how to learn lessons from concerns - patient safety wales · 2016-02-02 · appendix 1 – ptr...
TRANSCRIPT

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 1 of 43
How to Learn Lessons from Concerns:
All Wales Document

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 2 of 43
CONTENTS
1 Introduction
2 Grading Concerns
3 Investigation and Concerns Management Tools
4 Investigators
- Table 1: The WHEN, HOW & WHO to investigate
5 Key Stages in the investigation and management of concerns
6 Quality Improvement
7 Sources of help and support
8 Acknowledgements
Annex 1a – Completed examples of Concerns Report Writing
Template, Plans and Investigation Tools
Annex 1b – Templates for Concerns Report, Plans and Investigation
Tools
Appendix 1 – PTR Grading and Risk Ratings
Appendix 2 – Flow Chart: Key Stages in the Investigation and
Management of Concerns
Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 3 of 43
1 Introduction
This guide has been written to support the Welsh Government’s Putting Things Right Guidance (PTR) on dealing with concerns about the NHS, which details the arrangements for handling complaints, claims or reported patient safety incidents and learning from what has gone wrong.
What is a “concern?”
The term “concern” is used throughout this document and should be taken to mean any complaint, claim or reported patient safety incident (about NHS treatment or services) to be handled under the PTR arrangements.
The PTR arrangements represent a significant culture change for the NHS in Wales. It provides an integrated and consistent approach to the raising, investigation and learning from concerns. In line with this approach it is important that investigations are effectively conducted to identify the root causes of a concern. The intention is that a standardised and well established approach to the investigation process will support organisations to
“investigate once, investigate well”. This will enable them to achieve long term solutions
in order to prevent or reduce the likelihood of the concern recurring, thereby improving patient safety.
Purpose of this document
This document has been produced to enable healthcare organisations and their teams
determine:
When and how to undertake an investigation so that it is proportional to the level
of the concern
Which investigation and reporting tools to use at the various stages of an
investigation and grade of concern
How to manage the investigation of a concern through to its final closure to
ensure that lessons are learnt and patient safety is improved
This guide provides a toolkit to help establish a standardised approach to the
investigation and general management of concerns.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 4 of 43
The value of using a standardised approach to the investigation of concerns
Using a standardised approach to the investigation and management of concerns will
help demonstrate that investigations have been conducted to a satisfactory level. This in
turn will be the basis for the development and implementation of effective solutions
which address the root causes of concerns to ultimately prevent or reduce the likelihood
of concerns recurring.
Seeking and Providing Assurance
NHS organisations and stakeholders need to be assured that concerns are being
managed effectively and appropriately. It is essential that robust systems are in place
for the reporting and management of concerns to ensure that when concerns are closed
by the relevant group or committee that solutions have been implemented across the
various healthcare organisations involved and that lessons have been learnt.
“Investigate once investigate well”
In order to improve the quality of investigations the recommended approach is to focus
efforts on the simplest and most effective investigation tools to avoid confusion and
misapplication. This standardised approach will enable a consistent and appropriate use
of tools at the different stages of the investigation process as detailed below.
The Incident Management Process and Key Investigation Tools
WHAThappened
HOW ithappened
SolutionDevelopment
Chronology Unsafe Act (Key problems)
Fix WhatIs Broken
WHY ithappened
Contributory Factors
•TabularTimeline
•TabularTimeline
•Brainstorming•ChangeAnalysis
•Barrier Analysis
•PDSA Cycle•Report
Template
•Classification Framework &
Fishbone •Five Why’s
•Brainstorming
The RCA Tools selected are based on consultation with key investigation leads in organisations that have been responsible for
conducting investigations, overseeing the quality of investigations and for cascade training over the past 7 years. This feedback is
also concurrent with existing Investigation/PTR Leads and the RCA Task and Finish Working Group.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 5 of 43
2 Grading Concerns
Concerns are graded to help determine how they are to be managed within the
organisation. Grading should be considered a dynamic process that may change as the
investigation progresses. The initial grading may be subjective, and there may be a
need to take further advice from relevant people who would be able to advise on the
concern (Ref Table 1).
The grading of concerns in this document includes the following processes:
Risk Rating Matrix 5x5 Likelihood and Severity (Appendix 1)
PTR Grading Framework 1-5 in severity (Appendix 1)
3 Investigation and Concerns Management Tools
Table 1 below outlines the investigation tools which it is suggested should be used with
the various grades of concerns and by whom. However, it is important to note that
overall judgement on which tools to use and when, is on a case by case basis and will
depend on professional experience. The level of detail gathered will normally reflect the
complexity of the concern and grading assigned. The effectiveness of some tools will
be dependent on the nature of the incident e.g. Change Analysis is particularly effective
for well defined processes; 5 Whys is generally suitable for simpler problems which tend
to have a lower grading.
The standardised investigation tools which are referred to in this document are all
included and completed in Annex 1 of this document to provide examples and
explanations of how they should look. Annex 2 includes templates of these investigation
tools. They can also be downloaded from the Wales Patient Safety Website -
www.patientsafetywales.org.uk.
4 Investigators
It is strongly recommended, that investigations should not be undertaken by one person
alone, unless considered reasonable. This ensures that bias and assumption is
minimised and that a more objective approach is achieved throughout the investigation
process. Table 1 below suggests who should be involved in the investigation process.
An investigating officer should be identified for all serious concerns and will need to be
trained and have experience in the principles of investigating and managing Concerns.
NHS organisations are advised to hold a register of investigators who have received
training, which should include the level of experience they have gained. A system of

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 6 of 43
mentorship is also recommended as a highly effective approach to enable individuals to
gain familiarity and practice in the investigation process.
Table 1: The WHEN, HOW & WHO to investigate
This table outlines the recommended, standardised tools which should be used for
different grades of concerns and who should investigate.
Grading Investigation Tools and
plans (Ref Annex 1a)
Undertaken by
PTR Grading of 4 and 5
(Possibly 3 where
considered appropriate by
the organisation)
Risk Rating of : 9-15 high risk (Amber), 16-25 extreme risk
(Red & therefore
reportable to Welsh
Govt Improving Patient
Safety Team)
Tabular Timeline
(& brainstorming)
with
Classification
Framework (&
fishbone)
and/or
5 Why’s
and/or
Change Analysis
Barrier Analysis
Action Plan
Report Writing
Template
Investigation Team
E.g. Patient Safety
Lead, SIM (Senior
Investigation
Manager), lay
person, Senior
Nursing/medical or
Divisional staff
external to the
location and specialty
of the concern.
Expert in the specialty
or location and of the
concern.
PTR Grading of 1 and 2
(Possibly 3 where
considered appropriate by
the organisation)
Risk Rating of :
1-4 negligible risk
(Green)
5-8 minor risk
(Yellow)
Tabular Timeline
(&brainstorming)
5 Whys
Action Plan
Report Writing
Template
Ward Manager &
member of the local
team

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 7 of 43
It is essential that the investigation is proportionate to the grade of concern. Whilst
Table 1 above provides guidance its use will be dependent on the nature of the concern
and organisational arrangements which may already be in place.
Important Note
Not all concerns will require an investigation and some can be managed and closed
immediately at source e.g. an explanation and/or an apology given to the patient for a
waiting room being cold, car parking deficiencies. This is where the patient is satisfied
with the explanation and actions taken. These concerns are defined as “on the spot”,
1.12 of the PTR Guidance. These concerns are not dealt with under the Regulations and
thus will not be graded. In these cases this document does not apply. When
managed in a timely and effective manner, it is possible to avoid the concern progressing
to a more serious level.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 8 of 43
5 Key Stages in the Investigation and Management of Concerns
Key Stages
The stages listed below will enable an organisation to provide a standardised and
comprehensive approach to the investigation and management of concerns, including
the assurances required within the organisation and with key stakeholders that lessons
have been learnt.
Relevant organisational policies and procedures regarding the handling and
management of concerns will already be in place, however, it is recommended that they
include the following:
1. When a concern occurs, where appropriate, the patient should be assessed and the
immediate situation made safe. The concern should be reported to the appropriate
manager. Defined arrangements for managing concerns out of hours should be
established. In the case of any serious concerns e.g. all PTR grades 4/5, or all red risks
16-25 the Senior Investigation Manager (SIM) will also need to be alerted.
2. The appropriate manager will ensure that any action required to make the situation
safer is taken immediately and that any other relevant managers are informed.
3. Where appropriate the Being Open process is initiated by those with identified
authority as soon as feasibly possible. Those identified with responsibility by the
organisation for leading on Being Open conversations with patients/carers/relatives will
initiate this process as soon as considered feasibly possible and in line with the needs
of the patient/relatives/carers. Please note this is an ongoing process.
4. The concern will need to be reported using the local incident reporting system and
graded using the PTR and local Risk Rating process. It is important to note that the
concern grading is dynamic in nature throughout the investigation.
5. Those with responsibility for the line management of staff involved in the incident may
wish to initiate the Incident Decision Tree (IDT) (footnote) to establish if there has been
any intended harm. It is a tool which can be used to encourage an open and fair culture
and to avoid inappropriate suspensions. Please note that use of the IDT is not a one off
occurrence and can continue throughout the investigation.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 9 of 43
6. Those with responsibility for staff involved in the incident will also be responsible for
assessing the impact of the concern on staff and to provide de-briefing and support
where considered appropriate. Please note this is an ongoing process.
7. Some moderate and all low harm concerns (i.e. grade 2 and 3s) will be investigated
by the Ward/Departmental Manager in conjunction with a local member of staff using:
a) The Tabular Timeline, 5 Why’s (Please ref to Table1) will be used for this
level of incident,
b) Action plans to address the root causes will be developed and shared
locally and recorded on datix.
c) The investigation will be reported at the Local Safety Group and decisions
taken to share on a wider basis as considered appropriate.
8. Serious concerns (i.e. grade 4 and 5) will be investigated by an Investigation Team
that will be identified by the SIM or as per organisational arrangements. An executive
lead will also be identified to regularly track progress on the incident to final closure and
at least one member of the team will be trained and experienced in the RCA process.
9. The decision to escalate the concern to the organisation’s Board will be taken by the
Investigation Team. The decision to include the concern on the Risk Register will be
taken at the Board meeting.
10. Concerns, particularly serious and moderate concerns (i.e. grade 4 and 5) should be
investigated using all stages of the investigation process. Appropriate investigation tools
for both the level and nature of concern should be considered (Ref Table 1).
a) What happened – Tabular Timeline (& brainstorming)
b) How it happened – Tabular Timeline (& brainstorming), Change Analysis
c) Why it happened – Classification framework (& fishbone), 5 Whys
d) Solutions Development – Barrier Analysis, Plan, Do, Study, Act (PDSA) Cycle &
Report Writing Template (which includes the lessons that need to be learnt)
11. Solutions will be developed to address the root causes identified during the
investigation process, using the Barrier Analysis and a summary of control measures
included in the Action Plan. It is essential that the solutions are developed in conjunction
with local managers to ensure ownership and that there is a thorough consultation with
teams who will be required to adhere to any solutions. The PDSA cycle can also be
used at this stage to test solutions prior to spreading the solution to other areas.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 10 of 43
12. The local manager will ensure solutions are implemented and monitored to achieve
compliance with the new procedures wherever relevant.
13. The Concern will be closed via local organisational arrangements. If it is a Serious
Incident i.e. PTR 4/5 or Red (16-25) then the Welsh Government Closure form must be
approved and signed by an Executive Director.
A flow chart of this process is available in Appendix 2

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 11 of 43
6 Quality Improvement
Using the Concerns Investigation Report Template (Annex 1 and 2) can be a powerful
way of increasing focus and engagement with quality and safety issues. It allows
organisations to examine the quality of their investigations following the adoption of a
systematic and reliable approach as described in this document. Organisations will be
able to demonstrate how problems in the process of care have been identified; where
and which actions have been introduced to address these problems and to prevent the
likely recurrence of the concern. The PDSA cycle can be used to test the solution prior
to implementation etc.
Consultation with key staff and stakeholders is a key element in the development of
solutions and will directly affect the effectiveness of the solution and the likelihood of it
being adopted as a long term solution.
Where concerns recur organisations should consider the audit of new procedures to
identify gaps in implementation and reasons for non-compliance, so that further actions
can be focused on these specific areas.
7 Sources of help and support Wales Patient Safety Website www.patientsafetywales.org.uk:
- NPSA. (2004). Root cause analysis toolkit. - NPSA. (2008). RCA investigation tools: Guide to investigation report writing.
Document 0769B V1. - Incident Decision Tool (IDT) - Being Open - Investigation and Management of Concerns Training Programme
Putting Things Right – Guidance on dealing with concerns about the NHS from 1 April 2011 Version 2 – April 2012 Australian/New Zealand Risk management standards AS/NZS 4360:1999 now replaced by ISO 31000:2009 The Quality Improvement Guide – A method for improving public services in Wales 2011
Further guides are available from the 1000 Lives Plus office, or online at
www.1000livesplus.wales.nhs.uk to support you in your improvement work:
■ A Guide to Measuring Mortality
■ Improving Clinical Communication using SBAR
■ Learning to use Patient Stories
■ Using Trigger Tools
■ Reducing Patient Identification Errors

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 12 of 43
8 Acknowledgements
This guide has been produced by Patient Safety Wales in conjunction with the
Concerns Task and Finish Working Group; and following extensive consultation with
NHS organisations and lead individuals in the field of incident management.
We would particularly like to thank those who have fed back lessons and experiences
relating to their years in the area of incident management.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 13 of 43
Annex 1a - Completed examples of Concerns Report Writing
Template, Plans and Investigation tools
The following section, Annex 1a, provides examples and explanations of what should be
included in the completed templates for the investigation and management of Concerns.
Annex 1b contains all the templates for the investigation and management of Concerns.
There are over 40 different RCA tools available. However, it is suggested that the
limited number of tools below are used to simplify the investigation process and ensure
that they are used properly and systematically and at the appropriate stages of the
investigation process.
The recommended investigation tools for the key stages of the concerns management
process are as detailed below and need to be selected so that they are proportionate to
the grade of concern.
Wherever possible, investigations should not be conducted in isolation in order to avoid
potential bias and assumption (Ref: Table1)
The Incident Management Process and Key Investigation Tools
WHAThappened
HOW ithappened
SolutionDevelopment
ChronologyUnsafe Act
(Key problems))Fix WhatIs Broken
WHY ithappened
Contributory Factors
•TabularTimeline
•TabularTimeline
•Brainstorming•ChangeAnalysis
•Barrier Analysis
•PDSA Cycle•Report
Template
•Classification Framework &
Fishbone •Five Why’s
•Brainstorming
For further information on investigating and managing concerns, including training
material go to www.patientsafetywales.org.uk

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 14 of 43
1 Final Report for the Investigation of Concerns
Final Report for the Investigation of Concerns
Name of organisation
Summary CONFIDENTIAL
Please follow the arrangements in place in relation to the confidential nature of the report and
arrangements for circulation.
Concern Reference Number
(Datix number)
D23
Date of concern 15.3.11
Investigation lead T.Smith – Risk Manager
Investigating Group
Name, Designation, Department
R.Rovers – Ward Manager
L.Peters – Pharmacy Manager
Report Prepared by
Name, Designation, Department
T.Smith – Risk Manager
Report Date 6.11.11
Name of Executive Lead
(For Serious Concerns only)
W.Jones – Director of Medicine
Concern closed by:
Name, Designation, Department/Division
Or
Divisional Quality and Patient Safety
Committee
Concern sign off/or closed means that the actions
to address the concerns have been implemented.
Where this has not been possible e.g. quarterly
audit, this should be noted and monitored for
closure at a later date.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 15 of 43
TERMS OF REFERENCE
To establish the facts across all relevant disciplines and specialties
i.e.:- what happened, to whom, when, where, how and why
To establish whether problems occurred in care and/or service delivery
To look for improvements rather than to apportion blame
To establish how recurrence may be reduced or eliminated (solutions work)
To produce an action plan in conjunction with local leads.
Recommendations that feed in to the action plan should be developed by
Divisional staff to ensure local ownership.
To provide a report as a record of the investigation process
To provide a means of sharing learning from the concern
1. EXECUTIVE SUMMARY- Concise summary of the Concern
Putting Things Right
Initial Grading
4
Putting Things Right
Final Grading
4
Risk Rating (5 x 5 – severity
by Likelihood)
25
Date of Concern April 2010
Division / Service Area
Emergency Department
Source and implication of
concern
Examples: Adverse Incident, Formal/VerbalComplaint, Audit
(external and internal), adverse publicity etc, etc.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 16 of 43
2. MAIN BODY OF INVESTIGATION REPORT
Background to the concern
No more than a couple of paragraphs, a brief summary of what lead to the incident.
Scope of investigation
e.g. The investigation covers the period from when the Department admitted the patient to the ward
etc
Level of investigation – (Ref to Table 1 above)
For further guidance in relation to RCA see : www.patientsafetywales.org.uk
Involvement and support of patient and relatives
e.g. The patient has been informed about the incident and given the name of one contact. It has been
explained that further details will become available throughout the investigation process and that a
meeting to update them on initial findings has been arranged for the 3rd March 20012. Due to the
complexity of the incident it has been explained that they will need to be contacted with ongoing
updates as information becomes available.
Support and ongoing briefing for staff involved in the concern
This could include an initial de-briefing, but must not be seen as a one off process. Counselling support
also needs to be offered. Staff have been informed that an investigation is underway.
Description of key events (Tabular Timeline)
This should be concise and include the essential points only, as details will be included in the Tabular
Timeline (Annex 1 of the report).
Notable practice
Points in the incident or investigation process where care and/or practice had an important positive
impact and may provide valuable learning opportunities.
e.g. Actions taken to inform the patient and relatives of the error in an open and honest way, and
patient and carer having the opportunity to express their views on the incident.
Care delivery or local problems (Tabular Timeline/Brainstorming and/or Change
Analysis)
Care delivery or local problems are problems that relate to direct provision of care. They arise in the
process of care and are usually actions or omissions by members of staff. They have two essential
features a) care deviated beyond safe limits of practice b) the deviation had at least a potential direct or
indirect impact on the eventual adverse outcome for the patient, member of staff or "general public"
e.g. failure to monitor.
Service delivery or organisational problems (Tabular Timeline/Brainstorming and/or
Change Analysis)
Service delivery or organisational problems are failures identified during the analysis of the concern,
which are associated with the way a service is delivered and the decisions, procedures and systems that
are part of the whole process of service delivery.
e.g. No maintenance contract for equipment.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 17 of 43
Contributory factors (Classification Framework& Fishbone or 5 Why’s)
A summary of the significant problems need to be listed and each one analysed to identify the factors
which contributed to the problem.
Where many contributory factors are identified, the classification framework (and fishbone) should be
included in the Appendices to show the full list of factors identified.
e.g.
Staffing levels were low at the time due to unfilled vacancies.
There were no emergency ambulances available to respond to the initial emergency call as the Region has 5 ambulance outside **** emergency department waiting to handover their patients to emergency department staff.
Root causes (Classification Framework& Fishbone or 5 Why’s)
These are the most fundamental underlying factors which contributed to the incident that can be
addressed. Root causes should be meaningful, (not sound bites such as communication failure) and
there should be a clear link, by analysis, between root CAUSE and EFFECT on the patient.
Root causes will be a summary of the most important contributory factors identified in the process
above.
Lessons learned
Key safety and practice issues identified which directly contributed to the incident from which we can
learn to prevent the concern from recurring.
Incidental Learning: Other problems identified during the investigation which did
not impact upon the concern
Key safety and practice issues identified which may not have contributed to this incident but from which
others can learn.
e.g. During the investigation it became evident that the clinical information documented on the patient
clinical record was below an acceptable standard and hindered the investigation process i.e. results not
filed and observations not recorded.
Recommendations: including summary of solutions (Barrier Analysis & Action Plan,
PDSA Cycle)
Recommendations (numbered and referenced) should be directly linked to root causes and lessons
learned, they should be clear but not detailed (detail belongs in the action plan). It is generally agreed
that key recommendations should be kept to a minimum where ever possible.
Arrangements for sharing and learning
Describe how learning has been or will be shared with staff and other organisations (e.g. through
bulletins, professional networks, etc.). Must ensure that there is organisational wide learning. Where
appropriate the report will be shared with Welsh Government and other networks to support wider pan
NHS Wales learning.
Was this a joint investigation with another organisation?
Investigation undertaken in conjunction with WAST and etc.
External Organisations Informed
e.g. Welsh Government, Health and Safety Executive.

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 18 of 43
Please ensure that all completed Appendices are included with this report

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 19 of 43
2 Example of a completed Tabular Timeline Event Date and
Time
20/1/04 1/2/04 11.30 12:00 12:30
Event Pt (JH) contacts medical team
to rearrange treatment plan due
to work commitments
Mr R S, Pharmacist
contacts SpR Dr L
to query the
prescription for
methotrexate for
administration on
same day as
Vincristine
Dr L introduces Sr Lynch to Dr D Campbell, a
locum SpR who will be assisting the team
Pt rings ward and tells
Staff nurse Abe that she
is caught in traffic and
will be about 2 hours
late
A staff nurse delivers the
Vincristine for pt JH to the ward
Supplementary
Information
The Pts IV Vincristine was
already booked for the morning
of 1/2/04. The Consultant Dr M
agrees to allow pt to have
intravenous and intrathecal
chemotherapy on the same day.
Iv in the morning and Intrathecal
in the afternoon. The SpR
covering the day of planned
treatment is informed of the
change
Dr L informs Mr S
that it has been
authorised by the
Pts consultant, Dr M
and that she will
take full
responsibility
On enquiry Sr Lynch is informed that Dr Campbell
is able to carry out all clinical duties that she would
usually do.
Sr L raises concerns with Dr L about the
Intrathecal chemotherapy procedures and the fact
that Dr C is not on the register Dr L assures Sr L
that Dr C is competent, that he comes
recommended by Dr M, the Consultant, and that
he has authorised his inclusion on the register. Sr
L confirms that Pt (JH) treatment will still be under
Dr L’ s care
SN A Kamole informs
Sr L. Sr L tells SN K that
she has to leave early
for a dental appointment
and asks AK to ensure
that Sr Roberts knows
what is happening. She
tells Abe she will also
write it in the notes
SN arrived on ward and asked
SR Lynch for the keys. These
were handed over and the nurse
put the drug in the fridge. It was
not discovered until after the
incident that she had placed the
Vincristine in the Methotrexate
dedicated fridge.
Sr L then leaves before Sr
Roberts arrives
Good Practice
Pharmacist was
aware of departure
from protocol and
questioned this
change
Care/ Service
Delivery
Problems
Failure to heed concerns raised by
members of clinical team. Dr L
overruled or ignored queries from the
Pharmacist and ward sister

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 20 of 43
3 Example of a completed Change Analysis
Normal Procedure Procedure as occurred
during Incident
Is a change
in process
evident?
Did the
change
cause the
problem or
influence it?
Surgeon knew patient’s
condition - both feet
gangrenous
Theatre list correct &
reviewed by surgeon
after typing
Marking of site follows
procedure. Carried out
by surgeon prior to list
using skin pencil, after
checking with pt and
notes
Site prepared after
checking notes and
consent form
Surgeon knew patient’s
condition - both feet
gangrenous
Theatre list changed
hand written by SHO
and RIGHT leg not
clearly identified
Left calf marked by
Registrar using Biro
night before operation
when consent form
signed. Patient crossed
his legs and mark
transferred to left leg
Site prepared after
checking theatre list
and seeing mark on left
leg
No
Yes
Yes
Yes
No
Yes
Yes
Yes

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 21 of 43
4 Completed Fishbone. NB: Fishbone template MUST be used with the Classification Framework
Failure to identify
incorrect drug
and route
Patient Factors Task Factors
Education
and Training
Factors
Working
Conditions
Individual
Staff Factors
Team & Social
Factors
Equipment
and Resource
Factors
Communication
Factors
Organisational
and Strategic
Factors
Pt listening to walkman
and not included in
procedure
Interruptions from bleep
Pt had requested change
to treatment plan
Drug checking procedure
not followed (Further
analysis - 5 Whys)
SHO not trained or
registered to carry
out the task
Locum SpR
unfamiliar with ward
& policies
SHO unqestioning
and helpful working
outside
competence
Lack of team
safety vigilence
Lack of clarity of
roles & skills
No formal induction
for locum SpR
Able to connect an IV
syringe to an
Intrathecal route
Ward emergency
during procedure
took SN away
Hierarchical structure not
conducive to discussion or
questionning
Lack of safety
culture/awareness
Lack of Systems for
managing Locum staff
Pt was late & stressed
Workload and staff absence left
two staff unfamiliar with pt and
protocols to carry out procedure
Time pressures,
other pts waiting
Lack of senior medical
supervision of junior/
inexperienced staff
Lack of leadership - nobody revisited
allocation of staff as a result of changes to
treatment plan and staff absence
No check of
competence/experience
built into task
No safety features
on chemotherapy
drug fridge
SHO stated
“Vincristine” SpR
did not pick up
incorrect drug
SpR consistently
referred to
Methotrexate as
“Chemo”
Neither clinician
checked drug
route
No visual clues in
allocated bay about
risks associated with
procedure
Lack of appropriately
trained staff
Breakdown of
multidisciplinary
team communication
Lack of consultant
support for locum
when SpR left
Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 22 of 43
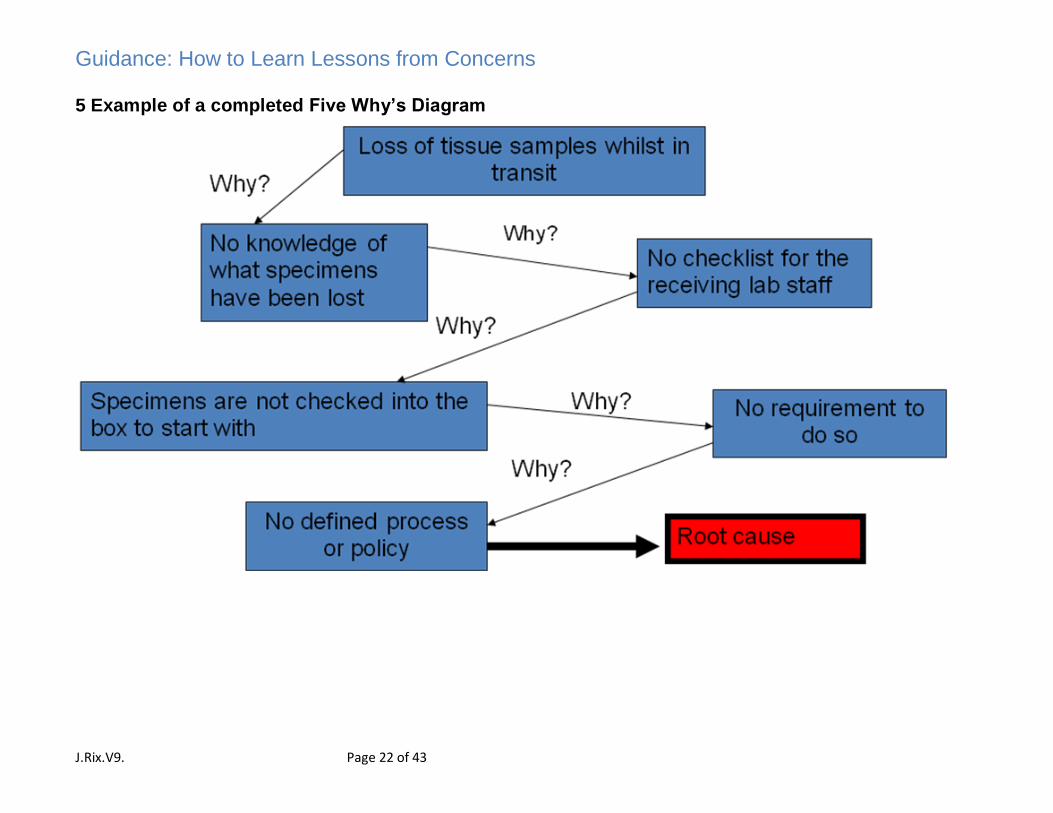
5 Example of a completed Five Why’s Diagram

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 23 of 43
6 Example of a completed Barrier Analysis
Activity/Incident: Giving a controlled drug to a specified person.
Hazard(s) What Barriers
are in place?
Importance
to safe
practice?
How
effective?
S/M/W
What additional
barriers are
required?
How
effective?
S/M/W
Cost
implications
Whose
responsibility
Wrong
drug
Two person
checks
Yes Weak Bar-coding Strong Medium Clinical Gov.
Committee
Wrong
patient
Patient ID
checks
Yes Weak Electronic
prescribing
Strong High Trust Board
Wrong
dose etc
Ward based
pharmacy
checks
Yes Medium ‘Time Gap’
between drawing
up drug, check and
administration
Medium Low Risk Man.
Committee

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 24 of 43
Annex 1b – Templates for Concerns Report, plans and
investigation tools
1 Final Report for the Investigation of Concerns
Final Report for the Investigation of concerns
Name of organisation
Summary CONFIDENTIAL
Concern Reference Number
(Datix number)
Date of concern
Investigation lead
Investigating Group
Name, Designation, Department
Report Prepared by
Name, Designation, Department
Report Date
Name of Executive Lead
(For Serious Concerns only)
Concern closed by:
Name, Designation, Department/Division
Or
Divisional Quality and Patient Safety
Committee

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 25 of 43
TERMS OF REFERENCE
To establish the facts across all relevant disciplines and specialties
i.e.:- what happened, to whom, when, where, how and why
To establish whether problems occurred in care and/or service delivery
To look for improvements rather than to apportion blame
To establish how recurrence may be reduced or eliminated (solutions work)
To produce an action plan in conjunction with local leads.
Recommendations that feed in to the action plan should be developed by
Divisional staff to ensure local ownership.
To provide a report as a record of the investigation process
To provide a means of sharing learning from the concern
1. EXECUTIVE SUMMARY- Concise summary of the Concern
Putting Things Right
Initial Grading
Putting Things Right
Final Grading
Risk Rating (5 x 5 – severity
by Likelihood)
Date of Concern
Division / Service Area
Source and implication of
concern

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 26 of 43
2 MAIN BODY OF INVESTIGATION REPORT
Background to the concern
Scope of investigation
Involvement and support of patient and relatives
Support and ongoing briefing for staff involved in the concern
Description of key events (Tabular Timeline )
Notable practice
Care delivery or local problems (Tabular Timeline/Brainstorming and/or Change
Analysis)
Service delivery or organisational problems (Tabular Timeline/Brainstorming and/or
Change Analysis)

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 27 of 43
Contributory factors (Classification Framework & Fish bone)
Root causes (Classification Framework & Fish bone)
Lessons learned
Incidental Learning: Other problems identified during the investigation which did
not impact upon the concern
Recommendations: including summary of solutions (Barrier Analysis & Action
Plan; PDSA Cycle)
Arrangements for sharing and learning
External Organisations Informed
Please ensure that all completed Appendices are included with this report

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 28 of 43
Tabular Timeline
Event date and
time
Event
Supplementary
information
Include cross –
referencing of
source
Notable Practice
Care / Service
delivery
problems
Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 29 of 43
Change Analysis Normal Procedure Procedure as
occurred during
Incident
Is a change in
process evident?
Did the change
cause the problem
or influence it?

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 30 of 43
Classification Framework & Fishbone
This Framework must be used in conjunction with the Fishbone diagram. Select
the relevant components which relate to the problem identified and add to the
appropriate factor.
Individual
Factors Components
Physical issues General Health (e.g. nutrition, diet, exercise, fitness)
Physical disability (e.g. eyesight problems, dyslexia) Fatigue
Psychological
Issues
Stress (e.g. distraction / preoccupation) Specific mental health illness (e.g. Depression) Mental impairment (e.g. illness, drugs, alcohol, pain) Motivation (e.g. boredom, complacency, low job satisfaction) Cognitive factors (e.g. attention deficit, distraction, preoccupation,
overload and boredom)
Social Domestic Domestic / lifestyle problems
Personality
Issues
Low self confidence / over confidence Gregarious / interactive, reclusive Risk averse / risk taker
Team Factors Components
Role
Congruence
Is there parity of understanding Are role definitions correctly understood Are roles clearly defined
Leadership Is there effective leadership – clinically Is there effective leadership – managerially Can the leader lead Are leadership responsibilities clear and understood Is the leader respected
Support and
cultural factors
Are there support networks for staff Team reaction to adverse events Team reaction to conflict Team reaction to newcomers Team openness

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 31 of 43
Communication
Factors
Components
Verbal
communication
Verbal commands / directions unambiguous Tone of voice and style of delivery appropriate to situation Correct use of language Made to appropriate person(s) Recognised communication channels used (e.g.head of service)
Written
communication
Are records easy to read Are all relevant records stored together and accessible when
required Are the records complete and contemporaneous (e.g. availability
of patient management plans, patient risk assessments, etc) Are memo’s circulated to all members of team Are communications directed to the right people
Non verbal
communication
Body Language issues (closed, open, aggressive, relaxed, stern faced)
Task Factors Components
Guidelines
Procedures and
Policies
Up-to-date Available at appropriate location (e.g. accessible when needed) Understandable / useable Relevant; Clear; Unambiguous; Correct Content; Simple Outdated; Unavailable/missing; Unrealistic Adhered to / followed Appropriately targeted ( e.g. aimed at right audience)
Decision making
aids
Availability of such aids e.g. CTG machine, risk assessment tool, fax machine to enable remote assessment of results
Access to senior / specialist advice Easy access flow charts and diagrams Complete information - test results, informant history
Procedural or
Task Design
Do the guidelines enable one to carry out the task in a timely manner
Do staff agree with the ‘task/procedure design’ Are the stages of the task such that each step can realistically be
carried out

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 32 of 43
Education and
Training
Components
Competence Adequacy of knowledge Adequacy of skills Length of experience Quality of experience Task familiarity Testing and Assessment
Supervision Adequacy of supervision Availability of mentorship Adequacy of mentorship
Availability /
accessibility
On the job training Emergency Training Team training Core skills Training Refresher courses
Appropriateness Content Target audience Style of delivery Time of day provided
Equipment Components
Displays Correct information Consistent and clear information Legible information Appropriate feedback No interference
Integrity Good working order Appropriate size Trustworthy Effective safety features Good maintenance programme
Positioning Correctly placed for use Correctly stored
Usability Clear controls User manual Familiar equipment New equipment Standardisation

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 33 of 43
Work Environment
Factor
Component
Administrative
factors
The general efficiency of administrative systems e.g. reliability Systems for requesting medical records Systems for ordering drugs Reliability of administrative support
Design of physical
environment
Office design: computer chairs, height of tables, anti-glare screens, security screens, panic buttons, placing of filing cabinets, storage facilities, etc.
Area design: length, shape, visibility, cramped, spacious
Environment Housekeeping issues – cleanliness Temperature Lighting Noise levels
Staffing Skill mix Staff to patient ratio Workload / dependency assessment Leadership Use Temporary staff Retention of staff / staff turnover
Work load and hours
of work
Shift related fatigue Breaks during work hours Staff to patient ratio Extraneous tasks Social relaxation, rest and recuperation
Time Delays caused by system failure or design Time pressure
Organisational Factor
Components
Organisational
structure
Hierarchical structure, not conducive to discussion, problem sharing, etc.
Tight boundaries for accountability and responsibility Clinical versus the managerial model
Priorities Safety driven External assessment driven e.g. Star Ratings Financial balance focused
Externally imported
risks
Locum / Agency policy and usage Contractors Equipment loan PFI
Safety culture Safety / efficiency balance Rule compliance Terms and Conditions of Contracts Leadership example (e.g. visible evidence of commitment to
safety) Open culture

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 34 of 43
Patient Factors Components
Clinical condition Pre-existing co-morbidity Complexity of condition Seriousness of condition Treatability
Social factors Culture / religious beliefs Life style (smoking / drinking / drugs / diet) Language Living accommodation (e.g. dilapidated) Support networks
Physical factors Physical state – malnourished, poor sleep pattern, etc.
Mental/
psychological factors
Motivation (agenda, incentive) Stress (family pressures, financial pressures) Existing mental health disorder Trauma
Interpersonal
relationships
Staff to patient and patient to staff Patient to patient Inter family – siblings, parents, children

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 35 of 43
Fishbone (NB: only to be used with classification framework)
Patient factors:
Clinical condition
Social factors
Physical factors
Psychological / mental factors
Interpersonal
relationships
Individual (staff) factors:
Physical issues
Psychological
Personality
Social / domestic
Task factors:
Guidelines /
procedures /
protocols
Decision aids
Task design
Communication factors:
Verbal
Non-verbal
Written
Electronic
Team + social factors:
Role congruence
Leadership
Support + cultural factors
Education + Training Factors:
Competence
Appropriateness
Availability
Accessibility
Supervision
Equipment + resources:
Equipment supplies
Visual display
Integrity
Positioning
Usability
Working condition factors:
Environment
Design of physical environment
Administrative
Staffing
Time / workload
Organisational + strategic factors:
Organisational structure
Policy, standards, goals
Externally imported risks
Safety culture
Priorities
Problem
or issue
(CPD/SDP)

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 36 of 43
BARRIER ANALYSIS
*Strong, Medium, Weak
Activity:
Hazard(s)/Issue What Barriers are in
place?
Importance to
safe practice?
How
effective?
S / M / W*
What additional barriers are
required?
How
effective?
S / M / W*
Cost
Implications
Who’s
responsibility?

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 37 of 43
Action Plan (Title)
* Strong, Medium, Weak
Recommended
Action
Action Control*
S
M
W
By Whom By When Actual
Completed
Date*
Progress/Remarks Monitoring
For
Compliance
1
2
3
4

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 38 of 43
Appendix 1: PTR Grading and Risk Ratings
Example Risk Rating Matrix - SIMPLE RISK QUANTIFICATION
AS/NZS 4360:1999 Risk Management defines risk as “The chance of something happening
that will have an impact on objectives. It is measures in terms of consequences and
likelihood”. Risk = Severity / Impact Likelihood
ESTIMATING RISK- QUALITATIVE MEASURES OF CONSEQUENCE (Impact / severity)
ESTIMATING RISK QUALITATIVE MEASURES OF LIKELIHOOD Whilst taking account of the controls in place and their adequacy, how likely is it that such an incident could occur?
5 Almost Certain Likely to occur on many occasions
4 Likely Will probably occur but is not a persistent issue
3 Possible / Moderate Do no expect it to happen but it is possible
2 Unlikely May occur occasionally
1 Rare Can’t believe that this will ever happen
Level Descriptor Actual or Potential
impact on individual
Actual or
Potential impact
on organisation
Number of
Persons
affected
The potential for
complaint /
litigation
5 Catastrophic DEATH
Sentinel event, Toxic offsite
Release
National Adverse
publicity, WG
investigation
Many, e.g. cervical screening disaster, evacuation etc.
Litigation expected /
Certain
4 Major Long Term Sickness. Permanent Injury Loss of body part(s), Mis-diagnosis, poor prognosis, RIDDOR Reportable Injury
Service closure RIDDOR reportable
Moderate number e.g. loss of
specimens etc
Litigation expected / Certain
3 Moderate SEMI-PERMANENT INJURY / DAMAGE e.g. taking up to 1 year to resolve
Needs careful PR, RIDDOR & MHRA Reportable Short Term Sickness
Small numbers e.g. 3 - 10
Litigation possible but not certain. High potential for complaint
2 Minor SHORT TERM – INJURY / DAMAGE e.g. injury that has been resolved in 1 month
Minimal Risk to organisation
One Complaint possible Litigation unlikely
1 Insignificant / Negligible
NO INJURY OR ADVERSE OUTCOME
No Risk to the Organisation
0-1 Unlikely to cause complaint Remote risk of litigation

Guidance: How to Learn Lessons from Concerns
J.Rix.V9. Page 39 of 43
RISK RATING CHART
Likelihood Severity/Impact
1 Insignificant
2 Minor
3 Moderate
4 Major
5 Catastrophic
1 - Rare 1 2 3 4 5
2 - Unlikely 2 4 6 8 10
3 - Moderate 3 6 9 12 15
4 - Likely 4 8 12 16 20
5 - Almost Certain
5 10 15 20 25
No Action this
12 months
Action within 12 months
Urgent Action

2 PTR GRADING FRAMEWORKS FOR DEALING WITH ALL CONCERNS
The All Wales grading framework is based on a risk matrix developed by the National Patient Safety Agency 1 and has been used to assess and manage risks and incidents. This approach has been built on to develop a framework for determining the level of investigation required in dealing with all types of concerns in order to promote a consistent approach across NHS Wales. The impact or harm experienced by the patient is always the overriding factor for grading concerns. The harm grading is dynamic in nature and must be considered throughout the investigation. Due consideration should also be given to the potential for litigation, regardless of the harm grading. However there may be situations where the grading of harm is low i.e. a grade 2, but there is indication there they will be pursuing a claim. The examples listed are meant only to be a guide and not an exhaustive list. Grade
Harm Examples of concerns Consider potential for qualifying liability / Redress

J.Rix.V9. Page 41 of 43
1 None a) Concerns which normally involve issues that can be easily / speedily addressed; b) Potential to cause harm but impact resulted in no harm having arisen; c) Outpatient appointment delayed, but no consequences in terms of health;, d) Difficulty in car parking; e) Patient fall – no harm or time of work; f) Concerns which have impacted on a positive patient experience.
Highly unlikely
2 Low a) Concerns regarding care and treatment which span a number of different aspects/specialities; b) Increase in length of stay by 1 - 3 days; c) Patient fall - requiring treatment; d) Requiring time off work - 3 days; e) Concern involves a single failure to meet internal standards but with minor implications for patient safety;
Unlikely

J.Rix.V9. Page 42 of 43
Moderate Serious
Concern occurs
Concern graded
(Putting Things Right & Risk Grading) (Appendix 2)
Appropriate Manager & Patient Safety Department Informed.
Immediate action taken to make situation safe by local team
Reported to Quality & Safety Mgnt. Board
Exec. Lead Identified Investigation Group Identified Ward/Local Manager to investigate with a number of staff
Consider if concern should be escalated &
included on risk register
Reported to local group
Consider if concern should be included on local risk register
1st test of Incident Decision Tree initiated by
appropriate manager
o Was there Intended Harm?
Being Open Conversation Initiated
o Contact with patients/carers
Appropriate Support Provided
De-brief staff involved in the incident &
keep them informed
Solutions Work/ Recommendations. Solutions to be developed with ownership by local managers.
Implementation of solutions – the responsibility of local manager
WHAT happened?
HOW it happened WHY it happened
Solution Development
Chronology
Unsafe Act Care & Service Delivery Problems (CDP/SDP) Contributory Factors Fix what is broken
Tabular Timeline
Tabular Timeline/Brainstorming/Change Analysis
Classification Framework Five Ways/Brainstorming
Barrier Analysis Plan,
Do, Study, Act (PDSA)
Consider if concern can
be managed & closed
immediately at source
Appendix 2 Key Stages in the Investigation and Management of Concerns

J.Rix.V9. Page 43 of 43
Sign off: exec Board & Welsh Government Serious Incident Report