icu perspectives in maternity critical care
TRANSCRIPT
Dr..Carl Waldmann Royal Berkshire Hospital
Reading
ICU perspectives in Maternity Critical care
October 5th 2018
Gary Masterson&
Audrey Quinn


8 MILLENIUM DEVELOPMENT GOALS
• Eradicate extreme poverty and hunger• Promote gender equality and empower women• Achieve universal primary education
• Reduce child mortality• Improve maternal health• Combat HIV/AIDS and other diseases• Ensure environmental sustainability• Develop a global partnership for developmentWHO involvement in patient safety starting in ICU

WHO AM I
• Consultant ICM and Anaesthesia
• Dean FICM
• Sat on the Multidisciplinary Group looking
at care for the pregnant and recently
pregnant individuals
• P/T work for Leyton Orient
• ID 10 T tab

ID 10 T
IDIOT


WHERE DO I WORK

Enlightened employersQuakers gained
favour with consumers due to their ethical business practises, Quaker principles
such as truth telling,simplicity and
fair pricing
ROYAL BERKSHIRE HOSPITALREADING
Background• Our ICU until recently– 17 bedded general
unit – Clinical Information
System• Staffing structure
– 10 intensivists5 anaesthetists 5 physicians– Nursing staff work
internal rotation – 24/7 Outreach service– Follow-up Clinic– TCCDG includes
Maternity representation
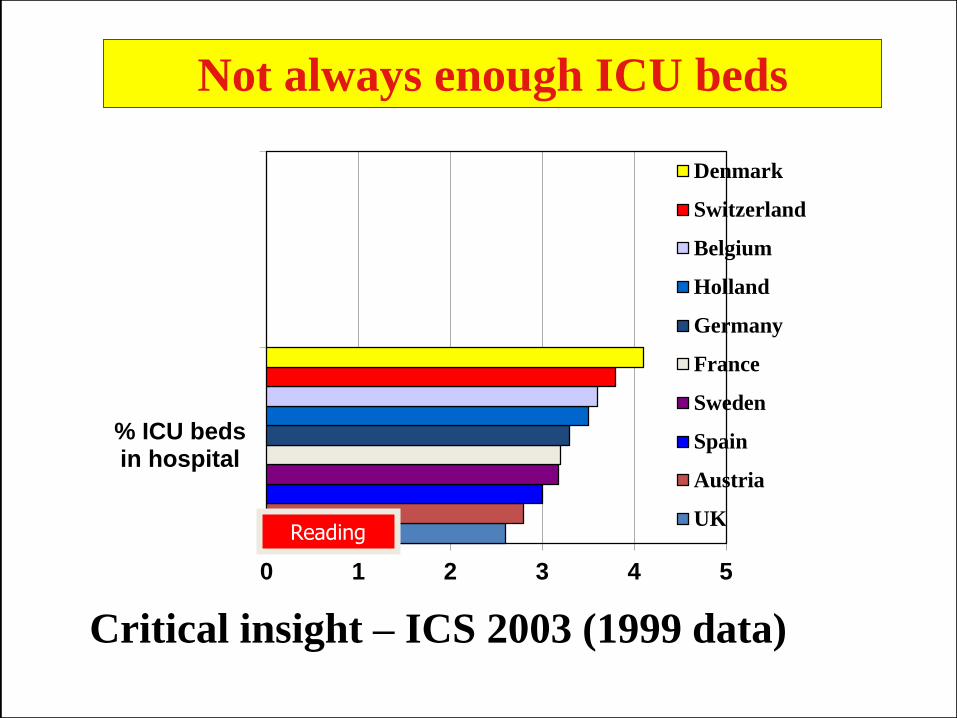
0 1 2 3 4 5
% ICU bedsin hospital
Denmark
Switzerland
Belgium
Holland
Germany
France
Sweden
Spain
Austria
UK
Critical insight – ICS 2003 (1999 data)
Not always enough ICU beds
Reading

ICM ALSO REFERRED TO AS CRITICAL CARE MEDICINE, IS A BODY OF SPECIALIST KNOWLEDGE AND PRACTICE RECOVERING FROM POTENTIALLY LIFE-THREATENING FAILURE OF ONE OR MORE OF THE BODY’S ORGAN SYSTEMS. IT INCLUDES END-OF-LIFE CARE, AND THE SUPPORT OF FAMILIES. IT INCLUDES OUTREACH AND POST-INTENSIVE CARE REHABILITATION
WHAT IS INTENSIVE CARE

LEVELS of CAREIntensive Care Society © 2009
• ICU HDU
• Now Level 0 1 2 3
Dr J Eddleston
Dr D Goldhill
Dr J Morris Chair
Not terribly useful in
Obstetrics
Maternal Critical Care
• ICNARC data has until recently not been sensitive enough to tell the story
• Big Issue
The Big Issue

Admission Diagnoses Reading ICU27 cases
• PPH 14
• APH 1
• RUPTURED UTERUS 1
• SEPSIS 1
• HELLP 4
• ECLAMPSIA 4
• FATTY LIVER 2
51 days total ICU care
Interventional
radiology

FLU H1N1
• The BMJ(2010;340:c1279) published the results of a study of women who were more than 20 weeks pregnant and suffering from 2009 H1N1 influenza in Australia and New Zealand.
• 13 times more likely to become critically ill



HONG KONG ICM exam
Long case was on Obstetric
haemorrhage

Florence Nightingale 1863
“In attempting to arrive at the truth, I have applied everywhere for information, but in scarcely an instance have I been able to obtain hospital records fit for any purpose…. If obtained…they would show subscribers how their money was spent…..’’

21
Manual flowsheet documentation


MBRRACE-UK

Conclusions
• “Equity of Care (2011)” Recommendations have failed to be implemented.
• Some patients cannot be moved to critical care
• Midwives not trained in critical care, directentry to Midwifery Training
• General view that most delivery suites cannot currently deliver level 2 care

• Obstetricians don’t do critical care
• Obstetric Anaesthetists do maternal critical care and need to keep up skills
• Need a flexible solution – one size won’t fit all
• Solution should be competency based rather than speciality based
Conclusions 2

KEY PUBLICATIONS IN 2017 INTENSIVE CARE is now a speciality in its own right.

What is happening in ICU ?
• Population Elderley, OBESE, EoL care
• Sepsis & Bundles
• Thromboprophylaxis v Bleeding
• TECHNOLOGY
• Winter pressure, Terrorism
• REHABILITATION & FOLLOW-UP
• Critical Futures FACULTY
• GIRFT GPICS HBN 04-02
• Maternity Critical Care


• Consultantreview in 14hours
• Formal handovers
• Access to Critical Care
• 24/7 Outreach

The Angel Catheter
Pregnancy increases the risk of VTE by 5 times
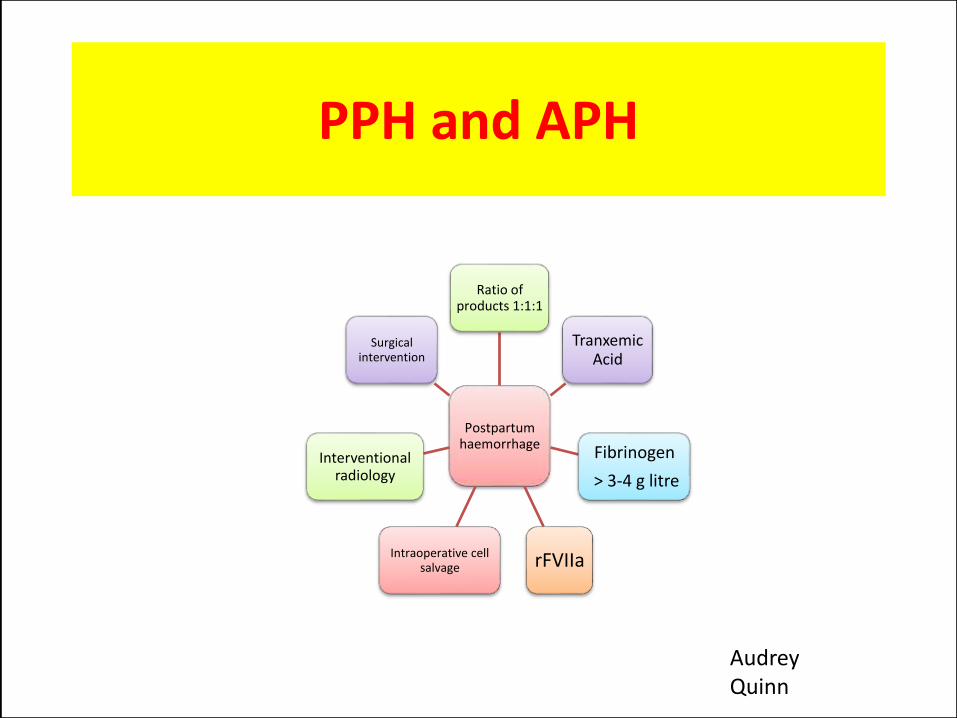
PPH and APH
Postpartum haemorrhage
Ratio of products 1:1:1
Tranxemic Acid
Fibrinogen
> 3-4 g litre
rFVIIaIntraoperative cell salvage
Interventional radiology
Surgical intervention
Audrey Quinn

Case JM• LSCS uneventful
• At end of procedure she failed to stabilise fluids.Bleeding Major Haemorrhage.
• Laparotomy- haemoperitoneum
• Packs, Clotting factors, Tr Acid
• Rusch Balloon,
• Interventional Radiology, Splenic Artery Aneurysm. Over weekend 2 more visits to Xray.



IT
Data for obstetrics is lacking

The pressures in critical care are intense across the board,” said Dr Gary Masterson, president of the
Intensive Care Society. “This is a bad winter, it’s the worst since 2010 when we had the H1N1 (swine flu) outbreak
There is more to life than measuring death
King’s Fund Report
Q O L REHABILITATION
PSYCHOLOGICAL
PHYSICAL


o
C I PCritical Illness Polyneuropathy
Rehabilitation in ICU
Sarah Eli, Royal Berkshire Hospital
4
12
5
3
0
CPAX Eve Corner



Getting It Right First Time
ACCPs

Diurnal rythmsSleep deprivation
BABY FRIENDLY!!



Key Messages
• Working in Teams
• Enhanced maternal care
• Education and training
• Early Warning score modified for obstetrics
• Where care is delivered
• Care on ICU rapid access to Obstetric expertise
• Follow up
• Dataset for QI project



Roto-Rest ™130 degrees total arc
65 degrees per side
ROTOPRONE


0
5
10
15
20
25
30
35
40
6 ml/kg
12 ml/kg
% M
ort
ality
ARDSnet mechanical ventilation protocol
results: mortality
Adapted from Figure 1, page 1306, with permission from The Acute Respiratory Distress
Syndrome Network. N Engl J Med 2000;342:1301-1378
PROTECTIVE VENTILATION
STRATEGY

CT
• 29 year old female
• PMH: 2009 stillborn was suing RBH
• Seen in antenatal clinic at Basingstoke
• Vaginal delivery at 40 +1
• Labour from 02.00
• Delivered 05.50
• Placenta 06.30 “ragged”

CT
• Bleeding++PV 13.15• 13.30, collapsed, midwife arrives at 13.50• 999 at 13.57 • At scene 14.03 – PEA→VF →ALS• Arrived at hospital at 14.35 in A&E• ROSC 14.48• Gas at 14.43: pH 6.3/ pO2 9.98/ pCO2 4.37/ Lac 23/
HCO3 1.9/ Hb 5• Placenta evacuated & manual compression
3rd degree tear sutured & Rusch balloon

CT
• To theatre →Subtotal hysterectomy 18.30
• Total: 25 units RBC, FFP 12 units, cryo 8 units and platelets 2 units
• Transferred to ICU post op at 19.30
• High dose inotropes
• Certified dead at 21.17

Summary
• Get patients the right care, at the right time, delivered by the right people in the right place
• Maternity Team (particularly obstetric anaesthetist) & Critical Care work together
• Enhance care on Delivery Suite (particularly for midwives) with EMC
• Crit Care input for non-EMC patients





27.09.18
Carter: ‘Vital’ improvements to tech,
fleets needed to save £50m

PneuX Pneumonia Prevention System

ORIGINAL ARTICLEVentilation with Lower Tidal Volumes as
Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome
The Acute Respiratory Distress Syndrome NetworkN Engl J Med 2000; 342:1301-1308May 4, 2000
VV CO2 removal
PRONE

Evidence
GPP Recommended good practice based on the clinical experience of the multidisciplinary working group


Recommendations
1.1 Obstetric units appoint lead clinician for the care of critically ill women.
1.2 Establish training resources to enable staff to achieve and maintain skills in EMC.
1.3 Women should have access to healthcare professionals who are EMC competent
1.4 The individual competence required should be recorded by the maternity team
1.5 The lead clinician participates in the hospital’s critical care delivery group
1.6 Escalation to critical care clearly defined, includes multidisciplinary discussion.
1.7 Outreach available and provides support and education delivering EMC.
1.8 Obstetric units should be part of the regional maternal critical care network .