immunity against infection - univerzita...
TRANSCRIPT

Jitka BrazovaJitka Brazova
Immunity Immunity against infectionagainst infection

Entrance
• Pathogenicity mechanisms• Escape mechanisms• Amount • Genes regulating immune reaction
• Actual state of host organism

Epithelial bariers against infections
• Mechanic (intact epithelial surface, longitudinal airand liquids flow)
• Chemical (fatty acids on the skin surface, enzymes –lysozyme in saliva, sweat and tears, pepsin in gut, low pH in stomach, antibacterial peptides in gut)
• Microbial (normal flora – compete, prevention of adhesion, production of antibacterial substances)


Recognition of pathogen
• Receptors on innate immune cells (APC) - Direct: Toll Like Receptors (TLR - 11),
lectin receptors, - Indirect: Fc receptors, complement
receptors (CR3,CR4)• Humoral factors: complement, CRP, MBL



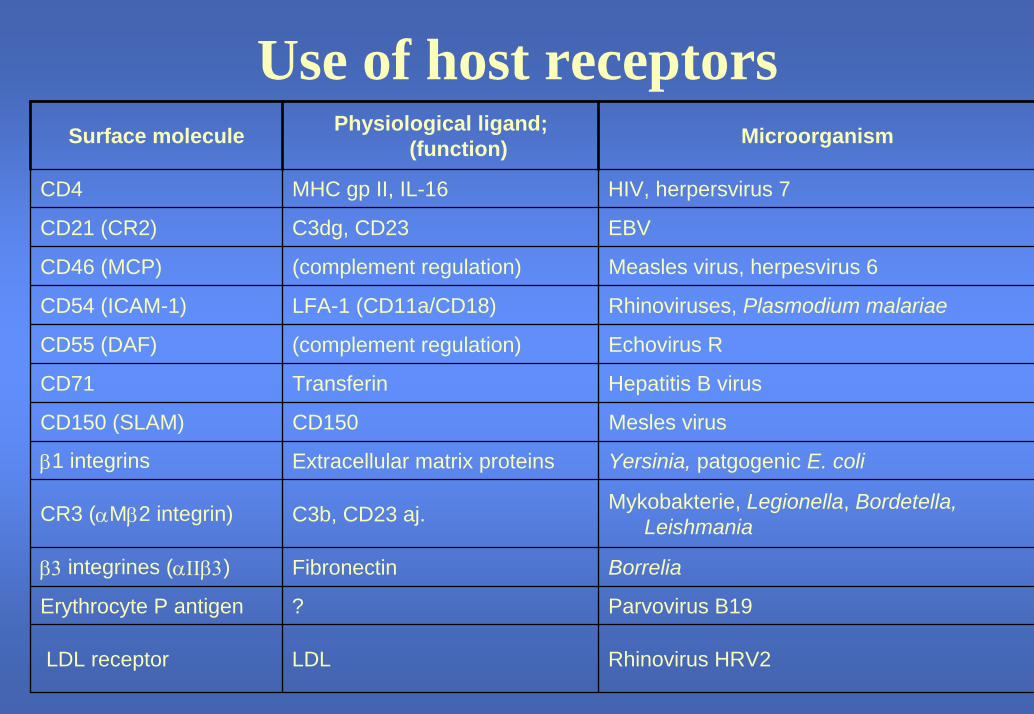
Use of host receptorsSurface molecule Physiological ligand;
(function) Microorganism
CD4 MHC gp II, IL-16 HIV, herpersvirus 7
CD21 (CR2) C3dg, CD23 EBV
CD46 (MCP) (complement regulation) Measles virus, herpesvirus 6
CD54 (ICAM-1) LFA-1 (CD11a/CD18) Rhinoviruses, Plasmodium malariae
CD55 (DAF) (complement regulation) Echovirus R
CD71 Transferin Hepatitis B virus
CD150 (SLAM) CD150 Mesles virus
β1 integrins Extracellular matrix proteins Yersinia, patgogenic E. coli
CR3 (αMβ2 integrin) C3b, CD23 aj. Mykobakterie, Legionella, Bordetella, Leishmania
β3 integrines (αΙΙβ3) Fibronectin Borrelia
Erythrocyte P antigen ? Parvovirus B19
LDL receptor LDL Rhinovirus HRV2

Adhesion of the pathogen andbeginning of immune response

Innate immunity components in infection defence
• alternative and lectin complement pathwayactivation – opsonisation, lysis
• phagocytosis - local inflammatory reaction• production of cytokines and acute phase
reactants• antigens presentation to specific immune
components (macrophages, DC, APC)

Innate immunity components in infection defence II.
• Interferons production• NK cells activity• gamma/delta T lymphocytes• B1 lymphocytes CD5+,
production of IgM antibodies

Specific immune components in infection defence
• APC• Activation of T lymphocytes• Th1 and Th2 subtype diferenciation of T
lymphocytes • efector mechanisms - cellular
- humoral• imunologic memory (afinit maturation,
CD45RO, persist IC on FDC)

Immune components in infection defence
• Extracelullar microorganisms (extracellular phase of microorganism life) – humoral immunity
• Intracellular microorganisms – cellularimmunity

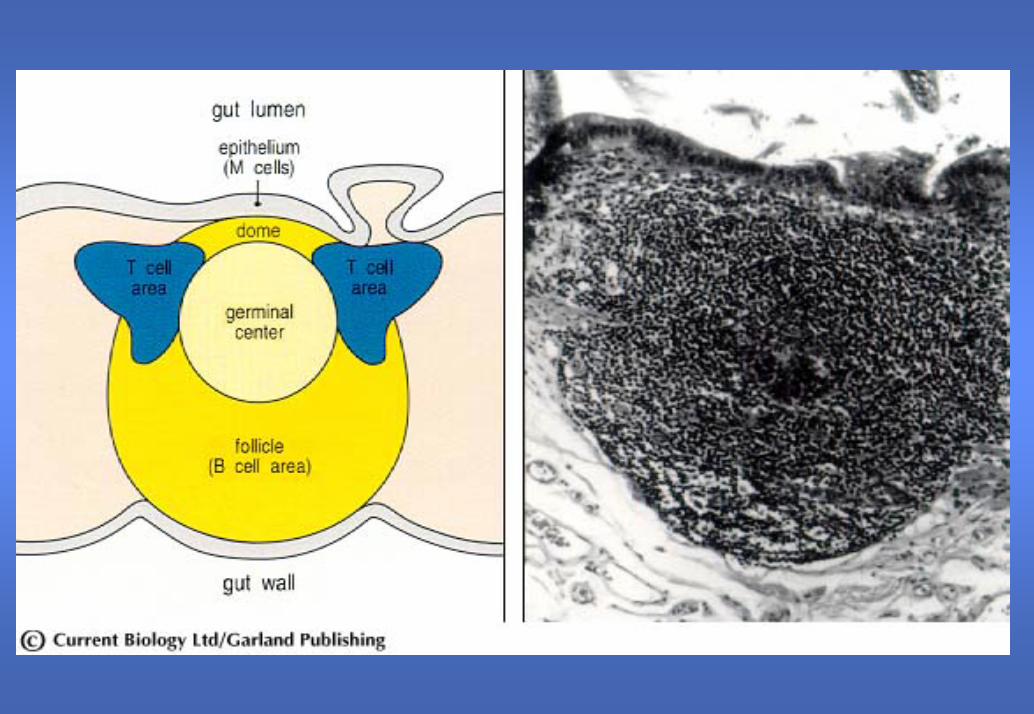
Mucous immunity
• 400 m2
• MALT, GALT , BALT, NALT• o-MALT (places of immune reaction
induction, Payer´s patches, lymphoidfolicules)
• d-MALT (efector places, IEL, lamina propria B and T lymphocytes, neutrophils, eosinophils, mast cells)

Immunoglobulin A
• IgA dimer binds to secretory componentand is transepithelialtransported
• Secretory IgA isresistant to protheolysis by mucous enzymes
• Nonspecific bind bacteria
• Antiinflammatoryefect (opsonin, neutralisation,phagocytes inhibition, do not activatecomplement)
• Sensitive to bacterial protease splitting(IgA1)

Immunoglobulin A - II.
• IgA1• IgA2• synthesis 24 mg/kg/day
(IgG 33 mg/kg/day)• liver transport and
catabolism
• 80 % serum IgA (87 % IgA monomer)
• Bown marrow (A2) andmucous (A1)

Oral tolerance
• Do not react to protein antigenes administeredto mucous tissue
• It is possible to change it by adding ofadjuvance
Mechanisms: • active supression by T
cells – secretion of TGF-b (Th3) and Treglymphocytes –secretion of IL-10
• clonal anergy
Immunity against extracelullar bacteria
• antibodies• complement• lectins+ phagocytosis and
killing (NADPHoxidase) by neutrophils
• Bacteria produce toxins(neutralisating Ab), capsulated bacteria(Streptococckai, Hi), polysascharide Ag (pneumococcai, H., meningococcai)
• Neisseriae (sensitive to complement MLC)
• Staphylococcai
Opsonisation by
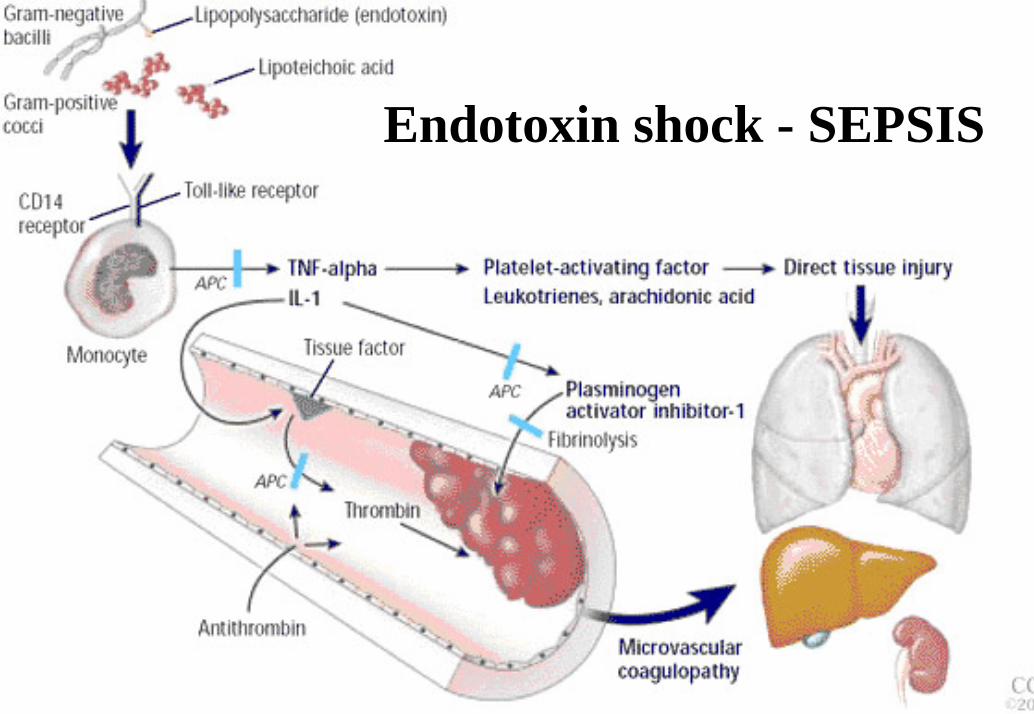
Endotoxin shock - SEPSIS

Defence against S. pneumonie
• Adhesion to epithelial cell surface
• Complementactivation via alternative and classical pathway
• opsonisation • Spleen function
Pathogenicity is caused by: • Mucous damage• Complement defects and
granulocyte defects infunction and number
• Ab defects
• Status after splenectomy

Defence against Str. pyogenes (A)
• Semmelweiss –puerperal sepsis, childbed fever
• M protein - resistence to phagocytosis
• Toxins production• cross antibodies
reactivity against M proteins
• antisepsis
• opsonisation• neutralisation• Rheumatic fever,
glomerulonefritis• (genetic determine
sensibility)

Defence against intracellular bacteria
Pathogens characteristics• intracelullar parasites• low toxicity• Mycobacteria, ListeriaLegionela
Defence mechanisms• In lysosomes -Th1, IFNg• macrophages,
granulomatous reaction• In cytoplasm – CD8• Antibodies play no role• Defence is almost always
connected with disease
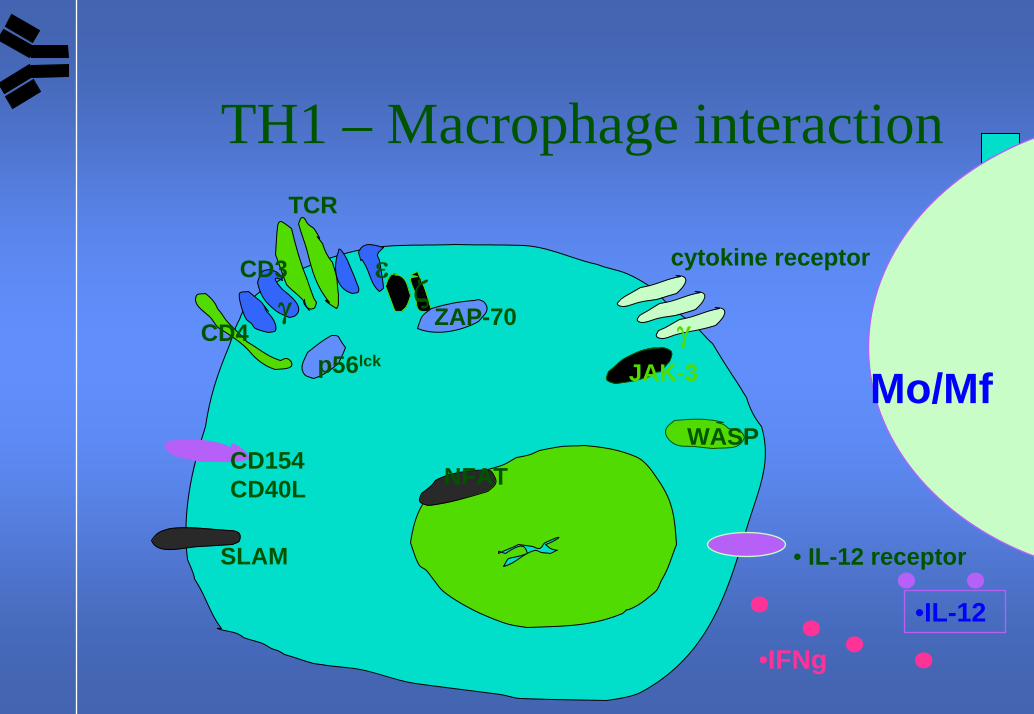
TH1 – Macrophage interactionTCR
CD3γ
εζ
ZAP-70
cytokine receptor
γJAK-3
WASP
p56lckCD4
CD154CD40L
SLAM
NFAT
• IL-12 receptor
Mo/Mf
•IL-12
•IFNg
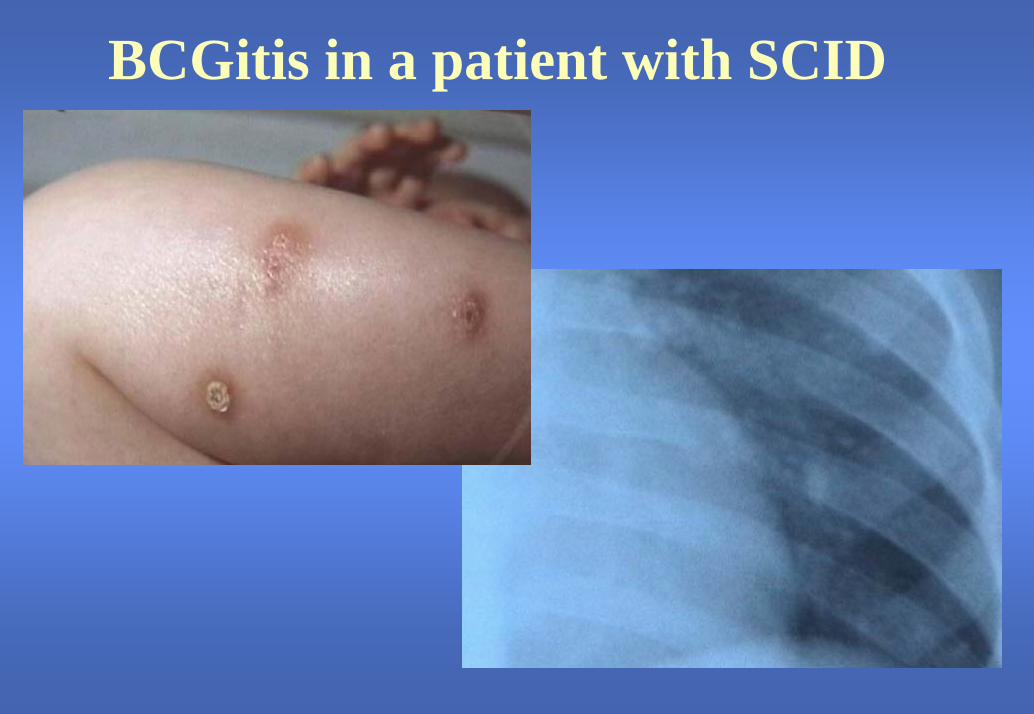
BCGitis in a patient with SCID

Defence against virusesPathogenicity mechanisms• using receptors• Obligate intracellular
parasites• Production of inhibiting
factors
Defence mechanisms• inteferons• NK cells• antibodies• Regional lymphnodes
- APC, T and B lymphocytes
• effector CD8 i CD4 lymphocytes
Use of host receptorsSurface molecule Physiological ligand;
(function) Microorganism
CD4 MHC gp II, IL-16 HIV, herpersvirus 7
CD21 (CR2) C3dg, CD23 EBV
CD46 (MCP) (complement regulation) Measles virus, herpesvirus 6
CD54 (ICAM-1) LFA-1 (CD11a/CD18) Rhinoviruses, Plasmodium malariae
CD55 (DAF) (complement regulation) Echovirus R
CD71 Transferin Hepatitis B virus
CD150 (SLAM) CD150 Mesles virus
β1 integrins Extracellular matrix proteins Yersinia, patgogenic E. coli
CR3 (αMβ2 integrin) C3b, CD23 aj. Mykobakterie, Legionella, Bordetella, Leishmania
β3 integrines (αΙΙβ3) Fibronectin Borrelia
Erythrocyte P antigen ? Parvovirus B19
LDL receptor LDL Rhinovirus HRV2

Different types of virus infectionsInitial infection consequences example
acute Recovery and elimination of virus
Inluenza virus, rotavirus
acute Latency (non-infectious virus); on
reactivation, new viruses are shed
Varicella zoster virus, herpes simplex
virus
acute Persistence with continuance or
intermittent shedding
Hepatitis B virus, EBV
not acute Persistent slow infection
Creutzfeld-Jacob disease, scrapie
Defence against viruses
Pathogenicity mechanisms• using receptors• Obligate intracellular
parasites• Production of inhibiting
factors
Defence mechanisms• inteferons• NK cells• antibodies• Regional lymphnodes
- APC, T and B lymphocytes
• effector CD8 i CD4 lymphocytesInfluenza
Ag driftInfluenzaAg shift
Antv.mov
Defence against fungi
Characteristics:• oportunne pathogens• Systemic disease only
in immunodeficiencies(Candida, Aspergillus,
Nocardia)
Defence mechanisms• neutrophils• monocytes and
macrophages• Th1 lymphocytes• Antibodies plays no
role

Lung aspergilosis, peripheral parenchyme condensation, nodules. Patient with chronic granulomatous disease, CGD, (inherited defect of phagocytosis – NADPH oxidase

• Lung nocardiosis, Dg CID• Brain - 2001• recidive 2002 (exitus)
Patient AJ,1983
ring saturation in occipit. Left lobe – nocardiosisabscessus
Nodule in right upper lobe dorsal With cavitation in lung nocardiosis

Immunity against protozoa
Character of the infection: chronic latente asymtomatic reactionhost specific
Antigenne variation, different development stage with different Ag
(Plasmodium,Entamoeba,Giardia,Trypanosoma,Leishmania,Toxoplasma,
Trichomonas...)
Protective immunity: cytokinebalance/dysbalance leads to infection character(Th1)
Decrease resistance of organism leads to clinicalmanifestation

Immunity against Spirochettes
Course of infection:primaresecundareterciare(Treponema, Borrelia,
Leptospira)
Defence mechanisms:antibody reactionTh1Failure of immune
mechanismsimunopathology: CIC,
autoantibodies

Immunity against multicell parasites
Pathogen• chronic infections with
long persistance• high morbidity, low
mortality• Do not multiply in
final organism - cycles• Reinfection(Toxocara, Taenia,
Enterobius, etc.)
Escape mechanisms• secvestration• Molecular mimicres• No expresion of
surfice molecules• secretion inhibiting
factors or proteases• Blocking antibodies
Immunity against multicell parasites II.
Pathology• Imunocomplexes
production• autoantibodies• granulomatous
reaction• alergic reactions
Physiology• Mechanic eviction• Mast cells• eosinophils• Th2• IgE • monocytes• Th1, CD8+
Hygiene hypothesis – more parasites, less alergies??
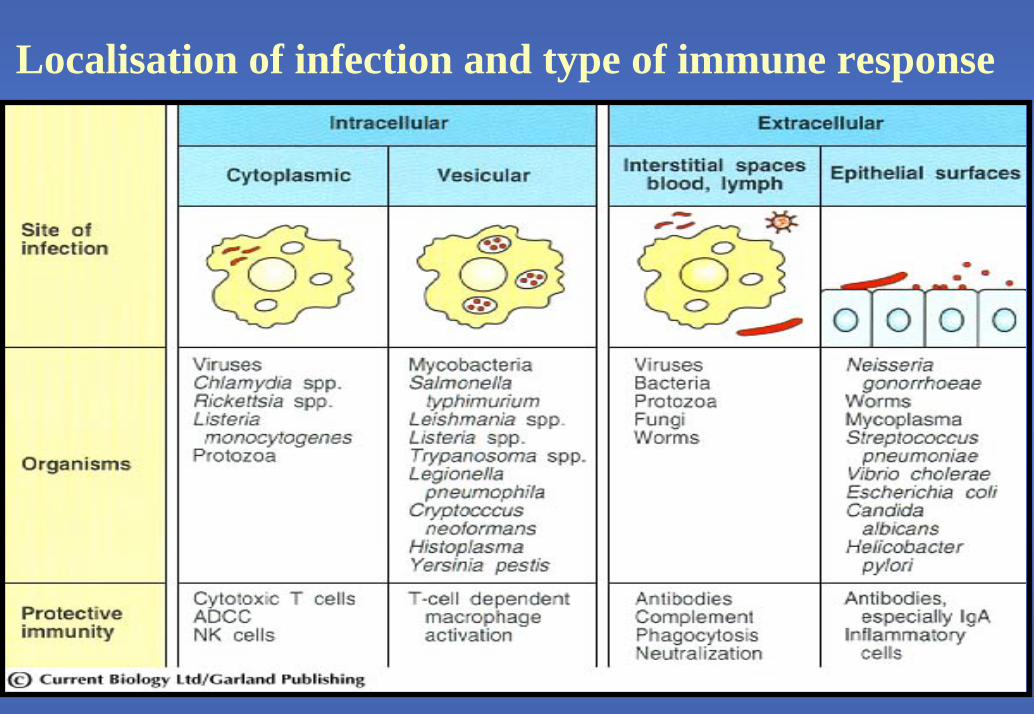
Localisation of infection and type of immune response

Vaccination
= Active immunizationSpecific immune reaction to given antigen to reach long term immune memory (protective circulatingantibodies, memory lymphocytes –quicker immune response)

Types of vaccines• live attenuated microorganisms (polio oral-Sabin, BCG, MMR, yellow fever, VZV)• inactivated whole microorganisms (polio-Salk, rabies, VHA, influenza, typhus, pertussis, typhoid, cholera)• subunit vaccines – capsular polysaccharides (pneumococcus, meningococcus, Hib)
- surface antigen (VHB)• recombinant vaccines – gene cloned and expressed (VHB)• toxoids (tetanus, diphtheria)•Adjuvans – enlargement vaccine immunogenicity (aluminium salts, Bordetella pertussis), enhance Ab production,stimulation of inflammation, DC activation, antigen longer time in organism

Memory B cell
Stimulated T-lymphocyte
T cell
Stimulated B-lymphocyte
Stimulated B-lymphocyte
differentiation
Plasmatic cellStimulated
B-lymphocyte
proliferation
proliferation
3. T-D (Thymus dependent exodogenous antigen), complex, live and atenuated vaccines (BCG, polio)
2. T-D (Thymus dependent endogenous antigen), protein, most of vaccines
1. T-I (Thymus independentendogenous antigen), polysaccharide (Pneumococcal vaccine, Meningococcus)
B-cell
TypesTypes of of vaccinationvaccination in CZin CZ
•• Compulsory Compulsory by by lawlaw ((§§ 258/2000 sb.)258/2000 sb.)regularregular ((vaccination calendarvaccination calendar))special special ((people at higherpeople at higher risk)risk)extraordinaryextraordinary (severe(severe epidemiological epidemiological situationsituation))
•• VaccinationVaccination onon requestrequest

Compulsory vaccinationCompulsory vaccination in CZin CZ
• TBCTBC•• PertussisPertussis, tetanus, , tetanus, diphtheriadiphtheria,, Haemophilus Haemophilus
influenzaeinfluenzae serotypeserotype b (b (HibHib))•• Hepatitis BHepatitis B•• RubellaRubella,, measlesmeasles,, mumpsmumps•• Polio Polio

Advantagages of vaccination before getting infection
• lower pathogenicity of vaccine than infectious agens
• avoid severe demage of target organs• timing of aplication• vaccine combination

ContraindicationsContraindications forfor vaccinationvaccination•• ForFor inactive vaccinesinactive vaccines:: acute illnessesacute illnesses, , during andduring and 2 2 weeksweeksafter illnesses with high feversafter illnesses with high fevers, , severe severe allergic reactions after previous vaccinationsallergic reactions after previous vaccinations,,pregnancypregnancy•• ForFor live vaccineslive vaccines:: the same abovethe same above++ immunodeficiencyimmunodeficiencytherapy with glucocorticoidstherapy with glucocorticoids,, antimetabolitsantimetabolits,,radiationradiation, ACTH, ACTH3 3 month after blood transfusionmonth after blood transfusion, plasma, plasma or Ig or Ig substitution substitution bone bone marrow malignanciesmarrow malignancies
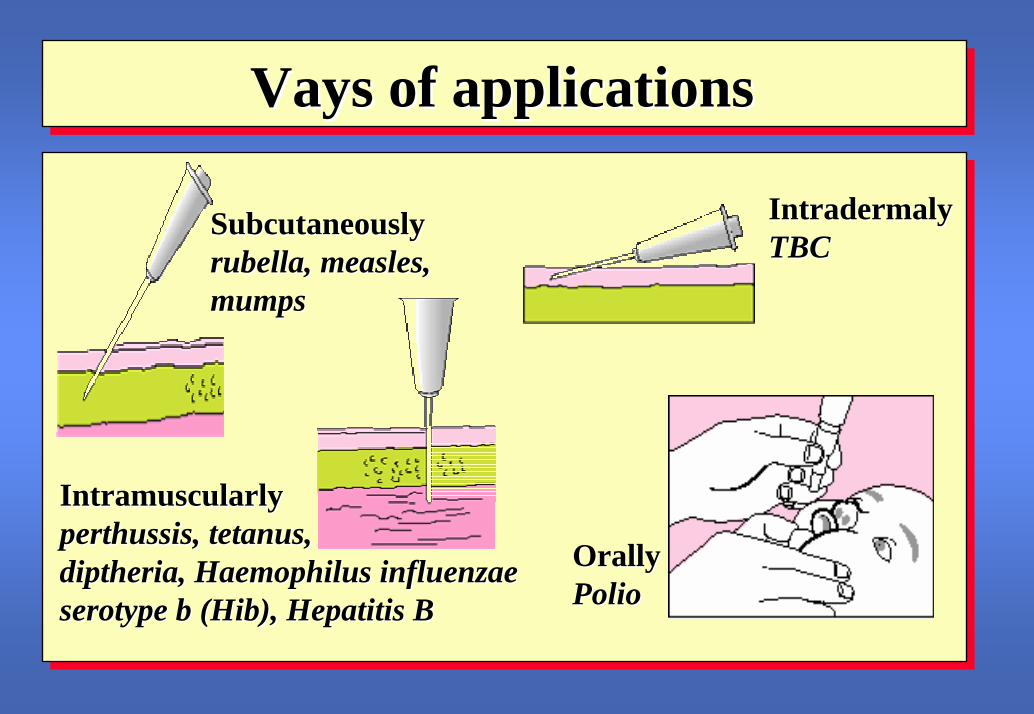
VaysVays ofof applicationsapplications
OrallyOrallyPolioPolio
IntradermalyIntradermalyTBCTBC
SubcutaneouslySubcutaneouslyrubellarubella,, measlesmeasles,,mumpsmumps
IntramuscularlyIntramuscularlyperthussisperthussis, tetanus,, tetanus,diptheriadiptheria,, Haemophilus influenzae Haemophilus influenzae serotypeserotype b (b (HibHib), Hepatitis B ), Hepatitis B

Vaccination in future
• recombinant vaccines (food like vaccines)• using genes and vectors to deliver Ag• vaccines against chronic infections (EBV, HIV, malaria)
• eradication of severe infections• decrease infection mortality and morbidity • vaccinating against cancer