i have no financial relationship with - school of medicine ... · step 3 –hysterectomy or not ......
TRANSCRIPT
Jon Ivar Einarsson MD PhD MPHDirector of Minimally Invasive Gynecologic SurgeryBrigham and Women’s HospitalAssociate Professor of Obstetrics and GynecologyHarvard Medical School

I have no financial relationship witha commercial entity producinghealth‐care related products and/orservices

To identify surgical strategies for safe completion of complex laparoscopic procedures
To identify methods of managing gastrointestinal endometriosis
To identify methods of managing urinary tract endometriosis
To compare postsurgical medical treatment options after endometriosis surgery

Improved visualization Less pain, faster recovery In a recent RCT comparing laparoscopic vs open segmental bowel resection for rectosigmoidendometriosis the laparoscopic approach was associated with significantly; Less pain Less blood loss Fewer severe complications Higher pregnancy rates
Darai et al. Ann Surg 2010; 1018-23
Maintain exposure at all times Do not proceed without having exposure Do not proceed without orientation/anatomic landmarks
Always know where your ureters are Enter the retroperitoneal space early in distorted anatomy

“You got to know when to hold ‘em, know when to fold‘em,
know when to walk away and know when to run”

Surgery is like chess – you should think at least 2 games ahead Communicate
What will you need next? Cystoscope Interceed Sutures
If you don’t have what you need, it is your fault
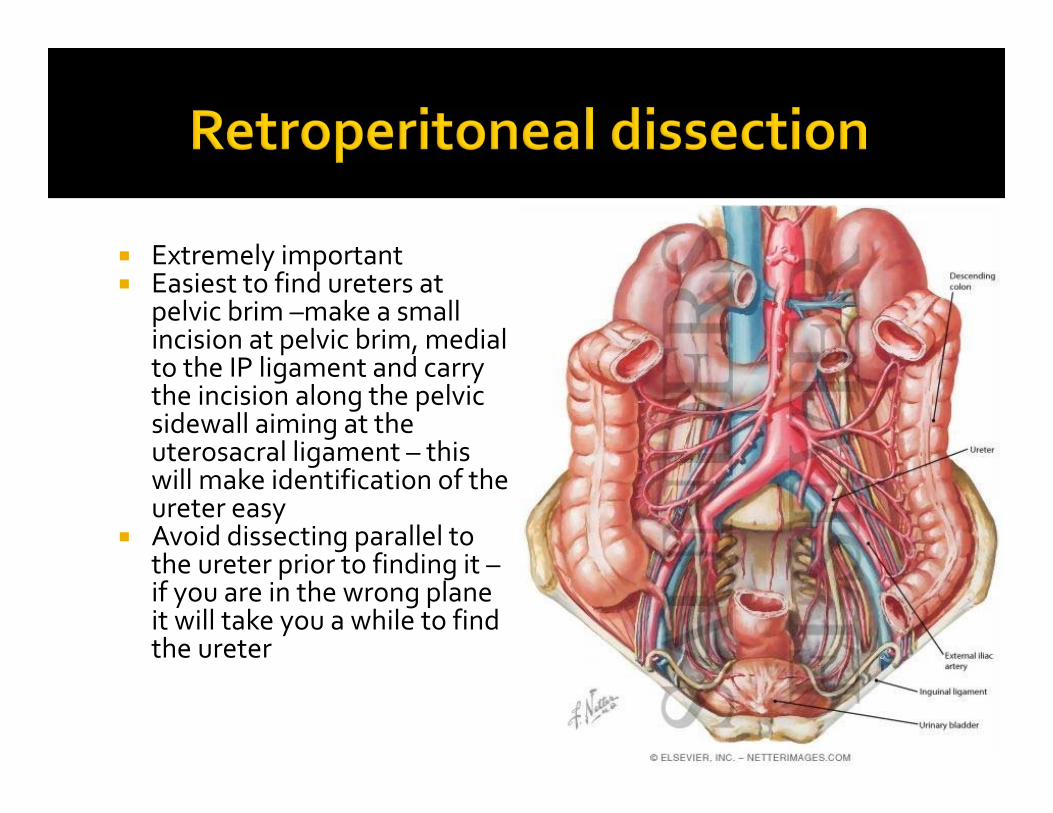
Extremely important Easiest to find ureters at
pelvic brim –make a small incision at pelvic brim, medial to the IP ligament and carry the incision along the pelvic sidewall aiming at the uterosacral ligament – this will make identification of the ureter easy
Avoid dissecting parallel to the ureter prior to finding it –if you are in the wrong plane it will take you a while to find the ureter

STRATEGY Follow similar principles throughout Break down into steps

Step 1 – Left ureteral dissection and bowel mobilization Dissection starts at left pelvic brim Mobilize sigmoid colon Enter retroperitoneum Find left ureter Follow ureter down to uterine vessels Drain ovarian endometrioma/free ovary and suspend to round ligament
Consider using plain gut to leave the ovaries suspended
Step 2 – Right ureteral dissection Open retroperitoneum at right pelvic brim and perform right sided ureterolysis
Important!! – the ureterolysis needs to be completed all the way down to uterines – the ureters can be distorted medially at any point…more often towards the lower end of their course
The ureters are pulled medially here and can be very close to bowel and uterosacral ligaments
Mobilize and/or drain right ovary and suspend to round ligament
Step 3 – Hysterectomy or not If hysterectomy is planned mobilize bladder and skeletonize uterines – coagulate IF bowel is away
If possible remove the uterus and then tackle bowel, but often need to partially mobilize bowel first
If no hysterectomy, consider suspending the uterus to anterior abdominal wall with sutures and remove the uterine manipulator
This frees up the vagina for manual exploration which can guide the dissection
Step 4 – Remove endometriosis off bowel/bladder/ureter Dissect rectosigmoid off uterus/cervix/vagina Prefer to stay on uterine/vaginal side Make sure the bowel is fully mobilized from ureters Can use dilute vasopressin to reduce oozing Don’t use energy next to the bowel/ureters

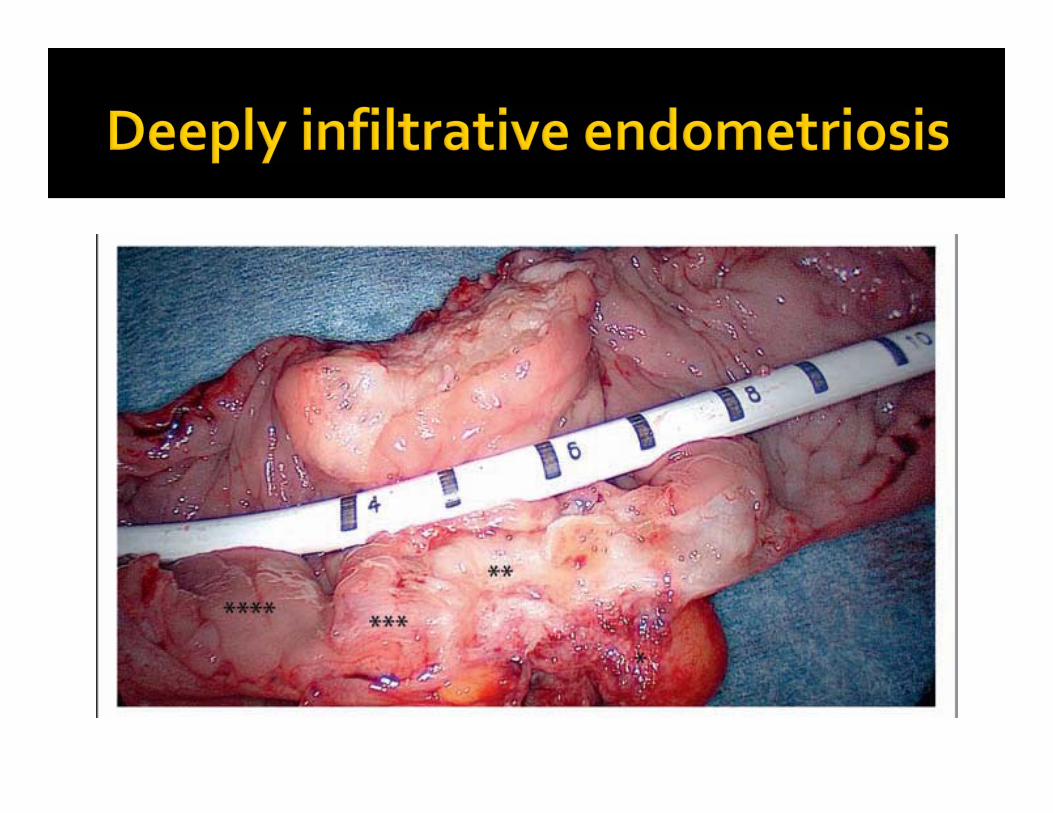
Incidence of bowel endometriosis 5.3‐12% Rectum and Sigmoid are most commonly affected with 90% cases in this area
Common symptoms include pelvic pain, dyschezia (especially during menses), deep dyspareunia and less frequently rectal bleeding
Diagnosis can be made by clinical exam, MRI, transvaginal ultrasound, transrectal ultrasound, virtual CT colonoscopy or Barium Enema

What causes these symptoms? Anterior or lateral fixation of the rectum to adjacent structures Rectal stenosis (more likely at rectosigmoid junction) Cyclic inflammation of the rectal wall, causes▪ Diarrhea▪ Dyschezia▪ Feeling of incomplete bowel emptying during menstruation
Concurrent IBS, Crohn’s and Ulcerative Colitis are fairly common
Some GI symptoms therefore may not be from endometriosis
Removing an endometriosis nodule may not improve GI symptoms
Constipation usually does not improve There is usually significant improvement in dyspareunia, pelvic pain and dyschezia after surgery
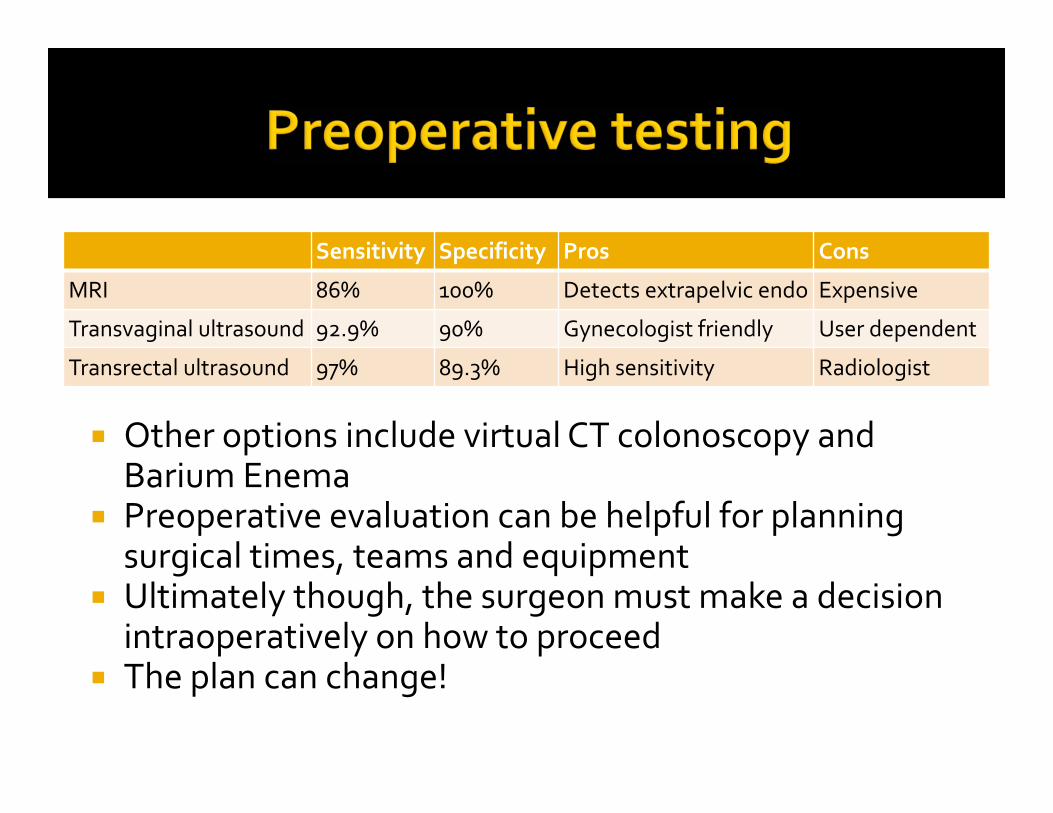
Sensitivity Specificity Pros Cons
MRI 86% 100% Detects extrapelvic endo Expensive
Transvaginal ultrasound 92.9% 90% Gynecologist friendly User dependent
Transrectal ultrasound 97% 89.3% High sensitivity Radiologist
Other options include virtual CT colonoscopy and Barium Enema
Preoperative evaluation can be helpful for planning surgical times, teams and equipment
Ultimately though, the surgeon must make a decision intraoperatively on how to proceed
The plan can change!


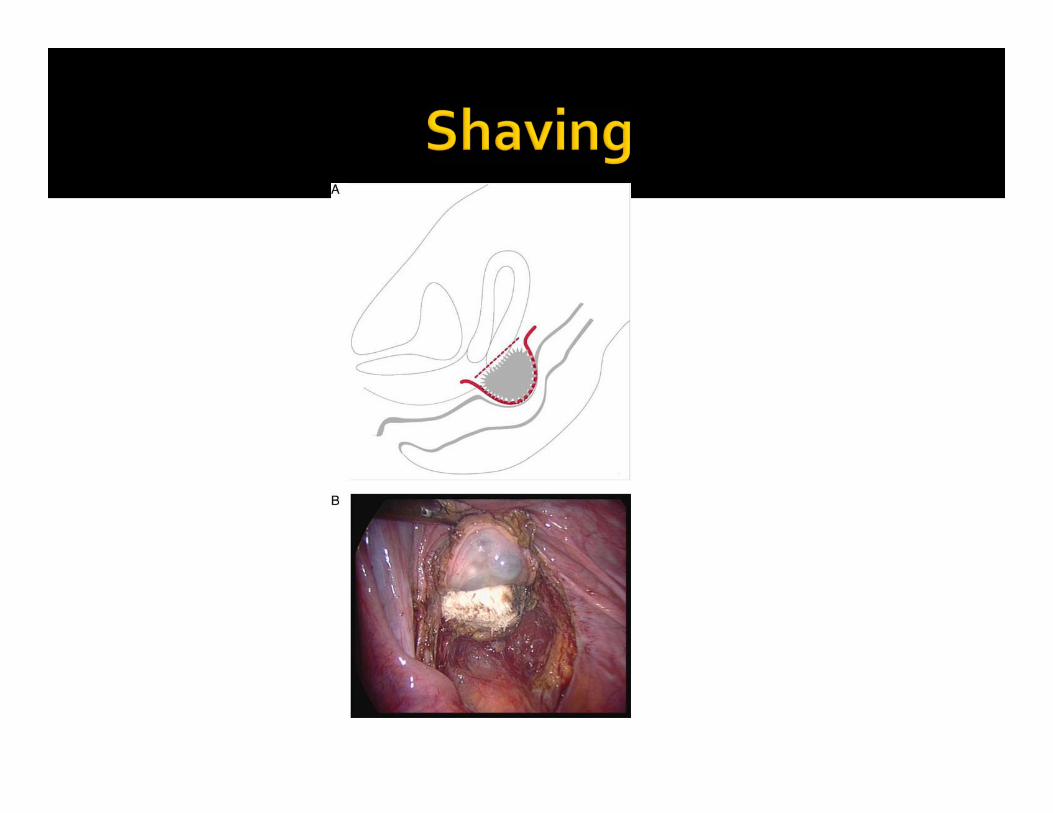
Laparoscopic shaving Partial or down to mucosa
Laparoscopic rectosigmoid discoid resection Segmental resection
Lesion size Repair Pros Cons
Shaving <1 cm Suturing Simple Not radical
Discoid <3 cm Circular stapler Simple Not radical
Segmental >3 cm Stapler Radical (?) Complications
Least invasive Effective A recent prospective series of 500 patients with mean follow up of 3.1 years showed high rates of symptom resolution, low recurrence rates (8%), high pregnancy rates (84%) and low complication rates
Mean lesion size 3.4 cm (range 2‐6 cm) Can be performed by the gynecologist Not as radical as resection
Donnez et al. Human Reproduction 2010;25(8):1949-58
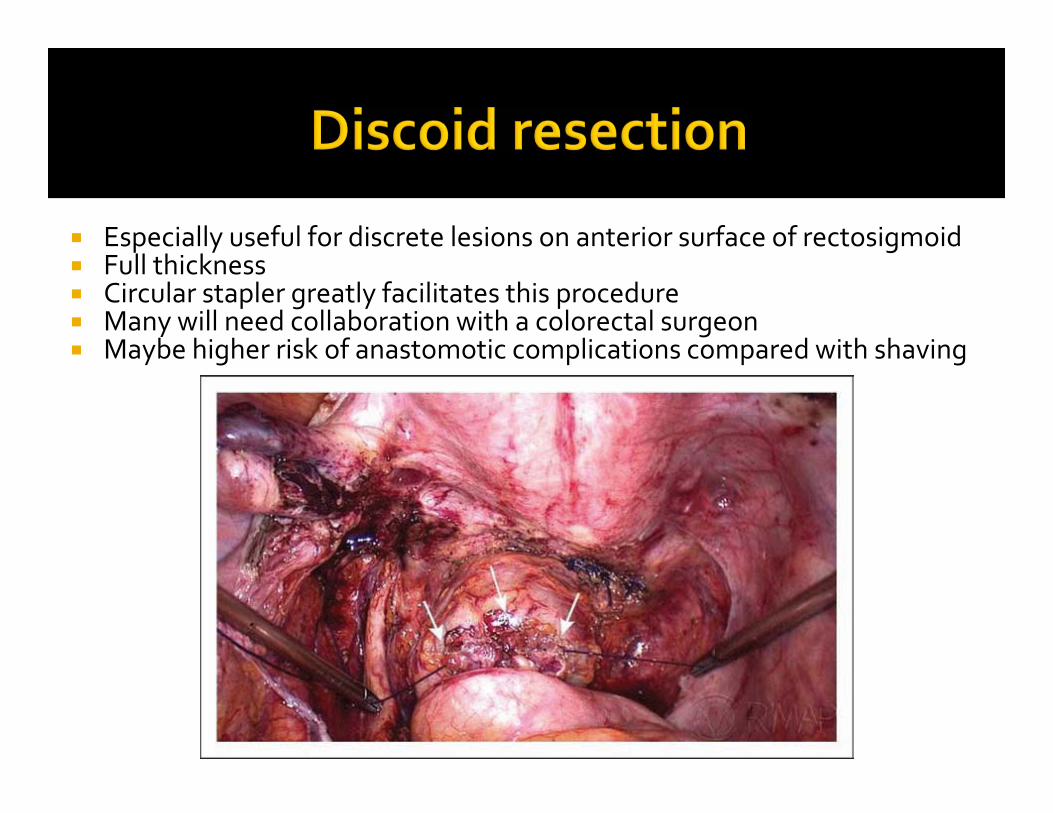
Especially useful for discrete lesions on anterior surface of rectosigmoid Full thickness Circular stapler greatly facilitates this procedure Many will need collaboration with a colorectal surgeon Maybe higher risk of anastomotic complications compared with shaving


For larger lesions or significant narrowing (>60‐80%) of the bowel lumen
Most often requires a team of colorectal and gyn surgeons Higher complications rates, but perhaps lower recurrence rates?


Segmental resection Shaving
Ureteral injury 0.9‐4% 0.8%
Anastomotic leak 3.5% 0%
Conversion to laparotomy 3‐11% 0%
Severe anastomotic stenosis 3% n/a
Rectovaginal fistula 3‐9% 0%
Sepsis and/or pelvic abscess 2‐4% 0%
Median operating time (min) 312 (60‐720) 78 (50‐218)
Rectal perforation 0.4 1.4%
Temporary urinary retention 3‐19.9% 0.8%
Primary temporary ileostomy 14% 0%


Repeat surgery was performed in 12 (2.4%) women after the shaving technique 7 nodule resections 3 segmental bowel resection 2 discoid resection
Recurrence of pelvic pain Overall 7.8% Women who got pregnant after surgery 3.6% Women who did not get pregnant after surgery 15.7%

Reported between 6‐20% Follow up variable A retrospective cohort study at one center compared women who had segmental resection vs women who underwent only “endometriosis removal”
Average follow up was 4 years The most common reason for not performing a bowel resection in patients with rectovaginalendometriosis was lack of adequate surgical consent
Stepniewska et al. Fertil Steril 2010;93:2444-6.

RCT between bowel resection and shaving Enrollment complete (60 total) Pts with symptomatic rectal endometriosis and at least on nodule >20 mm, less than 15 cm from the anus and less than 50% rectal circumference
Primary outcome; major constipation, increased stool frequency, anal incontinence, dysuria and bladder atony
Results presented at ESGE 2016 indicate similar efficacy

Mean follow up 80 months 49 patients had shaving and 25 colorectal resection
Patients had better quality of life and higher scores on GI QOL index after shaving
There were 8.7% recurrences after shaving This indicates that avoiding recurrence for one patient requires 11 patients to undergo a bowel resection
Roman et al. Am J Obstet Gynecol 2016;215:762.e1-9
The bladder or ureter are only involved in 1% of women with endometriosis
Specific symptoms are lacking Often an incidental finding during surgery for pelvic pain
Endometriosis of the ureter is usually involving the ureteric wall and only rarely is the mucosa involved
Ureteric endometriosis is clinically relevant when associated with ureteral stenosis and consequent hydroureter or hydronephrosis
Symptoms Flank pain (25%) Gross hematuria (15%) Asymptomatic (50%)
Suspect if large (>3 cm) rectovaginal lesion Renal ultrasound is a good first line test CT urogram is very helpful to map out the lesion
Surgical therapy is first line
Stenting should be the first step if resection is planned
Ureterolysis can be adequate if the disease is not infiltrating into the wall of the ureter
End to end anastomosis is often feasible If unable to perform without significant tension (lesion > 4 cm) then proceed to Psoas hitch Boari flap Ureteroneocystostomy


Symptoms include Frequency Urgency Dysuria Bladder spasms Hematuria
Diagnosis can be made by Pelvic ultrasound Pelvic MRI
Segmental bladder resection is the treatment of choice
Lesions at the bladder dome are more common and easily resected and repaired
Keep catheter in for 7‐10 days post op Can perform retrograde cystogram to confirm bladder integrity at that time
If the lesion is near the trigonal area, stentingis recommended and concurrent cystocopicguidance is advisable during the resection

Risk of complications Risk of recurrence Multi‐factorial causes of pain – the endometriosis may not be causing the pain
A multidisciplinary approach is preferable We have a good relationship with Pain clinic GI Physical therapy Urology

2
Surgical Treatment of Endometriosis: A 7‐Year Follow‐up on the Requirement for Further Surgery.Shakiba, Khashayar; Bena, James; McGill, Kimberly; Minger, Jill; Falcone, Tommaso
Obstetrics & Gynecology. 111(6):1285‐1292, June 2008.DOI: 10.1097/AOG.0b013e3181758ec6
Fig. 1. Reoperation‐free survival estimates are shown for groups defined by surgery type and ovary preservation.Shakiba. Surgical Treatment of Endometriosis. Obstet Gynecol 2008.
240 patients Removal of ovaries in the 30‐40 year age group did not affect risk of recurrence
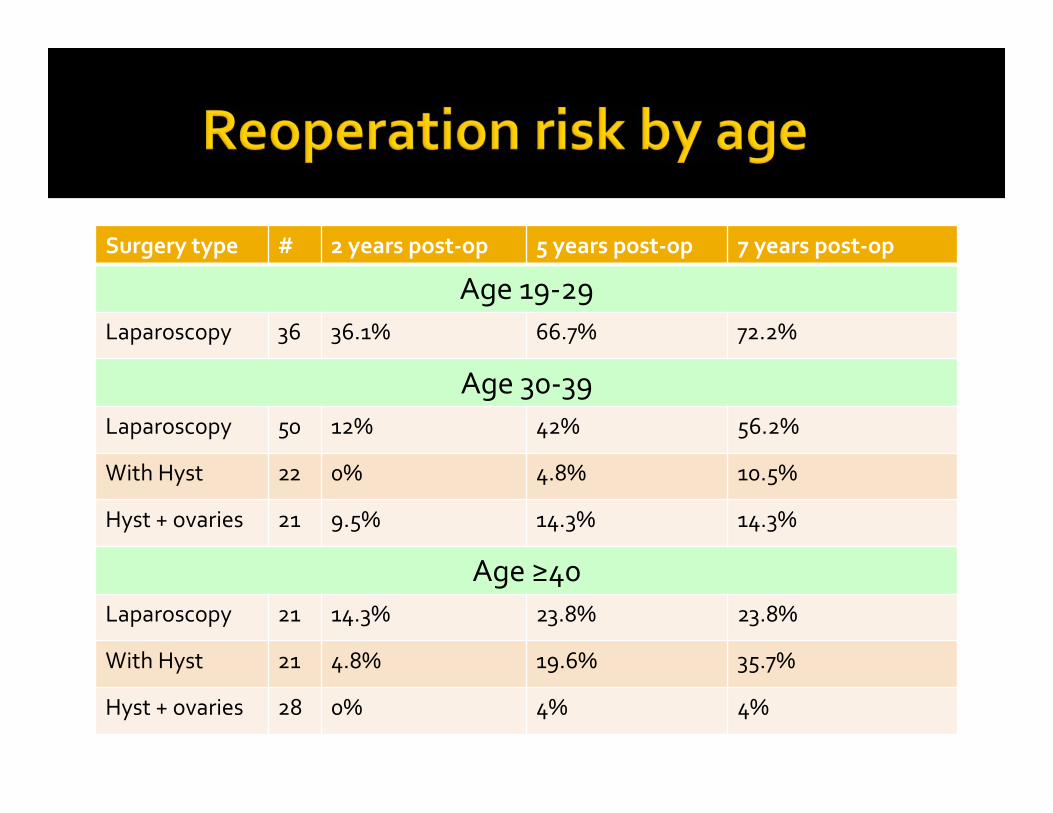
Surgery type # 2 years post‐op 5 years post‐op 7 years post‐op
Age 19‐29Laparoscopy 36 36.1% 66.7% 72.2%
Age 30‐39Laparoscopy 50 12% 42% 56.2%
With Hyst 22 0% 4.8% 10.5%
Hyst + ovaries 21 9.5% 14.3% 14.3%
Age ≥40Laparoscopy 21 14.3% 23.8% 23.8%
With Hyst 21 4.8% 19.6% 35.7%
Hyst + ovaries 28 0% 4% 4%

First line therapy Continuous OCPs NorethindroneAcetate Mirena IUD
Second line therapy GnRHa with add‐back▪ Norethindrone▪ Combined E+P
Depo‐provera Third line therapy Aromatase inhibitors Danazol Progesterone antagonists

Excision of endometriosis can be challenging Conversion to a laparotomy does not equal defeat
Doing nothing may be the best thing to do in some cases – then refer to a specialist
Master retroperitoneal anatomy – videos, cadaver courses, observe surgeries, participate in advanced cases
Proceed carefully, calmly and remain in control at all times

Daraï E, DubernardG, Coutant C, Frey C, Rouzier R, Ballester M. Randomized trial of laparoscopically assisted versus open colorectal resection for endometriosis: morbidity, symptoms, quality of life, and fertility. Ann Surg. 2010 Jun;251(6):1018‐23.
Donnez J, Squifflet J. Complications, pregnancy and recurrence in a prospective series of 500 patients operated on by the shaving technique for deep rectovaginal endometriotic nodules. Hum Reprod. 2010 Aug;25(8):1949‐58
Stepniewska A, Pomini P, Guerriero M, Scioscia M, Ruffo G, Minelli L. Colorectal endometriosis: benefits of long‐term follow‐up in patients who underwent laparoscopic surgery. Fertil Steril. 2010 May 1;93(7):2444‐6.
Shakiba K, Bena JF, McGill KM, Minger J, Falcone T. Surgical treatment of endometriosis: a 7‐year follow‐up on the requirement for further surgery. ObstetGynecol. 2008 Jun;111(6):1285‐92