition, this type of sterilization avoids
the damage to paint that sterilization with boiling water causes.
Many surgeons like to have their own individual sets of instruments. It is more
convenient to arrange for these to be sterilized in a room adjoining the operating room.
All other requirements for operations, including dressings, bowls, syringes, and so
forth, can be supplied to the operating room from the central sterilizing department.
In planning operating rooms and treatment areas generally, it is of vital importance to
separate clean and dirty areas and to ensure that clean material goes directly to its point
of use without coming into contact with any used material or with personnel concerned
with the handling of used material.
Proper techniques by staff and effective sterilization of instruments, bowls, and
dressings will combat infection arising from contact. Many infections are air borne, and
air hygiene is a vital part of hospital design. Air-borne organisms through the mouth and
nose may infect patients and staff. Open wounds are particularly subject to infection
from air-borne organisms. Hence, air hygiene must be considered as affecting the
atmosphere in the hospital as a whole, and particular regard must be paid to it in
operating rooms and treatment areas in which open wounds are exposed to the air.
So far as the general areas of the hospital are concerned, it is important to ensure a good
general rate of ventilation, and standards have been established for this purpose. It
should be noted, in addition, that isolation rooms should be provided with special
ventilation arrangements to ensure that contaminated air from them does not reach other
parts of the hospital. The ventilation of operating rooms is a highly technical matter on
which important research has recently been conducted; it is now possible to specify with
considerable exactitude the requirements for the special ventilating system needed in
operating rooms. Such systems need very careful design by engineers, and should be
subjected to bacteriological control.
When hospital sewage is not passed into the public sewage disposal system, it requires
treatment by an effective disposal plant kept under continuous bacteriological control.
All hospital drains, including those from washbasins and baths, must be fully enclosed.
A central incinerator should be provided in which all infected material is destroyed.
Opportunities should be taken whenever possible to use disposable materials, which can
be destroyed.

The Architect's Brief
The next stage in an actual project would be the preparation of the architect's brief. At
this point it is necessary to go into the needs of every service and department individually
and in great detail, always bearing in mind the general principles governing the plan as a
whole.
It is necessary to consider, first, the function and organization of each section, whether it
is the surgical service or the catering department. It is essential to decide on controlling
principles and to reach decisions on methods of working before attempting to draw up
schedules of rooms. At this stage advice should be sought from people with practical
experience in the running of the various services. It is important, however, to pose
problems in a general form to these advisers and to press them to think afresh to consider
not only how they have organized their work in the past, but also how they would
organize it for better service to patients, or for greater efficiency, if free to think things out
from first principles. Unless care is taken at this point, there is a risk that the architect's
brief will reflect, with minor improvements.
It is of the utmost importance in planning a hospital that a large measure of imaginative
foresight should be brought to bear in an endeavor to identify the probable growing
points and to plan the greatest degree of adaptability in those services that seem most
likely to expand.
HOSPITAL PLANNING AND PROJECT MANAGEMENT34 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 35
STEPS INVOLVED IN HOSPITAL DESIGN
CHAPTER 5
Planning the Grid
'Grid' is defined by Merriam-Webster's Collegiate Dictionary as: “a network of
uniformly spaced horizontal and perpendicular lines (as for locating points on a
map); also: something resembling such a network.”
A planning grid is an architectural design tool which is “something resembling such
a network.”
Healthcare designers can derive their planning grids in one of the two following
ways:
1. In urban situations, where the hospital takes the form of a vertical building
comprising of a podium containing diagnostic / therapeutic and interventional
services and a tower housing the inpatient facilities, the planning grid is determined
by the layout of the inpatient tower. The module(s) used to determine the shape and
size of this grid is the module(s) used to house the various kinds of inpatient facilities
(rooms + toilets) conceptualized by the designer. In the example given below you
can see how the planning grid modules (in red) of 3.90 M x 8.50 M is determined by
the accommodation desired for a single bed patient room, a double bed patient room
and their toilets.
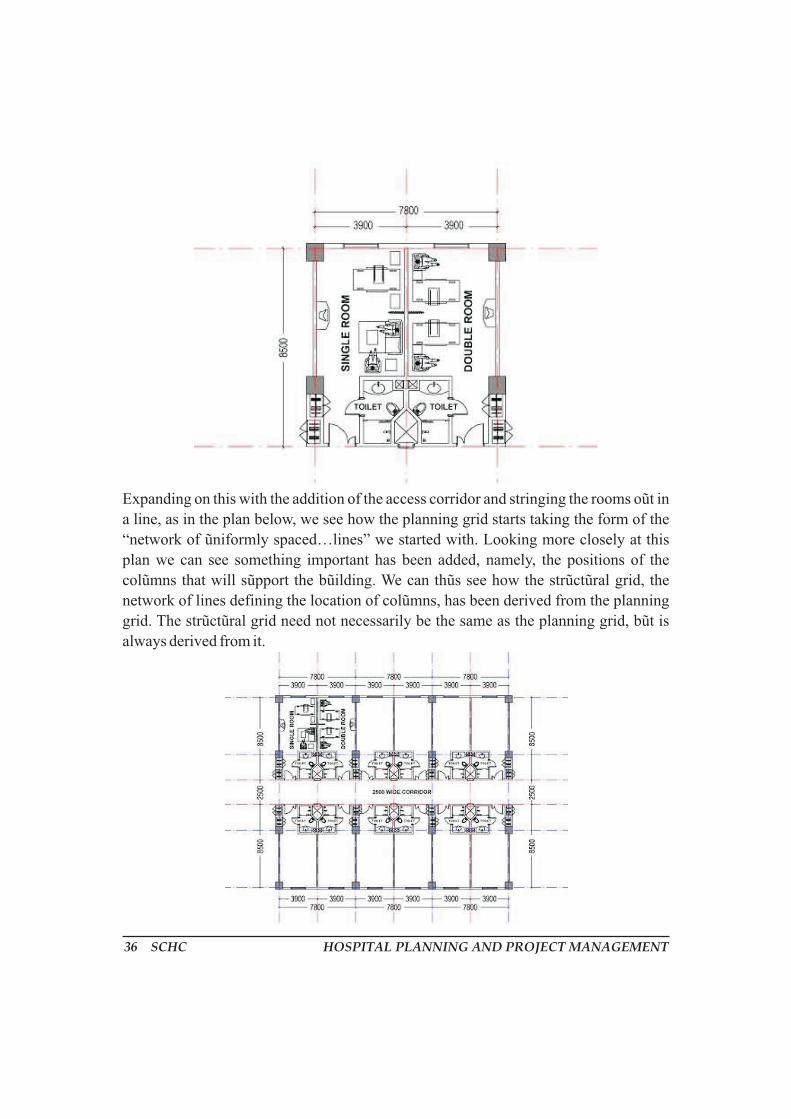
Expanding on this with the addition of the access corridor and stringing the rooms out in
a line, as in the plan below, we see how the planning grid starts taking the form of the
“network of uniformly spaced…lines” we started with. Looking more closely at this
plan we can see something important has been added, namely, the positions of the
columns that will support the building. We can thus see how the structural grid, the
network of lines defining the location of columns, has been derived from the planning
grid. The structural grid need not necessarily be the same as the planning grid, but is
always derived from it.
HOSPITAL PLANNING AND PROJECT MANAGEMENT36 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 37
The positions of the structural columns determined by this planning grid, twisted or
otherwise, will continue downwards through the rest of the hospital, through the lower
floors (the podium mentioned above) till their respective foundations, where they will
transfer their load to the ground below. Hence the lower floors (the podium), which will
contain the Operation Theater Suite, the Radiology and Imaging Sciences Department,
the Main Kitchen and the Mechanical Areas in the basement, to name just a few, will all
need to be designed within the constraints of these column positions. Extrapolating from
here, we can see how the façade of the hospital will need to be designed in harmony with
the windows of the inpatient rooms above, which will be designed with the use of the
planning grid. Even if the podium extends beyond the footprint of the tower above, it is
almost certain that the positions of the additional columns required would be derived
from the structural grid used for the tower, which has been derived from the planning
grid determined by inpatient facility design.
In vertically organized healthcare facilities, we design from the top
down.
2. In semi-urban or rural situations, where the land available is very likely to be larger
with respect to the built-up area desired, determining the planning grid is another
ballgame, one with much greater flexibility in the rules.
In this situation, the planning grid will be determined by what designers call as their
'concept' for the hospital. This 'concept' is also an ordering tool, and will have been used
to determine the form of the hospital in even the previous example of the urban site, but
with less freedom. When there is a lot of land available, it gives the architect more
elbowroom, and his hand is likely to move with more (hopefully graceful) abandon. This
freedom enables many different types of building layout and form.
The thought process behind design can be described as a process of analysis and
synthesis or divergent and convergent thinking. That is, a 'parting' followed by a
'meeting' of thought within their minds. At the point of separation, the designer throws
up a whole lot of different ways in which he could define an ordering principle that he
would use to design the hospital. Suffice it to say for now that based on his / her chosen
criteria the architect will (converge) select one or a combination of concepts to provide
the ordering principle. The focus of our discussion here, the 'planning grid', in this situation gets relegated to an
almost incidental design tool, subject to great local variation if the structure is single
storied, and might vary substantially even if the hospital is partially high rise and

partially low rise, as the two forms of building could have planning grids independent of
each other. Façade design might also vary greatly, there being less discipline to be
followed.
Different parts of the hospital may have different planning grids
derived from the functional planning requirements of the hospital
departments they house.
Another important design issue in the planning of a hospital is the layout of the major
circulation paths.
Circulation :
Hospitals, like the small cities they are likened to, contain main circulation routes often
described as hospital streets. The way in which the different parts of the hospital are
assembled, as a coherent whole but with the parts differentiated, make for analogies
with urban design; the way in which traffic moves, and the routes that are taken by
mechanical and electrical services are fundamental generators of the plan.
In a vertically stacked hospital, which could also be called a functionally stratified
hospital, almost always the inpatient areas are placed on the upper floors, to allow for a
more pleasant, naturally lit environment. As we read in an earlier lecture (entitled “The
Planning Grid”), the planning grid is determined by the layout of these inpatient floors.
Another important planning feature, the vertical circulation core, is also to some extent
located within the building by the layout of the inpatient floors. We somewhat
simplistically claimed in that earlier lecture that in vertically organized hospitals we
design “from the top down.” What we actually do is during the layout of the inpatient
floors, we provisionally decide on a position for the vertical circulation core and other
staircases that may be required, many times by the local building codes. This location,
however, is to be checked for it's design impact on the lower floors containing the
diagnostic / therapeutic / interventional departments. This 'checking' process is
described by the diagram of the design process presented in the self-same earlier lecture.
The pattern of circulation conceptualized for the hospital under design will be
considerably impacted by the location(s) of the vertical circulation core(s).
The vertical circulation core is the center, the focus of all the major circulation paths of
the hospital. An attempt can be made through design to minimize vertical transportation
HOSPITAL PLANNING AND PROJECT MANAGEMENT38 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 39
by siting (for example) all surgical beds, operating theatres and the intensive care unit on
the same floor. This design approach may be used as a justification to reduce the number
of elevators, or the width of the staircases, but in no way does this mean that the core can
be located more casually by the designer.
Avoidance of dependence on lifts is particularly important in places where maintenance
and availability of spare parts is unreliable; long waits for lifts are a major cause of
inefficiency and frustration to hospital users more of a problem the taller the building is.
It is important that patients, visitors and staff be able to orient themselves while moving
through the hospital by providing windows in corridors to enable them to look out and to
allow natural light in, important in alleviating the tedium of long corridors. If the site
enables them, courtyards are also an excellent means to this end.
As such there is no easily available prescription for the way the circulation pattern for a
healthcare facility should be. The qualities it should possess, however, I will try to
enumerate:
1. It should have conceptual clarity. By this I mean it should be designed with purpose,
and should not be leftover space or squeezed into the gaps between other areas.
Geometry can be a recourse, but it should work with other planning imperatives,
and junctions should be uniquely treated to avoid confusion over which corner of
the hexagon (for example) you have reached.
2. It should not be boring. Try to make walking from one place to another interesting,
modulate those corridors, color them differently, hang artwork along the way.
Niches, outside views, courtyards, all these will help.
3. It should enable wayfinding. In combination with well-designed signage and
maybe super-graphics, people should be able to find their way to their destination
with ease. Color-coding for floors or departments is sometimes used.
4. They should be wide enough to handle anticipated traffic. Stretcher traffic needs 8'-
0” width of corridor for easy movement (turning). 7'-0” will work, but use 8'-0” if
you can. Corridors between Operation Theaters make sense even with 10'-0” width.
There may be a lot of stuff parked along the sides, despite instructions to OT staff to
the contrary.
5. They should be indirectly lit. Patients on stretchers get to look at the ceilings. The

sign put up by the traffic police at the end of Marine Drive in Mumbai says, “Drive
carefully. Hospital ceilings are boring.” While not advocating rash driving, we
would advocate making the ceilings interesting.
Some of the hospitals currently existing in India have been provided with ramps in
addition to the usual elevators and stairs. Power cuts are realities that have to be
considered. But consider putting some (two) of the elevators on a generator, if this helps
in avoiding the ramp, which is wasteful of space and difficult to use, as the gradient is
often excessive. (With an acceptable gradient, the length becomes excessive,
considering that the lower floors of hospitals are considerably higher than those of the
usual non-hospital building.)
When planning for the area occupied by this circulation space (corridors) in the
architectural space plan, it can be provided for as a percentage of the department area
(usable, built-up area). This percentage will vary depending on the department and may
also vary if the architect has any special feature in mind for that department which is not
explicitly provided for in the room-by-room area statement (such as semi-covered,
landscaped waiting). The percentage can vary from 35% for an Operation Theater Suite
(with 8'-0” corridors) to 20 25% for the Administration Department.
On the Inpatient floors or even in the Outpatient Department, these corridors can be
modulated by recessing pairs of doors that occur at regular intervals, and using an accent
color in the niche so created. This helps relieve the boredom of walking through long,
uninteresting corridors.
Very frequently the major circulation paths through the hospital are laid out even before
the tentative space allocation for the hospital departments is done. Thus, the importance
of conceptualizing these paths in a way that they contribute to the concept and functional
layout of the hospital is not to be underestimated, the exercise should not be done
casually.
Frequently the manner in which the healthcare architect conceptualizes the working
(and therefore layout) of certain hospital departments, notably the Operation Theater
Suite and the Radiology & Imaging Sciences Department (as described in a later lecture
titled “The Architecture of Imaging”) will determine the circulation pattern through that
department, and hence affect the layout of circulation paths in contiguous areas of the
hospital.
HOSPITAL PLANNING AND PROJECT MANAGEMENT40 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 41
Defining major circulation paths through the proposed and future buildings is a design
decision that will considerably impact the form, layout and thus the eventual
functioning of the healthcare facility being designed.
Special Considerations for Designing for the Disabled
Identifying and understanding the conditions which constitute barriers to those with a
disability (this category includes, besides the wheelchair bound, those who for any
reason have difficulty in walking, and also those with a sensory that is, visual or hearing
impairment) is a fundamental requirement for the effective provision of
accommodation and facilities to be used by disabled people.
If the needs of people who have temporary or permanent disabilities are taken into
consideration, the resulting design can make the design easier and safer to use for those
with children, those using wheeled equipment and those carrying other items. The
principle of applying critical criteria should be used for example, where space is a
consideration, wheelchairs or other larger wheeled items need to be considered; for
vertical fixtures or fittings, the shorter person and wheelchair user must be considered;
and for wayfinding those with visual and hearing impairments must be considered. The
resulting design will help not only people who are ill or disabled but also those who are
suffering from shock or stress, as many users of health buildings are. Building design
that gives consideration to all users will also be easier and safer during an emergency
evacuation.
The best design philosophy is to consider the journey through the healthcare facility
from start to finish, analyzing all the related components of the task (negotiating
entrances, corridors, lifts, reception areas, toilets, etc) to ensure that the features,
equipment and fittings encountered in completing the journey are suitably designed so
that the overall task can be completed easily and conveniently, bearing in mind the
different requirements of staff, patients and visitors with varying degrees of functional
mobility. In this way building users will be more independent (less reliant upon staff)
and consequently less stressed, anxious and frustrated.
People with disabilities can be defined as those who, as a consequence of an
impairment, may be restricted or inconvenienced in their access to, and use of, buildings
because of the physical barriers such as doors that are too narrow, flights of steps, or
unsuitable facilities (for example inadequate lighting, or lack of handrails on staircases
or grab-rails in toilets.) Some people will be temporarily disabled as a result of their
need for hospital treatment.
The following categories of building user are generally recognized :
1. Fully-ambulant : persons who are fully physically capable of carrying out all
activities necessary to their role or function.
2. Semi-ambulant : persons who walk with difficulty or are otherwise insecure, as a
result of a temporary or permanent impairment of the lower limbs. They may walk
with or without a walking stick (sticks, crutches, walking-frames, etc) and/or require
the assistance of another ambulant person. Some people in this category will, in
addition, have reduced strength and dexterity in the upper body and/or a sensory
impairment. Semi-ambulant people find it difficult to cover long distances (even 50
M may be too far). Specific design requirements include: short distances; provision
of handrails and suitable spaces for taking a rest; and even non-slippery surfaces
without any changes in level;
3. Non-ambulant : persons who temporarily or permanently require to use a
wheelchair for mobility. They may propel themselves, or be pushed and maneuvered
by an assistant who may or may not be needed to assist with other tasks. Some people
will be using a wheelchair for the first time due to being in hospital and will be
unfamiliar with maneuvering it. Some people who use wheelchairs will, in addition,
have reduced strength and dexterity in the upper body and/or may also have sensory
impairment. Some will be able to stand on their feet whilst transferring to and from a
wheelchair or to and from other facilities (such as a toilet, chair, or bed); others will
require assistance to do so (in some cases the use of a hoist). Specific design
requirements include the provision of sufficient space for passing and turning; even
surfaces without changes in level; and ensuring that any counters, signs, handles, etc
are within the user's range of vision and grasp.
4. Manually-impaired : persons who have a temporary or permanent lack of strength
and/or dexterity in the shoulders, arms and/or hands. They may also be semi-
ambulant and/or have a sensory impairment. Specific design requirements include
doors which are not too heavy, suitably designed handrails and controls, etc.
5. Visually-impaired : persons who are totally blind or partially sighted. Blind people
find their way by noticing changes in the textures of floor or wall surfaces and
ambient sounds and smells; some also need the help of a cane for orientation and
detecting obstacles. Partially-sighted people need plenty of light and the colors of
any fixtures or fittings they are trying to locate (or are on their guard against) must
stand out plainly in contrast to the background. It must be remembered that vision
HOSPITAL PLANNING AND PROJECT MANAGEMENT42 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 43
deteriorates considerably with age. 40-year-olds need twice as much light and 60-
year-olds three times as much light to see the same object as clearly as a 20-year old.
The more strongly an object contrasts with its surroundings, the easier it is to see.
However, colors do not have to be garish; subtle changes in color can be aesthetically
pleasing, and can fit in with the general décor as well as providing contrast. Different
colors in the same tone can appear very similar to people who are color-blind for
example, a strong red and green together can look much the same and so,
contrasting tones, or a combination of tone and color, are very helpful for people
with poor sight. Any type of cluttered design should be avoided, for this makes it
more difficult for a visually-impaired person to “read” the shape of a space, and
consequently impedes their ability to navigate. Good design therefore should not
only contribute towards the legibility of a building, but also facilitate easy
navigation through it. Specific design requirements include: a simple, well-planned
layout even surfaces with tactile indications of direction; no obstructions in walking
areas; well-lit areas; signs placed at a convenient height, with space to stand in front
to read them.
6. Hearing-impaired: persons who are deaf and hard of hearing have the additional
problem that their disability cannot be seen and is therefore not noticed by other
people. For effective lip-reading, building areas must be well lit in order that the face
of the person speaking is illuminated. Specific design requirements include: a
simple, well-planned layout with well-lit areas; surfaces which dampen ambient
noise, signs placed at a convenient height, with space to stand in front; provision of
induction loops at reception areas and in auditoria.
A check-list giving a suggested sequence of activities to be followed in the planning and
design of access and facilities for disabled people is given below:
Healthcare Premises: Checklist of Access and Facilities for Disabled People
Parking :
1. Are there parking spaces adjacent to the buildings to minimize the distances to be
traveled?

2. Is the parking spaces wide enough to allow a car door to open fully to allow
unobstructed transfer into a wheelchair, either unassisted or assisted?
3. Is the location of the disabled parking spaces such that the approach route to the
building / facility is not obstructed by other parked cars and away from moving
traffic?
4. Are kerbs and other changes of level ramped?
5. Is the parking space and access route under cover?
6. Are there adequate signs to identify the reserved parking spaces and the best
routes into the premises?
Approach to Building :
7. Is the approach route smooth, slip resistant (whether wet or dry), free from incidental obstructions or hazards?
8. Are handrails provided on all slopes and resting places provided at intervals
where a ramp or approach is long?
9. Are all public entrances to the building / facility accessible?
10. Are access doors wide enough to facilitate wheelchair movement?
11. Are thresholds eliminated or kept to a minimum?
12. Do door characteristics and dimensions of related spaces allow it to be opened
(and closed) easily by independent wheelchair users, moving in either direction?
13. What doors can be eliminated?
Internal Circulation :
14. Are lobby sized adequate and safe for both independent and assisted wheelchair
use?
15. Are corridor and approach routes satisfactory? Do they allow passing and turning
and take adequate account of corridor traffic conditions?
HOSPITAL PLANNING AND PROJECT MANAGEMENT44 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 45
16. Have all obstructions and projections from walls (or ceiling) or similar hazards at
floor level such as changes of level been avoided? If unavoidable are they clearly
discernible?
017. Are internal door widths adequate to allow turning through 90 from the corridor
or lobby? Should either of both be increased?
18. Have safety handrails been provided on corridors, ramps, and steps or at other
points where they are required by persons with impaired mobility? Have they
been produced where they can be used as location aids by visually impaired
people?
19. Are any large areas of glass close to circulation areas marked or framed so as to be
clearly discernible to partially sighted people?
20. Are seats available at intervals to permit an ambulant disabled and elderly person
to take a short rest when faced with long corridors to negotiate?
Vertical Circulation :
21. Are staircases safe and optimally comfortable for elderly and disabled people?
Are handrail and landing characteristics satisfactory?
22. Are lifts available, conveniently placed, accessible and clearly signed?
23. Are lift controls accessible to the independent wheelchair user? Are the visual and
audible signals, alarms and floor designations satisfactory? Are digits embossed
and satisfactory for blind or partially sighted persons? Is there a
Toilets :
24. Are there correctly designed unisex toilets, that are where a husband and wife may
enter the cubicle together, available in the public areas of the premises?
25. Are there suitable cubicles for wheelchair users in other male and female toilets in
the building?
26. Do cubicles for wheelchair users provide adequate maneuvering space within, or
are turning space provided outside? Is the level of privacy afforded satisfactory?
27. Are there cubicles available with appropriate grab rails for the use of ambulant

disabled people?28. Are the WC and washbasin arrangements accessible to independent wheelchair
users? Are the grab rails, mirrors, towels, door closing bars and other aids placed
satisfactorily?
Outpatient And Treatment Areas :
29. Can ambulance discharge patients under cover within close proximity to the
entrance? Are waiting areas protected from draughts as patients move in and out
through the entrance doors? Can patients using wheelchairs (their own or hospital
chairs) whilst waiting for treatment, sit with other patients without obstructing the
corridors or circulation area?
30. Can patients in wheelchairs use the reception desk conveniently and privately?
31. Are all consulting and treatment areas fully accessible?
32. Are there changing cubicles suitable of wheelchair users, with room for
assistance to be given if required?
33. Are refreshment areas accessible to disabled people?
34. Are clear, well lit, signs posted to ensure easy circulation within the building?
35. Are telephones and other public mechanisms accessible to wheelchairs users? Are
knobs, dials, switches, handles and other controls operable and within convenient
reach?
Ward Facilities :
36. Do sanitary facilities offer maximum independence and privacy to disabled
patients, both those who will be using wheelchairs and those who have walking
difficulties?
37. Is the day room accessible, with a variety of seating heights to help ambulant
disabled people? Are all notices easy to see and understand?
38. Are window controls, radio and television and call bells easily reached by disabled
patients?
HOSPITAL PLANNING AND PROJECT MANAGEMENT46 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 47
39. Can disabled visitors conduct private conversations with their friends in bed or in
the ward?
Other features :
40. Could disabled employees work in the building with particular reference to
offices, laboratories, canteen, rest rooms and toilet facilities?
41. Are emergency evacuation routes and emergency exits satisfactory?
42. Are fire alarms readily accessible to the semi-ambulant and wheelchair disabled?
Are emergency call facilities installed to summon assistance to remove locations?
43. Are audiovisual alarm signals provided?
Hospitals should take the lead in providing disabled-friendly access to themselves as
well as wayfinding. Use the above checklist to make any facility you are planning easy
to enter and use by the disabled.
Another important design issue in hospital planning is the need to design for flexibility.
Designing for Flexibility
'Flexible' is defined by Merriam-Webster's Collegiate Dictionary as: “Characterized by
a ready capacity to adapt to new, different or changing requirements.”
Flexibility, as an architectural principle applied to the design of a hospital, would be the
inbuilt capacity of that hospital to adapt itself to “new, different or changing
requirements.”
John Weeks, the first architect in Britain to fully grasp the need for this flexibility in the
design of hospitals, made the then revolutionary point that ' user studies of function are
by themselves not a sound basis for hospital design. Functions change so rapidly that
designers should no longer aim for an optimum fit between building and function. The
real requirement is to design a building that will inhibit change of function least, and not
one that will fit specific function best.'
At Northwick park hospital, London, he designed a 'hospital street' along which were
placed blocks of buildings that could expand at right angles. Both the blocks and the

street were open ended. The plans of the hospital below illustrate this.
Shown above are three plans showing the development method at Northwick park
hospital and clinical research center. A linear hospital street forms the backbone to which
ribs can be attached with relative freedom. It is the earliest example of deliberate
indeterminacy in post-war hospital planning. The hospital and research departments can
be constructed and later altered or expanded, independently of one another.
Construction was carried out in phases over a period of nine years and during this time
extensions and alterations to the original brief were made without disturbing the basic
design.
This design concept proved very influential. However, the hospital sprawled over a great
deal of land. Then what could be done on urban sites where land was at a premium?
An answer to this was the concept of 'universal space': that is, a series of structurally
uninterrupted floors, to which any services such as electricity, gas, water, could be
brought from above, and from which all wastes could be taken from below.
The Greenwich Hospital, UK was the first hospital to have 'interstitial' spaces or services
sub-floors between each hospital floor. This solution is most strongly justified in
hospitals where the climate makes air-conditioning or mechanical ventilation
necessary throughout. The dedicated space for air-conditioning ducts, pipes and wiring
means a greater overall building volume, but the ability to service them without entering
HOSPITAL PLANNING AND PROJECT MANAGEMENT48 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 49
the hospital areas they are sandwiched between is an advantage; full benefits are only
reaped if three-dimensional zoning is maintained, by “reserved rights of ways” for the
various services. Shown below is a section showing 'interstitial' spaces or services sub-
floors.
This approach makes an important point. Making a building that is adaptable to
changing requirements is largely an issue of providing the necessary building services
required by the changing requirements at the desired point in the existing building. In
India, with our RCC column and beam method of construction, this need impacts the
structural system design for the building in that punctures in the slabs may be necessary
during this change of function and thus the structural system chosen initially has to cater
to that requirement.
In order to provide for planned expansion it is necessary to develop a master plan that
provides for both short - and long - term expansion and change within the hospital and
throughout the campus. The master plan should establish major paths of circulation
projected through foreseeable phases of new and renovated buildings. The design
concept should contain within it an overall ordering principle for the entire campus,
integrating into the design a building systems framework (See: Illustration below).

Source: Hospitals and Healthcare Facilities by Redstone
With hospital accreditation by health insurance companies in India being just around the
corner, old hospitals that are too tightly tailored to the needs of initial users will become
obsolete due to the changing standards demanded by these companies, who are likely to
emerge as the new drivers of the healthcare industry.
Changing market demands, new technology replacing the old at an ever-increasing rate
of change, advances in the science of medicine and changing patterns of disease all
HOSPITAL PLANNING AND PROJECT MANAGEMENT50 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 51
underline the need to design healthcare buildings for flexibility. The functional,
technical and hence financial success of hospitals thus depends on the ease with which
they can grow and change, and this dependence increases with time. The aesthetic
implications in designing buildings that will expand and change over time also become
an issue. An urban design approach is necessary; an initial building whose form is
symmetrical will tend to look skewed when expansion takes place. The higher the
buildings are, the greater the aesthetic, technical and functional difficulties in making a
workable addition.
The fact that many hospitals are built in a number of phases further complicates the
problem. There may be a series of replacements of older buildings on an existing site or
limits to the amount of investment possible at any one time. A comprehensive and firmly
established Development Control Plan is essential for a hospital built in phases to
specify the strategic direction of following phases, but not their detailed design.
The issue is complex; it involves a multiplicity of design factors that may be making
contradictory demands on the designer. We suggest you consider the various options
keeping in mind the needs of future generations to whom you will bequeath your design
solution in its built form.
stWhat does this requirement for flexibility augur for the hospitals to be built in the 21
century?
1. Buildings will be designed to facilitate the docking of mobile and plug-in modules.
It is likely that specialized major diagnostic and diagnostic-surgical equipment will
be manufactured in self-contained pre-constructed modules intended for docking at
strategic points “ports” in the building. Such mountable and demountable
components could be readily downloaded to other facilities for example, an ex-
urban satellite of the main hospital.
2. HVAC systems will be modularized and zoned, with vertical circulation,
mechanical shafts and transport systems moved from the core of the building to the
perimeter in order to create free fields within the core floor plate that are easily
adaptable to different layouts.
3. Interstitial concepts, which seemed promising in the early 1980's, but were mostly
found to be expensive in terms of capital investment, may well return as flexibility
becomes such a vital consideration that these initial capital costs will become
justifiable.
4. Other structural strategies that maximize flexibility and adaptability will be
used. Floor systems will have to allow for multiple penetrations for plumbing
and electrical lines, column spacing will need to be optimized so that
departmental redesign is not cramped by existing structural constraints.
5. Other strategies for maximizing flexibility will include the deliberate specification
of “swing” space to allow temporary relocation of departments during renovation,
and to allow greater flexibility in adapting to changes in patient population. Low-
tech departments can be zoned in 'soft” spaces adjacent to “high-tech” spaces.
6. Finally, some facilities may require the development of “universal floor plans”,
which can be adapted and readapted to accommodate virtually any need.
The concept of flexibility will extend beyond what the architect designs to the architect
him- or herself. The architect will provide a range of services beyond the traditional
architecture and engineering (A & E) tasks, including strategic business planning,
evaluation of lease-versus-build options, financial planning, mechanical and electrical
systems evaluation, space planning inventories, furniture inventories, long-range
planning and master planning. Once the building has been completed the architect will
remain in contact with the owners for the life of the facility, providing a full range of
services on a contractual basis. These services will include ongoing evaluation and
planning for expansion, contraction and adaptation to changing needs.
Aesthetic in hospital design
It is a mistake to think of the hospital architect only as a technician whose role is
primarily organizing detail. He has an aesthetic as well as an organizational and
conceptual
contribution to make. He is often the major - if not the only - participant in the
development of a hospital in a position to see it as a whole. This is seen in the attention
paid by him to the aesthetics of the exteriors and the interiors of the building. The
typical, somewhat forbidding, hospital facade of the past has given way to more
interesting configurations of building shapes which are based on the functional aspect of
interior communication and traffic requirements. There is also an increasing awareness
by hospital administrators and designers of the value of good graphic design and art as
part of the hospital environment. In good hospital architecture, the aesthetic and
functional unite to contribute to the well-being of both patient and staff. It has a
HOSPITAL PLANNING AND PROJECT MANAGEMENT52 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 53
beneficial effect on both. A pleasant environment increases efficiency and quality of
work. It helps the tolerance level in meeting the pressures of very demanding duties.
At the same time it should be kept in mind that primarily the hospital is a place for the
care of the sick where conditions may at times seem unattractive to the active and
healthy. To be aesthetically convincing the hospital must be itself and not an imitation of
something else. The patient needs most of all to feel that he is in the presence of
scientific competence as well as sympathetic attitudes.
Psychology-implications for health care design
A critical look at modern hospitals shows that they are designed for ease of maintenance
rather than human comfort. They seem to be resistant to human imprint - a definition of
an institutional environment. The architecture, instead of embracing and welcoming
inhabitants, seems to alienate and intimidate them. They resemble a Kafkaesque
labyrinth of corridors - endless in their dimly lit pallor and multiple layers of chipped
paint. If we stop thinking of patients as inmates and view them as guests, hospitals could
function more on the order of hotels and restaurants. If the individual can relate the
medical environment to something else that he or she has experienced with a positive
association, much has been achieved towards reducing anxiety.
THE DESIGN PROCESS
CHAPTER 6
Taste, unlike function, is indefinable.
We have Florence Nightingale saying:
“The very first consideration to be sought in planning a building is that it shall be fit for
its purpose. And the very first architectural law is that fitness is the foundation of beauty.
The hospital architect may feel reassured that, only when he has planned a building that
will afford the best chance of speedy recovery to sick and maimed people, will his
architecture and the economy he seeks be realized.”
Of course her heart is the right place. She was responsible for naturally well-lit and
ventilated wards, the well-known “Nightingale” ward. Do you see the convergence with
I.M. Pei and his proposal for the UCLA Medical Center, so many years later?
Then we have that connoisseur of architecture, HRH the Prince of Wales saying:
“Mammoth hospitals, built like dreary office blocks on a devastatingly functional basis,
depress the spirits, however good the care is.”
We agree. Taste may be indefinable, but let us hear Sir Norman Foster (RIBA Gold
Medal Winner) on the subject:
“Architecture is also about the spiritual needs of people as well as their material needs; it
has as much to do with optimism, joy and reassurance; of order in a disordered world; of
privacy in the midst of many; of space in a crowded site; of light on a dull day; it is about
quality.”
Quality need not be defined to be apparent. A building that is functional and pleasing to
those that use it, a building that sits easily in its surroundings, a building that is a pleasure
to behold, such a building is not a building at all! It is architecture.
The production of architecture starts with a concept. Here suffice it to be said that
concepts are usually presented in the form of drawings, with a written or verbal
commentary.
HOSPITAL PLANNING AND PROJECT MANAGEMENT54 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 55
Some explanation of terminology common to drawings developed during architectural
design work may be helpful at this point.
1. PLAN : The plan is the top view.
2. ELEVATION : The elevation is the side view.
3. SECTION : The section is similar to an elevation, but it shows what
remains after an imaginary slice (section) has been cut
through the object.
4. PERSPECTIVE : Perspective is a three-dimensional drawing of an object.
5. RENDERING : A rendering is a finished architectural perspective
drawing indicating materials and the effects of light,
shade and shadow to help explain form or shape. Plans,
elevations and sections are also referred to as “rendered”
when materials, light, shade and shadow are shown.6. PLAN SECTION : The term “plan” is used interchangeably to refer to a top
view and to what is actually a plan section. A plan section
is a horizontal (rather than vertical) section of a building.
It shows the top view of what remains after everything
above the slice has been removed.
After conceptual layouts have been approved (“signed off”) by the client, the architect
incorporates more detailed planning criteria into the drawings, the end product of which
is a schematic drawing. It is not done in isolation. All the various members of the design
team participate in giving inputs, comments, critical assessments and the schematic
drawings are the product of what may be a time-consuming and difficult process, it may
involve heated discussions, hopefully followed by “working” compromises between all
kinds of design factors and cost constraints.
These schematic drawings would include exterior elevations (quite likely rendered),
and fairly detailed sections, showing vertical stacking of functions. It may include
perspective views (nowadays increasing prepared and rendered on a personal computer)
and may also include a “walk-through”, a series of computer generated images giving
the illusion of a video clip starting maybe with the approach to the building and going all
the through the main entrance into the lobby and possibly beyond, depending on the time
and money spent making it.

Usually such rendered perspectives, scale models of the building and the walkthrough
are commissioned and paid for by the client at actual cost, falling outside the normal
scope of services of the architects.
After the schematic drawings have been approved, the architectural design development
stage begins, which is more technical and detailed.
Site : By this time the survey, soil investigation and utility information should be done.
If not, it needs to be done ASAP. This information will support development of
initial studies in foundation and structural framing, sanitary and storm sewer
systems, site development and grading, and electric power and energy services.
Access of traffic to the building entrance, separation of emergency and service
traffic elements and provision for parking are further studied at this time. The
site survey and soil investigation are usually paid for by the client along with
whatever legal services may be necessary in securing required easements,
change in land use, etc.
Building: Architectural development includes further study and decisions regarding
materials, windows, exterior finishes, architectural treatment and detail;
refinement of space layout within the facility, selection of finishes and materials
in keeping with maintenance and durability requirements; and comparative cost
studies of methods and materials for partition systems and exterior walls, ceiling
and windows.
Engineering: Further development is also required on concepts of air handling, air
conditioning, electrical distribution-lighting-communication-data systems and
medical gas, plumbing and piping systems. During design development these
systems are worked out sufficiently to allow cost studies and basic interfacing
decisions to be made. Drawings are normally single-line indications of piping or
ductwork. Total services requirements for electrical power, natural gas or fuel
oil, sanitary and storm sewers, water, and solid waste disposal are now
established.
Equipment: Hospital planning requires careful attention to the fixed and movable
equipment that will be needed to implement the operational program. Early in
design development, equipment and room detail interviews are held with
medical and staff personnel. In these sessions, equipment requirements are
documented. The information is used in coordinating room sizes, utility
services, lighting and workflow. Documentation usually takes the form of room-
HOSPITAL PLANNING AND PROJECT MANAGEMENT56 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 57
by-room equipment lists, or room data sheets, and are submitted for
administrative, medical staff and departmental review after compilation.
Systems: Complex systems of various types are often incorporated, in concept form, in
schematic design. Functionally, these include communications, data
transmission, storage and retrieval, materials handling, security, food
preparation and others. Each system that is to be incorporated must be studied in
detail and interfaced with equipment common to other building systems; space
and structural requirements are often extensive. Justification of systems is
critical, since initial and maintenance costs are usually high.
Design development drawings normally show considerably greater detail than
do schematic drawings. Major equipment and furniture are shown in the plans in
order to facilitate engineering coordination of utilities and lighting. Plans show
wall thickness, door and window function and more detail regarding vertical
circulation and materials. Sections and elevations at a larger scale depict
relationships between materials. Outline specifications, to supplement the
drawings, are compiled for each material, system and element of work. A room-
by-room equipment list, or room data book, is included to record equipment
requirements.
A design development is desirable to provide summary discussion of
operational concepts, materials, special equipment, and environmental systems.
When design development documents are completed, a cost estimate is
prepared and presented with the drawings, outline specifications and equipment
information for hospital review. The estimate provides a current check on
project scope related to budget.
After approval, design development documents provide the basis for the
working drawing or contract document phase of the project. The design
development phase sets the detailed operation of each room and leads to
approval of all systems, fixed equipment, material types and building
construction.
This is the most important part of the administrator's role on the team, as it sets all of the
ideas, programs, needs and designs into the final building plan. All anticipation of
future needs are now fixed, as the following phases only detail and construct what is
now the final design product.

The Production Phase:
The “production phase” of a health care facility is much more than just the construction
of the physical plant; in fact, it begins and ends with the execution of legal activities.
From the production and execution of the owner-contractor agreement, to the final
inspections and acceptance of the completed structure, the hospital administrator and
board will find themselves involved with complex and critical legal documents and
activities. In addition to these clearly legal activities, a new kind of architectural
drawing must now be produced: the working drawings. The working drawings, along
with the written specifications, are in themselves a form of legal document as they
describe in pictures and in words what the contractors have legally agreed to build and
the purchaser has legally agreed to pay for.
Given these considerations, it is as important that the hospital administrator and the
board members understand these documents and activities, as it was that they
understood the earlier design documents and activities.
The contract documents consist of the owner-contractor agreement, general conditions,
specifications, bill of quantities (BOQ) and drawings. At the time of signing the
agreement, a work order is issued, containing all addenda issued before execution of the
agreement, which is also signed by the client and contractor. The owner-contractor
agreement and the work order are considered the basic contract documents because they
are the only ones that require the signature of both the owner (client) and the contractor
and they incorporate all other documents referred to in them. The agreement provides a
statement of the contract sum, identifies the nature of the project, establishes the time of
commencement and completion, and describes the manner wherein the contractor will
be reimbursed for work performed.
The set of documents are as follows:
1. The Owner-Contractor Agreement
This is a legal document on stamp paper that sets forth the terms of agreement between
the owner and the contractor.
2. The General Conditions of Contract
The general conditions set forth the legal and regulatory requirements of the contract.
HOSPITAL PLANNING AND PROJECT MANAGEMENT58 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 59
3. The Specifications
These contain general specifications under various heads, such as RCC, Masonry etc.
4. The Bill Of Quantities (BOQ)
These contain additional specifications for various items with their rates.
5. Drawings
The drawings are graphic representations of the work to be performed and contain
information about design, location and dimensions of the elements of the project. The
working drawings, together with the BOQ and Specifications, are called the
contraction documents.
6. The Work Order
The work order contains all the addenda issued before execution of the agreement.
In smaller projects, if mutually agreed by the client and contractor, no agreement may
be signed, the only document that is signed by both being the work order. In this case, if
a dispute occurs, the recourse is only to arbitration, and not a court of law.
Reading the Working Drawings:
At first glance, working drawings are formidable, especially those of a typical hospital
project. Yet, if it is remembered that these documents tell the contractor exactly how the
building is to be built, they become like a foreign language; the more one learns about
them, the less mysterious they become. Taking part in the development of these
drawings, from schematics to working drawings, for a single hospital project would
provide a complete education, but it would take from two to four years on the average.
Essentially, each consultants drawing is meant to complement the others. The architect
is responsible for coordinating the different consultants drawings, while the general
contractor is charged with coordinating the work of subcontractors. In addition, the
specifications require that all contractors study the work of other contractors as defined
by the working drawings and specifications. The better architectural firms require

composite drawings that lay out the major elements of the plumbing, mechanical and
electrical systems. Such drawings not only force the engineers to coordinate their work
in the field, but dictate the order in which system components are to be installed.
Following completion, these drawings serve as as-built drawings, and are turned over to
the client to become a valuable record of construction. This enables the in-house
engineering personnel to more easily repair and control the systems. Should future
alterations or additions be needed, these as-built records will be extremely useful.
Bidding Requirements and Procedures:
Competitive bidding is the most widely used method of obtaining construction prices.
When using competitive bidding, it is wise to pre-qualify the contractors who will be
involved. That is, the architect designs a form that asks each interested contractor to
submit references and data on experience, financial conditions and ability to be bonded.
An invitation to bid, as described above, outlines the time, place, scope and location of
the final plans and the actual bid. The sets of plans and specifications are distributed to
the general contractor. The bidding contractors should be allowed 10 days to 3 weeks to
come up with their final price, depending on the size of project. When so may people are
looking at a set of plans and specifications there are bound to be questions. The architect
should issue clarifications to each bidder, as well as any item changes. The architect
analyzes the final price submittals, and advises the client as to technical accuracy. The
contract can then be awarded.
Once the bids are received and the contracts signed, the client has very little control over
the selection of subcontractors. The client can however require that a list of
subcontractors be submitted. Whatever prices the general contractor used to formulate
his total, he can now negotiate each item: any savings that result will not be available to
the client. The contractor must, however, meet the quality and quantity as described in
the drawings and specifications.
The general conditions defined the liabilities and role of all general contractors and
subcontractors. The contractor must also understand hospital operations in order to
disrupt hospital routine as little as possible. Construction touches special nerves of the
administrator and hospital staff. The administrator will be blamed for the noise, site
HOSPITAL PLANNING AND PROJECT MANAGEMENT60 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 61
confusion and distractions. These things are part of normal construction, but they place
an unfamiliar burden on the hospital's normal operation. Day-by-day construction
seems like endless delay and problems to the layman; it is a way of life for the architect
and the contractor. I think they have to both understand each other's problems and focus
on building an excellent facility.
One way to save the client some of the headaches mentioned above is to employ a clerk-
of-works. This person represents the client; he is experience in construction and is hired
by the client to check daily progress. Although the architect acts as the client's
representative during construction, he only performs inspection as it is required; he will
not be on site every day. The architect's duty here is to check shop drawings (detail of
each item specified and submitted by the manufacturer for approval), verify the
contractor's invoices to the owner, and see that quality and design are met. The architect
does not tell the contractor how to build the building: he defines the size, shape and
quality of the building.
PLANNING OF INPATIENT WARDS
CHAPTER 7
Patient Housing Systems:
Patient housing systems, typically known as wards are a key element of the hospital building and may occupy thirty-five to fifty percent of the hospital built up area. The current trend of corporate hospitals is making it necessary for promoters to think towards improving the traditional way of laying out these wards. These areas are becoming more comfort oriented from the customer's point of view. The important criteria for planning the patient hosing systems would be as under:
a) Ownership and Bed Mix of the hospital – corporate hospitals may have more single and double rooms than general wards. The bed mix of the hospital will decide the numbers in each category of beds. As per current practice approximately 20-25% beds may be planned in the critical beds and another 20-25% beds in general wards.
b) Age and Gender distribution – hospitals may need to have separate floors or ear marked areas for pediatrics, male, and female categories of patients
c) Specialty based distribution – this classification may be required more in large hospitals imparting medical education wherein one would need to plan for separate departments for surgery, medicine, orthopedics, obstetrics & gynecology, pediatrics, ENT, ophthalmology etc
d) Socioeconomic class based distribution – commonly practiced in all private hospitals in India wherein the patient wards are segregated on basis of the socioeconomic class of the patient
Classification of Wards
In-patient wards are classified by their specialty. In a General Hospital the usual ones are:
· the adult general acute
· the adult surgical
· the children's or pediatric
HOSPITAL PLANNING AND PROJECT MANAGEMENT62 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 63
· the old peoples or geriatric
· the maternity
· the orthopedic
· the psychiatric
Sometimes there are isolation wards for patients carrying an infection or who for some reason have suppressed immunity and need to be nursed in a bacteria free environment. There are also Intensive Care wards for patients needing special nursing and medical care. Adult wards are likely to be differentiated by sex, depending on the way they are planned and the customs of the country.
The efficient and economic running of hospital in-patient services is probably one of the most difficult problems of all continuously operating services. The organization of nursing care constitutes a subsystem that very directly aims at achieving the hospitals overall objectives.
Inpatient nursing units
Number of Beds
Over a hundred years ago Florence Nightingale held that thirty-two was the maximum desirable number of patients in a ward unit. Although there have been revolutionary developments in medicine and surgery since then, and many changes in the way the ward has been planned, the number of patients that can be cared for by the ward sister and her team has remained remarkably similar.
Today the preferred number of patients in the general acute and surgical wards may be some four beds less than Florence nightingales thirty-two but it seems to be universally recognized that one team should not deal with more. The number of beds under one sister is likely to vary from about 28 to 30 in general wards, or about 20 to 24 for children. These numbers may be affected by nursing team arrangements, but in the interests of flexibility and possible future changes and also for structural and servicing reasons (particularly in multi-storey buildings) ward units are usually about the same overall size, varying only in their internal planning. Wards with fewer beds tend to be those needing additional ancillary accommodation particular to their specialty and the sizes even out reasonably.
Location

The location of wards in relation to other departments of the hospital is rarely critical, except that surgical wards and those for intensive care are best in close proximity to the operating theaters. It is an advantage if this connection does not depend on the use of lifts, although this cannot always be achieved.
However, all wards need to be easily accessible from the hospitals main supply and disposal routes and to have convenient communication with the diagnostic and treatment departments, particularly such departments as physiotherapy which are visited by ambulant in-patients. In addition all wards should be capable of being reached by visitors along simple coherent routes from which they are unlikely to stray into other parts of the building from which they should be excluded, or pass sensitive areas where there are high risks of cross-infection. No ward should be used as the principal means of access to another. Even though it may not be entirely on a cul-de-sac, the entrance to every ward should be capable of strict control.
Accommodation
The ward combines clinical and housekeeping facilities with the psychologically important function of providing the patient with a reassuring home in which he can be encouraged and supported towards an early recovery. The housekeeping element used to represent a much larger part of the work of the ward staff than it does today. This is now much reduced by centralization of the supply of food, linen, drugs and sterilized articles, so that the ward no longer carries large local stocks of linen, crockery and medicines.
Apart from bathing, washing, toilet facilities and day spaces for ambulant patients, the ancillaries in the general ward normally consist of:·a treatment room where surgical dressings can be attended to and minor operative
procedures carried out with the minimum risk of cross-infection and without distressing other patients
·a clean utility room principally for the preparation of equipment used in the treatment room
·a dirty utility room for emptying and cleaning bedpans and urine bottles, cleaning other soiled items and disposing of materials such as dressings
·a pantry for the preparation of beverages and for washing and drying crockery·a small equipment store (mostly in critical care units)·one or more nurse stations·an office (optional)·provision for the storage of patients clothes·a staff cloakroom
HOSPITAL PLANNING AND PROJECT MANAGEMENT64 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 65
·a janitor closet
The treatment room is sometimes placed between the clean and dirty utility rooms so that sterilized equipment from the Central Sterile Supply Department (CSSD) can be received and prepared in the clean utility, and after use is passed through another hatch into the dirty utility, where it is washed before return to the CSSD.
Intensive Care Units
Intensive Care Units (ICUs) are specialty nursing units designed, equipped and staffed with specially skilled personnel for treating very critical patients or those requiring specialized care and equipment. Centralizing the acutely ill patients, as is often done, in contiguous units in an intensive care complex consisting of surgical-medical intensive care unit, coronary care unit and specialty units such as renal and burn units, results in multidisciplinary care and economical use of the space and equipment.
There is no unanimity among the medical and nursing experts as to where the ICU should be located. There are two schools of thought. One suggests that the ICUs should be in a centralized place and be contiguous with, or readily accessible to, one another. The argument is that patients admitted to the medical-surgical intensive care unit may have, or suddenly develop, cardiac complications. Having intensive care facilities in a centralized place allows the specially trained professionals and equipment an almost instant access to patients in all clinical services when an emergency develops. Such an arrangement also eliminates the need for duplication of costly equipment and personnel.
The second school of thought favors that the location should be dependent on the type of patients. For example, the surgical ICU should be close to the operating rooms while the medical ICU should be in close proximity to the medical ward to facilitate following the concept of progressive care, i.e. the patient is moved from the intensive care unit to intermediate care or step-down unit, and then to the general patient care area.
Intensive care units should be close to emergency, O.T. Suite, Respiratory Therapy, Laboratory and Radiology. Most admissions to ICUs are either through the emergency department or from the operating rooms following major surgery. They should not be too far away from general nursing units, as patients may need to be transferred in an emergency. They should be close to vertical transportation cores. They should be away from heavy traffic and noise. The electrical influence of equipment like elevator motors and X-ray equipment on the displays of monitors should be kept in mind. Accessibility and direct visual contact between patient and nurse is important. The patient should be close enough to permit observation of respiration, facial color and other revealing symptoms.It is generally recognized that for effective operation, there should be no more than

twelve to sixteen beds per intensive care unit. An intensive care unit of less than six beds is clearly uneconomical. The beds should be located permanently away from the wall, to give staff a 360 degree access to the patient.
An Intensive Coronary Care Unit is used to identify the units restricted to patients who are suffering from cardiac emergency conditions. Patients are transferred from here to an intermediate care section, which ought to have twice the number of intensive area beds. A Pulmonary Intensive Care Unit (PICU) is a major key in a comprehensive pulmonary care program for chronic obstructive lung disease. A laboratory for around-the-clock determination of arterial blood gases immediately adjacent to the PICU is required, since these patients are very unstable. Logistic delays due to laboratory remoteness or unavailable technical assistance is not acceptable. Neurovascular or stroke cases are admitted predominantly from the emergency department. In a Burns Care Unit two phases of the burns illness - the shock period and the healing period - have to be accommodated. Complete reverse isolation can be a significant factor in the prevention of bacterial contamination of individuals incurring major burns injuries. For maternity patients with complications and particularly for those in premature labor a special ante and intra partum unit also referred to as an obstetric or labor or maternity intensive care unit can be provided. In conjunction with this, a Neonatal Intensive Care Unit (NICU) can be provided, which is an intensive care nursery which provides the best chance of saving life and of improving physical and developmental status for survivors of serious perinatal illness.
Special Nursing Units
The Pediatric nursing unit is concerned with the care of children. It calls for an understanding of the unique needs, fears and behavior of children. It is generally accepted that children adjust to hospitalization better when they have the companionship of other children in the same room. The unit is generally noisy, and should be located away from the mainstream of hospital traffic. If possible, it should be located adjacent to a terrace to be used as a play area.
The responsibilities of the Obstetrical nursing unit include prenatal care, observation and comforting of patients in labor, providing assistance in the delivery room, care of the mother after delivery and care of the newborn. Ideally the unit should be located on the same floor as the labor-delivery suites and in close proximity to them. It should also be adjacent to the nursery
The Psychiatric nursing unit - many general hospitals recognize a responsibility for the mentally ill and provide facilities to treat them. The unit should be designed with a non-institutional atmosphere, with sensitive interior design to provide a desirable therapeutic effect.All hospitals knowingly or unknowingly admit patients with communicable diseases. It
HOSPITAL PLANNING AND PROJECT MANAGEMENT66 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 67
is the responsibility of the hospital to protect other patients and hospital staff from these diseases. Barrier nursing and other techniques are not enough. Physical barriers are necessary. Isolation rooms are therefore provided, and are located within the individual nursing units. They may also be grouped as a separate isolation unit. Rooms for specialized procedures such as organ transplants, bone marrow transplants and burn cases call for special design provisions to meet the needs of functional programs.
Newborn nurseries - they are one of the areas of the hospital where patients are most vulnerable to infections. They should be located in the obstetrical nursing unit as close to the mothers as possible. They should also be close to the premature baby or neonatal intensive care unit. The need for a close, natural adaptation of mother and the newborn infant to each other right from birth is ingrained in the Indian culture. It is therefore hardly necessary to have a large nursery for full-term infants as is the practice in the West. The basic physical and emotional needs of both the infant and the mother are best satisfied by 'rooming-in', that is, placing them together soon after birth.

PLANNING OF CLINICAL DEPARTMENTS
CHAPTER 8
General Planning Considerations
Early in the planning process, each department must be sized to accommodate the
functions necessary to accomplish its objectives. Early functional planning must
establish general concepts of operation, space needs, and required room relationships.
As a result, a functional space program can be developed by evaluating activities,
projecting work loads and assigning individual room requirements. In establishing
various work loads, a variety of utilization factors must be considered in light of the
operational procedures within each department. Such procedures vary from one
department to another. Work loads are established by considering such factors as
diagnostic tests and treatment procedures performed, patient visits, prescriptions
dispensed, meals served, and pounds laundered.
After space needs are established and preliminary plans begin, care should be taken in
the development of orderly circulation patterns, focusing on the separation of public
traffic, service traffic, and the movement of goods. It is desirable to have clear patterns
of circulation between departments as well as within each department.
A constant in the functioning of healthcare facilities is the continuing requirement for
change. Departments should be planned in a manner that supports independent, open-
ended growth and the location of "soft" space adjacent to high-tech functions likely to
grow. In addition, the proper use of modularity, multiuse space, and changeable walls
and systems can enhance a facility's ability to adapt to new technological and care
requirements.
Health facilities operate within a variety of settings, ranging from small community
hospitals to large academic medical centers, storefront clinics to multi-group practice
ambulatory care centers, and children's hospitals to specialty rehabilitation centers. The
quantity and types of ancillary departments are particular to each setting The rest of this
chapter identifies those departments most common in full-service healthcare facilities.
HOSPITAL PLANNING AND PROJECT MANAGEMENT68 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 69
Example of a relationship matrix
THE SURGICAL SUITE
Introduction
Planning for the surgical suite, one of the most important areas of the hospital involves
various disciplines. The emotional needs of patients must be catered for and also those of
their families. There is no other aspect of hospital care that creates the level of fear and
anxiety than surgery. Therefore, any planning process must involve administrators,
surgeons, anesthesiologists, surgical nurses, representatives of support areas
(housekeeping, pharmacy, central sterile supply, and laboratory) and individuals who
consider the needs of the patient and family.
Departmental Functions
The function of the department is to receive patients after diagnosis, to anaesthetize them
either before or after transfer to the operating table, to operate, and to supervise their
post-operative condition before returning them to the wards. The pre-eminent position
of the surgical department in the hospital can be appreciated when one realizes that in a
typical general hospital, surgical patients represent 50% to 60% of the admissions, and
account for an appreciable quantum of the work of and revenue from ancillary
departments. The surgical suite of a modern general hospital and everything that goes
with it make a very complex workshop. The surgical procedures of the present day,
involving more people and highly sophisticated equipment, have rendered ideas of
planning of operating rooms of the past somewhat obsolete. The major decision centers
on the number and type of operating rooms.
Criteria for department sizing
The basic criteria for determining the number of operating rooms are the total number of
procedures and number of minutes expected annually for the target year. Calculations
are made to determine the total volume of expected surgical operations. The total
number of procedures performed in a given period of time is measured against operating
room capacity, including procedure and clean-up time. Surgery generally takes place in a
seven-to-eight hour, six-day-a-week period beginning at 7.00 a.m. with emergency and
some elective surgery occurring during the weekend. When a shortage of operating
rooms occurs, it is not uncommon for surgery to take place in the evenings and on
weekends. As a thumb rule you can calculate one OT for every fifty beds.
HOSPITAL PLANNING AND PROJECT MANAGEMENT70 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 71
Composition of the Department
The department consists of one or more operating suites that share ancillary
accommodation such as staff changing and rest rooms, arrangements for the reception of
patients, and facilities for the disposal of soiled material. The general OT's should have a
desirable clear area of 400 sq. ft. (minimum 360 sq. ft.) with 20 ft. clear dimension
(minimum 18 ft.) between fixed cabinets and built -in shelves. Rooms for cardio-
vascular, orthopedic, neurological, and other special procedures shall have a desirable
minimum clear area of 600 sq. ft. (minimum for orthopedic is 360 sq. ft. and for
cardiovascular and neurological is 400 sq. ft.), with a desirable clear dimension of 20 ft.
(18 ft. for orthopedic). A room for surgical cystoscopic and other endo-urologic
procedure should have a desirable area of 350 sq. ft. (minimum 250 sq. ft.) with a clear
dimension of 15 ft. The suites may also share a unit for the supply of sterile material and
instruments. Each operating suite normally consists of a theater, an anesthesia room, a
sterile store and a scrub-up. The orthopedic OT shall have enclosed storage space for
splints and traction equipment, which may be outside the OT, but must be conveniently
located. The space occupied by the operating rooms is only about one fourth of the
surgical suite - the supportive services and functions account for the rest of the space.
Although the requirements of theaters can be met by an entirely internal placement,
from the point of view of staff that spends long periods in the department, some natural
light can be a valuable asset. This should be provided for some of the ancillary staff
rooms. The department should be on a cul-de-sac so that access to it can be strictly
controlled (there should be no non-related traffic through the suite). The Intensive Care
Unit should be preferably adjacent. X-rays are normally taken with the help of mobile
machines. The cleansing and the supply of sterile goods is done in a separate Central
Sterile Supply Department (CSSD) that can serve the whole hospital, or a Theater
Sterile Supply Unit (TSSU) which can serve a larger number of theaters via a small
sterile store attached to each of them.
Flow of Various Individuals
Workflow in the surgical suite must be considered in relation to several different groups:
patients, visitors, medical staff, nursing staff, and logistical support. Patients enter the
suite from inpatient nursing units, the same day surgery area, or emergency. Inpatients
generally go to a holding area for surgical preparation, then to their assigned operating
rooms. Outpatients are transported to their assigned operating room. After surgery,
patients are transported to the PACU for recovery. Next, they go to their assigned patient

rooms, or to phase 2 recovery. Visitors wait during surgery in the family waiting area. In
some facilities, inpatient family members or visitors wait in the patients' private room.
Outpatient and same day surgery visitors wait in the preoperative waiting area until after
the surgery, when a limited number of visitors may be allowed to attend to the patient
while he or she is in the phase 2 recovery area.
All surgical staff members change into sterile clothing in dressing areas and enter the
surgical suite through a lounge. They can consult the surgery schedule for room
assignments. All those participating in the surgery scrub and gown prior to entering the
operating room. After each surgery, the surgeon speaks with the patient's family in a
consultation room. Between surgical cases, physicians can take a break in the surgery
lounge. There they can utilize the physician dictation areas to record the
proceedings/outcome of the surgery.
A surgical suite flow diagram
An interrelationship diagram of a surgical suite
HOSPITAL PLANNING AND PROJECT MANAGEMENT72 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 73
Reducing Risk of Infection
Of prime importance in the design of the department is the need to reduce to a minimum
the risk of infection at the operating table. Ensuring the sterility of instruments and other
apparatus is relatively simple, but no less important is the reduction of the risks of
airborne infection. This depends upon management procedures and the physical
arrangement of the department and of its ventilation system. The physical arrangement
should ensure that not only are these procedures facilitated but that as far as possible
they are inescapable.
A surgical department could be divided into zones, where the quality of the environment
would conform to the cleanliness policy adopted by the individual hospital.
! The general zone - in this zone the requirements for cleanliness correspond to the
usual hospital cleanliness standard. This zone includes waiting areas for relatives,
catastrophe and triage areas, plaster rooms, offices, record rooms, laboratories, stores
for non-sterile material, staff lounge-refreshment rooms, toilets and changing rooms.
! The clean zone - this provides for the surgical department reception and holding area,
anesthesia rooms, delivery rooms, Endoscopy rooms, stores for blood, medicine,
parenteral solutions etc., stores for tubed medical gases, the sterile service area, the
general post-anesthesia area, X-ray apparatus stores, and clean bed stores.
! The super clean zone - this accommodates scrub-up and gowning areas, operation
theaters, sterile stores, sterile linen stores, and thoracic post-anesthesia rooms.
! The ultra clean zone - is determined by a circle with a one meter diameter from the
wound.
! The aseptic zone - is limited to the area of the incision.
To minimize the risk of infection the method of artificial ventilation should ensure that
within each suite there is a supply of pure air sufficient to reduce the bacterial count
below a critical level. There should be a positive pressure in the theater and sterile store
to provide a flow of air from the clean to the less clean areas. Each theater in the

department should have its own self-contained ventilation system in order to reduce the
risk of cross infection. There should be no movement of air from one suite to another.
Schematic Diagram of OT Suite Airflow
Other Area Requirements
A holding area is needed at the entrance of the department where patients are transferred
to a theater stretcher. Whether a separate anesthesia room is provided or not, the
anesthetist needs a wide variety of equipment, instruments and drugs which calls for
considerable storage space. In addition, equipment used in the department, some of
them bulky items such as the C-arm and portable X-rays need to be stored in alcoves.
After the operation the patient is transferred to a recovery area for recovery from the
anesthesia, and then either to his own ward or the ICU. The Post-Anesthetic Care Unit
(PACU) (Recovery) area needs to be easily supervised and readily accessible from all
the theaters. it should contain a medication station; hand-washing facilities; nurse
station with charting facilities; clinical sink; provisions for bedpan cleaning; and storage
space for stretchers, supplies and equipment. It would be desirable to have 80 sq. ft. for
each bed in addition to the above spaces and a clearance of at least 4 feet between beds
and between beds and adjacent walls. The thumb rule for sizing is one and a half to two
beds per operating room.
The procedures carried out in the surgical suite are probably the most precise and critical
of all the functions performed in a hospital. The suite itself makes the most exacting
HOSPITAL PLANNING AND PROJECT MANAGEMENT74 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 75
demands upon detailed design and is frequently the most remote form the average
designers direct experience. Ventilation and lighting are probably open to more refined
improvement than in any other part of the hospital building. For these reasons there may
be much to be said for a design approach that anticipates future flexibility and change
instead of attempting precise original design with materials and equipment that may be
difficult to alter later.
The following service areas shall be provided:
! A control station located to permit visual observation of all traffic into the suite! A supervisor's office or station! A sterilizing facility for immediate or emergency use! A medication station for distribution of drugs and routine medicine! An enclosed soiled workroom for the exclusive use of the surgical suite, for the
collection and disposal of soiled material! A clean workroom or clean supply room, where clean materials are assembled prior
to use or following the decontamination cycle! Medical gas storage facilities, in addition to the main storage, separate storage of
reserve gas cylinders necessary to complete at least one day's procedures! An anesthesia workroom for cleaning, testing and storing anesthesia equipment,
with space for anesthesia carts! An equipment storage room! Staff clothing change areas, containing lockers, showers and lavatories, and space
for donning surgical attire, with a one-way traffic pattern, from 'dirty' to 'clean'.! Staff lounge and toilet facilities! Dictation and report preparation areas! Outpatient recovery! Change areas for out-patients and same-day admissions! A space for patient examination, interviews, preparation, testing and obtaining vital
signs of patients for out-patient surgery! Storage areas for portable X-ray equipment, stretchers, fracture tables, warming
devices, auxiliary lamps, etc. These areas shall be out of corridors and traffic.! Housekeeping facilities! An area for the preparation and examination of frozen sections! Provisions for refrigerated blood storage! Where applicable, appropriate provisions for refrigeration facilities for harvested
organs! Provisions for pathological specimens storage prior to transfer to pathology section
Services, except for the soiled workroom and housekeeping room may be shared with
the obstetrical facilities if the functional program reflects this concept. Service areas,

when shared with delivery rooms, shall be designed to avoid the passing of patients or
staff between the operating room and the delivery room areas.
Operational Relationship
There are several operational issues that affect surgical suite design for example,
integrated versus independent outpatient facilities, perimeter work corridor versus
interior work core, and integrated versus separate central sterile supply.
The consideration of an integrated versus independent outpatient facility addresses the
question of the outpatient service location. Outpatient surgery can be an integrated part
of the inpatient surgery suite or separated in an independent outpatient suite that
includes both preoperative areas and operating rooms. These areas may be located on or
off campus. The appropriate location of this service will involve the medical staff and
hospital administration.
A perimeter work corridor layout circles the operating rooms. The layout provides a
single corridor system that is used to transport patients, physicians, nursing staff and
clean and soiled supplies. Closed clean and soiled case carts and double bagging of
waste products are used to maintain sterile conditions. An interior work core separates
clean distribution from the soiled distribution system. Placed between two rows of
operating rooms, the interior work core is used for sterile supplies and instruments.
The issue of an integrated versus separate central sterile supply (CSS) is whether central
sterile supply is placed adjacent to surgery or on another floor: if it is placed directly
above or below the surgical suite, it is linked by elevator or dumbwaiter. Although the
surgical and CSS staff normally prefer an adjacent relationship, physical building
constraints often have a bearing on the location of central sterile supply.
HOSPITAL PLANNING AND PROJECT MANAGEMENT76 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 77
A diagram of a surgical suite's perimeter corridor concept
A diagram of a surgical suite's interior work core concept

Trends
Surgical facilities will continue to separate outpatient cases from inpatient cases. The trend is, however, toward integrating outpatient with inpatient surgery for greater efficiency in the use of staff and instruments and cost reduction. This trend puts additional pressure on the surgery staff to maintain outpatient standards of care within the inpatient hospital setting. Outpatients will continue to require direct and convenient means of entering the outpatient area.
Pain management services will expand as new and better means of reducing pain are developed. The preoperative patient areas will continue to be key locations for pain management services. The integration of invasive imaging (cath lab) within the surgical suite will increase as a means of delivering invasive imaging in a surgical environment. A developing trend is to combine surgery with magnetic resonance imaging. Each of these trends carries with it the promise of improved surgical services and better care for the patient.
Intensive Care Units
Introduction
Many people – caregivers, architectural and design professionals, and patients, regard intensive care (critical care) units as the heart of the hospital. Here a seriously ill patient can expect the maximum of care: the very best the hospital has to offer in terms of personnel and technology.
Intensive Care Units (ICUs) are specialty nursing units designed, equipped and staffed with specially skilled personnel for treating very critical patients or those requiring specialized care and equipment. Centralizing the acutely ill patients, as is often done, in contiguous units in an intensive care complex consisting of surgical-medical intensive care unit, coronary care unit and specialty units such as renal and burn units, results in multidisciplinary care and economical use of the space and equipment.
Location
There is no unanimity among the medical and nursing experts as to where the ICU should be located. There are two schools of thought. One suggests that the ICUs should be in a centralized place and be contiguous with, or readily accessible to, one another. The argument is that patients admitted to the medical-surgical intensive care unit may have, or suddenly develop, cardiac complications. Having intensive care facilities in a centralized place allows the specially trained professionals and equipment an almost instant access to patients in all clinical services when an emergency develops. Such an arrangement also eliminates the need for duplication of costly equipment and personnel.
HOSPITAL PLANNING AND PROJECT MANAGEMENT78 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 79
The second school of thought favors that the location should be dependent on the type of patients. For example, the surgical ICU should be close to the operating rooms while the medical ICU should be in close proximity to the medical ward to facilitate following the concept of progressive care. That is, the patient is moved from the intensive care unit to intermediate care or step-down unit, and then to the general patient care area.
Whatever its location and adjacencies, the intensive care unit must exclude through-traffic.
Relationships with other Departments
Intensive care units should be close to emergency, Operation Theater Suite, Respiratory Therapy, Laboratory and Radiology. Most admissions to ICUs are either through the emergency department or from the operating rooms following major surgery. They should not be too far away from general nursing units, as patients may need to be transferred in an emergency. They should be close to vertical transportation cores. They should be away from heavy traffic and noise. The electrical influence of equipment like elevator motors and X-ray equipment on the displays of monitors should be kept in mind. Accessibility and direct visual contact between patient and nurse is important. The patient should be close enough to permit observation of respiration, facial color and other revealing symptoms.
Sizing Considerations
It is generally recognized that for effective operation, there should be no more than twelve beds per intensive care unit. Twelve beds is seen as the upper limit of what an ICU nursing staff and station can adequately monitor. An intensive care unit of less than six beds is clearly uneconomical.
This guideline of twelve beds maximum will become decreasingly significant as ICU's incorporate bedside computers that enable “paperless charting” and direct recording of vital signs through monitoring devices. Such technology will encourage “decentralized nursing” which will allow nursing staff to spend less time at a central nursing station and more time in patient rooms and at mini-work stations directly adjacent to these rooms.
As to the rooms themselves, the American Hospital Association (AHA) minimum is 150 square feet per room. This may be adequate for non-critical patients, but it is too small for patients on life-support and monitoring equipment. The task force on Guidelines of the Society of Critical Care medicine recommends 150 to 200 square feet in open units, while private patient rooms should contain 225 to 250 square feet. The ICU patient room should be planned to facilitate operations in the event of a crisis.

The beds should be located permanently away from the wall, to give staff a 360-degree access to the patient.
Technology and Humanity: Design Priorities
It is alarming to review the substantial literature that now exists on intensive care units of the recent past devoted to how the environment of the intensive care unit can adversely affect patient health while simultaneously increasing stress and fatigue among the physicians, nurses, and nurses, and others who work in these areas. The fact is that many ICU's and ICCU's – are literally – sickening.
In most ICU's, the focus is not so much on the patient as it upon a disease or disorder, as if the procedures necessary for sustaining life in the physical sense were somehow incompatible with simultaneously sustaining emotional well-being. The assumption seems to be that the ICU patient is either unconscious and unaware of his surroundings or too sick to care about them. The issue is that emotional health cannot be neatly isolated from physical health. The machinery makes many patients feel invaded and helpless. The sense of claustrophobia created by packing monitoring equipment, respirators, and IV delivery equipment into a small space can dramatically increase anxiety levels.
Windows are all too often absent from intensive care unit design. Not only does this heighten the sense of claustrophobia inherent in these technology-packed areas, but a number of studies have demonstrated that patients in windowless rooms are subject to temporal dislocation and even subject to “ICU psychosis”, which is characterized by delirium, hallucination and delusions.
Harsh lighting, especially from fluorescent fixtures often aggravates the disorienting effects of having no windows, and by lighting that is not dimmed to correspond to the body's circadian rhythms. Sleeplessness is a common problem in intensive care units, and it is not only due to lighting, but also to the remarkably high level of noise that prevails in many of the older units.
Excessive noise is particularly stressful for cardiac patients, who exhibit increased cardiac workloads and arrhythmias in noisy environments. In addition, pain perception is heightened by the presence of excessive noise. There are more diffuse negative responses reported by patients, including a sense that they could not “escape” their environment; a general and anxiety-provoking sense of unrelenting urgency in the environment; sensory deprivation; crowding; and loss of privacy. Many related feelings also affect those who work in the critical care unit, leading them to depersonalize patients.
All of these responses can at least be mitigated by design solutions.
HOSPITAL PLANNING AND PROJECT MANAGEMENT80 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 81
Technology and Design: Achieving a Balance
While emphasizing the human aspects of ICU design, the intention is not to denigrate technology. Not only does medical machinery save lives, it has the potential of actually humanizing the relation of caregiver to patient by saving staff time, for example in the automatic recording of data, enabling the time freed to be used to be in contact with and treating patients. The development of “bedside laboratory” technology can be employed to assess blood gases, electrolytes, glucose, and hemacrit using a very small blood sample – 0.5 ml – in less than ninety seconds.
Good design can do much to accommodate the machinery while keeping it out of the way. Particular attention should be devoted to the headwall, which, especially in the intensive care environment, bristles with connections for medical gases, suction, electrical power, and terminal hook-ups. Consideration must be given as to whether the hook-ups should fan out from the patient to the headwall, whether they will converge at a power column, or run to an overhead rail system. In general medical-surgical patient rooms – and even in some critical care facilities – attractive casework can be used to hide all or some of the hook-ups in the headwall.
The choice of headwall, power column or rail system is in large part determined by the layout of the room (especially the orientation of the bed), which, in turn, is a function of overall unit design and the need to balance the demands of technology, accessibility and privacy. The starting point for the layout of the room is the orientation of the bed. From the point of view of the nurse, the bed should be situated to allow ready observation of the entire body, especially the head. Tradition dictates that the head of a bed be against a wall, and certainly, headwalls accommodate readily to this approach. However, in a crisis, it is often essential to have access to the patient from all four sides. Certainly, the bed can be pulled quickly out from the wall, but tubes and monitor leads may continue to inhibit access or may even present a trip hazard. Some architects have proposed a partial solution to this in non-square rooms or rooms with one angled wall, meant to increase clearance around the bed (and to give the room greater sensory interest to the patient). However, a similar approach is to treat the bed as an island.
Specialized Intensive Care Units
An Intensive Coronary Care Unit is used to identify the units restricted to patients who are suffering from cardiac emergency conditions. Patients are transferred from here to an intermediate care section, which ought to have twice the number of intensive area beds. A Pulmonary Intensive Care Unit (PICU) is a major key in a comprehensive pulmonary care program for chronic obstructive lung disease. A laboratory for around-the-clock determination of arterial blood gases immediately adjacent to the PICU is required, since these patients are very unstable. A logistic delay due to laboratory remoteness or unavailable technical assistance is not acceptable. Neurovascular or

stroke cases are admitted predominantly from the emergency department. In a Burns Care Unit two phases of the burns illness - the shock period and the healing period - have to be accommodated. Complete reverse isolation can be a significant factor in the prevention of bacterial contamination of individuals incurring major burns injuries. For maternity patients with complications and particularly for those in premature labor a special ante and intra-partum unit also referred to as an obstetric or labor or maternity intensive care unit can be provided. In conjunction with this, a Neonatal Intensive Care Unit (NICU) can be provided, which is an intensive care nursery which provides the best chance of saving life and of improving physical and developmental status for survivors of serious perinatal illness.
These and other specialized units are discussed in greater detail below:
Intensive Coronary Care Unit
After the surgical-medical ICU, the intensive coronary care unit (ICCU) is the most commonly found critical care unit in the hospital. The central design issue in the ICCU is finding a strategy to promote tranquility and even relieve visual and acoustical isolation. So-called “ICU psychosis” is a shocking enough symptom of poor critical care design. In the case of an ICCU, noise and visual clutter have a readily demonstrable adverse effect on heart rates, arrhythmias, and blood pressure.
Respiratory Care and Step-Down Units
The respiratory care unit has developed as an alternative to the traditional ICU in response to the constraints of managed care and cost containment. Studies show that 35% of surgical and medical intensive care patients were admitted to these costly units strictly for the purposes of monitoring and did not require any active intervention. The patients were not suffering from any immediately life-threatening processes. The studies suggested a rationale for providing more cost-effective intermediate care units for those patients in need chiefly of close monitoring rather than aggressive intervention.
Cost savings are achieved in part through reduction in the amount and nature of required equipment and, in even larger part, through reduced staffing needs. Whereas the nurse to patient ratio in the ICU may be 1:2 or even 1:1, in the respiratory or step-down unit the ratio can safely be set at 1:3 or 1:4.
Critical Care of the Elderly
Until some time back, most buildings were standardized on the model of a thirty-year
HOSPITAL PLANNING AND PROJECT MANAGEMENT82 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 83
old healthy male user or occupant. Increasingly, however, architects and planners are designing for a seventy-year-old woman who is in less then optimum health. While no radical steps need to be taken to design special critical care facilities to accommodate older patients, certain design features can be incorporated into general ICU's to make them friendlier to the aged.
Gerontologists speak of an “environmental docility hypothesis”, which holds that as competence decreases, the probability that behavior will be influenced by environmental factors increases. We know that critically ill patients often feel at the mercy of their environment. This seems to be even more compelling among the critically ill elderly.
Some of the design areas discussed earlier, especially noise control, light and color, are particularly important in designing with the elderly in mind. Noise reduction should be a high design priority. Because of diminished visual acuity in the elderly, lighting should be planned to avoid glare. This also means keeping highly reflective surfaces to a minimum. Color discrimination also deteriorates with age. Differentiating among dark shades and among pastels is a particular problem. Thoughtful use of contrast to emphasize planes and corners aids orientation. However, the elderly person should not feel dominated by the colors in his environment.
Neurological Intensive Care
An array of neurological conditions may require intensive care. Many of these conditions can be treated appropriately in the general surgical or medical ICU, but the monitoring and treatment of intracranial pressure (ICP) in particular has been cited by many authorities as ample rationale for creating specialized neurological intensive care units.
Probably the best model for the neurological ICU is the Intensive Coronary Care Unit (ICCU), which focuses on continuous and sophisticated monitoring in order to achieve early detection of developing problems. Increasingly sophisticated monitoring devices will have to be accommodated in neurological critical care, and these must be added to a full array of respiratory and ventilation equipment.
Perhaps the single greatest design impact of the neurological ICU is the issue of adjacency. It is desirable to locate this unit near such diagnostic facilities as MRI and CT.
Burns Unit
Another specialized intensive care facility found in larger, often regional hospitals, is the burns unit. Some hospitals, most notably the network run by the shrine of North

America (Shriners), are devoted entirely to the treatment and rehabilitation of burn victims.
For design, the single most important clinical factor in treating burns is creating structures that minimize the risk of infection. Burns unit critical care patient rooms should be private, rather than an open ward, to minimize the risk of cross-infection.
The ICU at Shriner's Hospital Galveston Burns Institute (HDR Inc. were the architects) features patient rooms that are fully enclosed with glass to allow maximum visibility while providing for isolation. The HVAC system was designed to surgical operating room standards, and positive air pressure as well as HEPA filtering promotes surgical suite air quality.
The Galveston ICU patient rooms also include radiant heat systems above each bed. These are linked to thermal sensors mounted on patients who lack an insulating epidermal layer, and, in this way, heat loss is perfectly compensated for by the radiant panels. Environmental control extends to the maintenance of high relative humidity as needed to help prevent damaged skin from drying out.
In addition to meeting the demanding clinical conditions required by the advanced treatment of severe burns, the burns unit ICU should project as much of a non-institutional sense of well-being as possible. Severe burn injury is not only physically painful, but is especially depressing and anxiety provoking. Patients suffering from disfiguring injury benefit from maintenance of contact with the outside world. Tragically, it is also the case that a great proportion of burn victims are children. The focus of the Shrine-sponsored institutions is pediatric. But all advanced burns units should be designed with the younger patient in mind.
The Issue of Isolation in Intensive Care Units
In discussing the burns ICU we have touched upon the issue of isolation to prevent infection. Patients admitted to an intensive care unit have a higher risk of nosocomial infection than other hospitalized patients.
Most authorities believe that design for isolation is primarily a matter of ventilation, filtering, and maintaining positive air pressure in the patient room, for patients who are immuno-compromised. For patients who themselves are a source of infection, negative air pressure is maintained, other safeguards remaining the same. It is assumed that nursing the patient in a one-patient room with the door (or pair of doors with an air-lock lobby) closed is the best safeguard against infection in intensive care.
HOSPITAL PLANNING AND PROJECT MANAGEMENT84 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 85
The Neonatal Intensive Care Unit
This is discussed separately as a department.
THE NEONATAL INTENSIVE CARE UNIT (NICU)
The design and planning issues with respect to a neonatal intensive care unit (NICU)are sufficiently unique to warrant a separate discussion, apart from that of intensive care units in general, which are separately discussed above.
The discussion will be under two broad heads, These two heads are:
1. Design Issues for Neonatal Intensive Care Units
2. Design Guidelines for Neonatal Intensive Care Units
Design Issues for Neonatal Intensive Care Units
The modern neonatal intensive care unit is the product of two factors:
1. The development of an understanding that the pathophysiologic phenomena associated with the newborn are so distinctive that they require an appropriate setting where the critically ill infant can be effectively managed, and
2. Convergent advances in electronics and biochemistry, which made such a setting feasible.
These advances include:
1. Methods for continuous evaluation of numerous parameters of neonatal (and fetal) illness.
2. Methods of continuous monitoring of cardio-respiratory function.3. Micro-techniques for the rapid biochemical determinations from minute blood
samples.4. Servo-controlled radiant-heat incubators.
These advances, coupled with improved methods for controlling infection, prompted the development of the NICU: a common area where all medically and surgically ill infants are treated, premature and full term, infected and non-infected.

NICU's perform the following functions
1. Observe critical infants
2. Monitor critical infants electronically and bio-medically
3. Carry out advanced therapeutic procedures
4. Promote maternal-child contact to the fullest extent possible
The last functions is because it is realized by now that maternal handling as well as sensory stimulation (but not over-stimulation or inappropriate stimulation) are crucial in the neonate's earliest hours and days – even if the infant is critically ill. Thus designers of NICU facilities are faced with a set of requirements that are, in many points, contradictory. One the one hand, there is a call for a common technically sophisticated space, while, on the other, there is a call for a humane environment that facilitates maternal contact.
A number of studies have suggested that humanizing the NICU may be more of a clinically urgent matter than merely a desirable goal. Some authorities have suggested that continual exposure to bright lights may contribute to retinopathy of pre-maturity (ROP), a leading cause of blindness in premature infants. Another effect of continual high-level illumination is disruption of diurnal patterns at this earliest stage of development. Monitoring of cardio-respiratory function demonstrates that these vital signs tend to be more stable when infants are exposed to cycled lighting that mimics diurnal patterns.Also, when light levels are high, noise levels are commensurately high. When light levels are dimmed, noise levels also decline. Indeed, noise in traditional NICU's is often at a distressingly high level. Alarms and incubators are the biggest mechanical noise producers. These not only elevate levels of arousal, there is evidence that protracted exposure to incubator noise levels in excess of 70 decibels may contribute to actual cochlear damage and subsequent hearing loss. As in the adult ICU, sensory overload is also a threat to professional staff. In a more recent development, undertaken in part to minimize the ill effects of the traditional NICU unit, architects have moved away from the warehouse style NICU, designing instead smaller units of four to six bassinets.
The only humanizing architectural element that most authorities argue against including in the design of the NICU is windows, primarily due to their thermal effects, which can cause potentially harmful dips or spikes in ambient temperature. In settings where fully enclosed incubators are used, it is even possible that too much sunlight can cause excessive warming due to a greenhouse effect.
NICU's should incorporate muted colors, since babies especially under stress, do not
HOSPITAL PLANNING AND PROJECT MANAGEMENT86 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 87
respond well to bright colors. Lighting suggested is true-color fluorescent and indirect cove lighting. To maximize efficiency, place the nurse workroom immediately adjacent to the NICU, to enable nurses to monitor the unit more closely. A parent room should be provided close by to accommodate well parents who wish to be close to their baby. Lighting levels can be automatically cycled to promote the babies regular sleep schedule, and finishes throughout the facility should be more traditional than institutional. As far as possible, the NICU should maintain the homelike setting that predominates throughout the family birth unit.
Design Guidelines for Neonatal Intensive Care Units
The creation of formal planning guidelines for newborn intensive care units (NICU's) occurred in 1976 in the USA, and since then, the American Academy of Pediatrics (AAP) and American College of Obstetricians and Gynecologists (ACOG) have published a number of their comprehensive Guidelines for Perinatal Care, among other documents.
The purpose of this document is to provide health care professionals, architects, interior designers, health care facility regulators, and others involved in the planning of NICU's with a comprehensive set of standards based on many years of clinical experience.
These recommendations are planned to be upgraded on a regular basis, incorporating new research findings, experiences and suggestions.
While many of these standards are minimal, the intent is to optimize design within the constraints of available resources, and to facilitate excellent medical care for the infant in a setting that supports the central role of the family and the needs of the staff.
The latest revision of these standards can be found on the website:www.nd.edu/~kkolberg/DesignStandards.htm
These are the:Recommended Standards for Newborn ICU DesignReport of the Fifth Consensus Conference on Newborn ICU DesignJanuary 2002Clearwater Beach, Florida

MATERNITY / OBSTETRICS DEPARTMENT
Introduction
The maternity department, also referred to as the obstetrics department, is usually the setting for a natural process as opposed to a pathological one. This department differs from most other departments in a hospital because it is designed to house a happy event, also called a “wellness' event. It is dealing with a continuous process, maybe from insemination (if clubbed together with IVF) to pregnancy through delivery to post-natal care of both mother and child. It is not so much concerned with curing an illness but with the fulfillment of a natural act. It is important, therefore, that the design of the department should not be in any way be suggestive of ill health.
It is a good design response to keep this department separated from the rest of the hospital, it need not necessarily be on another site, but can certainly have it's own entrance and image distinct from the facility it is a part of, to foster the concept of a “wellness” place. If connected to a multi-specialty hospital, it could share support services such as food and laundry, as well as diagnostic and other services the “patients” may need.
The Maternity Department
The department is divided largely into two parts:
· The outpatient clinics.
· The inpatient accommodations concerned with delivery and post-natal care.
The outpatient clinics can be a part of the hospital's outpatient department or may be provided separately. These same rooms could also accommodate post-natal examinations, family counseling and gynecological outpatients.
The delivery suites have a lot in common with the operating theaters. There are similarities in the ways they are located and controlled. In laying out the labor and delivery suite, the designer should consider the functional areas comprising the department such as the preparation room, labor room, delivery room, recovery room and support services area. We recommend that there be a provision of an operation theater in the department where major obstetrical surgery can be performed. If this does not work within the area or budget constraints one of the delivery rooms should be designed and equipped to serve this purpose.
Antenatal patients are usually seen at the time of booking, at about the thirty-sixth week
HOSPITAL PLANNING AND PROJECT MANAGEMENT88 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 89
of pregnancy, and then weekly until admission for delivery. This clinic should preferably be accessed separately from the center's main entrance, and will comprise of a waiting space, rooms for history taking and examination, urine testing room and lavatory, and office and record space. Easy access to the clinical laboratory and imaging sciences is advantageous.
The layout of the department is dependent on the type of delivery envisaged by that particular facility and the number of projected deliveries. There are three main delivery models in obstetrics:
1. Traditional.
This is a process in which the patient moves through different rooms and areas during the various stages of giving birth. The patient is admitted to a triage area and transferred to a labor room. The patient is then transferred to a delivery room for the birthing process. The patient is transferred again to recovery post-delivery. The postpartum unit is the final stop for the new mother. The infant is placed in a nursery adjacent to or within this unit. Of the three models, this one involves the most movement of the patient.
2. Labor/Delivery/Recovery (LDR).
These are oversized single-occupancy patient rooms that are used for all the three processes of labor, delivery and recovery. These are an established feature of the healthcare industry in the West but have been introduced in India only in the early 2000's. They consist of a well-designed room that offers the expectant mother the advantages of a family-oriented birthing process in one room, other than when the case is a high-risk one. They are designed like a residential bedroom, with obstetrical equipment tucked away, out of sight. These rooms can be quickly converted to high-tech procedure rooms as the delivery progresses, with the necessary equipment brought in. This provision offers would-be mothers the best of both worlds - the comforts of their house in the setting of a hospital setting with competent medical care.
Although the trend in the West was to use these rooms as postpartum beds as well, this practice has changed there because of several issues: inefficiency in room utilization, difficulties with nurse cross-training, and patient preferences to continue recovery in a quieter setting. Consequently, many postpartum beds are located adjacent to LDR areas, in their own quiet rooms, frequently with newborns rooming-in with their mothers and with double beds provided for the fathers.
3. Labor/Delivery/Recovery/Postpartum (LDRP).
This facility consists of a single room used for the entire stay of the patient in the hospital. The newborn may stay in the room or in the nursery for full or partial care. In these three models of birthing, this one occasions the least movement of the patient.

Marketing opportunities for the main facility
Specialty care units like a maternity department or a comprehensive woman's care facility can provide valuable marketing opportunities for the hospital they are attached to not only through the services they provide but through their design as well.
Maternity units can constitute an effective marketing “niche” in today's times. They can be designed with a focus on “high touch”, and given a residential, non-institutional image. The unit can be designed to have a non-clinical atmosphere and can be a setting in which expectant mothers can meet, which can be desirable especially in new communities.
It could be a good marketing strategy for a healthcare facility based in a large community to reach out to it's primary market area by combining a birthing center with other diagnostic and treatment functions. This configuration can create a satellite ambulatory care center with integrated physician office practices with both affiliated and non-affiliated physicians.
The intention should be to create in the patient's mind a positive associative image of the hospital. This can be achieved by providing amenities not usually found in hospitals. These may range from attractive façade design and entrance areas, lounges located on the floor (for patients and families) to small reading areas, Internet access, and access to an electronic library, which can be educational. The ambiance in these units should be one that aids healing and produces tranquility, the very anti-thesis of institutional environments in hospitals of the past.
Patient and Work Flow
An easy and clearly indicated entrance for patients is an important design requirement because of the urgency of the labor and delivery process and the stress and anxiety that may accompany it. Patients come to the maternity department from a number of places, such as the women's center main entrance, the emergency department (especially after hours), and the doctor's office.
Today most healthcare facilities in the West direct patients through a central triage area. At this point, physicians decide whether to observe or advance a patient to an LDR/LDRP room or patient room or to a cesarean section room for immediate delivery. The area may be adjacent to or shared with a cesarean section recovery area for staffing efficiency and flexibility in assigning patient beds. Immediate proximity of this area to the cesarean section suite is essential for efficient transport time.
Patients in active labor are transferred to a labor room, an LDR room or a LDRP room, where family members may join them. The LDR/ LDRP design concept incorporates
HOSPITAL PLANNING AND PROJECT MANAGEMENT90 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 91
locating rooms around the perimeter of the facility for day-lighting and should allow direct access from triage, the cesarean section area, resuscitation, and the neonatal intensive care unit (NICU). Adequate patient and family amenities ensure a successful labor and delivery area.
In the LDRP model, staff flow begins with patient contact at the reception area, then continues to the triage area, labor and delivery/recovery areas, and postpartum or discharge area. In an LDR/LDRP concept, the patient will experience the same nursing staff throughout the labor/delivery process. Staff will move clean equipment into the room for delivery and remove post-delivery equipment for cleanup.
After post-delivery assessment, the infant often remains with the mother during recovery before being transported to the nursery for further assessment, cleaning and gowning. Infants in stress are transported directly to a transition nursery or an NICU if directed by the neonatologist. After a delivery occurs in the cesarean section room, the mother is transferred to the recovery area. At that point, the baby is observed in a resuscitation area or a transition nursery adjacent to the delivery suite.
Physician and staff gowning facilities should provide a one-way flow into the cesarean section suite, as in the surgery department. Physician and nurse work areas should be decentralized and located closer to the patient areas to improve patient care and staff efficiency.
Relationships with other Departments
The obstetrics area is the focal point of a comprehensive women's center. There are some departments and services that have strong ties with the women's center. The neonatal intensive care unit (NICU) should be contiguous because of the frequency and priority of the newborn being transferred to this facility.
The postpartum/ obstetrical inpatient unit and well-baby nursery require easy accessibility, separated from public traffic and with horizontal or vertical access to obstetrics. Emergency and surgery departments require easy access; cases might come in from emergency or go to surgery.
In recently designed facilities in the West, the trend is to combine all services necessary for comprehensive women's care, including perinatal services, pediatrics, breast health services, and education centers, in addition to labor, delivery, recovery and postpartum facilities.
Special Planning and Design Considerations
There are a number of special planning and design considerations for obstetrics, as

enumerated below:
1. Make the unit easily accessible to visitors, but separate patient and support traffic from visitor traffic. This is necessary to protect the patient's privacy and dignity.
2. The design of the unit should be sensitive to the needs of the families of the patients; the colors, materials, furnishings and the overall ambience should be appropriate to the activities and mood. The use of artwork in harmony with the overall interior design scheme can help create positive distractions and peaceful imagery desirable in the context.
3. The focus should be on creating an ambience of “wellness”, offering views of nature, landscape scenery, and water is very desirable.
4. In the inpatient areas (Rooms, LDR's, LDRP's), the design objective should be to give patients and their families control over their environment through permitting them to set lighting levels and the temperature to their comfort, providing adequate storage space, and TV/VCR/music with the controls at the bedside.
CLINICAL PATHOLOGY
INTRODUCTION
The essential function of the department is to carry out diagnostic tests on specimens from in-patients and outpatients. It may also be concerned with work for clinics, health centers, local practitioners and the public health services. Within the department the main divisions are those for histology and morbid anatomy, which involve the microscopic examination of tissues and cells; hematology, the study of blood; biochemistry, the study of living tissues and fluids, cytology, the study of body cells for malignancy etc. and microbiology, the study of micro-organisms. Each of these divisions may require sub-departments, their extent depending on the context and policy of the laboratory. Larger hospitals may have a separate unit for blood transfusion services (a blood bank).
In addition to those originating from outside the hospital specimens will be delivered from the wards, the operating theaters, the mortuary, the outpatient department and from the accident and emergency department. Some specimens, particularly blood and urine, will be obtained from outpatients on the spot, and for this a sample collection center is needed. Nearly all specimens will pass through a central reception and sorting office before distribution to the appropriate laboratory divisions. Small ancillary units are
HOSPITAL PLANNING AND PROJECT MANAGEMENT92 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 93
often sited in the ICU (for speedy blood gas analysis) or in the emergency unit. Planning for future expansion is important, as space requirements for laboratories tend to double every 10 years.
Laboratory requirements are inevitably complex, variable and confusing, and it is essential that the brief should be comprehensive and precise if the resulting design is to be successful. A bad brief is more likely to result in an unsatisfactory design than is usual. The brief can usually be obtained in two stages, which correspond to the stages in which the design team requires information to progress the scheme. The first is that needed to produce the initial sketch designs; the second is that needed to produce the detailed designs, from which the production information can be prepared.
The first stage brief consists of accommodation requirements. This should include:·accommodation schedule - a room-by-room list giving name, area and occupancy
of each;·room relationship statement - guidance on rooms that need to be grouped in close
proximity or en suite;·operational policy statement - a general explanation of how it is proposed to
operate the facility, e.g. how the facility will be supplied, how waste will be disposed of, hours of operation;
·general environmental conditions - whether mechanical ventilation or air conditioning is required in specific areas or throughout;
·non standard requirements - identification of any rooms or areas in which out-of-the-ordinary space, servicing or other demands will affect the building form.
The second stage brief consists of detailed requirements. This should include room-by-room details of:·engineering services requirements - e.g. power supplies, water supplies, special
gases;·environmental requirements - ventilation, temperature, humidity, lighting;·fittings and equipment - e.g. benching, cupboards, fume cupboards, equipment;·finishing's - floor, wall and ceiling finishes.
Information on the second stage is best gathered by means of room data sheets, on which the detailed requirements and content of each room are recorded on a standardized pro forma for the project.
LOCATION
The following factors should be borne in mind when considering the location of a pathology department:

·It should be easily accessible from the OPD, accident and emergency and maternity departments; surgical wards; operating theaters and intensive care unit. Medical wards and other clinical departments should also be within easy reach of these diagnostic facilities.
·There should be a close link with the main hospital routes for ease of distribution of laboratory specimen containers, reports and blood to the wards and other hospital departments; ease of transport of specimens from these to the pathology department and ease of access for medical and other hospital staff.
·The function of the hospital mortuary is closely linked with that of the pathology department, in particular the histopathology departments activities and personnel. The mortuary should be easily accessible to pathology staff.
·The whole department should be planned as an integral secure area. In particular, the total number of entrances from the exterior should be minimal, to deter unauthorized access. In addition, there should be no corridor traversing the department which could be used as a link between other departments or constitute a fire escape route except for users of the department.
·The receipt of bulk deliveries of laboratory supplies and large items of equipment may influence planning decisions on the size and number of stores, positions of lifts, hoists, corridors and doors.
·Laboratory areas are considered to be potential sources of infection and high fire-risk areas. For these and for aesthetic reasons, proximity to staff accommodation and to those areas frequented by the public is inadvisable.
·Good access must be available for fire brigade vehicles.
·Exhausts from ventilation systems servicing the pathology department must be discharged safely to avoid ingestion by neighboring supply ventilation systems or entry into adjacent windows of naturally ventilated spaces.
·Convenient access will be required to an incinerator for the safe disposal of laboratory waste.
·Easy access to external stores of gases and flammable materials is desirable.
Specifications
HOSPITAL PLANNING AND PROJECT MANAGEMENT94 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 95
·Lighting- Laboratory work requires a higher level of illumination at the workbench, generally 500 lux, and to conserve energy it is best to have light colored walls, ceiling, floor and furniture surfaces. High efficiency luminaires with mirror louvers and electronic ballasts are recommended.
·Walls and Ceilings-They should be impermeable, non-porous and smooth for easy cleaning.
·Floors- Laboratory floors should be level. If there is a particular requirement to wash down the floor as in, for example, an autopsy laboratory, floor waste gully traps will have to be installed. Floor coverings should be pre-finished sheet vinyl or equivalent material manufactured specially for the laboratory use with welded joints, taken 0'-6” up the walls. Abrasive-surfaced materials should not be used as they are difficult to clean. However, some laboratories such as for autopsy are washed down and need non-slip floors.
·Workbench Surfacing- When selecting bench surface materials, the design team should obtain samples of materials from the suppliers. The client can then apply the chemicals and test the stain removal procedure recommended by the suppliers. Other tests by the client may include heat, impact, cold (liquid nitrogen) and abrasion.
Chemical Pathology Department
Chemical pathology involves the detection and measurement of chemical and biological substances in body fluids, mainly blood, serum and urine. Quantitative changes give an indication of the progress of disease or response to treatment.
In general there are three types of activity that take place:
·Automated testing: high proportions of the most commonly requested tests are automated, with some equipment having a high capacity. Instruments may be linked to both data input at reception and download results to a laboratory computer. In general instruments are freestanding.
·Semi-automated or non-automated techniques: these cover a wide range of techniques such as flame atomic absorption, chromatography, electrophoresis and immunoassays, some of which utilize radioisotopes. The latter require a separate room conforming to statutory regulations regarding radioactive substances. Chromatographical techniques may require inflammable solvents and

electrophoresis, high voltage.
·Emergency laboratory: A separate emergency laboratory must be located in a position that allows inputs of urgent specimens at all times. It is advisable to have the emergency laboratory next to, or part of, the automated laboratory.
Hematology
Hematology is concerned with diseases of the blood and blood forming tissues. A hematology department should provide a comprehensive laboratory and clinical service for patients with blood disorders and provide hematology and blood transfusion support for clinicians caring for patients with other diseases.
The Hematology department will normally include the following sections:
·General Hematology: Core investigations such as full blood count, differential white cell count, erythrocyte sedimentation rate etc., are carried out in this area. Most routine estimations are performed using complex automatic analyzers, some of which utilize robotic sample handling and closed blood sampling. In many cases microscopic examination of a blood film or bone marrow smear is part of the diagnostic process.
·Special Hematology: The more specialized hematological investigations, such as clotting tests, test for the control of anticoagulant therapy and Vitamin B12, Folate and Ferritin assays amongst others, are carried out here.
·Blood bank: This section handles the receipt, storage and issue of blood and blood products for therapeutic use. Blood grouping and antibody screening and identification tests are performed and where necessary blood matching is done for donor and recipient.
Provision for antenatal and postnatal serology will be required if the hospital has a maternity unit.
Histopathology department
Histopathology is the study of tissues removed from the human body. This department
will normally include the following sections:·Histopathology: The majority of specimens are received in formalin from
operating theaters, out-patient clinics, post-mortem rooms and general
HOSPITAL PLANNING AND PROJECT MANAGEMENT96 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 97
practitioners, but items may also arrive in a fresh state. Some of the latter may require examination as frozen sections. Specimens are examined and selected portions of large, or the whole of small specimens, are passed through automatic tissue processing machines, before embedding in paraffin wax or resin blocks. These blocks are cut into sections that are transferred on to slides, stained, protected by a cover slip and labeled. Medical staff will then examine the section microscopically and make a report. Tissues remaining after the specimen has been cut up are stored for at least 4 weeks after the section has been reported.
·Cytopathology: Cytopathology is the study of individual cells collected by scraping from the surface of an organ, from a secretion or excretion, or by needle aspiration from an organ or body cavity. A proportion of the specimens received may already be fixed on slides. Others will be in suspension in fluid and will need either to be spread directly or first centrifuged before they are mounted and processed for staining. Some specimens may require handling in a safety cabinet. Subsequently cytopathology staff examines the stained slides and a report is made. All slides are usually stored for many years.
Provision should be made for the following:
1. The reception of specimens; their examination and dissection; dictation of findings; and photographing of specimens. The tissue is processed using automated systems and embedded in paraffin wax. Some tissue requires resin processing and embedding. Space is required for storage of gross specimens for a variable time during and after processing and for mounting of prepared tissue for demonstration purposes.
2. The cutting of tissue sections from cold wax blocks. These are mounted on microscope slides, de-waxed and stained by automated or manual systems using routine or special techniques. Frozen section investigations, involving freezing of selected portions of unfixed tissue and cutting sections are required for some examinations of specimens from operating theaters and for some immunohistochemical techniques. These are then dried or fixed and stained. All stained slides are placed in trays for dispatch to the pathologist for microscope examination.
3. Special histopathology procedures, which include resin work comprising section cutting, staining and mounting; histochemistry techniques or immunochemistry; immuno-fluorescence; and crystallography where slides prepared in the general laboratory are treated with antisera and dyes prior to microscopic examination. In most, but not all cases, these techniques would be performed in teaching hospitals
rather than general hospitals.

4. Cytopathology work which includes a processing area where slides are prepared and a screening area where they are examined microscopically.
Microbiology Department
Medical microbiology is the study of microorganisms that cause human infections, and is dependent on the provision of suitable laboratory facilities for the isolation and identification of bacteria, viruses, fungi and parasites from clinical specimens. Samples such as blood, urine feces and swabs are examined by a combination of techniques, including microscopic examination and culture of organisms. Detection of antibodies in serum samples may be undertaken. Both manual and automated methods are in use.
RADIOLOGY & IMAGING SCIENCES
Diagnostic Imaging
In the last two decades, the pace of advancement in imaging technology has drastically accelerated. This is due to the development of digitized information technology—the recording of images via electronic rather than film media. The first development with widespread clinical applications was computerized axial tomography, or the CT scan.Developments in digital technology will continue, making imaging more accessible and cost-effective. There are various ways in which a signal is created; for example, images are created with the use of isotopes generated by a cyclotron in positron emission transmission. Magnetic resonance imaging (MRI) also uses digital imaging technology. Not only does this afford a better way of imaging soft tissue, which does not have to be made radio-opaque, it portends the development of spectroscopy techniques allowing chemical diagnosis of the body without taking specimens.
ContextImaging Facilities can be located in many places: the traditional hospital radiology department, the ambulatory care center, freestanding imaging centers. In smaller facilities, one department typically contains all modalities. In larger facilities, inpatient and outpatient modalities may be separated. For example, there may be a separate nuclear medicine department or MRI facility. In some instances, imaging modalities can be collocated with other diagnostic/treatment facilities to create healthcare centers of excellence (various technologies to focus on a specific organ or patient type), such as mammography and ultra-sonography in a women's center.Many modalities can also be provided through portable devices. This allows procedures to be performed at the point of care in a patient's bedroom, in an examination room, or in other treatment areas, such as the operating room.
Patient and work flow
HOSPITAL PLANNING AND PROJECT MANAGEMENT98 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 99
Patients may receive more than one procedure per visit, so it is important to quantify the number and the average duration of procedures a patient undergoes.Patients can arrive at an imaging facility from a number of sources. Wheelchair or stretcher-borne patients may come from inpatient units or other treatment areas, such as emergency. Ambulatory patients may arrive—scheduled or without appointments—at a reception desk. Typically, departments are configured to separate the flow of these two types of patients.Another key consideration in patient flow is the requirement for changing— that is, donning a hospital gown in preparation for a procedure. Historically, patients were separated by gender and waited, gowned, in waiting areas. More recent departmental designs provide individual dressing rooms adjacent to the procedure room, where patients can change and wait with greater privacy.The flow of patients through the department intersects with the process of image generation, interpretation, and results reporting. Historically, this was a sequential process that involved.
1. Exposing the film, using the appropriate modality,
2. Developing and checking the quality of the film image,
3. Repeating the exposure if necessary,
4. Viewing and interpretation by a radiologist,
5. Dictation and transcription of the interpretation and forwarding the report to the requesting physician or surgeon,
6. Filing both the film and the written report.
This process required the radiologist's location to be central to the patient and work flow in order to expedite the interpretation of the film. With the development of digitized image storage systems, this need has dwindled.
An Imaging Departments Patient and Work Flow diagram

Relationships with other departments
The imaging department interacts with a large number of other departments. Both outpatients and inpatients can be referred to Imaging for diagnostic studies; however, certain departments have stronger relationships with imaging. The emergency department, for example, is frequently positioned adjacent to imaging because of the large proportion of emergency patients requiring prompt radiological studies.Other special situations include casting facilities, women's diagnostic centers, and nuclear cardiology. Casting facilities, for resetting broken bones, may be placed in emergency departments or in specialty clinics. These facilities require radiography to ensure that broken bones have been set properly. This is usually achieved by providing radiographic capabilities in or adjacent to cast rooms. Otherwise, the casting area should be next to imaging for confirming the appropriateness of bone reduction.
Women's diagnostic centers require mammography, ultra-sonography, and bone densitometry to test for osteoporosis. Satellite imaging facilities are often incorporated within these centers. Alternatively, women's imaging may be incorporated as a "sub-department" of imaging, with a separate entrance and waiting area.
Nuclear cardiology is a unique crossover of services providing cardiologic diagnosis via imaging technology. The process involves introducing a radioactive medium into the vascular system. The effectiveness of the patient's cardiovascular system is then observed by monitoring the movement of the medium through the body while the patient is "stressed" through exercise. Because this service treats cardiology patients, the usual preference is to perform such studies in cardio-diagnostic areas (e.g., in a noninvasive cardiac laboratory).
An Imaging Departments Interrelationship Diagram
HOSPITAL PLANNING AND PROJECT MANAGEMENT100 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 101
Space summary
Radiography room Radiography is the simplest form of radiology, relying on direct exposure of film (or a digital image processor) with an X-ray-emitting device called a tube. This is most useful for creating images of X-ray absorbing tissues such as bones. A variation of radiography is tomography, which uses a rotating tube source and film carrier to create a two-dimensional image of a "slice" of the body. Although the equipment is slightly different, the room requirements and considerations are essentially the same for both techniques. All types of radiography rooms require lead-lined walls.
Recommended dimensions: 17 ft x 15 ft; making the room 20 ft x 16 ft renders it capable of conversion to a radiography/fluoroscopy room, should that later become desirable.
Ceiling height: 9 ft 6 in.
Key design considerations:
?Configure the space to allow a stretcher to be maneuvered into the room with minimum turns, typically by placing the axis of the X-ray table perpendicular to the wall with the door by which the patient will enter the room.
?Place the control console opposite the door with direct access to the vertical work core.
Special equipment: Table and tube, wall bucky (a device that holds film in a position during exposure), control console, sink and casework, and transformer and power cabinet (the latter may be placed outside the room).
Individual supporting spaces: None.
General fluoroscopy room
Fluoroscopy makes use of radio-opaque media that may be introduced into the body to create images of tissue that would not otherwise show up well on an X-ray. Because the radio-opaque material is typically barium introduced through the mouth or the rectum, it is important to have a toilet room directly accessible from the procedure room.Recommended dimensions: 20 ft x 16 ft Ceiling height: 9 ft 6 in. Key design considerations:
·Configure the space to allow a stretcher to be maneuvered into the room with minimum turns, typically by placing the axis of the X-ray table perpendicular to the wall with the door by which the patient will enter the room.

·Place the control console opposite the door with direct access to the work core.·These rooms often serve as radiograhy rooms as well.
·Attach the toilet room directly to the fluoroscopy room.
·Barium may be prepared in the procedure room or a nearby "kitchen.''
Special equipment: Fluoroscopic X-ray tube and table, image intensifier, cine or "spot" film camera, video monitor, wall bucky, control console, sink and casework, and transformer and power cabinet (the latter may be placed outside the room).
Individual supporting spaces: Patient toilet, barium preparation area.
Chest room
Chest X-rays typically constitute the largest single category of diagnostic procedures. They are often performed as a screening tool in conjunction with hospital admission or invasive procedures that will require general anesthesia and suppression of respiration. Many radiography or radiography/fluoroscopy rooms are equipped with wall buckies for chest imaging. However, because chest imaging can constitute a high proportion of this department's activity, a large department can justify dedicating a room or rooms solely to chest imaging. Because such rooms are designed specifically for this purpose, they are typically more operationally efficient than multipurpose rooms. Even greater effic? enci es can be achieved by incorporating film processing with equipment that automatically feeds dir? ctly into the film processor.
Recommended dimensions: 12 ft x 11 ft (widiout in-room processing), 16 ft x 14 ft (with in-room processing)
Ceiling height: 9ft 6in.
Key design considerations;
?To maximize efficiency, the equipment control console is typically incorporated directly into the room.
?The focal length of the tube assembly is fixed and must be maintained.
?If in-room processing is utilized, chemicals and equipment must be accommodated outside the patient area.
HOSPITAL PLANNING AND PROJECT MANAGEMENT102 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 103
In larger rooms, it is possible that a stretcher-borne patient will be X-rayed. Thus, the room should have a door large enough to accommodate a stretcher and be configured to allow maneuvering of the stretcher.
Special equipment: Tube assembly, changer and stand, console control and transformer in room without processing; the same equipment, plus auto film transport, auto film processor, silver recovery, and chemical manifold in room with processing.
Individual supporting spaces: None.
Mammography room
Mammography is a specific type of radiography that employs low-level radiation to identify tumoral calcifications and to characterize palpable lumps and unpalpable cysts or lumps in breast tissue. The mammography room is single-purpose room with a X-ray unit. Using a specialized type of mammography, the stereotactic room provides the radiologist with a three-dimensional view of the breast for localizing neoplasms for biopsy.
Recommended dimensions: 10 ft x 12 ft for an upright unit, 18 ft X 12 ft for a prone or stereotactic unit
Ceiling height: 8 ft
Key design considerations:
As this is a smaller room and the patient will be disrobed, reverse swinging doors and/or cuutains are used to prevent exposure of the patient.
Special equipment: Mammography unit, film illuminators, and sink in a mammography room; stereo-tactic biopsy table, operators console and digitizer in a stereo-tactic room.
Individual supporting spaces: None.
Ultrasound roomUltrasound or sonography operates on the principles of sonar and records size and shape by tracking reflected sound waves. Typically, a hand-held transducer emits regular pulses of high-frequency sound and translates the received "echoes" into images. Because tissue density affects sound reflectivity, the returned sound wave's amplitude allows graphic depiction of different tissues. This procedure is especially beneficial when the use of ionizing rays could be harmful to tissue, such as when a fetus is present.
Recommended dimensions: 11 ft X 14 ft

Ceiling height: 8 ft
Key design considerations: Because this is a smaller room and the patient may be disrobed, reverse swinging doors and/or curtains are used to prevent exposure of the patient.
Special equipment: Ultrasound unit (console typically placed to the patient's right side), stretcher, film illuminators.Individual supporting spaces: None
CT scanning room A computed tomography (CT) room provides an X-ray source that rotates rapidly around a patient, generating digital data.
Recommended dimensions: 16 ft x 19 ft for a procedure room, 10 ft x 12 ft for a control room, and 7 ft X 10 ft for an equipment room.
Ceiling height: 9 ft 6 in.
Key desig? considerations: The patient access door should be positioned to minimize stretcher turning because of the length of the equipment. At the same time, the view from the control room of the patient on the table while positioned in the opening of the unit must be at least partially preserved. At times, a video camera is used to supplement this capability.
Special equipment: CT gantry and table in the procedure room. The control room includes operator's console, video monitor, injector control, laser imager, and physician's viewing or diagnostic station. (The last two items may be placed remotely in a multiunit suite.) An equipment room houses the power and computer equipment.
Individual supporting spaces: Control and equipment rooms. These may serve more than one procedure room.
MRI scanning room
Magnetic resonance imaging (MRI) is performed by placing the patient in a powerful magnetic field that aligns the magnetic spin of atomic nuclei. Radio frequency energy is introduced, which disturbs the alignment of the nuclei. Different atoms respond at different radio frequencies, thus providing a distinction between tissue types. This powerful tool does not utilize ionizing rays and can create detailed two-and three-dimensional images of both hard and soft tissue.
HOSPITAL PLANNING AND PROJECT MANAGEMENT104 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 105
Recommended dimensions: Varies with strength of magnet; generally, about 20 ft x 26 ft for procedure room with a mid-strength magnet; along with a 10 ft X 12 ft control room and an 8 ft x 18 ft adjacent equipment/computer room. With lower-strength magnets, the room can be as small as 12ftx 16 ft with a 9 ft x 12ft equipment room and the control station in the open. (Refer to manufacturer's specifications for specific model.)
Ceiling height: Varies.
Key design considerations:
·The MRI magnet creates a field whose strength diminishes with distance. Magnetic field strength is expressed in units of measure called gauss. More recent generations of MRI units contain the 5-gauss line within the procedure room itself.
·As MRI's use radio frequencies to generate images, they are susceptible to electromagnetic interference from outside sources. To shield the room it is often wrapped with a copper fabric.
·Because the patient is placed into a unit approximately 8 ft in length and 2'/2 ft in diameter, claustrophobia can be a problem. New-generation magnets have mitigated this problem with ultra-low field strength magnets designed with open architecture. Still, procedure room interior design should take into consideration exterior lighting (or the implication of it) and other devices to address this issue.
Special equipment: MRI unit, patient couch, and coil storage in procedure room. Control room includes operators console and video monitor. Equipment room houses the power and computer equipment.
Individual supporting spaces: Control and equipment rooms. These may serve more than one procedure room.
Nuclear medicine room
Unlike radiography, which transmits radiation in the form of X-rays, nuclear medicine introduces a low-strength, short-lived, radiation-emitting isotope into the body. The emissions are captured by a camera and translated into Images. By introducing the isotope or radio-pharmaceutical into specific tissues and organs, radiologists can capture images that would otherwise be unattainable. A recently developed type of nuclear medicine camera—single photon emission computed tomography, or SPECT—has gained wide acceptance and application. It combines a nuclear medicine or gamma camera with digital image acquisition and interpretation capabilities to generate tomographic portrayals of blood flow to the brain and heart.

Recommended dimensions: 18 ft X 16 ft for a single camera room. Because nuclear medicine does not involve the use of X-rays, multiple cameras may be placed in a single room with adequate space.
Ceiling height: 9 ft
Key design considerations:
?Because nuclear medicine involves the use of radioactive materials, special provisions must be made for their containment and disposal. Most of these are injectable substances. However, some are gaseous pharmaceuticals, such as xenon gas for ventilation studies, which must be specially contained and exhausted.
Special equipment: Control console, computer workstation, collimator, collimator stand, whole body scintillation camera and table, and xenon delivery system.
Individual supporting spaces:
?A hot lab where radiopharmaceuticals are prepared, equipped with cabinets and work counter, lead-lined containers for storing and working with radioactive substances, lead-lined refrigerator, 100 percent exhaust radioisotope hood, and approved system for radioactive waste collection and disposal.
?Dose room, where patients are injected with radio pharmaceuticals. The inclusion of this room enhances procedure room productivity.
Positron emission tomography scanning room
In the positron emission tomography (PET) scanning room, physicians introduce radioisotopes by injection or inhalation. The isotope attaches to the body's own molecules, becoming a tracer as it moves throughout the body. Typically, the isotope is very short-lived and must be generated on-site with a cyclotron. This makes PET an expensive, but effective, diagnostic tool.Recommended dimensions: 15 ft x 20 ft for scanner room alone
Ceiling height: 10 ft
HOSPITAL PLANNING AND PROJECT MANAGEMENT106 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 107
Key design considerations:
?Ideally, the scanning room is placed adjacent to the radiochemistry lab, which itself must be adjacent the cyclotron. When this is not possible, a pneumatic tube system can be used to deliver the radiopharmaceutical to the clinical lab.
Special equipment: Scanner and patient couch, computer. Individual supporting spaces:
?Cyclotron room of 500 sq ft with 10 ft ceiling. Because of the weight of these units (approximately 120,000 lb), a grade level location should be sought.
?Radiochemistry lab of 600 sq ft where the actual pharmaceuticals are prepared. Ideally, it is located adjacent to the cyclotron room.
?A control room, where computer equipment for data acquisition and processing is housed.
?Patient preparation rooms with stretchers or chairs.
Special radiography/fluoroscopy procedure rooms Special radiography/fluoroscopy procedures include techniques that employ radiographic or fluoroscopic imaging equipment for guidance during complex exploratory and interventional procedures.Although the procedures performed in these rooms may vary, they have in common the introduction of a catheter and the use of large and complex equipment, including one or two fluoroscopic C-arms. Because the introduction of a catheter invades the body, some minimally sterile techniques must be observed.
Recommended dimensions: 28 ft x 22 ft for the procedure room alone
Ceiling height: 10 ft Key design considerations:
?The equipment should be arranged to allow visibility of the patient's head from the control monitor.
?Many procedures occur while the patient is awake and acutely aware of his or her surroundings. Therefore, measures should be taken to create a soothing
environment.
?Because the procedures require a semi-sterile environment, extraneous traffic should be limited.

Special equipment:
Radiographic/fluoroscopic arm(s), one or two, depending on whether the unit has biplane capabilities; video monitors, patient table, injector, surgical lights and back tables, and catheter storage.
Individual supporting spaces:
?Control room 22 ft X 12 ft, containing control console, multi-format camera or laser imager, scrub sink, and storage cabinets.
?Equipment room 10 ft X 22 ft, housing electronics cabinets.
?Patient preparation and recovery area.
?Staff gowning and changing facilities.
Supporting spaces
The following list summarizes supporting spaces typically included in diagnostic imaging departments:
?Waiting/reception area
?Gowned waiting areas for departments
?Dressing areas for gowned waiting or individual procedure rooms
?Toilet rooms for patients
?Darkroom for processing conventional films
?Daylight processing area
?Digital image processing area« Light room/quality assurance area
HOSPITAL PLANNING AND PROJECT MANAGEMENT108 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 109
?
?Viewing/consultation areas " Film files area
?Clean supply room
?Soiled utility room
?Staff locker/lounge/toilets " Storage alcoves
Work core design
Historically, films have moved from the procedure rooms to a processing, checking, and assembly area that serves several rooms. Although conventional film processing is less prevalent, this "work core" design is still one of the most staff-efficient configurations for a department. Typically, procedure rooms encircle a work core, with staff access from within the core and patient access from the perimeter.
In larger departments, like modalities are grouped around these cores to create pods or clusters. For example, radiography and radiography/fluoroscopy rooms are typically grouped.
Mammography and ultrasound may be grouped to serve women patients. Most departments are made up of groups of clusters aggregated around common or complementary modalities.
Department organization
The pods or clusters organized around work cores are the clinical heart of the department. Typically, they are interposed between the public access areas— reception and waiting—and the staff areas—personnel facilities, storage and utility rooms, radiologist offices, and reading areas. It is important to organize the department to allow future expansion in key corridors. If any spaces are placed in the path of this expansion, they should be "soft" or easily relocated areas.
Departmental organization must recognize the potential use of mobile technology. This usually requires providing a sub-waiting area with access to the trailer in which the mobile device is contained. Depending on the climate, access may be via a covered, open-air, or pneumatically enclosed structure.
Interior design considerations An imaging department requires high-technology equipment for diagnosing and treating individuals who may already be in a heightened
Image reading or interpretation area

state of anxiety. Thus, it is most important to create environments that are friendly and non-threatening. In addition to the appropriate furniture, fabrics, and colors, positive distractions may be included, such as artwork, views to the outdoors, and aquariums, to relieve stress and anxiety.
Lighting is also used to create a more soothing environment. Particularly important is the use of reflected lighting in areas where patients will be lying on their backs on stretchers or procedure tables.
Trends
Imaging is clearly one of the areas most affected by developing technology, particularly digitally based equipment.
Special Diagnostic Departments
Functional overview
Special diagnostics services typically include noninvasive testing of the human body's cardiovascular or neurological performance. The tests principally use electronic, sonographic, or scintillation counter technology to monitor the body's anatomy or physiological activity. These procedures produce measurements that are recorded over time in hard copy or digital storage media for physician review and reference. Most measurements occur over periods of 5 to 45 minutes, although durations of 24 hours are useful in some studies.
Noninvasive diagnostic testing of the cardiovascular systems includes the following:
Electrocardiograph)/ (ECG).
Observation of cardiac performance through electronic physiological monitoring.
Echocardiography (Echo ECG)-Observation of cardiac performance through Doppler ultra-sonography monitoring coupled with physiological monitoring. Transthoracic echocardiography is the basic study, and transesophageal echocardiography (TEE) is a common procedure using the same technology.
Exercise stress testing. Observation of cardiac performance through physiological monitoring while the patient is subjected to varying levels of exercise demand by treadmill or exercycle. Tilt tables may also be provided in this area for identifying reflex-induced problems.
HOSPITAL PLANNING AND PROJECT MANAGEMENT110 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 111
Nuclear scans. Observation of cardiovascular performance through physiological monitoring and gamma camera or SPECT (single photon emission computerized tomography) camera imaging of absorbed substances tagged with radioactive isotopes. Patients are typically subjected to varying levels of exercise demand via treadmill or exercycle during these studies. Nuclear scans combined with computerized tomography, known as PET scanning (positron emission tomography), are also useful but remain cost-prohibitive in most cases. Thus, this technology is generally found only in teaching institutions to date.
Holter monitoring. An ambulatory ECG recorded continuously over a 24-hour period via portable magnetic tape media to monitor electro-physiological data related to cardiac behavior and performance.
Pacemaker verification. Periodic and routine testing of pacemaker devices inserted to assist in regularizing the behavior of the heart.
?Peripheral vascular studies (PV). Noninvasive testing of the arteries, veins, and lymphatic system in the body extremities, using Doppler ultra-sonography.
Noninvasive diagnostic testing of the neurological system utilizes the following studies:
Electroencephalography (EEC).
Observation of brain activity through electronic physiological monitoring.
Sleep studies. Extended observation via camera and microphone, along with electronic physiological monitoring via EEG and EKG, through normal (8-hour) or short-term periods of sleep.
Service locations
Special diagnostic services are typically found in hospital settings within departments including cardiology, cardiovascular, cardiopulmonary, neuro-diagnostic, or electro-diagnostic services. These services are often centralized for inpatients and outpatients, although most inpatient ECG and EEG studies are conducted at the patient's bedside. Stress testing, echo ECG, peripheral vascular (PV) studies, and isotope scans are usually centralized owing to equipment requirements. Outpatient ECGs are completed mainly in physicians' offices, except when required for hospital preadmission testing records. Holter monitoring, pacemaker verification, and sleep studies are entirely

outpatient services.
Key activity factors
Planning for special diagnostics is based on projected work load volumes for inpatients and outpatients. The work loads are categorized by average procedure time and distribution between inpatient and outpatient volumes (see table above). The percentage of inpatient services is important, because many procedures are performed in the inpatient's room, thus reducing demand for diagnostic space within the central area of the service.
Key capacity determinants The variety of special diagnostic services requires many distinct procedure rooms to separate functionally incompatible activities, facilitate efficient work flow, and avoid excessive waiting time for patients. Some procedures, such as exercise stress testing, require strenuous physical activity by the patient. Doppler equipment used in echocardiography studies may generate noise. Risk of exposure to radioactive materials used in nuclear scans must be carefully controlled. Sleep and EEG studies require quiet areas without significant audio stimuli. The number of these rooms required is based on an 8 hours per day, 5 or 6 days per week (excluding holidays) schedule. The service is available on a 24-hour basis in the acute care setting, but principally for emergency needs after regular hours.
Patient and work flow Easy patient access to special diagnostic procedure rooms is paramount. These rooms are designed for outpatient convenience. Scheduled appointments dictate that adequate parking, clear ambulatory care entrance points, and simple way finding to the reception and waiting areas be available. Ambulatory patients should have direct access between the waiting area and procedure rooms without passing through staff or physician work areas. Easy transfer of inpatients, as required, to procedure rooms is also a factor in design. Clear access to inpatient areas that keeps patients or staff from passing through public spaces is preferable.
The technician staff requires workroom space close to the procedure areas, to Inpatient access to testing areas must be available without transport through public areas.
?Centralized staff work areas, where charting is performed outside testing rooms, provide for quick room turnaround. These work areas must be close to the procedure space to minimize travel distance.
?Physician reading areas must be nearby, but separated for EGG (hard-copy review), echo EKG and peripheral vascular (video monitor review), and EEG (hard copy review) functions.
HOSPITAL PLANNING AND PROJECT MANAGEMENT112 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 113
A central location is required for observation of multiple EEG, sleep lab, and multiple stress testing stations.
Trends
The healthcare technology industry will continue to explore alternative imaging and physiological testing modalities that are faster, less intrusive, and more reliable than currently used tools. Efforts to simplify the patient care process and to minimize the specialized expertise required of staff will stimulate the development of smaller, more portable, and more rapid measurement devices capable of use at the point of care. Where such devices still require centralized use because of cost or lack of portability, the establishment of quick diagnostic centers will absorb many of these services into convenient areas of care where common testing required for outpatients and preadmission testing of inpatients are co-located.
Oncology
Oncology therapy is treatment for cancer patients. Two common forms of cancer treatment are chemotherapy and radiation therapy. Chemotherapy is the intravenous admission of chemicals that attack cancer cells. Radiation therapy is the exposure of cancer cells to radiation. This radiation can be introduced to the body either through direct implantation—called brachytherapy—or by means of a beam of radiation from a linear accelerator or a screened radioactive source. Because radiation is not selective regarding the type of cells it kills, treatment planning for radiation therapy is quite complex. Both chemotherapy and radiation therapy require patient preparation and recovery. Most chemotherapy and radiation therapies are provided in an ambulatory care setting. Because of the difference in treatment modalities, the two therapies can be separated from each other. However, 30 percent of cancer treatment regimens involve both chemotherapy and radiation therapy.
Patient examination and treatment, as well as treatment planning, are key activity factors. The number of patients being treated and the type of healing environment needed determine space requirements. In radiation therapy, equipment requirements are extensive, as are requirements for shielding. In both chemotherapy and radiation therapy, proper staff supervision is critical to the efficient utilization of space.
Chemoterapy is administered in a non-technical area designed as patient-friendly space. The process is traumatic, stressful, and lengthy. The amount of space required depends on the total patient volume and type of desired treatment. Separate patient rooms and individual cubicles provide privacy, while open treatment bays encourage interaction with other patients. Creating a healing environment is the design goal for the chemotherapy facility.
?

Radiation therapy is performed in an area housing highly technical equipment, operated by highly specialized staff. The therapy is usually administered by linear accelerators. A shield must confine the dangerous beam of radiation created by the linear accelerators.
Flow of patients
The flow of oncology patients is very predictable, because patients undergoing either chemotherapy or radiation therapy are usually ambulatory and regularly scheduled. Facilities are needed for those patients who are weak and nauseous following treatments. Radiation therapy involves initial examination and consultation with the patient, treatment planning by the staff, treatment simulation using diagnostic x-rays to confirm the treatment and then the radiation treatment. Both therapies usually consist of more than one treatment.
Oncology therapy has few relationships with other departments because most cancer patients are ambulatory. A key factor is direct exterior access to chemotherapy and radiation therapy, respecting patient privacy. Oncology does need access to emergency facilities, but not directly to the emergency department. Chemotherapy requires a connection to the pharmacy for preparations of administered chemicals.
Key spaces
The equipment and shielding requirements for radiation therapy are the most significant for any area in oncology. Linear accelerators aim and focus a beam of high-level radiation. To confine the effects of the beam to the treatment vault itself, substantial radiation shielding is required. Although lead and steel are highly effective shields, concrete is more commonly used because of its lower cost. Eighteen to 20 megavolt linear accelerators produce a beam that can be shielded by approximately 8 ft solid concrete.
To aim the beam, the linear accelerator must be capable of 360 degree rotation. In turn, a room with a 10 ft overhead clearance and a 360 degree shield along the sides requires a significant amount of floor area and building height. Because of the permanency of this kind of construction, careful planning for placement is imperative.
Typical room sizes for radiation therapy are as follows: Therapy vaults—high energy 600 sq ft Therapy vaults—low energy 500 sq ftControl areas 130 sq ftEquipment 100 sq ftEntry maze 140 sq ft
HOSPITAL PLANNING AND PROJECT MANAGEMENT114 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 115
Simulator 300 sq ftTreatment planning 200 sq ftDosimetrist's office 120 sq ftMold room 250 sq ftPatient toilets 60 sq ftSub-waiting areas 20 sq ft eachFamily waiting areas 18 sq ft each
Brachytherapy is the implantation of a radioactive source in or near the site of acancerous mass. Implantation can be implemented surgically or by catheter. A patient must be monitored during therapy, usually in a patient room that is specifically shielded to prevent exposure to other patients.
Typical room areas for chemotherapy are as follows:
Open treatment bays 60 sq ftTreatment cubicles 60—80 sq ftTreatment groups 100-150 sq ftNurses' station 150+ sq ftPatient toilets 50-60 sq ft
(ADA compliant) Family waiting areas 15 sq ft per person Examination rooms 120 sq ft
Key design considerations
The stress and anxiety felt by many cancer patients can be eased somewhat if there is an opportunity for camaraderie with other patients in mutual support.
The design of the facilities for oncology therapy should provide opportunities for such interaction. Because of the effects of therapy on the physical appearance of patients, privacy and discretion are key design considerations.
The need for staff to supervise patients during and after their treatment influences all design solutions. Treatment planning is a staff function that is screened from patients physically and audibly. A hot lab houses radioactive substances that are prepared for brachytherapy implantation. The room must be shielded and located adjacent to the room where implantation takes place. Preparation in the pharmacy for chemotherapy requires laminar flow mixing hoods to ensure the sterility of the administered agents.
Physical Medicine and Rehabilitation

Physical medicine and rehabilitation (PM&R) offers services to individuals who are physically disadvantaged, with the purpose of returning them to their maximum physical capabilities. These services may include physical therapy, occupational therapy, speech pathology, audiology, and specialized programs; they may be supported with the development of orthotics and prosthetics to assist in their functioning. Physical medicine and rehabilitation are provided on an inpatient, outpatient, or in-home basis.
Physical therapy
Physical therapy concentrates on gross neuromuscular and skeletal activity, with emphasis on regaining movement, circulation, and coordination of body and limbs. Typical components of the physical therapy service are treatment areas, a gymnasium, and a hydrotherapy area. Treatment areas may be individual cubicles or rooms. A number of therapies can be administered in these areas, including thermal therapy, electrical stimulation, massage, and manipulation. A gymnasium is generally configured with equipment for several functions located in a common space, such as mats, platforms, gait training stairs, parallel bars, and weights, as well as other resistive equipment and orthotic and prosthetic training services. The gym can also serve as a multipurpose space, supporting other uses such as sports events (e.g., wheelchair basketball) and community activities. In long-term rehabilitation facilities, the physical therapy program may be expanded into recreational therapy for patients.
Hydrotherapy is a treatment with warm to hot circulating water in tanks. The tanks are used either for the extremities, such as the legs and arms, or for full-body submersion. Hubbard tanks, which are configured to allow each limb to be fully extended, are also used. The warm to hot water circulating around the body or parts of the body stimulates blood circulation, promoting healing and reduction of pain. Larger therapy pools allow patients to exercise while suspended in water, thus reducing the impact of body weight during therapy. The humidity of these areas should be carefully controlled through the mechanical ventilation system.
Occupational therapy
Occupational therapy focuses on optimizing a patients independence while concentrating on finer physical movements. Activities of daily living (ADL), vocational training, and, in some cases, a work-hardening program are used to rehabilitate the patient.
The activities of daily living are routine tasks that individuals are required to perform. The area provided for this therapy includes a mock bedroom, kitchen, and bathroom. These areas provide the patient with an opportunity to learn the basic essentials of cooking, hygiene, and dressing with the benefit of an attending therapist.
The vocational training area houses a variety of equipment, including word processors,
HOSPITAL PLANNING AND PROJECT MANAGEMENT116 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 117
computers, cash registers, and telephone switchboards, simulating a work environment. The area may also include wood and metal workshops. Some occupational therapy services include work-hardening programs, which simulate an industrial environment, providing both education and therapy for a more rigorous work setting. Patients learn to perform work tasks and to protect themselves from further injury. Because of the noise made by equipment, it is important to address acoustics in the vocational training area.
Speech pathology and audiologyA patient's injuries or disease may result in communication disabilities. These are most commonly related to cerebrovascular (stroke) and head trauma. The purpose of therapy is to assist a patient in regaining control or adapting to a specific communication disability, which may include cognitive retraining. Communication disabilities include problems with speech and/or hearing. Audiology is most effectively supported diagnostically by two-compartment sound-isolated booths. In the booths patients are accurately tested for hearing loss, as well as the effectiveness of prescribed hearing devices.
Specialized programs Many providers have specialized programs in physical medicine and rehabilitation. These may include a pain clinic, cardiac rehabilitation, sports medicine, and hand therapy. Specialized areas may be required for these programs. However, many are similar in configuration to the areas for the services already described.
Settings
Physical medicine and rehabilitation services may be housed in a variety of settings, including hospitals, ambulatory care centers, and comprehensive specialty rehabilitation facilities. Care is provided under several physician specialties such as physiatry, orthopedics, neurology, cardiology, and others. The specialty centers may include rehabilitation treatment for cerebrovascular/stroke, spinal cord injury, head trauma, amputation, developmental disabilities, neurological degeneration, complicated fractures, cardiac conditions, or genetic disorders.
Operational considerations The size, internal relationships, configuration, and location of physical medicine and rehabilitation services are dependent on their work loads. Work load is determined by the number of inpatient or outpatient visits and treatments received within the operating hours of the services. Capacity is determined by such factors as the number of treatment cubicles, mats, therapy positions or stations, cognitive retaining rooms, and hydrotherapy tanks.
Patient and work flows shape the design of the PM&R area. Because of their various

disabilities, patients require convenient access to the services. In hospitals, the PM&R services are often located near the elevators at grade. This location is easily reached by inpatients and outpatients. Patients must be visible and accessible to staff. Satellite therapy areas may be located on nursing units for the convenience of less mobile patients. Many initial therapies occur in the patient's room.
PM&R services are related to other departments and services within a hospital. The most common relationships are with nursing units, such as orthopedic, cardiac, neurological, and other units. These services should also be accessible to outpatient entrances, with a dedicated entrance near convenient parking.
Support areas
The following are suggested support areas for PM&R:
?Lounge, personal lockers, toilet, and, possibly, a place to shower
?Meeting space for continued education and training
?Clean workroom, soiled utility, housekeeping, equipment storage, wheelchair and stretcher storage Larger facilities may also have an orthotics and prosthetics department. The department supplies, manufactures, and fits devices to assist patients' mobility and dexterity. These devices may include artificial limbs, assistive appliances, braces, crutches, and wheelchairs.
Space needs
According to the AIA 1996-1997 Guidelines for Design and Construction of Hospital and Health Care Facilities, typical physical medicine and rehabilitation services include five major areas:
?Administrative/work?Physical therapy?Occupational therapy?Speech pathology/audiology
?Support/staff
The following are areas typically required in the department:
?Reception and waiting (outpatient or staging of inpatients)
HOSPITAL PLANNING AND PROJECT MANAGEMENT118 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 119
?
?Patient toilet
?Wheelchair and stretcher storage
?Housekeeping closet
?Access to conference room
?Physical therapy
Individual therapy treatment areas with a minimum of 70 sq ft
Hand washing area
Exercise area (gym)
Clean linen storage
Equipment and supply storage
Soiled utility
Patient dressing areas, showers, and lockers (if required)
Hydrotherapy (when required)
?Occupational therapy
Patient work areas Hand washing area
Equipment and supply storage
Activities of daily living areas
? Speech pathology and audiology
Evaluation and treatment area
Administrative office and clerical space

Space for equipment and storage
?Orthotics and prosthetics
Work space
Space for fitting and evaluating
Space for equipment, supplies, and storage
These areas should be planned in a manner that encourages quality patient care, appropriate space for the proposed work load, and staff efficiency.
Special planning and design considerations
An overriding issue in PM&R is accessibility for patients with restricted mobility. In treatment areas, space must accommodate not only the patient and therapist but also the transportation modalities used to get the patient to therapy— such as a stretcher, wheelchair, or walker. Slip-resistant floor surfaces should have no tripping hazards and must accept wheelchairs and walking accessories.
Heating, ventilation, and air-conditioning systems should address several demands in the PM&R department. Humidity control is required in hydro-therapy and therapy pool areas. Orthotics and prosthetic manufacturing areas require special consideration of acoustical needs and control of fumes and dust.
Trends
Physical medicine and rehabilitation
services will be performed more often in outpatient and home care settings. These services will also be more and more decentralized within the community for convenience and ease of access. There is a trend toward the development of specialty centers of excellence for certain rehabilitation services such as those provided for spinal cord injuries, head trauma, stroke, and development rehabilitation. However, physical medicine and rehabilitation will continue to play an important role in the continuity of care—from inpatient to home care—in both medical and surgical specialties.
Renal Dialysis
Renal dialysis is the simulation of kidney functions for patients in chronic end-stage renal failure or temporary acute kidney failure. The simulation may be performed by two primary methods— hemodialysis or peritoneal dialysis. Hemodialysis is the filtering of an individual's blood to remove the uremic toxins and water typically
HOSPITAL PLANNING AND PROJECT MANAGEMENT120 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 121
removed by the kidneys. The process is implemented by a machine connected to the body's veins through large-bore needles and plastic tubes. These needles may be placed in surgically created fistulas or artificial implants. These are more commonly located in the arm, but the needles may also be placed in the neck or leg regions. The blood is circulated through a membrane filter whereby toxins and water are removed. Alarms on the machine monitor biophysical parameters such as the patients body temperature, relative blood volume, and hematocrit and electrolyte balances. This procedure may be required three days a week and varies in duration from two to four hours. Home dialysis with this method is possible, but limited by cost and caregiver availability.
Peritoneal dialysis is the removal of uremic toxins and water from the body through the peritoneal cavity around the abdominal organs. This is performed by perfusing specific warm, sterile chemical solutions through the cavity. An artificial opening is surgically created in the abdominal wall for this procedure. Dialysis by this method is typically performed several times daily, depending on the size and weight of the patient— which may also limit its practicality. Peritoneal dialysis is considered a less efficient method than hemodialysis; however, it is the most common home dialysis treatment.
Settings
Renal dialysis may occur in a variety of settings, including hospitals, physician's offices, and freestanding dialysis centers, as well as in the home. These settings vary in size and configuration, depending on types of inpatients and outpatients served.
Operational considerations
A renal dialysis unit or center is designed around several operational considerations. The number of patients treated, the hours and frequency of treatment required for patients, and the hours of operation are all items for discussion. Capacity is determined by the number of dialysis positions.
Patient and work flow through a dialysis unit includes several components. The patient is weighed upon arrival. Following this evaluation, the hemodialysis patient is connected to the dialysis machine. The machine is set to operate for a set amount of time. The patient is disconnected from the machine and reweighed, and fluid loss is recorded. An inpatient may return to his or her room and an outpatient may return home. Portable machines are becoming more popular in hospitals, allowing patients to remain in their rooms for treatment.
The treatment area can be open or partially enclosed, yet permitting visibility for 1nursing and technical staff. The nurses station is centrally located, allowing visual
observation of all patient treatment stations. Treatment positions are at least 80 sq ft (7.43 sq m) and at least 4 ft from other positions. Privacy should be addressed in the

layout and design of the treatment position. Isolation positions may also be required for infectious cases. Tables may be placed beside recliners and stretchers as a convenience for the patients.
When a facility for renal dialysis is combined with the physician's office, the nephrologist may schedule an office visit at the same time a renal dialysis procedure is scheduled. The appointment may include not only a visit with the physician, but also a visit with a dietitian or social worker to address specific issues regarding nutrition or personal resources.
Inpatient renal dialysis services should be closely related to inpatient units for convenience and ease of access. After undergoing a renal dialysis procedure, a patient may be weak and faint. Therefore, outpatient services should have immediate access to the parking lot.
Support areas
A number of support areas are provided for the dialysis patient during treatment:
?Nurses' station
?Medication preparation and dispensing station
?Examination room of at least 100 sq ft (9.29 sq m) If home training is provided, a separate room of 120 sq ft
(11.15 sq m) should be available.
?Clean workroom
?Soiled workroom
?Separate reprocessing area
?Nourishment stations
?Housekeeping closet
?General storage and storage alcoves
HOSPITAL PLANNING AND PROJECT MANAGEMENT122 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 3
?
?Patient toilet and personal storage
?Appropriate staff facilities
?In an outpatient setting, a waiting area and supporting offices
Space needs
According to the AIA 1996-1997 Guidelines for Design and Construction of Hospital and Health Care Facilities, a typical renal dialysis service should include the following:
Waiting and reception (in outpatient facilities)
Treatment positions
Isolation treatment position (if required by the program)
Nurses' station
Medication station (if required)
Home training room (if required)
Examination room
Clean workroom and linen storage
Soiled workroom
Reprocessing room (if required)
Nourishment station
Housekeeping closet
Equipment repair (if required)
Storage
Central batch delivery system and water treatment
Water treatment and dialysis preparation

Patient toilet
Patients' personal storage space
Supporting offices and staff facilities (if required)
Special planning and design considerations
It is important for the designer of a renal dialysis service to be sensitive to the patient's situation during treatment. Typically, a patient is in a recliner or on a stretcher, which makes lighting and ceiling treatments important. During the actual connection to the machine, adequate lighting is required. After the connection, a more indirect light is desirable. Many centers provide shared television sets for patients' entertainment. However, it is difficult to find television programs that interest everyone. Thus, individual television sets are preferable. Acoustical considerations are also important, especially for patients who prefer to sleep during treatment.
Trends
End-stage renal failure is affecting a larger percentage of patients because of the continued aging of our population. As a result, the growth of renal dialysis centers will continue. Outpatient centers are being developed by major providers nationally. The trend toward consolidation of major national and international dialysis providers is expected to continue. Currently, close to 50 percent of patients in the United States receive treatments from ten major national providers. Home dialysis is also expected to grow as the procedures continue to be simplified by new machines.
Respiratory Care
Respiratory care is the care of the respiratory system—primarily the lungs. There are two distinct areas of activity. The first is inhalation therapy, involving a variety of techniques ranging from simple oxygen supplementation to assisted breathing with the use of respirators or ventilators. Diagnosis, by calculating the respiratory system's effectiveness through pulmonary function studies and arterial blood gas analyses, is the second activity.
Context
Although the two activities have traditionally been grouped together, they are very different. Inhalation therapy is typically rendered at the patient's location—on nursing units, in outpatient treatment areas and physicians' offices, and even in the home. Increasingly, inhalation therapy is being decentralized to the hospital nursing areas such
HOSPITAL PLANNING AND PROJECT MANAGEMENT4 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 125
as critical care, pulmonary units, and neonatal units, which require its support. In many cases, inhalation therapists are integrated into nursing teams or nurses are cross-trained as inhalation therapists. The study of pulmonary function has remained a discrete activity, requiring specific equipment for diagnosis of pulmonary capacity and status, It may constitute a single department or be combined with other diagnostic activities in a multifunction diagnostic center within a hospital or ambulatory care facility.
Operational considerations
Activities and capacities The key activity factor or work load measure for inhalation therapy is number of procedures or hours of therapy. However, because these procedures occur outside the department—rather than in a procedure room—the key capacity determinants are the number of therapists and pieces of equipment. The key activity factor or work load measure for pulmonary function is the procedure. The key capacity factor is the number of procedure rooms.
Patient and work flow For pulmonary function testing, patient and work flow is similar to that of other diagnostic departments. The patient arrives, checks in, waits briefly, undergoes the procedure, and departs. The results of the testing are recorded, interpreted, and filed.
For inhalation therapy, the process is more complicated. As noted earlier, the therapy is typically rendered at the patient's location, with staff and equipment coming to the patient. However, following the procedure or treatment, the therapist must record observations on the patient. Traditionally, this was done within the department at charting positions. With the development of computerized records and specialized hand-held devices for recording inhalation therapy activity, this occurs on the nursing unit or at the point of care.
Another necessary process is the returning of equipment to a ready-to-use this trend can be expected to continue, separating this activity from pulmonary function testing.
Biohazard waste disposal Because inhalation therapy equipment may acquire infectious materials during the treatment process, care must be taken in disposing of these components. Containment and disposal of such waste is coordinated with the institution's overall biohazard waste disposal system.
Trends
With continuing pressure for cost containment, inhalation therapy services will more often be rendered in the home, where they are least costly. This trend is due to the development of smaller, simpler, and less expensive equipment.

SUPPORT SERVICES IN A HOSPITAL
CHAPTER 9
FOOD SERVICE DEPARTMENT
Suitable food well cooked and presented is an important part of the patients' treatment. Hospitals have long recognized the public relations value of the food service department. Unfortunately, criticism of the food is one of the most frequently heard complaints in any hospital. The food service department is responsible for all activities involving food, nutrition and beverages. The department's primary function is to provide nutrition and dietetic care to both inpatients and outpatients. Ancillary services include the operation of dining facilities for employees, visitors and physicians, catering and vending services, meal service for childcare centers and satellite facilities, and providing education in nutrition for all campus facilities, clinics, and long term care units.
Economics and convenience dictate the setting for the food services department. Ambulatory care centers, long- and short-term facilities, hospitals and surgical day clinics may all include an in-house food service department. The size and complexity of the operations are contingent on cost. A food service may also be operated as a satellite from a remote or centralized facility, although such operations have unique equipment and procedural requirements.
The departments work load hinges upon the number of meals served; operational factors such as food production methods, menu selection, staffing, and hours of operation play a key role. Capacity determinants may include food production methods, the size of production equipment, dry/refrigerated storage space, and the number of dining rooms, floor pantries, and warming kitchens.
HOSPITAL PLANNING AND PROJECT MANAGEMENT126 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 127
Work flow also affects an operations work load and capacity. Cross-traffic, double handling of good, and poor controls impact costs, efficiencies and food quality. Generally, products should flow as follows:
1. Receiving area
2. Prep area
3. Cooking line
4. Finished product assembly
5. Tray assembly
6. Dish washing
To ensure an optimal work flow and efficient service, the food service department and supporting spaces must adhere to particular adjacency requirements, as follows:
Receiving area. Locate near the loading and unloading dock for quick, safe food receiving.
Kitchen. Locate near the servery, conference/meeting rooms, service elevator to patients rooms, and auxiliary services, such as vending and catering.
Floor pantries. Locate near the service elevator core.
Vending. Locate next to the employee/visitor's dining facility, to accommodate late service, and at other strategic points throughout the facility.
Physician's dining. Locate next to the servery and dining room.
Employee/visitor's dining. Locate adjacent to the kitchen and food production area. The seating area should be placed next to the servery, providing easy access to foot traffic. Guest's need quick access to the visitor's parking lot.
Offices. Locate offices for management and supervisors near the appropriate production areas to foster communication with line workers.
Several methods are in use for delivery of meals from kitchen to wards. They differ in the method of processing, the palatability, the means of transport and the amount of labor that is necessary. Food may be transported to each ward in a bulk container by
heated trolley and served on to plate by the ward staff. This method has for a long time been the normal method and is simple and effective; it allows for immediate adjustments in the quantity given to individual patients but is relatively labor intensive in the wards. More recent methods are for individual meals to be portioned and plated up in the kitchen or served there on to insulated and compartmented trays, and delivered complete by trolley or conveyor. Alternatively and more rarely food may be cooked centrally, then frozen, and finally reheated in the ward kitchen, or even prepared centrally and cooked in the ward kitchen.
There is an increasing use of bulk frozen foods, with consequent implications on the storage requirements, and also of the bulk purchase of ready-made frozen meals from commercial sources. The catering may be run by the hospital or contracted out to external organizations. The different methods are reflected in the size, equipment and planning of both central and ward kitchens. The washing up of crockery and utensils has in the past done in ward kitchens. This is now usually centralized in the main kitchens, with the advantages of more efficient steam sterilization, less work for the ward staff and less noise in the ward itself.
A kitchen in the basement is certain to have a deleterious effect on the quality of food and efficiency of the department. It is likely to be dingy, dark and poorly ventilated. A ground floor location is preferable, and is also convenient for delivery of supplies. The storage area should be in close proximity to the unloading dock. Easy access to the vertical transportation system serving in-patient units is important to facilitate delivery of patient meals and return of used trays and utensils.
Delivering safe, high-quality food is paramount to the dietary services department. Efficient, cost-effective, and safe food production is based on a continuous system, with specific methods for raw product flow, preparation, cooking, assembly and dispensing. To prevent cross-contamination, clean and soiled areas and products must be segregated. These functions require adequate space and a designated flow pattern.
Cross-contamination must also be addressed in the receiving area. Boxes and containers may contain living organisms and so must not be directly loaded into the production kitchen holding coolers. Sufficient space is needed for receiving, weighing, and storing products to ensure product safety, strict inventory controls, and the proper rotation of goods.
The design and physical facilities of the food service department have an important bearing on the standard of food service, labor costs and the morale of the employees. For example, storage rooms far removed from the work area, poor arrangement of the preparation and production area for work flow, and long traveling distance for prepared food lower the level of efficiency and increase unnecessary steps for employees resulting in increased costs. In the general layout, the most important factor to be borne
HOSPITAL PLANNING AND PROJECT MANAGEMENT128 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 129
in mind is the logical workflow that is, receiving supplies, storing and refrigerating them, preparing and serving food, returning trays and washing dishes. The space and facilities should be adequate.
For decades, a simple concept dominated cafeteria service: recreate an army mess hall, with a long line of serving stations supported by an oversized kitchen or commissary. The demands of younger patients, staff, and visitors accustomed to a variety of dining options and the increasing need to find new revenue streams have spurred more flexible, innovative designs.
One of the latest developments is the food court and market designs, similar to those found in high-end food outlets and shopping malls. Employees, visitors and outpatients are able to move freely through food displays or boutiques, which are either self-service or staffed. The atmosphere promotes social activity and helps relieve stress. The variety of food offerings also satisfies more discriminating customers.
On the production side, new technologies and equipment have allowed kitchens to consolidate functions. These advances have enabled healthcare facilities to prepare products for inventory, rather than for immediate consumption, capitalizing on economies of scale.
CENTRAL STERILE PROCESSING
A hospital consumes a large quantity of new material that needs sterilization before use. It also processes other material that has to be cleaned and sterilized before it can be used again. Central Sterile Supply Department (CSSD) is a service whereby medical/surgical supplies and equipment – both sterile and non-sterile – are cleaned, prepared, processed, stored and issued for patient care. Hospital acquired infection remains a serious problem in health care today. The purpose of a sterile services department is to concentrate the skill and the responsibility for the supply of sterile material and to reduce the risk of error.
The primary activities to be undertaken within the CSSD are:1. Cleaning and disinfecting processes for instruments, trays, utensils, containers and
other reprocessable items.
2. Preparing and packaging contents of trays and packs and where appropriate, single-use items and other materials as supplementary packs.
3. Sterilizing trays and packs and disinfecting those items acceptable for patient use in this condition.

4. Storing non-sterile materials components.
5. Storing goods processed in the department and purchased sterile goods.
6. Distributing processed and purchased goods to users.
Sterilization of instruments, operating packs, trays etc., is performed is performed by heating them with pressurized steam or by gas sterilization. Steam sterilization is called autoclaving. However, certain items such as rubber, plastic and delicate instruments cannot be autoclaved and so have to be sterilized by using ethylene oxide or similar gases. Gas sterilization requires certain safety precautions such as aeration prior to use and special exhaust ventilation. Under both systems, sterilization is performed on cleaned instruments wrapped in special linen.
The department receives clean material from a laundry and new material from manufacturers and suppliers. It also receives for re-use, dirty articles from within the hospital. Clean and dirty materials require separate delivery points, the clean one serving a bulk store for new materials such as towels and masks, and the dirty one serving a clean-up room where all re-usable goods including instruments and syringes are washed, cleaned and dried. Rubber gloves may require a separate glove room for treatment.
The department is divided into three zones to accomplish the functions of decontamination, assembly and sterile processing, and sterile storage and distribution. These zones include the following:
1. Decontamination zone
2. Assembly/sterilization zone
3. Storage and distribution zone
The work flow for central sterile processing is centered on the processing of soiled instruments through the four zones. A distinct separation must be maintained between the soiled and sterile areas. The technical staff works on either the soiled side or the sterile side and cannot cross from one side to the other.
Decontamination zone: Reusable equipment and soiled instruments and supplies are received from surgery, labor/delivery and other departmental areas for initial or gross cleaning. These items are cleaned and decontaminated by means of manual or mechanical processes and chemical disinfection. The exchange cart is cleaned in a pass-through cart washer and readied in the assembly zone to carry items back to the departments. Items of equipment used in this area include the following:
HOSPITAL PLANNING AND PROJECT MANAGEMENT130 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 131
Biohazardous waste management systems
Washer/Decontaminator – used to clean heat-tolerant items
Ultrasonic Washer – used to remove fine soil from surgical instruments after manual cleaning and before sterilization
Healthcare decontamination systems (pass-through washer sterilizers or tunnel washers) – used to sterilize instruments in perforated or mesh-bottom trays
Cart washers – used to clean carts and other transport vehicles
Assembly/sterilization zone: After the instruments have been cleaned and inspected, they are typically assembled into sets or trays, according to detailed instructions. Each set or tray is wrapped or packed in a non-woven textile pouch or a rigid package/container system for terminal, or final, sterilization. At that point, the sets are prepared for issue, storage or further processing. After assembly, the instruments receive final sterilization. The cleaned instruments are issued to the sterile storage area until issued. Equipment used most commonly in this zone includes the following:
High-pressure sterile processing systems (steam or electric)
Low-pressure sterile processing systems
ETO (Ethylene Oxide) gas sterilizer and aerators
ETO gas aerators
Chemical sterilization systems
Microwave sterilization systems
Storage and distribution zone: Following the sterilization process the instruments are stored in sterile storage or sent to the appropriate department. Other functions of this zone include case cart preparation and delivery; telephone or requisition order filling, and delivery of patient care equipment.
It is advisable to have one high-speed autoclave, preferably in the surgical suite, as a standby in the event of a CSSD breakdown. Flash sterilization is performed in the user departments, particularly the operating rooms, to re-sterilize the instruments needed

immediately or those that have been dropped accidentally. Flash sterilization is autoclaving an instrument when it is unwrapped.
The department should be in the hospital service zone to simplify the reception of goods. Proximity to the boiler room is an advantage if steam is raised there. Good communication routes to most of the other departments of the hospital are essential. However, it has a relationship primarily with the Surgical Suite, and can be placed next to it. It can also be located above or below the Surgical Suite. This requires elevators or dumbwaiters to provide direct access for both clean and soiled materials to and from surgery. In some facilities, central sterile processing is collocated with materials management.
The size of the central sterile processing area depends on the number of surgical and obstetrics cases treated in a given period and the amount (cubic volume) of sterile storage required. In addition the number of open heart and/or orthopedic cases treated in a given period must be considered. Key capacity determinants include the number and type of sterilization instruments, the exchange case cart distribution system, and instrument holding and equipment cleaning in the CSSD department.
The trend is for central sterile processing to move into total integration with surgery. This move is in response to physicians' continued concern regarding the handling of surgical instruments and the need for nurses to prepare the case trays for sterilization.
HOSPITAL PLANNING AND PROJECT MANAGEMENT132 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 133
THE PHARMACY
The pharmacy serves the whole hospital. It stores pharmaceutical products manufactured elsewhere and may also store dressings. It usually manufactures some sterile and non-sterile products in bulk and dispenses prescriptions, sometimes direct to outpatients. It supplies all wards and other departments, often on the basis of daily deliveries. For smaller hospitals, the function of the department may be restricted to storage and distribution. It is one of the few areas where large amounts of money are spent on purchases on a recurring basis. It is also one of the highest revenue generating centers.
As a department, it provides prescription medications, intravenous (IV) solutions, and investigational drugs for clinical research, as well as other related products for patients. There are three primary services of the hospital pharmacy:
1. Receipt and preparation of prescriptions
2. Dispensing
3. Clinical consulting
Pharmacists receive orders or prescriptions from physicians. These prescriptions are prepared and dispensed to the patient by the pharmacist. In a hospital setting, medications may be dispensed in a variety of ways. They may be prepared in a central or satellite pharmacy and delivered to the patient care unit for administration by a physician, nurse or other caregiver. Moreover, automated vending systems may be positioned as satellites in high-use areas such as critical care, emergency and similar locations. A vending system allows the caregiver to administer physician directed medication and drugs using pharmacy-pre-stocked products in a high-use area. Pharmacists are commonly encouraged to consult clinically with the patient on the administration of a medication. This assists the patient in learning the risks and possible effects of the medicine.
Because supervision of drugs is essential and security is of first importance, manufactured goods are sometimes received direct by the pharmacy rather than via the hospitals main stores. The basic workflow in the department is reception of goods, unpacking and checking, then storage either in a dressings store or a drug store, and finally dispensing and distribution. Some of the products (poisons and dangerous drugs) require special security measures. Others need refrigeration, and some flammable liquids may demand particular precautions against fire or explosion involving storage outside the building.

From the drugs store, goods pass to the dispensing section either direct or via a bulk preparation room. In the dispensary they are broken down into correct quantities and from there distributed to the hospital or collected direct at a counter on prescription by outpatients. In many of our Indian hospitals, inpatients too are required to buy their medicine directly from the pharmacy on a cash 'n' carry basis. In this case a separate in-patient pharmacy may be needed. Ancillary accommodation includes staff offices, a laboratory, and a suite for the manufacture of sterile products, comprising preparation room, wash-up, autoclaves and a room for inspection, labeling and storage.
An inpatient pharmacy (in the Western model) is typically located near material management functions for convenience in receiving bulk items. It can also be located near inpatient care units for dispensing medications or at a central location, such as near elevator banks. Outpatient dispensing is provided in the hospital for outpatients requiring discharge medications and prescriptions. Outpatient dispensing should be conveniently located for serving departing patients.
The pharmacy department should have secure access control. Entry points should be limited, if possible, to receiving and dispensing. Ideally, both entry points are under the pharmacist's visual control. Space should be available to allow separate workflows for the preparation of prescriptions and IV solutions. Dispensing and storage areas must be located near these two flow areas. The IV preparation area and the fume hood should be near the bulk storage area and IV dispensing. Satellite pharmacies are integral to critical care, surgery and other areas. Automated materials movement systems, such as pneumatic tube stations, are desirable and efficient; A 6 inch pneumatic tube system is ideal for moving larger items such as IV bags.
Space determinants include the kind of drug distribution system – either centralized or decentralized – as well as the workload generated by the patients. The patient work load may include both inpatient and outpatient demands.
Flexibility within the pharmacy is paramount, especially during a facility's growth and change. Modular casework provides the flexibility of configuration and layout that is desirable in any pharmacy. Lighting should be adequate for reading small labels and finding medications in banks of shelves. Fume hood, to provide a sterile work environment for the admixtures and IV preparations, should be provided. A pass-through window, required for walk-up medication dispensing, must be secured. Security locks at all entrances is necessary.
Pharmacists are becoming active in the clinical administration of prescription medications in the inpatient and outpatient settings. With this responsibility, pharmacists are more likely to support a decentralized service encouraging their availability to the patients. Staffing remains a critical issue in cost control; thus many facilities still prefer a single centralized pharmacy, augmented with automated
HOSPITAL PLANNING AND PROJECT MANAGEMENT134 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 135
pharmaceutical vending machines that are decentralized throughout the hospital.
Environmental and Linen Services
The environmental services department is responsible for maintaining a clean and sanitary environment in die hospital, including floors, carpeting, tile, drapery, windows, lights, vents, and upholstered items. This department is also responsible for furniture moves, conference and classroom setups, replacement of patient room furniture, and trash collection. Environmental services typically contracts with outside vendors or arranges with the maintenance department for pest control, waste removal, exterior window washing, furniture repairs, window coverings, and the purchasing of trash receptacles and mattresses.
The number of housekeeping rooms or closets is determined by the needs of the facility. A service sink or floor well with a drain is provided for mops and other cleaning equipment. Shelves or carts for the storage of cleaning chemicals and supplies are also required.
Linen services are typically included within environmental services for the collection and distribution of linens and scrubs throughout the hospital. Linen services are typically contracted with vendors. However, some hospitals still operate full laundry services. Linen is stored on shelves or carts. Clean linen storage may be located in clean workrooms or linen storage alcoves. Soiled linen can be collected in carts in corridor alcoves or transferred to soiled utility rooms for pickup.
SettingsHospital environmental and linen services serve the hospital and satellite facilities, including medical office buildings, ambulatory care facilities, and other related campuses.
Operational considerations:
The environmental and linen services department is staff-intensive and should be near loading dock, materials management, and engineering/maintenance services, as well as close to elevators. Larger carts may be circulated throughout the hospital for restocking housekeeping carts located throughout the facility. Carts can also be delivered to the central department for restocking. Housekeeping carts are usually kept in the various housekeeping closets throughout the hospital. Linen carts are located in appropriate areas and are restocked on a "par" level or exchanged for a newly stocked cart.
Space needs
According to the AIA 1996-1997 Guidelines far Design and Construction of Hospital and Health Care Facilities, the following areas are generally accepted as appropriate for environmental and linen services:

Environmental services
Housekeeping closets
Housekeeping storage and supplies
Bed and equipment storage
Administrative offices
Vendor meeting room
Linen services
Linen storage
Receiving, sorting, and holding area for soiled linen
Centralized clean linen storage
Soiled and clean linen cart storage
Hand washing in soiled linen storage areas
Service entrance protected from inclement weather
Laundry or minimum laundry processing room for emergencies
Storage for laundry supplies
Staff facilities
Special planning and design considerations
Hospital finishes, furniture, and accessories are designed to withstand the rigors of constant cleaning and sanitizing. Such measures help to maintain standards of cleanliness that support a healing environment.
Trends
Outsourcing environmental and linen services is a growing trend in hospitals.
HOSPITAL PLANNING AND PROJECT MANAGEMENT136 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 137
Engineering and Maintenance
The engineering and maintenance department is typically responsible for the entire physical plant and grounds of the hospital. Services include preventive maintenance, corrective maintenance, casualty prevention, minor construction, and construction administration. Work load and departmental needs are directly related to the scope of the facilities and the campus for which the department is responsible.
Settings
These services should be convenient and accessible to all areas of the facilities and the campus. Access to the dock area is necessary for building materials, supplies, and equipment. Enclosed access to all hospital departments and areas is also desirable. The department may be responsible for off-site facilities, such as ambulatory care centers and medical office buildings, as well as for the hospital and grounds.
Operational considerations
Engineering and maintenance services are integral to the day-to-day operation of the hospital. These services are responsible for keeping the facilities in proper working condition and helping them function effectively. Engineering is responsible for monitoring the mechanical, plumbing, heat, ventilation, air-conditioning {HVAC), and electrical systems, as well as preventive maintenance and repair. Supporting shop work areas, such as carpentry, electrical, plumbing, paint, welding, and HVAC, may be provided in appropriate areas of the hospital. They may also be located in a separate outbuilding for better acoustical and dust control. If such shops are located in an outbuilding, covered access or transportation to the dock area should be provided.
Space needs
According to the AIA 1996-1997 Guidelines for Design and Construction of Hospital and Health Care Facilities, components of engineering and maintenance services include the following:
Central Energy Plant
Medical Gas Park
Dock area
Administrative offices (plan room, computer-aided drafting and design [CADD] room, environmental controls room, etc.)

Appropriate shops (carpentry, electrical, plumbing, paint, welding, HVAC, etc.) Supply storage
Flammable storage
Biomedical workshop
External grounds maintenance equipment storage
Staff facilities
Special planning and design considerations
Engineering and maintenance services require appropriate electrical and mechanical systems for shop operations meeting all requirements of the Occupational Safety and Health Administration (OSHA). Specifically, dust control and the storage of flammable fluids must be addressed.
Safety and Security
Safety and security services within a hospital setting provide general security, guard patrols, preliminary investigations, fire prevention, control policies and training, disaster planning and training, and other measures for the general safety of staff, patients, and visitors. Other services include lost-and-found and patient assistance, and transportation by vehicle. The department operates 24 hours per day, seven days a week.
Settings
Safety and security has high visibility near entrances and parking areas. It is common to place this function close to the emergency entrance, inasmuch as this is a 24-hour entrance to the hospital. The service has relationships to employee health, infection control, engineering, and risk management.
Operational Considerations
This service typically includes a suite arrangement, one component of which is a command post. At the post, security guards monitor closed-circuit television cameras. A director's office is usually adjacent to the command post. Storage is required for lost-and-found and disaster planning equipment. More healthcare facilities are establishing car patrols on their campuses.
HOSPITAL PLANNING AND PROJECT MANAGEMENT138 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 139
Space needs
Typical safety and security services include the following:
Command post
Director's office
Security supervisor's cubicle
Storage (lost-and-found, disaster planning equipment)
Trends
Greater emphasis is being placed on safety and security at healthcare campuses because of a rising perception of more violence and criminal activity. This activity, experts say, is attracted by the 24-hour operation of a hospital.
Materials ManagementFunctional overview
Materials management is responsible for the acquisition, general storage, daily inventory, and restocking of most, if not all, of the consumable materials used within a facility. This service may be provided for several facilities within a healthcare system to increase efficiency of operations, reduce total space requirements, and maximize purchasing power. The following services are provided:
·Management of consumable goods such as medical-surgical supplies and administrative paper goods
·Receiving, breakdown, and stowage of supplies, in bulk cases and in units of issue
·Storage of special supplies (chemical reagents, X-ray film; stock intravenous [IV] solutions, flammable or other hazardous materials)
·Receiving and temporary holding of new equipment or furnishings
·Distribution and restocking of supplies to consumer units on a scheduled and on-call basis using pre-established (PAR) levels
·Inventory management to maintain supply and to secure optimal purchasing agreements for operational economy

·Administration and management of the facility's supply system in cooperation with the managers of consumer units
Responsibilities of the materials management director may include managing the central sterile processing service (reprocessing/sterilizing reusable Stems) and overseeing the linen service. Materials management service excludes food products, which are managed by the food service department. Also, this department usually relies on the clinical lab for storage of radioactive materials or special products, such as reagents, which require refrigerated storage.
Service locations
A general storage area is required in facilities of all types. If serving a network of 1
facilities, material management is often centralized at a "hub' facility, with management and distribution services provided to satellites. Demand for storage space and staff will be driven by the mix of services and volume of activity at each site. Each consuming unit in smaller facilities may itself manage material acquisition and storage. However, this service is typically centralized to achieve economies of scale and to minimize staffing requirements.
Key activity factors
Planning for this service is driven by the array of clinical services to be supported and the operational concept for the materials management program. The projected volumes of patient care services, types of general and specialty supplies required, relative proportion of inpatient versus outpatient care, and the administrative needs of the clinical services are components to be addressed in determining demand for materials management services. More important to space planning, however, is the frequency of deliveries and the type of supply system—external and internal—as well as the functional work flow intended for the service. These components make up the operational concept.
A materials management flow diagram
HOSPITAL PLANNING AND PROJECT MANAGEMENT140 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 141
Key capacity determinants
The extent of centralized versus decentralized storage affects capacity. Inherently, decentralized storage requires more space. Some decentralization is necessary in all healthcare facilities for enhanced productivity. Capacity is determined by the on-site supply reserve and delivery frequency to bulk stores and local storage rooms. Capacity is driven by the storage system: fixed shelving or high-density movable shelving, the storage system volume—height in particular— and the extent of compartmentalization (separate areas for specialty storage, or bulk carton storage versus broken lot "unit of issue" storage).
Work flow
In materials management, work flow begins at the receiving service dock. Bills of lading and product condition are checked in the receiving area. This area must contain space for weather-protected products and temporary holding. Weighing scales are located in this area, as is a clerical work space. The dock area must be raised, often with dock levelers "for receiving materials from tractor-trailer and bobtail trucks, and must have an apron at grade for smaller delivery vehicles.
Cartons of received supplies are moved directly into bulk storage areas on pallets or placed on heavy-duty shelving. Equipment and furniture are moved to a temporary holding space until they can be installed by engineering or environmental service staff. Hazardous or flammable supplies are stored in dedicated rooms. These rooms are often accessible directly from the dock to facilitate exterior access for vendors and to provide ventilated, safe storage outside the building.
j From the cartons, daily-replenished supplies are moved onto more accessible shelves for ease of restocking by unit of issue. The "distribution room" or "clean/sterile supply area" is the principal storage room from which carts are loaded to restock each consumer department in the facility. Depending on the inventory management system, before distribution each item is usually marked with a bar code label to facilitate tracking and billing.
Bulk stores also hold cartons of prepackaged consumable sterile goods used in surgery, labor/delivery, or other special procedures areas. These items are distributed daily to the central sterile processing (CSP) area. The supplies delivered to the clinical areas may include both consumable and reprocessed goods. For this reason, CSP is often adjacent to the distribution room of materials management to optimize material flow over minimum distances. A "break-out" room between the distribution room and CSP typically serves as a vestibule, where supplies are removed from cartons to shelves.
The replenishment system for consuming units is an important determinant of necessary space. There are two basic approaches—replenishment or use of exchange carts. A hybrid of the two is often employed. Pure replenishment requires a periodic inventory, by the materials management staff, of items consumed in each consumer area; the collection of those items from the centralized supply distribution room onto a cart; and
the delivery and restocking of those items in the cabinets or on carts in the consumer unit. These storage areas are typically identified as the clean supply or clean utility rooms of the consumer units.
The pure exchange cart system requires the periodic replacement of the supply cart in the consumer unit with a cart fully stocked to PAR level, and then the return of the partially used supply cart to the distribution room for inventory and restocking. A key difference between these systems is the redundant cart holding space needed in the distribution room in the exchange cart system. Today's computerized inventory systems facilitate instant information to support the replenishment approach.
Because of their value or special storage requirements, specialty goods, such as imaging film supplies, lab reagents, and cath lab catheters, may be stored entirely within the consumer department. These goods are received by materials management and moved in bulk directly to the consumer departments.
Relationships with other departments Materials management must be directly accessible from the exterior via a receiving dock area. In planning this department, its activities should be kept away from circulation routes for the public, ambulatory patients, and most staff traffic. However, easy access to all consumer departments for distribution is desirable. The routes of such access should be separate from public thoroughfares. Central sterile processing should be located nearby for expedience in daily restocking. For operational reasons—often driven by preferences of surgery managers and physicians—CSP may be separate from or integrated with surgery.
Key spaces
Key design considerations
The design of the materials management scales, 36 to 42 in. deep pallet or deep area should address the followingconsiderations:
?Direct dock access for receiving, with staging space for checking deliveries prior to storage or distribution
?Breakdown area for unit of issue stock, with convenient waste management pathways (box bailer or access to trash compactors)
?Capability to segregate flow of clean and dirty activities at the dock (complete separation is not necessary); ability to move trash, hazardous waste, and soiled linen to holding areas or transport vehicles without conflicting with clean incoming goods
?Clear and adequate circulation pathways for materials movement equipment such as forklifts
HOSPITAL PLANNING AND PROJECT MANAGEMENT142 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 143
?such as for flammable or hazardous substances and portable medical gas cylinders of various sizes.
Special equipment and furniture requirements
Special equipment requirements may include dock levelers, in-floor industrial carton storage, forklifts or pallet lifts, 24 in. deep shelving for unit of issue supply holding (in fixed or movable high-density storage systems), and replenishment or exchange carts {typically 24 by 60 in.).
Supporting spaces In addition to basic storage and distribution areas, materials management should include support areas:
?Staff lounge, lockers with showers and changing areas, and toilets
? Administrative offices
Special planning and design considerations
Special design considerations include the following:
?Service traffic must be separated from patient vehicle traffic.?Weather protection and environmental control should be available at the portal to the
receiving dock.?Life safety codes require rated enclosures for certain types of storage, as well as
minimum ceiling or sprinkler head clearance vertically above the top levels of stored materials
?A pneumatic tube station within the or distribution room should be provided.?Various other types of automated conveyance systems may be considered, but most
are typically too costly to justify. Often, 6 in pneumatic tube transport systems are effectively used for immediately needed items not in stock on the user unit, and a station for this system should be provided in the distribution area (unless provided in adjacent CSP).
TrendsThe centralization of materials management services will continue or increase, in order to serve greater numbers of facilities within a system. Various approaches and applications of "just in time" delivery of supplies will continue to minimize inventory and requirements for storage space in healthcare facilities. Automation of processes for inventory, ordering, and restocking will be increased in an effort to minimize staffing requirements for materials handling. Distribution of supplies to the points of care will continue to be an expedient way to maximize use of clinical human resources. In addition, new ideas on achieving care goals without increasing material management staff requirements will be explored.
Exterior access for selected materials storage in dedicated, code-compliant rooms,

THE HOSPITAL PROJECT TEAM
CHAPTER 10
In the conceptualization, design, construction and commissioning of any successfully run healthcare facility project, the services of some or all of the following types of consultants will be required:
1. Hospital Consultant
2. Consulting Architect / Architect
3. Municipal Architect / Local Architect
4. Structural Consultant / MEP (Mechanical, Electrical, Plumbing) Consultants
5. Construction Manager
6. Landscape Architect
7. Interior Design Consultant / Graphic Designer
8. Bio-Medical Engineer / Medical Equipment Consultant
In addition to these consultants, the design team would also include:
9. The Client / Client's Representative
10. Hospital Administrator / CEO of Proposed Facility
11. User Groups / Representatives of Users of the Proposed Facility
We thus have eleven individuals / consulting firms or groups of people who would constitute the Design Team.
Starting with the consultants, their fields of expertise and thus scope of services would be as follows:
HOSPITAL PLANNING AND PROJECT MANAGEMENT144 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 145
1) The Hospital Consultant
At the start of the project, the hospital consultant's role is to do a market survey and financial feasibility report to establish what should be the role of the proposed healthcare facility in the region it is to serve. The consultant's recommendations focus on the total operational future of the facility, including the service area market financial future, proposed medical specialties and bed strength. His most important function is to provide an independent professional opinion and plan based on an unbiased look at the total operation. This consultant is usually retained to develop a long-range plan (also known as strategic plan.)
The hospital consultant's role in design and construction is thus that of a programmer. The consulting architect will help him in this. Once the facility's role in the community has been established, the operational and functional plans must be established. They should be based on department utilization projections.
This consultant has a role to play towards the end of construction too. He can offer services relating to recruitment of staff, setting of tariffs, formulating operating procedures for the different medical departments, may offer consulting services on the evaluation of medical equipment to be purchased and may facilitate computerization of hospital functions. He may formulate marketing strategies and offer TQM / ISO 9000 solutions.
In an existing facility he may advise on turn around strategies, do operational audits, costing of services and systems study and redesign. He may advise on hospital waste management practice.
Fees are not regulated, and will vary depending on the scope of services.
2) The Consulting Architect / Architect
Consulting Architects offer specialized healthcare programming and design services. They may offer these services on a national or international basis. The national firm may have either many offices throughout the country or a home base and a few regional offices. It's design expertise includes master planning, layout, and equipment from projects ranging from medical colleges to rural primary health care centers.
The Consulting Architect may also extend his scope of services to do conceptual planning and schematic layouts for individual hospital projects. This will then be then the input to the next consultant, the Architect.
If the Architect has the necessary expertise to design and produce construction drawings and documents for the hospital project himself, and if the scale of the project is within

his design and production capabilities, the consulting architect's services are not needed for that project.
Selecting the consulting architect / architect can be a difficult and tiring process. The selection committee may sit through four presentations a day, hearing equally good demonstrations of expertise. The following tips may help narrow the choice:
a) Find out which member of the firm will handle the job and evaluate his or her responses. You will be working closely with this person for a long time, and this is the key to a firm's selection.
b) Study the proposed team and it's organizations appearance. Ask about the teams members' experience and request a reference of complete work.
c) Check the firm's references.
d) Explain your needs and the goals of your project, such as design excellence, mechanical systems and functional concerns, and ask questions as to how these can be met for your facility.
e) Relate the fee quoted to the larger costs, those of construction and efficient operation. Do not pick the lowest fee just because it is low. Once a fee is verbalized, it greatly influences a committee. However this fee amounts to only a small fraction of the total amount you will spend for construction, and an even smaller amount of the total project cost, including land and medical equipment. Money is not saved if the building does not operate efficiently. Every 3 to 5 years of operations will cost as much as the initial construction. The building will in all probability operate for around 50 years. It is important to trust in your selection.
3) Municipal Architect / Local Architect
The Municipal Architect is the consultant who will be responsible for obtaining all the
requisite permissions / No Objection Certificates (NOC's) from the concerned
regulatory authorities. This would include approval of the land use, the proposed built-
up area, the open spaces around the building, the provision for parking, any recreational
space / gardens that may need to be provided and the plans showing the individual rooms
with sizes. He would also be responsible for obtaining clearance as to fire-fighting
provisions and means of exit such as staircases.
HOSPITAL PLANNING AND PROJECT MANAGEMENT146 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 147
If the hospital is being designed by an architectural firm that does not have representation in the city / town / rural area where it is proposed, a Local Architect may be appointed, who, as his designation suggests is based in the locality of the project. He may be the same as the Municipal Architect. He would then, in addition to the above-mentioned functions, supervise the day-to-day activities on site, reporting to the main architect. He could also provide information on locally available materials and local methods of construction. He could advise on the traditional architecture of the region, if the main architects desire to respond to it in their proposed aesthetic for the facility.
Both these architects are better selected by the Main Architect than the client, as the working relationship between all these architects needs to be based on mutual respect and hence cooperation. Many a project has come to grief over disputes or differences in outlook between different firms of architects working on the same project. Creative professionals can often be prima donnas, or behave like them.
4) Structural Consultants / MEP (Mechanical, Electrical, Plumbing) Consultants
Structural and MEP Consultants are engineers. Structural engineers are
moregenerically called civil engineers.
Historically, engineers who worked on non-military projects became known as civil engineers. Three main divisions of civil engineering exist today:
a) Transportation Engineers
b) Structural Engineers
c) Sanitation Engineers
Civil Engineers contribute their talents to hospital construction in three areas:
a) Site Planning
b) Structural Design
c) Construction
Site planning: Site planning is the art and science of arranging the uses of land. Site planning is done professionally by architects, landscape architects and civil engineers. The civil engineer plays a role in readjusting the existing landform through designed grading and providing for proper drainage.

Structural Design: The structural engineer's role is that of providing the optimum support for the building. Structural work needs to be coordinated with the architect and the other engineering consultants; this coordination is absolutely essential in hospital projects. He will decide in consultation with the architect the structural system to be used.
It is in the preliminary stages of design that the structural engineer can effect the most
savings. He must be appointed at the beginning of the project, and work with the architect
even during conceptual design.
Construction: The civil engineer is responsible for inspection and testing of the
materials used in construction, to make certain the owner gets the quality and quantity
specified. His role is that of Construction Manager, dealt with in detail later on.
Mechanical Engineers study the conservation of energy and apply it in the most
efficient and economical way. They design the heating / air-conditioning loads for the
hospital, design the system and specify the necessary equipment. He will design the
incorporation of the necessary filters into the air-conditioning system to produce the
desired sterility conditions in that space.
Electrical Engineers design the electrical systems of the hospital and calculate the
electrical loads based on lighting and equipment loads. He should be aware of the public
utility supply and rates to ensure economical power distribution and the required
emergency supply. He will specify the equipment needed. He will design control and
monitoring systems (Building Management Systems) and cater to communications and
data processing requirements.
Plumbing Engineers are responsible for the processed water supply and liquid waste
disposal throughout the building. They design the capacity of the water tanks (overhead
and underground) required based on occupancy and applicable regulations. They design
the fire-fighting systems required, the sewage treatment plant (if required) and water
purification plants for the hospital.
In it's engineering requirements, each hospital presents a unique problem. There is no
universal solution to the selection of a system even after the problem is defined. There are
HOSPITAL PLANNING AND PROJECT MANAGEMENT148 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 149
many technical considerations depending on the medical equipment to be housed and
the medical procedures to be performed within the proposed facility.
It is important that the MEP design team is hired as early on in the proceedings as
possible, ideally at the start of the project, as they can advise on many decisions that are
often taken without their involvement, presenting them later on with a de facto situation
resulting in inefficient design and / or construction.
Coordination of the work of the engineering design team and the architectural
design team is of crucial importance. A lot can go wrong if this is not rigorously
done, especially in hospital design.
Very often, at the end of the project, few among the consultants and sometimes the client
too are not satisfied with the outcome. Too often the client is heard to say, “ Well, it is not
what I expected or what I wanted.”
This condition of dissatisfaction can be avoided with value management. This performs
the following functions:
a) Understanding the client's expectations
b) Understanding the constraints on the clients
c) Understanding the expectations and limitations of the architect, engineer and
construction manager
d) Helping the design team communicate their expectations and needs to one another
e) Helping the architect and engineer make changes and stay with schedule and
budget

f) Monitoring and reporting issues that seem likely to delay design or cause
dissatisfaction among members of the design team.
g) Preparing and conducting special problem solving sessions to clarify values and
objectives, improve design, maintain or lower total cost, maintain or shorten
schedule, improve life cycle costs and improve energy design and costs.
h) Employing the methods and procedures of all problem-solving systems, including
value engineering, value clarification, design-to-cost and Delphi.
Value engineering is a set of concepts and methods used to adjust designs to acquire the
best total value. Using definition and analysis of function, value engineering is aimed at
achieving the lowest total cost commensurate with design excellence. Specific methods
include function analysis, brainstorming sessions, matrix comparisons and analysis of
life-cycle costs.
5) Construction Manager
Construction Management of hospital projects in the West began in the 1960's. By now,
almost all projects include a construction manager to save time. The advantages of
including a construction manager early in the design phase can be great. For example,
the construction manager is familiar with:
i) Current building systems that are available on the regional market at a competitive
price.
j) Current labor and industrial prices, enabling him to establish a proper estimate in the
specific area.
k) Sub-contracting trades that can advise on detail.
l) Specification review.
HOSPITAL PLANNING AND PROJECT MANAGEMENT150 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 151
m) Cost consulting and scheduling.
n) Management.
o) Inspections.
p) Insurance programming.
q) Samples and Testing.
r) Shop drawing and Coordination.
This knowledge, if applied in the design phase, can lead to cost improvements, time-
savings and fewer change orders. The expected contingencies now budgeted and used
should be reducible. Many architect-engineer firms offer construction management
services.
The construction manager performs a variety of functions, such as managing general
conditions on site, including start-up and overall supervision. Towards the end of
construction, the construction manager is responsible for drawing up a certificate of
substantial completion.
6) Landscape Architect
The landscape architect is responsible for the design of outdoor areas, around the
hospital or the spaces in-between buildings on a campus. While the architect usually
does the layouts of motorable roads, the landscape designer suggests the layout of
pedestrian pathways, paved outdoor areas and plantation. He may also suggest water
bodies, fountains, street furniture and lighting and provide detailed construction
drawings for all these elements. He will work in close coordination with the main
architect.

7) Interior Design Consultant / Graphic Designer
We are in an era in which interior architecture design has become an integral part of the
architectural process; it begins with the earliest architectural concepts and ends with the
client occupying the completed space. In the case of a hospital, it is best that the interior
designer is able to work as a direct extension of the architect and is often hired directly
by the architect to perform work included in the basic architectural contract. The
architects firm may itself contain an interior design division. Such designers are best
qualified to perform the total range of services needed to complete any medical facility
including basic design and functional considerations, durability and maintenance of
product, and control of costs.
Fees vary, based on scope of work. The earlier the consultant is retained, the better. Listed below in chronological order are some of the interior design services available:
a) Preliminary consultation, analysis of scope and architectural review.
b) Interior design materials and color coordination.
c) Environmental programming based on social and behavioral factors.
d) Operational programming for efficient use of space and furniture.
e) Inventory analysis and evaluation for existing furniture reuse.
f) Preliminary budget.
g) Space planning of detailed layouts.
h) Lighting design, coordination and review.
i) Furniture selection or design, budget and specifications.
“Corporate image” does not sound like a term that should be applied to the design and construction of hospitals, but it is an area of design that is of great importance. The overall concept of a hospital's image includes graphic art and design. The interior of a hospital should be tied to a graphics program and that requires the services of a Graphic Designer.
HOSPITAL PLANNING AND PROJECT MANAGEMENT152 SCHC
HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 153
Two types of programs are of interest to the hospital designer. One is that of directional graphics, a signage program. A mass of information must be transmitted visually to the patients, visitors and staff so that time and motion are not wasted. The program develops a consistent lettering font and style and a directional program. The second is that of the corporate image of the hospital, the hospital logo and master program for all printed data. Graphic design should be thought through early in the design stage, allowing incorporation of the graphic design into the total design concept.
8) Bio-Medical Engineer / Medical Equipment Consultant
The responsibilities of the medical equipment consultant can be limited or quite broad.
Basic equipment planning services might include:
a) Assisting the client in making equipment selections.
b) Establishing and tracking the equipment budget
c) Compiling an “equipment book” including manufacturer's installation data and “cut sheets” (equipment specifications) and obtaining other relevant data from equipment vendors.
d) Developing room-by-room equipment lists and indicating the general location of equipment.
e) Obtaining from the vendor and forwarding to the architect (via the owner) installation data necessary to develop architectural and engineering components of the building.
f) Organizing and directing equipment user group meetings in which the specific equipment needs of facility users are identified.
Additional services, which may go beyond the scope of basic equipment planning services, may include
a) Assisting the owner in procuring and installing equipment and negotiating a purchase agreement with the vendor.
Although the equipment planner can be quite helpful in this area, many health care providers may be affiliated with some type of bulk purchasing service and can negotiate competitive prices themselves. The difference between an aggressively negotiated price and list price is considerable. Negotiated pricing also should include extended service contracts, which in themselves can eventually add up to a considerable sum.

b) Additional user group meetings.
Departmental user group meetings consist of a series of long, intense, interactive work sessions. In order for these meetings to be conducted in a time-efficient manner, each department user group should have a general idea about the equipment it is considering to purchase or reuse. The equipment planner can be an additional resource in describing some of the specific attributes and requirements of each unit, instead of having to begin with more basic issues. The equipment planner will bring a more objective viewpoint than the equipment vendor.
c) Coordinating tours to visit facilities where similar equipment is in operation and presentations by equipment vendors.
One good way to learn more about the equipment that currently is in use is to visit similar facilities that have recently opened. When conducting such a tour, it is best to select a facility that is similar in scope to the one being designed. It should also have been operational long enough for the staff to develop more than just first impressions, but not one that is so old that the equipment does not compare with what is currently on the market. Equipment vendors may also organize tours of their showrooms and current facilities showcasing their equipment. Such tours can be both educational and economical. However vendor organized tours tend to be less objective than those organized by the architect or equipment planner.
Trade shows are another good source for learning about current equipment as well as staffing, management and business issues relating to the operations of health care facilities. Many equipment vendors unveil their latest technology at such shows.
9) The Client / Client's Representative
As a client or his representative who intends building a new healthcare facility or adding to or renovating an existing facility, you will be working with the above-mentioned design team. Long before the first shovel hits dirt or hammer is swung, you will find yourself committed to many hours of planning meetings with professionals such as the above. You will be an integral part of the design team.
This is what Vincent Wang, Design Director, Stanhope Properties plc, has to say on the subject:
“Quality is a state of mind, not an optional extra. It cannot be bolted on. The lead must come from a strong and committed client and the pursuit of quality must form every strand of the process”
An essential function you will perform right at the beginning of the project will be to
HOSPITAL PLANNING AND PROJECT MANAGEMENT154 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 155
state the project goal/s, or 'statement of intention”. This will form a reference point for policy decisions taken by the design team, which will need to be consistent with this formulation of project goals or intention. Keep it short and state it with clarity. Weigh each word that forms part of this statement.
The whole team will look to you to provide direction and purpose to the whole effort. If you falter or show signs of indecision this will communicate itself to the entire team, and if this goes on for an extended period of time, the whole group will come apart at the seams. You have to project, as Mr. Wang says above, strength and commitment, and lead from the front. If you are perceived as losing interest in the project, maybe you show the team that you are more concerned about your other business then it is bad for morale. You must always communicate keen interest in the project. Make an effort to establish a rapport with the key members of the design team. Consultants work harder for clients they like as people; you can't always buy that kind of extra effort with money. (Of course, you can try it won't do any harm!)
Maintain project momentum. If you drag out the process, all concerned will lose interest.
10) Hospital Administrator / CEO of Proposed Facility
It is a good move to appoint the CEO of the proposed hospital or the HOD of the additional department/s being added / renovated right from the design stage. If they are already working in the existing facility they need to get themselves a hardhat and take on a part-time job. They will be liaison and interpreter between their staff and the design team.
My advice to this CEO is:
A) You need to be an active member of the planning and design team as early on as possible.
B) Try to keep a copy of the most up-to-date plans. This way you can keep up with progress and revisions.
C) Keep a current plan located in a strategic location so staff and physicians can become familiar with the project.
D) Take your own project meeting notes. You can double check them with the architectural minutes to make sure you don't forget anything. You should be on the mailing list for project meeting notes.

E) Involve your staff. Invite key members of your department to architectural planning sessions.
F) Form a staff planning committee and meet regularly for feedback and plan reviews. Involve a cross section of staff from different shifts, those that embrace change and yes, those that are most resistant.
G) Create flow charts of critical work processes. Determine what your problems and issues are with your current plan. How will these processes be supported in the new plan? Examples of processes to consider include chart flow within a department, supply flow and storage, soiled / clean linen flow and clean / soiled instrument / procedure tray pathways.
A little advice on reading architectural drawings: drawings or plans are produced in a reduced scale. The most common scale is 1:100 where 1 drawing unit is equal to 100 units in reality. This scale is by-and-large the same as 1/ 8 of an inch equals 1 foot. The other common scale is 1:50 or 1 / 4 of an inch equals 1 foot. Once you have your first plan to review, get a scale or architectural ruler to help read the drawings and determine the planned size of spaces.
On relating plans to space: once you can read the blueprints, relating them to your frame of reference of space is critical in planning. Here are a few quick tricks:
A) Find a room in your current department such as a patient room or supply room. Measure the size of the room. A room that is close to 8 feet by 10 feet is a good manageable frame of reference. You can then relate the size of your room to a comparable size room on the plans.
B) Measure doorways both on the plan and in your department. Doors through which patients on stretchers are to be moved are usually 60 inches wide, with two equal shutters. Patient room doorways and doorways for handicapped people are usually 48 inches wide. What is planned to go through the doorway in question will determine it's width.
C) Acute care hallways and hallways in public spaces should be 8 feet wide (7 feet at a pinch goes in India).
HOSPITAL PLANNING AND PROJECT MANAGEMENT156 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 157
D) Compare the new space with what you have. For example if the supply and equipment rooms are changing sizes, compare the new space with what you have.
E) The amount of square footage doesn't always provide a guide for actual usable space. The two rooms shown here give examples of different shaped rooms that are the same square footage.
Room A would make for a good equipment room because of the amount of space in the middle of the room for equipment needing floor space.
not to scale10'-0” x 12'-0”120 sq. Ft.
Room B would make a better supply room as the wall space can be used for shelving.
not to scale8'-0” x 15'-0”120 sq. Ft.
On being a proactive participant: don't let anyone tell you it's too early to start determining your departments needs. The earlier you have information, the more appropriate input you can give early on in the planning process.
Internal resources:
A) An essential place to start with is your information services department. When planning workspaces such as nurse stations and patient rooms, many of the issues will relate to technology. Discuss technology for your department and facility for the next 2 to 5 years so your department plans can be designed with enough flexibility to support change.
B) Meet with key support department heads. Their future plans may impact your department. Or, you may be considering changing a work process that impacts another department. In either case, inputs from these departments can provide you with valuable decision making information and ideas.

C) Visit other departments that have undergone recent construction, renovation and / or have purchased new equipment. Get their feedback on how the process was managed and the quality of decisions made. Check with the purchasing department and facilities department to see what current information they may have from vendors about new equipment. The internet is also an excellent source of product information!
D) Depending on the scope of the project it may be practical to build a mock-up room, for example a patient room, trauma room or an or somewhere on your campus. This is a great place not only to actually see the proposed size of the rooms but also to have mock-up products and equipment brought in for staff to see and touch.
External resources:
A) Your peers in other facilities. If you haven't already done so, talk to managers who have been or are going through their own construction project. Visit their departments and have them share their experiences with you.
B) Sales reps. Word gets around the sales community pretty quickly so sales reps may be contacting you before you think you are ready for them. They are a great resource for up-to-date information and future trends in their industries and for references regarding other new facilities. They should have a list of installed or built sites for you to see or key contacts for you to talk to. Trial and mock-up products are frequently available to assist you and your staff in making purchasing decisions.
C) Site and / or factory visits. Many people feel that a site visit to another health care facility is as good or better use than the traditional factory visit. Some of the advantages of a factory visit include being able to see the full range of products and services available to you from a manufacturer and obtaining customer references.
D) Professional meetings. Professional meetings that have large exhibit areas provide the opportunity to see many different kinds of technology and to touch, move and learn product features and benefits in a short condensed period of time. Registering at each booth may not only get you a free gift, but also put you in touch with a local representative.
E) The internet. More and more manufacturers and professional organizations have web sites that will let you research information and / or shop right from your office. Professional organizations such as the American Institute of Architects have web sites with articles on architectural trends and current projects.
Many construction projects, especially renovations, are phased construction unless you
HOSPITAL PLANNING AND PROJECT MANAGEMENT158 SCHC

HOSPITAL PLANNING AND PROJECT MANAGEMENT SCHC 159
can relocate to another hospital space or temporary building during construction. Disruption in operations, patient care delivery and compromises of work areas are to be expected. Working closely with project team members including infection control staff will ensure a smooth process.
A) Identify your priorities for the order of phasing and match them with the reality of construction constraints.
B) Get as realistic a schedule as possible, accepting the fact that time lines are bound to change.
C) Keep your staff up to date so there are a minimal number of surprises for them.
D) Visit the construction site frequently. As the building is being completed it will be easier for you to visualize what was on the plans. You will also be able to recognize situations that do not match the plans. It may be something as simple as a missing electrical outlet or a thermostat placed where furniture or equipment will obstruct it.
E) When construction is far enough along, usually after the walls are put up, bring your staff through and start orienting them to the new space. A three-dimensional space is very different from the flat blueprints you have been reviewing for a long time.
F) Keep your sense of humor! Generally, even if you had to make some compromises, the new department will be better then what you are currently working in.
All in all, the process of renovation or new construction can be challenging and fun if you are well prepared. You are the key to creating a more effective, functional and efficient clinical department or facility that supports both staff and patient care. This is your opportunity to make a difference in this important work and acre environment.
11) User Groups / Representatives of Users of the Proposed Facility
As we have mentioned above, in an existing hospital addition or renovation, staff members of the concerned departments are invited to attend what are called “user group meetings” in which they, as the eventual users of the proposed facility comment on the plans prepared by the design team. Their comments can offer insights into the efficient operations of the proposed facility, helping the design team get in touch with reality. These could be meetings with physicians, nurses, support staff, anyone who would be using the proposed facility.
For the design of Inpatient units, patients can be interviewed through questionnaires relating to their experience in the hospital, and asked for suggestions as to how their stay could have been made more comfortable. Designing for the patient costs no more

initially, and it will boost public relations for many years. This information can be obtained by “patient profiles”.
Patient profiles represent patient's needs, tastes, and opinions on their hospital stay directly to the architects and design people. Profiles will not only directly affect the administrator, as a buyer of hospital products, but will establish the patient and hospital staff as a partnership that works together to achieve a good professional environment that ministers to the physical and emotional needs of the patient.
With a patient profile system, reported patient needs can be analyzed in order to improve design standards. Whether a hospital has hired a consulting architect for a completely new facility or a phased renovation, the patient profile information is a valuable tool in design. It is time the design profession reflects on the needs of patients themselves, not on what we perceive to be their needs, for “their” needs are truly our own.
Community outreach programs are increasingly becoming important for hospitals to educate the community which they serve about the services they offer, and to get feedback from the same community as to what additional services they need to provide or change in the way they provide their current services. When designing a new facility it is well worth the designers while to present the proposed scheme to representatives of the community it is located in, to inform and to get feedback. In the United States it can be mandatory to this in particular cases. For a corporate hospital, it generates important feedback on the needs of the community, and would help determine which medical specialties should be their thrust area. Meetings with local physicians who would possibly refer patients to the proposed facility and asking their opinions on what medical facilities the proposed facility should offer would be at least a good marketing move, and might be of help too.
HOSPITAL PLANNING AND PROJECT MANAGEMENT160 SCHC