improving access by improving utilization€¦ · · 2015-04-28improving access by improving...
TRANSCRIPT
Improving Access
by
Improving Utilization
November 12, 2012
Gina Cronin
Nate Hurle

Agenda
• What is Access?
• How is Access managed?
• Utilization Improvements in Outpatient
Setting
• How to rapidly expand improvements?
What is Access?

Key Access Measures

Cleveland Clinic
Access to Care
Right Patient with Right
Caregiver at Right Time

Appointment Access
Pre-2010
• Decentralized by department
• Personalized by provider preferences
• Highly variable by time of day
• Highly variable by staffing levels
• Disproportionate Resources
Huge Variations Average Speed of Answer
Call Abandonment

To provide an ideal patient experience by creating an environment
that delivers improved patient access to services
Efficiency
Patient
Experience
Access
Cleveland Clinic Contact Center:
The Vision
Caregiver Fears
• Loss of Control
• Wrong patients on Schedule
• Subspecialty knowledge
• Same Day Access/Nightmare
Centralized Approach >>>> Physician Mistrust

At Cleveland Clinic
• 1.5+ Million Annual
Appointments
• For 2,700+ Physicians
• In 26 Institutes
• At 25 Regional Locations
• Through 1 Access
Number
At Cleveland Clinic
Future State
• Single Point of Access
• First Time Call Resolution
• Priority Handling for Appointment Calls
• Consistent Patient Interaction
• Improve template utilization

Now Appointment Center:
• Physical Location:
- 250 Schedulers (and growing)
• Skilled Work-team:
- Schedulers for all Departments and Locations
• Technology-enabled:
- Epic Front-end Scheduling System
- Comprehensive, Specialty-Specific Questionnaires

Now Appointment Center:
• Physical Location:
- 185 Schedulers (and growing)
• Skilled Work-team:
- Schedulers for all Departments and Locations
• Technology-enabled:
- Epic Front-end Scheduling System
- Comprehensive, Specialty-Specific Questionnaires
Appointment Scheduling
as Patient Service


1) Right Appointment
2) Right Physician
3) Right Place
Clinically-Driven, Technology-Enabled
Appointment Scheduling as a Patient Service
1 + 1 Number Scheduler
= 3 + 1 Nurse

Institute Ambulatory Issues
• Provider Complaints…..
- Need more rooms
- Need more support staff
• Chairman and Administrator Partnership
with Continuous Improvement
• Deploy team to assess and recommend

Is This Access?
Institute Ambulatory Issues
• What is Reality….
• Are the rooms level scheduled?
• Are patients happy with the experience?
• Are we really managing throughput?

Outpatient Clinics
• OPDs while clinically different are
operationally similar
• We don’t have a space problem
- We have a perception of a space
problem
- The utilization of current resources
is ineffective
• We do have a patient wait time problem

Analytical Approach
1. Conduct internal caregiver survey
2. Review of Patient Experience Data
3. Perform Observational Analysis
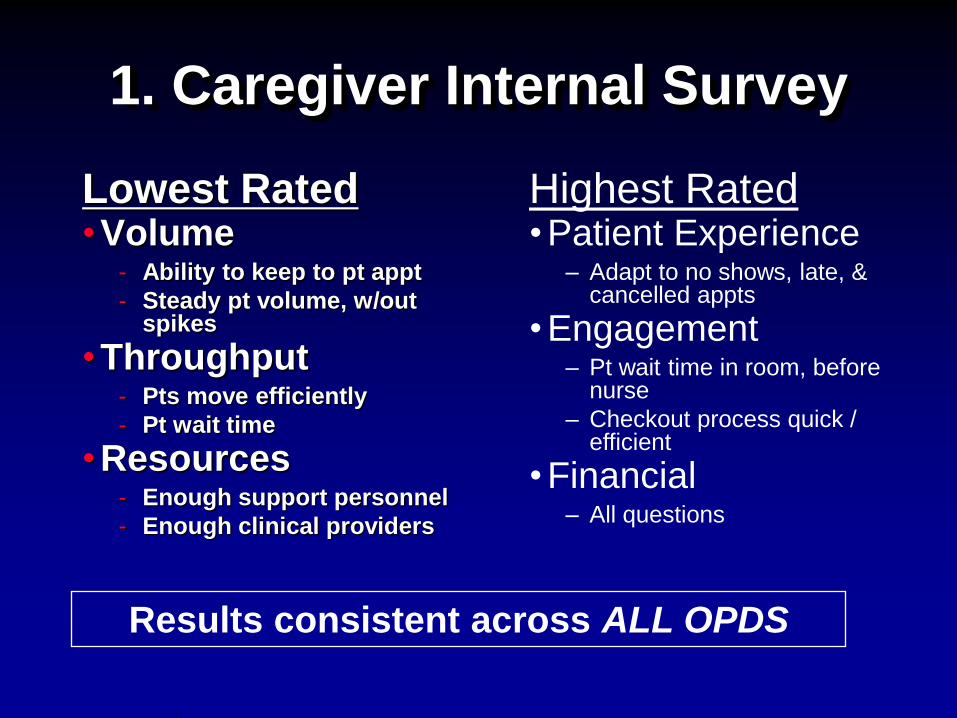
1. Caregiver Internal Survey
Lowest Rated • Volume
- Ability to keep to pt appt
- Steady pt volume, w/out spikes
• Throughput - Pts move efficiently
- Pt wait time
• Resources - Enough support personnel
- Enough clinical providers
Highest Rated • Patient Experience
– Adapt to no shows, late, & cancelled appts
• Engagement – Pt wait time in room, before
nurse
– Checkout process quick / efficient
• Financial – All questions
Results consistent across ALL OPDS
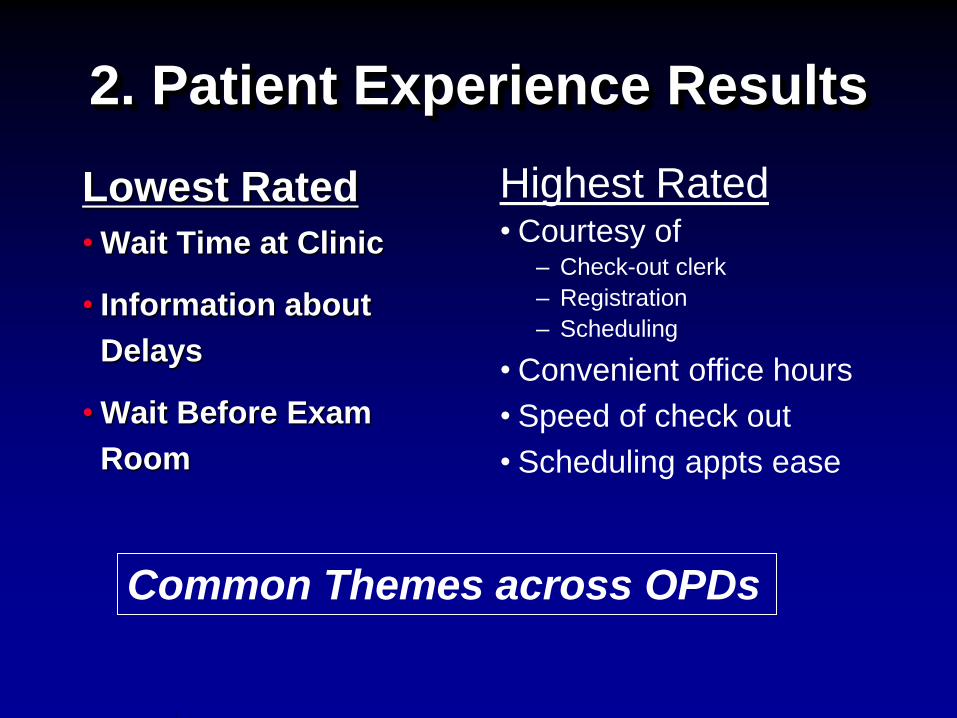
2. Patient Experience Results
Lowest Rated
• Wait Time at Clinic
• Information about
Delays
• Wait Before Exam
Room
Highest Rated • Courtesy of
– Check-out clerk
– Registration
– Scheduling
• Convenient office hours
• Speed of check out
• Scheduling appts ease
Common Themes across OPDs
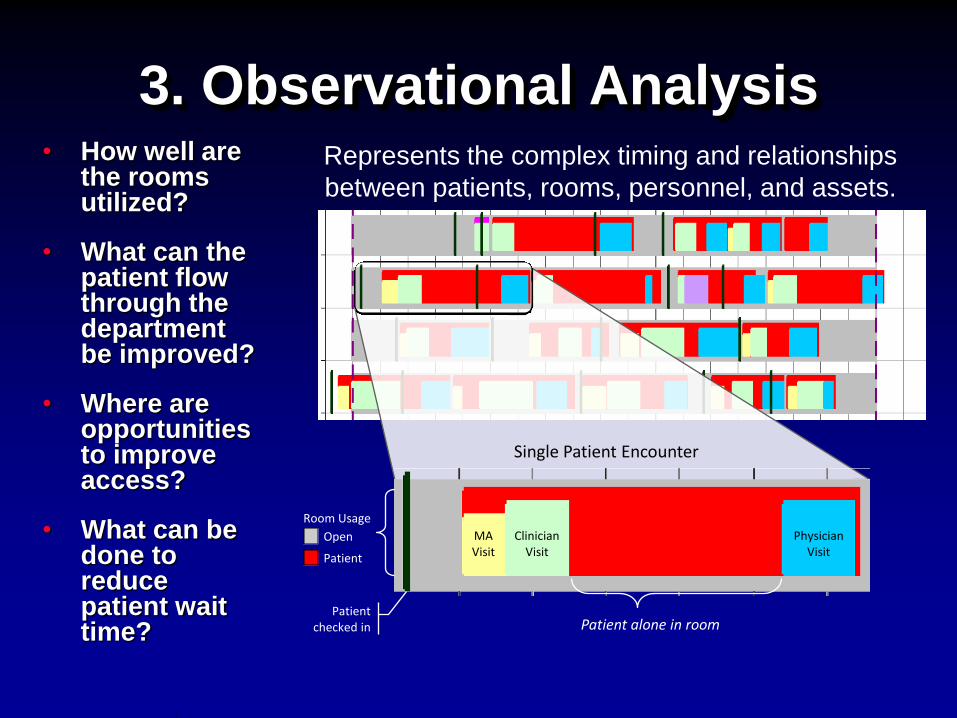
3. Observational Analysis • How well are
the rooms utilized?
• What can the patient flow through the department be improved?
• Where are opportunities to improve access?
• What can be done to reduce patient wait time?
Represents the complex timing and relationships
between patients, rooms, personnel, and assets.
Single Patient Encounter
Open
Patient
Room Usage
Patient alone in room Patient
checked in
MA Visit
Clinician Visit
Physician Visit
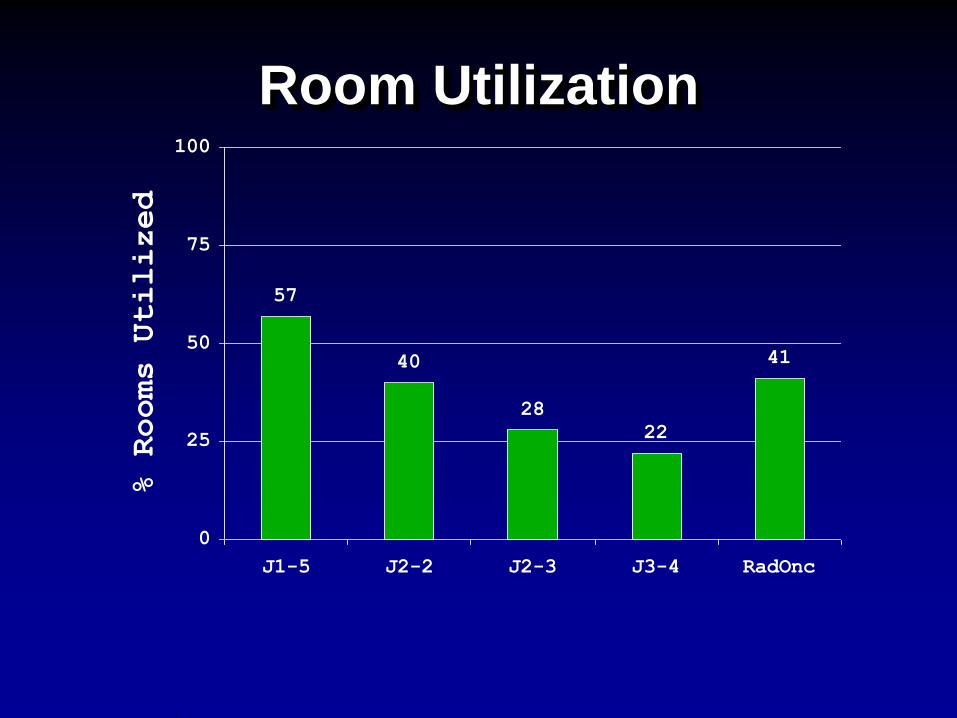
Room Utilization
57
40
28
22
41
0
25
50
75
100
J1-5 J2-2 J2-3 J3-4 RadOnc
% Rooms Utilized

Patient Total Visit Time
44 4063
33
144
31
5131
59
37
59
28
0
50
100
150
200
250
J1-5 J2-2 J2-3 J3-4 J4-1
(TCI)
RadOnc
Total Visit (mins)
Time Waiting Time With Provider

Utilization of Outpatient Departments
• “We need more rooms and support staff to see more patients” - Volume by 15% without more support staff or
rooms
- Decreased patient visit time by 22%
Process Changes
• Level schedule by day and within day
• Adjusted work content for MAs and RNs
• Changed room allocation
“The greatest waste, is the waste we don’t see.”
- Shigeo Shingo
Effective Way to See the Waste
• Real-Time Location Systems
- Patients and Caregivers wear Badges
- Sensors detect locations
- Software provides real-time views

Real-Time Views
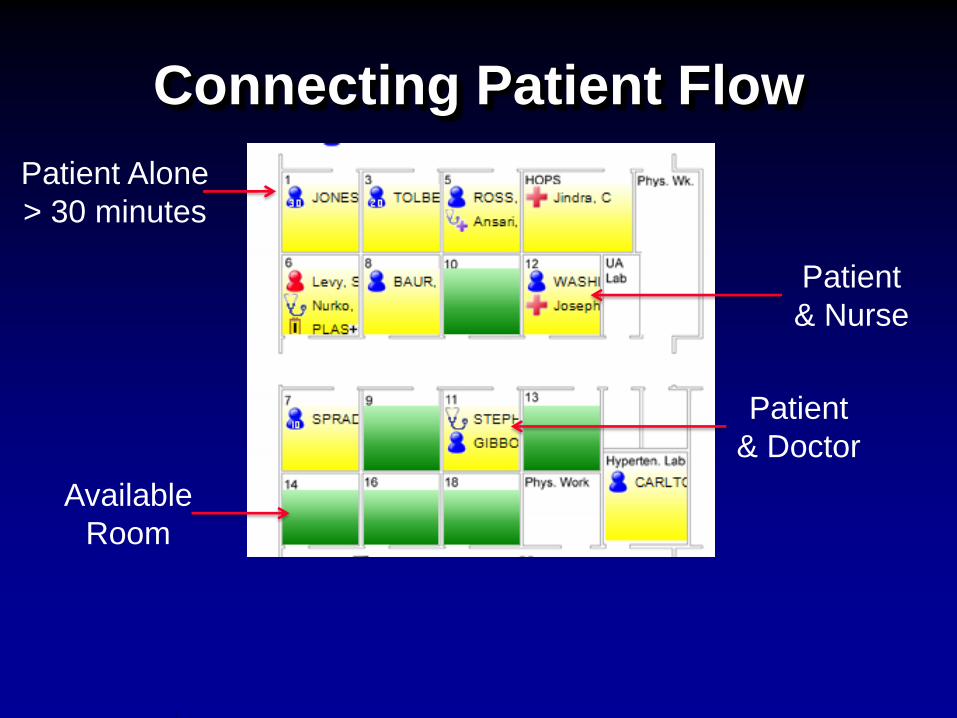
Connecting Patient Flow
Patient
& Nurse
Patient
& Doctor
Available
Room
Patient Alone
> 30 minutes

Direct Connections
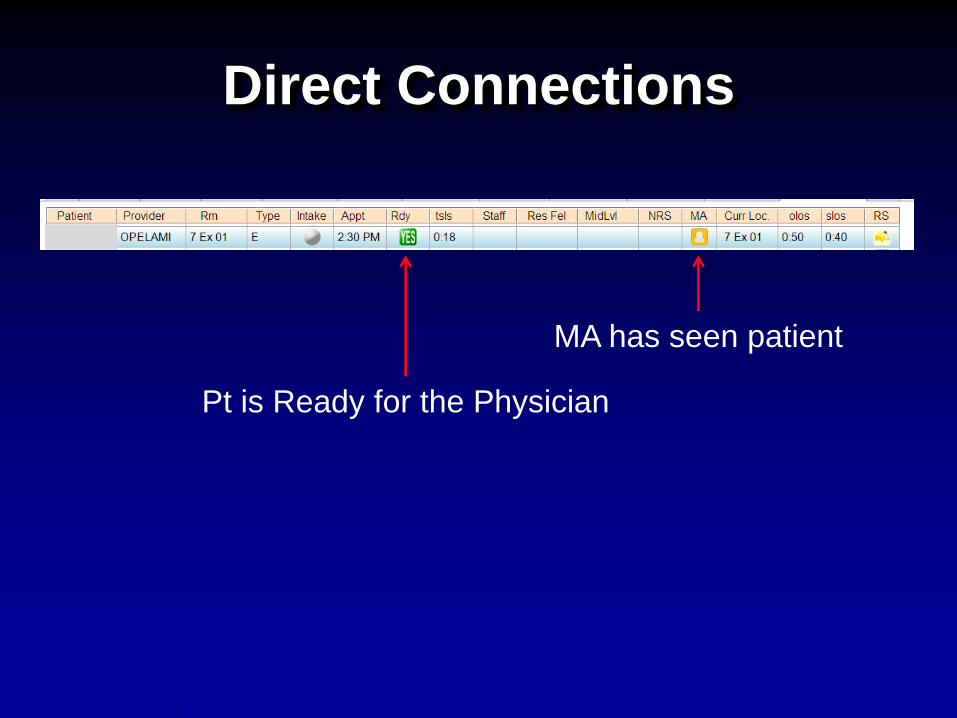
Direct Connections
MA has seen patient
Pt is Ready for the Physician

How is the system performing?
Visit : 1:50- 4:20
Provider: 52 mins
Pt Alone: 148 mins

Room Utilization
Low Room Usage
Low Usage
Early Afternoon

Conclusion
• Create baseline measures to
understand how resources are utilized
today
• Develop system for ongoing
measurement and communication
• Modify process to improve utilization
before adding resources
Thank You!
Questions?
