antwerpen 2011 a zriel perel professor and chairman department of anesthesiology and intensive care...
TRANSCRIPT

Antwerpen 2011
Azriel Perel
Professor and ChairmanDepartment of Anesthesiology and Intensive CareSheba Medical Center, Tel Aviv University, Israel
Techniques for the Future: Continuity versus Accuracy?

Disclosure
The speaker cooperates with the following companies
BMEYE
FlowSense
Pulsion

What are your indicators for volume expansion?
Cardiac output (CO) is the main determinant of oxygen delivery.
Physical examination and vital signs alone often fail to reflect significant derangements in CO.
Many of our therapeutic efforts are aimed at increasing the CO.
The monitoring of CO is therefore very useful for proper decision-making in critically ill and high-risk surgical patients.
Some statements on CO measurement

The main 2 reasons to measure CO are: Identification of patients who have low (or
high) CO values that are not evident clinically.
Measurement of the response to diagnostic and therapeutic interventions.
It is time to consider CARDIAC OUTPUT as just another vital sign!
Because of the complexity of assessment
of clinical variables in septic patients,
direct measurement of CO by invasive
hemodynamic monitoring is advisable.

Perioperative optimization

Nexfin NICOM-3 Doppler
PulsioFlex (ProAQT) Vigileo LiDCOrapid
Are uncalibrated CO monitors accurate enough to guide therapy?

Although PAC, FloTrac, LiDCO and PiCCO display similar mean CO values, they often trend differently in response to therapy and show different inter-device agreement.
In the clinically relevant low CO range (< 5 L/min), agreement improved slightly.
Thus, utility and validation studies using only one CO device may potentially not be extrapolated to equivalency of using another similar device.

This study helps to confirm what is already suspected about the reliability of pulse contour devices; that these devices do not track changes in cardiac output reliably.
There is growing evidence that the pulse contour method is not the solution to providing reliable cardiac output monitoring at the bedside.
Anesthesia Analgesia 2009, 108:707
When evaluating the role of new CO devices in clinical care, the fundamental question is whether the new device can replace thermodilution CO measurement as a guide to clinical decisions.
Despite the large number of studies evaluating new CO devices, few, if any, answer this fundamental question.
Anesthesia Analgesia 2009, 108:707
When evaluating the role of new CO devices in clinical care, the fundamental question is whether the new device can replace thermodilution CO measurement as a guide to clinical decisions.
Despite the large number of studies evaluating new CO devices, few, if any, answer this fundamental question.
A. Maximize the information that can be provided by real-time continuous measurements
How should we deal with the inaccuracies and limitations of our
monitored parameters?

The power of Continuity
The analog signals often contain vital
information that is not provided by the digital
values.
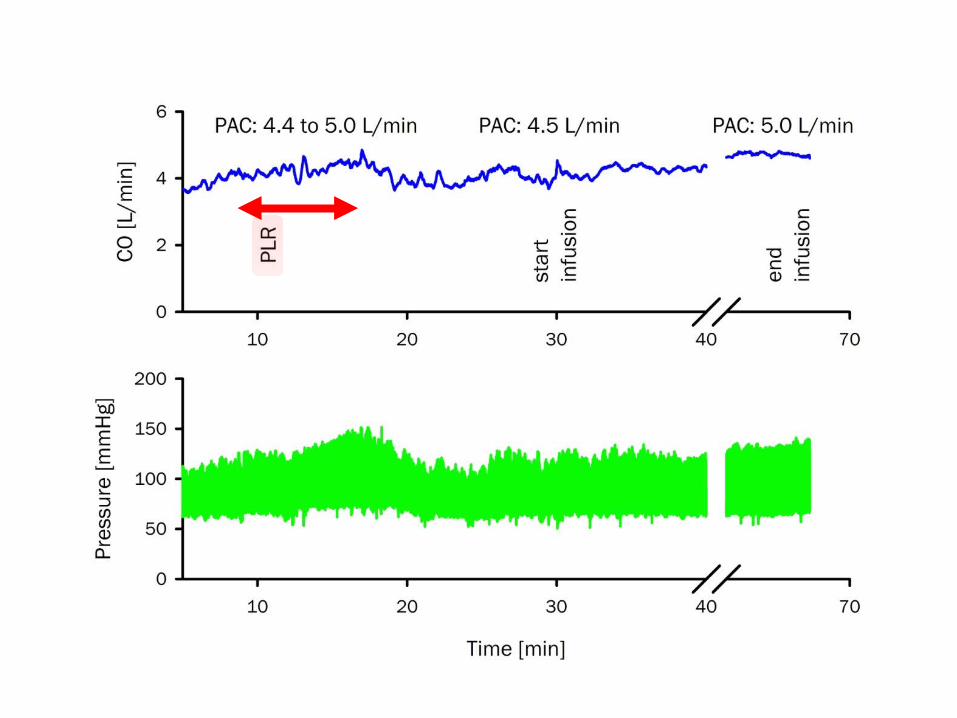
When it comes to assessing the response to therapeutic or diagnostic events with short time constants, a continuous real-time CO is more useful and informative than CO measured by intermittent thermodilution.
Fluid loading
Passive leg raising
Immediate response to inotropes

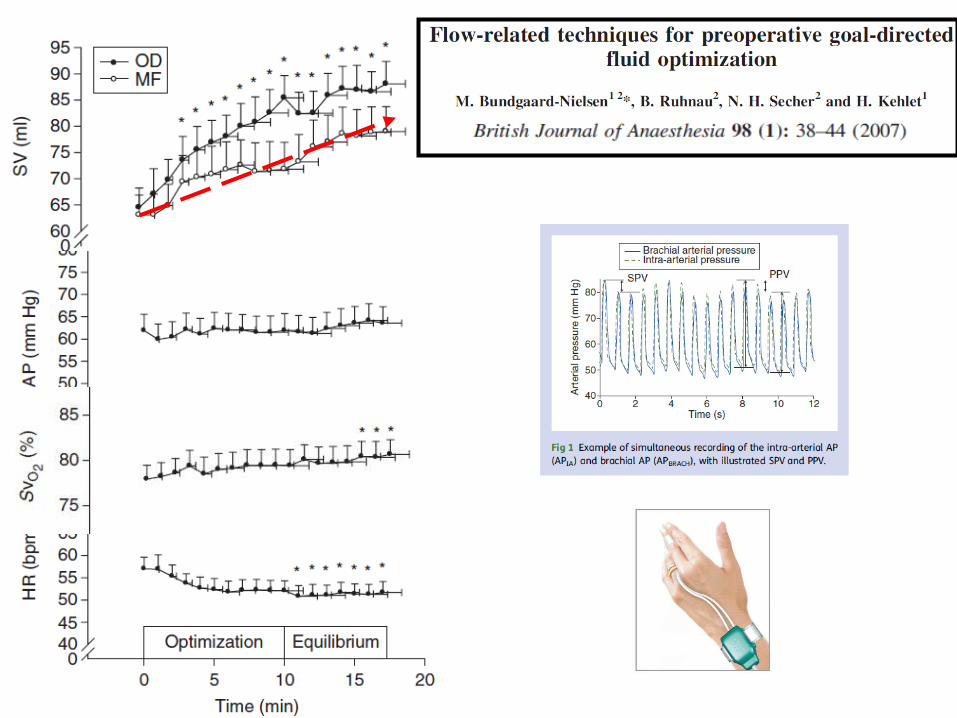
A fluid challenge identifies and simultaneously treats volume depletion, whilst avoiding deleterious consequences of fluid overload through its small volume and targeted administration.
The gold standard to monitor the response to a fluid challenge is using a continuous cardiac output monitoring.

DO2 = SpHb* SpO2* CO

The effects of Preload Modifying Maneuvers on CCO measured by the non-invasive Nexfin methodology compared with TD CO (PAC) in patients undergoing
cardiac surgery. Bubenek S et al (in preparation)

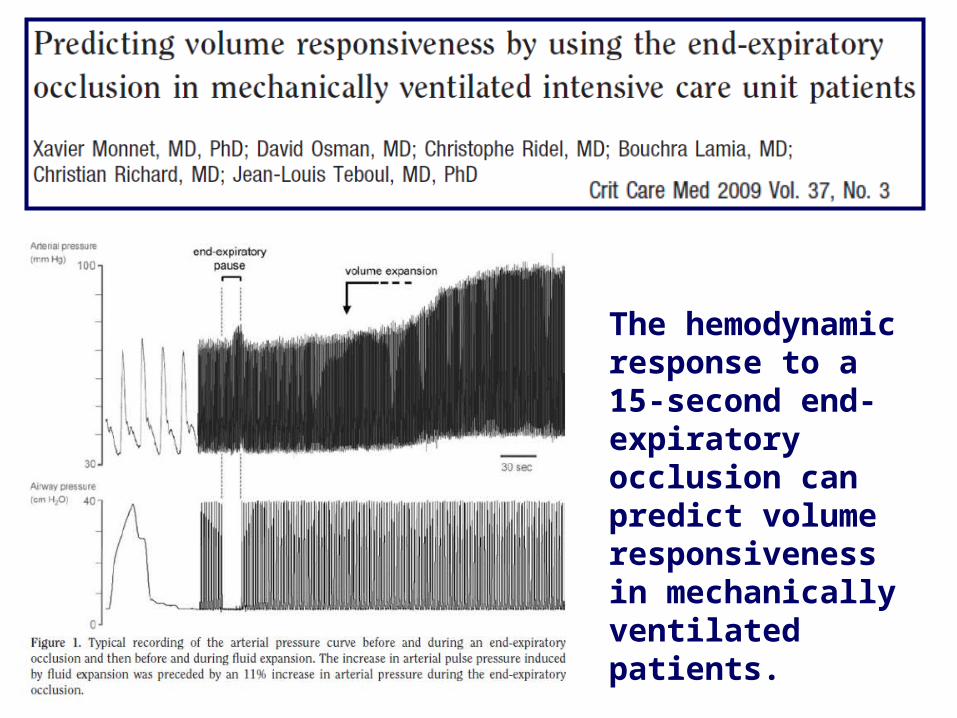
The hemodynamic response to a 15-second end-expiratory occlusion can predict volume responsiveness in mechanically ventilated patients.
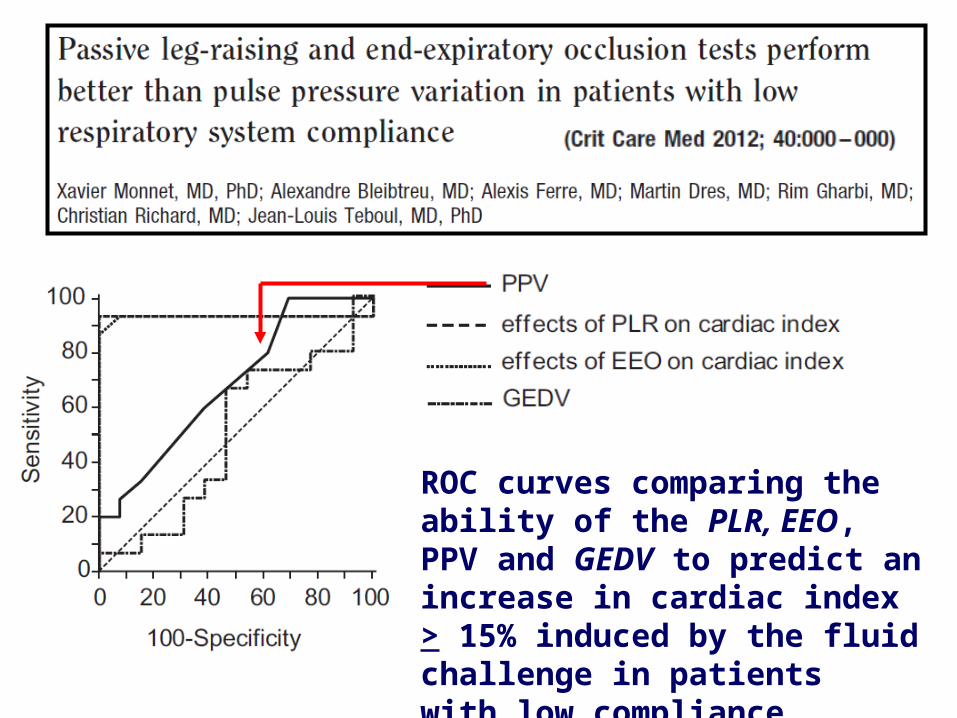
ROC curves comparing the ability of the PLR, EEO, PPV and GEDV to predict an increase in cardiac index > 15% induced by the fluid challenge in patientswith low compliance.

The power of Continuity
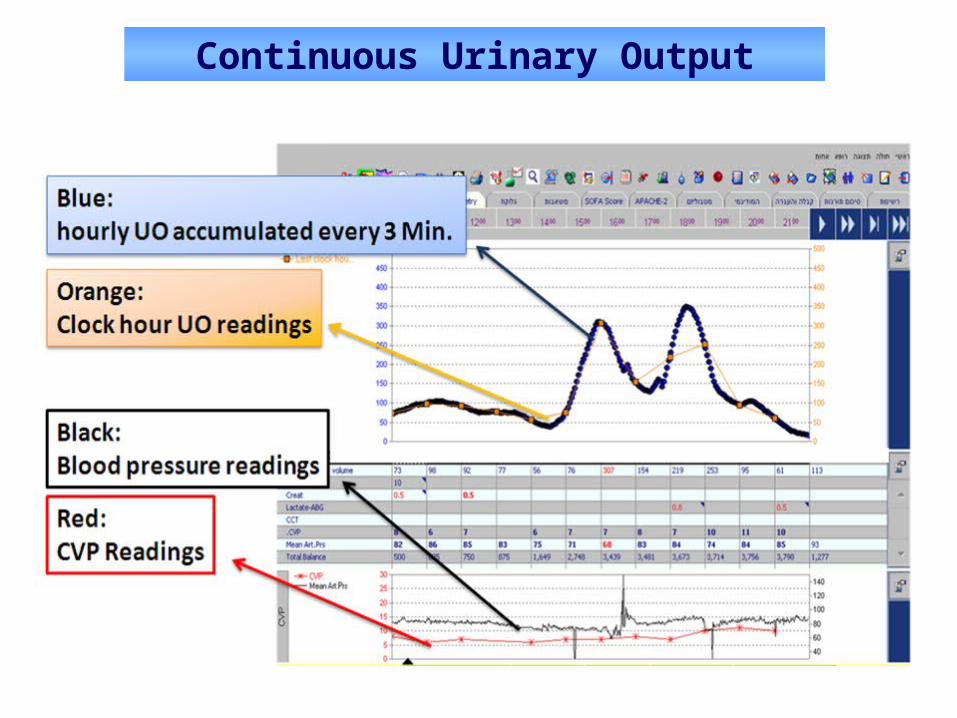
Continuous Urinary Output
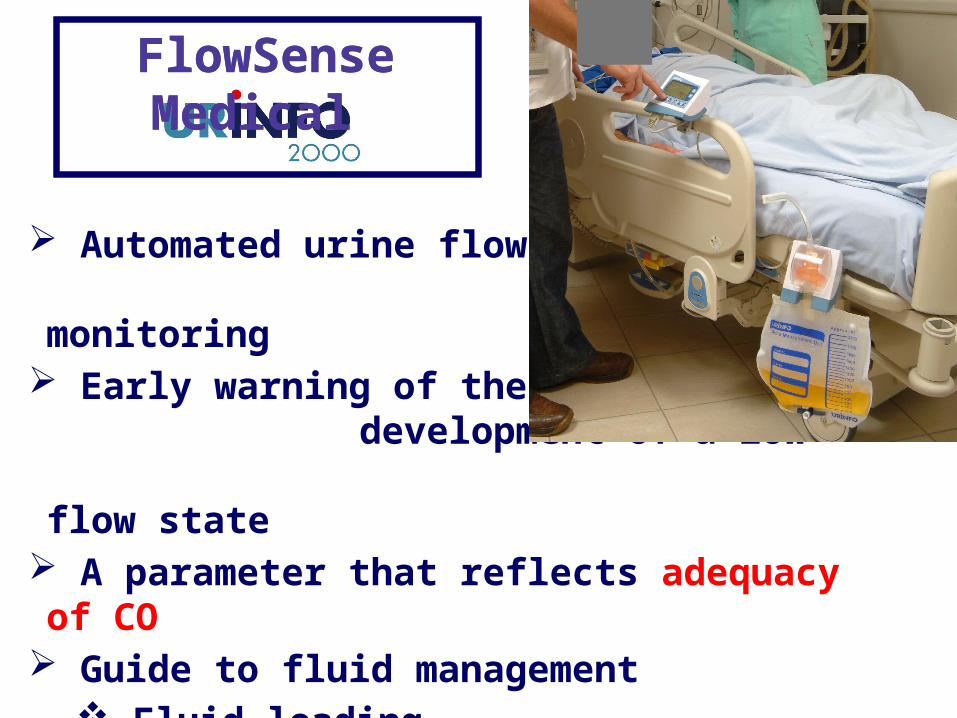
Automated urine flow and output monitoring
Early warning of the development of a low- flow state
A parameter that reflects adequacy of CO Guide to fluid management
Fluid loading Standardized diuretic test
FlowSense Medical FlowSense Medical
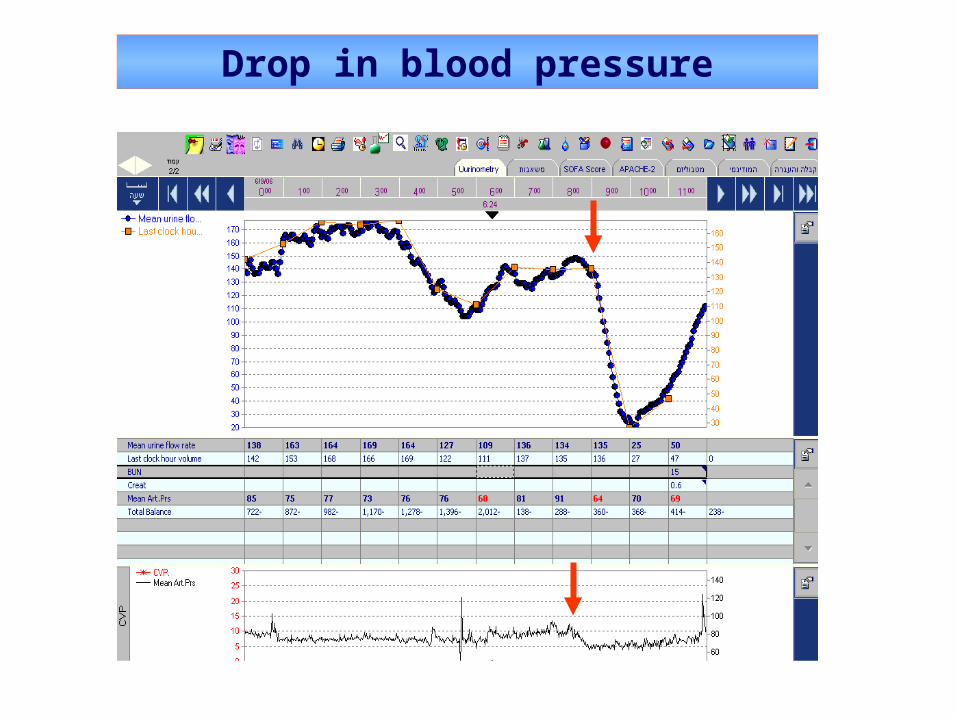
Drop in blood pressure
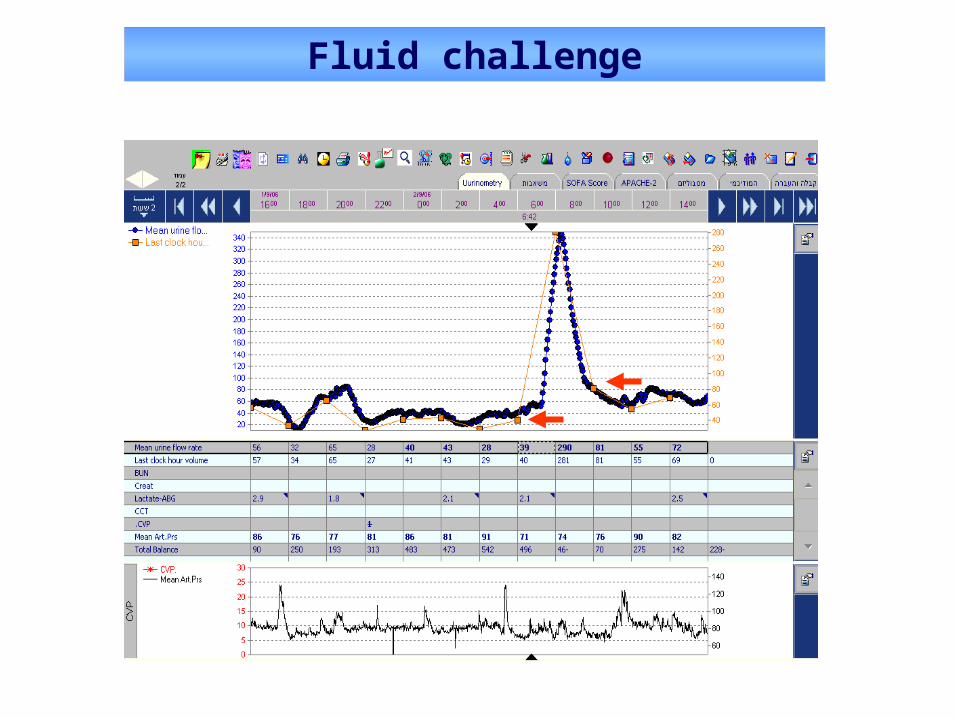
Fluid challenge
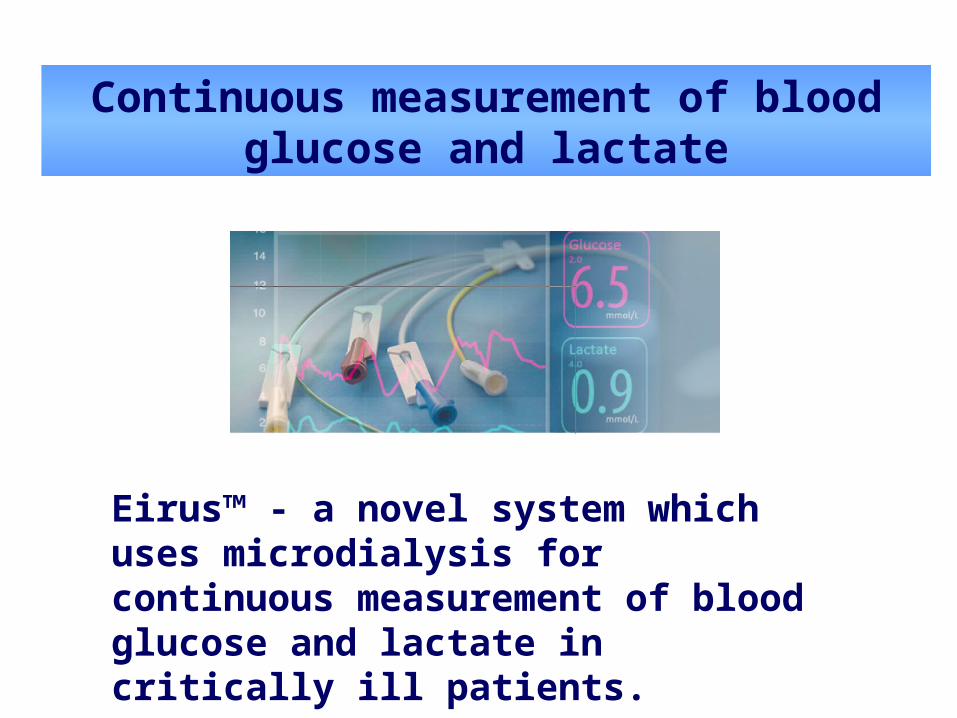
Continuous measurement of blood glucose and lactate
Eirus™ - a novel system which uses microdialysis for continuous measurement of blood glucose and lactate in critically ill patients.

The future of hemodynamic monitoring is already here.
Examples include sublingual PCO2, tissue oxygen saturation, and capillary blood flow measured under the tongue.
Such novel monitoring devices may add an extra dimension by allowing real-time assessment of response to therapy and potentially when to stop.
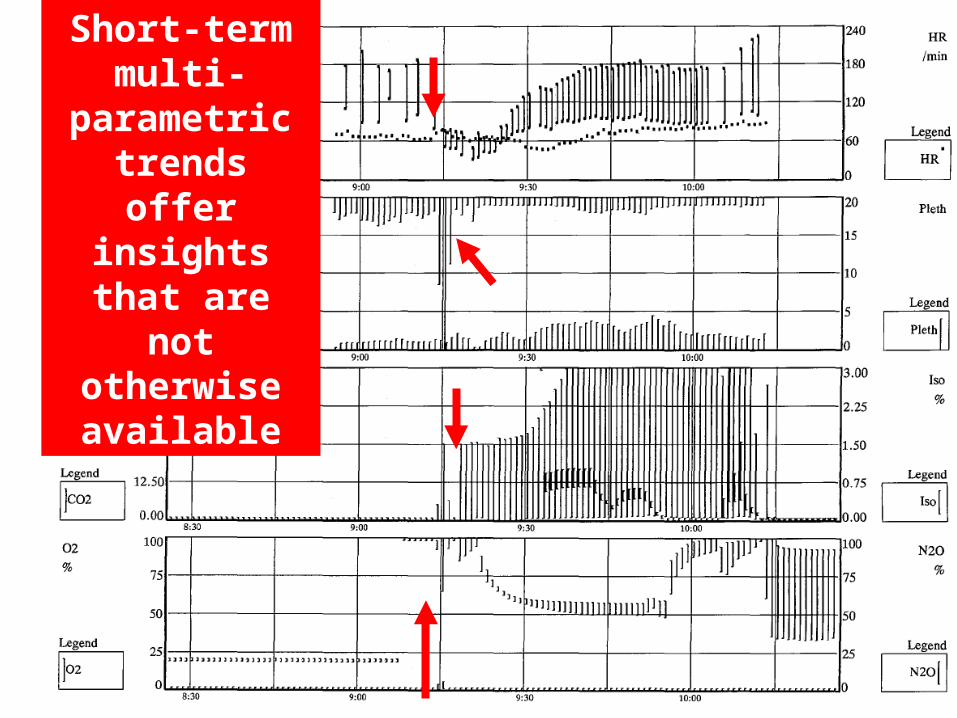
Short-term multi-
parametric trends offer insights that
are not otherwise available
The close assessment of continuous physiological analog signals :
Should Receive the recognition that classical Physical Examination has had in medicine for decades
Should be termed Physiological Examination
Should become a part of formal medical training
A. Maximize the information that can be provided by real-time continuous measurement
B. Beware of protocols, especially those with pre-defined physiological end-points
How should we deal with the inaccuracies and limitations of our
monitored parameters?

During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol:

“The reported improved survival following the adoption of these (SSC) Guidelines….cannot be viewed as justification of the initial hemodynamic resuscitation protocol.
Physiologically and clinically this protocol may be wrong for many septic patients.”
Attainment of a CVP of >8 mmHg and ScvO2 of >70% did not influence survival in patients with septic shock.
The only early interventions found to be independently associated with survival benefit were timely antibiotics and blood cultures prior to administration (p<0.0001).

The sensitivity of a 10% decrease in esophageal Doppler–measured SV in identifying fluid responsiveness was only 37% in our study.
Our data indicate that reductions in SV of >10% as measured by esophageal Doppler can be related to other factors aside from preload.
Fluids should be given to increase CO, and inodilators added once the patient is no longer fluid (preload) responsive or not achieving the goals:
CI > 4.5 L/min/m2
DO2I ≥ 600 ml/min/m2
When striving to achieve a pre-defined level of CO, one has to use an ACCURATE device!
No monitoring device can improve patient-centered
outcomes unless it is coupled to a treatment that
improves outcome.
Takala et al
Minimally-invasive CO monitoring added to usual care does not facilitate early hemodynamic stabilization in the ICU, nor does it alter the hemodynamic support or outcome.
A. Maximize the information that can be provided by real-time continuous measurement
B. Beware of protocols, especially those with pre-defined physiological end-points
C. Adopt a multi-parametric approach when making a potentially critical decision
How should we deal with the inaccuracies and limitations of our
monitored parameters?

Since the cardiopulmonary status
is often very complex, and since
no hemodynamic parameter is
perfect, a multi-parametric
approach may reduce the chance
of erroneous decisions.
The optimal CO for an individual patient is difficult to assess.
A low CO does not tell us WHAT to do.
A ‘normal’ or even high CO does not preclude the presence of inadequate regional and microcirculatory flow.
The limitations of cardiac output

Because of the complexity of assessment of
clinical variables in septic patients, direct
measurement of CO by invasive hemodynamic
monitoring is advisable, but other end-points of
global perfusion (e.g., SVO2) should be followed
as well.
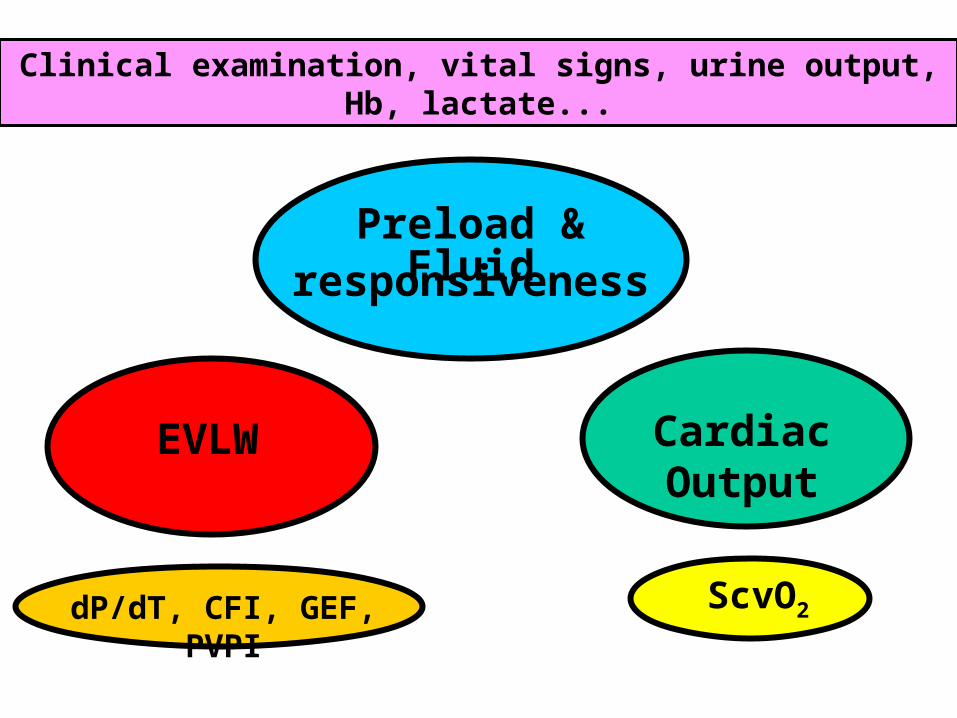
Preload &Fluid responsiveness
Cardiac OutputEVLW
ScvO2
Clinical examination, vital signs, urine output, Hb, lactate...
dP/dT, CFI, GEF, PVPI

A. Maximize the information that can be provided by real-time continuous measurement
B. Beware of protocols, especially those with pre-defined physiological end-points
C. Adopt a multi-parametric approach when making a potentially critical decision
D. Adopt decision-making strategies that take into account the uncertainty of our measurements
How should we deal with the inaccuracies and limitations of our
monitored parameters?

The gray zone approach applied to PPV forprediction of fluid responsiveness (FR) identifies a range of PPV values (9%-13%) for which FR cannot be reliably predicted in 25% of mechanically ventilated patients during GA .
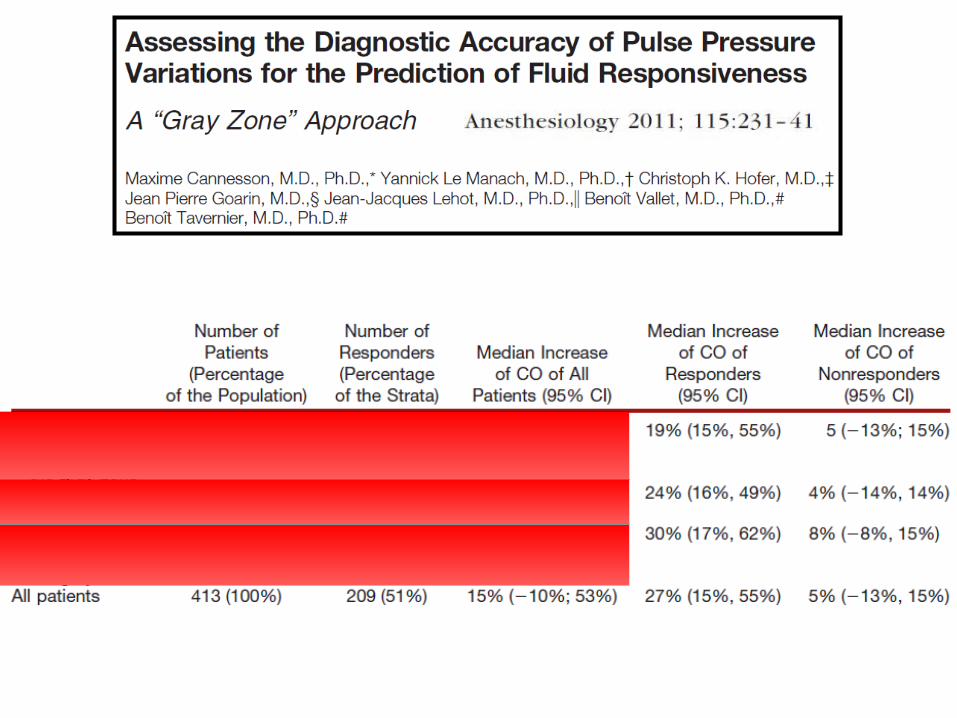
Using the “gray zone” findings, the authors defined 2 opposing fluid management strategies according to the individual risk:
1. Tight fluid control: Excessive fluid loading would be 2 times more deleterious than non-optimal CO maximization (cost ratio=2); The gray zone for PPV was 11–14%.
2. Liberal fluid control: Non-maximized CO would be 2 times more deleterious than an excessive fluid loading (cost ratio=0.5); The gray zone for PPV was 8–11%.
In a situation where fluid overload may be particularly deleterious, higher-than-normal PPV values should serve as indication for
fluid administration.

A therapeutic approach that targets and attempts to normalize abnormal physiological variables may be hazardous because of
Ignoring the underlying problem Inducing harm Ablation of physiological benefit Generation of associated errors Training effect (certain interventions that may seem
to make sense from past experience may ultimately
be detrimental when used in an alternative context)
A therapeutic conflict is a situation where each of the possible therapeutic decisions carries some potential harm.
In high-risk patients, the decision about fluid administration should be done within the context of a therapeutic conflict.
Therapeutic conflicts are a the biggest challenge for protocolized CV management in anesthetized and critically ill patients.
A therapeutic conflict is where our decisions can make the most difference.
Therapeutic Conflicts
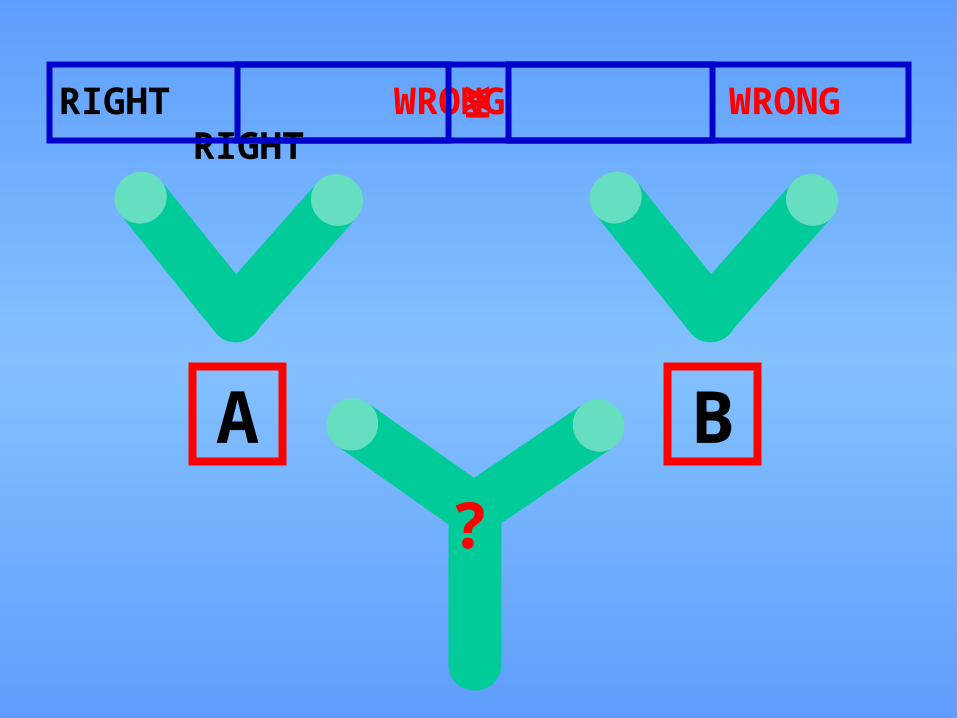
A B
RIGHT WRONG WRONG RIGHT≥≥
?
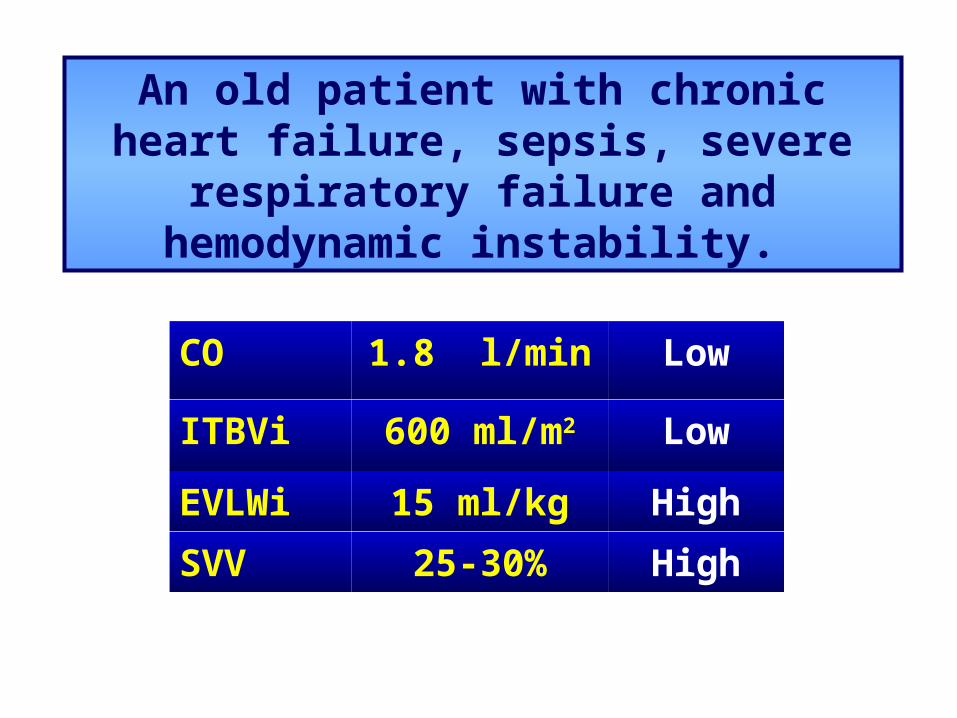
An old patient with chronic heart failure, sepsis, severe respiratory failure and
hemodynamic instability.
CO 1.8 l/min Low
ITBVi 600 ml/m2 Low
EVLWi 15 ml/kg High
SVV 25-30% High

Question 4: What would you do now?
A. Fluids
B. Inotropes
C. Vasopressors
D. Diuretics
E. I need more information
Please vote now!

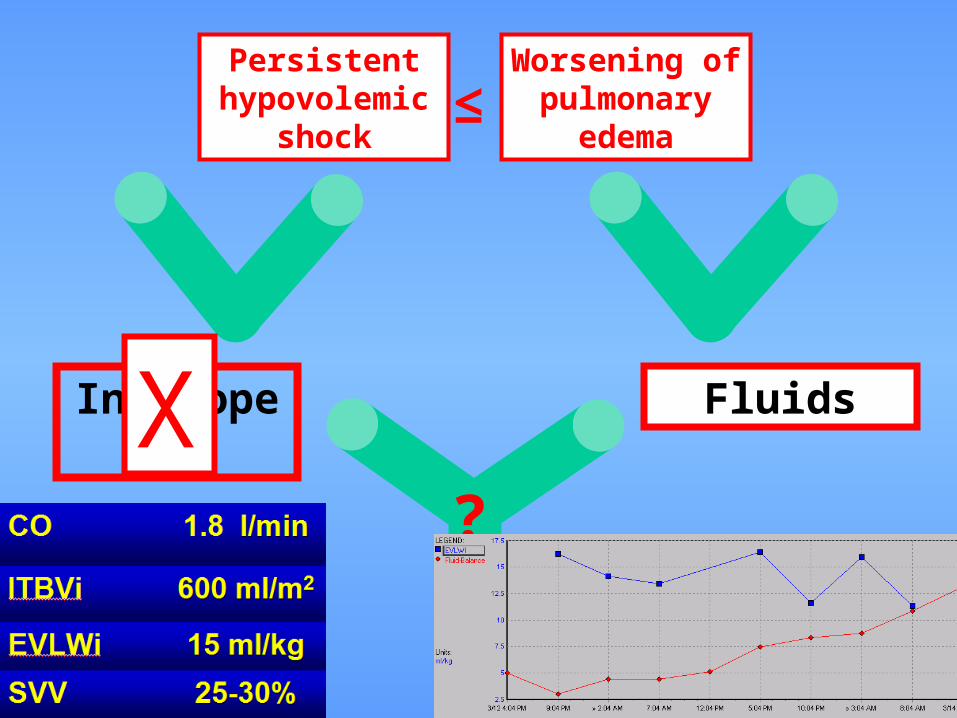
Inotropes Fluids
Persistent hypovolemic
shock
Worsening of pulmonary
edema≥
X Fluids
Cumulative fluid balance EVLW
?
We have to recognize that ALL our measurements are a lot less informative and accurate than we may want (or think)
Continuity of measurement offers vital insights which may be hidden in the analog signals of our monitors
“Physiological Examination” - observing multiple parameters on the monitor in real time - should be considered to be (at least) as important as the classic “Physical Examination”
Beware of protocolized care that is based on pre-defined specific ”goals”
The future depends not only on new technologies but also on our recognition of the complexities of hemodynamic monitoring
Conclusions:
We must live within the ambiguity of partial freedom, partial power, and partial knowledge.
All important decisions must be made on the basis of insufficient data.
Yet we are responsible for everything we do.
No excuses will be accepted.
If you meet the Buddha on the road, kill him!
Sheldon Kopp Lowe & Brydon 1974
Thank you for your attention! [email protected]