imaging of salivary gland tumours
TRANSCRIPT

INTRODUCTION
ANATOMY AND PHYSIOLOGY
IMAGING METHODS
bull BENIGN
bull MALIGNANTNEOPLASMS
Introduction
bull Saliva is a clear alkaline somewhat viscid secretion from the parotid submandibular sublingual and smaller mucous glands of the mouth - Dorlandrsquos Medical Dictionary
bull Saliva is a clear taste less odorless slightly acidic viscous fluid consisting of secretions from the parotid submandibular amp mucous glands of oral cavity - Stedmanrsquos Medical Dictionary
SALIVARY GLANDS
MAJOR SALIVARY GLANDS (paired structures)
PAROTID
SUBMANDIBULAR (SUBMAXILLARY)
SUBLINGUAL
MINOR SALIVARY GLANDS (diffusely scattered in oral cavity)
BUCCAL (cheek)
PALATINE (palate)
LABIAL (lip)
LINGUAL (tongue)
Secrete 10 of total volume of saliva
Account for about 70 of mucus secreted
Parotid
Glands of Von r
Mucous
Serous
Mixed
Labial amp Buccal Glands
Glossopalatine
Palatine
Posterior tongue
Submandibular amp Sublingual
Anterior tongue
Parotid
Glands of Von Bender
5
Types of Salivary Glands
Development of Salivary Glands
bull Individual salivary glands arise as a proliferation of oral epithelial cells forming a focal thickening that grows into the underlying ectomesenchyme
bull Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells with mesenchyme condensing around the bud
bull Clefts develop in the bud forming two or more new buds continuation of this process called branching morphogenesis produces successive generations of buds and a hierarchical ramification of the gland
bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Introduction
bull Saliva is a clear alkaline somewhat viscid secretion from the parotid submandibular sublingual and smaller mucous glands of the mouth - Dorlandrsquos Medical Dictionary
bull Saliva is a clear taste less odorless slightly acidic viscous fluid consisting of secretions from the parotid submandibular amp mucous glands of oral cavity - Stedmanrsquos Medical Dictionary
SALIVARY GLANDS
MAJOR SALIVARY GLANDS (paired structures)
PAROTID
SUBMANDIBULAR (SUBMAXILLARY)
SUBLINGUAL
MINOR SALIVARY GLANDS (diffusely scattered in oral cavity)
BUCCAL (cheek)
PALATINE (palate)
LABIAL (lip)
LINGUAL (tongue)
Secrete 10 of total volume of saliva
Account for about 70 of mucus secreted
Parotid
Glands of Von r
Mucous
Serous
Mixed
Labial amp Buccal Glands
Glossopalatine
Palatine
Posterior tongue
Submandibular amp Sublingual
Anterior tongue
Parotid
Glands of Von Bender
5
Types of Salivary Glands
Development of Salivary Glands
bull Individual salivary glands arise as a proliferation of oral epithelial cells forming a focal thickening that grows into the underlying ectomesenchyme
bull Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells with mesenchyme condensing around the bud
bull Clefts develop in the bud forming two or more new buds continuation of this process called branching morphogenesis produces successive generations of buds and a hierarchical ramification of the gland
bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

SALIVARY GLANDS
MAJOR SALIVARY GLANDS (paired structures)
PAROTID
SUBMANDIBULAR (SUBMAXILLARY)
SUBLINGUAL
MINOR SALIVARY GLANDS (diffusely scattered in oral cavity)
BUCCAL (cheek)
PALATINE (palate)
LABIAL (lip)
LINGUAL (tongue)
Secrete 10 of total volume of saliva
Account for about 70 of mucus secreted
Parotid
Glands of Von r
Mucous
Serous
Mixed
Labial amp Buccal Glands
Glossopalatine
Palatine
Posterior tongue
Submandibular amp Sublingual
Anterior tongue
Parotid
Glands of Von Bender
5
Types of Salivary Glands
Development of Salivary Glands
bull Individual salivary glands arise as a proliferation of oral epithelial cells forming a focal thickening that grows into the underlying ectomesenchyme
bull Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells with mesenchyme condensing around the bud
bull Clefts develop in the bud forming two or more new buds continuation of this process called branching morphogenesis produces successive generations of buds and a hierarchical ramification of the gland
bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Parotid
Glands of Von r
Mucous
Serous
Mixed
Labial amp Buccal Glands
Glossopalatine
Palatine
Posterior tongue
Submandibular amp Sublingual
Anterior tongue
Parotid
Glands of Von Bender
5
Types of Salivary Glands
Development of Salivary Glands
bull Individual salivary glands arise as a proliferation of oral epithelial cells forming a focal thickening that grows into the underlying ectomesenchyme
bull Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells with mesenchyme condensing around the bud
bull Clefts develop in the bud forming two or more new buds continuation of this process called branching morphogenesis produces successive generations of buds and a hierarchical ramification of the gland
bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Development of Salivary Glands
bull Individual salivary glands arise as a proliferation of oral epithelial cells forming a focal thickening that grows into the underlying ectomesenchyme
bull Continued growth results in the formation of a small bud connected to the surface by a trailing cord of epithelial cells with mesenchyme condensing around the bud
bull Clefts develop in the bud forming two or more new buds continuation of this process called branching morphogenesis produces successive generations of buds and a hierarchical ramification of the gland
bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Parotid glands begin development at 4-6 weeks IU
bull Submandibular glands 6 weeks IU
bull Sublingual and minor glands 8-12 weeks IU
bull The cells of the secretory end pieces and ducts attain maturity during last two months of gestation
bull The glands continue to grow postnatally with the volume proportion of acinar tissue increasing and the volume proportion of ducts connective tissue and vascular elements decreasing up to 2 years of age
Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Anatomy
Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Parotid Gland
bull Para around otic ear
bull Largest of the glands 14-28g
bull Situated below the external acoustic meatus between the ramus of the mandible and the sternomastoid
bull The investing layer of the deep cervical fascia forms a capsule for the gland ndash parotid capsule
bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull The parotid gland is composed of adipose and glandular tissues in nearly equal proportions
bull The parotid gland is divided into the larger superficial and smaller deep lobes by the retromandibular or facial vein
bull It is located posterior to the ramus of mandible and drains via the Stensons duct traversing superficial to the masseter muscle and passing through the buccinator muscle before finally opening into the oral cavity at the ipsilateral 2ndmaxillary molar
bull The distal part of facial nerve and its terminal branches passes through the parotid parenchyma
bull Multiple nodes are located superficially and within the parotid gland
bull Accessory parotid gland is noted in 20 subjects and is usually located anterior to the main parotid and superior to the Stensonsduct draining in to the latter through an accessory duct
External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

External Featuresbull Resembles a three sided pyramid the apex of the pyramid is
directed downwards
bull Gland has four surfacesndash Superior (base of the pyramid)
ndash Superficial
ndash Anteromedial and
ndash Posteromedial
bull The surfaces are separated by three bordersndash Anterior
ndash Posterior
ndash Medial
Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Relations of the Gland
bull APEX ndash It overlaps the posterior belly of the digastric
ndash The cervical branch of the facial nerve and the two divisions of the retromandibular vein emerge through it
bull SUPERIOR SURFACEndash Is small and concave
ndash Related to cartilaginous part of external acoustic meatus posterior part of TMJ superficial temporal vessels and auriculotemporal nerve
bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull ANTEROMEDIAL SURFACEndash Grooved by posterior border of ramus
ndash Related to the masseter TMJ posterior border of ramus medial pterygoid muscle and emerging branches of facial nerve
bull POSTEROMEDIAL SURFACEndash Molded to the mastoid amp styloid process
ndash Related to the sternomastoid and posterior belly of digastric styloid process and its structures
ndash External carotid artery enters the gland through this surface
bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull SUPERFICIAL SURFACE
ndash Covered by skin superficial fascia with superficial parotid lymph nodes parotid fascia and deep parotid lymph nodes
bull From the anterior border emerges
ndash Parotid duct
ndash Terminal branches of facial nerve
Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Parotid Duct
bull Thick walled 5cm long
bull Emerges from the middle of the anterior border of the gland
bull Runs forward and slightly downwards on the masseter where it is relatedto the upper and lower buccal branch of the facial nerve and theaccessory parotid gland
bull At the anterior border of the masseter it turns medially to pierce thebuccal pad of fat buccopharyngeal fascia and the buccinator to runforward between the muscle and the oral mucosa
bull Before finally piercing it opposite the crown of the upper second molar
Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Blood Supplybull Arterial supply External carotid artery and its
branchesbull Venous drainage External jugular vein
Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Nerve Supply
PARASYMPATHETIC SUPPLY
Inferior salivatory nucleus
9th cranial nerve
Otic ganglion
Auriculotemporal nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the external carotid artery
Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Lymphatic Drainage
bull Drains first to the parotid lymph nodes then to the upper deep cervical lymph nodes
bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull (a) Diagram shows the location of the Stenon duct 1 = parotid gland 2 = Stenonduct 4 = masseter muscle 5 = surface of the mandible 6 = buccal muscle large arrow = retromandibular vein and external carotid artery(b) Panoramic US image shows a dilated Stenon duct in a patient with sialolithiasis and inflammation 1 = inflamed left parotid gland 2 = dilated Stenon duct 3 = stone 4 = masseter muscle 5 = surface of the mandible 6= buccal muscle large arrow = retromandibular vein and external carotid artery
bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull This illustration represents a horizontal section through the lateral portion of the pharynx and mandible at the level of the mastoid process The parotid gland is traversed by the facial nerve and the deep portion of the gland narrows and is bounded by the posterior of the ramus of the mandible muscles of the styloid process and medial pterygoid muscle Right Tumors that arise within the deep portion of the gland may expand into the lateral pharyngeal space and produce swelling of the lateral pharyngeal wall
bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull This lateral view of the head shows the anatomic position and relationship of the parotid and submandibular glands to the ear zygomatic arch mandible and masseter muscle The parotid gland duct (Stensens duct) crosses the masseter muscle and penetrates the buccal tissues Lobules of accessory parotid tissue are located along the course of the duct
Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Non-contrast axial CT image show normal appearing parotid (white arrows) gland in a young subject
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated
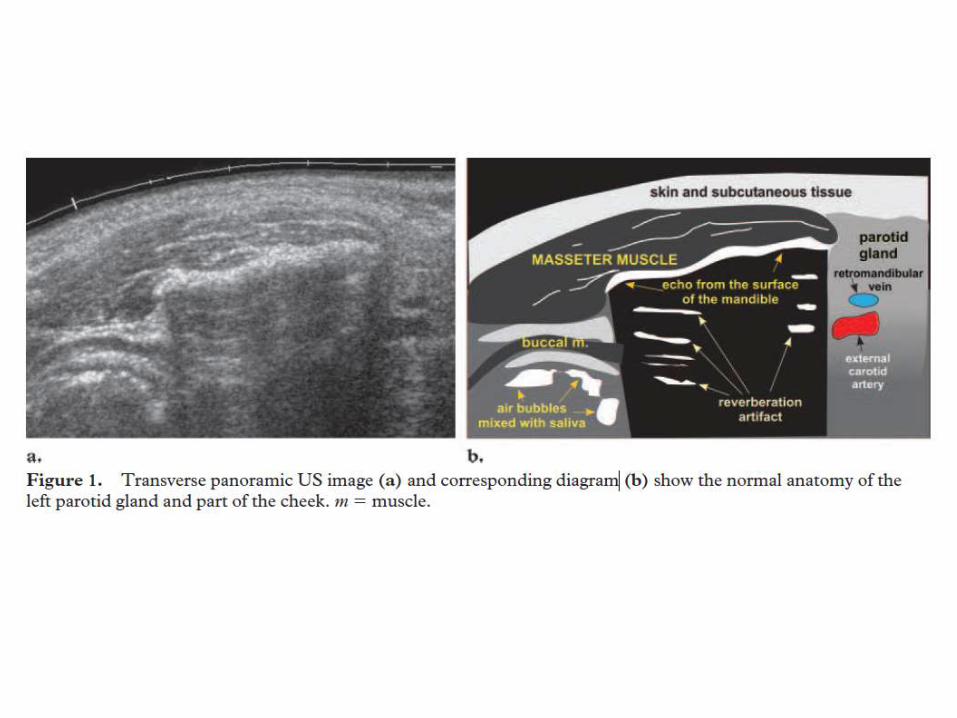
SUBMANDIBULAR GLAND
bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Also called submaxillary gland
bull The submandibular gland is the second largest salivary gland and is located in the floor of the mouth adjacent to the posterior body of mandible along the free edge of the mylohyoid muscle
bull Partially enclosed between two layers of the deep cervical fascia
bull In submandibular triangle formed by anterior and posterior bellies of digastric muscle and inferior margin of mandible- Weighs 50 of parotid gland
bull The amount of adipose tissue is relatively lower than that of parotid gland The lingual nerve and submandibular ganglion are noted superficial to the submandibular gland while the hypoglossal nerve lies deep to it
bull It drains through the Whartons duct in the anterior sublingual region at the papilla in paramidline location
Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Superficial Part
bull It hasndash Inferiorndash Lateral andndash Medial surfaces
Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Relations
bull INFERIOR SURFACE covered by ndash Skinndash Platysmandash Cervical branch of facial nervendash Deep fasciandash Facial veinndash Submandibular lymph nodes
bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull LATERAL SURFACEndash Submandibular fossandash Medial pterygoid musclendash Facial artery
bull MEDIAL SURFACE may be divided into three partsndash Anterior part related to mylohyoid muscle nerves and vesselsndash Middle part hyoglossus styloglossus lingual nerve submandibular ganglion
hypoglossal nervendash Posterior part styloglossus stylohyoid ligament 9th nerve
Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Deep Partbull Small in sizebull Lies deep to the mylohyoid and superficial to the hyoglossus and
styloglossusbull Posteriorly it is continuous with the superficial part around the posterior
border of the mylohyoidbull Anteriorly it extends up to the posterior end of the sublingual gland
Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Submandibular Ductbull Thin walled 5cm longbull Emerges at the anterior end of the deep part of the glandbull Runs forward on the hyoglossus between lingual and hypoglossal nervesbull It opens on the floor of the mouth on the summit of the sublingual
papilla at the side of the frenulum of the tongue
Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Blood Supply and Lymphatic Drainage
bull Arterial supply Facial artery
bull Venous drainage Common facial or lingual vein
bull Lymph Passes to the submandibular lymph nodes
Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Nerve Supply
PARASYMPATHETIC SUPPLY
Superior salivatory nucleus
7th cranial nerve
submandibular ganglion
CN VII nerve
Gland
SYMPATHETIC SUPPLY
Vasomotor
Plexus around the facial artery
bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull (a) US image shows a nondilated Wharton duct (arrow) in a slim patient Arrowheads = submandibular gland 1 = mylohyoid muscle (b)Diagram shows the course of the Wharton duct (arrow) Arrowheads = submandibular gland 1 = mylohyoid muscle 2 = sublingual gland
SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

SUBLINGUAL GLAND
Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Sublingual Glandbull Smallest of the three major glands
bull Almond shaped and weighs about 3-4 g
bull Lies above the mylohyoid muscle and below the mucosa of the floor of the mouth
bull Medial to the sublingual fossa and lateral to genioglossus
Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Sublingual gland
bull The Whartons duct and lingual nerve separate the sublingual gland from the medial genioglossusmuscle
bull It opens via multiple ducts usually 20 in number (known as ducts of Rivinus) directly into the floor of mouth along sublingual papillae and folds
bull Occasionally some of the ducts unite to form the Bartholins duct that drain into the Whartons duct
bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull 15 ducts emerge from the gland most of which open directly into the floor of the mouth
bull A few join the submandibular duct
bull Blood supply from lingual and submentalarteries
bull Nerve supply is same as that for submandibular gland
Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Minor salivary glands
bull - Except for the gingiva and anterior hard palate minor salivary glands (500-1000 1-5 mm each) are located throughout the submucosa of the oral cavity- More numerous in posterior hard palate- Each salivary unit has its own simple duct- Most of these minor salivary glands are mucinous with the main exception of Ebnerrsquosglands which are serous glands located in the circumvallate papillae of the tongue
Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Innervation
bull Salivary glands are innervated either directly or indirectly by the parasympathetic and sympathetic arms of the autonomic nervous system Both result in increased amylase output and volume flow
bull Parasympathetic innervation to the salivary glands is carried via cranial nerves The parotid gland receives its parasympathetic input from the glossopharyngeal nerve (CN IX) via the otic ganglion while the submandibular and sublingual glands receive their parasympathetic input from the facial nerve (CN VII) via the submandibular ganglion
bull Direct sympathetic innervation of the salivary glands takes place via preganglionic nerves in the thoracic segments T1-T3 which synapse in the superior cervical ganglion with postganglionic neurons that release norepinephrine which is then received by β-adrenergic receptors on the acinar and ductal cells of the salivary glands leading to an increase in cyclic adenosine monophosphate (cAMP) levels and the corresponding increase of saliva secretion
SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

SALIVARY GLAND FUNCTION
SECRETION OF SALIVA
bull DIGESTIVE ENZYMES
bull MOISTENING OF FOOD
bull PROTECTIVE FUNCTION
PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

PATHOLOGY AND IMAGING
bull The common clinical indications of salivary gland imaging are pain and swelling
bull Imaging is useful in identifying the masses of salivary glands and also in differentiating them from the massespathologies of adjacent cervical spaces especially parapharyngeal masticator and submental spaces and mandibular lesions
bull Nodal masses peripheral nerve schwannomas and masseteric hypertrophy may mimic tumors of salivary glands clinically
bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull In proven cases of salivary gland tumors imaging helps in delineating the extent of the lesion and invasion of adjacent cervical spaces skull base mandible and nervesmeninges
bull The disease of major salivary gland can be broadly categorized into the inflammatory neoplastic systemic and congenital conditions
Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Imaging Armamentarium for Salivary Gland Imaging Includes
bull Plain radiography
bull Sialography (conventional CT MRI)
bull High-resolution ultrasonography (HRUS)
bull Computed tomography (CT)
bull Magnetic resonance imaging (MRI)
bull Radionuclide scintigraphy
ReferrencePictorial essay Salivary gland imaging Rajul Rastogi et al
Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Plain Radiography
bull This is the simplest oldest and cheapest way of studying the salivary glands It is useful in detecting ductal calculi calcifications (as in hemangioma and lymph nodes) and adjacent osseous lesions Only one-fifth of the salivary ductal calculi are radiolucent
bull Parotid gland radiography requires posteroanterior projection with extended chin open mouth and cheeks blown out to delineate Stensons duct lesion
bull Submandibular gland radiography requires posteroanteriorand ipsilateral oblique projection with extended chin open mouth and tongue depressed by patientsrsquo finger
bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Plain radiograph of the submandibular region in AP (A) and lateral oblique (B) projection showing soft tissue swelling associated with a small calculus (arrow) visible on lateral oblique view taken with depressed tongue
Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Sialography
bull It refers to the evaluation of the ductal system of the salivary glands It is considered the gold standard technique for studying the ductal morphology
bull It is commonly used for parotid and submandibular glands and its main indication is chronic sialadenitis unrelated to sialolithiasis
bull Acute sialadenitis is a contraindication for sialography Irregular pooling of contrast and ductal obstruction without presence of calculus are indirect signs of malignancy
bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Sialography is rarely used for sublingual imaging because of numerous small ducts opening directly into the floor of mouth
bull Sublingual glands may however be visualized in an anatomic variation where the Bartholins duct is outlined following injection of the contrast medium into the Whartons duct
bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull This test is performed by injecting oil water soluble iodine containing contrast solution into the Stensonrsquos Whartonrsquos duct
bull Water soluble diatrizoate meglumine and iodipimide meglumine are preferred because of their low viscosity and ease of injection Water soluble agents also cause very little foreign body reaction
bull This imaging modality is very rarely used in sublingual imaging because the ducts are numerous and small
bull They open directly to the floor of the mouth Sublingual Sialography is possible only in patients with anatomic variations like filling up of Bartholinrsquos duct from injection of Whartonrsquos duct during submandibular Sialography
bull Since about 80 of salivary gland calculi are radio opaque plain film study is a must before Sialography
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated
Procedure
bull Stensonrsquos duct Whartonrsquos duct is progressively dilated gently Infiltration of local anesthetic agent may be necessary Sialographic canula is connected to a contrast laden syringe and is inserted into the duct After fluoroscopically verifying the position of the canula the contrast material is slowly injected Irregular contrast pooling and ductal obstruction are considered features of malignancy
bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Conventional sialographyof submandibular (A) and parotid glands (B) showing ductal system
bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull However 3DCT performed especially with cone-beam CT following injection of the contrast medium into the ductal system without intravenous injection of contrast can provide images similar to or better than conventional sialography and is often referred to as CT sialography
bull MR Sialography by contrast delineates the ductal system of the gland without injection of ductalintravenous contrast by utilizing the highly fluid-sensitive sequences similar to that used for magnetic resonance cholangiopancreatography(MRCP)
bull MR Sialography can be performed in patients of acute sialadenitis Prior administration of a sialogogue agent may improve ductal visualization in MR Sialography
bull MR Sialography has poor spatial resolution as compared to conventional sialography
bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull MR sialography shows bilateral Stemsons duct (arrows)
High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

High-resolution Ultrasonography
bull It is a quick and noninvasive method of evaluating parotid and submandibular glands Both glands appear homogeneously hyperechoicon HRUS and retromandibular vein can be noted within the parotid gland
bull It is performed by a high-frequency linear (7-10 MHz) transducer
bull It helps in differentiating cystic from solid lesions and also aids in guiding the exact site of Fine N eedle A spiration C ytology (FNAC) in suspected salivary gland lesions
bull It fails to demonstrate the parotid gland in its entirety because of intervening mandible It also does not clearly demonstrate the intraglandular facial nerve branches
bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull HRUS images showing normal parotid and submandibular glands (top row) and retromandibularvein in the parotid gland (arrow)
bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull When combined with color Doppler imaging it helps in assessing the vascularity and nature of the lesion (malignant lesions of salivary glands are highly vascular as compared to their benign counterparts ndash peripheral vascularity with hypovascular central area in the tumoral lesion is highly suggestive of pleomorphic adenoma)
bull RI and PI values of greater than 07 and 12 respectively coupled with high PSV (greater than 443 cms) ill-defined margins and nodal involvement with central vascularity are highly indicative of malignant salivary gland lesion
bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull In experienced hands it helps in differentiating intra-parotid nodes from true intraparenchymal lesions picking soft calcificationsdiffuse lesions and detecting major ductal dilatation with intraductal calculi
bull However it cannot optimally evaluate the deep lobe of the parotid gland
HRUS images show altered echopattern of the parotid gland with ductal dilatation (thin arrow) and small calculus (thick arrow) at its terminal end
CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

CT and MRI
bull These cross-sectional studies help in true and near complete imaging of the salivary glands
bull MRI because of its multiplanar capability and higher soft tissue resolution has an upper hand over CT in demonstrating the extent of lesion and their perineuralmeningeal spread
bull However CT (especially cone-beam CT) demonstrates the osseous lesionsextension and calcificationcalculus better than MRI
bull Noncontrast CT may be enough in cases of sialolithiasis However ductal system is not optimally evaluated by any of these techniques
bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Non-contrast axial CT image showing submandibular sialolithiasis on right side (white arrow) and normal gland on left side
bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Non-contrast T2W axial amp coronal images (top row) and T1W axial and coronal images showing parotid (thick white arrows) and submandibular glands (thin white arrow)
bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull These studies are often performed after intravenous injection of the contrast media for better delineation of the anatomy and the extent of lesion
bull Diffusion-weighted (DW) images and gadolinium-enhanced dynamic MR (Gd-MRI) imaging have proven to be very useful in differentiating benign from malignant tumors
bull DW images can be used to calculate apparent diffusion coefficient (ADC) values which are different for different salivary gland tumors
bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Gd-MR with dynamic imaging using 120 s as cut-off for time to peak enhancement and 30 wash-out ratio can differentiate benign and malignant tumors as the latter take less time for peak enhancement and show rapid wash-out
bull Plateau type of timendashintensity curve in dynamic Gd-MR coupled with low ADC values is also highly suggestive of malignancy
bull Proton MR Spectroscopy has also been described for differentiation of benign from malignant tumors by some authors
bull Cholinecreatinine ratios are significantly lower in malignant than in benign salivary gland tumors
PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

PET Scanbull Very sensitive for metastatic LN lt 8mmbull Helpful for previously treated H + N cancersbull Positron emission tomography (PET) imaging using 2-deoxy-2-[18F]
fluoro-d -glucose (FDG) can be used to differentiate benign from malignant tumors of the salivary glands as the former appear as cold spots with the exception of Warthins tumor and oncocytoma
PETCT Scanbull Has increased value in salivary gland tumour stagingbull Pittsburgh study(55pts) showed
bull sensitivity of 744bull specificity of 100
Angiography or MRI-Angiobull Can be used to assess carotid artery involvement
Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Radionuclide Imaging
bull It is a rarely used technique for salivary gland imaging Sodium pertechnetate (Tc[99]) is actively concentrated and secreted by salivary gland cells while it is not taken up by majority of neoplastic lesions hence the latter appear as cold spots Warthins tumor is an exception to the rule and appears as a hot spot
bull Actively dividing cells take up Gallium-67 hence it is useful in detecting diffuse inflammatoryneoplastic processes such as sarcoidosis and lymphoma
Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Salivary Gland Neoplasms
bull Diverse histopathology
bull Relatively uncommon
ndash 2 of head and neck neoplasms
bull Distribution
ndash Parotid 80 overall 80 benign
ndash Submandibular 15 overall 50 benign
ndash SublingualMinor 5 overall 40 benign
Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Staging
bull AJCC Cancer Staging Manual (sixth edition)
bull Based on tumor size local extension of tumor nodal metastasis and distant metastasis
bull Histologic grade patient age and tumor site are important additional factors that should be considered in future staging systems
TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

TNM
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor 2 cm or less in greatest dimension without gross
extraparenchymal extension
T2 Tumor more than 2 cm but not more than 4 cm in greatest
dimension without gross extraparenchymal extension
T3 Tumor more than 4 cm andor tumor having gross
extraparenchymal extension
T4a Tumor invades skin mandible ear canal andor facial nerve
T4b Tumor invades skull base andor pterygoid plates andor encases
carotid artery
TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

TNM
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in a single ipsilateral lymph node 3 cm or less in
greatest dimension
N2a Metastasis in a single ipsilateral lymph node more than 3 cm but
not more than 6 cm in greatest dimension
N2b Metastasis in multiple ipsilateral lymph nodes none more than 6
cm in greatest dimension
N2c Metastasis in bilateral or contralateral lymph nodes none more
than 6 cm in greatest dimension
N3 Metastasis in a lymph node more than 6 cm in greatest dimension
TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

TNM
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Stage GroupingStage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1 N1 M0
T2 N1 M0
T3 N1 M0
Stage IVA T4a N0 M0
T4a N1 M0
T1 N2 M0
T2 N2 M0
T3 N2 M0
T4a N2 M0
Stage IVB T4b Any N M0
Any T N3 M0
Stage IVC Any T Any N M1
Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Histologic Grade
bull Histologic grading is applicable only to some types of salivary gland cancer (mucoepidermoid carcinoma adenocarcinoma not otherwise specified)
bull In most instances the histologic type defines the grade (ie salivary duct carcinoma is high grade basal cell adenoma is low grade)
bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Benign Neoplasmsndash First branchial cleft cysts
ndash Hemangiomas
ndash Lymphangiomas
ndash Pleomorphic adenomasbull Carcinoma ex pleomorphic adenoma
bull Carcinosarcoma
bull Metastasising mixed tumour
ndash Warthins tumour
ndash Rare bull Oncocytomas
bull Myoepitheliomas
bull Monomorphic adenomas
bull Basal cell carcinoma
ndash Lipomas
First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

First branchial cleft cysts
First branchial cleft cysts typically manifest in middle aged women with a history of recurrent parotid gland infection unresponsive to antibiotics Occasionally a fistula can be observed at the angle of the mandible First branchial cleft cysts account for 8 of all branchial complex anomalies These cysts occur in or directly adjacent to the parotid gland At ultrasound (US) these cysts may look solid due to internal haemorrhage or infection Colour Doppler does not show any flow suggesting the cystic nature of the lesion At CT or MRI after administration of contrast medium the cyst wall may be thickened and enhance due to infection Increased signal intensity on T1-weighted sequences suggests prior bleeding or infection
Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Haemangiomas
Haemangiomas manifest as unilateral parotid swelling shortly after birth A bluish discoloration of the skin can often be seen These lesions are the most common benign salivary gland masses in children with a female predilection
They are classified as capillary or cavernous at pathology About 90 represent congenital capillary haemangiomas which spontaneously regress until adolescence Cavernous haemangiomas are rare manifest in older children and do not undergo resolution
At CT or MRI capillary haemangiomas are seen as welldefinedmasses with strong enhancement Flow voids due to prominent vasculature are often present in or around the mass
Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Axial grey-scale ultrasound shows
a solid hypoechoic well-circumscribed mass (arrows) involving superficial and deep lobes of the parotid gland
Power Doppler ultrasound shows marked vascularity within the mass consistent with hemangioma
Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Transverse section of the masseter muscle reveals a hypoechoic compressible vascular mass diagnosis - hemangioma
T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

T1-weighted axial (A) and T2-weighted axial images with fat saturation demonstrate enlargement and replacement of the left parotid gland by a cystic-appearing lesion
The lesion remains well encapsulated and has an enlarged flow void in the retromandibular vein consistent with a hemangioma
Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Lymphangiomas
Lymphangiomas are congenital malformations of the
lymphatic system with an incidence of 90 at the age of
2 years Infection or haemorrhage may occur however
in contrast to haemangiomas spontaneous regression is
rare
At imaging lymphangiomas consist of cystic areas
and thin septations but also solid enhancing portions
Haemorrhage can lead to fluid levels with variable signal
intensities depending on the duration of the bleeding
Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Hypoechoic septated compressible lesion with no detectable flow on Colour Doppler assessment Lymphangioma of the neck was histologically proven
CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

CT scan (A) and T2-weighted MR image (B) with fat saturation demonstrate a cystic nonenhancing lesion replacing the left parotid gland
There is extension beyond the capsule into the floor of the mouth and into a retropharyngeal location consistent with a lymphangioma
Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Pleomorphic Adenomabull Most common of all salivary gland
neoplasmsndash 70 of parotid tumors
ndash 50 of submandibular tumors
ndash 45 of minor salivary gland tumors
ndash 6 of sublingual tumors
bull 4th-6th decades
bull FM = 3-41
bull The alternative term mixed tumours is attributed to the histological heterogeneity suggesting a variety of imaging findings
bull Slow-growing painless mass
bull Parotid 90 in superficial lobe most in tail of gland
bull Minor salivary gland lateral palate submucosal mass
There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

There are three malignancies associated with pleomorphic adenoma
(1) The carcinoma ex-pleomorphic adenoma
ndash The carcinoma ex-pleomorphic adenoma is a malignant change of a benign mixed tumour or a malignant tumour in a patient who previously underwent surgery for a pleomorphic adenoma
ndash Carcinoma ex-pleomorphic adenomas have a high metastatic rate varying from 25 to 76 into regional lymph nodes lungs bones and brain
(2) The rarer variant the true malignant mixed tumour (carcinosarcoma)
ndash The carcinosarcoma is rare and has a bad prognosis
(3) The metastasising mixed tumour
ndash The metastasising lsquobenignrsquo mixed tumour is the rarest variant
ndash Metastases may be multiple and occur in the lung bone and soft tissue often over decades
Small benign mixed tumours are usually hypointense in T1- and hyperintense in T2-weighted sequences Inhomogeneity is seen in larger tumours whereas low signal intensity on T2-weighted images may be observed in carcinoma ex-pleomorphic adenomas
bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Gross pathology
ndash Smooth
ndash Well-demarcated
ndash Solid
ndash Cystic changes
ndash Myxoid stroma
bull Histologyndash Mixture of epithelial myopeithelial and
stromal componentsndash Epithelial cells nests sheets ducts
trabeculaendash Stroma myxoid chrondroid fibroid osteoidndash No true capsulendash Tumor pseudopods
Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Imaging findings
bull Usually depend on tumour size
bull Small tumours
ndash more homogeneous and well defined
ndash strong enhancement after contrast medium administration in CT and MRI
bull Larger tumours
ndash pedunculated outgrowth from the main lesion (lobulated contour)
ndash more heterogeneous including necrotic and haemorrhagic areas
bull The recurrence rate varies between 1 - 50 depending on the initial surgical procedure
bull Recurrences are often multiple and clustered
bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Radiographic features
ndash Although findings do depend on tumour size in general they are well circumscribed rounded masses most commonly located within the parotid gland
ndash When they arise from the deep lobe of the parotid they can appear entirely extraparotid seen in the parapharyngeal space without a fat plane between it and the parotid and widen the stylomandibular tunnel
ndash Pleomorphic adenomas can also arise from salivary rest cells in the parapharyngeal space itself without connection to the parotid gland
bull Ultrasound
ndash Typically hypoechoic May show a lobulated distinct border +- posterior acoustic enhancement
ndash Ultrasound is also useful in guiding biopsy (both FNAC and core biopsies) but needs to be carried out with care to avoid facial nerve damage
bull Doppler
ndash Vascularization in pleomorphic adenomas is often poor or absent (even when the sensitive power Doppler mode is used) but may be abundant After inadequate surgery pleomorphic adenomas often recur usually multifocally
Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Longitudinal section through the left parotid gland demonstrates a lobulated mass in the superficial lobe of the gland distorting the capsule There is associated distal acoustic enhancement Note marked heterogeneity of internal architecture Biopsy confirmed this lesion to represent a pleomorphicadenoma The mandible is indicated by arrowheads
Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Ultrasound image shows well defined hypoechoic structure with slightly lobular contours increased through-transmission of ultrasound and mild vascularity
Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Pleomorphic adenoma
CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

CTSmoothly marginated or lobulated homogeneous small spherical mass is the most common appearance When larger they can be heterogeneous with foci of necrosis Small regions of calcification are common 1When small enhancement tends to be prominent In larger tumours enhancement is less marked but can demonstrate delayed enhancement
MRIThey are commonly seen as well-circumscribed and homogeneous when small Larger tumours may be heterogeneousT1 - usually of low intensityT2
usually of very high intensity (especially myxoid type) 6
often have a rim of decreased signal intensity on T2-weighted images representing the surrounding fibrous capsule
T1 C+ (Gd) - usually demonstrates homogeneous enhancement
Angiography (DSA)Typically hypovascular
(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

(a) Transverse early phase helical CT scan shows multinodular heterogeneous enhancement of the mass The central portion (short arrows) of the mass is more strongly enhanced than is the peripheral area (long arrow) of the mass (b)Transverse delayed phase CT scan shows slightly increased enhancement of the two parts of the tumor which are labeled as in a (c) Coronal image obtained 7 minutes after contrast material injection shows that the multinodular enhancement of the tumor(arrows) has disappeared and become homogeneous
Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Pleomorphic Adenoma
bull Treatment complete surgical excision
ndash Parotidectomy with facial nerve preservation
ndash Submandibular gland excision
ndash Wide local excision of minor salivary gland
bull Avoid enucleation and tumor spill
Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Warthinrsquos Tumor
bull AKA (adenolymphoma or papillary cystadenoma lymphomatosum)
bull 6-10 of parotid neoplasms
bull Older Caucasian males
bull 10 bilateral or multicentric
bull 3 with associated neoplasms
bull Presentation slow-growing painless mass
bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Warthin tumours present as well-circumscribed partly cystic partly solid lesions in CT or MRI often located in the tail of the parotid gland
bull Enhancement after contrast medium administration is often relatively poor
bull In the differential diagnoses of multiple lesions metastases lymphoma or inflammatory disease must be considered
Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Gross pathology
bull Encapsulated
bull Smoothlobulated surface
bull Cystic spaces of variable size with viscous fluid shaggy epithelium
bull Solid areas with white nodules representing lymphoid follicles
Histology
bull Papillary projections into cystic spaces surrounded by lymphoid stroma
bull Epithelium double cell layerndash Luminal cellsndash Basal cells
bull Stroma mature lymphoid follicles with germinal centers
Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Warthin tumor in the parotid gland in a 45-year-old man (a) Transverse early phase helical CT scan shows a well-defined mass (arrows) in the left parotid gland There is strong enhancement of the tumor with central low attenuation suggestive of a cystic or necrotic area (b) Transverse delayed phase scan shows decreased enhancement of the tumor (arrows)
Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Bilateral Warthin tumors Bilateral parotid masses (arrows) are seen on this transverse contrast materialndashenhanced fat-saturated T1-weighted spin-echo (SE) (75030 repetition time msececho time msec]) MR image The multiplicity and location at the tail of the parotid gland (near the lower mandible) are typical features of this tumor
Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Proton density-weighted (200030) MR image shows a 1-cm lesion (arrow) in superficial aspect of left parotid gland
bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Other benign tumours such as oncocytomas myoepitheliomas monomorphic adenomas and basal cell adenomas are relatively rare benign tumours of the parotid gland and lack typical imaging patterns
bull Lipomas however can easily be diagnosed by CT or MRI thanks to their fat content with typical low attenuation values on CT and signal intensities isointense to fat on all pulse sequences on MR imaging
Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Oncocytoma
bull Rare 23 of benign salivary tumors
bull 6th decade
bull MF = 11
bull Parotid 78
bull Submandibular gland 9
bull Minor salivary glands palate buccal mucosa tongue
Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Oncocytoma
bull Presentation
ndash Enlarging painless mass
bull Technetium-99m pertechnetate scintigraphy
ndash Mitochondrial hyperplasia
Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Oncocytoma
bull Grossndash Encapsulated
ndash Homogeneous smooth
ndash Orangerust color
bull Histologyndash Cords of uniform cells and
thin fibrous stroma
ndash Large polyhedral cells
ndash Distinct cell membrane
ndash Granular eosinophilic cytoplasm
ndash Central round vesicular nucleus
A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

A left parotid oncocytoma in a 68-year-old woman
CT scan reveals a large deformable tumor (white asterisk) which extends medially into the parapharyngealspace through the stylomandibulargap
The contour of the tumor is distorted by the styloid process (black arrow) and the left medial pterygoid muscle (black arrowheads)
Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Monomorphic Adenomas
bull Monomorphic adenomas include basal cell adenoma clear cell adenoma glycogen-rich adenoma and other rare tumors
bull Treatment consists of resection with a margin of normal tissue
Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Basal cell adenoma Canalicular adenoma
Rarity Most common (18) Relatively less common
Age 6th decade 7th decade
Sex (MF) 11 118
Location Most commonly parotid and minor salivary glands of upper lip
Minor salivary glands of upper lip (74)
Presentation Painless submucosal mass
Characteristics Well circumscribed and encapsulated mass
bull Solid type solid nests of tumour cells present
bull Trabecular type cells in trabecular pattern with vascular stroma
bull Tubular type Multiple duct-like structures and vascular stroma
Well circumscribed with multiple foci
Tubular structures line by columnar or cuboidal cells with vascular stroma
Radiological features lack typical imaging patterns lack typical imaging patterns
A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

A 59-year-old woman with a palpable mass in the left parotid
regionContrast-enhanced axial CT scan shows a round well-defined mass in the superficial lobe of left parotid gland with homogeneous enhancement
Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Myoepithelioma
bull lt1 of all salivary neoplasms
bull 3rd-6th decades
bull FgtM
bull Minor salivary glands gt parotid gt submandibular gland
bull Presentation asymptomatic mass
Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Precontrast axial CT scan shows a round well-defined mass (2739 HU) in the superficial lobe of the right parotid gland abutting on the capsule of gland (arrow) B Contrast-enhanced axial CT scan shows the mass (10211 HU) with homogeneous strong enhancement (arrow)
Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Precontrast axial CT scan shows an indistinct margin mass in the superficial lobe of the left parotid gland abutting on the capsule of the gland with calcification (arrow) B Contrast-enhanced axial CT scan shows the mass with inhomogeneous enhancement It contains a central enhancing nodule (small black arrow) and a nonenhancing peripheral cystic component (white arrow)
MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

MALIGNANT NEOPLASMS
bull Mucoepidermoid carcinomabull Adenoid cystic carcinomabull Acinic cell carcinomabull Polymorphous low grade adenocarcinomabull Adenocarcinomabull Primary squamous cell carcinomabull Salivary duct carcinomabull Primary lymphomabull Godwinrsquos tumorbull Metastases
Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Mucoepidermoid Carcinoma
bull Most common salivary gland malignancy
bull 5-9 of salivary neoplasms
bull Parotid 45-70 of cases
bull Palate 18
bull 3rd-8th decades peak in 5th decade
bull FgtM
bull Caucasian gt African American
Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Mucoepidermoid Carcinoma
bull Presentation
ndash Low-grade slow growing painless mass
ndash High-grade rapidly enlarging +- pain
ndash Minor salivary glands may be mistaken for benign or inflammatory process
bull Hemangioma
bull Papilloma
bull Tori
Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Mucoepidermoid Carcinoma
bull Gross pathology
ndash Well-circumscribed to partially encapsulated to unencapsulated
ndash Solid tumor with cystic spaces
Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Lateral view of a parotid sialogram shows a mass that has caused ductal erosion and lack of parenchymal filling
These findings suggest a high-grade malignancy
This patient had a highgrade MEC
Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Mucoepidermoid carcinoma of theparotid gland
Transverse CT scan shows anill-defined mass (C) that has less attenuation than that of enhancing parotid tissue in the right parotid gland
bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Treatment
ndash Influenced by site stage grade
ndash Stage I amp II
bull Wide local excision
ndash Stage III amp IV
bull Radical excision
bull +- neck dissection
bull +- postoperative radiation therapy
Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Adenoid Cystic Carcinoma
bull Overall 2nd most common malignancy
bull Most common in submandibular sublingual and minor salivary glands
bull M = F
bull 5th decade
bull Presentation
ndash Asymptomatic enlarging mass
ndash Pain paresthesias facial weaknessparalysis
bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Gross pathology
ndash Well-circumscribed
ndash Solid rarely with cystic spaces
ndash infiltrative
Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Histology
bull Cribriform pattern
ndash Most common
ndash ldquoswiss cheeserdquo appearance
bull Tubular pattern
ndash Layered cells forming duct-like structures
ndash Basophilic mucinous substance
bull Solid pattern
ndash Solid nests of cells without cystic or tubular spaces
A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

A coronal T1 weighted MR images (repetition timeecho time (TRTE) = 50015) of the sublingual gland tumour
The margin of the tumour is well-defined and the tumour is composed of cystic and solid components The solid area (lingual side) of the tumour shows isointense to the surrounding muscle and extends into the hyperintense cystic area
A coronal fat-saturated T2 weighted image (TRTE = 350096) The tumour is circumscribed by a hypointense fibrous capsule The signal intensity of the tumour is heterogeneous
bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Treatmentndash Complete local excision
ndash Tendency for perineural invasion facial nerve sacrifice
ndash Postoperative XRT
bull Prognosisndash Local recurrence 42
ndash Distant metastasis lung
ndash Indolent course 5-year survival 75 20-year survival 13
Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Acinic Cell Carcinoma
bull 2nd most common parotid and pediatric malignancy
bull 5th decade
bull FgtM
bull Presentationndash Solitary slow-growing often painless mass
bull Tumors occur in several configurations including cystic papillary vacuolated or follicular
Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Acinic Cell Carcinoma
bull Gross pathology
ndash Well-demarcated
ndash Most often homogeneous
bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Treatment
ndash Complete local excision
ndash +- postoperative XRT
bull Prognosis
ndash 5-year survival 82
ndash 10-year survival 68
ndash 25-year survival 50
Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Salivary duct carcinoma
bull Uncommon but highly aggressive malignant tumour
bull Mainly of the parotid gland
bull Male predilection
bull Perineural spread as well as lymph node involvement (70) are frequent findings observed in this particular tumour type
bull MR features Ill-defined margins and low to moderately high signal intensity on T2-weighted images could be observed in all patients on MR imaging
bull Differential diagnosis to a benign salivary gland cyst can be difficult on non-contrast images only
Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Axial CT scan showing no mass lesion in right submandibular gland (white arrow) but multiple metastatic nodes in right upper neck (open arrows) (B and C) 8F-FDG PET scans showing focal 18F-FDG uptake in submandibular area (black arrow) as well as on right side of upper neck (open arrows) Salivary duct carcinoma of 17 cm arising in right submandibular gland with multiple cervical metastases was demonstrated histologically after surgery (D) Newly diagnosed lung metastasis (arrow) 10 mo after surgery and postoperative radiotherapy
Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Polymorphous Low-Grade Adenocarcinoma
bull 2nd most common malignancy in minor salivary glands
bull 7th decade
bull F gt M
bull Painless slowly growing indolent submucosal mass
bull Soft tissue of the palate followed by the lips buccal mucosa tongue floor of the mouth and pharynx are the most affected areas
bull The main histological aspects of PLGA are cytological uniformity and a broad spectrum of growth patterns within the same lesion
bull These growth patterns are represented by lobular cribriform tubular trabecular papillary and cystic structures
Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Squamous Cell Carcinoma
bull 16 of salivary gland neoplasms
bull 7th-8th decades
bull MF = 21
bull MUST RULE OUTbull High-grade mucoepidermoid carcinoma
bull Metastatic SCCA to intraglandular nodes
bull Direct extension of SCCA
bull This malignancy occurs more often in the submandibular gland than the parotid gland
Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Squamous Cell Carcinoma
bull Gross pathology
ndash Unencapsulated
ndash Ulcerated
ndash Fixed
ndash firm indurated mass
bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Proper diagnosis of squamous cell carcinoma requires exclusion of contiguous spread of a squamous cell carcinoma into the gland metastases to the gland and high-grade mucoepidermoid carcinoma
bull There is a high incidence of regional and distant metastases
bull The prognosis for squamous cell carcinoma of the salivary gland is poor
bull Therapy consists of complete surgical resection and postoperative radiation therapy
The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

The typical imaging features are necrotic areas in solid tumours best recognised in fat suppressed T1- weighted MR images after administration of contrast medium or in enhanced CT images
Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Axial contrast-enhanced CT scan shows a necrotic right parotid mass that has infiltrated the entire gland and the adjacent masseter muscle This patient had an SCC of the parotid gland
Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Squamous Cell Carcinoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosis
ndash 5-year survival 24
ndash 10-year survival 18
Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Adenocarcinoma
bull Rare
bull 5th to 8th decades
bull F gt M
bull Parotid and minor
salivary glands
bull Presentation
ndash Enlarging mass
ndash 25 with pain or facial weakness
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland This neoplasm represents approximately 15 of malignant parotid neoplasms Adenocarcinomas usually present as a palpable mass They behave aggressively with a strong propensity to recur and metastasize
Grossly adenocarcinoma is firm or hard and attached to the surrounding tissue Microscopically the cylindric cells of variable height form papillae acini or solid masses
Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining
The degree of glandular formation has been used as a means of grading these tumors
Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Adenocarcinomas can be classified according to their histological findings
bull grade 1 tumours are circumscribed and minimally invasive
bull grade 2 tumours are in between grade 1 and grade 3
bull grade 3 tumours are more solid with a greater mitotic rate
bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

bull Treatmentndash Complete local excision
ndash Neck dissection
ndash Postoperative XRT
bull Prognosisndash Local recurrence 51
ndash Regional metastasis 27
ndash Distant metastasis 26
ndash 15-year cure ratendash Stage I = 67
ndash Stage II = 35
ndash Stage III = 8
Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Malignant Mixed Tumors
bull Carcinoma ex-pleomorphic adenomabull Carcinoma developing in the epithelial component
of preexisting pleomorphic adenoma
bull Carcinosarcomabull True malignant mixed tumormdashcarcinomatous and
sarcomatous components
bull Metastatic mixed tumorbull Metastatic deposits of otherwise typical
pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinoma Ex-Pleomorphic Adenoma
bull 2-4 of all salivary gland neoplasms
bull 4-6 of mixed tumors
bull 6th-8th decades
bull Parotid gt submandibular gt palate
bull Risk of malignant degenerationbull 15 in first 5 years
bull 95 after 15 years
bull Presentationbull Longstanding painless mass that undergoes sudden
enlargement
Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinoma Ex-Pleomorphic Adenoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Hemorrhage and necrosis
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated
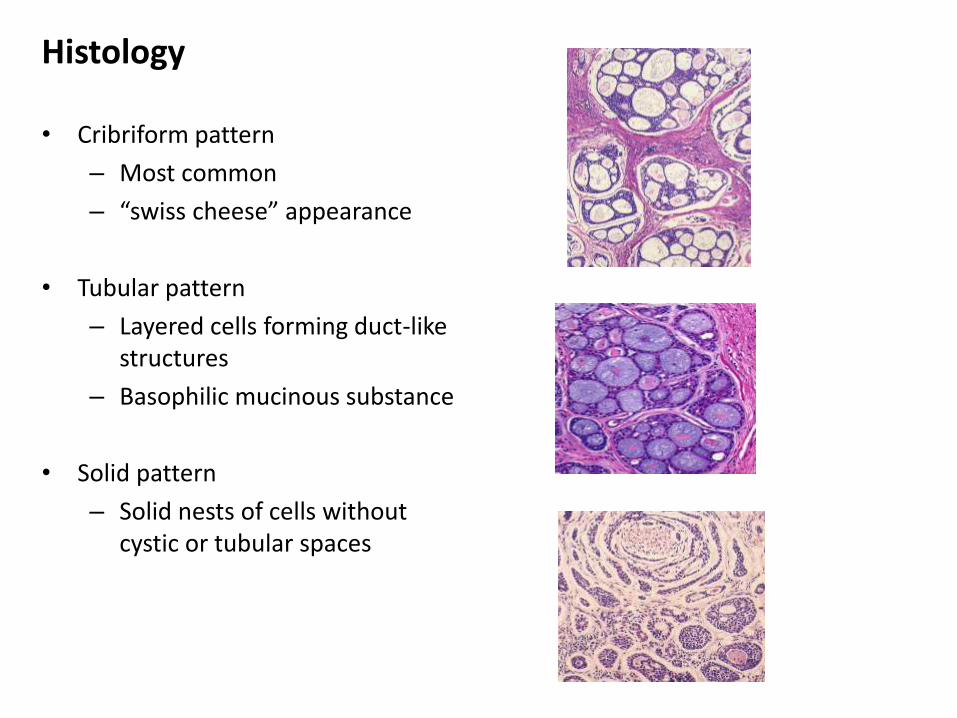
There is a large nonhomogeneous mass in the left submandibular gland
Septations are present within the mass and there is a lobulated contour
This was a carcinoma ex pleomorphic adenoma
Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinoma Ex-Pleomorphic Adenoma
bull Treatment
ndash Radical excision
ndash Neck dissection (25 with lymph node involvement at presentation)
ndash Postoperative XRT
bull Prognosis
ndash Dependent upon stage and histology
Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinosarcoma
bull Rare lt05 of salivary gland neoplasms
bull 6th decade
bull M = F
bull Parotid
bull History of previously excised pleomorphic adenoma recurrent pleomorphic adenoma or recurring pleomorphic treated with XRT
bull Presentation
Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinosarcoma
bull Gross pathology
ndash Poorly circumscribed
ndash Infiltrative
ndash Cystic areas
ndash Hemorrhage necrosis
ndash Calcification
A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

A 55-year-old woman with carcinosarcomaof tonsillar minor salivary glandorigin
CT scan of the head and cervical regionshows a large 60 3 62 3 75-cmheterogeneously enhancing mass obstructing the oropharynx The mass involves the soft palate and extends into the left parapharyngeal and pharyngeal mucosal spaces the masticator space and the prevertebral space The mass abuts the left carotid space posteriorly displacing the left internal and external carotid arteries (arrows) Nolymphadenopathy is seen
Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Contrast-enhanced T1-weighted MR image (500251) of the mass shows moderate homogeneous enhancement
Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Carcinosarcoma
bull Treatment
ndash Radical excision
ndash Neck dissection
ndash Postoperative XRT
ndash Chemotherapy (distant metastasis to lung liver bone brain)
bull Prognosis
ndash Poor average survival less than 2 frac12 years
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated
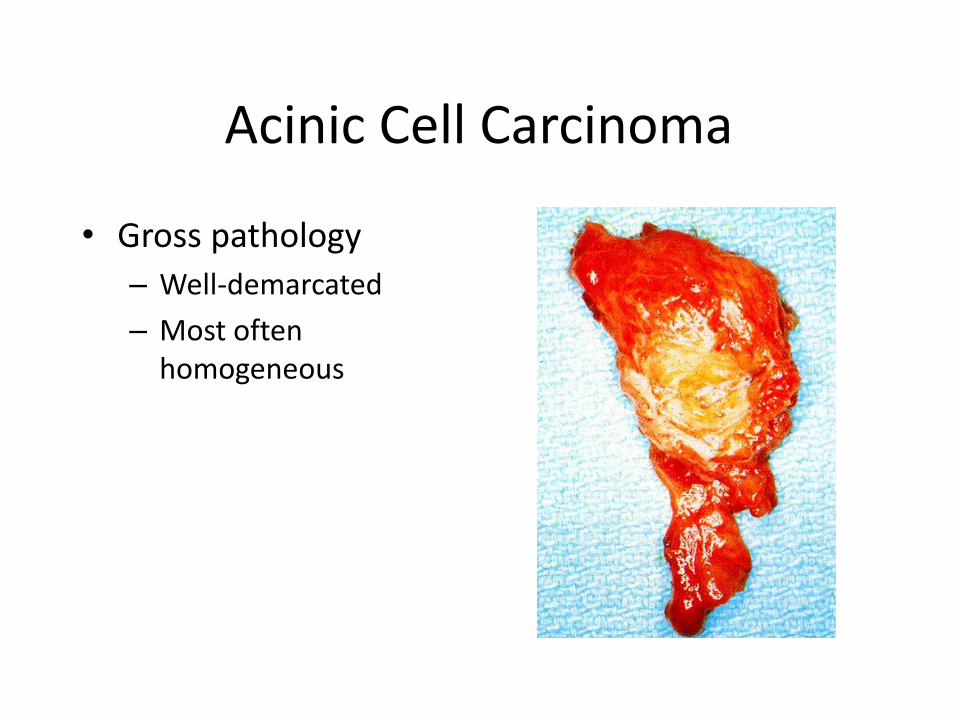
Clear Cell Carcinoma
bull AKA glycogen-rich
bull Palate and parotid
bull 6th-8th decade
bull M = F
bull Histologybull Uniform round or
polygonal cells
bull Peripheral dark nuclei
bull Clear cytoplasm
bull Treatmentbull Complete local excision
Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Epithelial-Myoepithelial Carcinoma
bull lt 1 of salivary neoplasmsbull 6th-7th decades F gt M
parotidbull Increased risk for 2nd
primarybull Histology
bull Tumor cell nestsbull Two cell typesbull Thickened basement
membrane
bull Treatmentbull Surgical excision
Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Primary lymphomabull Rare
bull Can only be diagnosed if there is no evidence of intra-or extraglandularnodal involvement
bull These lymphomas are considered as extranodal marginal zone B-cell lymphomas
bull Incidence 1 and 8 of the patients with lymphomas
bull All forms of Hodgkinrsquos and non-Hodgkinrsquos lymphomas have been reported
bull In the case of secondary lymphomatous involvement of the salivary glands the parotid gland is involved in about 80
bull In patients with Sjogrenrsquos syndrome the prevalence of non-Hodgkinrsquos lymphoma is about 44 times greater compared to control subjects therefore lymphoma has to be ruled out by imaging in this particular patient population
Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Undifferentiated Carcinoma
bull Lymphoepithelialbull Eskimos parotid F gt M
familial
bull Asian submandibular M gt F
bull Large-cellbull Bimodal peaks
bull M gt F
bull Parotid
bull Small-cellbull 6th-7th decades
bull MF = 161
bull parotid
Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Metastases
bull Metastases to salivary glands are mainly observed in the parotid gland due to the presence of intraglandular lymph nodes which drain the face external ear and scalp
bull Skin malignancies (melanoma squamous cell carcinomas) are the most common primary tumours metastasising to the salivary glands therefore careful clinical examination has to be performed
bull However other malignancies such as renal cell carcinomas lung breast and gastrointestinal carcinomas can also metastasise to the parotid gland or periparotid lymph nodes
US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

US image shows an oval well-defined homogeneous tumor with even margins (arrows) in the right submandibular gland the parenchyma of the gland (arrowheads) has been changed by therapeutic neck irradiation Despite its benign features the tumor proved to be a metastasis from a squamous cell carcinoma at the base of the tongue
Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Power Doppler US image shows a metastasis (arrowheads) to the superficial lobe of the parotid gland (arrows) from a melanoma The tumor is lobulated inhomogeneous and virtually anechoic with posterior acoustic enhancement and chaotic mainly peripheral vessel segments
Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Represents a manifestation of autoimmune disease in the salivary glands
This benign entity may be difficult to distinguish from malignant tumours due to bull its focal characterbull contrast medium enhancement bull its irregular margins
The benign lymphoepithelial lesion (BLEL) or Godwinrsquos tumour
Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated

Conclusions
bull Hugely diverse histopathology
bull Accurate pathologic diagnosis does influence management
bull Relatively rare malignancies
bull Utilize preoperative studies when indicated
