icu acquired weakness: role of specific nutrients · icu acquired weakness: role of specific...
TRANSCRIPT

ICU Acquired Weakness: Role of Specific Nutrients
Dr Jonathan TAN Senior Consultant
Dept of Anaesthesiology, Intensive Care & Pain Medicine Tan Tock Seng Hospital, Singapore

Purpose?
Healthcare professionals? Nutrition Therapy?
“Are we creating survivors?... Or
victims”

ICUAW
Generalised muscle weakness developing during ICU stay; acute critical illness
“Loss of flesh and strength” Osler W 1892 Critical illness Polyneuropathy; CIP Critical illness Myopathy; CIM Retained sensory function Post Intensive care syndrome ;PICS
Hermans & Van den Berghe Critical Care 2015

ICUAW: OUTCOMES
Prolonged ICU, Hospital LOS Prolonged Mech Ventilation Increased Hospital and ICU Mortality ARDS survivors: weakness and decline at 1,
2, 5 years post ICU discharge Functional survival limited!
Hermans & Van den Berghe Critical Care 2015 Herridge et al NEJM 2003 & 2011 Needham et al Eden trial 1 year follow up AJRCCM 2013 Fan E et al CCM 2014
ICUAW
Patients ventilated > 10days: ICUAW up to 67% with 25% still weak after a week
ICUAW of 11% in ICU > 24hrs; 24-55% when in ICU 7-10days
ARDS: ICUAW 60% at awakening and 36% at hospital discharge
Common!
Hermans & Van den Berghe Critical Care 2015

Pathophysiology Complex functional, structural
alterations in nerves and muscles Sepsis mediated microvascular effects Mitochondrial dysfunction Hyperglycaemia Protein catabolism, muscle atrophy - Inflammation; Immobilisation; endocrime
stress response; nutrition deficit; microcirculation; dennervation
Pathophysiology
Altered excitation – contraction coupling Deficient Autophagy

Risk factors SEPSIS MOF Drugs: Corticosteroids,
aminoglycosides, NMBs, Vasopressors Hypergylcaemia Immobilisation Premorbid nutrition deficit and functional
status; Frailty; Sarcopenia Mech ventilation induced diaphragmatic
atrophy

Diagnosis Scoring systems Handgrip strength Respiratory muscle strength Muscle ultrasound: atrophy detection;
but muscle size not correlated with function Electrophysiological testing Clinical Biomarkers???

Prevention / Treatment Aggressive Sepsis management Avoid risk factors Glycaemic control with Insulin ICU Early Mobilisation strategies Nutrition strategies
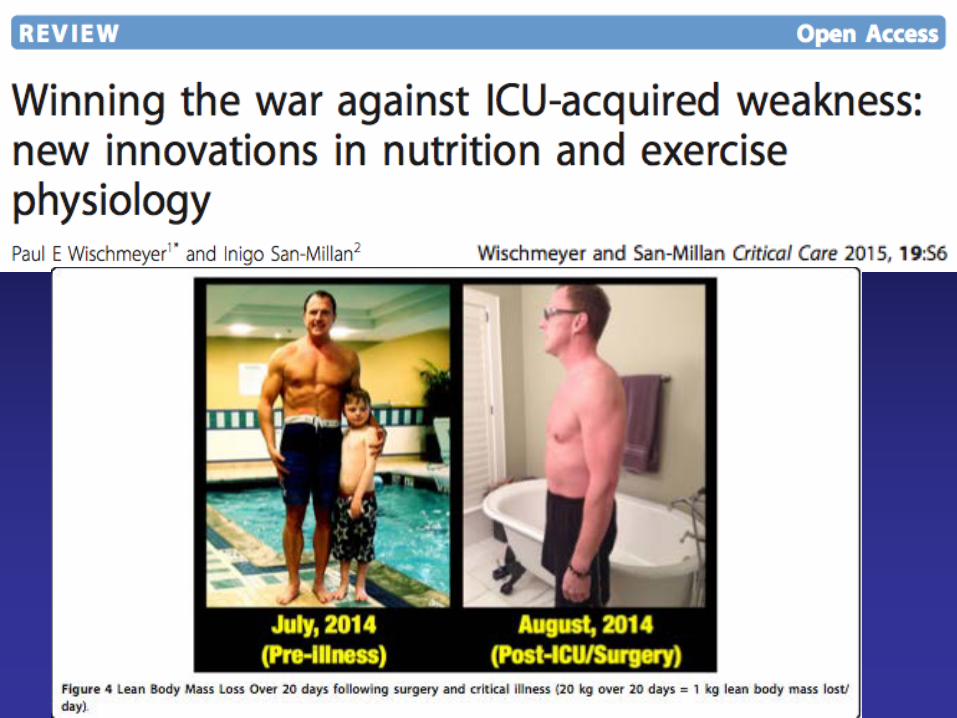
Lean body mass preservation Recovery of muscle mass and
function

ICU-Acquired Weakness Sarah E. Jolley, MD; Aaron E. Bunnell, MD; and Catherine L.
Hough, MD. CHEST 2016; 150(5):1129-1140
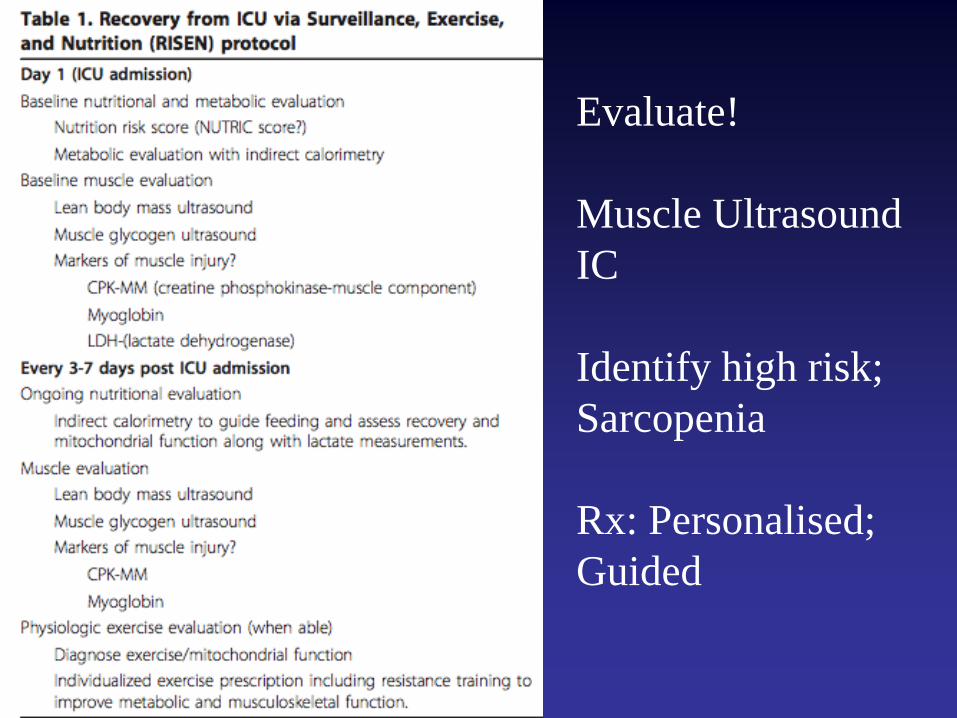
Evaluate! Muscle Ultrasound IC Identify high risk; Sarcopenia Rx: Personalised; Guided

Beyond 101… Should THIS patient survive? Evolution
and survival of the fittest Autophagy and trophic or intentional
underfeeding HMB Anabolic & Anticatabolic agents Mitochondrial failure Specific nutrient magic bullets?

Optimal Nutrition & Protein: “DuH”??!!!!!
• ASPEN; ESPEN; Canadian; Local… • EN vs PN • Commence within 48hrs • IC vs weight based vs equation: calorie target • 1.2- 2.0g/protein/day; 1.3-1.5g/kg • Minimise Interruptions • Minimise caloric debt
• Prescribed vs Reality

Optimal feeding Recent trials advocate early ICU
intentional underfeeding; trophic feeding INS Data: how are YOU doing? < 50% prescribed: Mortality risk up Every 25% increase in calorie delivery
in 1st week incr 3 month post ICU SF36 Calories vs Protein: under vs enough Trials with protein delivery of
>1.0g/kg/day show benefit in the higher nutrition delivery group

Platelet Function!!??

Autophagy
• Inhibition of autophagy by early nutrition therapy (protein) : reduces tolerance to oxidative stress; incr risk of organ failure
• Avoid early mandatory feeding to preserve autophagy




Optimal feeding Avoid hypergylcaemia: Insulin therapy Avoid over feeding; inappropriate PN Optimal feeding: maintaining autophagy
while promoting protein synthesis via mTOR pathway Optimal. Personalized. Timing, Amount,
Escalation, Route, Constituents….. Coupled with Optimal Rx

The Right “Whey” Highest biological value protein type Non Coagulating Higher Cysteine and Leucine Preserve muscle mass better May increase muscle synthesis Intermittent bolus feeding + Omega 3
FA Confirmation in trials needed Marik PE. Feeding critically ill patients the right ‘whey’: thinking outside of
the box. A personal view. Ann Intensive Care. 2015;5:11.

HMB
Metabolite of Leucine (20g to 1g) Increases lean body mass with plateau
effects in trained atheletes Prevent muscle loss with bed rest, increased
skeletal muscle mass or secondary measures of function?
Stabilization of cholesterol membrane in muscle cell?
2-3g/day safe; effective?



Protein
Duration? Muscle mass +++/- Function ++/- Criticall ill: Inflamm markers decreased
but no muscle or functional data

Promising? Need a well designed RCT in Critically
ill…

Anabolic; Anticatabolic
• Anticatabolic: Beta Blockers • Burns; “De-Cathecolamine” • Anabolic: Oxandrolone • Reduce LOS, faster wound healing,
improved survival in burns patients • WHEN? Evidence of glycogen stores
increasing signal switch to anabolism?

Defining current STANDARD of care is difficult Much current areas of uncertainty Top 10 trials for next 10 years
suggested, rated

Substrate requirements: proteins, carbohydrates, and micronutrients What is optimal protein dose in general and
nutritionally high-risk patients Is there any interrelationship between calorie
and protein “dose”? What is the amount of substrate that is
actually absorbed in critically ill patients given gut dysfunction and malabsorption?
What is the role of whey-based protein (high in leucine) in muscle synthesis and facilitating recovery from critical illness?

What combinations of amino acids are optimal: should they mimic “normal” intake or be aimed at inducing metabolism or supporting hostdefense What is the role of small peptide vs
polymeric formulae in patients at high risk of intolerance? What is the appropriate amount of
micronutrients to be provided in ICU patients?

Nutrition and functional recovery What is the best way to measure the effect of
nutrition on physical recovery outcomes of survivors of ICU?
Is there a role for bedside measures to monitor the impact of feeding practices on muscle (such as blood, urine, or muscle imaging) and how to correlate these measures with long-term functional and vital outcomes?
What is the effect of combination of ranges of proteins + physical activity + monitoring of muscle mass/function?


What do I do now????


Conclusion Do ALL the BASICS of critical care right Focus on current guidelines and what
we know is safe Enough, is good. More? Not necc…. Specific assessment and plan for the
patient and the resources available Prescribed vs Delivered! New knowledge fast and furious: keep
coming to PEN meetings! “Functional Living”
