ifad antwerpen 2014 azriel perel professor of anesthesiology and intensive care sheba medical...
TRANSCRIPT

IFAD Antwerpen 2014
Azriel Perel
Professor of Anesthesiology and Intensive Care
Sheba Medical Center, Tel Aviv University, Israel
Rational Perioperative
Goal-Directed Therapy (GDT)

Disclosures
Member of the Medical Advisory Board of
Pulsion Medical Systems,
Germany
Consultant to IMACOR, USA
Speaking fees from Masimo, USA


The mortality rate for patients undergoing non-cardiac surgery is higher than anticipated.
There is a need for strategies to improve care for this group of patients.

A variety of proactive therapeutic strategies
that aim to achieve better patient outcome
by improving the hemodynamic status in the
perioperative period, especially in high-risk
patients undergoing non-cardiac surgery.
Perioperative goal-directed therapy (GDT)
A bolus of 200 ml colloid is administered over 2 min, and 5 min later the stroke volume (SV) is assessed.
The procedure is repeated if there was an increase in SV of >10%.
When the fluid bolus does not result in a SV increment >10%, optimization is regarded as achieved.
The basic technique - SV optimization

Fluids should be given to increase CO, and inodilators added once the patient is no longer fluid (preload) responsive or not achieving the following goals:
CI > 4.5 L/min/m2
DO2I ≥ 600 ml/min/m2
GDT aimed at ‘supra-normal’ values of oxygen delivery
“It may be considered unethical not to use goal-directed perioperative therapy”
A preemptive strategy of hemodynamic monitoring and
coupled therapy reduces surgical mortality and
morbidity.
The mortality benefit of GDT was confined only to the subgroup of patients at extremely high risk of death.
The reduction of complication rates was seen across all subgroups of GDT patients.

GDT may improve long-term outcomes, in part due to its ability to reduce the number of peri-operative complications.

Crit Care Med. 2014 May;42(5):1194-203.

The oesophageal Doppler monitor ‘‘should be considered for use in patients undergoing major or high-risk surgery…(since its use is associated with) a reduction in post-operative complications, use of central venous catheters and in-hospital stay…The cost saving per patient…is about £1100 based on a 7.5-day hospital stay.’’
There is a considerable gap between the
accumulating evidence about the benefits of
perioperative hemodynamic optimization
and its clinical implementation in both
Europe and the US.
And yet…

This large body of evidence cannot be simply ignored, and, therefore, puts the pressure on clinicians to either adopt GDT strategies or find a good reason for why they do not.
One such reason may be the remaining doubt that many clinicians still have about the robustness of the concept and the quality of the evidence supporting it.
Perioperative Goal-Directed Therapy: Some remaining questions
Azriel Perel (in press)
The evidence behind GDT
is still being questioned





Goal-directed fluid therapy to near-maximal SV guided by ED adds no extra value to fluid therapy using zero balance and normal body weight in patients undergoing elective colorectal surgery.
Intraoperative SV optimization conferred no additional benefit over standard fluid therapy.
In an aerobically fit subgroup of patients, GDT was associated with detrimental effects on the primary outcome.
GDT focusing on SV maximization may have important limitations including a risk of iatrogenic fluid overload which may be associated with prolonged hospital stay.

GDFT did not provide clinical benefit in
patients undergoing elective colectomy
within a protocol incorporating fluid
restriction.

RCT including 142 patients in 6 hospitals. GDT including fluids and vasoactive drugs based on noninvasive CO monitor was compared with standard practice.
GDT was not associated with a decrease in the incidence of overall complications or LOS.
Anesth Analg. 2014 Sep;119(3):579-87
In a randomized trial of high-risk patients undergoing major GI surgery, use of a CO–guided hemodynamic therapy algorithm compared with usual care did not reduce a composite outcome of complications and 30-day mortality.
However, inclusion of these data in an updated meta-analysis indicates that the intervention was associated with a reduction in complication rates.
JAMA. Published on line May 19, 2014.



The terminology used to describe GDT
is inconsistent and confusing.

There are distinct challenges associated with
the design and conduct of GDT trials which
are not easily solved.
Blinding is an important potential source of
bias and small GDT trials in particular are
vulnerable to bias.

There is an urgent need to evaluate the
pathophysiological mechanisms that are
responsible for the positive results reported
by most clinical GDT studies.

GDT is safe, and can bring both clinical and economical benefits in the greatest-risk patients.
All therapy should be goal directed; the challenge is how to set the right goals.
GDT may now not show the strong difference in outcome observed in the first studies, but it does not mean that we should get rid of it.

Can GDT lead to
detrimental fluid overload?



A reductions in SV of >10% as measured by the E-Doppler has a sensitivity of only 37% in identifying fluid responsiveness, and therefore may be related to other factors aside from preload.
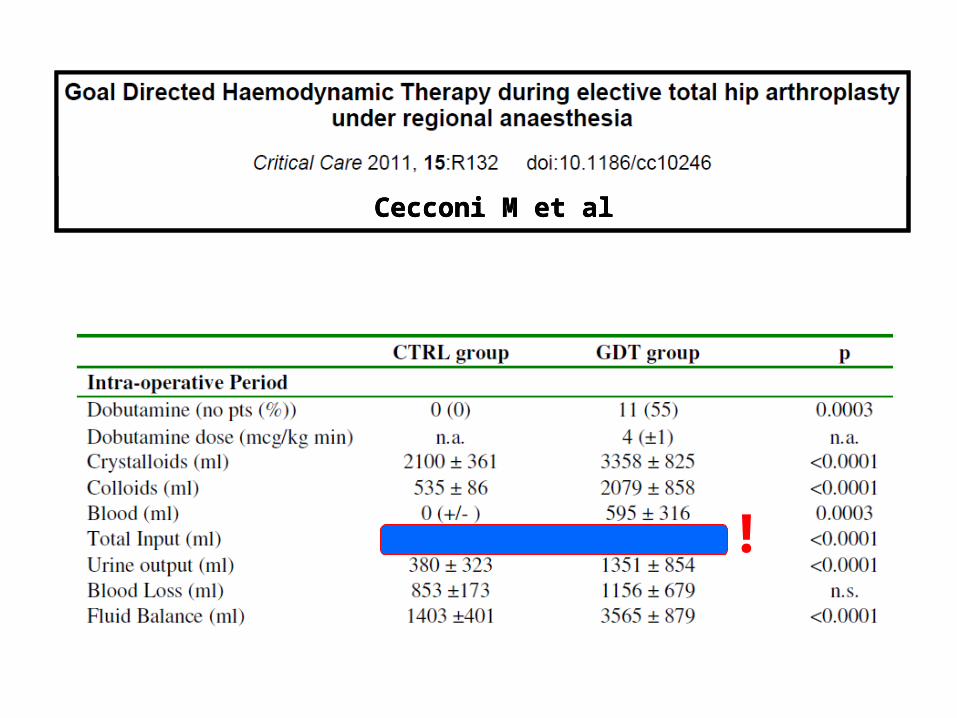
!
Cecconi M et alCecconi M et alCecconi M et al

Cecconi M et alCecconi M et alCecconi M et al

Crit Care Med 1990; 18:728
Patients who had >20% weight gain had more vasopressor dependence and higher mortality.
Our results suggest that the morbidity of fluid overload can be significant, and warrants a fresh look at the methods of intraoperative fluid resuscitation.
Fluid overload occurs early after cardiac
surgery and is associated with prolonged
PICU length of stay and ventilation.
(Crit Care Med 2014; 42:2591–9)

Impact of Different Crystalloid Volume Regimes on Intestinal Anastomotic Stability
Marjanovic G, et al. Ann Surg 249:181-185, 2009
The effect of fluid overload in the presence of an epidural on the strength of colonic anastomoses.Nessim C, et al. J Surg Research 183: 567-573, 2013
Intraoperative crystalloid overload leads to substantial inflammatory infiltration of intestinal anastomoses – a histomorphological analysis
Kulemann B, et al. Surgery 154:596-603, 2013
Volume overload and the risk of anastomotic leaks
Intraoperative use of restrictive fluid management reduces postoperative morbidity and shortens hospital stay.
National Confidential Enquiry into Patient Outcome and Death.
1999 Report: Extremes of Age. http://www.ncepod.org.uk
National Confidential Enquiry into Perioperative Death have highlighted over-hydration as a contributory cause in the genesis of postoperative problems leading to death.
We recommend careful fluid management (the implication being restriction) in vulnerable patients and those most at risk, such as the elderly.

British consensus guidelines on intravenous fluid therapy for adult surgical patients. 2011.
Powell-Tuck J, et al. www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf.
Concern arose from a high incidence of post-operative sodium and water overload, and evidence to suggest that preventing or treating this, by more accurate fluid therapy, would improve outcome.

British consensus guidelines on intravenous fluid therapy for adult surgical patients. 2011.
Powell-Tuck J, et al. www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf.

The real danger in GDT
A forgiving attitude towards aggressive fluid administration may encourage practitioners with inadequate training and experience to simply overload their patients with fluids without appropriate monitoring.

It seems clear that the continued pursuit of hemodynamic goals in patients who do not respond is harmful.
The adverse effects of fluid and inotropic therapy will be most serious for patients with significant heart disease.

It is essential that the GDT approach includes optimization within the limit of the individual patient’s cardiac capacity.
The concept is therefore different from the original Shoemaker concept which used predetermined supra-physiologic values of CI and DO2 as therapeutic goals.

Rational Perioperative GDT (?)
Maximize the value of basic hemodynamic monitoring (BP, PLET, PetCO2).

Hypotension should not serve as an automatic trigger of fluid administration since not all hypotensive events are due to hypovolemia.
A low PetCO2 (relative to the minute ventilation) may be the only(!) sign of low CO.
The combination of BP and capnography is a powerful tool to differentiate between vasodilation and low CO.
The amplitude of the plethysmographic signal is an important source of information about vascular tone and, at times, the nature of hypotension.
Blood pressure + capnography + plethysmography

Rational Perioperative GDT (?)
Maximize the value of basic hemodynamic monitoring (BP, PLET, PetCO2).
Assess fluid responsiveness by following dynamic parameters, when appropriate.

SPV PPV SVV PVI
Benes J,…, Michard F

Rational Perioperative GDT (?)
Maximize the value of basic hemodynamic monitoring (BP, PLET, PetCO2).
Assess fluid responsiveness by following dynamic parameters, when appropriate.
Monitor continuous CO to assess the effects of a fluid challenge in order to avoid fluid overload.
The gold standard to monitor the
response to a fluid challenge is using
continuous CO monitoring.


Rational Perioperative GDT (?)
Maximize the value of basic hemodynamic monitoring (BP, PLET, PetCO2).
Assess fluid responsiveness by following dynamic parameters, when appropriate.
Monitor continuous CO to assess the effects of a fluid challenge in order to avoid fluid overload.
Use more advanced hemodynamic monitoring in the higher-risk patients and procedures.*

High-risk patients should be admitted to an ICU or intermediate care unit
High-risk patients should be admitted to an ICU or intermediate care unit with postoperative monitoring of ScvO2. *

The limitations of a single intervention (fluid
management) to determine outcome have to be
recognized, since many other factors, like type of
anesthesia, ICU availability, early mobilization and
adequate analgesia, may be of even greater
importance.
Perioperative Goal-Directed Therapy: Some remaining questions
Azriel Perel (in press)

Fast-Track Surgery Kehlet H, et al. Ann Surg 248:189, 2008
Enhanced Recovery After Surgery
(ERAS)Knott A, et al. BMJ Open 2, 2012
The Perioperative Surgical Home Kain ZN, et al. Anesth Analg 118:1126, 2014

Conclusions:
The reported benefits of perioperative GDT
are too important to be ignored, but are not
supported by the most recent literature.
Rational perioperative hemodynamic
management should be individualized.
GDT should not lead to a forgiving attitude
towards aggressive fluid administration.
GDT should be viewed as part of a more
holistic approach to perioperative care.
Thank you for your attention!