imaging of viral encephalitis
TRANSCRIPT


Imaging of viral encephalitis
Osama A. RagabAssist,Lec of Neurology

introduction The word “virus” is derived from the Latin word for
poison.
Viruses are infectious, obligate intracellular parasites
whose genomes consist of either DNA or RNA.
A minimal virus consists of a genome plus a
proteinaceous coat, known as a capsid.
Enveloped viruses, are enclosed by a host cell-
derived lipid bilayer studded with virus-specified
glycoproteins.
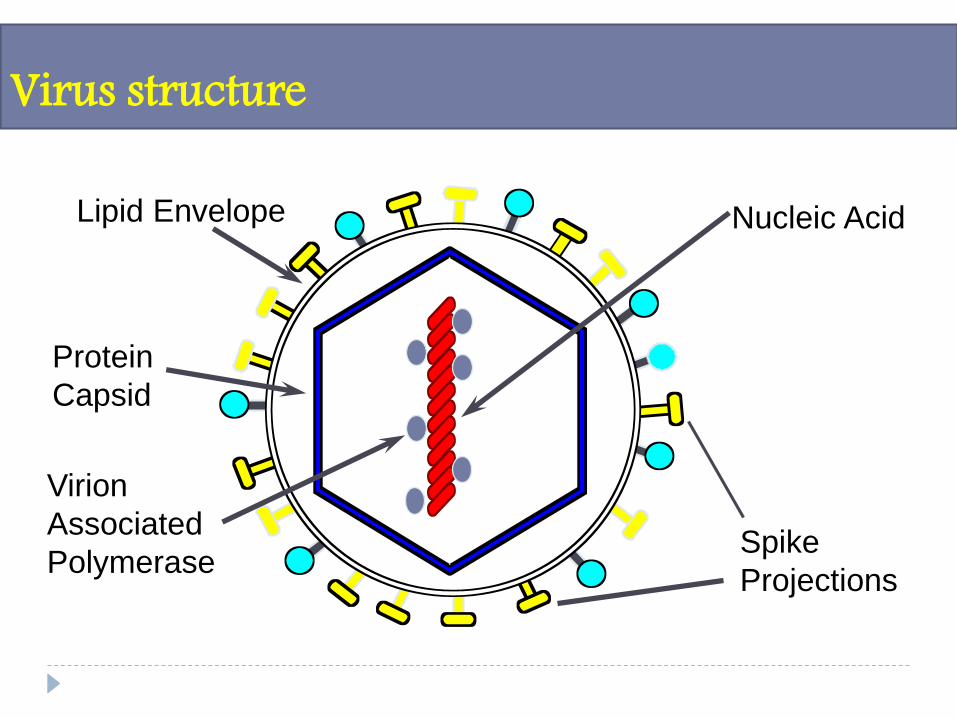
Virus structure
Nucleic Acid
Spike
Projections
Protein
Capsid
Lipid Envelope
Virion
Associated
Polymerase

Virus taxonomy
Within the ICTV( the International Committee for
Taxonomy of Viruses) system ,the two major
taxonomic divisions are the viruses with RNA
genomes and those with DNA genomes.
Subsequent taxonomic levels are based on the size
and structure of the capsid and then the nature of
the genome (single-stranded or double-stranded,
linear or circular, segmented or non-segmented).

HERPESVIRIDAE
HEPADNAVIRIDAE
ENVELOPED
PAPILLOMAVIRIDAE
POLYOMAVIRIDAE(formerly grouped together as the
PAPOVAVIRIDAE)
CIRCULAR
ADENOVIRIDAE
LINEAR
NON-ENVELOPED
DOUBLE STRANDED
PARVOVIRIDAE
SINGLE STRANDED
NON-ENVELOPED
POXVIRIDAE
COMPLEX
ENVELOPED
DNA VIRUSES
Virus taxonomy

FLAVIVIRIDAETOGAVIRIDAE
RETROVIRIDAE
ICOSAHEDRAL
CORONAVIRIDAE
HELICAL
ENVELOPED
ICOSAHEDRAL
PICORNAVIRIDAECALICIVIRIDAE
ASTROVIRIDAE
NONENVELOPED
SINGLE STRANDEDpositive sense
BUNYAVIRIDAEARENAVIRIDAE
ORTHOMYXOVIRIDAEPARAMYXOVIRIDAE
RHABDOVIRIDAEFILOVIRIDAE
SINGLE STRANDEDnegative sense
REOVIRIDAE
DOUBLE STRANDED
RNA VIRUSES
ENVELOPED
HELICAL ICOSAHEDRAL
NONENVELOPED
Virus taxonomy

Geographic distribution of selected viruses causing central nervous system infection.

Neurotopic virus

HERPESVIRUSES

HERPESVIRUSES
Family Herpesviridae includes over 80 viruses
distributed among three subfamilies: Alpha, Beta and
Gamma.
Human viruses are members of the Alpha
herpesvirinae: HSV-1 and HSV-2 and varicella-
voster virus .
Human Beta herpesvirinae include human
cytomegalovirus human herpesviruses 6A and 6B
and human herpesviruses 7.
Human Gamma herpesvirinae are hosts to Epstein–
Barr virus and human herpesvirus 8 .

These viruses are neurotropic and establish latent
infections in ganglionic neurons during primary
infection, subsequently reactivating to cause
recurrent disease or subclinical virus shedding,
promoting spread to new hosts.
Associated diseases include peripheral neuropathies
such as postherpetic neuralgia, Bell’s palsy, and
potentially life-threatening encephalitis .
HERPESVIRUSES
Pathologically, HSV-1 results in a necrotizing
infection involving the :
inferomedial aspect of the temporal lobes.
the inferior frontal cortex .
the cingulate cortex .
the subfrontal and insular regions.
Further progression of disease may result in
petechial hemorrhages and eventual cavitation
Herpes simplex virus 1 (HSV-1)

CT is often normal, although non-specifichypoattenuating lesions in the temporal and/orfrontal lobes with or without enhancement andsuperimposed hemorrhage may be demonstrated insevere illness .
MRI can be normal in up to 10% of patients.
The most characteristic pattern finding is unilateralhigh T2 signal involving the insula, medial temporaland inferior frontal lobes with or withoutinvolvement of the adjacent limbic structures.
Enhancement and hemorrhage become moreprominent with disease progression
Herpes simplex virus 1 (HSV-1)

51-year-old diabetic woman with fever and confusion. (a) Unenhanced axialCT scan shows no significant changes in the left temporal lobe. (b) 2 dayslater unenhanced axial CT scan is still unremarkable. (c) 14 days later,unenhanced axial CT scan shows marked hypodensity in the left temporallobe
Herpes simplex virus 1 (HSV-1)
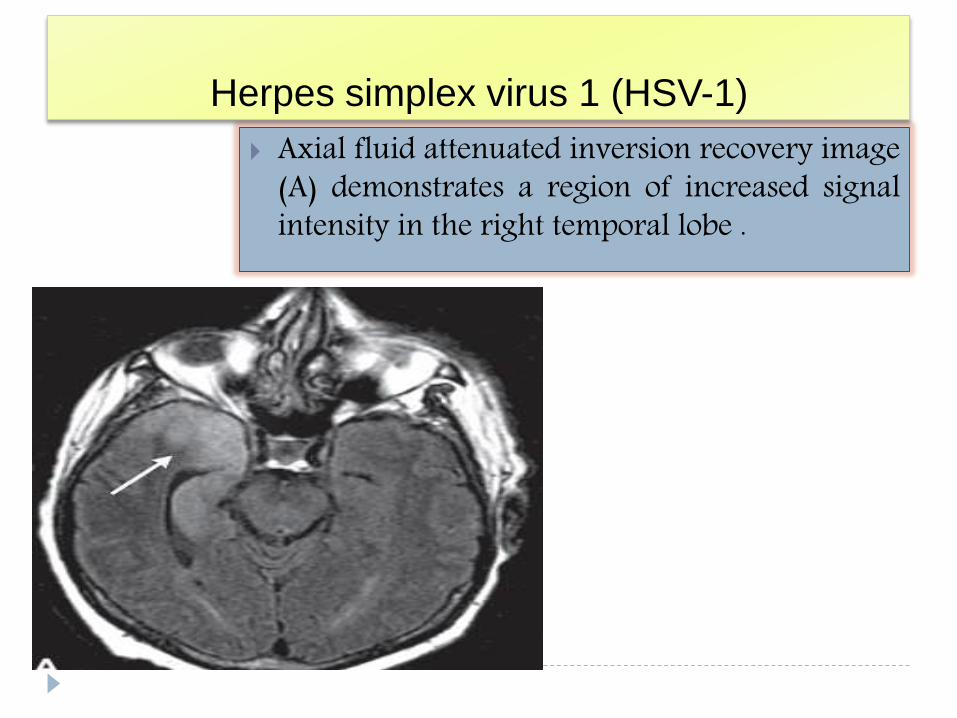
Axial fluid attenuated inversion recovery image(A) demonstrates a region of increased signalintensity in the right temporal lobe .
Herpes simplex virus 1 (HSV-1)

Herpes simplex virus 1 (HSV-1)Axial T1 Image demonstrate curvilinear regions of high T1 signal intensitywithin the right temporal lobe (arrow,), compatible with petechialhemorrhage in this patient with herpes encephalitis.

DWI demonstrates regions of patchy
restricted diffusion and may be more sensitive
than T2-weighted or FLAIR imaging in
depicting regions of encephalitis
Herpes simplex virus 1 (HSV-1)

DWI classic herpes encephalites note abnormalhyperintense signal abnormallity in bilateal mesialtemporal corex .
Herpes simplex virus 1 (HSV-1)

classic herpes encephalites noteabnormal hyperintense signalabnormallity in bilateal mesial temporalcorex & cingulate gyri on T2 & FLAIRimages with reduced diffusivity.
Herpes simplex virus 1 (HSV-1)

T1 with contrast

HSV-2 may result in severe neonatal encephalitis,
with transmission most commonly occurring through
an infected birth canal .
Pathologic examination demonstrates diffuse
parenchymal and leptomeningeal inflammation
which can progress to hemorrhage and necrosis.
MR demonstrating loss of gray–white differentiation
and high T2 signal within the periventricular and
subcortical white matter, with relative sparing of the
central gray matter (basal ganglia, thalami) and
posterior fossa.
Herpes simplex virus 2 (HSV-2)

With disease progression, decreased T2 signal
intensity within the cortex may develop
corresponding to the presence of focal hemorrhagic
necrosis and parenchymal calcifications .
Severe cerebral sequelae such as cystic
encephalomalacia or hydranencephaly may
eventually be seen with more advanced disease
Herpes simplex virus 2 (HSV-2)

Cortical blurring and gyral/leptomeningeal enhancement in neonatal HSV-2encephalitis in different patients.
A Axial T2-weighted image demonstrates reduced cortical gray white matterdifferentiation (arrowheads) in the right temporal lobe.
B Gyral/leptomeningeal contrast enhancement (arrows) in the right temporalregion on the coronal image after gadolinium administration in the samepatient .

a Axial FLAIR image is normal in this 13-dayold patient presenting with signs of sepsis andculture negative meningitis 2 days prior to thisexamination. No abnormality was seen on anyof the conventional MR images .
Herpes simplex virus 2 (HSV-2)
Axial DW image demonstrates a focus of
restricted diffusion (arrow) in the uncal
region of the medial anterior left temporal
lobe,

Axial DW image demonstrates
restricted diffusion in the left caudate
nucleus head (arrowhead) and the right
lentiform nucleus (arrow) in addition to
the left occipitotemporoparietal and
right parietal regions
Herpes simplex virus 2 (HSV-2)
Axial CT image of the same patient as in a
obtained 3 years later demonstrates cystic
encephalomalacia in the left occipito-
temporo-parietal region (asterisk).
There is also hypoattenuation in the left
caudate nucleus head (arrowhead) and the
right lentiform nucleus (arrow), indicative
of old necrosis.

Axial DW image in another patientdemonstrates restricted diffusionin the pons (arrow) and deepcerebellar hemispheres(arrowheads).
Herpes simplex virus 2 (HSV-2)
End-stage neonatal HSV-2 encephalitis
This axial noncontrast CT image
demonstrates severe necrotic changes
and encephalomalacia involving the
frontal and parietal lobes bilaterally. The
relative prominence of the basal ganglia
(arrowheads) and thalami (arrows)

Meningoencephalitis with MRI demonstrating diffuse,
multifocal areas of high T2 signal intensity within the
cerebral cortex.
Diffuse encephalitis results in non-specific regions of
high T2 signal within the white matter.
VZV involvement of large vessels at the base of the
brain may result in a variety of pathologic findings,
ranging from necrotizing arteritis to remote vascular
occlusion within the small blood vessels of the brain
resembling atherosclerotic disease.
Varizella-zoster virus (VZV)

The spread of VZV from blood vessels to the
ependymal cells lining the ventricles may result in
ventriculitis, resulting in abnormal ependymal
enhancement and high T2/FLAIR signal intensity.
spread of VZV to oligodendrocytes can result in a
multifocal leukoencephalopathy which manifests as
subcortical high T2 signal plaques which may
demonstrate enhancement after gadolinium contrast
administration
Varizella-zoster virus (VZV)

Varicella-zoster virus encephalitis with multifocal vasculopathy. Axial fluid
attenuated inversion recovery (FLAIR) (A) and T2-weighted image (B)
demonstrate high FLAIR signal in the left caudate nucleus and in the posterior
limb of the internal capsule as well as hyperintense T2 signal along the right
paramedian frontal lobe. Magnetic resonane angiogram (C) demonstrates
irregular narrowing in the left proximal middle cerebral and right anterior cerebral
artery.

Magnetic resonance image of a 6-month-old boy. (a, b) AxialT2 gradient echo sequence: blood in the ventricles andhydrocephaly. (c) Axial TI sequence after gadolinium infusion:no abnormal enhancement. (d) FLAIR sequence: noparenchymal abnormality.

Magnetic resonance image of a 35-year-old man. (a-c) Cranial magnetic resonance image, FLAIRsequence showing punctiform hyperintensities subcortical (right frontal and left temporal) and in thepons. (d) Sagittal dorsal spinal cord, T2 sequence: hypersignal at the T7-T8 level.

Magnetic resonanceimage of a 20-year-oldman. Narrowing of the Mlsegment of the middlecerebral artery.

Epstein-Barr virus (EBV)
EBV infection of the nervous system is uncommon
but may result in meninigitis, encephalitis, myelitis,
and/or cranial nerve palsies .
CT findings are often normal .
MRI may demonstrate non-specific high signal
intensity within the cerbral cortex, at the gray–white
junction, and/or within the deep nuclei (basal
ganglia, thalamus) on T2-weighted images which
may resolve on subsequent imaging.

case reports of progression to hemorrhagic
encephalitis have been published and should be a
consideration with worsening neurologic deficits.
EBV infection has a high association with primary
CNS lymphoma in the setting of acquired immune
deficiency syndrome (AIDS) .
Epstein-Barr virus (EBV)

Epstein–Barr virus. Axial T2-weighted image (A) imaging demonstrates
abnormal increased signal in the right temporal lobe. Axial T2-weighted image
(B) performed 3 days later demonstrates progression of abnormal signal in the
right temporal lobe.
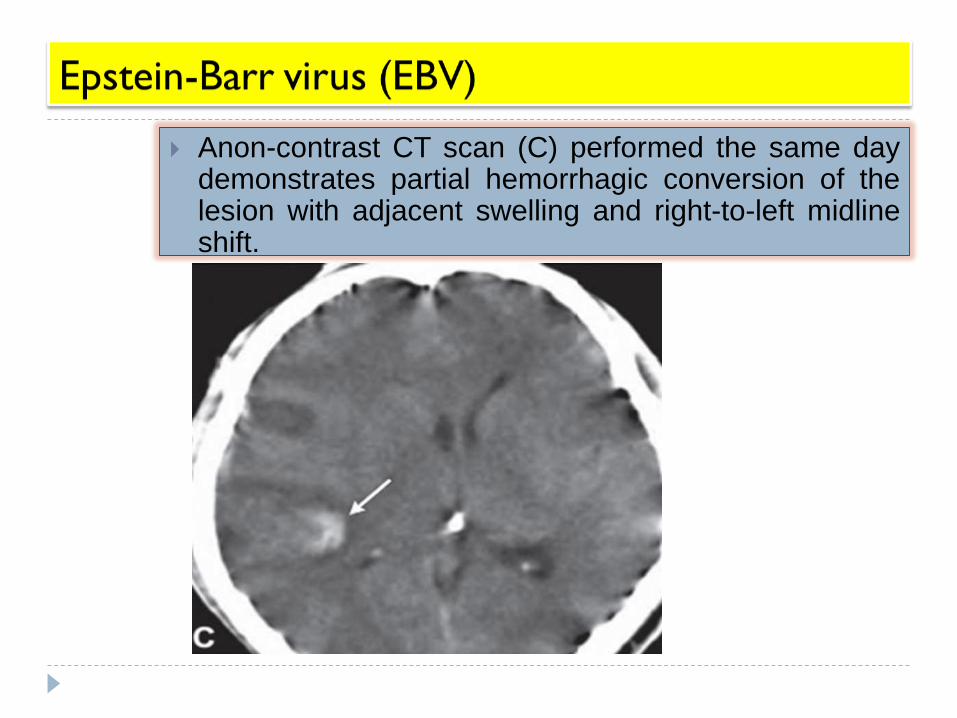
Anon-contrast CT scan (C) performed the same daydemonstrates partial hemorrhagic conversion of thelesion with adjacent swelling and right-to-left midlineshift.
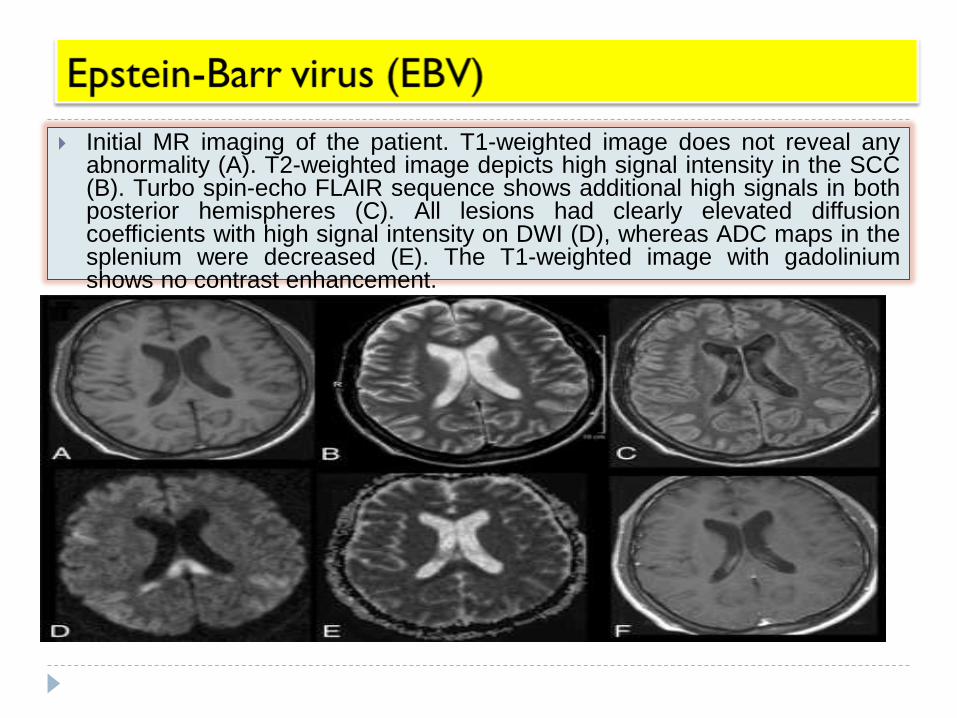
Initial MR imaging of the patient. T1-weighted image does not reveal anyabnormality (A). T2-weighted image depicts high signal intensity in the SCC(B). Turbo spin-echo FLAIR sequence shows additional high signals in bothposterior hemispheres (C). All lesions had clearly elevated diffusioncoefficients with high signal intensity on DWI (D), whereas ADC maps in thesplenium were decreased (E). The T1-weighted image with gadoliniumshows no contrast enhancement.

Brain MRI scan findings in a 12-year-old boy with Epstein–Barr virusencephalitis. The scans were performed 1 day before the patient died. (A,B)These axial diffusion-weighted images show focal lesions of increasedsignal intensity— indicative of cytotoxic edema in the cerebellum, brainstem,basal ganglia and hippocampus—scattered throughout the subcortical whitematter and cerebral cortex. Ventricles are not significantly narrowed. (C)Sagittal T1-weighted image that shows generalized cerebral edema withherniation of the brainstem and cerebellar tonsils into the foramen magnum.

CMV infection of the nervous system is most often seen
with immunocompromised patients .
CMV is the leading cause of congenital CNS infection,
with an incidence of approximately 1–2% of live births.
The resultant imaging findings reflect the distribution of
disease: meningitis, encephalitis,
ventriculoencephalitis, myelitis, and retinitis .
CT imaging is less sensitive than MRI and may
demonstrate non-specific cortical atrophy and/or
decreased attenuation within the white matter .
With contrast-enhanced imaging, periventricular
enhancment may be present, indicative of underlying
ventriculoencephalitis .
Cytomegalovirus (CMV)

MRI demonstrates non-specific increased T2 and
decreased T1 signal abnormalities in the white
matter which may have a patchy or confluent
distribution .
Nodular increased T2 signal abnormalities may also
be noted within the brainstem, basal ganglia,
cerebellum, and hippocampus, some of which may
undergo hemorrhagic transformation.
Occasionally, CMV infection may present as a ring-
enhancing cerebral mass with marked edema
mimicking an intracranial neoplasm.
Cytomegalovirus (CMV)
CT imaging in infants with congenital CMV infection
classically shows intracranial calcifications in a
periventricular distribution, hydrocephalus, cortical
atrophy, subdural hematomas, or effusion and non-
specific white-matter hypodensities
CMV infection early in utero results in abnormal fetal
brain development, migrational, cortical gyral
abnormalities, delayed myelination, cerebellar
hypoplasia and porencephalic cysts.
Cytomegalovirus (CMV)

In uterocytomegalovirus (CMV) infection. Coronal true inversion recovery image
demonstrates thickened and disordered cortex in the right frontal and temporal
lobes (arrows) compatible with pachygyria in this infant within uteroCMV infection.

In utero cytomegalovirus (CMV) infection. Axial non-contrast computed
tomography scan of the head demonstrates massive hydrocephalus as well as
bilateral periventricu-lar calcifications in this infant with in utero CMV infection.

In uterocytomegalovirus (CMV) infection. Coronal T2-weighted image
demonstrates thickened and disordered cortex in the right frontal and temporal
lobes (arrows) compat-ible with pachygyria in this infant with in utero CMV
infection.

Axial (a) T1 and (b) T2 weighted MRI show mild ventricular dilatation and multiple tiny nodular T2 high-signal intensity lesions in basal ganglia and right frontal subcorticalwhite matter without definite periventricular signal change. (c) Axial fluid attenuated inversion recovery image shows thin curvilinear high-signal intensities along the walls ofboth lateral ventricles and multifocal faint high-signal intensities at right frontal and basal ganglia regions. (d) Axial contrast enhanced T1 weighted image shows subtlesubependymal enhancement (arrow). (e,f) Diffusion weighted image shows striking curvilinear high-signal intensities along the ventricular wall with a subtle low apparentdiffusion coefficient value (arrow).

Reactivation of latent HHV-6 infection in
immunocompromised patients, may result in an
encephalitis, leptomeningitis, or neuritis .
The most common findings include symmetric or
asymmetric high T2 signal within the uncus,
amgydala, and hippocampal body with extension to
the rhinal cortex .
DWI may show the earliest signs of the underlying
inflammatory changes with patchy regions of
restricted diffusion in the involved neural tissue
Herpes simplex virus 6 (HSV-6)

Herpes simplex virus 6 (HSV-6)
Human herpesvirus-6 (HHV) infection. Axial fluid attenuated inversion recovery
image of the brain demonstrates symmetric high signal abnormalitywithin the
limbic system in this patient who developed HHV-6 infection after a bone mar-
row transplant for treatment of lymphoma.

Flaviviruses

Humans typically acquire infection through the bite ofan infected mosquito or tick .
The major human pathogens among the Flavivirus genusare yellow fever virus, Dengue virus, Japaneseencephalitis virus (JEV), St. Louis encephalitis virus(SLEV), tick-borne encephalitis virus (TBEV), and WNV
( West Nile virus ).
Flaviviruses

JEV primarily affects developing neurons in thalamus,hippocampus, and midbrain, while anterior horn cells ofthe spinal cord and brainstem are the primary targets ofTBEV.
The disease spectrum of JEV ranges from non-specificfebrile illness to aseptic meningitis, meningoencephalitis,flaccid paralysis, and encephalitis .
Parkinsonian movement disorder and seizures have alsobeen reported. Clinical syndromes associated with WNVinclude meningitis, encephalitis, and acute flaccidparalysis
Flaviviruses

St. Louis encephalitis (SLE)
SLE is transmitted through a mosquito-borne virus
and has resulted in several epidemics in the eastern
and central United States .
perivascular inflammatory changes with neuronal
degeneration and microglial proliferation, most
prominent within the substantia nigra , pons ,insular
cortex and thalami

St. Louis encephalitis. Axial T2-weighted images demonstrate symmetricincreased signal intensity involving the insular cortex and thalami as wellas the substantia nigra, midbrain, and pons
St. Louis encephalitis (SLE)

West Nile encephalitis
West Nile encephalitis is an emerging infection with
a rapid increase in incidence and geographic range.
Transmission is most often through a mosquito-
infected vector, although transmission through
breastfeeding, transplacental has been reported .
Imaging findings in cases of West Nile encephalitis
are non-specific, with a case series reporting
increased T2 signal abnormality most often within
the mesial temporal lobe and midbrain .
Meningeal, cerebellar, cortical, and white-matter
imaging abnormalities are less commonly found .

West Nile encephalitis. Axial fluid attenuated inversion recoveryimages (A, B) demonstrate increased signal in the thalami andcorpus striatum. Increased signal intensity is also noted in themedial temporal lobes and cerebellum (curved arrow,B). Axial T1postcontrast image (C) demonstrates enhancement in the thalami.
West Nile encephalitis
Japanese encephalitis
Japanese encephalitis (JE) is the most frequent
global cause of mosquito-borne encephalitis and is
associated with significant morbidity and mortality.
Pathology studies have demonstrated diffuse
inflammatory changes involving the basal ganglia,
thalamus, cerebral cortex, brainstem, and
cerebellum.
The most consistent finding on MRI is bilateral
increased T2 signal abnormality in the thalami with
or without hemorrhage.

Japanese encephalitis
Japanese encephalitis. Axial fluid attenuated inversion recovery images in
two different patients with Japanese encephalitis demonstrate bilateral
symmetric increased signal intensity (A) and asymmetric right thalamus
signal abnormality B) respectively.

Bunyaviridae

Between the period of October 2003 and April 2005
an epidemic of RVF encephalitis appeared in the
region of Khafer Al-Sheikh Governorate.
Humans can get RVF as a result of bits from
mosquitoes and possibly other blood sucking insects
that serve as vectors. Humans can also get the
disease if they are exposed to either the blood or
other body fluids of infected animals.

MRI of the brain demonstrated the following: patchy
areas of edema targeting the cortical and subcortical
deep white matter and diffusely involving both
cerebral hemispheres. These were evident in the
temporal, frontal, perisylvian and occipitoparietal
regions. Patchy involvement of the mesencephalon,
basal ganglia and posterior nuclei of both thalami .
the affected tissues are emitting subtle decrease in
signal intensity on T1-Weighted images and bright
signal intensity on T2-weighted and FLAIR pulse
sequences
. No associated enhancement or leptomeningeal
reaction.

C.T brain scan demonstrate gray matter affection with
diffuse white matter affection & mainly in the region of
basal ganglia
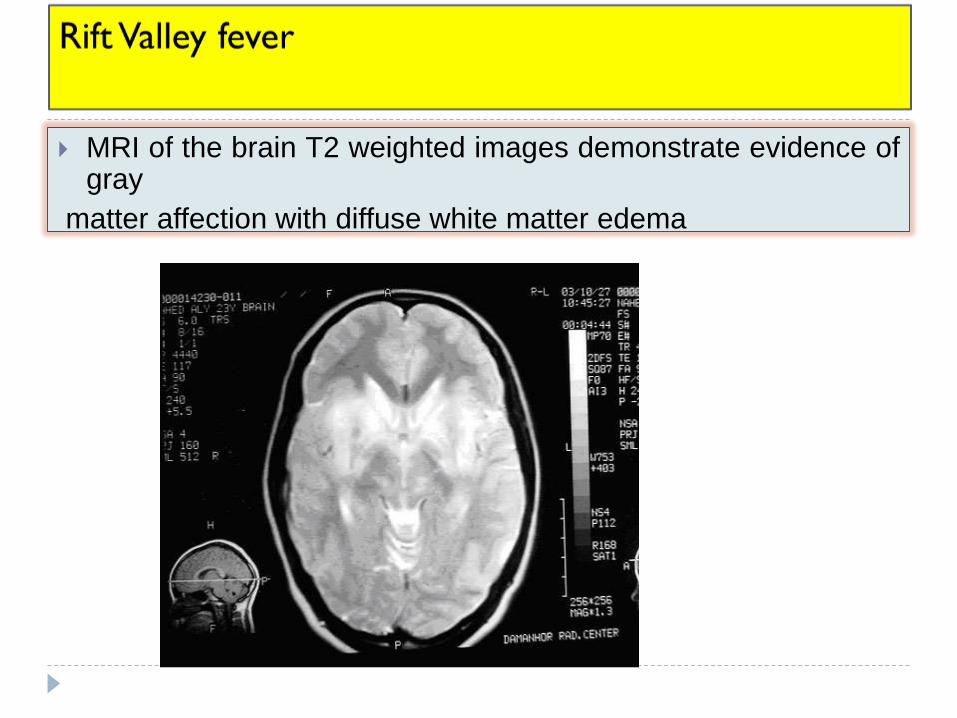
MRI of the brain T2 weighted images demonstrate evidence ofgray
matter affection with diffuse white matter edema

Arenaviruses

Arenaviruses
Lymphocytic choriomeningitis virus can cause
aseptic meningitis (rarely fatal), hydrocephalus, and
more severe CNS disease.
Transmission to human via contact with rodents .
Encephalitis develops in 5–34% of patients.

lymphocytic choriomeningitis virus (LCMV)
prenatal disease may result in devastatingneuroteratogenic effects.
the most common abnormalities included microcephalyand periventricular calcification. Other additionalabnormalities included prominent gyral malformation,ventriculomegaly, hydrocephalus, porencephalic andperiventricular cysts, encephalomalacia, and isolatedcerebellar hypoplasia

2 children with congenital LCMV infection (B, C). (B) The most common abnormalitiesin congenital LCMV infection include periventricular calcifications (arrows) andventriculo-megaly (V), often due either to noncommunicating hydrocephalus or tocerebral atrophy. (C) Some patients with congenital LCMV infection have regions ofencephalomalacia (*), reflecting focal tissue destruction. In addition to massiveencephalomalacia, this patient has periventricular calcifications (arrow). LCMV,lymphocytic choriomeningitis virus.

(B) In congenital LCMV infection, the virus can impair
cerebellar growth and lead to cerebellar hypoplasia
(arrow).

Retroviruses

Retroviruses
The major human retroviruses include human T
lymphotropic viruses 1 and 2 and HIV-1 and -2.
Both HTLV-1 and HTLV-2 have been associated with
HTLV-associated myelopathy/ tropical spastic
paraparesis, a chronic progressive demyelinating
disease that affects the spinal cord and white matter
of the CNS.

Retroviruses
HIV-associated neurologic disorders include
neurocognitive disorders and peripheral
neuropathies as well as vacuolar myelopathy
Other primary neurologic syndromes associated with
HIV include aseptic meningitis, multiple sclerosis-like
disorders, ischemic and hemorrhagic strokes,
primary HIV-induced headache and psychiatric
disorders.

Early changes of HIV encephalitis manifest as
multifocal subcentimeter white-matter lesions
appearing bright on T2-weighted images. These are
generally symmetric and spare the subcortical U-
fibers.
The chronic stage of HIV infection manifests as
progressive white-matter signal abnormality in
conjunction with brain atrophy.
With progression of disease, however, these become
confluent and may extend to involve the basal
ganglia, cortex, cerebellum, brainstem, and spinal
cord
Human immunodeficiency virus

Another chronic feature of HIV infection is
progressive cerebral atrophy, which is most
prominent centrally, resulting in ex vacuo ventricular
dilatation out of proportion to sulcal prominence.
Human immunodeficiency virus

Polyomaviruses

The first human members of family Polyomaviridae, JCvirus (JCV) and BK virus (BKV) (both of genusOrthopolyomavirus).
Reactivation of latent JCV in immune-compromisedindividuals may cause PML.
Polyomaviruses

Progressive multifocal leukoencephalopathy
PML is most commonly seen in the setting of
underlying HIV-1 infection, it may also be seen in the
context of hematologic malignancies and treatment
with immunosuppressive medications.
Lesions appear hyperintense on T2-weighted
images and hypointense on T1-weighted images.
Lesions are most commonly found in the subcortical
and periventricular white matter of the frontal and
parieto-occipital lobes; they are also seen in the
white matter of the cerebellar peduncles or
hemispheres, and in the brainstem

Early on, the lesions may be small but then progress
to form larger areas of involvement, often with a
scalloped border.
The lesions are classically bilateral, asymmetric,
multifocal, and lacking in mass effect. Only 9% of
cases demonstrate enhancement, which is typically
faint and peripheral .
Spinal cord involvement is rare.
Progressive multifocal leukoencephalopathy

This is an MRI of the brain of a PML survivor (PML-S).On the left is a fluid attenuated inverse recovery (FLAIR)image, which shows a large hyperintense lesion in theleft cerebral hemisphere, sparing the cortex. On the rightis the corresponding T1 with gadolinium (contrast) image,which shows no enhancement within the hypointensePML lesion.

This is an MRI of the brain of a PML- survivor. On the left, FLAIR imageshows a large hyperintense lesion in the white matter of the left hemisphere.There is also a shift of the midline (arrow) and disappearance of the sulci(arrowheads), signifying mass effect, as seen in excessive inflammation. Onthe right is the corresponding T1+Gad image; the arrows show enhancementwithin the PML lesion.
Progressive multifocal leukoencephalopathy

Paramyxoviruses

Paramyxoviruses
Measles virus infections can lead to three neurologic
diseases.
Acute disseminated encephalomyelitis that occurs
about a week after the rash phase .
inclusion body encephalitis in immune-suppressed
individuals .
subacute sclerosing panencephalitis .
Aseptic meningitis is the most common neurologic
manifestation of mumps virus infection.
Subacute sclerosing panencephalitis (SSPE)
SSPE is a chronic and progressive encephalitis
caused by a persistent infection of the brain by
measles virus.
Early changes include bilateral, multifocal,
asymmetric T2 hyperintense lesions of the
periventricular and subcortical white matter .
There is a predilection for involvement of the parietal
and occipital lobes .
With time, these lesions may become larger, more
numerous, and more confluent, and appear more
symmetric. Late changes of SSPE include abnormal
signal in the basal ganglia (typically the putamen),

subacute sclerosing panencephalitis (SSPE). Axial T2-weighted image
demonstrates symmetric regions of increased signal intensity in the
subcortical white matter, predominantly in the posterior cerebrum. Serology
titers and electroencephalogram findings were compatible with SSPE.

Rhabdoviruses

Rhabdoviruses
Rabies virus transmitted through skin by animal bites
the virus is transmitted directly to peripheral neurons
and then to the brain, or neuronal transmission
occurs after amplification in skeletal muscles.
Disseminated infection, including transmission from
the brain to salivary glands, occurs late in disease.

Rabies encephalitis
MR features of rabies encephalitis describe ill-
defined mild areas of T2 hyperintensity in the
brainstem, hippocampi, hypothalami, deep and
subcortical white matter, and deep and cortical gray
matter .

Picornaviruses

that include viruses of humans are Enterovirus,Hepatovirus, and Parechovirus. The human enterovirusesinclude poliovirus types 1–3, coxsackieviruses,echoviruses, and rhinoviruses.
Neurologic diseases include the flaccid paralysis of polio,aseptic meningitis, and encephalitis
Picornaviruses

Enteroviral encephalitis
EV71 characteristic MR findings are hyperintensity in
the posterior portions of the medulla and pons,
Severe cases demonstrated involvement of the
ventral horns of the spinal cord, basal ganglia, and
thalami.
The MR finding most characteristic of poliomyelitis is
hyperintensity involving the region of the anterior
horn cells on T2-weighted images .

Enteroviral encephalitis. Axial T2-weighted image demonstrates
symmetric regions of increased signal intensity involving the posterior
pons

Orthomyxoviruse
s

Orthomyxoviruses
Influenza viruses A, B, and C are well known as the
causes of influenza.
Neurologic manifestations of influenza virus include
Reye’s syndrome, febrile seizures, encephalitis,
myelitis, and acute necrotizing encephalopathy
(ANE).
ANE is characterized by bilaterally symmetric
necrotic brain lesions in the thalami, cerebral white
matter, brainstem, and cerebellum .

Influenza A. Axial fluid attenuated inversion recovery (A)andT1postcontrastimage(B)demonstrate bilateral asymmetric non-enhancing regions of high signal intensityinvolving the thalami. A peripheralrim of restricted diffusion is demonstrated on thediffusion-weighted images (arrow,C). The imaging findings are consistent with acutenecrotizing encephalopathy in this patient with serologic titers positive for underlyinginfluenza A infection.
Influenza
