il metodo dell'ecg intracavitario come nuovo standard per
TRANSCRIPT

Il metodo dell'ECG intracavitario come nuovo standard per la verifica
intraprocedurale della posizione dell'accesso venoso centrale
Simposio Satellite Vygon Vantaggi clinici, organizzativi ed economici dell'utilizzo del Nautilus nel posizionamento
degli accessi venosi centrali
Antonio La Greca Dip.to Scienze Chirurgiche
POLICLINICO “A. GEMELLI” - ROMA

WE ASSUME THAT the optimal tip position for infusion central catheters is the superior cavo-atrial junction, as it prevents:
– Venous thrombosis – Malfunction – Tip migration – Arrythmias

• Incidence of primary malposi1on: 2-‐30%
• Time consump1on and costs of post-‐procedural 1p control (chest X-‐Ray)
• Time consump1on, costs and logis1cs of fluoroscopy
• Accuracy of radiological 1p control (chest X-‐Ray, Fluoroscopy) • Costs of a primary malposi1on
• Time consump1on and costs of reposi1oning procedures
• Home placement of PICCs
• Operators’ discomfort and frustra1on
Malposition: logistic problems

COSTI PER PROCEDURA STANDARD non complicata
COSTO (Euro) Catetere con kit introduzione 200-300 Materiale di consumo (teli, disinfettante, siringhe, etc.) 75 Esami laboratorio 14 Tempo medico 1 ora 75 Tempo infermiere 1 ora 33 Utilizzo cardiomonitor + pulsiossimetro 30 Utilizzo ecografia 75 Addestramento utente alla gestione 48 Rx 150 Totale 700-800
ECG Guida risparmio 100 Euro
Fluoroscopia incremento 500 Euro
De Lillas, Emoli - Master Universitario I livello “Nursing degli accessi venosi” Università Cattolica Roma, Anno Accademico 2007-2008.

Cos1 dell’impianto di un PICC
• Da1 presenta1 da M.Smith (Wisconsin) al congresso DIVLD – Parigi, 2011
operatore ambiente a,rezzatura altri op.
$ 5000 chirurgo Sala operatoria fluoroscopia ferrista
$ 2800 radiologo Sala radiologica fluoroscopia tecnico rad.
$ 1800 anestesista bedside no fluoro
$ 875 infermiere bedside no fluoro
N.B.: tutti i PICC erano posizionati per via ecoguidata NON DIFFERENZE in termini di outcome clinico

Cos1 dell’impianto di port
• Da1 presenta1 al congresso AVA 2010
Accesso venoso
Verifica della punta
Ambiente
Port posizionato negli anni 90
Tecnica chirurgica
Fluoroscopia Sala operatoria
$ 5000
Port posizionato oggi
Venipuntura ecoguidata
ECG intracavitario
Ambiente dedicato del Day Hospital
$ 950

E in caso di malposizione ?
THE IDEAL METHOD SHOULD:
– Allow intraprocedural control of both DIRECTION and LENGTH of the catheter defining “in real 1me” where the 1p is
• Avoid primary malposi1on • Avoid mul1ple adempts at reposi1oning the catheter – Allow post-‐procedural control and documenta1on of the final 1p posi1on
– Be accurate – Be easy to perform, easy to teach, easy to learn – Be cheap – Be manageable by the vascular operator in all its details
Control of tip position

WHAT HAVE WE GOT AVAILABLE ?
Control of tip position

Chest XRay Fluoroscopy Surface anatomical landmarks and antropometric methods US explora1on of large cervicothoracic vessels to rule out gross catheter maposi1on Magne1c tracking Intracavitary ECG guidance Combina1on methods (ECG + magne1c/doppler) Trans-‐esophageal echocardiography CT and MRI
Control of tip position
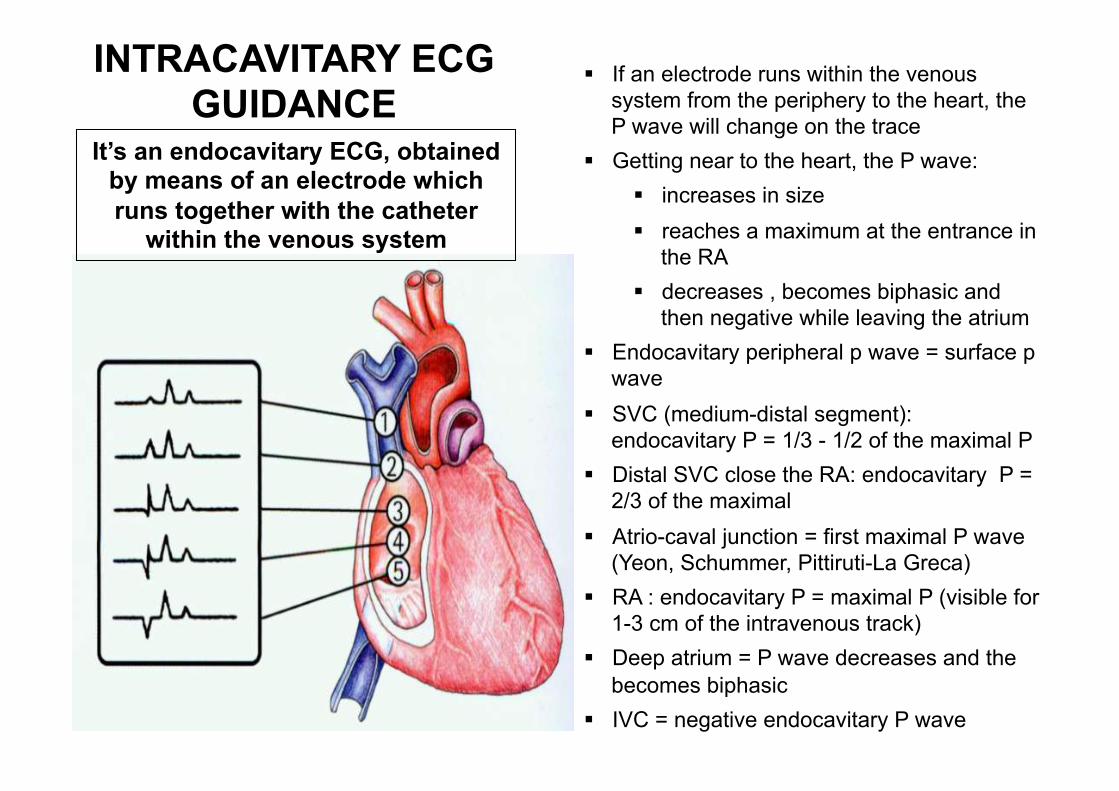
§ If an electrode runs within the venous system from the periphery to the heart, the P wave will change on the trace
§ Getting near to the heart, the P wave: § increases in size § reaches a maximum at the entrance in
the RA § decreases , becomes biphasic and
then negative while leaving the atrium § Endocavitary peripheral p wave = surface p
wave § SVC (medium-distal segment):
endocavitary P = 1/3 - 1/2 of the maximal P § Distal SVC close the RA: endocavitary P =
2/3 of the maximal § Atrio-caval junction = first maximal P wave
(Yeon, Schummer, Pittiruti-La Greca) § RA : endocavitary P = maximal P (visible for
1-3 cm of the intravenous track) § Deep atrium = P wave decreases and the
becomes biphasic § IVC = negative endocavitary P wave
INTRACAVITARY ECG GUIDANCE
It’s an endocavitary ECG, obtained by means of an electrode which runs together with the catheter
within the venous system

1c. SVC, superior 1/3
2. SVC, medium-distal 1/3 and junction 3. RA (junction and superior 1/3 sup)
5. IVC
4. Deep atrium
1b. Brachiocephalic
1a. Axillary
INTRACAVITARY ECG GUIDANCE

1. The red lead (right shoulder) becomes endocavitary and reads the atrial electric ac1vity FROM WITHIN THE VENOUS SYSTEM
2. If the endocavitary electrode runs together with catheter 1p, the 1p itself can be localized by means of P wave amplitude
INTRACAVITARY ECG GUIDANCE

INTRACAVITARY ECG GUIDANCE
DII lead: -‐ parallel to the direc1on of the main atrial ac1vity -‐ beder visualiza1on of P wave amplitude varia1ons

SVC
INTRACAVITARY ECG GUIDANCE

Medium-‐distal IVC
Endocavitary p wave = 1/3 - 1/2 of the maximal
GUIDA ECG ENDOCAVITARIA

Distal segment of SVC / AC juncBon
GUIDA ECG ENDOCAVITARIA
Endocavitary P = 2/3 of the maximal or first
maximal

Atriocaval junction/entrance of right atrium (crista terminalis)
Endocavitary P = first maximal
GUIDA ECG ENDOCAVITARIA

GUIDA ECG ENDOCAVITARIA
First 1/3 of atrium
Endocavitary P = Maximal for 1-3 cm, then decreases; appearance of a negative component

Deep atrium
Biphasic
GUIDA ECG ENDOCAVITARIA
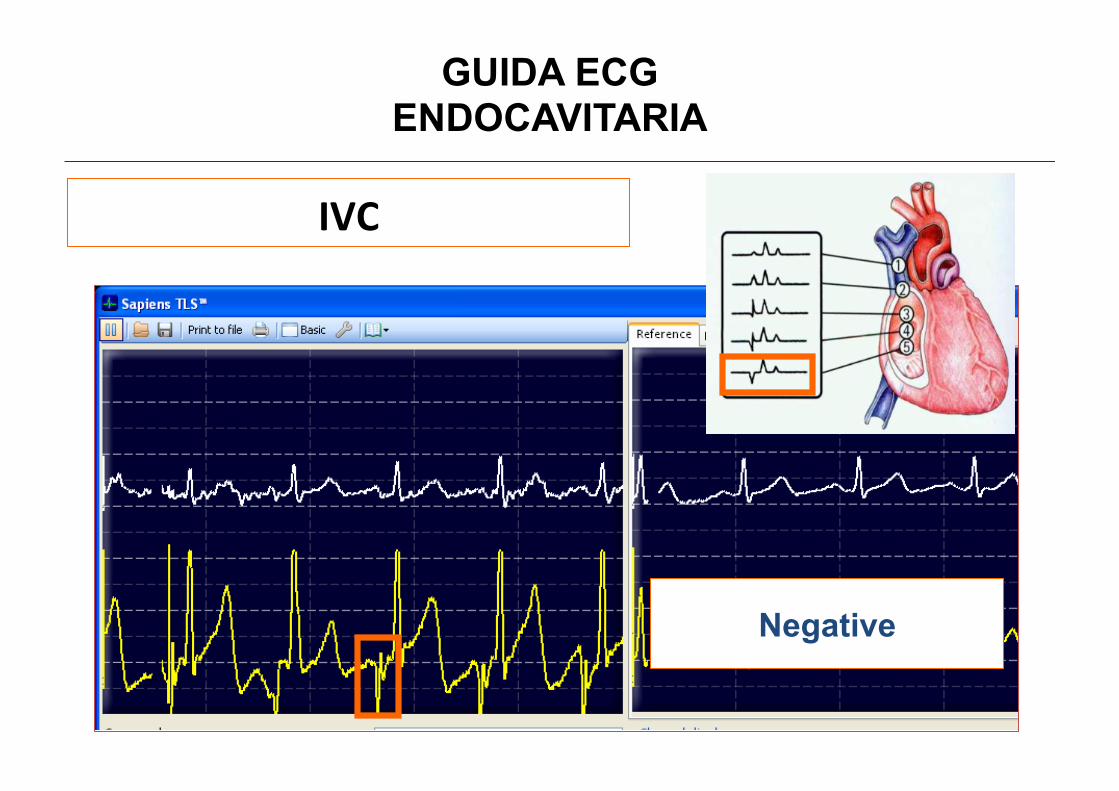
IVC
GUIDA ECG ENDOCAVITARIA
Negative

Which monitor ?
• NAUTILUS – Digital system, specifically created for intracavitary ECG
– Monitor = personal computer – Simultaneous visualiza1on of endocavitary DII lead and surface ECG (DIII or DI)
– Comparison of different endocavitary tracks (freeze)
– Final paper documenta1on



New Vygocard


PICC tagliabile prossimlamnete

Precisione metodo ECG Eventuale tunnel sia retrogrado che anterogrado Non necessaria misurazione preventiva del tunnel Spazio per biopatch “a misura”
PICC tagliabile prossimalmente

VANTAGGI
• Economico, rapido, emplice da imparare • Preciso (criterio eledrofisiologico) • Aduabile anche ‘bedside • Interamente ges1bile dall’operatore • Consente:
– controllo INTRAPROCEDURALE – controllo FINALE – DOCUMENTAZIONE della posizione della punta
• Sicuro per il paziente e per l’operatore • SE CON SOL. FISIOLOGICA:
– bedside più semplice (no guide lunghe) – ripe1bile a distanza per controllo migrazione secondaria:
• a basso costo (no mandrini monouso) • A basso rischio (non è necessario riarmare il catetere)
– eseguibile anche con cateteri a punta chiusa
GUIDA ECG ENDOCAVITARIA

PUO’ IL METODO ECG SOSTITUIRE DEFINITIVAMENTE IL CONTROLLO
RADIOLOGICO ?
GUIDA ECG ENDOCAVITARIA

INDICAZIONI “CLASSICHE” AL CONTROLLO RX
1) Rule out complicanza immediata (PNX, versamento pleurico)
GUIDA ECG ENDOCAVITARIA

ESPEN 2009
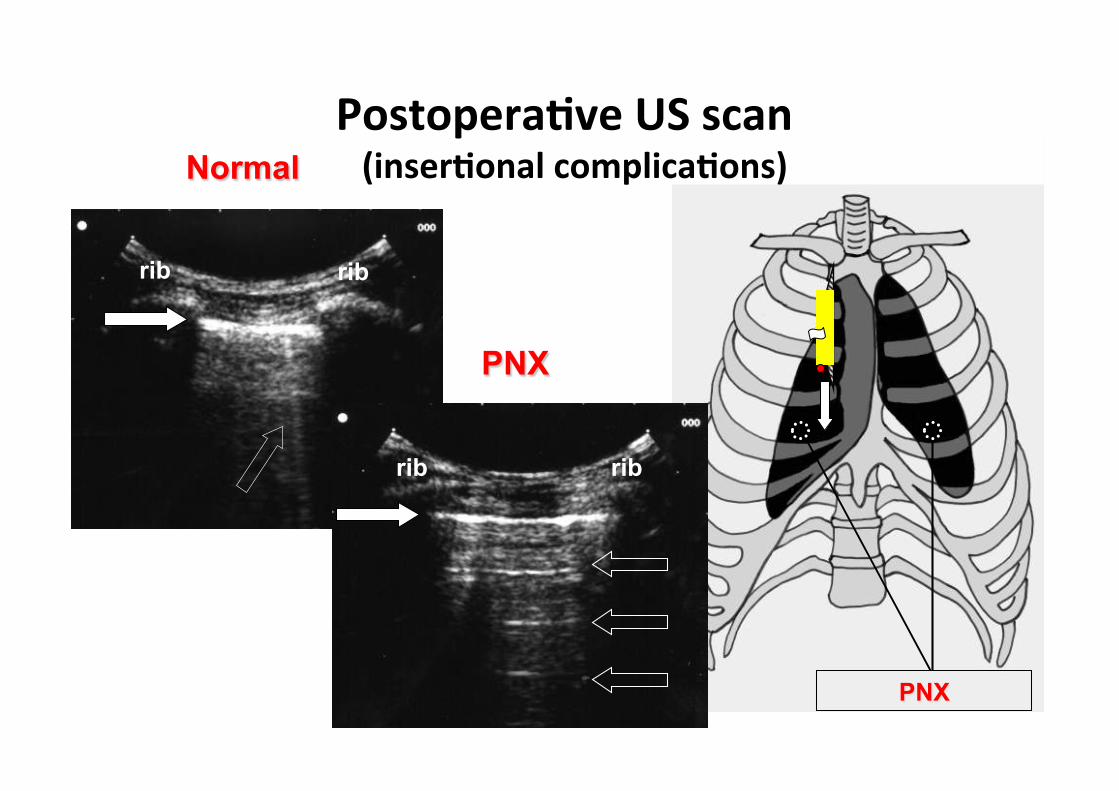
PNX
rib rib
Normal
rib rib
PNX
PostoperaBve US scan (inserBonal complicaBons)

INDICAZIONI “CLASSICHE” AL CONTROLLO RX
GUIDA ECG ENDOCAVITARIA
2) Controllo posizione punta

La Lederatura a sostegno del metodo ECG è fortemente
sugges1va
GUIDA ECG ENDOCAVITARIA

95.4%
1444 paz

GUIDA ECG ENDOCAVITARIA

In Germania, la locale società di anestesia già dal 1998 conclude che è lecito u1lizzare il metodo ECG in sos1tuzione del controllo radiologico (purchè si possano altrimen1 escludere complicanze immediate): -‐ metodo consolidato e di pari efficacia rispedo alla radiologia (sia tecnica con guida metallica che colonna di liquido)
-‐ minor dispendio di risorse -‐ minor esposizione a radiazioni ionizzan1
GUIDA ECG ENDOCAVITARIA

• Ideally, the posi/on of the /p should be checked during the procedure, either by fluoroscopy or by the ECG method.
• If the posi/on has not been checked intraopera/vely, a post-‐procedural chest X-‐ray should be performed to check the posi/on of the /p.
ESPEN 2009
GUIDA ECG ENDOCAVITARIA

FDA 2010

The CICC-‐PICC inser1on bundle
Target: zero malposi1ons ! “X-‐Ray free” inser1on bundle
(GAVeCeLT, 2009-‐2010)
1) US guided venipuncture 2) Es/mated length of the catheter by anatomical landmarks 3) US check of the absence of the catheter in abnormal sites 4)ECG method for confirming the final posi/on of the /p 5) Rule out of pleural complica/ons by mans of thoracic US
GUIDA ECG ENDOCAVITARIA

SILTA = Safe Implanta1on of Long Term Access (GAVeCeLT, 2007) Point 2 of the Bundle : Intraprocedural check of the posiBon of the Bp, preferably by the ECG method
GUIDA ECG ENDOCAVITARIA

GUIDA ECG ENDOCAVITARIA

DATO PER ASSUNTO CHE: • La posizione ovmale per CVC u1lizza1 per scopi infusionali (NON per monitoraggio emodinamico o dialisi) è la giunzione cavo-‐atriale;
• Il gold standard per il controllo è rappresentato dalle metodiche di imaging radiologico (Rx torace-‐fluoroscopia) o dall’ecocardiografia trans-‐esofagea;
• Il gold standard presenta comunque limi1 clinici e logis1ci che ne limitano l’accuratezza e la costo-‐efficacia;
GUIDA ECG ENDOCAVITARIA
1. Consente controllo INTRAPROCEDURALE 2. E’ favbile NELLA STRAGRANDE MAGGIORANZA DEI PAZIENTI 2. E’ accurato (correlazione anatomo-‐eledrofisiologica) 3. E’ sicuro 4. E’ ripe1bile (non invasivo) 5. E’ interamente ges1bile dall’impiantatore 6. E’ riproducibile (tra operatori diversi) 7. E’ economico e logis1camente sostenibile 8. E’ semplice da u1lizzare e da apprendere 9. Consente la documentazione finale su supporto fisico
(monitoraggio malposizionamen1 secondari, tutela medico-‐legale dell’impiantatore)
IL METODO ECG (in particolare con colonna di liquido) SUPERA I LIMITI DEI METODI STANDARD
GUIDA ECG ENDOCAVITARIA

• Il metodo ECG (specie se con colonna di liquido) può rientrare in un BUNDLE mul1procedurale di controlli non radiologici a basso costo
• Cateteri tagliabili prossimalmente migliorano favbilità e accuratezza del metodo
• L’ECG PUO’ VICARIARE L’UTILIZZO DEI CONTROLLI RADIOLOGI, posto che – la venipuntura venga eseguita con tecnica a basso tasso di complicanze toraco-‐medias1niche (linee guida ESPEN 2009)
– venga defini1vamente validato il metodo ECG (consensus nazionale, procedure aziendali)
GUIDA ECG ENDOCAVITARIA