human factors in investigations undertaken by the rail accident investigation branch (raib)...
TRANSCRIPT
Human factors in investigations undertaken by the Rail Accident Investigation Branch (RAIB)
Presentation to the International Railway Safety Conference
October 2012
Simon FrenchDeputy Chief Inspector, RAIB
John CopePrincipal Inspector, RAIB
What is the RAIB?
The RAIB is the independent railway accident investigation organisation for investigating accidents and incidents occurring in the UK
The RAIB’s sole purpose is to improve safety of railways.
The RAIB does not apportion blame or liability, nor enforce law or carry out prosecutions
The Chief Inspector reports to Secretary of State for Transport on investigations

How does the RAIB investigate human factors?
All accidents are subject to detailed analysis of the causal chain
This will lead to the exposure of human factors issues in the same way that ‘pure’ engineering or operational issues are identified

Example of causal analysis
Driver unaware of opendoor
Delayed response followingpassenger observation of
open door
Train not immediatelybrought to stop
Contradictory indicationsassociated with illuminationof desk Pass Comm lamp
No Level 3 driver alarm toDriver for door open
Loss of illumination of doorinterlock lamp is not
observed
No passenger pulls PassComm handle
Customer Host does notimmediately pull Pass
Comm handle on receivingpassenger report
Door opens(after Kettering)
Case study – Derailment of a freight train
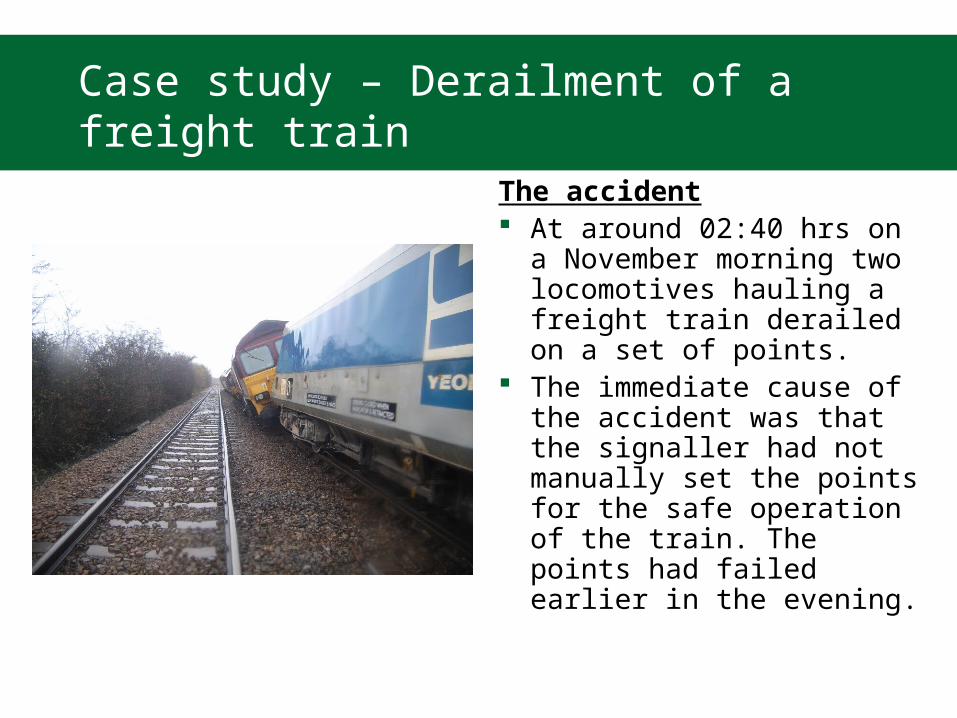
The accident At around 02:40 hrs on a
November morning two locomotives hauling a freight train derailed on a set of points.
The immediate cause of the accident was that the signaller had not manually set the points for the safe operation of the train. The points had failed earlier in the evening.

Case study (cont’d)
The report findings fell into many categoriesTechnical The initial failure of the signalling equipment was causalOperational Signallers had limited opportunity to practise emergency skills There was a lack of guidance to managers on how to deal with such incidentsManagerial There had been limited safety learning from previous similar safety incidents The roster worked by the signaller was not subject to assessment using fatigue
assessment tools. The duty holder had no suitable framework of controls to manage fatigue in
safety-critical staff.Human Factors The support tools available to the signaller to help him when equipment failed
were insufficient It is probable that the signaller’s actions were affected by fatigue, as a result of
the number of hours and the nature of the shifts that he had worked.

RAIB’s general experience
RAIB’s experience is biased towards higher risk events and the analysis therefore provides useful data on the impact of human factors in the causation of high risk events.
Of the 222 accidents and serious incidents investigated by the RAIB since October 2005, the actions of train drivers featured in 47 of them and the actions of track workers in 26.
It should be recognised that the potential consequences of errors by these staff are much greater, so they tend to be more prominent in RAIB investigations.

Types of activity where human actions are linked to accident or incident causation
The RAIB analysed the investigations it has carried out in order to: identify the types of railway activity and human
error that feature in RAIB investigations;
find typical examples of the factors that apply; and
categorise and describe the types of barriers that feature in recommendations.

Train driving error (features in 47 investigations)
Loss of alertness leading to signals passed at danger, collisions, derailments or loss of control
Misjudgements Errors while undertaking
unfamiliar tasks Errors arising from
competence management failings
Inappropriate/slow response to alarms
Violations (e.g. overspeeding)

Error while working on the track (26)
Lack of appropriate experience
Misunderstanding of rules Competence shortcomings Cultural issues Violation of rules including
disregard of warnings and briefings
Workload and competence issues
Insufficient planning Planning errors Insufficient communication
and coordination

Error during shunting and train preparation (16)
Competence issues Ergonomic issues Violations Errors and oversights Characteristics of
individuals

Intentional or unintentional misuse of level crossings (16)
Violations or inappropriate behaviour
Misjudgement Environmental factors Disregard of warning lights Design and ergonomic issues Sighting of approaching trains Information deficiencies Audibility of train horns at
footpath crossing Conspicuity of lights at Automatic
Open Crossing (with no barriers) Capabilities of users (eg
eyesight)

Staff error at level crossing (9)
Individual performance Competence Distraction Lapses in attention

Signalling error (13)
Competence - mismanagement of points and signaller authorised movement of train when route not correctly set
Violation - unauthorised system of work during equipment failure
Human capabilities - poor communications

Missed defect – infrastructure (15)
Work overload leading to missed inspection of points in degraded condition
Competence Supervision and instruction Monitoring and review

Third parties (eg road vehicle incursion) (5)
Various lapses on the part of road vehicle drivers leading to incursions

Error during operation of road rail vehicles (4)
Competence - poor on-tracking technique and over-reliance on interlock and insufficient allowance made for affect of poor adhesion on steep gradient
Training - lack of awareness of how to respond to runaway

Error during dispatch from stations (4)
Ergonomics Competence Individual errors

Key themes
Seven broad areas: knowledge-based mistakes
leading to a task being carried out incorrectly;
distraction, loss of concentration;
cognitive lock-up; loss of situational
awareness; inaccurate mental models; omissions; and deliberate violations
Barriers (as reflected in RAIB recommendations) [1]
Removal of the hazard Enhancement of design:
physical measures to reduce the likelihood of staff or members of the public making errors or to minimise their consequences
Enhancement of design assurance and approvals: these recommendations are typically designed to prevent design deficiencies that have led to human error from being replicated in future trains and infrastructure.
Steps to address safety culture: such recommendations are designed to address attitudes and behaviours within railway organisations

Management process; typically these are changes to management arrangements in order to better manage a particular risk:
Enhancement of procedures (operational, maintenance, etc.): this can be done to implement an improved process or alternatively to improve the clarity of existing procedures.
Training & competency: since the safety of the railway is critically dependent on the professionalism of its staff many recommendations address the way that staff are trained and assessed as competent.
Barriers (as reflected in RAIB recommendations) [2]
Final thoughts Human factors are a
significant feature in the causation of many accidents
Investigating the underlying issues can be difficult
It is often easier to understand why humans behave in the way they do than it is to define a course of action that will correct that behaviour
That does not prevent us from trying to identify the role that human factors play in accidents and incidents

Further work
In conclusion There is much to be learnt from a detailed analysis of
accidents and incidents The RAIB plans to extend and refine its analysis, and to
prepare a database of the human factors that have been identified in investigations, and the associated mitigation measures
• to inform future investigations• as a source of data for investigators and researchers
• We intend to do this in consultation with RSSB and others in the railway industry

Thank you