improving orthopedic value from the buy side – perspectives from the alliance minnesota health...
TRANSCRIPT
Improving Orthopedic Value from the Buy Side –
Perspectives From The Alliance
Minnesota Health Action GroupCommunity Dialogue
Improving Value for Hip and Knee Replacements
March 28, 2014
About The Alliance®
> Not-for-profit, employer-owned cooperative• Shareholders = customers
> Founded in 1990 by 7 employers; now over 200 employers
• 90,000 employees and family members• 23 counties in WI, IA and IL• $500,000,000 in health care/yr
> Move health care forward by controlling costs, improving quality and engaging individuals in their health
Our Genesis
> Mid 1980’s: State of WI pursues “managed competition”
> Large multi-specialty medical groups and hospitals form their own HMO’s– Favorable unit prices made up by shifting
costs to the rest of the market> 1990: The Alliance
– Direct contracting with providers, data warehouse, cost and quality comparisons

Employer Perspectives on Orthopedic Care
1. Source of significant and rising costs2. Increase in volume
> Shift to younger patients> Questions about appropriate use (NEJM Sept
11, 2008)
3. Uncertain quality> Limited information to distinguish better and worse
performance
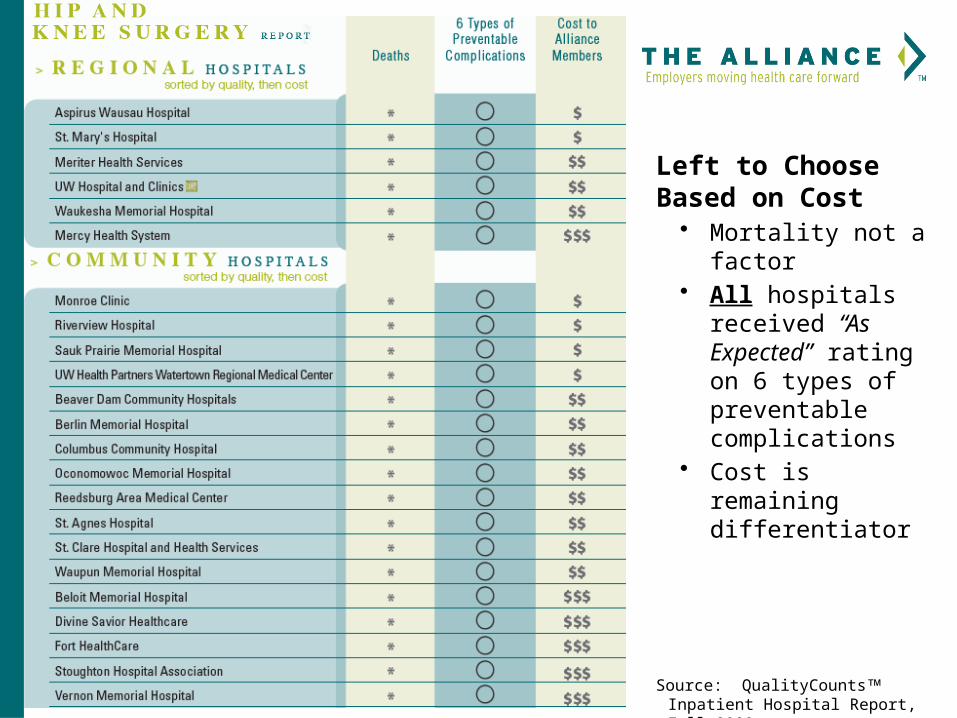
Left to Choose Based on Cost
• Mortality not a factor• All hospitals
received “As Expected” rating on 6 types of preventable complications
• Cost is remaining differentiator
Source: QualityCounts Inpatient Hospital Report, Fall 2009
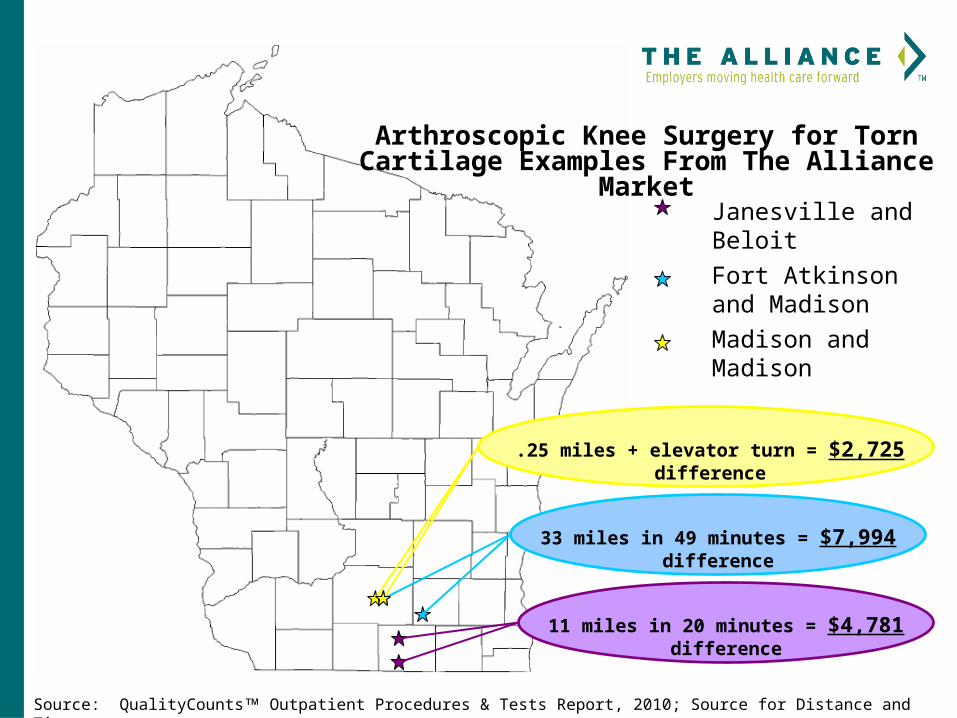
33 miles in 49 minutes = $7,994 difference
Arthroscopic Knee Surgery for Torn Cartilage Examples From The Alliance Market
.25 miles + elevator turn = $2,725 difference
11 miles in 20 minutes = $4,781 difference
Source: QualityCounts Outpatient Procedures & Tests Report, 2010; Source for Distance and Time: www.mapquest.com
Fort Atkinson and Madison
Janesville and Beloit
Madison and Madison
AAOS’ Modest Choosing Wisely List
1. Avoid performing routine post-operative deep vein thrombosis ultrasonography screening in patients who undergo elective hip or knee arthroplasty
2. Don’t use needle lavage to treat patients with symptomatic osteoarthritis of the knee for long-term relief.
3. Don’t use glucosamine and chondroitin to treat patients with symptomatic osteoarthritis of the knee.
4. Don’t use lateral wedge insoles to treat patients with symptomatic medial compartment osteoarthritis of the knee.
5. Don’t use post-operative splinting of the wrist after carpal tunnel release for long-term relief.
The QualityPath to Higher Value
1. Identify common, expensive elective procedures
2. Evaluate physicians + hospitals on important quality measures and characteristics
• Involve clinicians in the process
3. Negotiate lower bundled payments
4. Use benefit plan designs to move market share to high value physicians + hospitals
Common, Expensive Elective Procedures
> Heart Bypass Surgery> Elective Angiography and Angioplasty> Knee Replacement> Hip Replacement
Unit of Analysis
> Physician/surgeon + Hospital Pairs– Physician-level information important to
employers to create benefit plan-based incentives> Variation in performance between physicians> Role of steward/fiduciary of resources
– Impact of ordering and billing practices– Specialists account for 8 – 15% of charges, but can
control/influence much more
Hip and Knee Criteria
1. Registry Participation• Accelerate progress to include patient-reported
outcomes
2. Full transparency with results at or above average for individual physicians + hospitals
• 5-year revision rates• THA/TKA 30-day readmission rates• THA/TKA complication rates• Patient experience/CAHPS results• Additional measures via CMS “Compare”
programs
Hip and Knee Criteria cont.
3. Standardized Clinical Processes in Routine Usea. Consistently collected pre and post
patient-reported outcome measures
b. Decision support for ordering high tech imaging (e.g. MRI)
c. Shared decision-making > Quality of process assessed
4. Pre-procedure joint school
Hip and Knee Criteria cont.
5. Disclosure of all industry payments to patients
6. Conversation about future care needs documented in an advanced directive, as appropriate
Quality First, Then Price
> Bundled payments for episodes of care Less than today’s reimbursement
Employer Commitment
> Benefit plans to encourage patients to use QualityPath designated hospital and physicians Reference pricing: 100% coverage for
QualityPath providers Lower co-pays and deductibles for
QualityPath providers
Positive Incentives> Patients
Better odds of getting appropriate, high quality care Lower cost Easy to understand and use
> Physicians and Hospitals Reputation – public reporting, QualityPath designation Financial – greater market share
> Employers Better odds of getting appropriate, high quality care Lower cost
Process and Timeline
1. Provider engagement - ongoing
2. Quality criteria established – review and comment period: Jan 2014
3. RFI released – Feb 13
4. Responses due – April 3
5. Employer engagement – ongoing
6. Evaluation period – April 4 – April 27 Feedback to applicants – April 27 – 30
Process and Timeline cont.
7. Designated hospitals + surgeons announced
8. Contract Negotiations: 5/1 – 9/1 Aggressive bundled pricing + warranties
9. Benefit plan design: 5/1 – 8/1
10.Consumer support: 2/1 – 12/1
11.Evaluation: 2/14 - ongoing