how to read a head ct (or “how i learned to stop worrying and love computed tomography”)
TRANSCRIPT

How to Read a Head CTHow to Read a Head CT
(or “How I learned to stop worrying and love computed tomography”)
Andrew D. Perron, MD, FACEPAndrew D. Perron, MD, FACEP
EM Residency Program DirectorEM Residency Program Director
Department of Emergency MedicineDepartment of Emergency MedicineMaine Medical CenterMaine Medical Center
Portland, MEPortland, ME
Andrew D. Perron, MD, FACEP
Andrew D. Perron, MD, FACEP3
Head CTHead CT• Has assumed a critical role in the daily
practice of Emergency Medicine for evaluating intracranial emergencies. (e.g. Trauma, Stroke, SAH, ICH).
• Most practitioners have limited experience with interpretation.
• In many situations, the Emergency Physician must initially interpret and acton the CT without specialist assistance.

Andrew D. Perron, MD, FACEP4
Head CTHead CT• Most EM training programs have no
formalized training process to meet this need.
• Many Emergency Physicians are uncomfortable interpreting CTs.
• Studies have shown that EPs have a significant “miss rate” on cranial CT interpretation.

Andrew D. Perron, MD, FACEP5
Head CTHead CT
• In medical school, we are taught a systematic technique to interpret ECGs (rate, rhythm, axis, etc.) so that all aspects are reviewed, and no findings are missed.

Andrew D. Perron, MD, FACEP6
Head CTHead CT
• The intent of this session is to introduce a similar systematic method of cranial CT interpretation, based on the mnemonic…

Andrew D. Perron, MD, FACEP7
Head CTHead CT
“Blood Can Be Very Bad”

Andrew D. Perron, MD, FACEP8
BBlood lood CCan an BBe e VVery ery BBadad
• Blood
• Cisterns
• Brain
• Ventricles
• Bone

Andrew D. Perron, MD, FACEP9
BBlood lood CCan an BBe e VVery ery BBadad
• Blood
• Cisterns
• Brain
• Ventricles
• Bone

Andrew D. Perron, MD, FACEP10
BBlood lood CCan an BBe e VVery ery BBadad
• Blood
• Cisterns
• Brain
• Ventricles
• Bone

Andrew D. Perron, MD, FACEP11
BBlood lood CCan an BBe e VVery ery BBadad
• Blood
• Cisterns
• Brain
• Ventricles
• Bone

Andrew D. Perron, MD, FACEP12
BBlood lood CCan an BBe e VVery ery BBadad
• Blood
• Cisterns
• Brain
• Ventricles
• Bone

Andrew D. Perron, MD, FACEP13
CT Scan BasicsCT Scan Basics• Introduced in 1974 by Sir Jeffrey Hounsfield.• The original “Siretom” Circa 1974

Andrew D. Perron, MD, FACEP14
CT Scan BasicsCT Scan Basics• A CT image is a computer-generated
picture based on multiple x-ray exposures taken around the periphery of the subject.
• X-rays are passed through the subject, and a scanning device measures the transmitted radiation.
• The denser the object, the more the beam is attenuated, and hence fewer x-rays make it to the sensor.

Andrew D. Perron, MD, FACEP15
CT Scan BasicsCT Scan Basics• The denser the object, the whiter it is on CT
– Bone is most dense = + 1000 Hounsfield U.
– Air is the least dense = - 1000H Hounsfield U.
Andrew D. Perron, MD, FACEP16
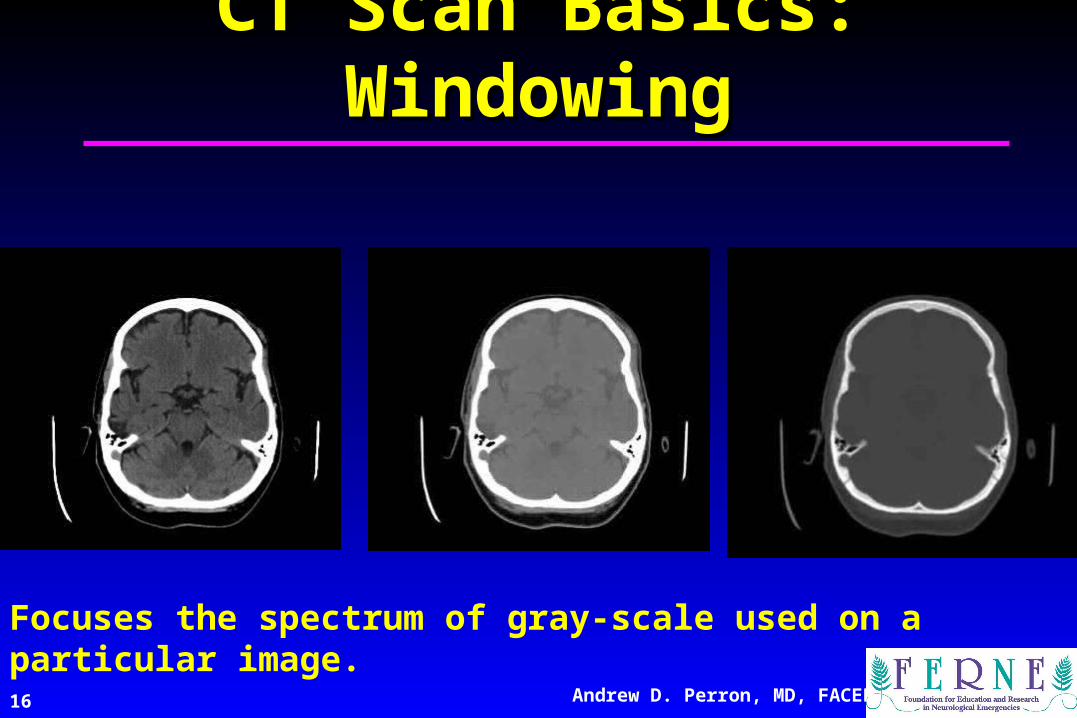
CT Scan Basics: WindowingCT Scan Basics: Windowing
Focuses the spectrum of gray-scale used on a particular image.
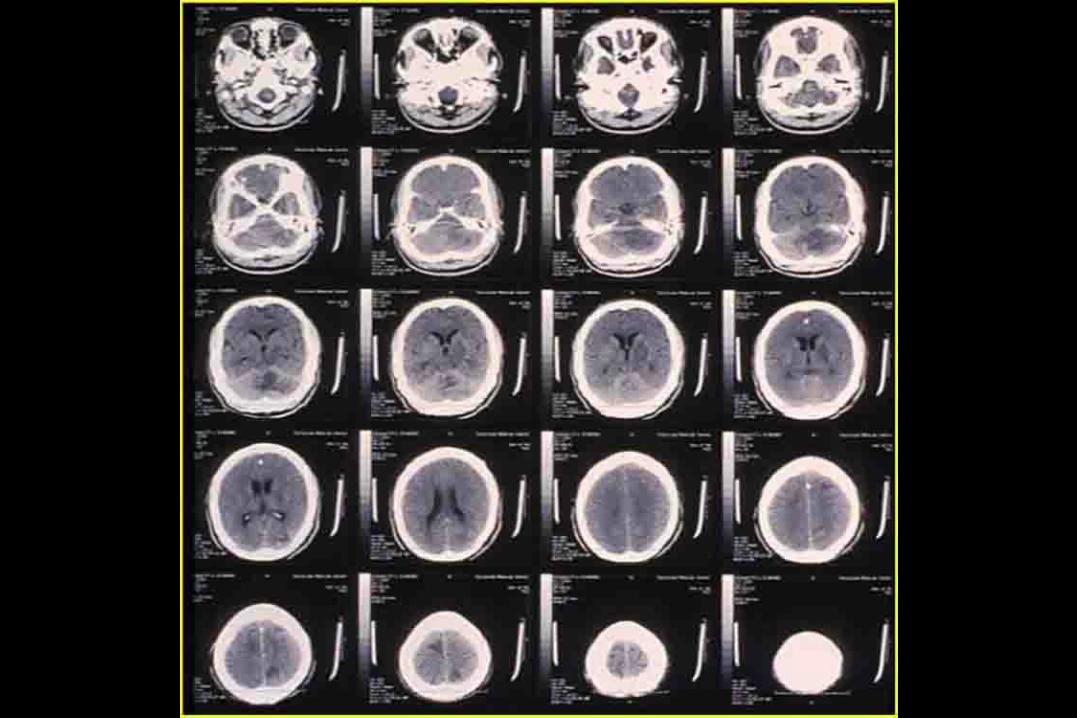
2 Sheet Head CT

Andrew D. Perron, MD, FACEP18
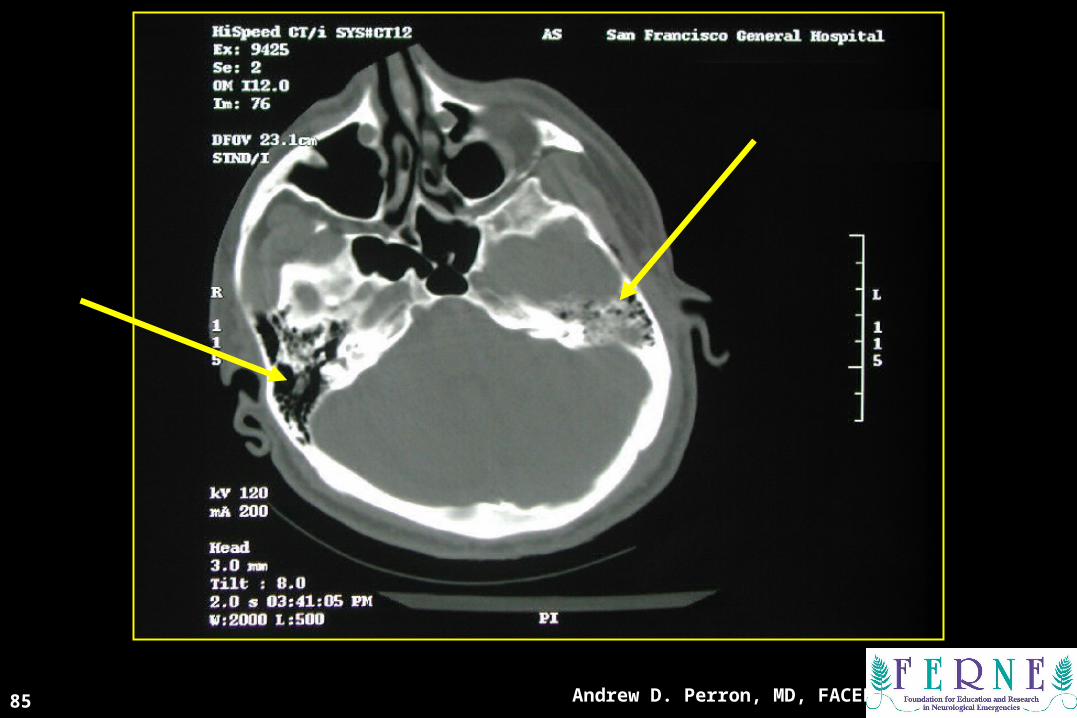
•Brainstem•Cerebellum•Skull Base
–Clinoids–Petrosal bone–Sphenoid bone–Sella turcica–Sinuses
Posterior FossaPosterior Fossa

Andrew D. Perron, MD, FACEP19
CT ScanCT Scan

CT ScanCT Scan

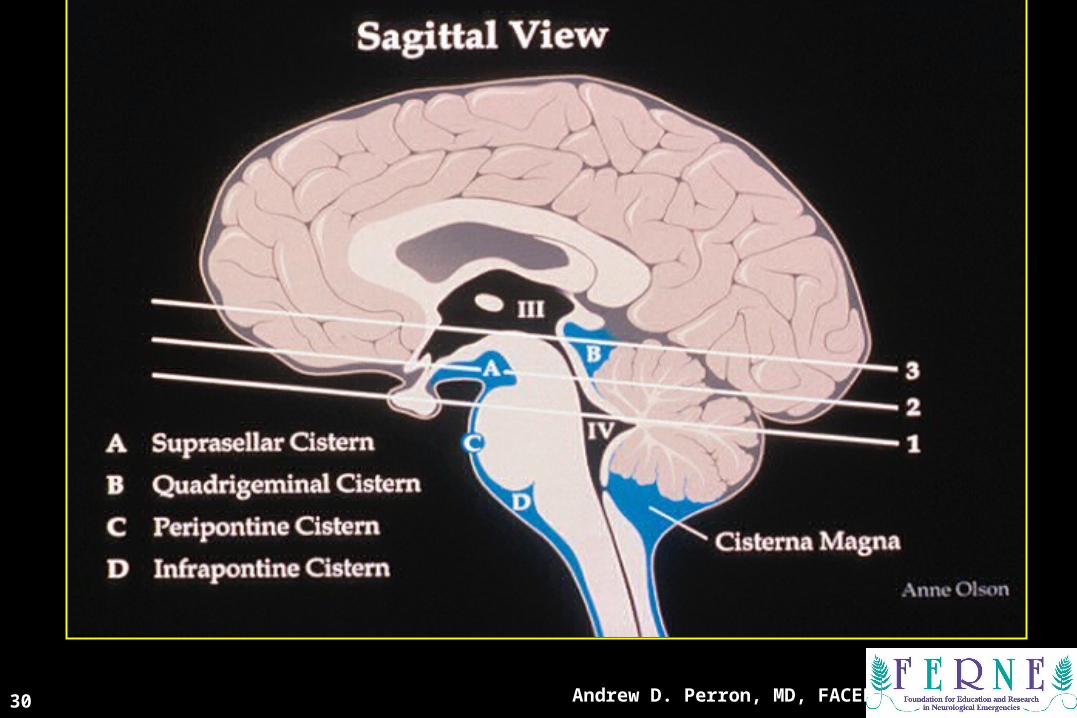
Sagittal ViewSagittal View

Andrew D. Perron, MD, FACEP22
CisternsCisterns

Andrew D. Perron, MD, FACEP23
CT ScanCT Scan

Andrew D. Perron, MD, FACEP24
Brainstem Lateral ViewBrainstem Lateral View

Andrew D. Perron, MD, FACEP25
2nd Key Level22ndnd Key Level Sagittal View Key Level Sagittal View

Andrew D. Perron, MD, FACEP26
Cisterns at Cerebral Cisterns at Cerebral Peduncles LevelPeduncles Level
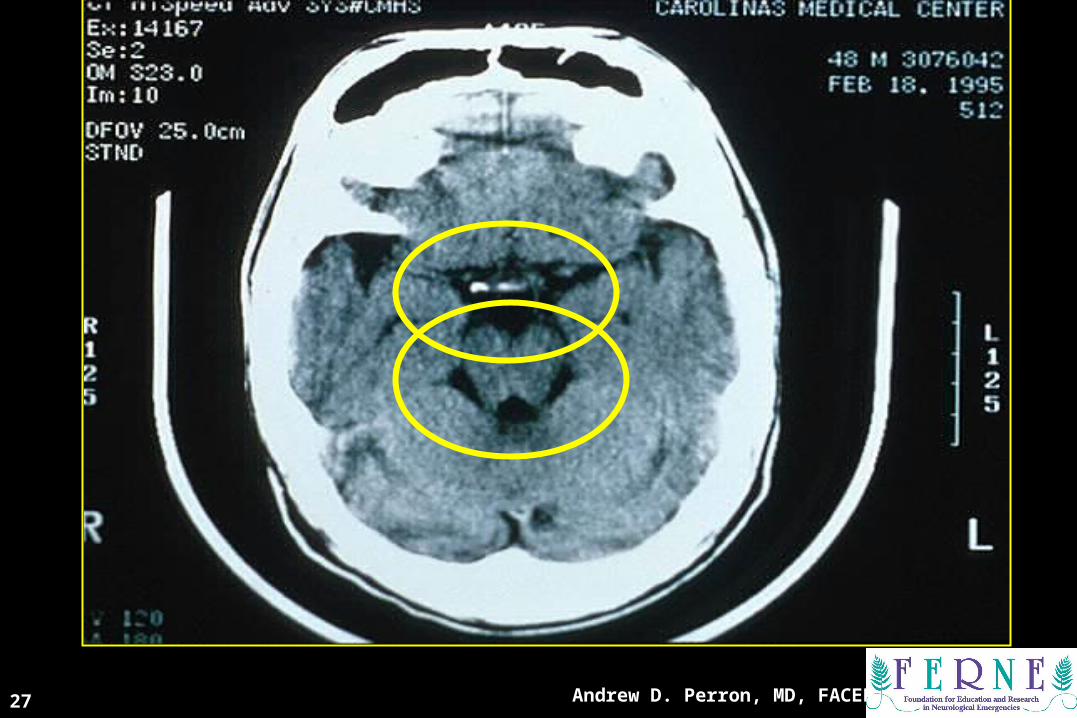
Andrew D. Perron, MD, FACEP27
CT ScanCT Scan

Andrew D. Perron, MD, FACEP28
Suprasellar CisternSuprasellar Cistern

CT ScanCT Scan
Andrew D. Perron, MD, FACEP30
33rdrd Key Level Sagittal View Key Level Sagittal View

Andrew D. Perron, MD, FACEP31
Cisterns at High Mid-Brain LevelCisterns at High Mid-Brain Level

CT ScanCT Scan
Andrew D. Perron, MD, FACEP33
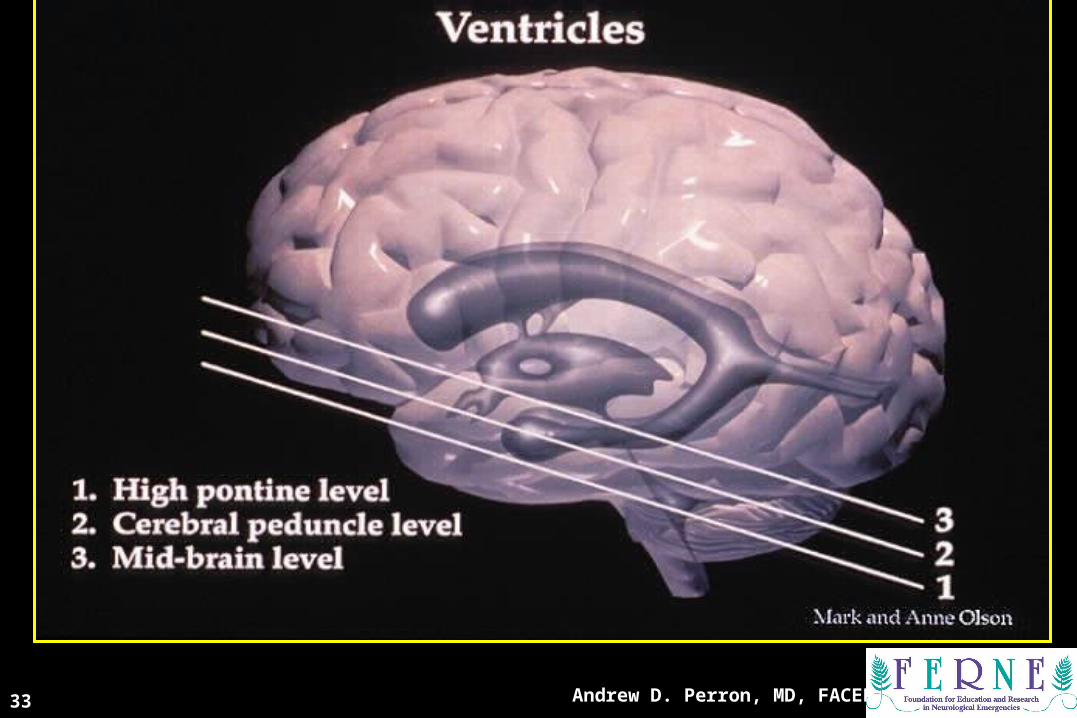
VentriclesVentricles

Andrew D. Perron, MD, FACEP34
CSF ProductionCSF Production• Produced in choroid plexus in the
lateral ventricles Foramen of Monroe IIIrd Ventricle Acqueduct of Sylvius IVth Ventricle Lushka/Magendie
• 0.5-1 cc/min• Adult CSF volume is approx. 150 cc’s.• Adult CSF production is approx. 500-
700 cc’s per day.

CT ScansCT Scans
Andrew D. Perron, MD, FACEP36

Trauma PicturesTrauma Pictures

PATHOLOGYPATHOLOGY

Andrew D. Perron, MD, FACEP39
BB is for Blood is for Blood• 1st decision: Is blood present?
• 2nd decision: If so, where is it?
• 3rd decision: If so, what effect is it having?

BB is for Blood is for Blood
• Blood becomes hypodense at approximately 2 weeks.
•Blood becomes isodense at approximately 1 week.
• Acute blood is bright white on CT (once it clots).

BB is for Blood is for Blood
• Blood becomes hypodense at approximately 2 weeks.
• Blood becomes isodense at approximately 1 week.
• Acute blood is bright white on CT (once it clots).

BB is for Blood is for Blood
• Blood becomes hypodense at approximately 2 weeks.
• Blood becomes isodense at approximately 1 week.
• Acute blood is bright white on CT (once it clots).

Andrew D. Perron, MD, FACEP43
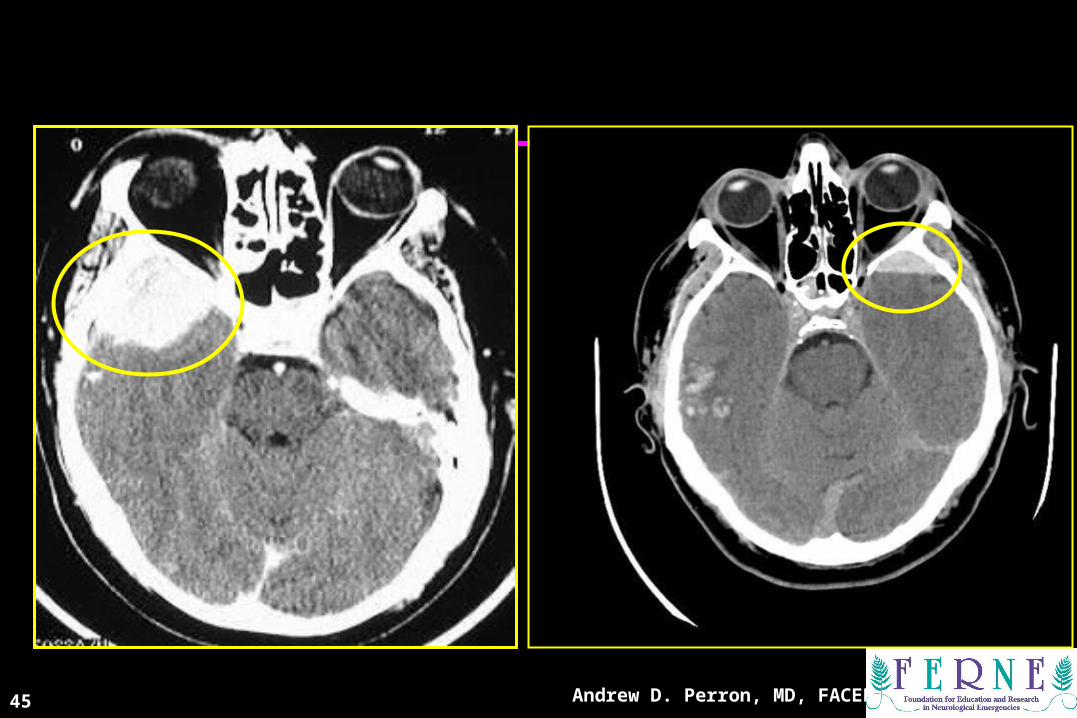
Epidural HematomaEpidural Hematoma
• Lens shaped
• Does not cross sutures
• Classically described with injury to middle meningeal artery
• Low mortality if treated prior to unconsciousness
( < 20%)

CT ScanCT Scan
Andrew D. Perron, MD, FACEP45
CT ScansCT Scans

Andrew D. Perron, MD, FACEP46
Subdural HematomaSubdural Hematoma• Typically falx or sickle-
shaped.• Crosses sutures, but does
not cross midline.• Acute subdural is a marker
for severe head injury. (Mortality approaches 80%)
• Chronic subdural usually slow venous bleed and well tolerated.

CT Scan CT Scan
Andrew D. Perron, MD, FACEP47

CT ScanCT Scan
Andrew D. Perron, MD, FACEP48
Andrew D. Perron, MD, FACEP49
Subarachnoid HemorrhageSubarachnoid Hemorrhage

Andrew D. Perron, MD, FACEP50
Subarachnoid HemorrhageSubarachnoid Hemorrhage• Blood in the cisterns/cortical gyral surface
– Aneurysms responsible for 75-80% of SAH– AVM’s responsible for 4-5%– Vasculitis accounts for small proportion (<1%)– No cause is found in 10-15%– 20% will have associated acute hydrocephalus

Andrew D. Perron, MD, FACEP51
• 98-99% at 0-12 hours
• 90-95% at 24 hours
• 80% at 3 days
• 50% at 1 week
• 30% at 2 weeks
Depends on generation of scanner and who is reading scan.
CT Scan Sensitivity for SAHCT Scan Sensitivity for SAH

Andrew D. Perron, MD, FACEP
CT ScanCT Scan
52

CT ScanCT Scan
Andrew D. Perron, MD, FACEP53

Intraventricular/Intraventricular/Intraparenchymal Intraparenchymal
HemorrhageHemorrhage
Andrew D. Perron, MD, FACEP54

CT ScanCT Scan
Andrew D. Perron, MD, FACEP55

Andrew D. Perron, MD, FACEP56
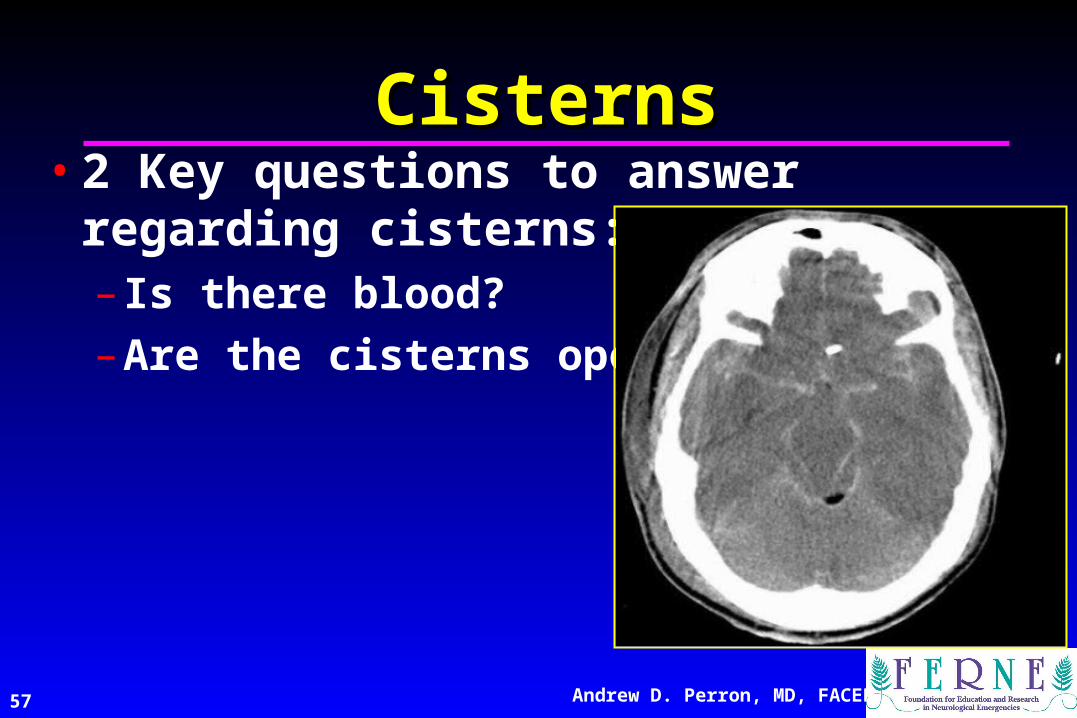
CC is for CISTERNS is for CISTERNS
• 4 key cisterns– Circummesencephalic
– Suprasellar
– Quadrigeminal
– Sylvian
((BBlood lood CCan an BBe e VVery ery BBad)ad)
Andrew D. Perron, MD, FACEP57
CisternsCisterns• 2 Key questions to answer regarding
cisterns:– Is there blood?
– Are the cisterns open?

Andrew D. Perron, MD, FACEP58

Andrew D. Perron, MD, FACEP59

Andrew D. Perron, MD, FACEP60

BB is for is for BBRAINRAIN((BBlood lood CCan an BBe e VVery ery BBad)ad)
Andrew D. Perron, MD, FACEP61

Andrew D. Perron, MD, FACEP62
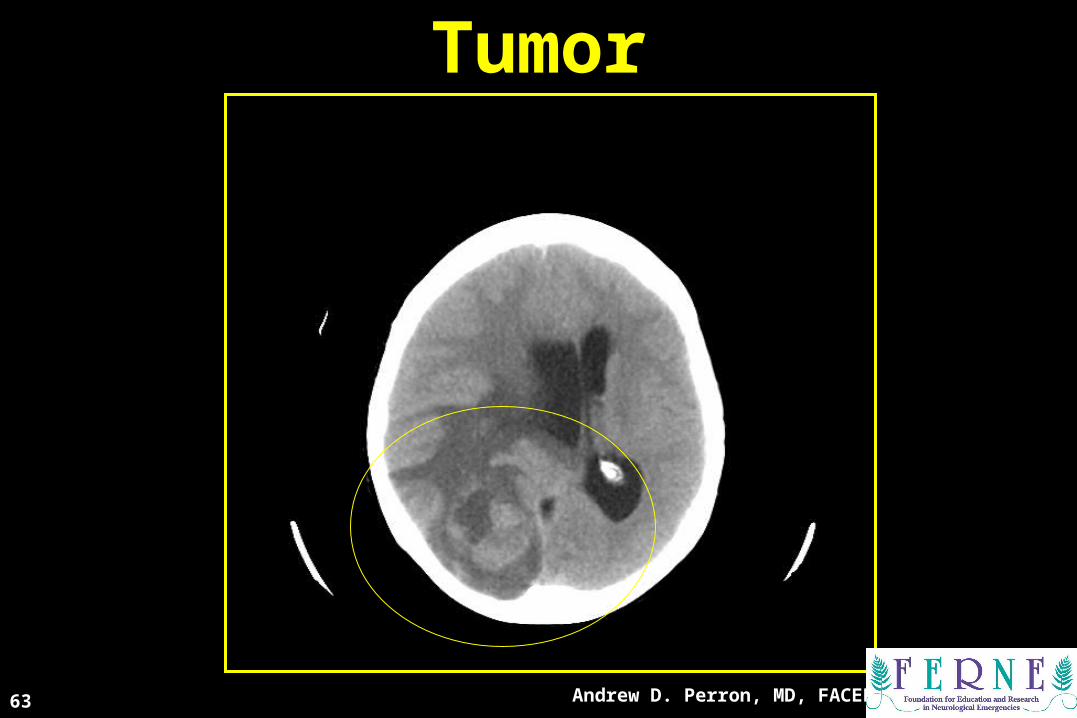
TumorTumor
Andrew D. Perron, MD, FACEP63

AtrophyAtrophy
Andrew D. Perron, MD, FACEP64

AbscessAbscess
Andrew D. Perron, MD, FACEP65

Hemorrhagic ContusionHemorrhagic Contusion
Andrew D. Perron, MD, FACEP66

Andrew D. Perron, MD, FACEP67

Andrew D. Perron, MD, FACEP68

Mass EffectMass Effect
Andrew D. Perron, MD, FACEP69
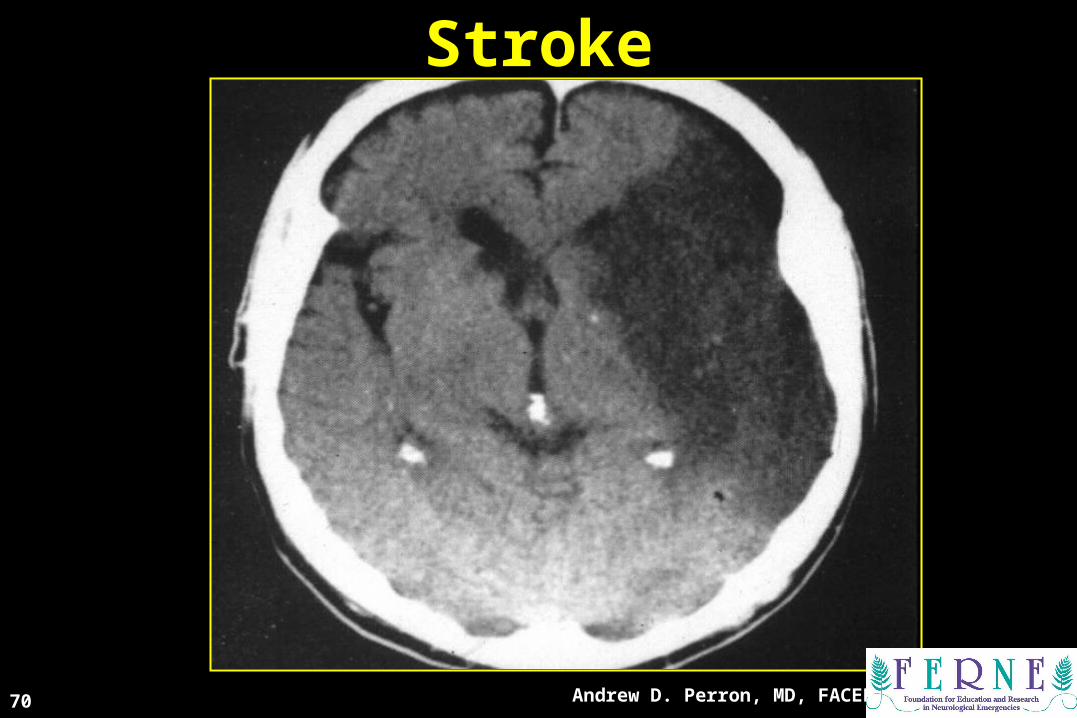
StrokeStroke
Andrew D. Perron, MD, FACEP70

Andrew D. Perron, MD, FACEP71

Andrew D. Perron, MD, FACEP72
Andrew D. Perron, MD, FACEP73
Intracranial AirIntracranial Air

Intracranial AirIntracranial Air
Andrew D. Perron, MD, FACEP74

Intracranial AirIntracranial Air
Andrew D. Perron, MD, FACEP75

Andrew D. Perron, MD, FACEP76
VV is for is for VVENTRICLESENTRICLES((BBlood lood CCan an BBe e VVery ery BBad)ad)

Andrew D. Perron, MD, FACEP77

Andrew D. Perron, MD, FACEP78

Ex-Vacuo PhenomenonEx-Vacuo Phenomenon
Andrew D. Perron, MD, FACEP79

Andrew D. Perron, MD, FACEP80

Andrew D. Perron, MD, FACEP81
BONEBONE
Andrew D. Perron, MD, FACEP82

Andrew D. Perron, MD, FACEP83

Andrew D. Perron, MD, FACEP84
Andrew D. Perron, MD, FACEP85

Andrew D. Perron, MD, FACEP86

Three StoogesThree Stooges

Andrew D. Perron, MD, FACEP88
If no blood is seen, all cisterns are present and open, the brain is symmetric with normal gray-white differentiation, the ventricles are symmetric without dilation, and there is no fracture, then there is no emergent diagnosis from the CT scan.
Blood Can Be Very Bad
RIPRIP

QuestionsQuestions
ferne_acep_2005_spring_perron_ich_bcbvb.ppt 04/19/23 01:28
[email protected]@ferne.org
Andrew D. Perron, MD, FACEPAndrew D. Perron, MD, FACEP
[email protected](207) 662-7015207) 662-7015
Andrew D. Perron, MD, FACEP